Embed Size (px)
Citation preview

Stroke RoundsStroke Rounds
Core RoundsCore Rounds
Shawn DowlingShawn Dowling
Preceptors: Dr. Coutts, Dr. VipondPreceptors: Dr. Coutts, Dr. Vipond

Thank yousThank yous
Dr. Colleen CareyDr. Colleen Carey Dr. R Burton-MacLeodDr. R Burton-MacLeod Dr. CouttsDr. Coutts Dr. VipondDr. Vipond

Outline Outline
Defining strokeDefining stroke PathophysiologyPathophysiology Stroke syndromesStroke syndromes ThrombolyticsThrombolytics Hypertension management in acute Hypertension management in acute
strokestroke TIATIA ICHICH

EpidemiologyEpidemiology
Stroke is the #3 leading cause of Stroke is the #3 leading cause of death and # 1 cause of disability in death and # 1 cause of disability in adultsadults
In-hospital mortality rates = 15%, In-hospital mortality rates = 15%, 30-day mortality rates = 25%30-day mortality rates = 25% Of those that survive Of those that survive
– 50% are fully functional, 50% are fully functional, – 30% are disabled and 30% are disabled and – 20% are institutionalized20% are institutionalized

Definitions - StrokeDefinitions - Stroke Stroke = Stroke =
permanent permanent neurological deficit neurological deficit of vascular of vascular etiology (>24 etiology (>24 hours)hours)
TIA= transient TIA= transient neurological deficit neurological deficit of vascular of vascular etiology (<24 etiology (<24 hours)hours)

Risk Factors – ischemic Risk Factors – ischemic stroke ?stroke ?
Non-modifiable:Non-modifiable:– AgeAge– Family historyFamily history– Gender (M>F)Gender (M>F)– RaceRace
Modifiable:Modifiable:– DiabetesDiabetes– HypercholesterolemiaHypercholesterolemia– Cardiovascular diseaseCardiovascular disease– A fibA fib– SmokingSmoking– AlcoholAlcohol– Inactivity Inactivity – TIA TIA – Carotid stenosisCarotid stenosis

Case #1Case #1
70F. R sided arm/ (leg) hemiparesis 70F. R sided arm/ (leg) hemiparesis + aphasia from Retirement lodge. + aphasia from Retirement lodge. EMS arrives BP 175/75, HR-80(reg), EMS arrives BP 175/75, HR-80(reg), RR16, sats=98%, T=36.3.RR16, sats=98%, T=36.3.
DDx?DDx?

Acute stroke differential diagnosisAcute stroke differential diagnosis
Focal CauseFocal Cause Lower motor neuron Lower motor neuron
disorders (Lyme, Bell’s)disorders (Lyme, Bell’s) Intracerebral hemorrhageIntracerebral hemorrhage Brain tumorBrain tumor Brain abscessBrain abscess Infective endocarditis with Infective endocarditis with
cerebral embolicerebral emboli MigraineMigraine Head trauma – EDH/SDHHead trauma – EDH/SDH Seizures/Todd's paralysisSeizures/Todd's paralysis
Diffuse/Systemic CauseDiffuse/Systemic Cause HypoglycemiaHypoglycemia HHNKHHNK Functional deficit Functional deficit
(conversion disorder)(conversion disorder) Encephalopathy (HTN, Encephalopathy (HTN,
hepatic, metabollic)hepatic, metabollic) IntoxicationIntoxication
Stroke mimic rate consistently around 10%

Case Case
78M suffered a large hemispheric 78M suffered a large hemispheric stroke. stroke.
Mechanisms of strokes?Mechanisms of strokes?– What if I told you he was HTN, smoker, What if I told you he was HTN, smoker,
diabetic, prior MI?diabetic, prior MI?– Known afib – not compliant with medsKnown afib – not compliant with meds– In the ICU with Septic shockIn the ICU with Septic shock– Hx of nephrotic syndromeHx of nephrotic syndrome

Mechanisms of ischemic strokeMechanisms of ischemic stroke Thrombosis (MC)Thrombosis (MC)
– Large vesselLarge vessel– Small vesselSmall vessel
EmbolusEmbolus– Cardiac sourceCardiac source– Artery –to- artery Artery –to- artery – IdiopathicIdiopathic
HypoperfusionHypoperfusion Blood disorders (i.e. sickle cell, HIT, Blood disorders (i.e. sickle cell, HIT,
hypercoagulable)hypercoagulable)

Vascular AnatomyVascular Anatomy

Vascular AnatomyVascular Anatomy

Anterior vs Posterior circulationAnterior vs Posterior circulation

What does the Anterior What does the Anterior Circulation Supply?Circulation Supply?
www.strokecenter.org

What does the Posterior What does the Posterior Circulation Supply?Circulation Supply?
www.strokecenter.org

Vessel? Deficits?Vessel? Deficits?

Anterior cerebral artery s/oAnterior cerebral artery s/o

ACAACA
Frontal lobe dysfunctionFrontal lobe dysfunction Contralateral motor and sensory Contralateral motor and sensory
deficits LE>UEdeficits LE>UE Apraxia/Clumsiness Apraxia/Clumsiness ConfusionConfusion Primitive reflexesPrimitive reflexes Bowel/Bladder IncontinenceBowel/Bladder Incontinence

Vessel? Abnormality?Vessel? Abnormality?

Middle cerebral artery syndromeMiddle cerebral artery syndrome(MC)(MC)

MCA strokeMCA stroke Contralateral hemiplegiaContralateral hemiplegia
– Why can both the arm and leg be affected?Why can both the arm and leg be affected? Contralateral hemianopsiaContralateral hemianopsia Contralateral hemianesthesiaContralateral hemianesthesia Gaze Preference – towards or away from Gaze Preference – towards or away from
lesion? What about in a seizure?lesion? What about in a seizure? Dominant hemisphere: aphasia (types?), Dominant hemisphere: aphasia (types?),
apraxia – which is this for righties? lefties?apraxia – which is this for righties? lefties? Non-dom hemisphere:anosagnosia Non-dom hemisphere:anosagnosia
(neglect)(neglect)

Case from SaturdayCase from Saturday
75F. L Lacunar infarct May 975F. L Lacunar infarct May 9thth – Admitted – Admitted to stroke service – dopplers carotids. D/c to stroke service – dopplers carotids. D/c back to Fanning. Presents to ED 2 in the back to Fanning. Presents to ED 2 in the last week with last week with ↓LOC x 2 – CT at first visit ↓LOC x 2 – CT at first visit showed evolution of stroke but no bleedshowed evolution of stroke but no bleed
May 24May 24thth – sudden onset of ↓LOC – GCS 6 – sudden onset of ↓LOC – GCS 6 (E1V1M4).140/60, 80, 99%,36.5, c/s-11(E1V1M4).140/60, 80, 99%,36.5, c/s-11
Intubated by us in EDIntubated by us in ED What do you want to do ASAP?What do you want to do ASAP?

What could be 4 causes of her decreased LOC?

Decreased LOC in MCA strokeDecreased LOC in MCA stroke
SeizureSeizure
EdemaEdema
Old contralateral strokeOld contralateral stroke
Brainstem herniationBrainstem herniation

Vessel?Vessel?

PCA anatomyPCA anatomy
Branches off Branches off basilar arterybasilar artery– 30% from ICAs 30% from ICAs
Travels around Travels around midbrainmidbrain
Supplies midbrain, Supplies midbrain, thalamus, mesial thalamus, mesial inferior temporal inferior temporal lobe, occipital and lobe, occipital and occipitopariental occipitopariental cortices.cortices.

Posterior cerebral artery Posterior cerebral artery syndromesyndrome
Contralateral homonymous hemianopsiaContralateral homonymous hemianopsia Contralateral hemisensory deficitContralateral hemisensory deficit
– Usually no persistent motor deficitUsually no persistent motor deficit Memory disturbanceMemory disturbance AmnesiaAmnesia Visual agnosia Visual agnosia AlexiaAlexia A number of interesting presentations – A number of interesting presentations –
see emedicine article for listsee emedicine article for list

Lacunar strokesLacunar strokes
Lacune = LakeLacune = Lake
Cells necrose Cells necrose and are and are reabsorbedreabsorbed
A small cavity A small cavity is leftis left
www.strokecenter.org

Lacunar StrokesLacunar Strokes
Small zone of ischemia (0.2 to 15mm)Small zone of ischemia (0.2 to 15mm) Usually from a single penetrating vesselUsually from a single penetrating vessel Micro atherosclerosis or lipohyalinosis Micro atherosclerosis or lipohyalinosis Micro emboli of penetrating vesselsMicro emboli of penetrating vessels Fluctuate with timeFluctuate with time Better recovery and prognosisBetter recovery and prognosis Typically lack “cortical” signsTypically lack “cortical” signs
– aphasia, agnosia, neglect, apraxia, or aphasia, agnosia, neglect, apraxia, or hemianopsia hemianopsia

Lacunar SyndromesLacunar Syndromes
MC LocationsMC Locations Internal capsule Internal capsule Corona radiataCorona radiata Basal gangliaBasal ganglia BrainstemBrainstem

Lacunar syndromesLacunar syndromes Pure motor Pure motor
– Contralateral hemiparesisContralateral hemiparesis Mixed Sensorimotor Mixed Sensorimotor
– Hemiparesis/hemiplegia with ipsilateral Hemiparesis/hemiplegia with ipsilateral sensorysensory
Ataxia-hemiparesis Ataxia-hemiparesis – ipsilateral cerebellar and motor symptoms: ipsilateral cerebellar and motor symptoms:
weakness, clumsinessweakness, clumsiness Clumsy hand-dysarthria – pons lesionClumsy hand-dysarthria – pons lesion Pure sensory Pure sensory
– numbness/tingling/other sensations to half of numbness/tingling/other sensations to half of bodybody

CaseCase
Recall earlier case of patient who Recall earlier case of patient who clinically had a MCA strokeclinically had a MCA stroke
Sx started 60 minutes agoSx started 60 minutes ago What is the main reason to CT early?What is the main reason to CT early? What changes do you expect to see What changes do you expect to see
on CT?on CT? What changes could you see on CT?What changes could you see on CT?







CT findings of acute strokeCT findings of acute stroke Often normal 6-12H post-infarct, sensitivity best Often normal 6-12H post-infarct, sensitivity best
>24H>24HEARLY FINDINGS – seen in 61% of CT w/I 6HEARLY FINDINGS – seen in 61% of CT w/I 6H mass effect*mass effect* sulci effacementsulci effacement insular stripe sign(w/mca)insular stripe sign(w/mca) MCA sign/hyperdense artery - clot in mcaMCA sign/hyperdense artery - clot in mca acute hypodensity*acute hypodensity**only these signs are associated w/increased *only these signs are associated w/increased
bleedingbleedingrisk post-lysis BUT these are not contra-indications risk post-lysis BUT these are not contra-indications
Wardlaw JM; Mielke O . Early signs of brain infarction at CT: observer reliability and outcome
after thrombolytic treatment--systematic review. Radiology 2005 May;235(2):444-53

Case Case
56M. Brought in by cops for intoxication 56M. Brought in by cops for intoxication (stumbling around, slurred speech) and (stumbling around, slurred speech) and ongoing, intractable N,Vongoing, intractable N,V
VS N, c/s NVS N, c/s N You give him some fluids, thiamine, You give him some fluids, thiamine,
maxeran and send off some b.w. - would maxeran and send off some b.w. - would you send an EtOH on him?you send an EtOH on him?
EtOH <2.2EtOH <2.2 What do you want to do know?What do you want to do know?

Brainstem syndromesBrainstem syndromes

Vertebrobasilar systemVertebrobasilar system
The vertebral arteries The vertebral arteries and the basilar are and the basilar are straight arteries and straight arteries and therefore less likely to therefore less likely to form plaques than IC’s. form plaques than IC’s.
vertebral arteries vertebral arteries ascend through the s.c. ascend through the s.c. and enter the brain and enter the brain through the magnum through the magnum foramen foramen

Impressive nystagmus in both directions of gaze. Nystagmus at central position.
Loss of facial sensation on L Horners’ syndrome on L
– Best way to assess for miosis? Falls to L when walking Loss of pain and temperature
sensation on R side of body

Wallenberg (aka PICA Wallenberg (aka PICA syndrome)syndrome)
Contralat body pain and temp loss - LSTContralat body pain and temp loss - LST Ipsilat facial pain and temp loss – CN VIpsilat facial pain and temp loss – CN V Nystagmus/NV/vertigo – CN VIIINystagmus/NV/vertigo – CN VIII Hoarse/Dysphagia/dysarthria –CN IX, XHoarse/Dysphagia/dysarthria –CN IX, X Ipsilateral Horner syndrome – Sympathetic Ipsilateral Horner syndrome – Sympathetic
chainchain Ipsilateral ataxia - cerebellumIpsilateral ataxia - cerebellum

Brainstem strokesBrainstem strokes
In particular cerebellar strokes – In particular cerebellar strokes – NCCT does not visualize the posterior NCCT does not visualize the posterior fossa very well – because of artifactfossa very well – because of artifact
As a result – ask for posterior fossa As a result – ask for posterior fossa cuts – thinner slices cuts – thinner slices
May need CTA or MRI if high clinical May need CTA or MRI if high clinical suspicionsuspicion

CaseCase
67M. Suddenly became 67M. Suddenly became unresponsive – witnessed by wife. unresponsive – witnessed by wife. Preceded by nausea and vomiting, Preceded by nausea and vomiting, and some bizarre behaviour and some bizarre behaviour (answering questions (answering questions inappropriately), and increasingly inappropriately), and increasingly drowsydrowsy
GCS – 9 (E3V2M4), pinpoint pupils,GCS – 9 (E3V2M4), pinpoint pupils, DDx? General approach? Strokes?DDx? General approach? Strokes?

Top of the basilar syndromeTop of the basilar syndrome
Occlusion of the top of the basilar artery Occlusion of the top of the basilar artery can cause ischemia to midbrain, thalami, can cause ischemia to midbrain, thalami, and temporal and occipital lobe and temporal and occipital lobe
Clinical picture can be very confusingClinical picture can be very confusing Multiple emboli give a variable Multiple emboli give a variable
presentationpresentation Must be on your differential for sudden Must be on your differential for sudden
unexplained comaunexplained coma Can get IA rtPA up to 24H after Sx onset, Can get IA rtPA up to 24H after Sx onset,
but the earlier the better.but the earlier the better.

PresentationPresentation
Nausea/vomiting Nausea/vomiting Headache, neck painHeadache, neck pain DrowsinessDrowsiness ComaComa Bilateral motor findings/sensory Bilateral motor findings/sensory
findings –can be present but are findings –can be present but are often absentoften absent
-because of multiple emboli-because of multiple emboli

Quiz time - Anterior or posterior Quiz time - Anterior or posterior circulation?circulation?
Vertigo?Vertigo? Diplopia?Diplopia? Apraxia?Apraxia? Deafness?Deafness? Crossed symptoms (right face, left body)?Crossed symptoms (right face, left body)? Homonymous hemianopsia?Homonymous hemianopsia? Aphasia? What are the two MC types?Aphasia? What are the two MC types? Dysarthria?Dysarthria? Hemiplegia (arm and leg)?Hemiplegia (arm and leg)? Hemiplegia (face, arm and leg)?Hemiplegia (face, arm and leg)?

So it’s an ischemic stroke!So it’s an ischemic stroke!
MANAGEMENTMANAGEMENT-GENERAL-GENERAL IV, O2 monitor, sats, O2 (sats >92%), Tx feverIV, O2 monitor, sats, O2 (sats >92%), Tx fever Do not give glucose containing solutions unless Do not give glucose containing solutions unless
hypoglycemichypoglycemic Avoid placing NG/foleys initiallyAvoid placing NG/foleys initially-SPECIFIC-SPECIFIC RecanalizationRecanalization Antiplatelet agents Antiplatelet agents Neuroprotective agents – will not discuss Neuroprotective agents – will not discuss

CaseCase
53y.o. right handed diabetic male presents 53y.o. right handed diabetic male presents to Foothills with 30 minutes of right arm to Foothills with 30 minutes of right arm weakness/numbness, and speech difficultyweakness/numbness, and speech difficulty
c/s - Nc/s - N What key piece of info do you want to What key piece of info do you want to
know? Why?know? Why?– Sx started 35 minutes agoSx started 35 minutes ago
What do you want to do next?What do you want to do next?

Within 50 minutes of Sx onset – CT – no ICH, no ischemic changes.
What do you want to do?

THROMBOLYSIS IN THROMBOLYSIS IN ACUTE STROKEACUTE STROKE

How does tPA work?How does tPA work?
tPA converts tPA converts cleaves cleaves plasminogen to plasminogen to plasminplasmin
Plasmin then Plasmin then cleaves fibrin (clot) cleaves fibrin (clot) resulting in lysis of resulting in lysis of thrombusthrombus
Know of any trials Know of any trials for tPA and stroke?for tPA and stroke?

N=624N=624 Inclusion criteria: Inclusion criteria:
measurable neurological deficit due to ischemic strokemeasurable neurological deficit due to ischemic stroke onset within 3 hoursonset within 3 hours age > 18age > 18
Exclusion criteria numerous: Exclusion criteria numerous: ICH, elevated BP, recent anticoagulationICH, elevated BP, recent anticoagulation
RDBPCT rtPA (alteplase) versus placeboRDBPCT rtPA (alteplase) versus placebo– 2 part study – 1) rtPA and o/c at 24H, 2) rtPA and o/c at 2 part study – 1) rtPA and o/c at 24H, 2) rtPA and o/c at
3/123/12– ½ required to be treated within 90 minutes of Sx onset½ required to be treated within 90 minutes of Sx onset
4 Outcome measures: mRS, GOS, NIHSS, Barthel4 Outcome measures: mRS, GOS, NIHSS, Barthel

Results of part 1 – at 24HResults of part 1 – at 24H

Results at 3/12Results at 3/12

ICH ICH


rtPA and SurvivalrtPA and Survival

NINDS summaryNINDS summary
tPA improved neurological scores by 33-50% tPA improved neurological scores by 33-50% (relative risk reduction)(relative risk reduction)
NNT = 12 (little or no neuro deficits)NNT = 12 (little or no neuro deficits) NNH = 17 - Increased risk of ICH NNH = 17 - Increased risk of ICH
(symptomatic - 6.4% vs 0.6%) but survival (symptomatic - 6.4% vs 0.6%) but survival similarsimilar
Improvement in functional outcome to 1 Improvement in functional outcome to 1 yearyear
Earlier treatment better: Earlier treatment better: Tx 0–90 mins more favourable outcome than 90–Tx 0–90 mins more favourable outcome than 90–
180 mins 180 mins

NINDS RECOMMENDATIONSNINDS RECOMMENDATIONS
Door to physician Door to physician 10 min10 min Door to CT completionDoor to CT completion 25 min25 min Door to CT readingDoor to CT reading 45 min45 min Door to Tx decisionDoor to Tx decision 60 min60 min Access to Neuro expertiseAccess to Neuro expertise 15 min15 min Access to NSx expertiseAccess to NSx expertise 2 hours2 hours

Mandated by Canadian federal Mandated by Canadian federal government as condition for licensure of government as condition for licensure of alteplase for ischemic stroke – Phase IV alteplase for ischemic stroke – Phase IV study - Bill Thollstudy - Bill Tholl
To assess safety and effectiveness of tPATo assess safety and effectiveness of tPA Feb 1999-June 2001Feb 1999-June 2001 Prospective observational cohort study Prospective observational cohort study N=1135N=1135 60 Canadian centres60 Canadian centres

Protocol violations and Protocol violations and symptomatic ICH ratesymptomatic ICH rate
Protocol violations (154): Protocol violations (154): – onset-to-treatment time > 180 – onset-to-treatment time > 180 minutes, platelet count < 100 minutes, platelet count < 100 101099/L, INR > 1.4, tPA dose > 90 mg/L, INR > 1.4, tPA dose > 90 mg
Symptomatic ICH rate:Symptomatic ICH rate:– 7.8% (violation) v. 3.9% (no – 7.8% (violation) v. 3.9% (no violation)violation)--RR 2.0 (RR 2.0 (95% CI 1.1–3.895% CI 1.1–3.8))

10 May 2005
CASES - Original article available at www.cmaj.ca
Frequency
Onset-to-treatment time, min0 60 120 180 240 300 360
0
215
Time to treatment
median 155minmedian 155min

Excellent outcome in 36.8% Excellent outcome in 36.8% – NINDS 39.9% NS differenceNINDS 39.9% NS difference
Overall mortality 22.3% (20-25%)Overall mortality 22.3% (20-25%) Serious adverse events in 6.6% of Serious adverse events in 6.6% of
pts:pts:– Symptomatic ICH 4.6%Symptomatic ICH 4.6%– Angioedema 1.3%Angioedema 1.3%– Acute hypotension 0.4%Acute hypotension 0.4%

rtPA trials synopsis rtPA trials synopsis ECASS ECASS
ECASS IIECASS II
ATLANTISATLANTIS
NINDSNINDS
CASES and SITS-MOSTCASES and SITS-MOST
< 6h: tPA too risky< 6h: tPA too risky
< 6h: No significant < 6h: No significant improvements with tPAimprovements with tPA
3-5h: No benefit and more 3-5h: No benefit and more AEAE
<3h: Benefits outweigh <3h: Benefits outweigh risksrisks
<3h as per strict protocols <3h as per strict protocols effectiveness and safety effectiveness and safety similar to NINDSsimilar to NINDS

Case cont…Case cont…
So patients meet rtPA inclusion So patients meet rtPA inclusion criteriacriteria– Stroke with measurable deficits (not Stroke with measurable deficits (not
minor and not improving)minor and not improving)– Onset w/i 3 hoursOnset w/i 3 hours– CT head – no ICHCT head – no ICH– At a site that meets NINDS protocolsAt a site that meets NINDS protocols
What are contraindications to rtPA in What are contraindications to rtPA in setting of a stroke?setting of a stroke?

Contra-Indications to LyticsContra-Indications to Lytics
Hemorrhagic Stroke (ever)Hemorrhagic Stroke (ever) Minor or rapidly improving Minor or rapidly improving
SxSx High suspicion of SAHHigh suspicion of SAH Active internal bleeding Active internal bleeding
(w/i last 21/7)(w/i last 21/7) Known bleeding diathesis Known bleeding diathesis
(plts<100,000, recent (plts<100,000, recent heparin or a/c use)heparin or a/c use)
Recent intracranial Recent intracranial surgery, serious head surgery, serious head trauma or previous stroke trauma or previous stroke (3/12)(3/12)
Witnessed seizure at Witnessed seizure at onsetonset
Major surgery or Major surgery or trauma w/I 14/7trauma w/I 14/7
LP w/i 7/7LP w/i 7/7 Hx of ICH, AVM or Hx of ICH, AVM or
aneurysmaneurysm Recent MI (w/i 3/12)Recent MI (w/i 3/12) SBP >185, DBP >110 SBP >185, DBP >110
despite Txdespite Tx

What fraction of stroke patients are What fraction of stroke patients are eligible for thrombolysis?eligible for thrombolysis?
Less than Less than
5 %5 %

TimelinesTimelines
IV rtPA: IV rtPA: ≤≤3 hours3 hours – NINDS study (Class I) – NINDS study (Class I)
IA pro-UK to MCA and not a candidate for IA pro-UK to MCA and not a candidate for rtPA: rtPA: ≤≤ 6 hours – PROACT II (Class I) 6 hours – PROACT II (Class I)– IA pro-UK for individuals with CI to rtPA (i.e. IA pro-UK for individuals with CI to rtPA (i.e.
recent surgery) Class II recent surgery) Class II
IA pro-UK to vertebro-basilar system: IA pro-UK to vertebro-basilar system: ≤≤ 24 24 hours (prognosis is so poor otherwise)hours (prognosis is so poor otherwise)

The controversy The controversy – Dr. J Hoffman– Dr. J Hoffman
Efficacy vs effectiveness – i.e. would real Efficacy vs effectiveness – i.e. would real world application give as robust results world application give as robust results
Only 1 +ve trial – many –ve. Many Only 1 +ve trial – many –ve. Many examples from other interventions that examples from other interventions that impressive single study results were impressive single study results were eventually disproveneventually disproven
If only 5% are eligible and only 1 in 10 If only 5% are eligible and only 1 in 10 benefit – then the impact of rtPA is smallbenefit – then the impact of rtPA is small

CAEP position on thrombolytics for CAEP position on thrombolytics for acute ischemic strokeacute ischemic stroke
““Stroke thrombolysis should be limitedStroke thrombolysis should be limited to centers to centers with appropriate neurological and neuro-imaging with appropriate neurological and neuro-imaging resources that are resources that are capable of administering capable of administering treatment within three hourstreatment within three hours. In such centres, . In such centres, emergency physicians should identify eligible emergency physicians should identify eligible patients, inItiate low-risk interventions and facilitate patients, inItiate low-risk interventions and facilitate prompt CT scanningprompt CT scanning… … Neurologists should be directly Neurologists should be directly involved prior to the thrombolytic administration.”involved prior to the thrombolytic administration.”
““Until it is clear that the benefits of this therapy Until it is clear that the benefits of this therapy outweigh the risks, thrombolytic therapy for acute outweigh the risks, thrombolytic therapy for acute stroke should be restricted to use within formal stroke should be restricted to use within formal research protocols or in a monitored practice research protocols or in a monitored practice protocols that adhere to the NINDS eligibility protocols that adhere to the NINDS eligibility criteria.”criteria.”

CaseCase
After the bloodwork is drawn on your After the bloodwork is drawn on your patient, waiting for CT head, the RN patient, waiting for CT head, the RN informs you his BP is 210/110.informs you his BP is 210/110.
Should you lower it?Should you lower it? Does it matter if they are a rtPA candidate?Does it matter if they are a rtPA candidate? What if they are not?What if they are not? If yes, how?If yes, how?

Theoretical Reasons for Theoretical Reasons for lowering BPlowering BP
Reducing formation of cerebral Reducing formation of cerebral edemaedema
↓ ↓ risk of hemorrhagic transformationrisk of hemorrhagic transformation Preventing further vascular damagePreventing further vascular damage Minimizing risk of early recurrent Minimizing risk of early recurrent
strokestroke

Eligibile for rtPAEligibile for rtPA
Dr. Coutts - What BP do you target with you treatment?

Not eligible for rtPANot eligible for rtPA
Treat other potential causes of HTNTreat other potential causes of HTN– Pain, anxiety, fever, drain bladder, Pain, anxiety, fever, drain bladder,
Do not treat Do not treat – unless SBP >220 mmHg or unless SBP >220 mmHg or – DBP >120 mmHgDBP >120 mmHg– And goal is to lower 15% w/i 24HAnd goal is to lower 15% w/i 24H

Hypotension and ischemic Hypotension and ischemic strokesstrokes
Less common than HTNLess common than HTN SBP <100 or DBP < 70 are associated with SBP <100 or DBP < 70 are associated with
worsening neuro status, poor neuro worsening neuro status, poor neuro outcomes and increased risk of deathoutcomes and increased risk of death
Seek and Tx causes; AoD, volume deplete, Seek and Tx causes; AoD, volume deplete, blood loss, blood loss, ↓ cardiac output (2º to MI or ↓ cardiac output (2º to MI or dysrhythmias)dysrhythmias)
May need vasopressors if BP does not May need vasopressors if BP does not improve with management of primary improve with management of primary issueissue

CaseCase
You are at the bedside explaining the You are at the bedside explaining the evidence regarding BP management in evidence regarding BP management in acute stroke to the nurse when your acute stroke to the nurse when your patient begins to use his right arm. Then patient begins to use his right arm. Then he says “Hey doc, I can speak!”he says “Hey doc, I can speak!”
It is 45 minutes since his symptoms began It is 45 minutes since his symptoms began
What now?What now?

Transient Ischemic AttackTransient Ischemic Attack
Rapidly developing clinical signs of Rapidly developing clinical signs of focal (or global) disturbance of focal (or global) disturbance of cerebral function, with symptoms cerebral function, with symptoms lasting less than 24 hours, with no lasting less than 24 hours, with no apparent cause other than that of apparent cause other than that of vascular origin.vascular origin.
World Health Organization definitionWorld Health Organization definition

TIAsTIAs
24 hours was arbitrarily chosen24 hours was arbitrarily chosen
Majority resolve in less than 60 Majority resolve in less than 60 minutesminutes
In the placebo arm of NINDSIn the placebo arm of NINDS– Only 2% of those who had not improved Only 2% of those who had not improved
by 3 hours improved by 24 hoursby 3 hours improved by 24 hours

Proposed new definitionProposed new definition
A brief episode of neurologic A brief episode of neurologic dysfunction caused by focal brain or dysfunction caused by focal brain or retinal ischemia, with clinical symptoms retinal ischemia, with clinical symptoms typically lasting less than one hour, and typically lasting less than one hour, and without evidence of acute infarction.without evidence of acute infarction.
Persistent clinical signs or characteristic Persistent clinical signs or characteristic imaging abnormalities define infarction.imaging abnormalities define infarction.
Albers et al. Albers et al. NEJM 2002NEJM 2002

Approach to TIAApproach to TIA Consider DDxConsider DDx Arrange work-upArrange work-up
– CT head – helps r/o other causes, old infarctsCT head – helps r/o other causes, old infarcts– CTA or Carotid dopplerCTA or Carotid doppler– ECGECG– ? Echo? Echo
ASA +/- Plavix – Dr Coutts; when do you add/substitute ASA +/- Plavix – Dr Coutts; when do you add/substitute plavix?plavix?– Rough rule of thumb – cardioembolic (AF, valvular dz, post-MI) Rough rule of thumb – cardioembolic (AF, valvular dz, post-MI)
cause for stroke – anticoagulatecause for stroke – anticoagulate– Non-cardioembolic – antiplatelet agents (ASA, aggrenox)Non-cardioembolic – antiplatelet agents (ASA, aggrenox)
Follow up for definitive treatment Follow up for definitive treatment – Carotid endarterectomy (NASCET and ECST trials) for Carotid endarterectomy (NASCET and ECST trials) for
symptomatic patients w/70-99% stenosissymptomatic patients w/70-99% stenosis Risk reduction: HTN control, statin, DM control, stop Risk reduction: HTN control, statin, DM control, stop
smokingsmoking

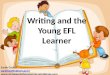
California scoreCalifornia score
Cohort study Cohort study March 1997-Feb 1998March 1997-Feb 1998 16 hospitals in California16 hospitals in California N=1707N=1707 Main outcomes: risk of stroke within 90 Main outcomes: risk of stroke within 90
days after index TIA, death, recurrent days after index TIA, death, recurrent TIA, hospitalization for CV eventsTIA, hospitalization for CV events

California scoreCalifornia score
180 patients (10.5%) had stroke 180 patients (10.5%) had stroke within 90 dayswithin 90 days
91 strokes (half) in first 2 days91 strokes (half) in first 2 days
Derived 5 risk factors for stroke Derived 5 risk factors for stroke within 90 dayswithin 90 days



A simple ABCD ScoreA simple ABCD Score A: age A: age >> 60 years – 1 point 60 years – 1 point B: BP (systolic>140mmHg, diastolic>90 B: BP (systolic>140mmHg, diastolic>90
mmHg). Either 1 point. (max 1 point)mmHg). Either 1 point. (max 1 point) C: clinical – unilateral weakness =2, speech C: clinical – unilateral weakness =2, speech
only = 1, only = 1, D: Duration, D: Duration, >>60 minutes =2, 10-59 =1, <10 60 minutes =2, 10-59 =1, <10
=0.=0. Recently added diabetes=1 (ABCDRecently added diabetes=1 (ABCD2 2 Score)Score)
Rothwell PM, Lancet 2005; 366:29-36, Johnston, SC, Lancet 2007;369:283-292.
Thanks Dr. Coutts

What is done in Calgary?What is done in Calgary? Review high risk patients – motor or Review high risk patients – motor or
speech longer than 5 minutes.speech longer than 5 minutes. Sensory events or isolated vertigo Sensory events or isolated vertigo
seen in clinic.seen in clinic. Delayed presentation gets seen in Delayed presentation gets seen in
clinic urgently.clinic urgently. AllAll get CT imaging and carotid get CT imaging and carotid
imaging emergently - usually CTA.imaging emergently - usually CTA. ECG – looking for atrial fibrillation.ECG – looking for atrial fibrillation. All get loaded with aspirin.All get loaded with aspirin.
Thanks Dr. Coutts

CHR-FMC stroke prevention CHR-FMC stroke prevention clinicclinic

SummarySummary
TIA is a historical diagnosis so you TIA is a historical diagnosis so you need to take a good history!need to take a good history!
The risk of a recurrent stroke is high 5-The risk of a recurrent stroke is high 5-20%.20%.
Time window for prevention is short.Time window for prevention is short. We want to see high risk patients We want to see high risk patients
urgently.urgently. Page Stroke Team if concerned or have Page Stroke Team if concerned or have
questions about how urgently we would questions about how urgently we would like to see an individual patient.like to see an individual patient.

CaseCase
57M. Longstanding HTN, EtOH 57M. Longstanding HTN, EtOH abuse. Presents with 8 hours Hx of abuse. Presents with 8 hours Hx of progressive HA, N/V, garbled speechprogressive HA, N/V, garbled speech
BP – 250/140, HR – 80, c/s – 9, 99%, BP – 250/140, HR – 80, c/s – 9, 99%, 37.0, now GCS -337.0, now GCS -3
What are you concerned aboutWhat are you concerned about Are there clues on physical exam?Are there clues on physical exam?


Management?Management?
ABC’s – capture airway if neededABC’s – capture airway if needed Elevate HOBElevate HOB BP Management? When? How?BP Management? When? How?
– Labetalol drug we are most comfortable withLabetalol drug we are most comfortable with Reverse any coagulopathyReverse any coagulopathy Treat hyperglycemia/hyperthermiaTreat hyperglycemia/hyperthermia Manage Manage ↑ ICP as needed↑ ICP as needed rVIIa? – Come to j.c. June 12rVIIa? – Come to j.c. June 12thth to find out to find out

BP Management from AHA BP Management from AHA 20072007

CaseCase 29F. 5 days post-partum. 2 day history of 29F. 5 days post-partum. 2 day history of
progressive HA – severe, a few episodes of progressive HA – severe, a few episodes of vomiting, vision “off”. Becoming vomiting, vision “off”. Becoming increasingly altered. Has a seizure on increasingly altered. Has a seizure on route - resolved.route - resolved.
VS – N. c/s – N, no bleeding RF. VS – N. c/s – N, no bleeding RF. Planned c/s (too proud to push)Planned c/s (too proud to push) Prev well – other than prtn c deficiencyPrev well – other than prtn c deficiency B.w. all normal.B.w. all normal. What are you concerned about?What are you concerned about? What tests do want to arrange?What tests do want to arrange?

Cerebral venous sinus Cerebral venous sinus thrombosisthrombosis
May get thrombosis May get thrombosis of cerebral veins of cerebral veins with local effects with local effects from obstructionfrom obstruction
May get thrombosis May get thrombosis of major sinuses of major sinuses causing intracranial causing intracranial HTNHTN
Or both may occur Or both may occur together (most together (most common)common)
JAMA 2000;284:2901-2906
Kaplan-Meier Survival-Free from StrokePatients Presenting with TIA in Emergency Room (N=1707)
10.5%
High risk of stroke during 1st few days after TIA
JAMA 2000;284:2901-2906
Kaplan-Meier Survival-Free from StrokePatients Presenting with TIA in Emergency Room (N=1707)
10.5%
High risk of stroke during 1st few days after TIA
J A M A 2 0 0 0 ;2 8 4 :2 9 0 1 -2 9 0 6K a p la n -M e ie r S u rv iv a l-F re e fro m S tro k eP a tie n ts P re s e n tin g w ith T IA in E m e rg e n c y R o o m (N = 1 7 0 7 )1 0 .5 %H ig h ris k o f s tro k e d u rin g 1 s t fe w d a y s a fte r T IA
JAMA 2000;284:2901-2906
Kaplan-Meier Survival-Free from StrokePatients Presenting with TIA in Emergency Room (N=1707)
10.5%
High risk of stroke during 1st few days after TIA

Predisposing factors Predisposing factors
Prothrombotic Prothrombotic conditionsconditions
Pregnancy, Pregnancy, puerperiumpuerperium
Inflammatory Inflammatory disease (SLE, disease (SLE, Wegners, sarcoid, Wegners, sarcoid, IBD)IBD)
Cancer Cancer
Infections (staph Infections (staph infections of face, infections of face, meningitis, sepsis)meningitis, sepsis)
Drugs (OCP)Drugs (OCP) Trauma (head Trauma (head
injury)injury) Iatrogenic (LP, Iatrogenic (LP,
neurosurg neurosurg procedures)procedures)

Clinical presentation Clinical presentation Severe HA (70-90%) – usu gradual but can be Severe HA (70-90%) – usu gradual but can be
suddensudden Because process is non-focal, findings may be as Because process is non-focal, findings may be as
wellwell Focal deficits (hemiparesis, seizures, ALOC, Focal deficits (hemiparesis, seizures, ALOC,
papilledema) in 33-75% of casespapilledema) in 33-75% of cases Characteristic is hemispheric Sx than progress to Characteristic is hemispheric Sx than progress to
other hemisphere within a few daysother hemisphere within a few days Benign intracranial HTN features (HA, Benign intracranial HTN features (HA,
papilledema, vision disturbances) 18-38%papilledema, vision disturbances) 18-38% Seizures and Todd’s paresis in 30-50%Seizures and Todd’s paresis in 30-50%

PresentationsPresentations Cavernous sinus thrombosis: ocular signs Cavernous sinus thrombosis: ocular signs
dominate the clinical picture with orbital pain, dominate the clinical picture with orbital pain, chemosis, proptosis, and oculomotor palsies. chemosis, proptosis, and oculomotor palsies.
With sagittal sinus occlusion, motor deficits, With sagittal sinus occlusion, motor deficits, bilateral deficits, and seizures are frequentbilateral deficits, and seizures are frequent
Patients with isolated lateral sinus thrombosis Patients with isolated lateral sinus thrombosis present mostly with isolated intracranial present mostly with isolated intracranial hypertension. hypertension.
Jugular vein or lateral sinus thrombosis may Jugular vein or lateral sinus thrombosis may present as isolated pulsating tinnitus present as isolated pulsating tinnitus
Multiple cranial nerve palsies may occur in Multiple cranial nerve palsies may occur in thrombosis of the lateral sinus, jugular, or thrombosis of the lateral sinus, jugular, or posterior fossa veins thrombosis. posterior fossa veins thrombosis.

ImagingImaging
Generally start with NCCTGenerally start with NCCT– Normally in up to 30%Normally in up to 30%– Can see venous infarcts or hemorrhagesCan see venous infarcts or hemorrhages
But, this is not enough to rule-out the But, this is not enough to rule-out the diagnosisdiagnosis
CT venogram if NCCT is normalCT venogram if NCCT is normal MR +/- MRV – the gold standardMR +/- MRV – the gold standard
– Difficult to read/access, artifact, false Difficult to read/access, artifact, false positivespositives

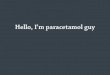
Cord Sign Delta sign


CT findingsCT findings
DIRECT SIGNSDIRECT SIGNS Empty delta sign—opacification of collateral veins Empty delta sign—opacification of collateral veins
in wall of superior sagittal sinus (10-20%) after in wall of superior sagittal sinus (10-20%) after enhanceenhancenn
Cord sign—hyperdense thrombosed cortical veinCord sign—hyperdense thrombosed cortical veinINDIRECT SIGNSINDIRECT SIGNS Local or generalized swelling (40-70%)Local or generalized swelling (40-70%) Intense enhancement of falx and tentorium (20%)Intense enhancement of falx and tentorium (20%) Gyral enhancement (10-20%)Gyral enhancement (10-20%) Localized hypo/hyperdense areas showing Localized hypo/hyperdense areas showing
hemorrhage (10-40%)hemorrhage (10-40%)

CT findingsCT findings
A) Hemorrhagic infarct with sinus thrombosis
B) thalamic edema caused by thrombosis of straight sinus

CVST treatment?CVST treatment?
Despite the fact that 40% of patients w/CVST Despite the fact that 40% of patients w/CVST have hemorrhages (before a/c)have hemorrhages (before a/c)
Heparin is the Tx of choice based:Heparin is the Tx of choice based:– Three small nonrandomized trials-Three small nonrandomized trials-
May reduce risk of fatal outcome / severe May reduce risk of fatal outcome / severe disability disability
No increase in ICHNo increase in ICHUnfortunately all are underpowered – but all Unfortunately all are underpowered – but all
showed trend towards benefitshowed trend towards benefit M.A. – OR of 0.46 (95%CI 0.16-1.31)for M.A. – OR of 0.46 (95%CI 0.16-1.31)for
reduction in death /dependency reduction in death /dependency

CVST treatment CVST treatment
Thrombolysis:Thrombolysis:– Case reports and uncontrolled studiesCase reports and uncontrolled studies– Usually restricted to pts with poor Usually restricted to pts with poor
prognosis due to risk of bleeding prognosis due to risk of bleeding complicationscomplications
Stam, J. Thrombosis of the cerebral veins and sinuses. NEJM Stam, J. Thrombosis of the cerebral veins and sinuses. NEJM 2005.2005.
Great CVST reference:Great CVST reference:– Stam J. Thrombosis of the Cerebral Stam J. Thrombosis of the Cerebral
Veins and Sinuses. NEJM 2005: 352;17.Veins and Sinuses. NEJM 2005: 352;17.

ReferencesReferences Adams HP Adams HP et al. et al. Guidelines for the early management of patients with Guidelines for the early management of patients with
ischemic strokeischemic stroke: a scientific statement from the Stroke Council of the : a scientific statement from the Stroke Council of the American Stroke Association. American Stroke Association. StrokeStroke 2003;34:1056 2003;34:1056
Adams HP Adams HP et al. et al. Guidelines for the Early Management of Patients With Guidelines for the Early Management of Patients With Ischemic Stroke. A Scientific Statement From the Stroke Council of the Ischemic Stroke. A Scientific Statement From the Stroke Council of the American Stroke Association. American Stroke Association. StrokeStroke 2003;34: 1056-1083. 2003;34: 1056-1083.
Albers Albers et al. et al. Transient ischemic attack- proposal for a new definition Transient ischemic attack- proposal for a new definition NEJM NEJM 2002;347:1713-17162002;347:1713-1716
Anticoagulants and Antiplatelet Agents in Acute Ischemic Stroke. Report Anticoagulants and Antiplatelet Agents in Acute Ischemic Stroke. Report of the joint stroke guideline development committee of the American of the joint stroke guideline development committee of the American academy of neurology and American stroke association. academy of neurology and American stroke association. StrokeStroke 2002;33:1934-1942.2002;33:1934-1942.
Barber Barber et al. et al. Imaging of the brain in acute ischemic stroke: comparison Imaging of the brain in acute ischemic stroke: comparison of computed tomography and magnetic resonance diffusion-weighted of computed tomography and magnetic resonance diffusion-weighted imaging, imaging, Journal of Neurology, Neurosurgery and PsychiatryJournal of Neurology, Neurosurgery and Psychiatry 2005;76:1528-15332005;76:1528-1533
Borg KT Borg KT et alet al TIA: an emergency medicine approach. TIA: an emergency medicine approach. Emergency Emergency Medicine Clinics of North America;Medicine Clinics of North America; 2002:20( 3) 2002:20( 3)
Broderick Broderick et al. et al. Guidelines for the management of spontaneous Guidelines for the management of spontaneous intracerebral hemorrhageintracerebral hemorrhage. . StrokeStroke 1999;30:905-915. 1999;30:905-915.

Buring Buring et alet al. Established treatments for acute ischemic stroke Khaja . Established treatments for acute ischemic stroke Khaja et al Lancetet al Lancet 2007;369:319-330 2007;369:319-330
CAST: randomized placebo-controlled trial of early aspirin use in CAST: randomized placebo-controlled trial of early aspirin use in 20000 patients with acute ischemic stroke20000 patients with acute ischemic stroke. Lancet. Lancet 1997; 349: 1641- 1997; 349: 1641-16491649
Claiborne Johnston. Transient ischemic attack Claiborne Johnston. Transient ischemic attack NEJM NEJM 2002;347:1687-2002;347:1687-16921692
Claiborne Johnston Claiborne Johnston et al. et al. Validation and refinement of scores to Validation and refinement of scores to predict very early stroke risk after transient ischemic attack predict very early stroke risk after transient ischemic attack LancetLancet 2007;369:283-2922007;369:283-292
Clark Clark et alet al. Recombinant tissue-type plasminogen activator . Recombinant tissue-type plasminogen activator (alteplase) for ischemic stroke 3 to 5 hours after symptom onset. (alteplase) for ischemic stroke 3 to 5 hours after symptom onset. The ATLANTIS Study: a randomized controlled trial. Alteplase The ATLANTIS Study: a randomized controlled trial. Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic Thrombolysis for Acute Noninterventional Therapy in Ischemic Stroke. Stroke. JAMA JAMA 1999;282:2019-26.1999;282:2019-26.
Clark WM Clark WM et al.et al. Recombinant tissue-type plasminogen activator Recombinant tissue-type plasminogen activator (Alteplase) for ischemic stroke 3 to 5 hours after symptom onset. (Alteplase) for ischemic stroke 3 to 5 hours after symptom onset. (The alteplase thrombolysis for acute noninterventional therapy for (The alteplase thrombolysis for acute noninterventional therapy for ischemic stroke [ATLANTIS] study). ischemic stroke [ATLANTIS] study). JAMA JAMA 1999;282:2019-261999;282:2019-26
Del Zoppo Del Zoppo et al.et al. PROACT: a phase II randomized trial of recombinant PROACT: a phase II randomized trial of recombinant pro-urokinase by dircet arterial devlivery in acute middle cerebral pro-urokinase by dircet arterial devlivery in acute middle cerebral artery stroke: PROACT investigators: Prolyse in Acute Cerebral artery stroke: PROACT investigators: Prolyse in Acute Cerebral Thrombolembolism. Thrombolembolism. Stroke Stroke 1998; 29:4-111998; 29:4-11

Brott T Brott T et al.et al. Hypertension and its treatment in the NINDS rtPA Hypertension and its treatment in the NINDS rtPA stroke trial. stroke trial. StrokeStroke 1998;29:1504-1509 1998;29:1504-1509
Buring Buring et al.et al. Migraine and subsequent risk of stroke in the Migraine and subsequent risk of stroke in the physician’s health study physician’s health study Archives of NeurologyArchives of Neurology 1995;52:129-134 1995;52:129-134
Furlan A Furlan A et alet al. Intra-arterial prourokinase for acute ischemic stroke. . Intra-arterial prourokinase for acute ischemic stroke. The PROACT II study: a randomized controlled trial. The PROACT II study: a randomized controlled trial. JAMAJAMA 1999;282:2003-111999;282:2003-11
Hacke Hacke et al.et al. Randomized double-blind placebo-controlled trial of Randomized double-blind placebo-controlled trial of thrombolytic therapythrombolytic therapywith intravenous alteplase in acute ischemic stroke (ECASS II). with intravenous alteplase in acute ischemic stroke (ECASS II). Second European-Second European-Australasian Acute Stroke Study Investigators. Australasian Acute Stroke Study Investigators. Lancet Lancet 1998;352:1245-51.1998;352:1245-51.
Hacke W Hacke W et alet al. Intravenous thrombolysis with recombinant tissue . Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. European plasminogen activator for acute hemispheric stroke. European Cooperative Acute Stroke StudyCooperative Acute Stroke Study(ECASS). (ECASS). JAMA JAMA 1995;274:1017-25.1995;274:1017-25.
Hill MD, Hill MD, et al. et al. Thrombolysis for acute ischemic stroke: results of the Thrombolysis for acute ischemic stroke: results of the Canadian Alteplase for Stroke Effectiveness Study Canadian Alteplase for Stroke Effectiveness Study CMAJCMAJ. May 10, . May 10, 2005. 172(10):1307-12.2005. 172(10):1307-12.
Johnston SC. American Heart Association Guidelines TIA. Johnston SC. American Heart Association Guidelines TIA. NEJMNEJM 2002. 2002. Johnston SCJohnston SC, et al, et al. Short-term prognosis after ED diagnosis of TIA. Short-term prognosis after ED diagnosis of TIA. .
JAMAJAMA 2000. 2000.

Mayer, SA, Mayer, SA, et al. et al. Recombinant Activated Factor VII for Acute Recombinant Activated Factor VII for Acute Intracerebral HemorrhageIntracerebral HemorrhageNEJMNEJM. Feb 2005.. Feb 2005.
National Institute of Neurological Disorders and Stroke rt-PA Stroke National Institute of Neurological Disorders and Stroke rt-PA Stroke StudyStudyGroup. Tissue plasminogen activator for acute ischemic stroke. Group. Tissue plasminogen activator for acute ischemic stroke. NEJMNEJM1995;333:1581-7.1995;333:1581-7.
Oliveira-Filho J Oliveira-Filho J et al. et al. Detrimental effect of blood pressure reduction in Detrimental effect of blood pressure reduction in the first 24 hours of acute stroke onset. the first 24 hours of acute stroke onset. NeurologyNeurology 2003;61:1047-1051. 2003;61:1047-1051.
Position Statement on Thrombolytic Therapy for Acute Ischemic Stroke, Position Statement on Thrombolytic Therapy for Acute Ischemic Stroke, The CAEP Committee on Thrombolytic Therapy for Acute Ischemic The CAEP Committee on Thrombolytic Therapy for Acute Ischemic Stroke Stroke http://www.caep.ca/002.policies/002-01.guidelines/thrombolytic.htmhttp://www.caep.ca/002.policies/002-01.guidelines/thrombolytic.htm
Powers WJ Powers WJ et al.et al. Acute hypertension after stroke: the scientific basis for Acute hypertension after stroke: the scientific basis for treatment decisions. treatment decisions. Neurology Neurology 1993;43:461-4671993;43:461-467
Powers WJ Powers WJ et al. et al. Autoregulation of cerebral blood flow surrounding acute Autoregulation of cerebral blood flow surrounding acute (6 to 22 hours) intracerebral hemorrhage. (6 to 22 hours) intracerebral hemorrhage. NeurologyNeurology 2001;57:18-24. 2001;57:18-24.
Rothwell Rothwell et al. et al. A simple score (ABCD) to identify individuals at high A simple score (ABCD) to identify individuals at high early risk of stroke after transient ischemic attack early risk of stroke after transient ischemic attack LancetLancet 2005;366:29- 2005;366:29-3636
Sacco Sacco et al. et al. Experimental treatments for acute ischemic stroke Experimental treatments for acute ischemic stroke LancetLancet 2007;369:331-3412007;369:331-341

Stam, J. Thrombosis of the cerebral veins and sinusesStam, J. Thrombosis of the cerebral veins and sinuses NEJM NEJM 2005. 2005. Semplicini A Semplicini A et al. et al. Hypertension in acute ischemic stroke: a Hypertension in acute ischemic stroke: a
compensatory mechanism or an additional damaging factor? compensatory mechanism or an additional damaging factor? Arch Int Arch Int MedMed 2003;163:211-216 2003;163:211-216
Streifler JY, Streifler JY, et alet al. The risk of stroke in patients with first-ever retinal vs. . The risk of stroke in patients with first-ever retinal vs. hemispheric TIA and high-grade carotid stenosis. hemispheric TIA and high-grade carotid stenosis. Arch NeurolArch Neurol 1995. 1995.
Wahlgren Wahlgren et al. et al. Thrombolysis with alteplase for acute ischemic stroke in Thrombolysis with alteplase for acute ischemic stroke in the Safe Impletmentation of Thrombolysis in Stroke Monitoring Study the Safe Impletmentation of Thrombolysis in Stroke Monitoring Study (SITS-MOS): an observational study (SITS-MOS): an observational study LancetLancet 2007;369:275-282 2007;369:275-282
Clinical Neuroanatomy Made Ridiculously SimpleClinical Neuroanatomy Made Ridiculously Simple, 2nd ed. Goldberg S. , 2nd ed. Goldberg S. MedMaster Inc 2000MedMaster Inc 2000
Atlas of Human AnatomyAtlas of Human Anatomy, 2nd ed. Netter FH, Novartis 1997, 2nd ed. Netter FH, Novartis 1997 Initial assessment and management of acute strokeInitial assessment and management of acute stroke Oliveira-Filho J, Oliveira-Filho J,
Koroshetz WJ, UpToDate 2007Koroshetz WJ, UpToDate 2007 Clinical diagnosis of stroke subtypesClinical diagnosis of stroke subtypes Caplan LR UpToDate 2007 Caplan LR UpToDate 2007 Overview of the evaluation of stroke Overview of the evaluation of stroke Caplan LR UpToDate 2007Caplan LR UpToDate 2007 Locked-in syndromeLocked-in syndrome Savitz SI, Caplan LR UpToDate 2007 Savitz SI, Caplan LR UpToDate 2007 Salter Di, Curtin S Salter Di, Curtin S Middle cerebral artery strokeMiddle cerebral artery stroke, , www.emedicine.comwww.emedicine.com Baird A Baird A Anterior circulation stroke,Anterior circulation stroke, www.emedcine.comwww.emedcine.com Hill MD, Buchan AM Hill MD, Buchan AM Posterior cerebral artery strokePosterior cerebral artery stroke, , www.emedicine.comwww.emedicine.com Agranoff AB, Wong EH Agranoff AB, Wong EH Lacunar Stroke,Lacunar Stroke, www.emedicine.comwww.emedicine.com www.strokecentre.orgwww.strokecentre.org