Embed Size (px)
Citation preview
Strengths and Weaknesses of Strengths and Weaknesses of
Falls Prevention Strategies Falls Prevention Strategies
Dr Dawn Skelton,
Reader in Ageing & Health, Glasgow Caledonian University

My presentation will….My presentation will….
�� Very briefly explore the prevalence and Very briefly explore the prevalence and consequences of fallsconsequences of falls
�� Discuss the evidence base in relation to Discuss the evidence base in relation to single interventions and populationsingle interventions and population--based based interventionsinterventions–– Strengths and WeaknessesStrengths and Weaknesses
�� Very briefly explore the gaps in the evidence Very briefly explore the gaps in the evidence base base
�� Be available to downloadBe available to download

Prevention of Falls Network Prevention of Falls Network
Europe (ProFaNE)Europe (ProFaNE)
www.profane.eu.orgwww.profane.eu.org
Discussion BoardDiscussion Board
ResourcesResources
InformationInformation
22--Monthly eMonthly e--newsletternewsletter

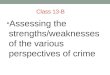
Figure 9. Mortality rate (age standardised - per 100,000) due to
falls in the elderly (65+) in the EU25 and EEA, in countries having
less than 10% "Other and unspecified" (Table 1)
164.5
112.2
94.9
89.1
73
66.4
65.3
61.7
57.8
50.3
38.9
35.1
33.1
24.8
14.4
0 20 40 60 80 100 120 140 160 180
Hungary
Czech Republic
Finland
Slovenia
Italy
Poland
Latvia
Ireland
Belgium
Austria
Iceland
Li thuania
Slovakia
Estonia
Greece
European Network on Safety among Elderly (EUNESE)
Priorities for Elderly Safety in Europe 2006
10 fold difference in mortality from falls in different EU countries

Falls in the UKFalls in the UK
�� 11 million people aged > 65 yrs11 million people aged > 65 yrs
�� 28,000 women aged > 90 yrs28,000 women aged > 90 yrs
�� Fractures costs Fractures costs ££1.81.8 billion pabillion pa
�� 1 Hip Fracture every 10 1 Hip Fracture every 10 minsmins
�� 1 Wrist Fracture every 9 1 Wrist Fracture every 9 minsmins
�� 1 Spine Fracture every 3 1 Spine Fracture every 3 minsmins
�� 500 admitted to Hospital every day500 admitted to Hospital every day
�� 3333 never go homenever go homeAnnual European Home and Leisure Accident Surveillance Survey (EHLASS) Report UK 2000
DoH Prevention Package 2009

How common are falls?How common are falls?
�� In In > 75s> 75s, falls are the leading cause , falls are the leading cause of of deathdeath resulting from injuryresulting from injury
�� 7575--80%80% of falls are not reportedof falls are not reported
�� 1 in 3 >65’s1 in 3 >65’s and 1 in 2 >80’s fall p.a.and 1 in 2 >80’s fall p.a.
�� 10%10% of all callof all call--outs for outs for UK UK Ambulance ServiceAmbulance Service are for people are for people aged 65+ who have ‘fallen’ but aged 65+ who have ‘fallen’ but nearly nearly half half are not taken to Hospital.are not taken to Hospital.
Skelton & Todd, WHO 2004, Gillespie 2005, Close 2008

EPIDEMIOLOGY OF FALLING EPIDEMIOLOGY OF FALLING
cont.cont.
�� Falls more common in people with Falls more common in people with multiple medical multiple medical conditionsconditions and with and with poor function and mobilitypoor function and mobility
�� There are There are global variationsglobal variations in fall rates (in fall rates (egeg China 6China 6--20%, 20%, Japan 20%), and few figures are available for developing Japan 20%), and few figures are available for developing worldworld
�� Appear to be Appear to be racial differencesracial differences in likelihood of a fall (white in likelihood of a fall (white Caucasians particularly at risk)Caucasians particularly at risk)
�� WomenWomen are more likely to fall than men, and to suffer are more likely to fall than men, and to suffer nonnon--fatal injuries (higher risk of osteoporosis)fatal injuries (higher risk of osteoporosis)
�� Social deprivationSocial deprivation linked to linked to nocturia nocturia and falls at nightand falls at night(WHO 2007, Booth 2009)(WHO 2007, Booth 2009)
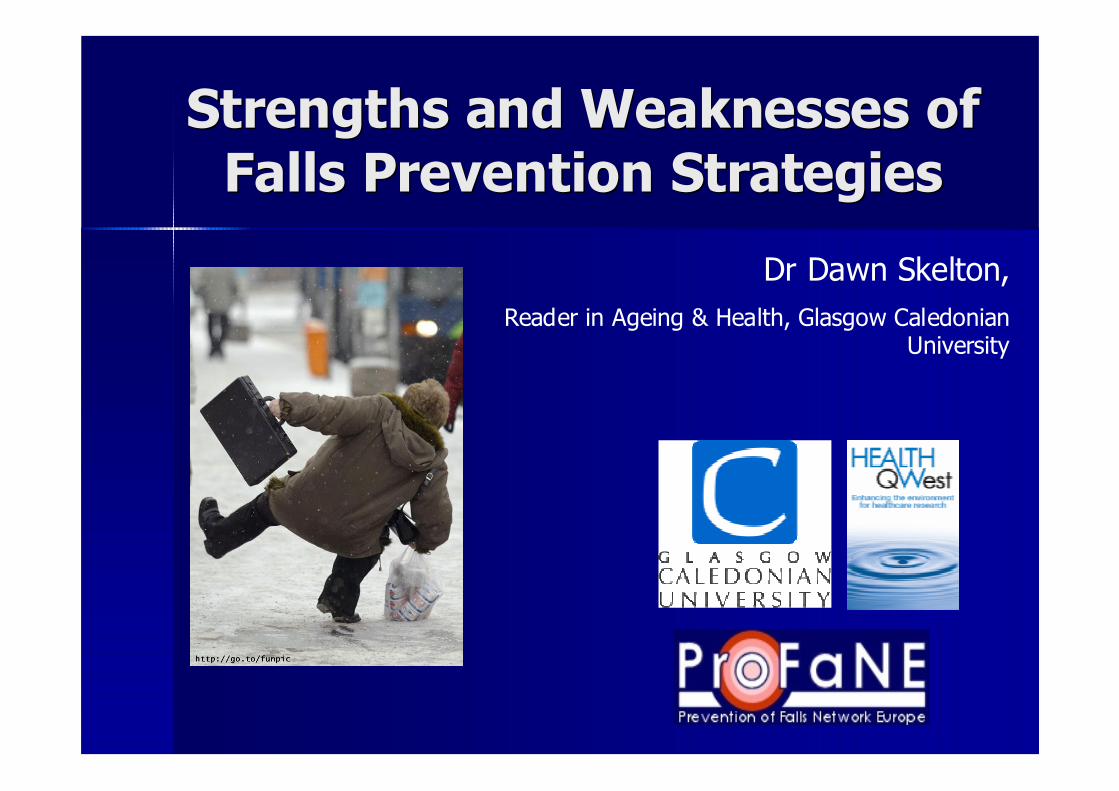
With thanks to Dr David Reid, University of Aberdeen & NOS

Consequences of Hip FractureConsequences of Hip Fracture
�� By Year 2030 expected 100,000 By Year 2030 expected 100,000
hip fractures a year.hip fractures a year.
�� RiskRisk of a hip # of a hip # 10x10x
higher for those in higher for those in residential residential
settingssettings than in than in own homeown home
�� 50%50% of individuals will die, of individuals will die,
move into a nursing home or move into a nursing home or
be in hospital within be in hospital within sixsix months of Hip #months of Hip #
�� 80%80% do not regain predo not regain pre-- fracture mobilityfracture mobilityDoH Prevention
Package 2009

Cost to the IndividualCost to the Individual
�� InjuriesInjuries include: include:
–– Cuts and lacerations, Cuts and lacerations,
–– Deep bruises, Soft Tissue Injuries,Deep bruises, Soft Tissue Injuries,
–– Dislocations, SprainsDislocations, Sprains
–– Increase in joint painIncrease in joint pain
�� Less than Less than 5%5% of all falls result in a of all falls result in a
fracturefracture
�� Long lie’s (floor) & complications Long lie’s (floor) & complications
�� Depression, fear of fallingDepression, fear of falling
�� Avoidance of activitiesAvoidance of activities and social and social
isolationisolation
Skelton & Todd, WHO, 2004
When do we become “fallers” When do we become “fallers”
instead of “trippers”?instead of “trippers”?
Fracture site changes
with age, wrist
fractures more common
in younger people, hip
fractures more common
in older people
Reaction times and gait
speed slows, balance
deteriorates, strength
reduces…..

Functional Ability in older ageFunctional Ability in older age
�� Strength (1 % to 2% p.a.)Strength (1 % to 2% p.a.)
�� Power (3% to 4% p.a.)Power (3% to 4% p.a.)
�� Bone density (Women:1% to 3%, Bone density (Women:1% to 3%, Men:0.4% p.a.)Men:0.4% p.a.)
�� Balance, Coordination and Balance, Coordination and reactionreaction
�� Transfer skillsTransfer skills
�� Maintenance of temperature Maintenance of temperature controlcontrol
�� Vision, hearing and other balance Vision, hearing and other balance sensory inputssensory inputs
EVEN HEALTHY OLDER PEOPLE LOSE...EVEN HEALTHY OLDER PEOPLE LOSE...
SedentarySedentary behaviourbehaviour increases the loss of performance...increases the loss of performance...

Falls Prevention ApproachesFalls Prevention Approaches
�� Individual Approach (high risk patients) Individual Approach (high risk patients)
–– MultiMulti--factorial (factorial (egeg. PROFET . PROFET -- Close et al, 1999Close et al, 1999))
�� 2004 Review 2004 Review -- MultifactorialMultifactorial trials reduce risk (RR 0.82) Chang 2004trials reduce risk (RR 0.82) Chang 2004
�� 2008 Review 2008 Review -- MultifactorialMultifactorial trials ineffective trials ineffective -- Gates 2008Gates 2008
–– UniUni--factorial (factorial (egeg.. FaMEFaME -- Skelton et al, 2005Skelton et al, 2005))
�� Exercise only trials reduce risk (RR 0.86) Chang 2004Exercise only trials reduce risk (RR 0.86) Chang 2004
�� Pacemakers, Cataract Removal, Medication Withdrawal Pacemakers, Cataract Removal, Medication Withdrawal
�� Population based approach (targeting communities)Population based approach (targeting communities)
–– Emerging evidence (Emerging evidence (McClure, 2005McClure, 2005))
–– Most include increasing awareness and Most include increasing awareness and physical activityphysical activity, ,
medication and home hazard reviewsmedication and home hazard reviews
�� Reductions in injuries 6Reductions in injuries 6--33% but no 33% but no RCTsRCTs

Falls ClinicsFalls Clinics
�� Geriatrician, Geriatrician, PhysioPhysio, OT, nurse, OT, nurse
�� StrengthsStrengths: Intensive CGA assessment and onward : Intensive CGA assessment and onward referralreferral–– Intended interventions not always undertakenIntended interventions not always undertaken
–– Not always evidence based interventions Not always evidence based interventions
� Weaknesses: different messages from different professionals, lots of double handling and assessment but little ‘action’, lots of waiting around, concern about institutionalisation….lots of DNAs…
� Reports of attendance suggest that the population reach of fall clinics is low (<3% of the population at risk)
Lamb 2008, Gates 2008

OT InterventionOT Intervention
Cumming et al, JAGS 1999 - 65+ years, 1 year, n= 530, RCT- OT home visit < 3 wks hospital discharge- list of recommendations and telephone call 2 wks later - Subjects with fall(s): 36% vs 45% [p=0.05]
Interactive interventions delivered by professionals involving older people in discussion around falls, behaviour and lifestyle are more
successful with high risk groups
(WHO 2007)

Objective 1: Improve outcomes and improve efficiency of care after hip
fractures – by following the 6 “Blue
Book” standards
Hip
fracture patients
Objective 2: Respond to the first
fracture, prevent the second – through
Fracture Liaison Services in acute and primary care
Non-hip fragility fracture patients
Objective 3: Early intervention to restore
independence – through falls care pathway linking acute and
urgent care services to
secondary falls prevention
Individuals at high risk
of 1st fragility fracture or other injurious falls
Objective 4: Prevent frailty, preserve bone health, reduce accidents –
through preserving physical
activity, healthy lifestyles and reducing environmental hazards
Older people
DH 2009: falls & fracture care & DH 2009: falls & fracture care &
prevention: four key objectivesprevention: four key objectives

–– Consider major modifiable Consider major modifiable risk factorsrisk factors
–– Consider bone health / Consider bone health / risk of fracturerisk of fracture
–– Consider if onward Consider if onward referral necessaryreferral necessary
–– Not be repeated by Not be repeated by everyone that comes into everyone that comes into contact with an older contact with an older person!person!
–– Lead to effective Lead to effective interventionsinterventions
–– Be predictive??Be predictive??
Oliver 2009Oliver 2009

Falls prediction tools in Falls prediction tools in
different settingsdifferent settings
�� Systematic review of tools to predict falls (up to June 2004)Systematic review of tools to predict falls (up to June 2004)
�� Validity and reliabilityValidity and reliability
�� Wide range of tools and settingsWide range of tools and settings
–– Community setting Community setting –– 23 tools (14 studies)23 tools (14 studies)
–– Acute setting Acute setting –– 8 tools (12 studies)8 tools (12 studies)
–– Long term care setting Long term care setting –– 10 tools (6 studies)10 tools (6 studies)
�� Of the 38 tools Of the 38 tools
–– 11 were 11 were multifactorialmultifactorial toolstools
–– 27 were functional mobility assessment tools27 were functional mobility assessment tools
�� Few tools were found that were tested more than once or in more Few tools were found that were tested more than once or in more than one settingthan one setting
�� No single tool can be recommended for use in all settings or forNo single tool can be recommended for use in all settings or for all all subpopulations within each settingsubpopulations within each setting..
Scott V et al. Age Ageing. 2007; 36:Scott V et al. Age Ageing. 2007; 36: 130130--99

Systematic reviews of tools Systematic reviews of tools
that predict risk of a future fallthat predict risk of a future fall
�� Myers H 2003Myers H 2003
�� Oliver D et al 2004Oliver D et al 2004
�� Scott V et al 2007Scott V et al 2007
�� Hill K and Haines T 2008Hill K and Haines T 2008
�� All cast doubt on predictive validity of falls toolsAll cast doubt on predictive validity of falls tools
�� And show up the almost total lack of validated tools And show up the almost total lack of validated tools
in community or nursing home or mental health in community or nursing home or mental health
settingsetting

So what about case So what about case
finding for bone fragility?finding for bone fragility?
Used to determine 10 year fracture risk in community dwelling adults –
then NOGG suggests guidance on treatment

How useful is the fracture Risk How useful is the fracture Risk
Assessment Tool (FRAX) in a falls clinic Assessment Tool (FRAX) in a falls clinic
population?population?
�� NOGG advice (DEXA or treat) followed:NOGG advice (DEXA or treat) followed:
–– 46% (n=6) of those with OP at either spine and/or hip would 46% (n=6) of those with OP at either spine and/or hip would not be treated or advised a DEXAnot be treated or advised a DEXA
–– Of those where DEXA was advised (n=18), 72% did not have Of those where DEXA was advised (n=18), 72% did not have osteoporosis (n=13)osteoporosis (n=13)
–– Treatment advised in 2 patients both of whom had osteoporosis Treatment advised in 2 patients both of whom had osteoporosis on subsequent DEXAon subsequent DEXA
�� McCarthy C, Skelton DA,McCarthy C, Skelton DA, GallacherGallacher S, Mitchell LE S, Mitchell LE �� Abstract presented at 10Abstract presented at 10thth National Conference on Postural Stability and Falls, National Conference on Postural Stability and Falls,
Blackpool, 07/09/09Blackpool, 07/09/09

Tools to target your Tools to target your
intervention intervention egeg. .
Balance and Strength Exercise (group or home) /
Walking aids
Lower Urinary Tract Symptoms Continence training /
Surgical / Medical
Fear of Falling CBT / Counselling /
Exercise / Hip Protectors
Vestibular Function Vestibular Rehabilitation Exercise
Surgery
Postural Hypotension Pre-transfer exercise / Behavioural
Surgical stockings / Medical
Vision Surgery / Glasses / OT
Foot health Chiropody / Insoles / Surgery
……

Different costs to interventionsDavis 2010

Weaknesses in EvidenceWeaknesses in Evidence
�� Falls definitionFalls definition
�� Consensus on outcome measuresConsensus on outcome measures
�� Consensus on reporting intervention detailConsensus on reporting intervention detail
�� ? Fall per unit of activity ? Fall per unit of activity –– exposure to riskexposure to risk
�� Different models of delivery?Different models of delivery?
�� Cost effectiveness and utility reporting rareCost effectiveness and utility reporting rare
�� Poor fidelity at implementation (Poor fidelity at implementation (egeg. 12 week exercise . 12 week exercise
programme programme ��))Lamb 2005, 2008,
Skelton & Todd 2004

Exercise to Prevent FallsExercise to Prevent Falls
Exercise Exercise couldcould help fallers in a number of ways:help fallers in a number of ways:
�� Reducing Falls (or injurious falls) Reducing Falls (or injurious falls)
�� Reducing known Risk Factors for Reducing known Risk Factors for
Falls Falls
�� Reducing Fractures ? (or changing Reducing Fractures ? (or changing
the site of fracture)the site of fracture)
�� Increasing Quality of Life & Social Increasing Quality of Life & Social
ActivitiesActivities
�� Improving bone densityImproving bone density
�� Reducing FearReducing Fear
�� Reducing Long LiesReducing Long Lies
�� Reducing InstitutionalisationReducing Institutionalisation
Sherrington 2008; Skelton & Dinan 1999; NICE 2004

Not all physical activity is Not all physical activity is
safe for fallers!safe for fallers!
�� RCT Increasing physical activity in RCT Increasing physical activity in
people with previous upper arm people with previous upper arm
fracturefracture
�� Intervention: Brisk walkingIntervention: Brisk walking
�� Control: exercise of upper armControl: exercise of upper arm
�� Falls risk Falls risk ↑↑ (Brisk walking > control)(Brisk walking > control)
�� Fracture risk Fracture risk ↑↑ (Brisk walking > (Brisk walking >
control)control)
�� Beware unsafe pavements!Beware unsafe pavements!
Ebrahim et al. (1997)
NICE 2004 do not recommend brisk walking!

Tai Chi Tai Chi –– secondary secondary prevention in younger years ?prevention in younger years ?
-- Community Dwelling older people Community Dwelling older people -- mild deficits of strength/balancemild deficits of strength/balance-- 2x/week for 15 weeks2x/week for 15 weeks–– Cut trip and fall rate byCut trip and fall rate by halfhalf
- Frail older adults aged 70-97- 2 x/week for 48 weeks- no significant reduction in risk of falls
Wolf et al. J Am Wolf et al. J Am Wolf et al. J Am Wolf et al. J Am GeriatGeriatGeriatGeriat Soc 2003; 55: 1693Soc 2003; 55: 1693Soc 2003; 55: 1693Soc 2003; 55: 1693----1701170117011701
Wolf et al. Wolf et al. Wolf et al. Wolf et al. Wolf et al. Wolf et al. Wolf et al. Wolf et al. (1996)(1996)(1996)(1996)(1996)(1996)(1996)(1996)
- Community Dwelling older people aged 70+ Community Dwelling older people aged 70+ Community Dwelling older people aged 70+ Community Dwelling older people aged 70+ - 3 x/week for 24 weeks3 x/week for 24 weeks3 x/week for 24 weeks3 x/week for 24 weeks
- IncreasedIncreasedIncreasedIncreased Falls SelfFalls SelfFalls SelfFalls Self----EfficacyEfficacyEfficacyEfficacy (ABC) and (ABC) and (ABC) and (ABC) and DecreasedDecreasedDecreasedDecreased Fear of FallingFear of FallingFear of FallingFear of Falling (SAFFE) (SAFFE) (SAFFE) (SAFFE) Li et al. J Li et al. J Li et al. J Li et al. J Li et al. J Li et al. J Li et al. J Li et al. J GerontolGerontolGerontolGerontolGerontolGerontolGerontolGerontol B B B B B B B B PsycholPsycholPsycholPsycholPsycholPsycholPsycholPsychol SciSciSciSciSciSciSciSci Soc Soc Soc Soc Soc Soc Soc Soc SciSciSciSciSciSciSciSci 2005; 60:P342005; 60:P342005; 60:P342005; 60:P342005; 60:P342005; 60:P342005; 60:P342005; 60:P34--------4040404040404040

Overall (I-squared = 61.5%, p = 0.000)
Ebrahim, 1997
Barnett, 2003
Woo, Tai Chi, 2007
Luukinen, 2007
Campbell, 2005
Schoenfelder, 2000
Sihvonen, 2004
Lord, 2003
Buchner, 1997
Author,
Nowalk, Tai Chi, 2001
Mulrow, 1994
Day, 2002
Reinsch, 1992
Skelton, 2005
Wolf, Balance, 1996
Woo, Resistance, 2007
Wolf, Tai Chi, 1996
year
McMurdo, 1997
Korpelainen, 2006
Morgan, 2004
Campbell, 1999
Hauer, 2001
Voukelatos, 2007
Faber, Functional walking, 2006
Li, 2005
Lord, 1995
Schnelle, 2003
Steinberg, 2000
Faber, Tai Chi, 2006
Liu-Ambrose, Resistance, 2004
Lin, 2007
Bunout, 2005
Liu-Ambrose, Agility, 2004
Resnick, 2002
Latham, 2003
Madureira, 2007
Carter, 2002
Green, 2002
Toulotte, 2003
Wolf, 2003
Cerny, 1998
Sakamoto, 2006Rubenstein, 2000
Means, 2005
Protas, 2006
Suzuki, 2004
Campbell, 1997
Nowalk, Resist./Endurance, 2001
Robertson, 2001
0.83 (0.75, 0.91)
1.29 (0.90, 1.83)
0.60 (0.36, 0.99)
0.49 (0.24, 0.99)
0.93 (0.80, 1.09)
1.15 (0.82, 1.61)
3.06 (1.61, 5.82)
0.38 (0.17, 0.87)
0.78 (0.62, 0.99)
0.61 (0.40, 0.94)
Effect
0.77 (0.46, 1.28)
1.26 (0.90, 1.76)
0.82 (0.70, 0.97)
1.24 (0.77, 1.98)
0.69 (0.50, 0.96)
0.98 (0.71, 1.34)
0.78 (0.41, 1.48)
0.51 (0.36, 0.72)
size (95% CI)
0.53 (0.28, 0.98)
0.79 (0.59, 1.05)
1.05 (0.66, 1.68)
0.87 (0.36, 2.10)
0.75 (0.46, 1.25)
0.67 (0.46, 0.97)
1.32 (1.03, 1.69)
0.45 (0.33, 0.62)
0.85 (0.57, 1.27)
0.62 (0.38, 1.00)
0.90 (0.79, 1.03)
0.96 (0.76, 1.22)
1.80 (0.67, 4.85)
0.67 (0.32, 1.41)
1.22 (0.70, 2.14)
1.03 (0.36, 2.98)
0.71 (0.04, 11.58)
1.08 (0.87, 1.35)
0.48 (0.25, 0.93)
0.88 (0.32, 2.41)
1.34 (0.87, 2.07)
0.08 (0.00, 1.37)
0.75 (0.52, 1.08)
0.87 (0.17, 4.29)
0.82 (0.64, 1.04)0.90 (0.42, 1.91)
0.41 (0.21, 0.77)
0.62 (0.26, 1.48)
0.35 (0.14, 0.90)
0.68 (0.52, 0.89)
0.96 (0.63, 1.46)
0.54 (0.32, 0.91)
100.00
2.64
1.88
1.22
3.85
2.74
1.40
0.98
3.38
2.21
%
1.88
2.75
3.80
2.04
2.81
2.86
1.41
2.67
Weight
1.48
3.05
2.04
0.88
1.89
2.56
3.31
2.87
2.38
1.98
3.97
3.34
0.72
1.13
1.67
0.65
0.11
3.46
1.34
0.70
2.21
0.10
2.58
0.31
3.341.11
1.40
0.88
0.80
3.13
2.27
1.84
0.83 (0.75, 0.91)
1.29 (0.90, 1.83)
0.60 (0.36, 0.99)
0.49 (0.24, 0.99)
0.93 (0.80, 1.09)
1.15 (0.82, 1.61)
3.06 (1.61, 5.82)
0.38 (0.17, 0.87)
0.78 (0.62, 0.99)
0.61 (0.40, 0.94)
Effect
0.77 (0.46, 1.28)
1.26 (0.90, 1.76)
0.82 (0.70, 0.97)
1.24 (0.77, 1.98)
0.69 (0.50, 0.96)
0.98 (0.71, 1.34)
0.78 (0.41, 1.48)
0.51 (0.36, 0.72)
size (95% CI)
0.53 (0.28, 0.98)
0.79 (0.59, 1.05)
1.05 (0.66, 1.68)
0.87 (0.36, 2.10)
0.75 (0.46, 1.25)
0.67 (0.46, 0.97)
1.32 (1.03, 1.69)
0.45 (0.33, 0.62)
0.85 (0.57, 1.27)
0.62 (0.38, 1.00)
0.90 (0.79, 1.03)
0.96 (0.76, 1.22)
1.80 (0.67, 4.85)
0.67 (0.32, 1.41)
1.22 (0.70, 2.14)
1.03 (0.36, 2.98)
0.71 (0.04, 11.58)
1.08 (0.87, 1.35)
0.48 (0.25, 0.93)
0.88 (0.32, 2.41)
1.34 (0.87, 2.07)
0.08 (0.00, 1.37)
0.75 (0.52, 1.08)
0.87 (0.17, 4.29)
0.82 (0.64, 1.04)0.90 (0.42, 1.91)
0.41 (0.21, 0.77)
0.62 (0.26, 1.48)
0.35 (0.14, 0.90)
0.68 (0.52, 0.89)
0.96 (0.63, 1.46)
0.54 (0.32, 0.91)
100.00
2.64
1.88
1.22
3.85
2.74
1.40
0.98
3.38
2.21
%
1.88
2.75
3.80
2.04
2.81
2.86
1.41
2.67
Weight
1.48
3.05
2.04
0.88
1.89
2.56
3.31
2.87
2.38
1.98
3.97
3.34
0.72
1.13
1.67
0.65
0.11
3.46
1.34
0.70
2.21
0.10
2.58
0.31
3.341.11
1.40
0.88
0.80
3.13
2.27
1.84
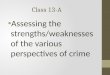
Favours exercise Favours control
1.25 .5 1 2 4
RR = 0.8395%CI 0.75-0.91
P<0.001
17%
reduction
in falls
ResultsResults
I² = 62% moderate
heterogeneity
Sherrington et al., JAGS 2008

Highly challenging Balance TrainingHighly challenging Balance Training
�� Exercise in standing involving:Exercise in standing involving:
–– movement of the centre of massmovement of the centre of mass
–– narrowing of the base of supportnarrowing of the base of support
–– minimisingminimising upper limb supportupper limb support
24%
RR 0.76(95%CI =0.62 to 0.93)
Sherrington et al., JAGS 2008

High DoseHigh Dose
�� 50+ hours 50+ hours
–– At least 2 hours a week of exercise At least 2 hours a week of exercise for at least 6 monthsfor at least 6 months
–– Home or groupHome or group--based or a based or a combination of bothcombination of both
20%
RR 0.80(95%CI =0.65 to 0.99)
Sherrington et al., JAGS 2008

No reduction:
RR 0.95 (0.78 to 1.16)
No reduction:
RR 0.96 (0.80 to 1.16)
No reduction:
RR 0.91 (0.79 to 1.05)
Increased risk: RR 1.20 (1.00 to 1.44)
High balanceLow dose
Walking
Low balanceLow dose
Walking
Low balanceLow dose
No walking
Low balance
High doseWalking

Reducing barriersReducing barriers
��Walk from Home Walk from Home
��Keighley Peer MentorsKeighley Peer Mentors
Mary Moffat Mary Moffat -- 9393
–– Referred by physio after a fallReferred by physio after a fall
–– Loss of confidence and fear of Loss of confidence and fear of
fallingfalling
–– Isolated and lonely and Isolated and lonely and
dependent upon others to get dependent upon others to get
outout

Wider Benefits of ExerciseWider Benefits of Exercise
�� PsychologicalPsychological
–– Anxiety, depression, sleep, fear of fallingAnxiety, depression, sleep, fear of falling
�� PhysiologicalPhysiological
–– Maintain bone density, ability to perform everyday Maintain bone density, ability to perform everyday activities, reduce breathlessness, reduce stiffness and activities, reduce breathlessness, reduce stiffness and
chance of injurychance of injury
�� PsychosocialPsychosocial
–– Isolation, social contacts, peer support, playing with Isolation, social contacts, peer support, playing with grandchildren, using the bathgrandchildren, using the bath
�� Even the very frailEven the very frail
–– DVT, constipation, transfer skills DVT, constipation, transfer skills

Gaps in evidence….Gaps in evidence….
� Patient concordance and presentation of information
� Fear of falling and activity avoidance
� Ethnicity and Socioeconomic deprivation
� Reducing falls and injury in stroke, parkinson’s, dementia….
� Different professionals or models of delivery
� Different models of exercise (home vs group, games for health) and
necessary duration / intensity / frequency and type
� Different exercise in different population groups?
� Value of falls prevention on other outcomes (quality of life, depression,
other syndromes of ageing)
� Getting people to USE fall alarms
� Tele-health and technology opportunities

New technologies ?
•• Whole Body Vibration Whole Body Vibration •• 66 mthsmths, 3 x p/w, 3 x p/w
•• postpost--menopausal women menopausal women •• Strength 15%, Balance 20%,Strength 15%, Balance 20%,•• Hip BMD 1%Hip BMD 1%
VerschuerenVerschueren SM et al. 2004SM et al. 2004
Wii-fit (Nintendo) ?

Glasgow SECC Aug 13Glasgow SECC Aug 13--1717thth 20122012
www.wcaa2012.comwww.wcaa2012.com
dawn.dawn.skeltonskelton@@gcalgcal.ac..ac.ukuk