Embed Size (px)
Citation preview

Strengthening the Six Building Blocks of Local Nutrition Systems for the First 1000 Days
A City/Municipal Mayor’s Guide

Strengthening the Six Building Blocks of Local Nutrition Systems for the First 1000 Days: A City/Municipal Mayor’s Guide
Published by the Zuellig Family FoundationISBN Number 978-621-96188-0-9
Copyright 2019Zuellig Family Foundation (ZFF)Institute of Human Nutrition and Food (IHNF), College of Human Ecology (CHE), University of the Philippines Los Baños (UPLB)
EDITORIAL TEAM
IHNF, CHE, UPLBAngelina dR. FelixAna Lorraine D. Dela VegaGuien Eidrefson P. GarmaLeila S. Africa
ZFFAustere A. PanaderoAnthony Rosendo G. FaraonAxell M. Alterado
WRITERSAna Lorraine D. Dela VegaAngelina dR. FelixGuien Eidrefson P. GarmaAna B. CastañedaJoyce P. ParcoPamela A. Gonzales
LAYOUT ARTISTJanica M. Gan
i
Table of Contents
List of Acronyms — iiAcknowledgments — ivMessage from ZFF — vMessage from CHE, UPLB — viAbout the Guide — vii
OVERVIEW — 1Ang Kwento ni Mayumi — 2Your Journey Begins Here — 4
SECTION 1: INTRODUCTION — 8First 1000 Days of Life — 9The Nutrition Situation of My Community — 11What Can You Do as the Mayor? — 13Where is My Local Government Now? — 17Benefits of Investing in Nutrition as Development Priority — 20
SECTION 2: THE BUILDING BLOCKS OF LOCAL NUTRITION SYSTEM — 212.1: Strong Nutrition Leadership and Governance — 222.2: Efficient Nutrition Financing — 292.3: Adequate, Competent, and Client-Centered Human Resource — 312.4: Quality and Timely Nutrition Information System — 352.5: Equitable Access to Medicines, Vaccines, and Technology — 392.6: Responsive Delivery of Health and Nutrition Services — 40
SECTION 3: INNOVATION FOR SUSTAINABLE SERVICE DELIVERY — 45
SECTION 4: ESTABLISHING A FUNCTIONAL REFERRAL SYSTEM — 48
SUMMARY — 52
APPENDICES A: Medicines, Vaccines, and Technology — 56B: Evidence-Based Action on First 1000 Days — 62
ii
List of Acronyms
4Ps Product, Price, Place, PromotionAIP Annual Investment Plan/ProgramANC Antenatal CareBCPC Barangay Committee for the Protection of ChildrenBDC Barangay Development CouncilBDP Barangay Development PlanBHS Barangay Health StationBHW Barangay Health WorkerBL4ND Barangay Leadership for Nutrition and DevelopmentBNAP Barangay Nutrition Action PlanBNC Barangay Nutrition CommitteeBNS Barangay Nutrition ScholarCAN Compendium of Actions for NutritionCDP Comprehensive Development PlanCHE College of Human EcologyCHT Community Health TeamC/MHO City/Municipal Health OfficerC/MNAO City/Municipal Nutrition Action OfficerC/MNAP City/Municipal Nutrition Action PlanC/MNC City/Municipal Nutrition CommitteeC/MPDO City/Municipal Planning and Development OfficeDDS Diet Diversity ScoreDepEd Department of EducationDILG Department of the Interior and Local GovernmentDOH Department of HealthDOST Department of Science and TechnologyEBF Exclusive BreastfeedingELA Executive and Legislative AgendaF1KD First 1000 DaysFMRs Farm-to-Market Roads FNRI Food and Nutrition Research InstituteGAD Gender and DevelopmentGIDA Geographically Isolated and Disadvantaged AreaHCM Health Change ModelHH HouseholdIHNF Institute of Human Nutrition and FoodIRA Internal Revenue Allotment IYCF Infant and Young Child FeedingKGJF Kristian Gerhard Jebsen FoundationLCPC Local Committee for the Protection of ChildrenLDIP Local Development Investment PlanLGC Local Government CodeLGU Local Government UnitLINIS Local Integrated Nutrition Information SystemLIP Local Investment PlanLNAP Local Nutrition Action PlanLNC Local Nutrition CommitteeMAM Moderate Acute MalnutritionMAO Municipal Agriculture OfficeMC Memorandum Circular
iii
MELLPI Pro Monitoring and Evaluation of Local Level Plan Implementation ProtocolMNAS Municipal Nutrition Action ScorecardMNCHN Maternal Neonatal and Child Health NutritionMNP Micronutrient PowderMOOE Maintenance and Other Operating ExpensesMPDO Municipal Planning and Development OfficeMSWDO Municipal Social Welfare Development OfficeNGO Non-Government OrganizationNIS Nutrition Information SystemNNC National Nutrition CouncilNPM Nutrition Program ManagementOPT+ Operation Timbang PlusPCSO Philippine Charity Sweepstakes OfficePDP Philippine Development PlanPHN Public Health NursePIR Program Implementation ReviewPO People’s OrganizationPPA Programs, Projects, and ActivitiesPPAN Philippine Plan of Action for NutritionRA Republic ActRHM Rural Health MidwifeRHU Rural Health UnitRPRH Responsible Parenthood and Reproductive HealthSAM Severe Acute MalnutritionSDG Sustainable Development GoalsSMR Severe Malnutrition ReviewUNICEF United Nations Children’s Fund UPLB University of the Philippines Los BañosVAD Vitamin A Deficiency WASH Water Sanitation and HygieneWHO World Health OrganizationZFF Zuellig Family Foundation
iv
Acknowledgments
The editorial and writing team of this guide expresses its sincerest gratitude to the following, without whom, this guide would not be made possible.
• the Zuellig Family Foundation, for giving the team the opportunity and all the necessary support to work on this guide;
• to the Municipal Local Government Units of Looc, Romblon and Gamay, Northern Samar, for their invaluable inputs during the pretesting;
• to Prof. Nelson Jose Vincent B. Querijero, the project consultant for governance, for his constructive comments and suggestions for the improvement of the guide; and
• to Ms. Ma. Cristina L. Lanorio and Ms. Jazellee V. Laroza for their significant contributions and help to the team in the process of crafting this guide.
Maraming salamat po!
v
Message from ZFF
A 2015 assessment on the Philippines by the United Nations Children’s Fund found the country losing $4.5 billion annually due to undernutrition. This is brought by costs to treat otherwise preventable nutrition-related diseases, and deficits in performance and productivity.
Since Zuellig Family Foundation is focused on making sure maternal and health outcomes improve, we cannot overlook the nutrition of pregnant women and their babies. And of the types of child undernutrition, we found stunting to be far more complex since it requires a holistic and more focused intervention on the First 1000 Days.
There have been noteworthy programs introduced in the country. Key interventions are already known. There are even several feeding programs, and regular nutrition month activities. Yet all these have not been enough to address the country’s lingering stunting burden, which now affects over three million children.
With a problem this big, we cannot afford to have business as usual.
With over 10 years of experience implementing our Health Change Model, we learned that better health outcomes are more likely to be achieved in localities governed by Local Chief Executives (LCEs) who understand the complexity of health issues and are guided on what needs to be done to improve their local health systems.
With support from the Kristian Gerhard Jebsen Foundation, we applied the Health Change Model to nutrition. And in 2019, the partnership completed the pilot governance-based and systems-directed program for nutrition in First 1000 Days in Gamay, Northern Samar and Looc, Romblon.
The intervention successfully lowered the prevalence of stunting and wasting among 0-to-23-months old children, as well as anemia among pregnant women and 6-to-23-months old children.
Through our experiences and in collaboration with the University of the Philippines Los Baños Institute of Human Nutrition and Food, we wish to share with you, our Mayors, our learnings, while also guiding you as you improve your local nutrition systems for the First 1000 Days.
We hope you find this Guide useful, and we wish you all the best as you journey toward a malnutrition free municipality!
ERNESTO D. GARILAOPresident and ChairmanZuellig Family Foundation
vi
Message from CHE, UPLB
The United Nations Sustainable Development Goals (SDGs 2 and 3) clearly state the aim of achieving zero hunger and good health and well being, making nutrition a development priority. These goals recognized that nutrition remains a prevalent and relevant development concern in the Philippines and in the world.
With this important concern, nutrition needs to go beyond the usual programs and interventions to be addressed by all sectors of the government and society. Therefore, it is imperative to improve the nutritional status of population of a city or municipality by improving its local nutrition systems thereby transforming it into an integrated system, where various local government unit instrumentalities, stakeholders from the public and private sector, and the people in the community are actively involved and participating
This guide for local chief executives (LCEs), written by our professional colleagues at the Institute of Human Nutrition and Food (IHNF), College of Human Ecology (CHE), University of the Philippines Los Baños (UPLB), and published by the Zuellig Family Foundation (ZFF) will most certainly be useful for these administrators, particularly mayors, in making their local nutrition systems more responsive to the needs of the people in their areas. This publication also calls for an integration of all sectors of local government units (LGUs), enabling the interaction among city/municipal line agencies to provide nutrition-specific programs, with a focus on the first 1000 days of life of an individual.
Thus, I would like to congratulate ZFF and IHNF-CHE-UPLB for coming up with this initiative in preparing a manual on Improving Local Nutrition Systems in the First 1000 Days through the Six Building Blocks of Health. We look forward to having more collaborations like this for the improvement of nutrition and general welfare of the people in our communities and for the whole country.
Mabuhay!
RADEN G. PIADOZODeanUPLB College of Human Ecology

vii
About the Guide
This book is a concise, politically savvy guide that mayors can use to develop an integrated local nutrition system. The guide aims to inspire and entice mayors to pay utmost attention to nutrition in their community, and how many aspects of life in their community is affected by arising problems in nutrition, especially in the first 1000 days (F1KD) of life of a child. This guide can also be used by the various city/municipal local government unit (C/MLGU) instrumentalities, such as the local health office, local nutrition office, and representatives from the Department of Health (DOH).
The guide has four sections. The first section discusses an overview of the entire guide. It gives a sneak peek into why malnutrition should be addressed immediately, and how mayors can sys-tematically take action. ZFF Health Change Model (HCM), which outlines how dedicated leaders can achieve improved nutrition outcomes through developing an integrated local nutrition sys-tem based on the six building blocks of health, is also highlighted in the first part of the guide.
The second section discusses the importance of the first 1000 days, especially for mothers and their children. It also discusses the Philippine Plan of Action for Nutrition (PPAN) 2017-2022, the Philippines’ blueprint in combatting malnutrition. It also highlights how local government units (LGUs) contribute to achieving PPAN’s goals. How the concept of Bridging Leadership effectively contributes to the development of an integrated local nutrition system in the community is also discussed; mayors are then encouraged to become bridging leaders.
Further details on the building blocks, and the specifics on what to look out for in building the community’s nutrition system is discussed on the remaining sections of the guide. These focus on the enabling policies, mechanisms, and other key elements in nutrition leadership and gover-nance, nutrition financing, human resource, nutrition information system, medicines, vaccines, and technology, and services delivery.

1
ANG KWENTO NI MAYUMI
Mayumi, a one-year-old baby, and fifth child of her parents was born with a low birth weight (2.2 kg) and suffering from Severe Acute Malnutrition (SAM). She lives with her family in a Geographically Isolated and Disadvantaged Area (GIDA) barangay. Her parents, Samuel and Divina, were married at an early age. Divina was only 18 years old when she gave birth to her first child.
Because of their early marriage,
both Samuel and Divina stopped attending school. Samuel was forced to work at an early stage of his life. He is an on-call construction worker; his source of income is only Php 3,000 a month. Divina, meanwhile, is a housewife taking care of Mayumi and her siblings.
They are living with Divina’s
relatives, and their makeshift house is made up of poor and light materials. The foundation, roof, and walls are made of bamboo and nipa. They have no proper flooring in their house, thus, exposing Mayumi to dirt. They do not
have a proper toilet facility in their house, so they defecate in an open pit beside it. The only source of water in their house is a man-made well and they do not boil the water used for drinking.
Divina is unable to breastfeed her
child because she herself is suffering from malnutrition. As an alternative, she feeds her child with am, that is, only when they are able to buy rice.
Because their family lives in a GIDA, they have limited access to health services. Health workers also have difficulties in reaching their community. While the barangay has a Barangay Health Worker and a Barangay Nutrition Scholar, they are unable to deliver health services and they do not feel empowered in doing their work because of the low incentives given by the municipality. The Barangay Health Station on the island is also empty, owing to the lack of facilities and even educational and informational materials.
Are there similar stories like Mayumi’s in your area? Are you going to act if you have the same case as
Mayumi’s? If yes, what actions will you take?
4
Your Journey Begins Here
Just like Mayumi, there are many children in the Philippines that are affected by malnutrition. The number of stunted (bansot) and wasted (payat) children in the country remains significant. Urgent actions must be done to address this.
As the mayor, you can act on this problem and help in solving the woes of malnutrition in your community and in our country. This guide will discuss everything that you and your local government unit (LGU) instrumentalities need to improve your local food and nutrition system, with a focus on the first 1000 days of life.
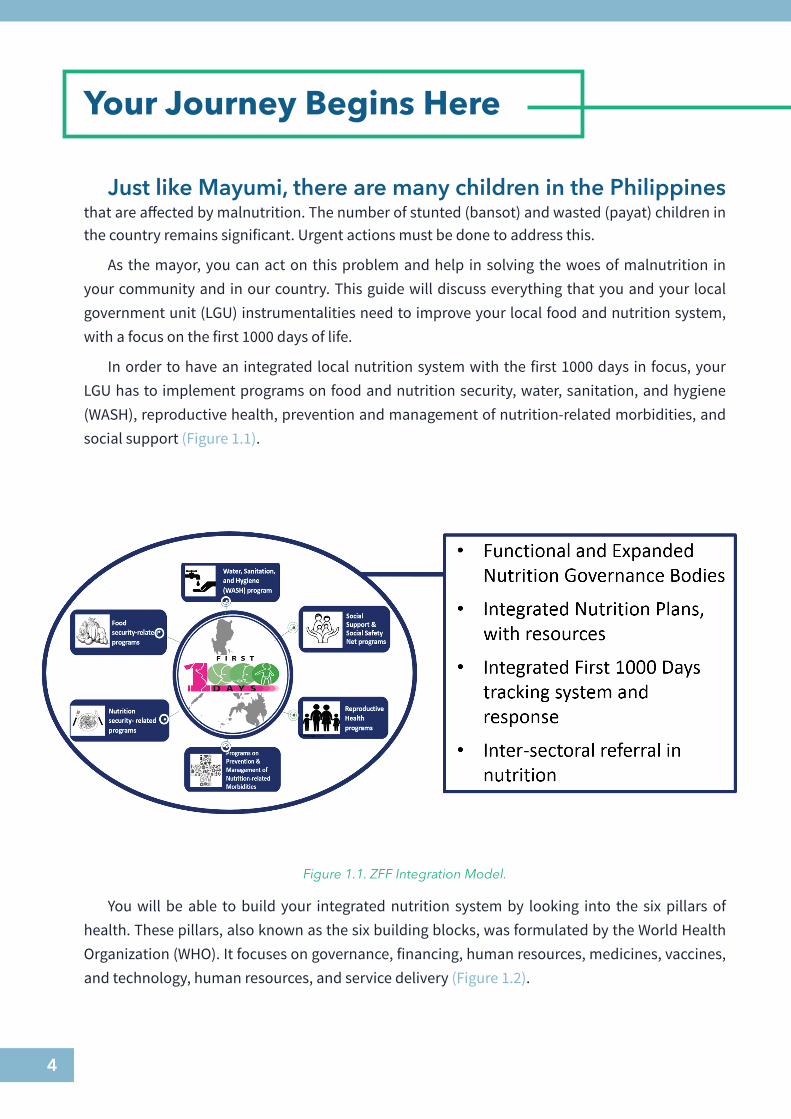
In order to have an integrated local nutrition system with the first 1000 days in focus, your LGU has to implement programs on food and nutrition security, water, sanitation, and hygiene (WASH), reproductive health, prevention and management of nutrition-related morbidities, and social support (Figure 1.1).
You will be able to build your integrated nutrition system by looking into the six pillars of health. These pillars, also known as the six building blocks, was formulated by the World Health Organization (WHO). It focuses on governance, financing, human resources, medicines, vaccines, and technology, human resources, and service delivery (Figure 1.2).
Figure 1.1. ZFF Integration Model.

5
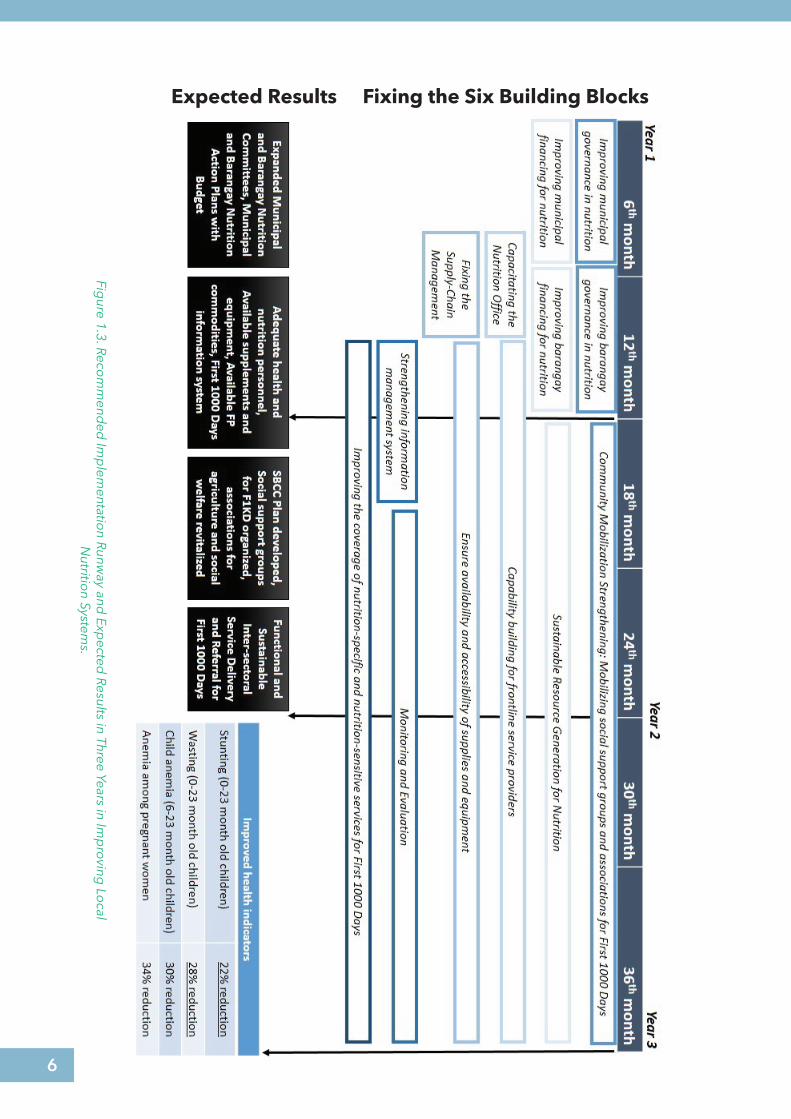
The integration model and the building blocks may look daunting. However, you can do everything that you need to do to improve your nutrition system within your three-year term. By focusing on particular building blocks first and foremost, then starting to improve on the other building blocks as time goes, your area will then have an improved and integrated local nutrition system before the end of your term (Figure 1.3).
Figure 1.2. Health Systems Framework (WHO, 2009).
6
Figure 1.3. Reco
mm
ended
Imp
lementatio
n Runway and
Expected
Results in Three Years in Imp
roving
Local
Nutritio
n Systems.
Expected Results Fixing the Six Building Blocks
7
Investing in nutrition reflects good governance. This means that by paying attention to your nutrition system, you and your community will have political and development benefits. A well-nourished citizenry contributes more and better to the development of your community.
Politically, LGUs that are excellent in implementing their nutrition programs are rewarded with awards from various national government entities, such as the National Nutrition Council (NNC). These LGUs are also promoted as champions in nutrition. If these LGUs are able to do it, despite how hard the challenge is, you can, too.
Are you ready to take on the challenge? The following sections of the guide will discuss everything in detail. Carry on with your nutrition journey towards having a healthier community!
SECTION 1: IntroductionSECTION 2: The Building Blocks of Local Nutrition SystemSECTION 2.1: Strong Nutrition Leadership and GovernanceSECTION 2.2: Efficient Nutrition FinancingSECTION 2.3: Adequate, Competent, and Client-Centered Human ResourceSECTION 2.4: Quality and Timely Nutrition Information SystemSECTION 2.5: Equitable Access to Medicines, Vaccines, and Technology SECTION 2.6: Responsive Delivery of Health and Nutrition ServicesSECTION 3: Innovation for Sustainable Service DeliverySECTION 4: Establishing a Functional Referral System
8
Introduction 1
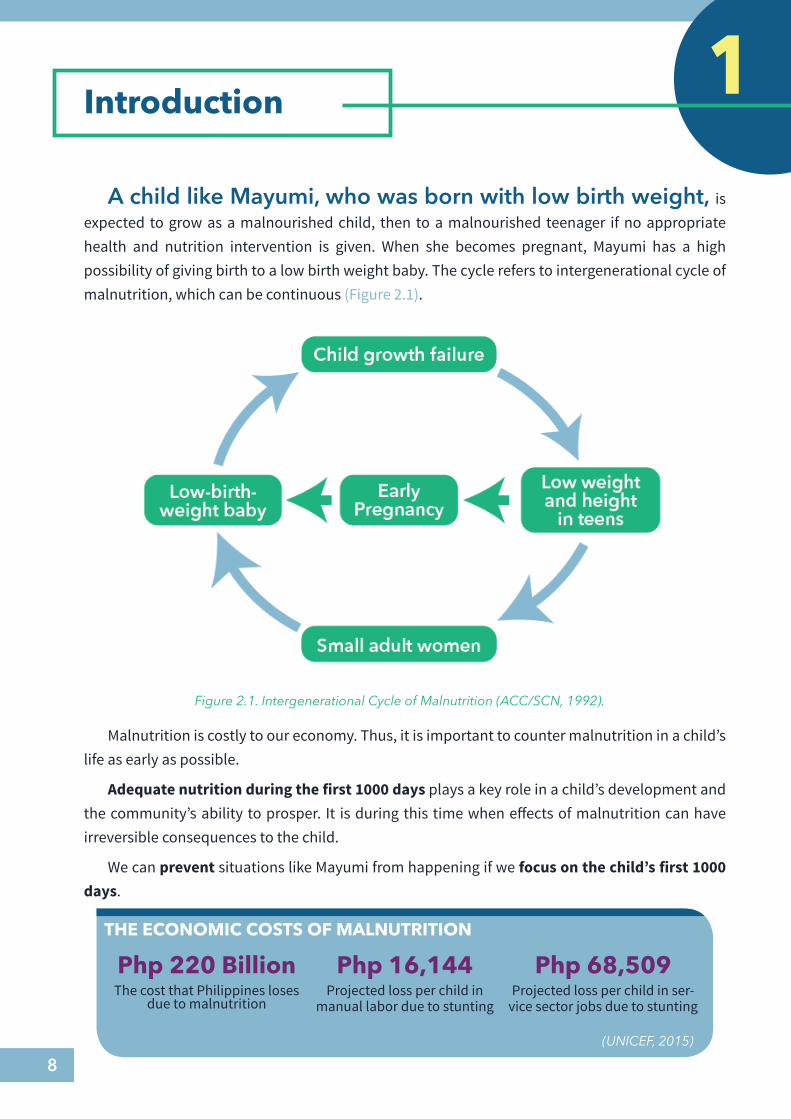
Figure 2.1. Intergenerational Cycle of Malnutrition (ACC/SCN, 1992).
THE ECONOMIC COSTS OF MALNUTRITION
Php 220 BillionThe cost that Philippines loses
due to malnutrition
Php 16,144Projected loss per child in
manual labor due to stunting
Php 68,509Projected loss per child in ser-
vice sector jobs due to stunting
(UNICEF, 2015)
A child like Mayumi, who was born with low birth weight, is expected to grow as a malnourished child, then to a malnourished teenager if no appropriate health and nutrition intervention is given. When she becomes pregnant, Mayumi has a high possibility of giving birth to a low birth weight baby. The cycle refers to intergenerational cycle of malnutrition, which can be continuous (Figure 2.1).
Malnutrition is costly to our economy. Thus, it is important to counter malnutrition in a child’s life as early as possible.
Adequate nutrition during the first 1000 days plays a key role in a child’s development and the community’s ability to prosper. It is during this time when effects of malnutrition can have irreversible consequences to the child.
We can prevent situations like Mayumi from happening if we focus on the child’s first 1000 days.
9
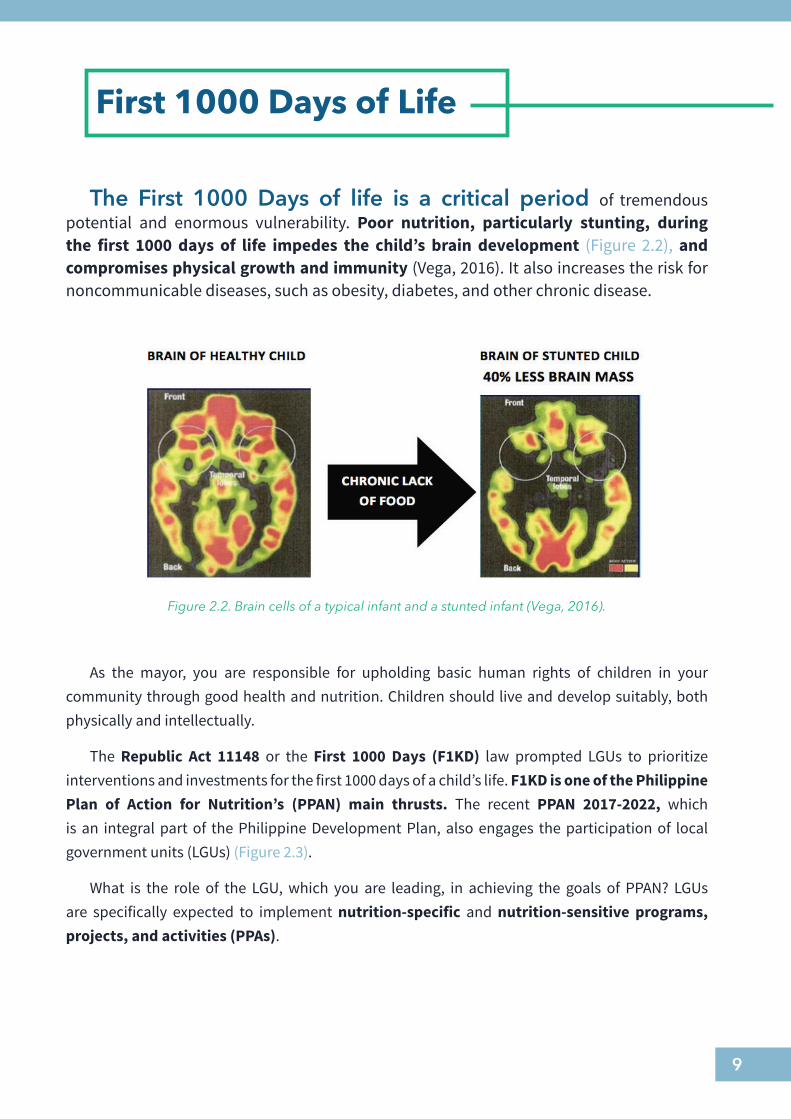
The First 1000 Days of life is a critical period of tremendous potential and enormous vulnerability. Poor nutrition, particularly stunting, during the first 1000 days of life impedes the child’s brain development (Figure 2.2), and compromises physical growth and immunity (Vega, 2016). It also increases the risk for noncommunicable diseases, such as obesity, diabetes, and other chronic disease.
Figure 2.2. Brain cells of a typical infant and a stunted infant (Vega, 2016).
As the mayor, you are responsible for upholding basic human rights of children in your community through good health and nutrition. Children should live and develop suitably, both physically and intellectually.
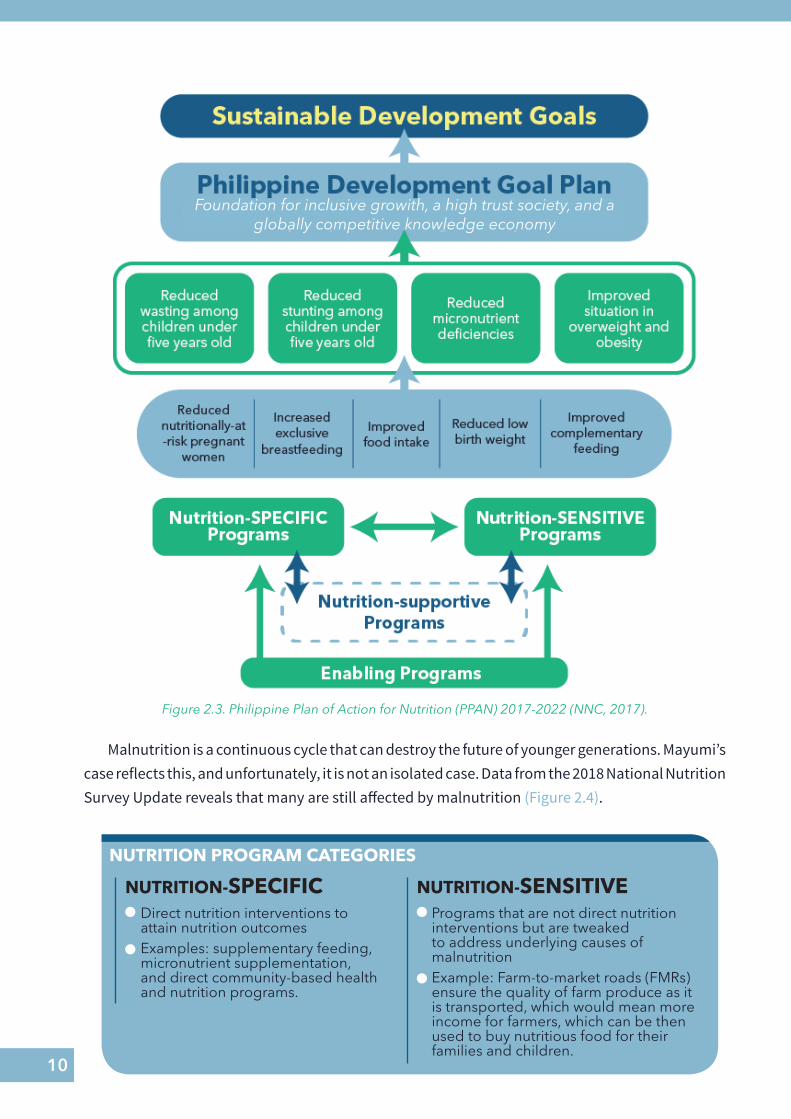
The Republic Act 11148 or the First 1000 Days (F1KD) law prompted LGUs to prioritize interventions and investments for the first 1000 days of a child’s life. F1KD is one of the Philippine Plan of Action for Nutrition’s (PPAN) main thrusts. The recent PPAN 2017-2022, which is an integral part of the Philippine Development Plan, also engages the participation of local government units (LGUs) (Figure 2.3).
What is the role of the LGU, which you are leading, in achieving the goals of PPAN? LGUs are specifically expected to implement nutrition-specific and nutrition-sensitive programs, projects, and activities (PPAs).
First 1000 Days of Life
10
Figure 2.3. Philippine Plan of Action for Nutrition (PPAN) 2017-2022 (NNC, 2017).
NUTRITION PROGRAM CATEGORIES
NUTRITION-SPECIFIC NUTRITION-SENSITIVEDirect nutrition interventions to attain nutrition outcomesExamples: supplementary feeding, micronutrient supplementation, and direct community-based health and nutrition programs.
Programs that are not direct nutrition interventions but are tweaked to address underlying causes of malnutritionExample: Farm-to-market roads (FMRs) ensure the quality of farm produce as it is transported, which would mean more income for farmers, which can be then used to buy nutritious food for their families and children.
Foundation for inclusive growith, a high trust society, and a globally competitive knowledge economy
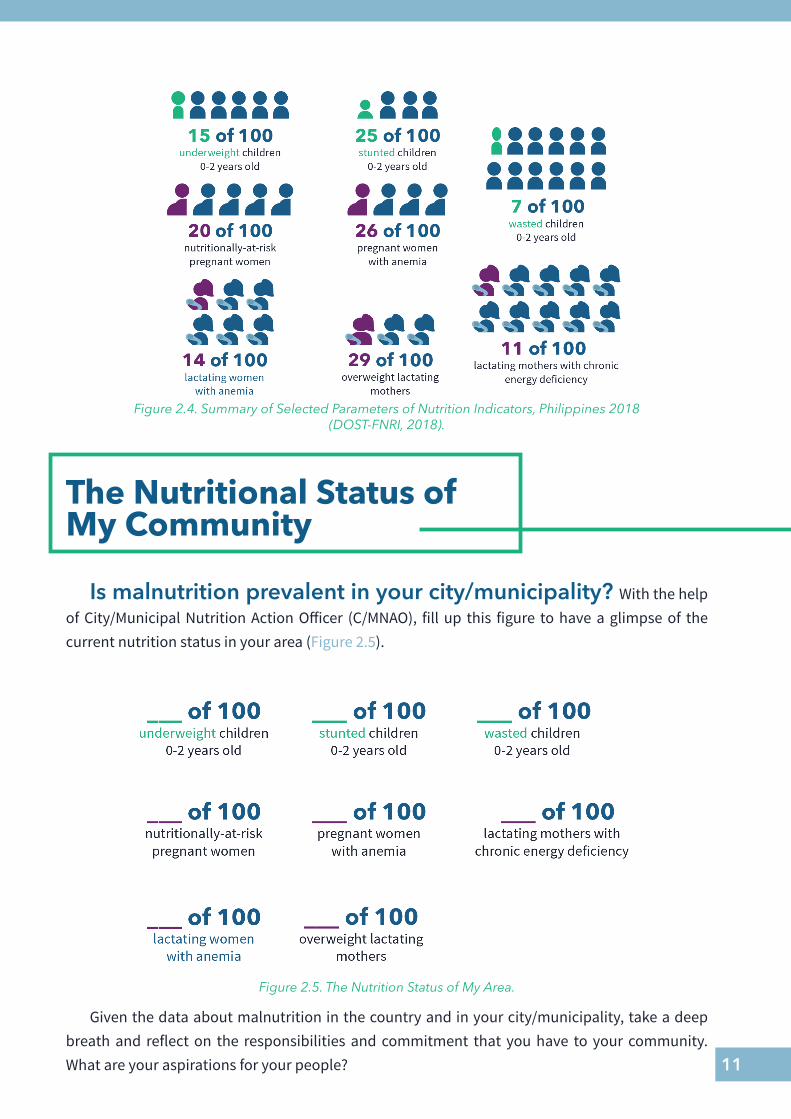
Malnutrition is a continuous cycle that can destroy the future of younger generations. Mayumi’s case reflects this, and unfortunately, it is not an isolated case. Data from the 2018 National Nutrition Survey Update reveals that many are still affected by malnutrition (Figure 2.4).
11
Figure 2.4. Summary of Selected Parameters of Nutrition Indicators, Philippines 2018 (DOST-FNRI, 2018).
The Nutritional Status of My Community
Is malnutrition prevalent in your city/municipality? With the help of City/Municipal Nutrition Action Officer (C/MNAO), fill up this figure to have a glimpse of the current nutrition status in your area (Figure 2.5).
Given the data about malnutrition in the country and in your city/municipality, take a deep breath and reflect on the responsibilities and commitment that you have to your community. What are your aspirations for your people?
Figure 2.5. The Nutrition Status of My Area.
12
You can lead us towards attaining good nutrition!
With your CHAMPIONING, you can lead your community towards attaining better nutrition
outcomes. Your leadership has the influence to fight malnutrition, especially on the first 1000 days of
life. As the mayor, you have the capacity, ability and influence to improve nutrition services of the mothers
and children in your community.
Each one of us has the responsibility in promoting good nutrition. It is our responsibility to fulfill the rights
of children like Mayumi to be well-nourished!
13
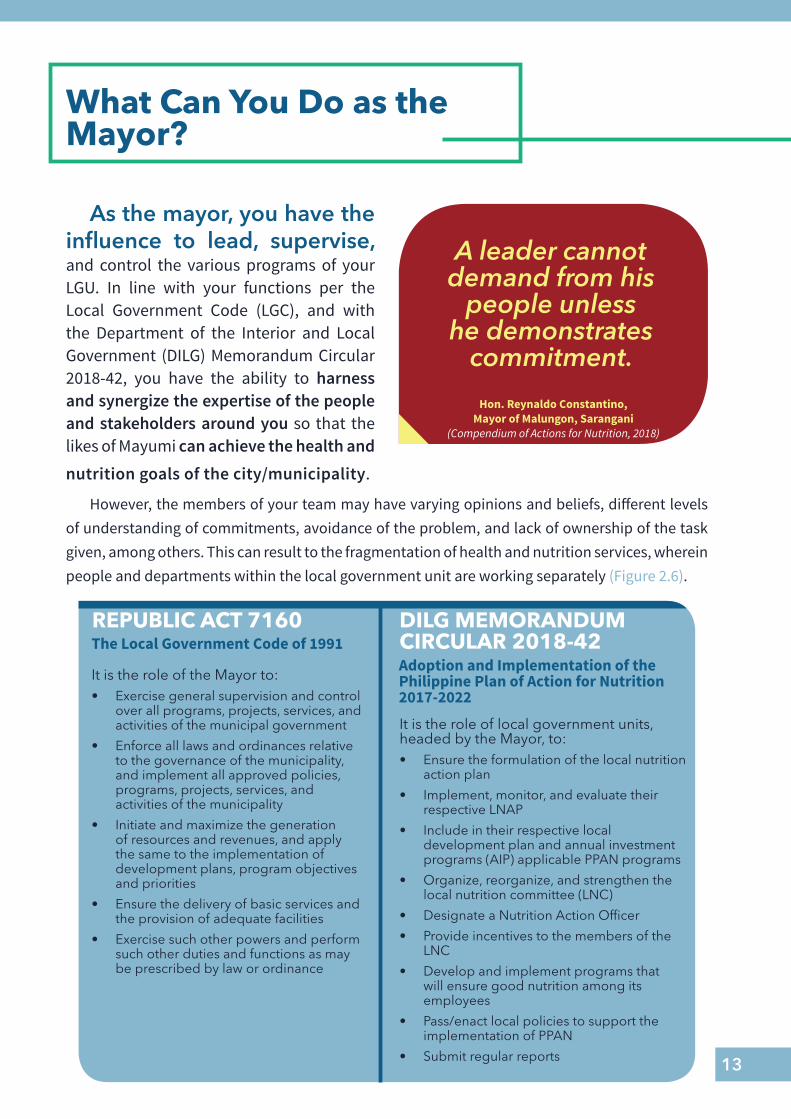
As the mayor, you have the influence to lead, supervise, and control the various programs of your LGU. In line with your functions per the Local Government Code (LGC), and with the Department of the Interior and Local Government (DILG) Memorandum Circular 2018-42, you have the ability to harness and synergize the expertise of the people and stakeholders around you so that the likes of Mayumi can achieve the health and
What Can You Do as the Mayor?
A leader cannot demand from his
people unless he demonstrates
commitment.
Hon. Reynaldo Constantino, Mayor of Malungon, Sarangani
(Compendium of Actions for Nutrition, 2018)
nutrition goals of the city/municipality.
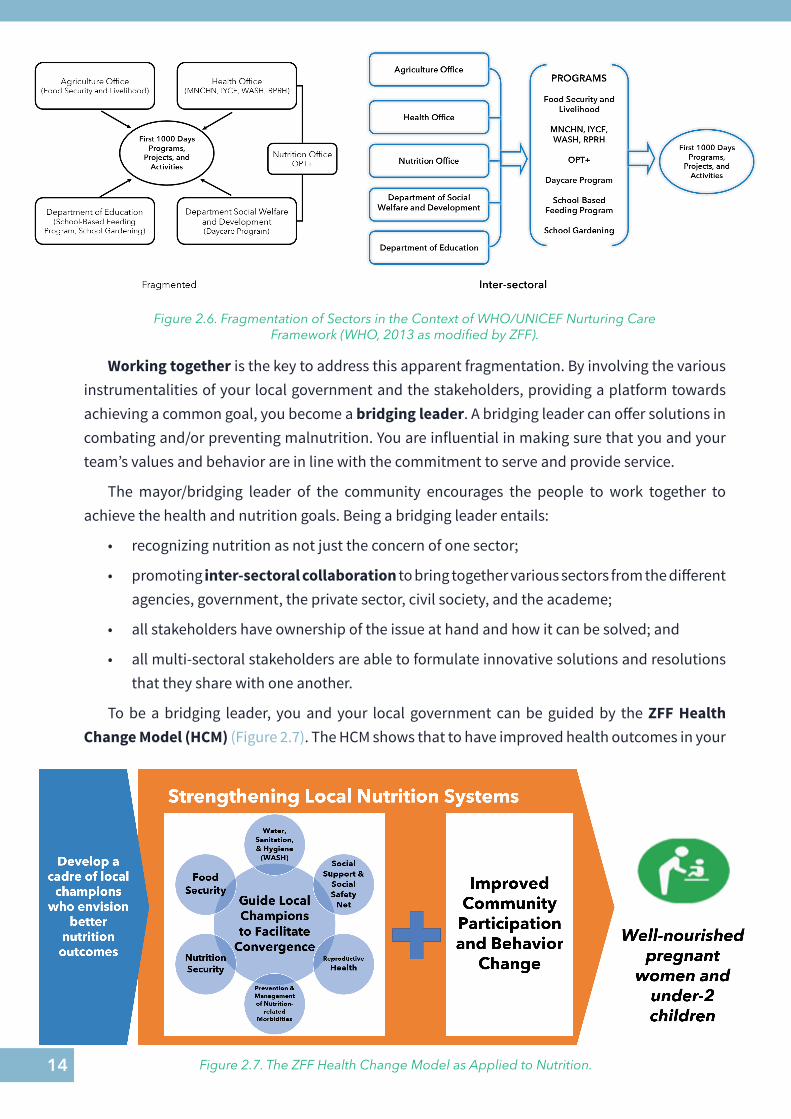
However, the members of your team may have varying opinions and beliefs, different levels of understanding of commitments, avoidance of the problem, and lack of ownership of the task given, among others. This can result to the fragmentation of health and nutrition services, wherein people and departments within the local government unit are working separately (Figure 2.6).
REPUBLIC ACT 7160
It is the role of the Mayor to:• Exercise general supervision and control
over all programs, projects, services, and activities of the municipal government
• Enforce all laws and ordinances relative to the governance of the municipality, and implement all approved policies, programs, projects, services, and activities of the municipality
• Initiate and maximize the generation of resources and revenues, and apply the same to the implementation of development plans, program objectives and priorities
• Ensure the delivery of basic services and the provision of adequate facilities
• Exercise such other powers and perform such other duties and functions as may be prescribed by law or ordinance
The Local Government Code of 1991DILG MEMORANDUM CIRCULAR 2018-42Adoption and Implementation of the Philippine Plan of Action for Nutrition 2017-2022
It is the role of local government units, headed by the Mayor, to:• Ensure the formulation of the local nutrition
action plan
• Implement, monitor, and evaluate their respective LNAP
• Include in their respective local development plan and annual investment programs (AIP) applicable PPAN programs
• Organize, reorganize, and strengthen the local nutrition committee (LNC)
• Designate a Nutrition Action Officer
• Provide incentives to the members of the LNC
• Develop and implement programs that will ensure good nutrition among its employees
• Pass/enact local policies to support the implementation of PPAN
• Submit regular reports
14
Working together is the key to address this apparent fragmentation. By involving the various instrumentalities of your local government and the stakeholders, providing a platform towards achieving a common goal, you become a bridging leader. A bridging leader can offer solutions in combating and/or preventing malnutrition. You are influential in making sure that you and your team’s values and behavior are in line with the commitment to serve and provide service.
The mayor/bridging leader of the community encourages the people to work together to achieve the health and nutrition goals. Being a bridging leader entails:
• recognizing nutrition as not just the concern of one sector;
• promoting inter-sectoral collaboration to bring together various sectors from the different agencies, government, the private sector, civil society, and the academe;
• all stakeholders have ownership of the issue at hand and how it can be solved; and
• all multi-sectoral stakeholders are able to formulate innovative solutions and resolutions that they share with one another.
To be a bridging leader, you and your local government can be guided by the ZFF Health Change Model (HCM) (Figure 2.7). The HCM shows that to have improved health outcomes in your
Figure 2.6. Fragmentation of Sectors in the Context of WHO/UNICEF Nurturing Care Framework (WHO, 2013 as modified by ZFF).
Figure 2.7. The ZFF Health Change Model as Applied to Nutrition.
15
community, even in such communities where Mayumi lives, you have to be a responsive leader, and that the health systems in your area should be responsive as well.
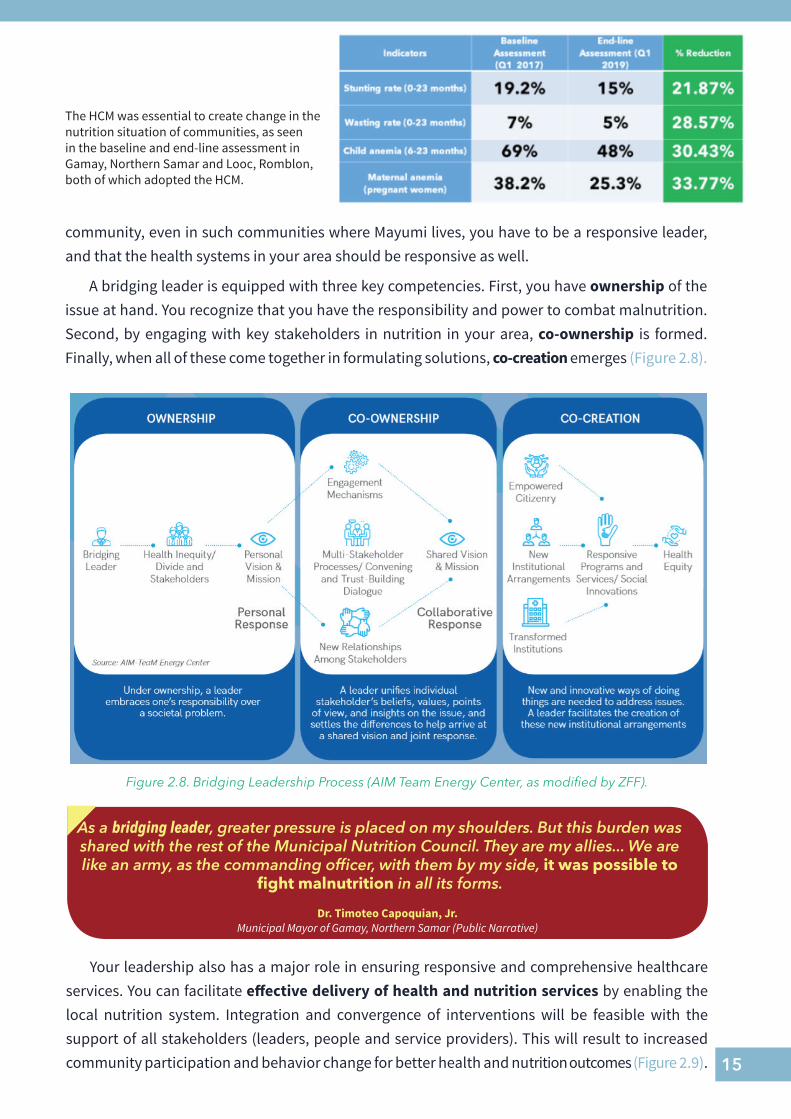
A bridging leader is equipped with three key competencies. First, you have ownership of the issue at hand. You recognize that you have the responsibility and power to combat malnutrition. Second, by engaging with key stakeholders in nutrition in your area, co-ownership is formed. Finally, when all of these come together in formulating solutions, co-creation emerges (Figure 2.8).
As a bridging leader, greater pressure is placed on my shoulders. But this burden was shared with the rest of the Municipal Nutrition Council. They are my allies... We are like an army, as the commanding officer, with them by my side, it was possible to
fight malnutrition in all its forms.
Dr. Timoteo Capoquian, Jr. Municipal Mayor of Gamay, Northern Samar (Public Narrative)
The HCM was essential to create change in the nutrition situation of communities, as seen in the baseline and end-line assessment in Gamay, Northern Samar and Looc, Romblon, both of which adopted the HCM.
Figure 2.8. Bridging Leadership Process (AIM Team Energy Center, as modified by ZFF).
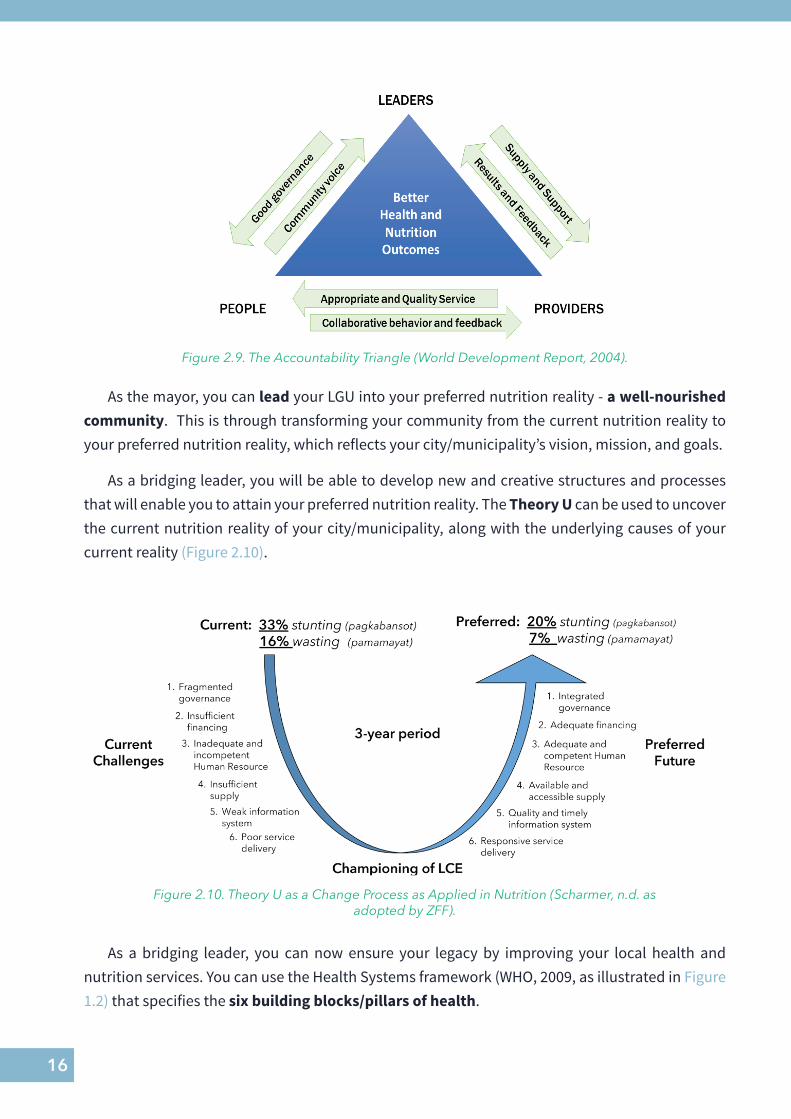
Your leadership also has a major role in ensuring responsive and comprehensive healthcare services. You can facilitate effective delivery of health and nutrition services by enabling the local nutrition system. Integration and convergence of interventions will be feasible with the support of all stakeholders (leaders, people and service providers). This will result to increased community participation and behavior change for better health and nutrition outcomes (Figure 2.9).
16
Figure 2.9. The Accountability Triangle (World Development Report, 2004).
Figure 2.10. Theory U as a Change Process as Applied in Nutrition (Scharmer, n.d. as adopted by ZFF).
As the mayor, you can lead your LGU into your preferred nutrition reality - a well-nourished community. This is through transforming your community from the current nutrition reality to your preferred nutrition reality, which reflects your city/municipality’s vision, mission, and goals.
As a bridging leader, you will be able to develop new and creative structures and processes that will enable you to attain your preferred nutrition reality. The Theory U can be used to uncover the current nutrition reality of your city/municipality, along with the underlying causes of your current reality (Figure 2.10).
As a bridging leader, you can now ensure your legacy by improving your local health and nutrition services. You can use the Health Systems framework (WHO, 2009, as illustrated in Figure 1.2) that specifies the six building blocks/pillars of health.
17
GUIDE QUESTIONS TOWARDS BRIDGING LEADERSHIP
1. Why do we need to invest in solving the problem of malnutrition in the first 1000 days, particularly in GIDA areas?
2. Why are you important in the fight against malnutrition?
3. What are your health and nutrition services roles and functions in the community including accountability of actions?
4. What is your existing health facility system that is helpful for health and nutrition?
5. Do the supervisory, administrative, and coordinative connections exist among the health and nutrition services providers and health facility system?
Where is My Local Government Now?
Looking at the current situation of your community, where would you focus your attention to solve malnutrition?
The six building blocks provide a guide to assess where your LGU’s current health and nutrition systems are functional, semi-functional, or non-functional.
The Kristian Gerhard Jebsen Foundation (KGJF) and the Zuellig Family Foundation (ZFF) modified the WHO six building blocks health systems into Municipal Nutrition Action Scorecard (MNAS), as presented in Figure 2.11. It was an effort to translate the six building blocks into actionable areas for integrated nutrition development in different localities. The tool hopes to provide mechanism to objectively monitor the progress of the integrated local nutrition system development.
... to be able to attain a sustainable program, one has to think of the six pillars [of the health
system].Hon. Leila Arboleda
Municipal Mayor of Looc, Romblon (Public Narrative)
To attain zero malnutrition and hunger through responsive and equitable health and nutrition services on the first 1000 days of life, your city/municipality should have the following six building blocks as applied to nutrition:
• Nutrition leadership and governance• Nutrition financing• Nutrition human resource• Medicines, vaccines, and technology• Nutrition information system• Health and nutrition service delivery
18
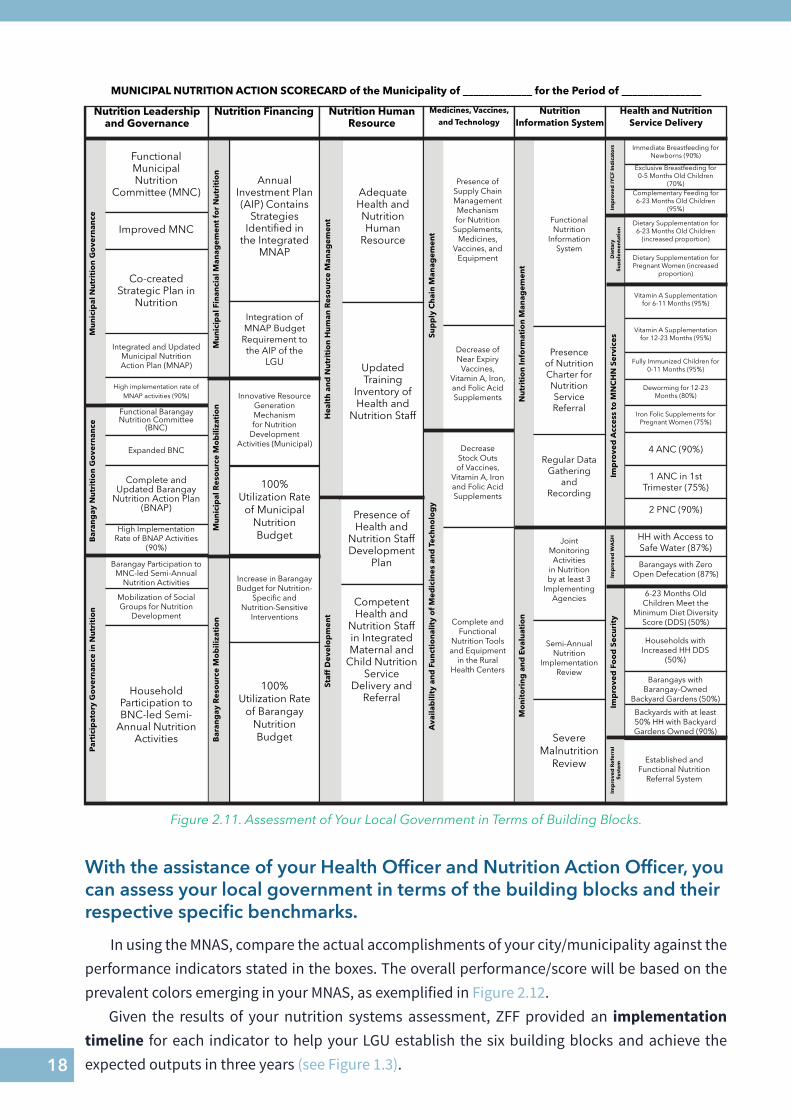
Figure 2.11. Assessment of Your Local Government in Terms of Building Blocks.
MUNICIPAL NUTRITION ACTION SCORECARD of the Municipality of _____________ for the Period of _______________
Nutrition Leadership and Governance
Nutrition Financing Nutrition Human Resource
Medicines, Vaccines, and Technology
Nutrition Information System
Health and Nutrition Service Delivery
Functional Municipal Nutrition
Committee (MNC)
Improved MNC
Co-created Strategic Plan in
Nutrition
Integrated and Updated Municipal Nutrition Action Plan (MNAP)
High implementation rate of MNAP activities (90%)
Functional Barangay Nutrition Committee
(BNC)
Expanded BNC
Complete and Updated Barangay
Nutrition Action Plan (BNAP)
High Implementation Rate of BNAP Activities
(90%)
Barangay Participation to MNC-led Semi-Annual
Nutrition Activities
Mobilization of Social Groups for Nutrition
Development
Household Participation to BNC-led Semi-
Annual Nutrition Activities
Mu
nic
ipal
Nu
trit
ion
Go
vern
ance
Bar
ang
ay N
utr
itio
n G
ove
rnan
cePa
rtic
ipat
ory
Go
vern
ance
in N
utr
itio
n
Mu
nic
ipal
Fin
anci
al M
anag
emen
t fo
r N
utr
itio
n
Annual Investment Plan (AIP) Contains
Strategies Identified in
the Integrated MNAP
Integration of MNAP Budget
Requirement to the AIP of the
LGU
Innovative Resource Generation Mechanism for Nutrition
Development Activities (Municipal)
100% Utilization Rate
of Municipal Nutrition Budget
Increase in Barangay Budget for Nutrition-
Specific and Nutrition-Sensitive
Interventions
100% Utilization Rate
of Barangay Nutrition Budget
Mu
nic
ipal
Res
ou
rce
Mo
bili
zati
on
Bar
ang
ay R
eso
urc
e M
ob
iliza
tio
n
Adequate Health and Nutrition Human
Resource
Updated Training
Inventory of Health and
Nutrition Staff
Presence of Health and
Nutrition Staff Development
Plan
Hea
lth
an
d N
utr
itio
n H
um
an R
eso
urc
e M
anag
emen
t
Competent Health and
Nutrition Staff in Integrated Maternal and
Child Nutrition Service
Delivery and Referral
Staf
f D
evel
op
men
t
Presence of Supply Chain Management Mechanism for Nutrition
Supplements, Medicines,
Vaccines, and Equipment
Decrease of Near Expiry
Vaccines, Vitamin A, Iron, and Folic Acid Supplements
Decrease Stock Outs of Vaccines,
Vitamin A, Iron and Folic Acid Supplements
Complete and Functional
Nutrition Tools and Equipment
in the Rural Health Centers
Sup
ply
Ch
ain
Man
agem
ent
Ava
ilab
ility
an
d F
un
ctio
nal
ity
of
Med
icin
es a
nd
Tec
hn
olo
gy
Functional Nutrition
Information System
Presence of Nutrition Charter for Nutrition Service Referral
Regular Data Gathering
and Recording
Joint Monitoring Activities
in Nutrition by at least 3
Implementing Agencies
Semi-Annual Nutrition
Implementation Review
Severe Malnutrition
Review
Nu
trit
ion
Info
rmat
ion
Man
agem
ent
Mo
nit
ori
ng
an
d E
valu
atio
n
Immediate Breastfeeding for Newborns (90%)
Exclusive Breastfeeding for 0-5 Months Old Children
(70%)Complementary Feeding for
6-23 Months Old Children (95%)
Dietary Supplementation for 6-23 Months Old Children
(increased proportion)
Dietary Supplementation for Pregnant Women (increased
proportion)
Vitamin A Supplementation for 6-11 Months (95%)
Vitamin A Supplementation for 12-23 Months (95%)
Fully Immunized Children for 0-11 Months (95%)
Deworming for 12-23 Months (80%)
Iron Folic Supplements for Pregnant Women (75%)
4 ANC (90%)
1 ANC in 1st Trimester (75%)
2 PNC (90%)
HH with Access to Safe Water (87%)
Barangays with Zero Open Defecation (87%)
6-23 Months Old Children Meet the
Minimum Diet Diversity Score (DDS) (50%)
Households with Increased HH DDS
(50%)
Barangays with Barangay-Owned
Backyard Gardens (50%)
Backyards with at least 50% HH with Backyard Gardens Owned (90%)
Established and Functional Nutrition
Referral System
Imp
rove
d IY
CF
Ind
icat
ors
Die
tary
Su
pp
lem
enta
tio
nIm
pro
ved
Acc
ess
to M
NC
HN
Ser
vice
sIm
pro
ved
WA
SHIm
pro
ved
Fo
od
Sec
uri
tyIm
pro
ved
Ref
erra
l Sy
stem
With the assistance of your Health Officer and Nutrition Action Officer, you can assess your local government in terms of the building blocks and their respective specific benchmarks.
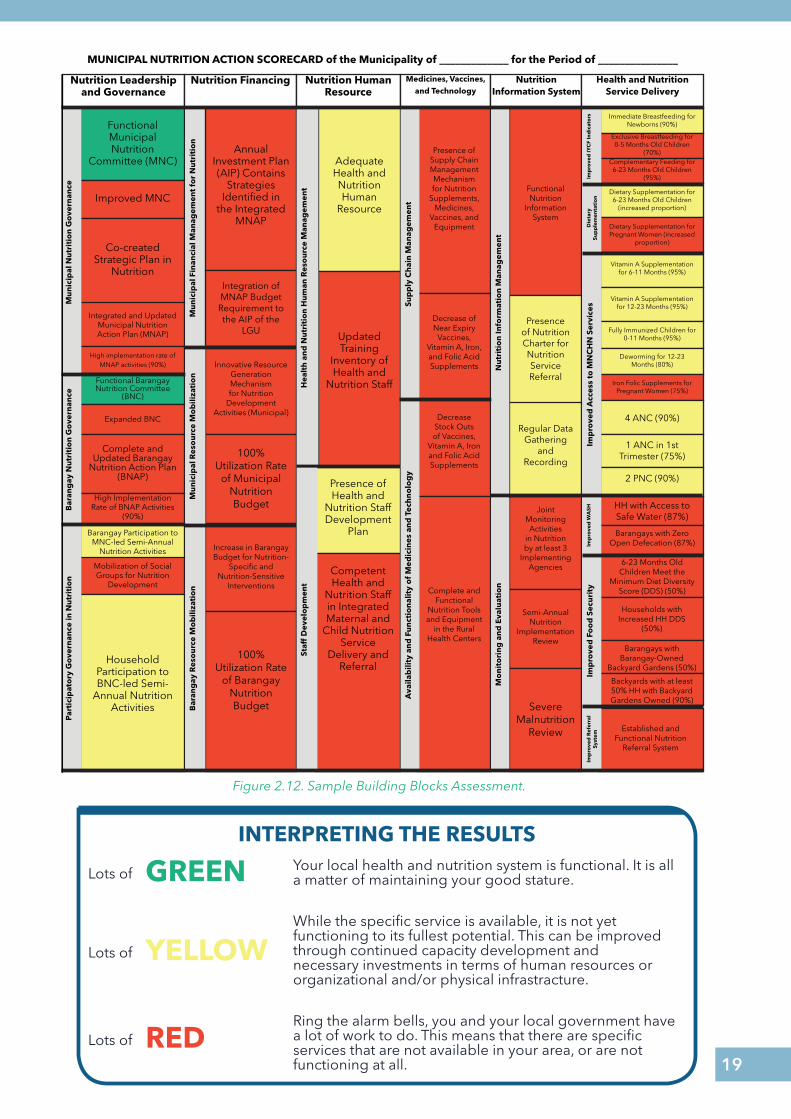
In using the MNAS, compare the actual accomplishments of your city/municipality against the performance indicators stated in the boxes. The overall performance/score will be based on the prevalent colors emerging in your MNAS, as exemplified in Figure 2.12.
Given the results of your nutrition systems assessment, ZFF provided an implementation timeline for each indicator to help your LGU establish the six building blocks and achieve the expected outputs in three years (see Figure 1.3).
19
INTERPRETING THE RESULTSYour local health and nutrition system is functional. It is all a matter of maintaining your good stature.
While the specific service is available, it is not yet functioning to its fullest potential. This can be improved through continued capacity development and necessary investments in terms of human resources or organizational and/or physical infrastracture.
Ring the alarm bells, you and your local government have a lot of work to do. This means that there are specific services that are not available in your area, or are not functioning at all.
GREENLots of
YELLOWLots of
REDLots of
MUNICIPAL NUTRITION ACTION SCORECARD of the Municipality of _____________ for the Period of _______________
Nutrition Leadership and Governance
Nutrition Financing Nutrition Human Resource
Medicines, Vaccines, and Technology
Nutrition Information System
Health and Nutrition Service Delivery
Functional Municipal Nutrition
Committee (MNC)
Improved MNC
Co-created Strategic Plan in
Nutrition
Integrated and Updated Municipal Nutrition Action Plan (MNAP)
High implementation rate of MNAP activities (90%)
Functional Barangay Nutrition Committee
(BNC)
Expanded BNC
Complete and Updated Barangay
Nutrition Action Plan (BNAP)
High Implementation Rate of BNAP Activities
(90%)
Barangay Participation to MNC-led Semi-Annual
Nutrition Activities
Mobilization of Social Groups for Nutrition
Development
Household Participation to BNC-led Semi-
Annual Nutrition Activities
Mu
nic
ipal
Nu
trit
ion
Go
vern
ance
Bar
ang
ay N
utr
itio
n G
ove
rnan
cePa
rtic
ipat
ory
Go
vern
ance
in N
utr
itio
n
Mu
nic
ipal
Fin
anci
al M
anag
emen
t fo
r N
utr
itio
n
Annual Investment Plan (AIP) Contains
Strategies Identified in
the Integrated MNAP
Integration of MNAP Budget
Requirement to the AIP of the
LGU
Innovative Resource Generation Mechanism for Nutrition
Development Activities (Municipal)
100% Utilization Rate
of Municipal Nutrition Budget
Increase in Barangay Budget for Nutrition-
Specific and Nutrition-Sensitive
Interventions
100% Utilization Rate
of Barangay Nutrition Budget
Mu
nic
ipal
Res
ou
rce
Mo
bili
zati
on
Bar
ang
ay R
eso
urc
e M
ob
iliza
tio
n
Adequate Health and Nutrition Human
Resource
Updated Training
Inventory of Health and
Nutrition Staff
Presence of Health and
Nutrition Staff Development
Plan
Hea
lth
an
d N
utr
itio
n H
um
an R
eso
urc
e M
anag
emen
t
Competent Health and
Nutrition Staff in Integrated Maternal and
Child Nutrition Service
Delivery and Referral
Staf
f D
evel
op
men
t
Presence of Supply Chain Management Mechanism for Nutrition
Supplements, Medicines,
Vaccines, and Equipment
Decrease of Near Expiry
Vaccines, Vitamin A, Iron, and Folic Acid Supplements
Decrease Stock Outs of Vaccines,
Vitamin A, Iron and Folic Acid Supplements
Complete and Functional
Nutrition Tools and Equipment
in the Rural Health Centers
Sup
ply
Ch
ain
Man
agem
ent
Ava
ilab
ility
an
d F
un
ctio
nal
ity
of
Med
icin
es a
nd
Tec
hn
olo
gy
Functional Nutrition
Information System
Presence of Nutrition Charter for Nutrition Service Referral
Regular Data Gathering
and Recording
Joint Monitoring Activities
in Nutrition by at least 3
Implementing Agencies
Semi-Annual Nutrition
Implementation Review
Severe Malnutrition
Review
Nu
trit
ion
Info
rmat
ion
Man
agem
ent
Mo
nit
ori
ng
an
d E
valu
atio
n
Immediate Breastfeeding for Newborns (90%)
Exclusive Breastfeeding for 0-5 Months Old Children
(70%)Complementary Feeding for
6-23 Months Old Children (95%)
Dietary Supplementation for 6-23 Months Old Children
(increased proportion)
Dietary Supplementation for Pregnant Women (increased
proportion)
Vitamin A Supplementation for 6-11 Months (95%)
Vitamin A Supplementation for 12-23 Months (95%)
Fully Immunized Children for 0-11 Months (95%)
Deworming for 12-23 Months (80%)
Iron Folic Supplements for Pregnant Women (75%)
4 ANC (90%)
1 ANC in 1st Trimester (75%)
2 PNC (90%)
HH with Access to Safe Water (87%)
Barangays with Zero Open Defecation (87%)
6-23 Months Old Children Meet the
Minimum Diet Diversity Score (DDS) (50%)
Households with Increased HH DDS
(50%)
Barangays with Barangay-Owned
Backyard Gardens (50%)
Backyards with at least 50% HH with Backyard Gardens Owned (90%)
Established and Functional Nutrition
Referral System
Imp
rove
d IY
CF
Ind
icat
ors
Die
tary
Su
pp
lem
enta
tio
nIm
pro
ved
Acc
ess
to M
NC
HN
Ser
vice
sIm
pro
ved
WA
SHIm
pro
ved
Fo
od
Sec
uri
tyIm
pro
ved
Ref
erra
l Sy
stem
Figure 2.12. Sample Building Blocks Assessment.
20
Benefits of Investing in Nutrition as a Development Priority
While we have extensively discussed the importance of investing in nutrition, one question still remains: What does it mean for you and your community?
We can help children like Mayumi become healthy and well-nourished. If we focus our efforts in proper governance, appropriate programs, and dedication of the leaders and his team, Mayumi will be saved from the intergenerational cycle of malnutrition. In the future, she can contribute more and become a progressive citizen.
Having a well-nourished citizenry means that a community, town, city, and/or an entire nation has a healthy human capital, who can then contribute to the development of your community. Thus, the nutritional state of your constituents is a reflection of your leadership.
Most of all, investing in nutrition entails you to become a bridging leader, helping your stakeholders and constituents reach your
With good governance comes better delivery of health and nutrition
services which leads to poverty reduction and genuine development.
(National Nutrition Council, 2010)
THE ECONOMIC BENEFITS OF INVESTING IN NUTRITION
If you invest Php 52 in nutrition programs and interventions, you could save Php 626 of forgone earnings and/or health expenditures due to undernutrition.
(UNICEF, 2015)
REMEMBER
Malnutrition remains prevalent in the Philippines, you as the head of your local government unit have the ability and influence to improve the health and nutrition status of your people.
preferred reality - having a well-nourished community.
Are you ready to take on your constituency’s nutrition journey? Let’s keep the ride going towards improved nutrition health and nutrition systems for the mothers and children of your community, and of the country!
21
The Building Blocks of Local Nurition Systems
2
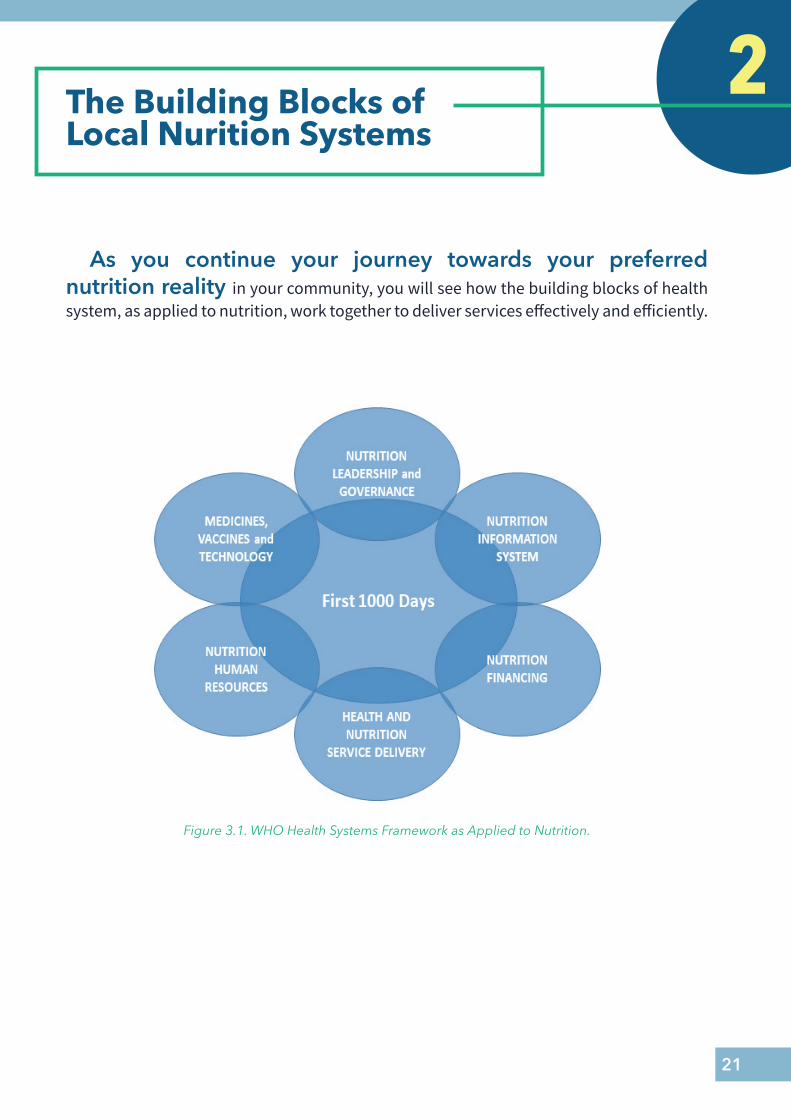
As you continue your journey towards your preferred nutrition reality in your community, you will see how the building blocks of health system, as applied to nutrition, work together to deliver services effectively and efficiently.
Figure 3.1. WHO Health Systems Framework as Applied to Nutrition.
22
Strong Nutrition Leadership and Governance
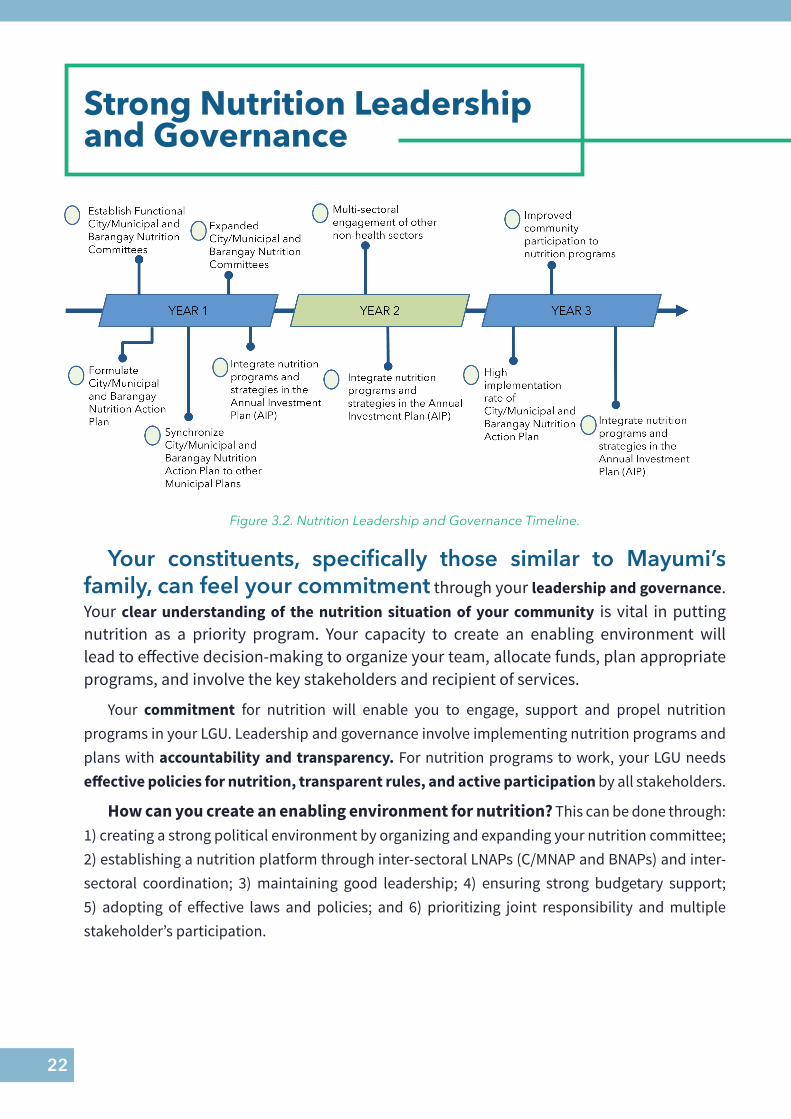
Your constituents, specifically those similar to Mayumi’s family, can feel your commitment through your leadership and governance. Your clear understanding of the nutrition situation of your community is vital in putting nutrition as a priority program. Your capacity to create an enabling environment will lead to effective decision-making to organize your team, allocate funds, plan appropriate programs, and involve the key stakeholders and recipient of services.
Your commitment for nutrition will enable you to engage, support and propel nutrition programs in your LGU. Leadership and governance involve implementing nutrition programs and plans with accountability and transparency. For nutrition programs to work, your LGU needs effective policies for nutrition, transparent rules, and active participation by all stakeholders.
How can you create an enabling environment for nutrition? This can be done through: 1) creating a strong political environment by organizing and expanding your nutrition committee; 2) establishing a nutrition platform through inter-sectoral LNAPs (C/MNAP and BNAPs) and inter-sectoral coordination; 3) maintaining good leadership; 4) ensuring strong budgetary support; 5) adopting of effective laws and policies; and 6) prioritizing joint responsibility and multiple stakeholder’s participation.
Figure 3.2. Nutrition Leadership and Governance Timeline.
23
1. Organize Functional and Expanded Local Nutrition Committee (City/Municipal Nutrition Committee and Barangay Nutrition Committees)
A functional Local Nutrition Committee (LNC) will be the major nutrition body of your LGU. As mandated by the DILG Memorandum Circular 2018-42 1.4, all LGUs should organize, reorganize and
HERE’S HOW THEY DID IT
In Looc, Romblon and Gamay, Northern Samar, the expanded MNC promoted the strong linkage between MNC and BNCs, wherein the Barangay Captain sit down in the MNC meetings. This reinforces good nutrition governance of the mayor and respective barangays.
Dr. Timoteo Capoquian, Jr. and Mayor Leila Arboleda
(Public Narratives)
strengthen functional local nutritional committees with the mayor as chairperson through the enactment of a local ordinance that entails continuity.
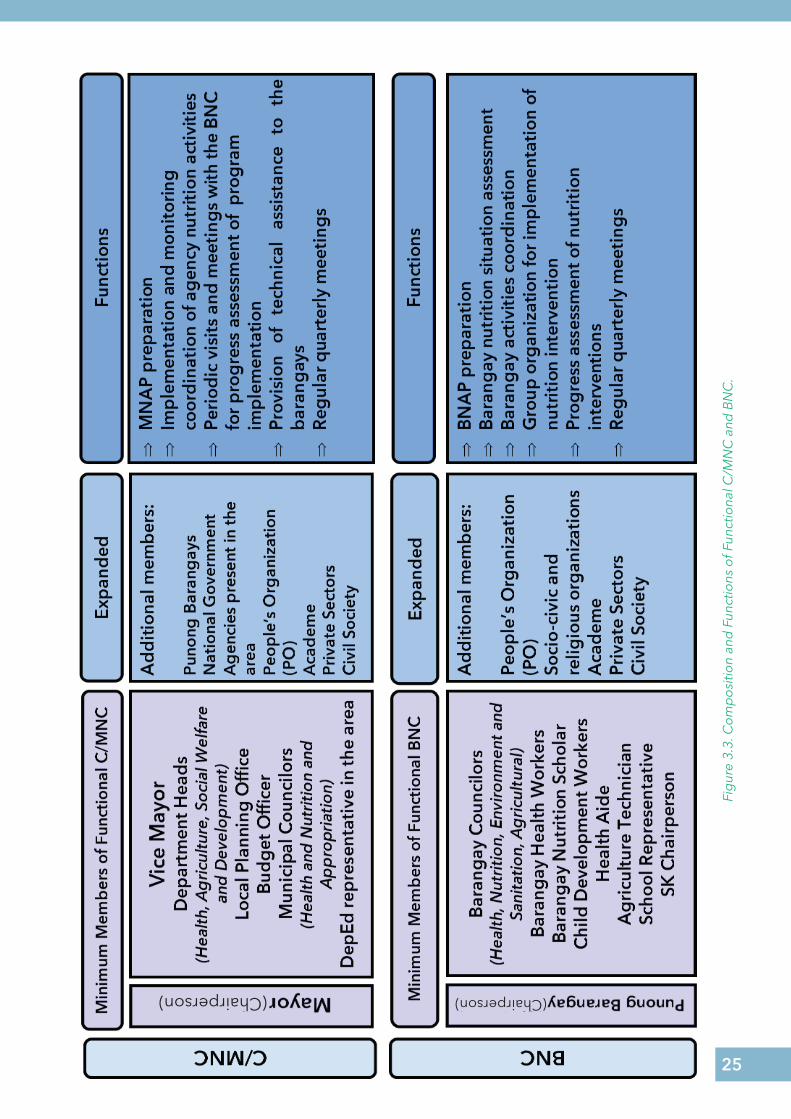
Through the LNC, you will harmonize the efforts from the various line agencies of the local government and other key stakeholders. Expanding the LNC membership at the city/municipal and at the barangay level will increase inter-sectoral participation and engagement of key stakeholders in addressing problems on health and nutrition (Figure 3.1).
All department heads and other municipal officials should also have commitment and are willing to work together to achieve the goals for nutrition improvement. You may lead them by involving them in setting of strategic directions, effective administration and management, policy making, planning, decision-making process, implementing programs and projects, and other partnerships.
HERE’S HOW THEY DID IT
Calamba City mobilized the city nutrition committee, barangay nutrition committees and the barangay nutrition scholars as the key partners for effective nutrition program management and implementation. There is a strong policy support for evidence-based nutrition actions by the issuance of an executive order creating the committee, the presence of an approved City/Local Nutrition Action Plan (C/LNAP), the BNAP and the implementation of the LNAP activities by the member-agencies that help the LGU implement their nutrition projects more effectively. In its barangays, cooperation and involvement of the community, especially the parents or mothers helps in better delivery of health and nutrition services.
(Laguna LGUs Best Practices and Strategies for Nutrition, NNC 2017)
24
2. Establish Nutrition Platform Through Integrated and Inter-Sectoral City/Municipal and Barangay Action Plans
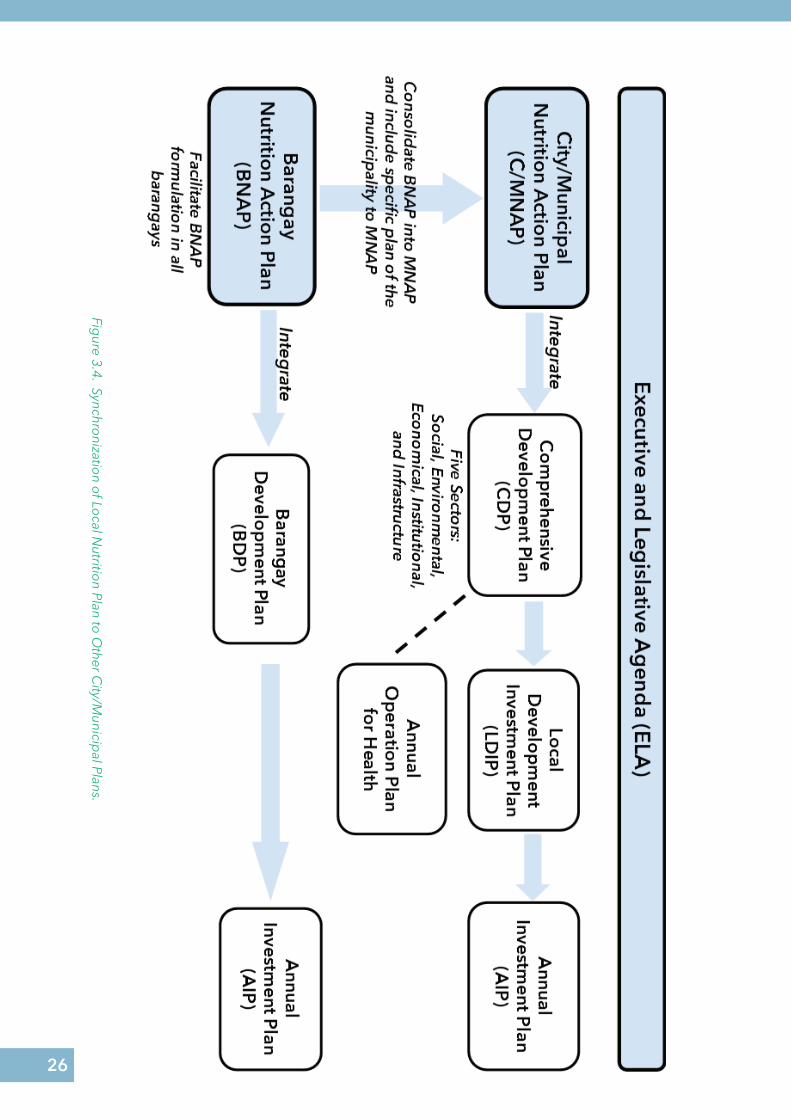
Lay down your nutrition platform through the formulation of integrated and inter-sectoral C/MNAP. Translate the nutrition thought of your Executive and Legislative Agenda (ELA) and integrate the nutrition needs of your barangays by formulating a C/MNAP. The C/MNAP focuses on the achievement of nutrition program objectives in a coordinated and consistent manner (Figure 3.4).
You need to synchronize the C/MNAP to other inter-sectoral plans and formulate an integrated city/municipal plan, such as the Comprehensive Development Plan. This will ensure that your Local Investment Plan (LIP) and Annual Investment Plan (AIP) are sensitive in addressing malnutrition problem in your city/ or municipality.
The harmonization of your plans, in accordance to Local Budget Memorandum 77-A, 2018 and pursuant to Section 305 (h) of the LGC, will optimize the utilization of resources and will avoid duplication in the use of fiscal and physical resources (Figure 3.4).
In accordance to the Local Government Code (LGC), you can promote the participation of non-government or private sector, civil society, and people’s organizations in local governance. Through the creation of local special bodies and other private-public partnership mechanisms, you can make full use of your corporate powers in improving the delivery of basic services such as health and nutrition. Adhering to these LGC provisions will help you shape and strengthen your local governance (Figure 3.3).
25
Fig
ure
3.3.
Co
mp
osi
tion
and
Fun
ctio
ns o
f Fun
ctio
nal C
/MN
C a
nd B
NC
.
(Chairperson) (Chairperson)
26
Figure 3.4. Synchro
nization o
f Local N
utrition Plan to
Other C
ity/Municip
al Plans.
27
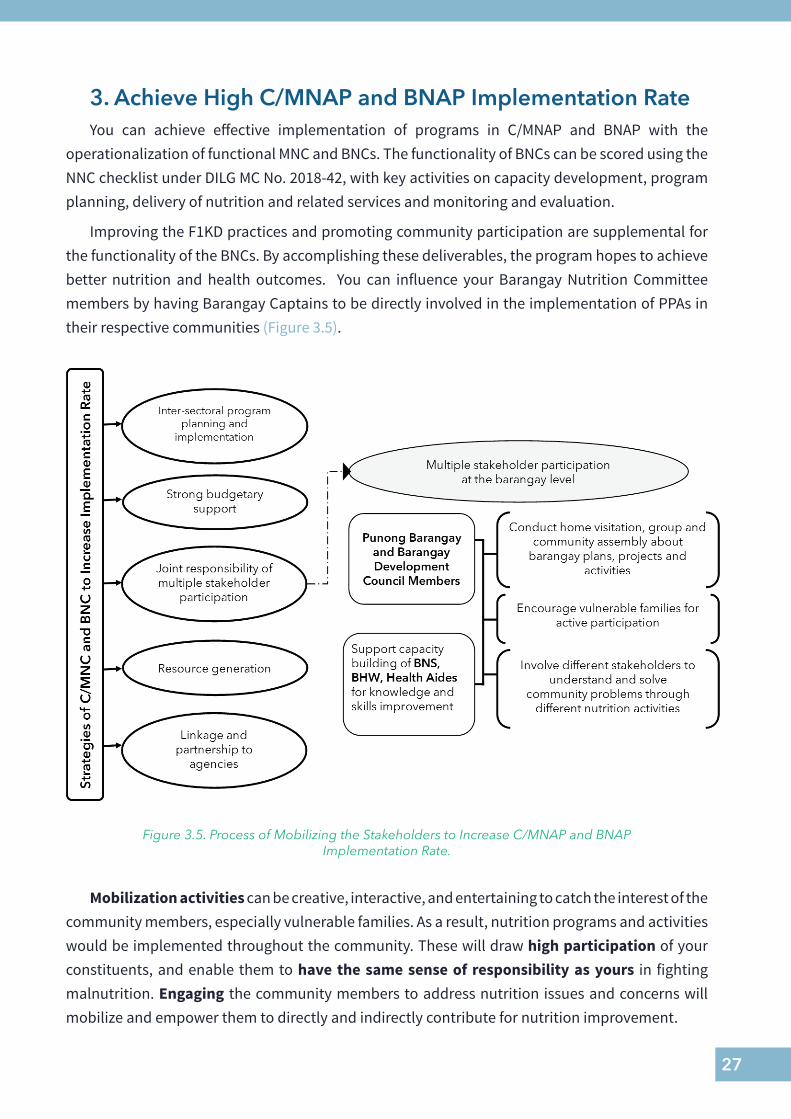
3. Achieve High C/MNAP and BNAP Implementation Rate You can achieve effective implementation of programs in C/MNAP and BNAP with the
operationalization of functional MNC and BNCs. The functionality of BNCs can be scored using the NNC checklist under DILG MC No. 2018-42, with key activities on capacity development, program planning, delivery of nutrition and related services and monitoring and evaluation.
Improving the F1KD practices and promoting community participation are supplemental for the functionality of the BNCs. By accomplishing these deliverables, the program hopes to achieve better nutrition and health outcomes. You can influence your Barangay Nutrition Committee members by having Barangay Captains to be directly involved in the implementation of PPAs in their respective communities (Figure 3.5).
Figure 3.5. Process of Mobilizing the Stakeholders to Increase C/MNAP and BNAP Implementation Rate.
Mobilization activities can be creative, interactive, and entertaining to catch the interest of the community members, especially vulnerable families. As a result, nutrition programs and activities would be implemented throughout the community. These will draw high participation of your constituents, and enable them to have the same sense of responsibility as yours in fighting malnutrition. Engaging the community members to address nutrition issues and concerns will mobilize and empower them to directly and indirectly contribute for nutrition improvement.
28
HERE’S HOW THEY DID IT
In Gamay, Northern Samar, the Mayor initiated an increase in budget for nutrition programs and its inclusion in the Annual Investment Plan (AIP) to ensure that the program is sufficiently funded for implementation. The barangays were capacitated on budgeting and prioritized allocation for health and nutrition programs. Continuous capacity-building for the BNS and RHU personnel were done to ensure that nutrition programs are integrated in the health service delivery system.
Mothers and caregivers were also empowered on proper nutrition and care for their young children through the conduct of nutrition education programs and Pabasa sa Nutrition. The LGU utilized linkages and partnerships with different organizations to implement a community-based supplementary feeding program for all pregnant and lactating mothers, children from 6-24 months, senior citizens, and persons with disability, vitamins, micronutrient powders and other micronutrient supplementation for moderate acute malnutrition (MAM) and severe acute malnutrition (SAM) patients.
Different nutrition-sensitive interventions were done simultaneously at the LGU to address their malnutrition problem, such as improving food security in each household by improving their existing agriculture programs and the allocation of Php 1 million annual budget for agriculture.
The LGUs likewise engaged the different fisher-folks, farmers, and POs in different barangays, conducted various capacity-building activities to educate them on new farming techniques and technology and provided them farm implements and necessary equipment that would help in applying the new farming methods. They also implemented integrated service delivery especially to SAM patients with the use of effective communication within the between departments. Different policies have been in place to help institutionalize all their efforts and strategies and to provide support in the implementation of nutrition program throughout the municipality.
Dr. Timoteo Capoquian, Jr. (Public Narrative)
You can learn from the experience of Gamay Mayor Dr. Timoteo Capoquian, Jr. the importance of strong leadership; promoting inter-sectoral program implementation and cooperation; strong budgetary support to nutrition programs; linkages and partnership to agencies; and joint responsibility and multiple stakeholders’ participation, especially at the barangay level.
29
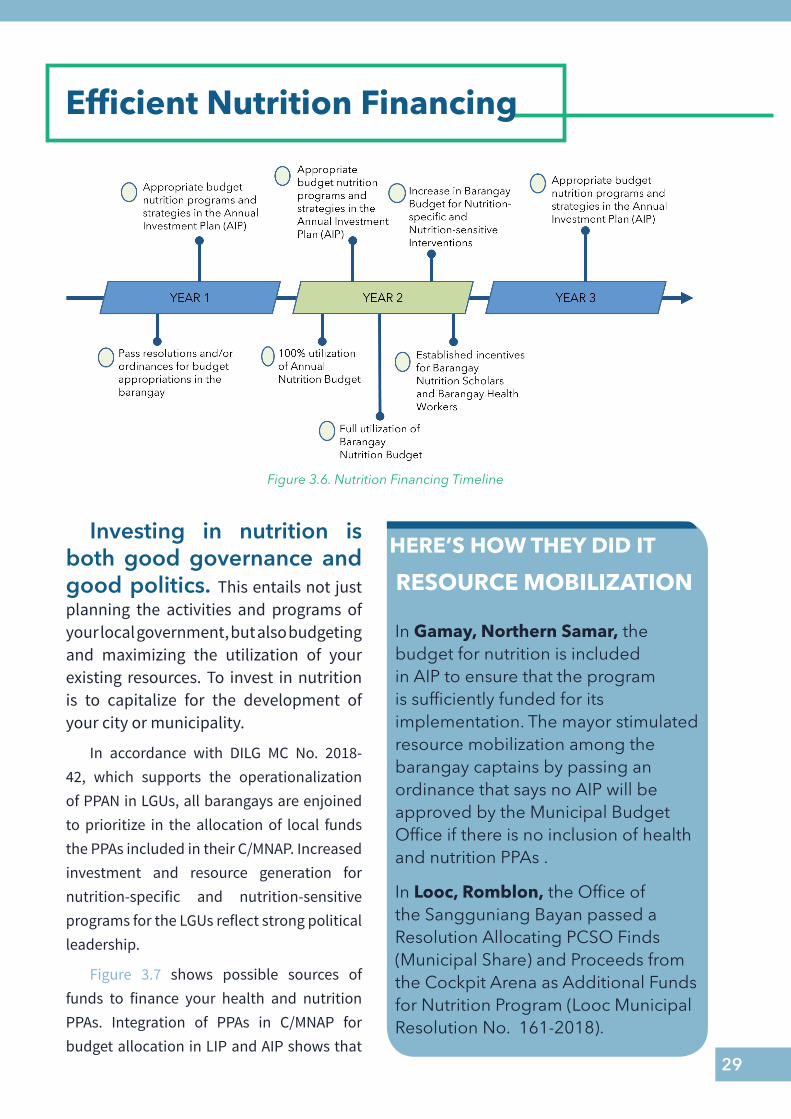
Efficient Nutrition Financing
Investing in nutrition is both good governance and good politics. This entails not just planning the activities and programs of your local government, but also budgeting and maximizing the utilization of your existing resources. To invest in nutrition is to capitalize for the development of your city or municipality.
In accordance with DILG MC No. 2018-42, which supports the operationalization of PPAN in LGUs, all barangays are enjoined to prioritize in the allocation of local funds the PPAs included in their C/MNAP. Increased investment and resource generation for nutrition-specific and nutrition-sensitive programs for the LGUs reflect strong political leadership.
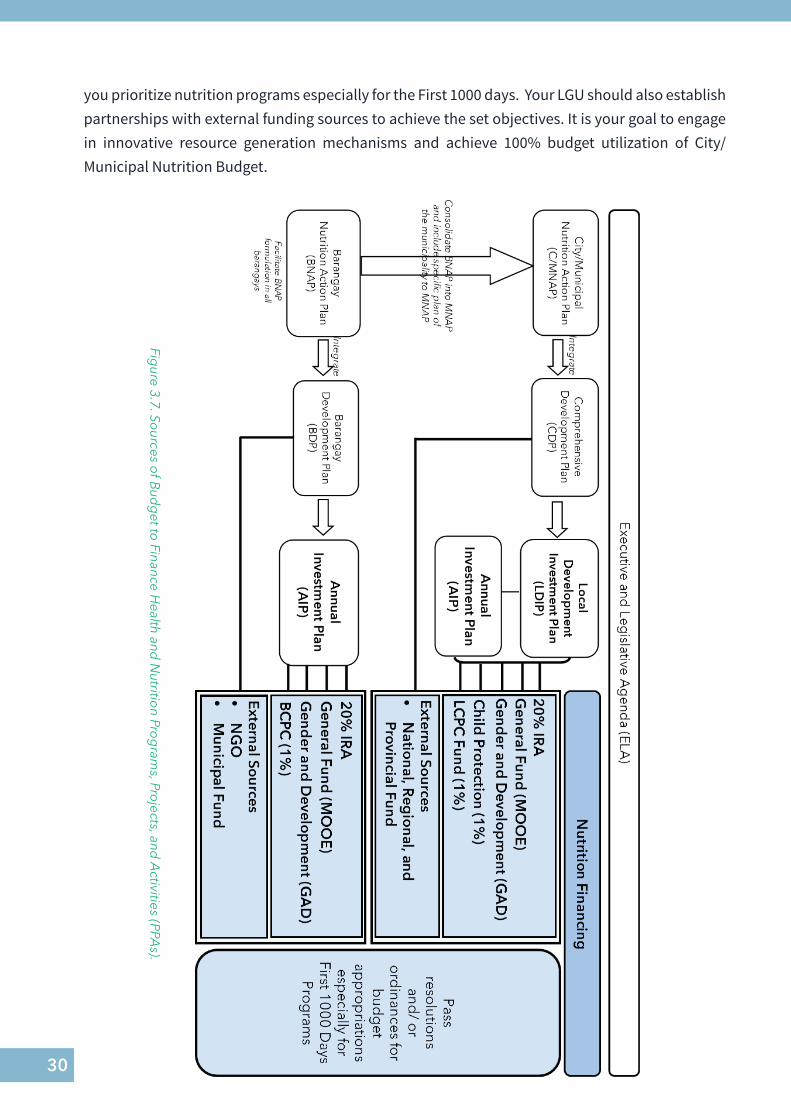
Figure 3.7 shows possible sources of funds to finance your health and nutrition PPAs. Integration of PPAs in C/MNAP for budget allocation in LIP and AIP shows that
Figure 3.6. Nutrition Financing Timeline
HERE’S HOW THEY DID IT
In Gamay, Northern Samar, the budget for nutrition is included in AIP to ensure that the program is sufficiently funded for its implementation. The mayor stimulated resource mobilization among the barangay captains by passing an ordinance that says no AIP will be approved by the Municipal Budget Office if there is no inclusion of health and nutrition PPAs .
In Looc, Romblon, the Office of the Sangguniang Bayan passed a Resolution Allocating PCSO Finds (Municipal Share) and Proceeds from the Cockpit Arena as Additional Funds for Nutrition Program (Looc Municipal Resolution No. 161-2018).
RESOURCE MOBILIZATION
30
Figure 3.7. So
urces of B
udg
et to Finance H
ealth and N
utrition Pro
gram
s, Projects, and
Activities (PPA
s).
you prioritize nutrition programs especially for the First 1000 days. Your LGU should also establish partnerships with external funding sources to achieve the set objectives. It is your goal to engage in innovative resource generation mechanisms and achieve 100% budget utilization of City/Municipal Nutrition Budget.
31
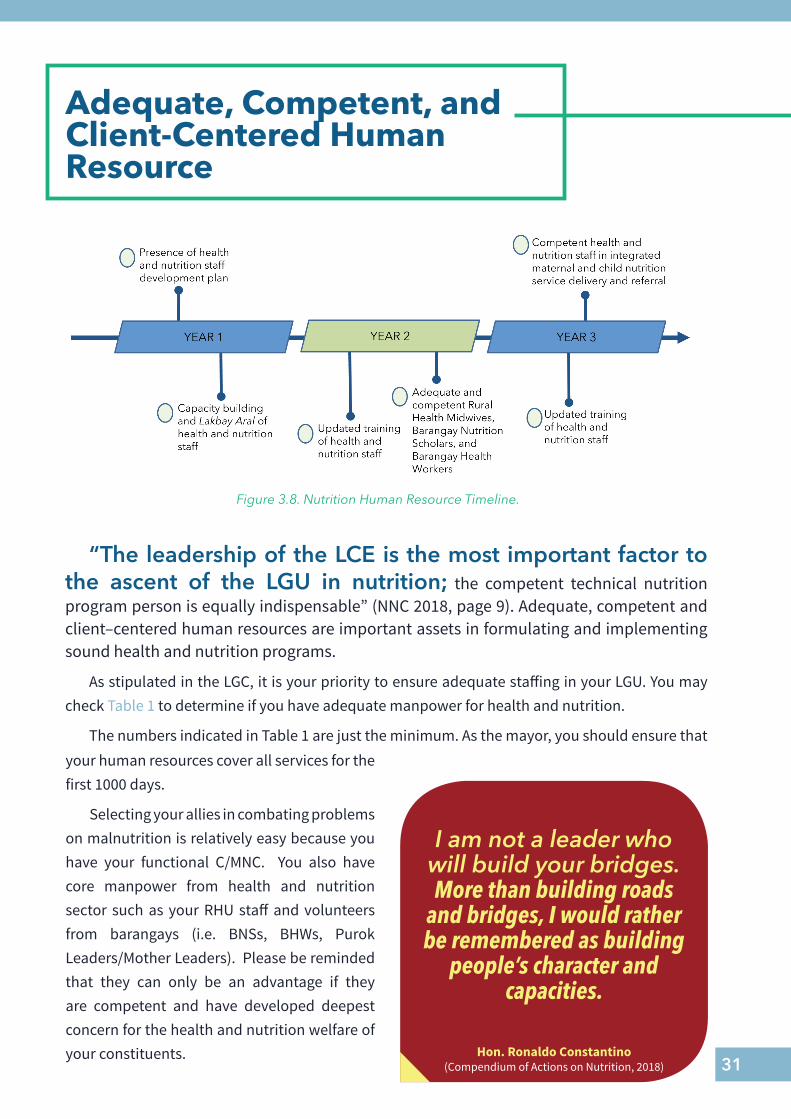
Adequate, Competent, and Client-Centered Human Resource
“The leadership of the LCE is the most important factor to the ascent of the LGU in nutrition; the competent technical nutrition program person is equally indispensable” (NNC 2018, page 9). Adequate, competent and client–centered human resources are important assets in formulating and implementing sound health and nutrition programs.
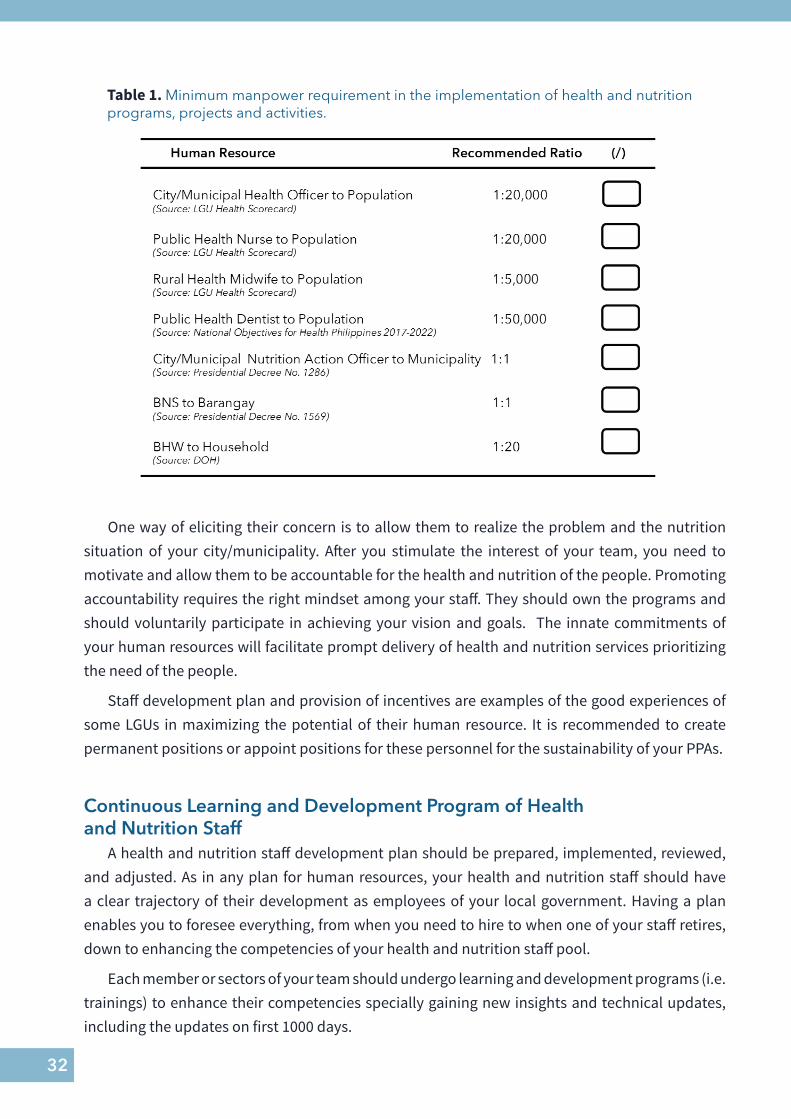
As stipulated in the LGC, it is your priority to ensure adequate staffing in your LGU. You may check Table 1 to determine if you have adequate manpower for health and nutrition.
The numbers indicated in Table 1 are just the minimum. As the mayor, you should ensure that
I am not a leader who will build your bridges. More than building roads
and bridges, I would rather be remembered as building
people’s character and capacities.
Hon. Ronaldo Constantino(Compendium of Actions on Nutrition, 2018)
your human resources cover all services for the first 1000 days.
Selecting your allies in combating problems on malnutrition is relatively easy because you have your functional C/MNC. You also have core manpower from health and nutrition sector such as your RHU staff and volunteers from barangays (i.e. BNSs, BHWs, Purok Leaders/Mother Leaders). Please be reminded that they can only be an advantage if they are competent and have developed deepest concern for the health and nutrition welfare of your constituents.
Figure 3.8. Nutrition Human Resource Timeline.
32
Table 1. Minimum manpower requirement in the implementation of health and nutrition programs, projects and activities.
One way of eliciting their concern is to allow them to realize the problem and the nutrition situation of your city/municipality. After you stimulate the interest of your team, you need to motivate and allow them to be accountable for the health and nutrition of the people. Promoting accountability requires the right mindset among your staff. They should own the programs and should voluntarily participate in achieving your vision and goals. The innate commitments of your human resources will facilitate prompt delivery of health and nutrition services prioritizing the need of the people.
Staff development plan and provision of incentives are examples of the good experiences of some LGUs in maximizing the potential of their human resource. It is recommended to create permanent positions or appoint positions for these personnel for the sustainability of your PPAs.
Continuous Learning and Development Program of Healthand Nutrition Staff
A health and nutrition staff development plan should be prepared, implemented, reviewed, and adjusted. As in any plan for human resources, your health and nutrition staff should have a clear trajectory of their development as employees of your local government. Having a plan enables you to foresee everything, from when you need to hire to when one of your staff retires, down to enhancing the competencies of your health and nutrition staff pool.
Each member or sectors of your team should undergo learning and development programs (i.e. trainings) to enhance their competencies specially gaining new insights and technical updates, including the updates on first 1000 days.
33
Capacity development of your health and nutrition staff is very significant to promote holistic management of the health and nutrition programs. Also, you may check Appendix B to know the key trainings required for effective and efficient delivery of services. Attendance to these training requires support from the LGU.
Allow your team to observe the good practices of other LGUs. Lakbay Aral or visiting other performer LGUs in nutrition will serve as eye opener to your team. Attending conferences and workshops are also found beneficial to have wider perspectives in nutrition program management.
You can also solicit more support through close linkage to regional and provincial nutrition and health coordinators. They are mandated to mentor and coach your team for better implementation of health and nutrition programs.
REMEMBERAssembling a team and supporting them by providing incentives will
greatly contribute to the success of the program implementation for First 1000 Days.
AVAILABLE TRAINING PROGRAMSIn managing your nutrition programs, you can take advantage of the available training programs offered by the Zuellig Family Foundation. ZFF has trainings on Bridging Leadership for local chief executives, Barangay Leadership for Nutrition and Development (BL4ND), and Local Integrated Nutrition Information System (LINIS), and the Nexus Training for nutrition program implementors.
The National Nutrition Council (NNC) with the University of the Philippines Los Baños (UPLB) also formulated a training on Nutrition Program Management. The NPM training guides the implementers, specially the MNC members, on how they can have right perspective of the problem and how they can contribute to address malnutrition problems.
Incentive for Health WorkersMany LGUs found that providing incentive through appropriations of budget for honorarium of
health and nutrition workers contribute to their motivation which in return affect the sustainability of programs. There are fewer turnovers of staff to implement the programs, especially at the village or barangay level. As front liners in delivering services it is best to retain the hard-working and highly-committed BNS volunteers and investing will not be futile.
34
HERE’S HOW THEY DID IT
In the Philippines, the delivery and utilization of health and nutrition services are affected by lack of trained providers in the health and nutrition systems. The success of health and nutrition programs implementation largely depends upon the capacity of the health and nutrition workers to deliver a quality health and nutrition intervention. Barangay health and nutrition workers, with adequate capacity-building, can effectively deliver health and nutrition services in the community.
The local health and nutrition workers need continuing education, study and exposure tours, training, grants, field immersion, and scholarships as stipulated in the Republic Act No. 7883, an act granting benefits and incentives to accredit barangay health workers and for other purposes. Building the capacity of the local health and nutrition workers needs continuous training of the frontline workers. In Cebu, majority of the C/MLGUs has trained their MNC members and health and nutrition workers for nutrition program management. In Cebu and Bohol, BLGUs provide a counterpart to the monthly honorarium of this BNS
(LGUs Best Practices for Nutrition, NNC 2017)
INCENTIVE TO MOTIVATE THE TEAM MEMBERS
35
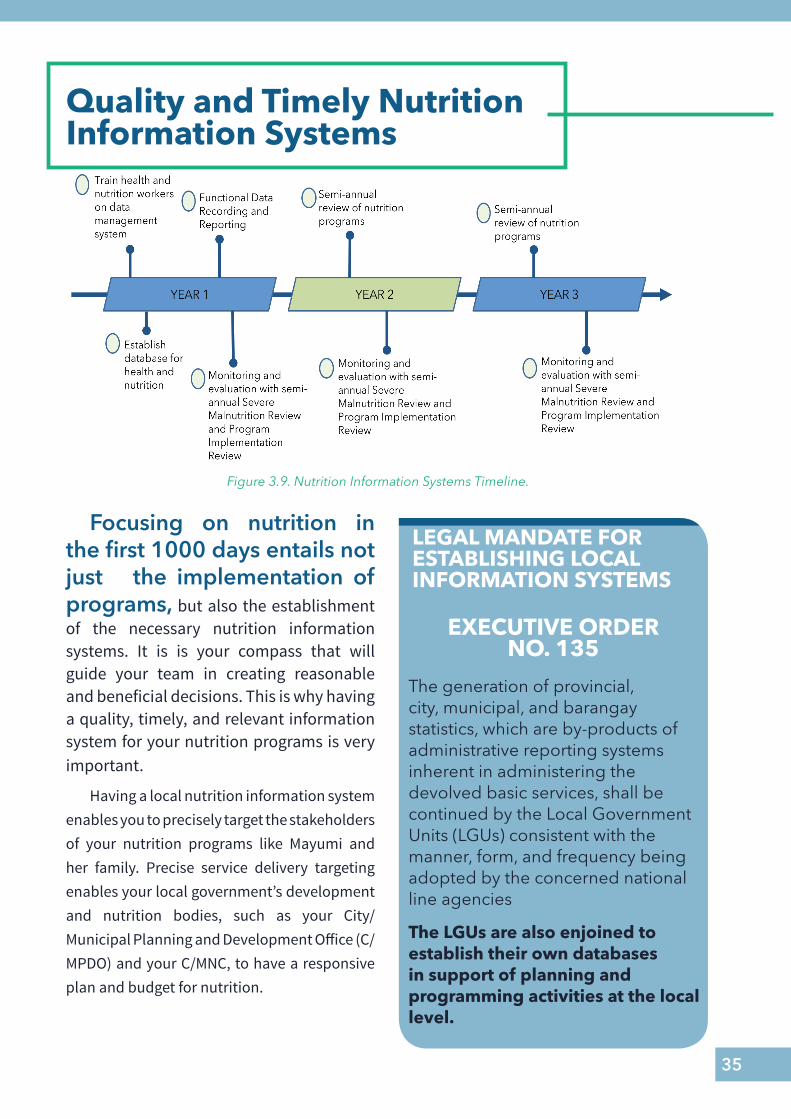
Quality and Timely Nutrition Information Systems
Focusing on nutrition in the first 1000 days entails not just the implementation of programs, but also the establishment of the necessary nutrition information systems. It is is your compass that will guide your team in creating reasonable and beneficial decisions. This is why having a quality, timely, and relevant information system for your nutrition programs is very important.
Having a local nutrition information system enables you to precisely target the stakeholders of your nutrition programs like Mayumi and her family. Precise service delivery targeting enables your local government’s development and nutrition bodies, such as your City/Municipal Planning and Development Office (C/MPDO) and your C/MNC, to have a responsive plan and budget for nutrition.
LEGAL MANDATE FOR ESTABLISHING LOCAL INFORMATION SYSTEMS
The generation of provincial, city, municipal, and barangay statistics, which are by-products of administrative reporting systems inherent in administering the devolved basic services, shall be continued by the Local Government Units (LGUs) consistent with the manner, form, and frequency being adopted by the concerned national line agencies
The LGUs are also enjoined to establish their own databases in support of planning and programming activities at the local level.
EXECUTIVE ORDER NO. 135
Figure 3.9. Nutrition Information Systems Timeline.
36
Fig
ure
3.10
. Id
entifi
catio
n o
f Tar
get
for
Del
iver
y o
f Ser
vice
s B
ased
on
Nut
ritio
n Si
tuat
ion
Ana
lysi
s.
37
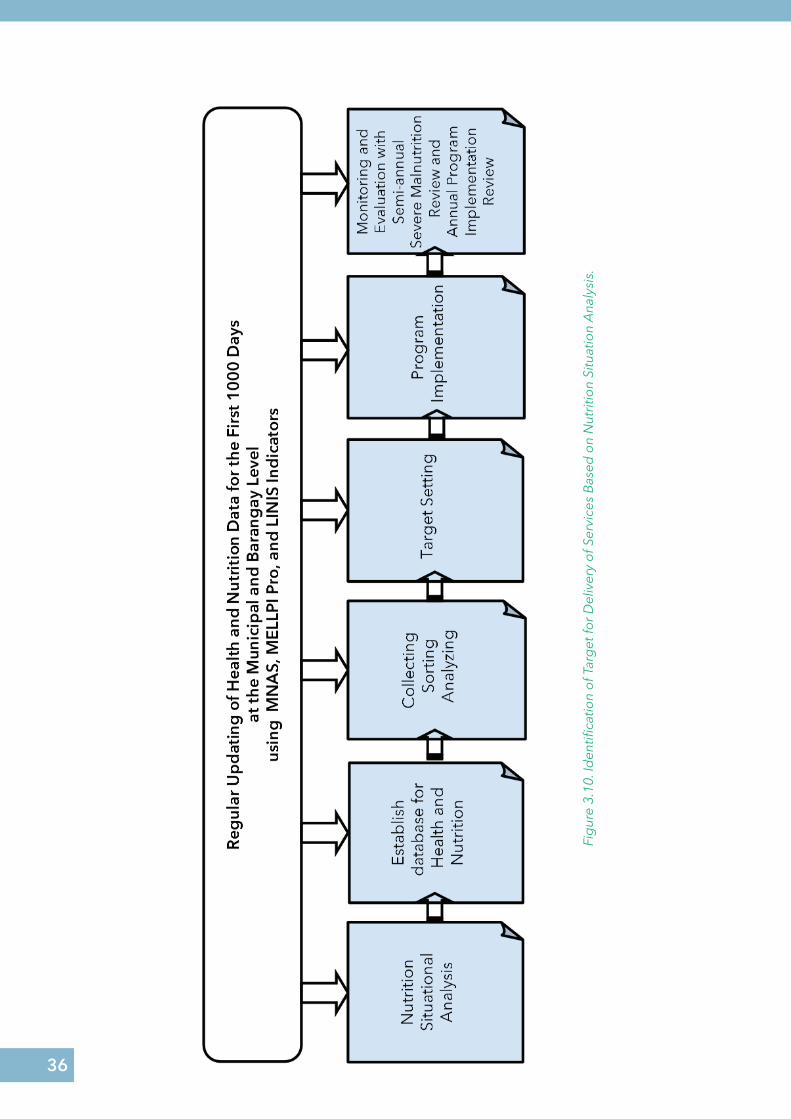
Establish a Functional Nutrition Information SystemEstablish a functional Nutrition Information System in all barangays and at the municipal/
city level. Functional nutrition information system involves regular updating of health and nutrition data through creation of database. Each barangay should keep its own database to be consolidated at the municipal level.
You may align the information that you want to collect or generate from the MNAS, MELLPI, and LINIS indicators. These may serve as basis in your nutrition situation analysis, target setting program implementation and monitoring and evaluation (Figure 3.10).
Monitoring and Evaluation of Local Level Plan Implementation Protocol (MELLPI Pro) of the NNC, and MNAS of the ZFF, are tools that can be used to assess governance, nutrition financing, and
THE ROLE OF YOUR LOCAL AND BARANGAY NUTRITION COMMITTEES IN THE SEVERE MALNUTRITION REVIEW
• Track the mothers and children two years old and below in your community
• BNS and BHW should identify the children who are suffering from any of the following:
◊ Severe underweight◊ Severe wasting◊ Severe stunting◊ Severe acute malnutrition (SAM)◊ Moderate acute malnutrition (MAM)
• Local health and nutrition workers should work together with the parents of severely malnourished children for proper treatment and/or referral. This should be inter-sectoral. Joint implementation means that aside from direct nutrition from F1KD interventions, the various social determinants of malnutrition afflicting the child can and should be addressed as well (e.g. lack of access to potable drinking water, poverty or lack of income).
• Monitoring of response
• Results of the reviews at the barangay level are to be consolidated at the municipal/city level.
• Consolidate and elevate lessons learned to provincial and regional level
38
health and nutrition service delivery of your city/municipality. You can also use the Local Nutrition Information System (LINIS) of ZFF to specifically assess the services of your local government unit for the First 1000 Days.
Monitoring and Evaluation
Tracking of your progress to meet your goals and objective in your 3-year term can be facilitated by regular monitoring and evaluation. We have to monitor the progress of the programs, and evaluate them in order to take steps in improving, if not revising, the programs that are currently being implemented. As mandated by the NNC, your LNC should assure the inclusion of monitoring and evaluation mechanisms in your LNAP.
Since your LNC is composed of multiple line agencies, you may opt to have joint monitoring activities in nutrition by assigning three heads of your line agencies to monitor your LGU’s nutrition activities. Aside from being a planning body, your LNC can also serve as a monitoring and evaluation body of your local government’s nutrition projects.
Start to monitor your programs and activities for health and nutrition using the MNAS, MELLPI Pro, and LINIS tools to have a clear grasp of your performance. The result can also influence further improve the program implementation.
The LNC should conduct regular evaluation of PPAs to assess program implementation and consider points for improvement. Evaluation activities include the Severe Malnutrition Review (SMR), which is conducted every six months; and the annual program implementation review of your accomplishment against MNAS, MELLPI, and LINIS indicators.
Monitoring and evaluation will also motivate you achieving awards in nutrition such as Green Banner Award, Consistent Regional Outstanding Winner on Nutrition, or Nutrition Honor Award.
REMEMBER
Establishment of functional nutrition system will ensure sound target setting, planning and monitoring, and evaluation of programs and projects for nutrition.
39
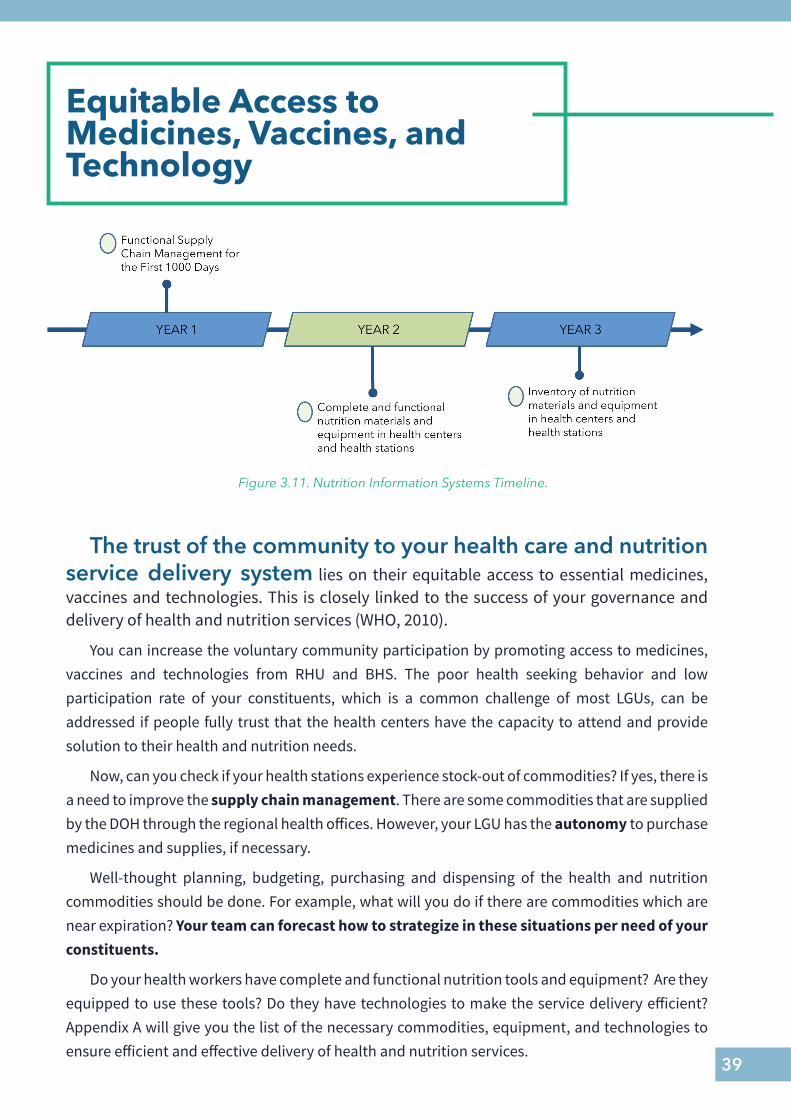
Equitable Access to Medicines, Vaccines, and Technology
The trust of the community to your health care and nutrition service delivery system lies on their equitable access to essential medicines, vaccines and technologies. This is closely linked to the success of your governance and delivery of health and nutrition services (WHO, 2010).
You can increase the voluntary community participation by promoting access to medicines, vaccines and technologies from RHU and BHS. The poor health seeking behavior and low participation rate of your constituents, which is a common challenge of most LGUs, can be addressed if people fully trust that the health centers have the capacity to attend and provide solution to their health and nutrition needs.
Now, can you check if your health stations experience stock-out of commodities? If yes, there is a need to improve the supply chain management. There are some commodities that are supplied by the DOH through the regional health offices. However, your LGU has the autonomy to purchase medicines and supplies, if necessary.
Well-thought planning, budgeting, purchasing and dispensing of the health and nutrition commodities should be done. For example, what will you do if there are commodities which are near expiration? Your team can forecast how to strategize in these situations per need of your constituents.
Do your health workers have complete and functional nutrition tools and equipment? Are they equipped to use these tools? Do they have technologies to make the service delivery efficient? Appendix A will give you the list of the necessary commodities, equipment, and technologies to ensure efficient and effective delivery of health and nutrition services.
Figure 3.11. Nutrition Information Systems Timeline.
40
REMEMBEREquitable access of the community to medicines, vaccines and
technology is closely linked to the success of your governance and delivery of health and nutrition services.
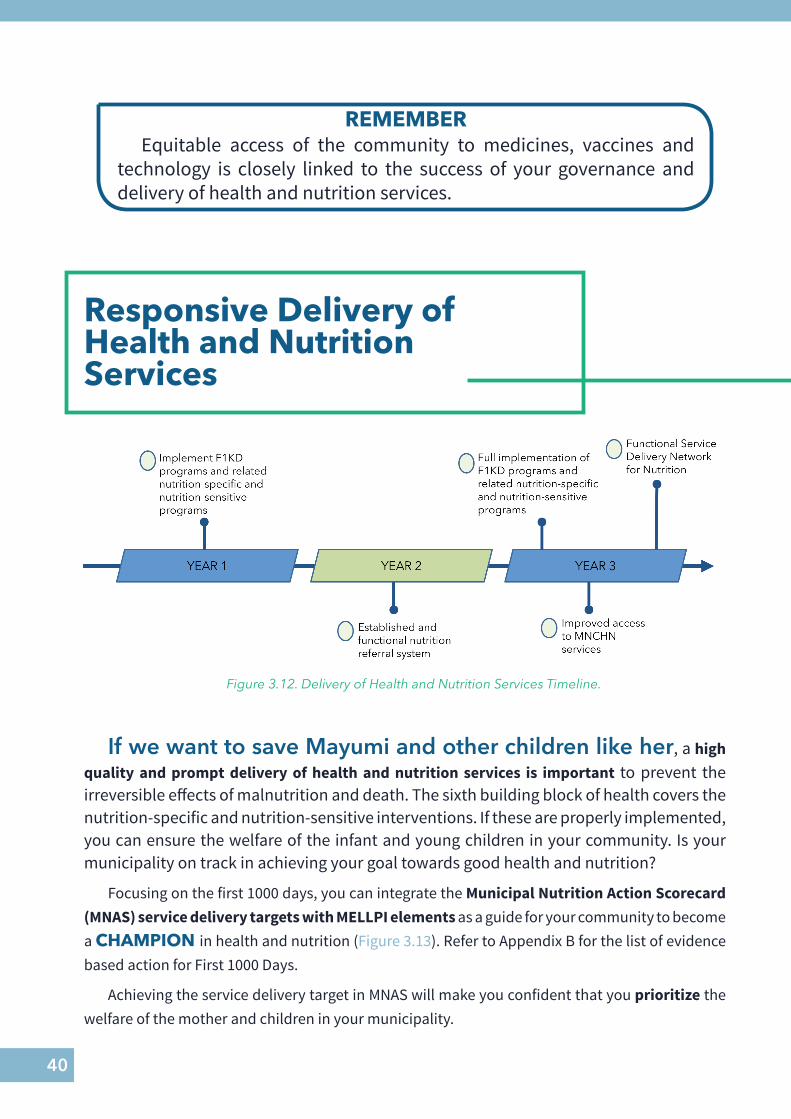
Responsive Delivery of Health and Nutrition Services
If we want to save Mayumi and other children like her, a high quality and prompt delivery of health and nutrition services is important to prevent the irreversible effects of malnutrition and death. The sixth building block of health covers the nutrition-specific and nutrition-sensitive interventions. If these are properly implemented, you can ensure the welfare of the infant and young children in your community. Is your municipality on track in achieving your goal towards good health and nutrition?
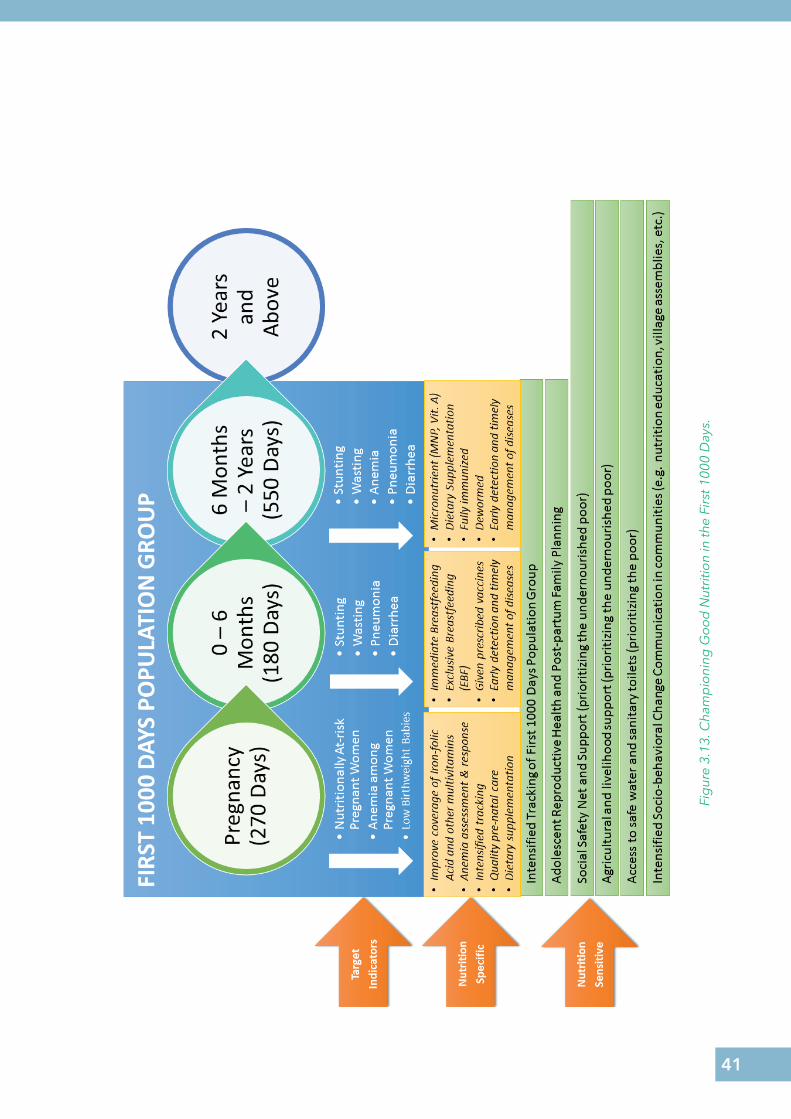
Focusing on the first 1000 days, you can integrate the Municipal Nutrition Action Scorecard (MNAS) service delivery targets with MELLPI elements as a guide for your community to become a CHAMPION in health and nutrition (Figure 3.13). Refer to Appendix B for the list of evidence based action for First 1000 Days.
Achieving the service delivery target in MNAS will make you confident that you prioritize the welfare of the mother and children in your municipality.
Figure 3.12. Delivery of Health and Nutrition Services Timeline.
41
Fig
ure
3.13
. Cha
mp
ioni
ng G
oo
d N
utri
tion
in th
e Fi
rst 1
000
Day
s.
42
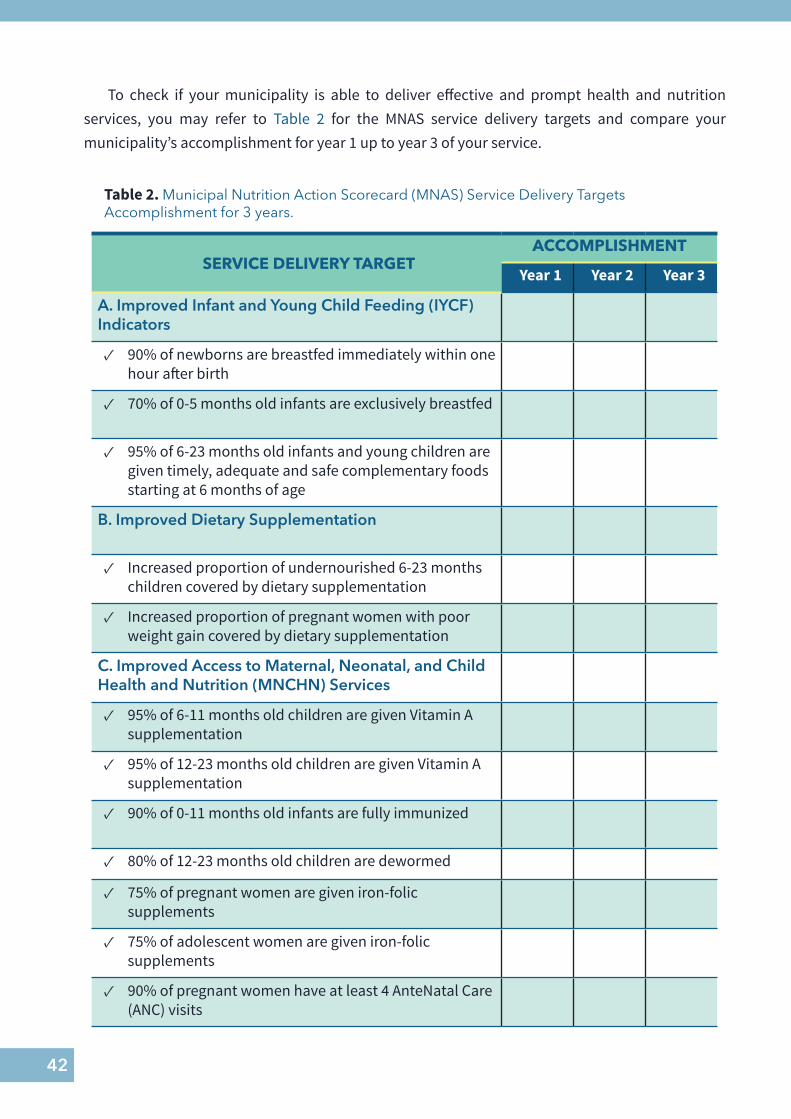
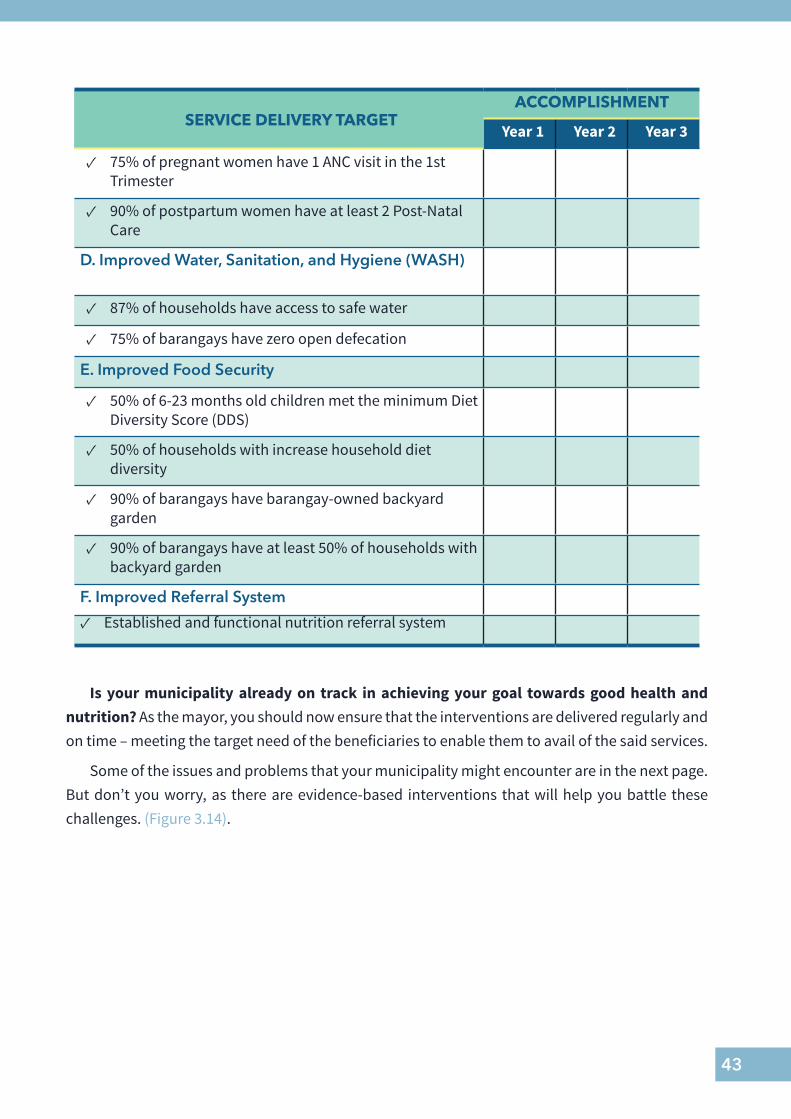
To check if your municipality is able to deliver effective and prompt health and nutrition services, you may refer to Table 2 for the MNAS service delivery targets and compare your municipality’s accomplishment for year 1 up to year 3 of your service.
Table 2. Municipal Nutrition Action Scorecard (MNAS) Service Delivery Targets Accomplishment for 3 years.
SERVICE DELIVERY TARGETACCOMPLISHMENT
Year 1 Year 2 Year 3
A. Improved Infant and Young Child Feeding (IYCF) Indicators
✓ 90% of newborns are breastfed immediately within one hour after birth
✓ 70% of 0-5 months old infants are exclusively breastfed
✓ 95% of 6-23 months old infants and young children are given timely, adequate and safe complementary foods starting at 6 months of age
B. Improved Dietary Supplementation
✓ Increased proportion of undernourished 6-23 months children covered by dietary supplementation
✓ Increased proportion of pregnant women with poor weight gain covered by dietary supplementation
C. Improved Access to Maternal, Neonatal, and Child Health and Nutrition (MNCHN) Services
✓ 95% of 6-11 months old children are given Vitamin A supplementation
✓ 95% of 12-23 months old children are given Vitamin A supplementation
✓ 90% of 0-11 months old infants are fully immunized
✓ 80% of 12-23 months old children are dewormed
✓ 75% of pregnant women are given iron-folic supplements
✓ 75% of adolescent women are given iron-folic supplements
✓ 90% of pregnant women have at least 4 AnteNatal Care (ANC) visits
43
SERVICE DELIVERY TARGETACCOMPLISHMENT
Year 1 Year 2 Year 3
✓ 75% of pregnant women have 1 ANC visit in the 1st Trimester
✓ 90% of postpartum women have at least 2 Post-Natal Care
D. Improved Water, Sanitation, and Hygiene (WASH)
✓ 87% of households have access to safe water
✓ 75% of barangays have zero open defecation
E. Improved Food Security
✓ 50% of 6-23 months old children met the minimum Diet Diversity Score (DDS)
✓ 50% of households with increase household diet diversity
✓ 90% of barangays have barangay-owned backyard garden
✓ 90% of barangays have at least 50% of households with backyard garden
F. Improved Referral System
✓ Established and functional nutrition referral system
Is your municipality already on track in achieving your goal towards good health and nutrition? As the mayor, you should now ensure that the interventions are delivered regularly and on time – meeting the target need of the beneficiaries to enable them to avail of the said services.
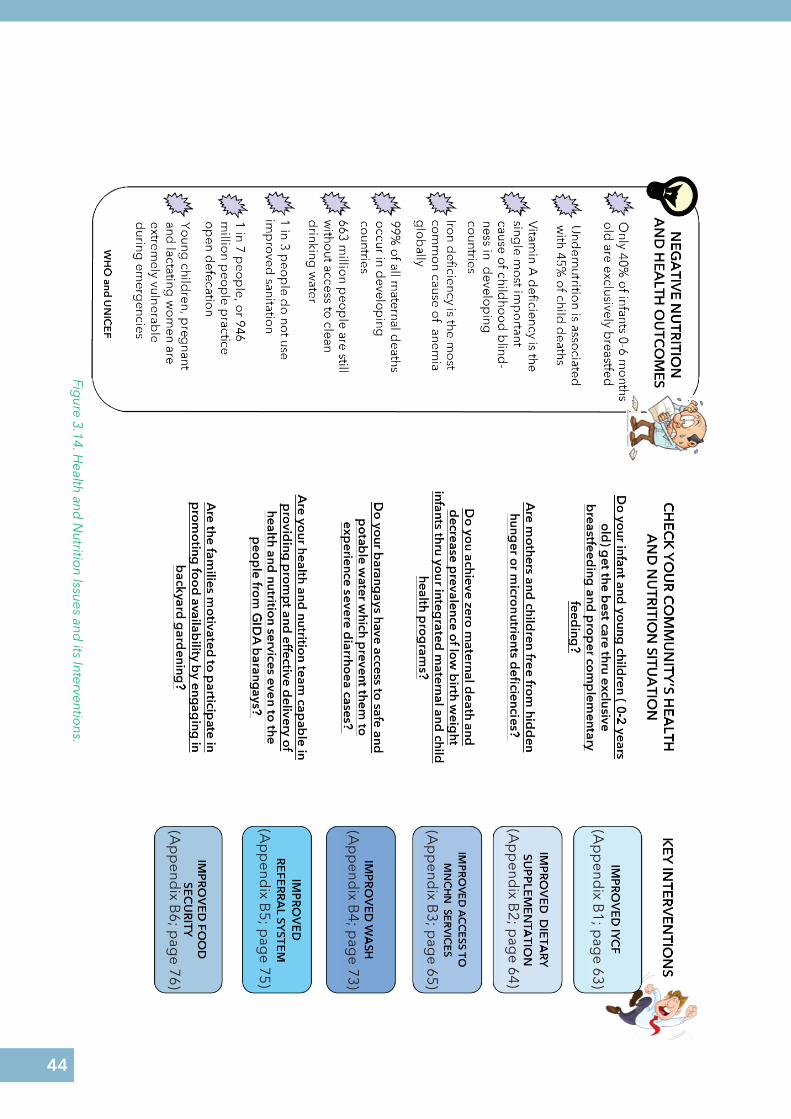
Some of the issues and problems that your municipality might encounter are in the next page. But don’t you worry, as there are evidence-based interventions that will help you battle these challenges. (Figure 3.14).
44
Figure 3.14. H
ealth and N
utrition Issues and
its Interventions.
(Ap
pend
ix B1; p
age 63)
(Ap
pend
ix B2; p
age 64)
(Ap
pend
ix B3; p
age 65)
(Ap
pend
ix B4; p
age 73)
(Ap
pend
ix B5; p
age 75)
(Ap
pend
ix B6; p
age 76)
45
Innovation for Sustainable Service Delivery
3
You can translate your vision and mission to doable innovative programs and interventions to ensure sustainable service delivery. This will increase the participation of community stakeholders, particularly its vulnerable members.
From your C/MNAP, you can package interventions in a unified program, specifically on the first 1000 days. In the experiences of successful LGUs, well-packaged programs that elicit high participation, generate fun, and achieve promotion, education, and behavior change are well-received by the communities (Compendium of Actions on Nutrition, 2018).
Sustainability does not only rely on the competency of implementers. It also depends on how the stakeholders change their behavior and have control over their actions towards better health and nutritional status.
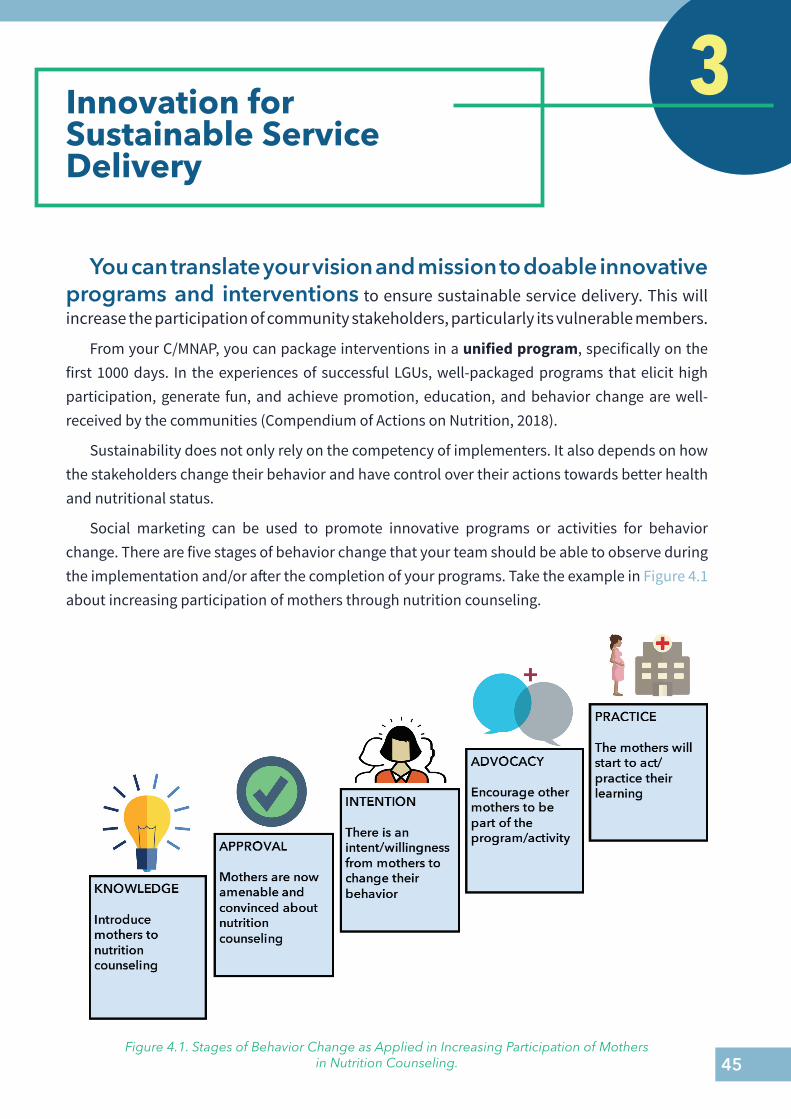
Social marketing can be used to promote innovative programs or activities for behavior change. There are five stages of behavior change that your team should be able to observe during the implementation and/or after the completion of your programs. Take the example in Figure 4.1 about increasing participation of mothers through nutrition counseling.
Figure 4.1. Stages of Behavior Change as Applied in Increasing Participation of Mothers in Nutrition Counseling.
46
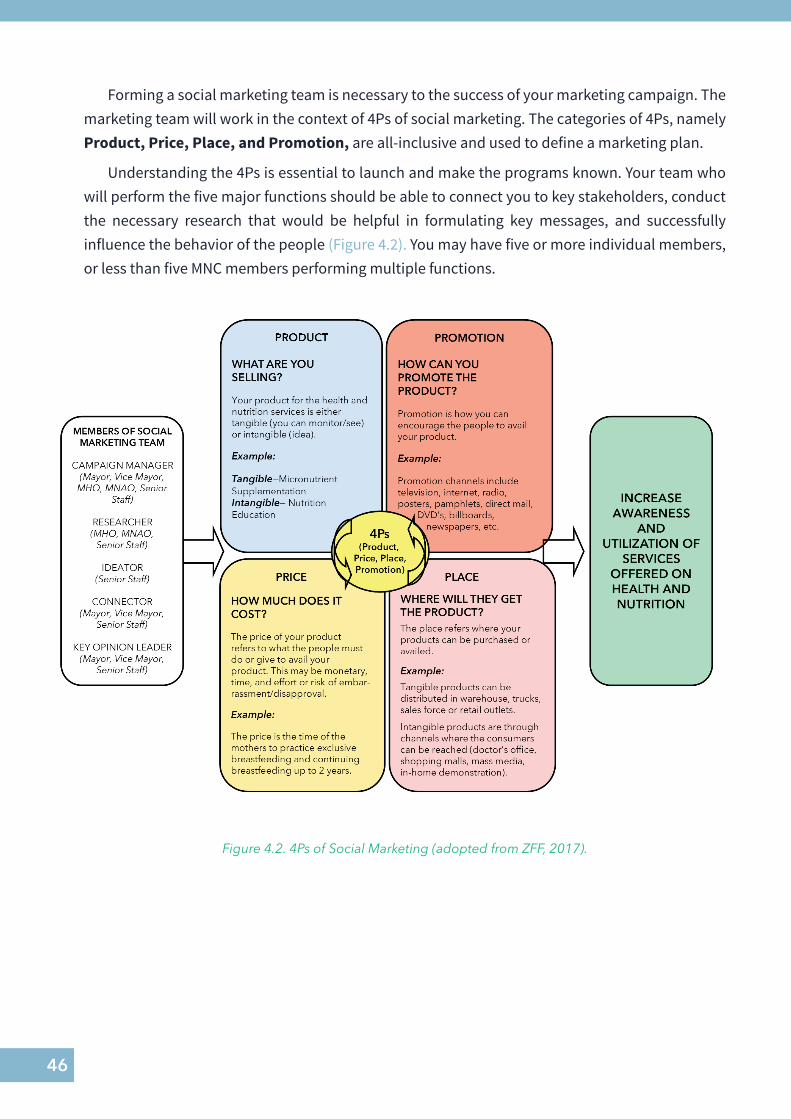
Forming a social marketing team is necessary to the success of your marketing campaign. The marketing team will work in the context of 4Ps of social marketing. The categories of 4Ps, namely Product, Price, Place, and Promotion, are all-inclusive and used to define a marketing plan.
Understanding the 4Ps is essential to launch and make the programs known. Your team who will perform the five major functions should be able to connect you to key stakeholders, conduct the necessary research that would be helpful in formulating key messages, and successfully influence the behavior of the people (Figure 4.2). You may have five or more individual members, or less than five MNC members performing multiple functions.
Figure 4.2. 4Ps of Social Marketing (adopted from ZFF, 2017).

47
How to Market Your Programs
General Social Marketing Steps
The Example of Maternal and Child Care Incentive Programs by Gamay,
Northern Samar 1. Identify the problem to be
addressedLow pre-natal and post-natal visit of mothers to health facility
2. Determine intervention/s to address the problem. You may use catchy title that is unique in your city/municipality
Maternal and Child Care Incentive
Buntis Pares
3. Choose your audience. You can choose primary or secondary audience
Primary Audience: Pregnant WomenSecondary Audience: Barangay Health Workers
4. Define the actions you want each audience to take
Pregnant women should have at least four pre-natal visits and two post-partum visits
5. Know your audience by conducting research
Because of location, some pregnant women need to travel from GIDA barangays. Mothers have low motivation and fear of giving birth at the health facility.
6. Implement the program or project Buntis Pares was intended to promote partnership between the BHWs and the pregnant women. The BHWs regularly monitored the pregnant women in their respective barangays and ensured that they will have pre-natal check up every trimester. They are trained to build the confidence of the mothers to give birth at the health facility.Through the RHM and BHWs the pregnant women are informed prior to delivery that RHUs has 2-4 beds for them. An incentive was given to those who completed four pre-natal and four post-partum visit. The amount of Php 500 is given to the mother and Php 350 to the health worker assigned. To ensure success of the program, incentive can only be collected from the Treasurer’s Office 1 ½ months after delivery.
7. Evaluate the effect of intervention The MNC, through the MHO, regularly check the clients who completed the requirements. During PIR, the feedbacking to the health workers are done to intensify the monitoring of mothers and increase delivery at the health facility.
8. Refine the program Based on the result of evaluation, the MNC can recommend to add more support to the RHU and/or increase the incentive.
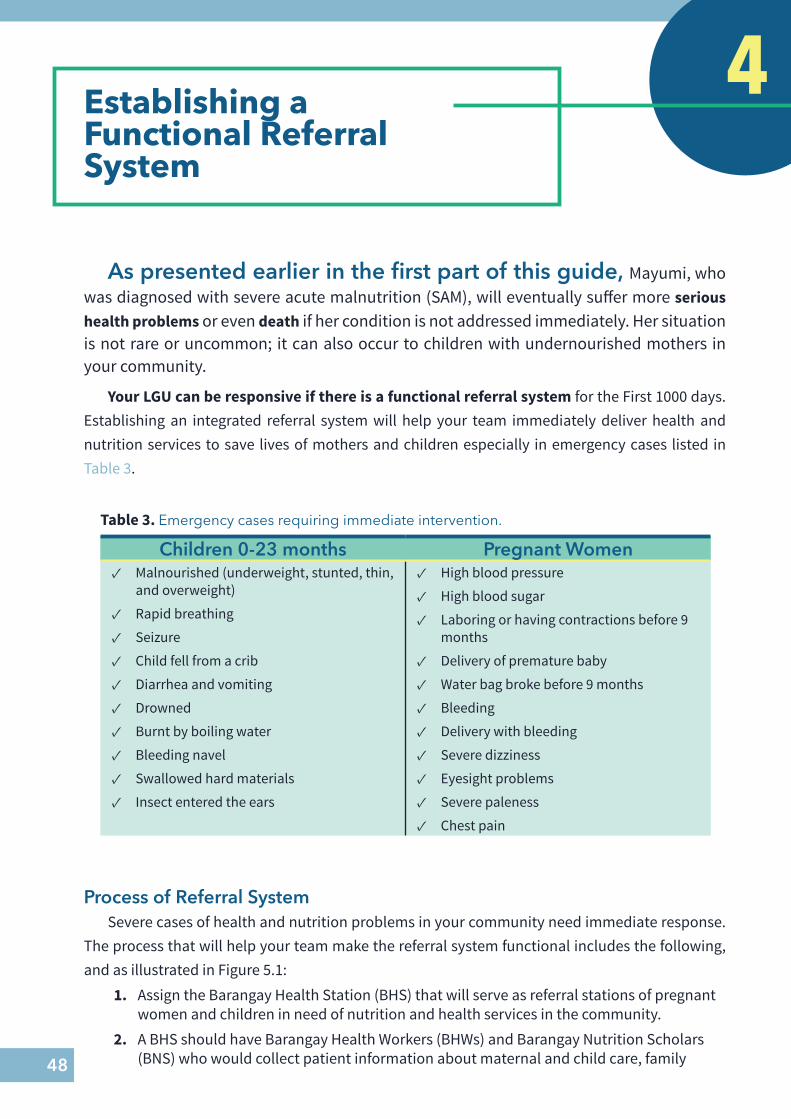
48
Establishing a Functional Referral System
4
As presented earlier in the first part of this guide, Mayumi, who was diagnosed with severe acute malnutrition (SAM), will eventually suffer more serious health problems or even death if her condition is not addressed immediately. Her situation is not rare or uncommon; it can also occur to children with undernourished mothers in your community.
Your LGU can be responsive if there is a functional referral system for the First 1000 days. Establishing an integrated referral system will help your team immediately deliver health and nutrition services to save lives of mothers and children especially in emergency cases listed in Table 3.
Table 3. Emergency cases requiring immediate intervention.
Children 0-23 months Pregnant Women ✓ Malnourished (underweight, stunted, thin,
and overweight)
✓ Rapid breathing
✓ Seizure
✓ Child fell from a crib
✓ Diarrhea and vomiting
✓ Drowned
✓ Burnt by boiling water
✓ Bleeding navel
✓ Swallowed hard materials
✓ Insect entered the ears
✓ High blood pressure
✓ High blood sugar
✓ Laboring or having contractions before 9 months
✓ Delivery of premature baby
✓ Water bag broke before 9 months
✓ Bleeding
✓ Delivery with bleeding
✓ Severe dizziness
✓ Eyesight problems
✓ Severe paleness
✓ Chest pain
Process of Referral SystemSevere cases of health and nutrition problems in your community need immediate response.
The process that will help your team make the referral system functional includes the following, and as illustrated in Figure 5.1:
1. Assign the Barangay Health Station (BHS) that will serve as referral stations of pregnant women and children in need of nutrition and health services in the community.
2. A BHS should have Barangay Health Workers (BHWs) and Barangay Nutrition Scholars (BNS) who would collect patient information about maternal and child care, family
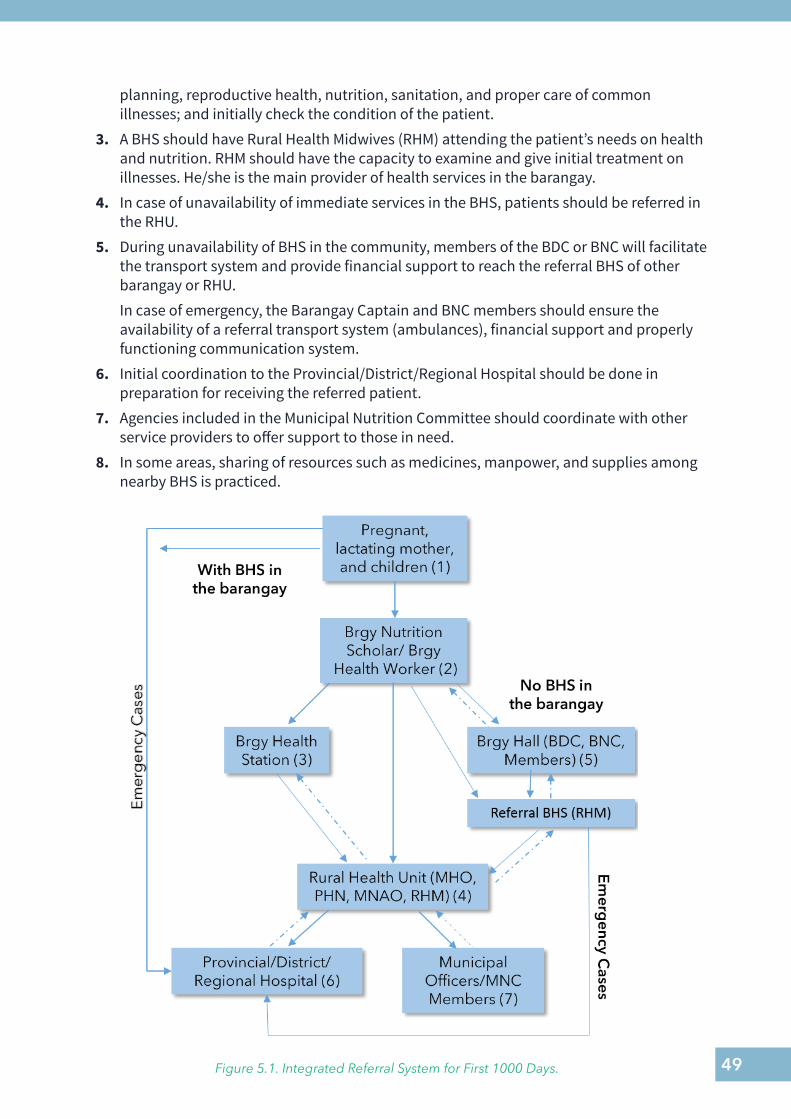
49
planning, reproductive health, nutrition, sanitation, and proper care of common illnesses; and initially check the condition of the patient.
3. A BHS should have Rural Health Midwives (RHM) attending the patient’s needs on health and nutrition. RHM should have the capacity to examine and give initial treatment on illnesses. He/she is the main provider of health services in the barangay.
4. In case of unavailability of immediate services in the BHS, patients should be referred in the RHU.
5. During unavailability of BHS in the community, members of the BDC or BNC will facilitate the transport system and provide financial support to reach the referral BHS of other barangay or RHU.In case of emergency, the Barangay Captain and BNC members should ensure the availability of a referral transport system (ambulances), financial support and properly functioning communication system.
6. Initial coordination to the Provincial/District/Regional Hospital should be done in preparation for receiving the referred patient.
7. Agencies included in the Municipal Nutrition Committee should coordinate with other service providers to offer support to those in need.
8. In some areas, sharing of resources such as medicines, manpower, and supplies among nearby BHS is practiced.
Figure 5.1. Integrated Referral System for First 1000 Days.
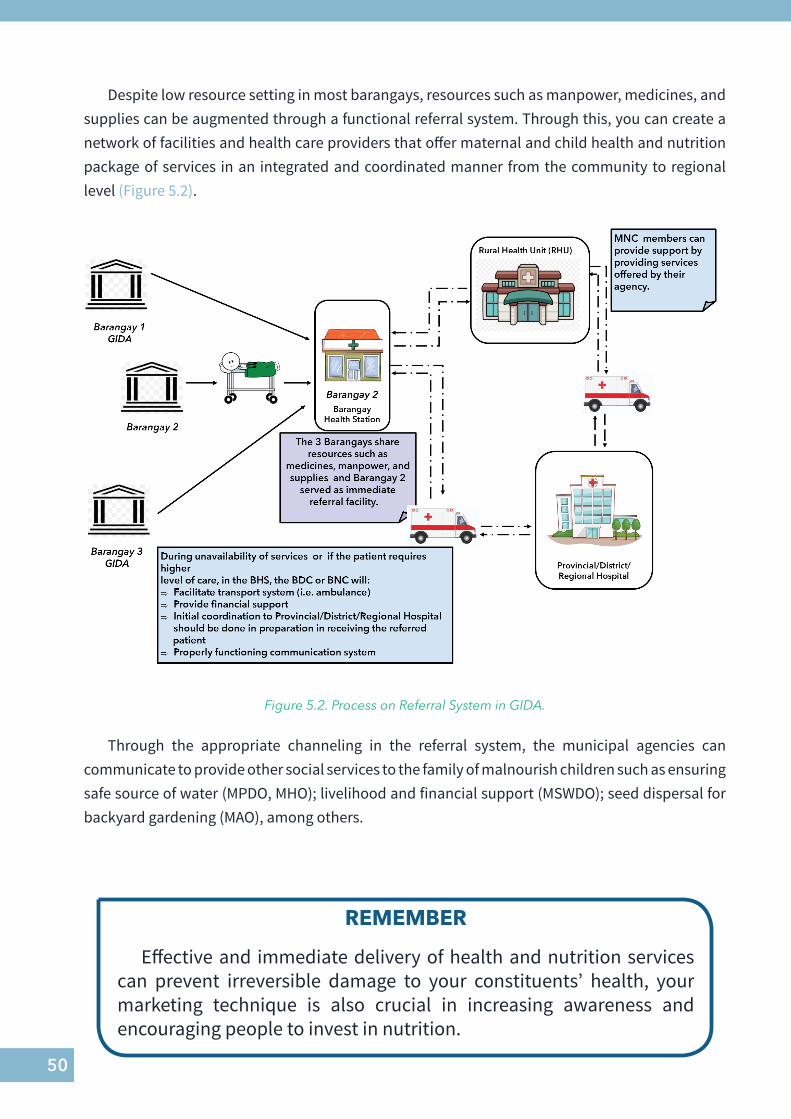
50
Despite low resource setting in most barangays, resources such as manpower, medicines, and supplies can be augmented through a functional referral system. Through this, you can create a network of facilities and health care providers that offer maternal and child health and nutrition package of services in an integrated and coordinated manner from the community to regional level (Figure 5.2).
Figure 5.2. Process on Referral System in GIDA.
REMEMBER
Effective and immediate delivery of health and nutrition services can prevent irreversible damage to your constituents’ health, your marketing technique is also crucial in increasing awareness and encouraging people to invest in nutrition.
Through the appropriate channeling in the referral system, the municipal agencies can communicate to provide other social services to the family of malnourish children such as ensuring safe source of water (MPDO, MHO); livelihood and financial support (MSWDO); seed dispersal for backyard gardening (MAO), among others.
51
HERE’S HOW THEY DID IT
In Gamay, Northern Samar and Looc, Romblon, effective communication within and between departments enabled them to have an integrated service delivery to their clients especially to the SAM patients. The LGUs have a referral system wherein patients identified by the barangay local health and nutrition workers are referred to the Municipal Health Officer for medical intervention, and likewise referred to the MSWDO for other social services which can be provided to the family. If the need arises, the family will be referred to the Municipal Agriculture Office for livelihood assistance through inclusion in the different agricultural extension programs. Through the system, the LGUs put their focus to the patients and provide increased access of patients to the local health and nutrition services. The LGUs consider the system as an integral and co-creating part of achieving of their goals.
Dr. Timoteo Capoquian, Jr. and Mayor Leila Arboleda (Public Narratives)
GAMAY’S AND LOOC’S REFERRAL SYSTEM
52
Summary
What have you learned to help your community and children like Mayumi?
✓ As the mayor, investing in nutrition is essential in the progress of your community.
✓ As stated in Republic Act 11148 or the First 1000 Days (F1KD) Law, LGUs should prioritize interventions and investments for the first 1000 days of a child’s life.
✓ As stated in DILG Memorandum Circular 2018-42, you and your LGU have roles and responsibilities to ensure good health and proper nutrition in your community.
✓ As a Bridging Leader, you are influential in bringing together different agencies to achieve your preferred nutrition reality.
✓ The Six Building Blocks of Health System will help you build a stronger local health system towards a more efficient and responsive system, social and financial risk protection of your constituents, and most of all, improved health for your community.
✓ Social marketing strategies can help you innovate your nutrition programs, and make them sustainable to achieve a good and integrated local nutrition system for better health and community development.

53
YOU CAN MAKE A DIFFERENCE!
As the leader of your community, guided with the knowledge on the
six building blocks of health, you can influence other people to help Mayumi
and other children like her. It’s never too late to ACT! Your community can become a champion in health and
nutrition.
54
Literature Cited
Department of Health. (2018). National objectives for health Philippines 2017-2022. Manila, Philippines: Department of Health. Retrieved from: https://www.doh.gov.ph/sites/default/files/health_magazine/NOH-2017-2022-030619-1%281%29_0.pdf
Department of Health. (2017). LGU Health Scorecard. Retrieved from: http://ro8.doh.gov.ph/lgu-scorecard/
Department of Science and Technology – Food and Nutrition Research Institute (DOST-FNRI). (2018). National Nutrition Survey 2018 Update. Taguig City, Philippines: Author.
Department of the Interior and Local Government. (2018). Memorandum Circular 2018-42: Adoption and Implementation of the Philippine Plan of Action for Nutrition 2017-2022. Quezon City, Philippines: Author.
National Nutrition Council. (2017). Laguna LGUs share best practices and strategies to Region 1 Local Nutrition Planners. Retrieved from: https://www.nnc.gov.ph/index.php/regional-offices/region-i-lupangilocos/2055-laguna-shares-best-nutrition-practices-and-strategies-in-nutrition-programs-to-region-i-delegates.html
National Nutrition Council. (2017). Philippine Plan of Action for Nutrition 2017-2022. Taguig City, Philippines: Author.
National Nutrition Council. (2018). Compendium of Actions on Nutrition. Taguig City, Philippines: Author.
Savigny D and Adam T (Eds). (2009). Systems thinking for health systems strengthening. Alliance for Health Policy and Systems Research, WHO. Retrieved from: https://www.who.int/alliance hpsr/resources/9789241563895/en/
United Nations Children’s Fund (UNICEF). (2018). Breastfeeding in emergency situation. Retrieved from: https://www.unicef.org/nutrition/files/8_Advocacy_Brief_on_BF_in_Emergencies.pdf
United Nations Children’s Fund (UNICEF). (nd). Water, Sanitation and Hygiene. Retrieved from: https://www.unicef.org/wash/
United Nations System Standing Committee on Nutrition (UNSCN). (nd). Summary Chapter 3: Maternal nutrition and intergenerational cycle of growth failure. Retrieved from: https://www.unscn.org/files/Publications/RWNS6/report/chapter3.pdf
World Bank. (2004). World Development Report 2004: Making Services Work for Poor People. Washington DC, USA: The International Bank for Reconstruction and Development/World Bank.
World Health Organization. (2010). Monitoring the Building Blocks of Health Systems: A Handbook of Indicators and Their Measurement Strategies. Switzerland. Retrieved 3 August 2019 from https://www.who.int/healthinfo/systems/WHO_MBHSS_2010_full_web.pdf
World Health Organization (WHO). (2018). Malnutrion. Retrieved from: https://www.who.int/news-room/fact-sheets/detail/malnutrition
World Health Organization (WHO). (2018). Maternal mortality. Retrieved from: https://www.who.
55
int/en/news-room/fact-sheets/detail/maternal-mortality
World Health Organization (WHO). (2018). Infant and young child feeding. Retrieved from: https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding
World Health Organization (WHO) and United Nations Children’s Fund (UNICEF). (nd). Global prevalence of vitamin A deficiency: Overview. Retrieved from: https://www.who.int/nutrition/publications/micronutrients/vitamin_a_deficiency/WHO_NUT_95.3/en/
World Health Organization (WHO). (2019). Anaemia. Retrieved from: https://www.who.int/topics/anaemia/en/
Vega, M. (2016). The MRI evidence in favor of cash transfers. Retrieved from: http://www.globalhealthhub.org/2016/09/19/mri-evidence-favor-cash-transfers/
56
APPENDIX A.MEDICINES, VACCINES, AND TECHNOLOGY
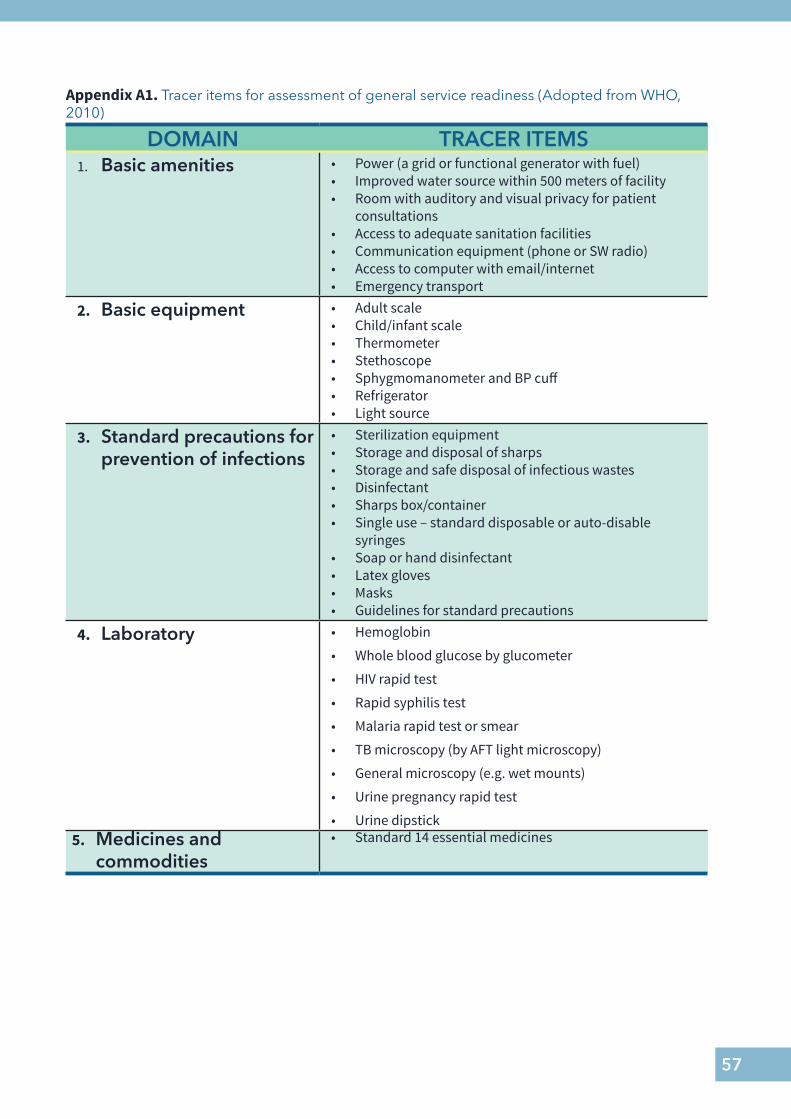
57
Appendix A1. Tracer items for assessment of general service readiness (Adopted from WHO, 2010)
DOMAIN TRACER ITEMS1. Basic amenities • Power (a grid or functional generator with fuel)
• Improved water source within 500 meters of facility • Room with auditory and visual privacy for patient
consultations • Access to adequate sanitation facilities • Communication equipment (phone or SW radio) • Access to computer with email/internet• Emergency transport
2. Basic equipment • Adult scale• Child/infant scale • Thermometer • Stethoscope • Sphygmomanometer and BP cuff • Refrigerator • Light source
3. Standard precautions for prevention of infections
• Sterilization equipment • Storage and disposal of sharps • Storage and safe disposal of infectious wastes • Disinfectant • Sharps box/container • Single use – standard disposable or auto-disable
syringes • Soap or hand disinfectant • Latex gloves • Masks • Guidelines for standard precautions
4. Laboratory • Hemoglobin
• Whole blood glucose by glucometer
• HIV rapid test
• Rapid syphilis test
• Malaria rapid test or smear
• TB microscopy (by AFT light microscopy)
• General microscopy (e.g. wet mounts)
• Urine pregnancy rapid test
• Urine dipstick5. Medicines and
commodities• Standard 14 essential medicines
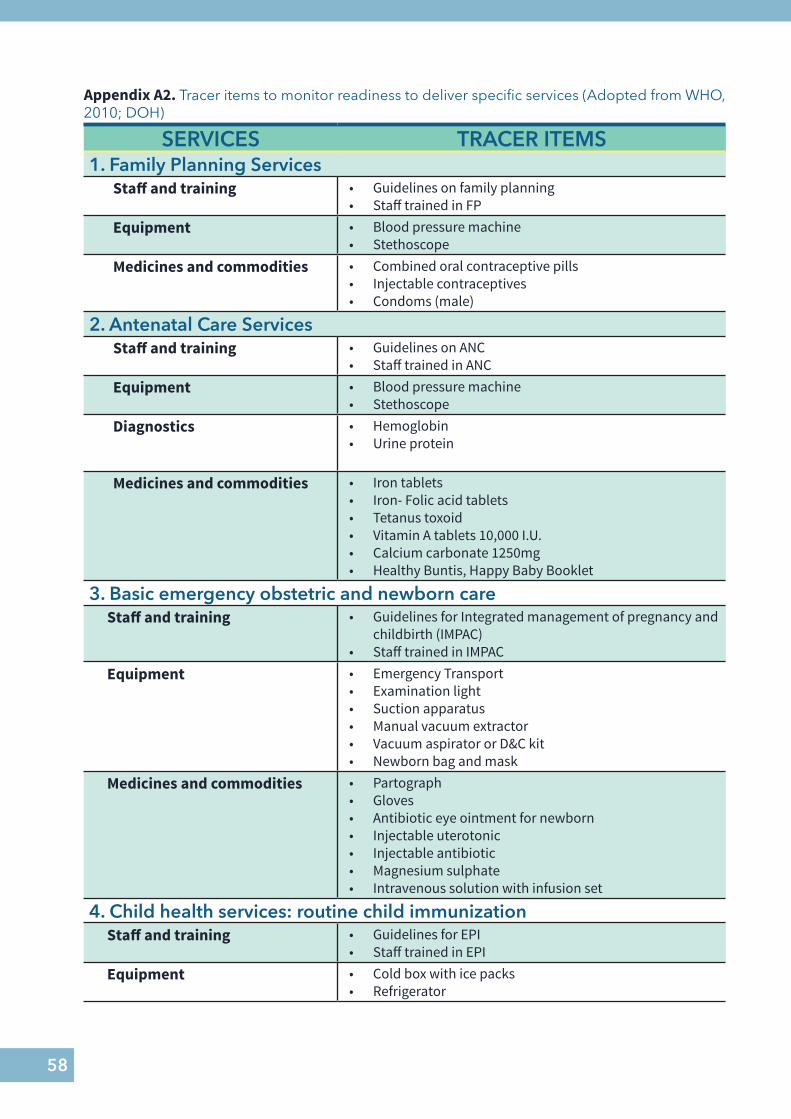
58
Appendix A2. Tracer items to monitor readiness to deliver specific services (Adopted from WHO, 2010; DOH)
SERVICES TRACER ITEMS1. Family Planning Services
Staff and training • Guidelines on family planning • Staff trained in FP
Equipment • Blood pressure machine • Stethoscope
Medicines and commodities • Combined oral contraceptive pills • Injectable contraceptives • Condoms (male)
2. Antenatal Care ServicesStaff and training • Guidelines on ANC
• Staff trained in ANCEquipment • Blood pressure machine
• StethoscopeDiagnostics • Hemoglobin
• Urine protein
Medicines and commodities • Iron tablets • Iron- Folic acid tablets • Tetanus toxoid• Vitamin A tablets 10,000 I.U. • Calcium carbonate 1250mg • Healthy Buntis, Happy Baby Booklet
3. Basic emergency obstetric and newborn careStaff and training • Guidelines for Integrated management of pregnancy and
childbirth (IMPAC) • Staff trained in IMPAC
Equipment • Emergency Transport • Examination light • Suction apparatus • Manual vacuum extractor • Vacuum aspirator or D&C kit • Newborn bag and mask
Medicines and commodities • Partograph • Gloves • Antibiotic eye ointment for newborn • Injectable uterotonic • Injectable antibiotic • Magnesium sulphate • Intravenous solution with infusion set
4. Child health services: routine child immunizationStaff and training • Guidelines for EPI
• Staff trained in EPIEquipment • Cold box with ice packs
• Refrigerator
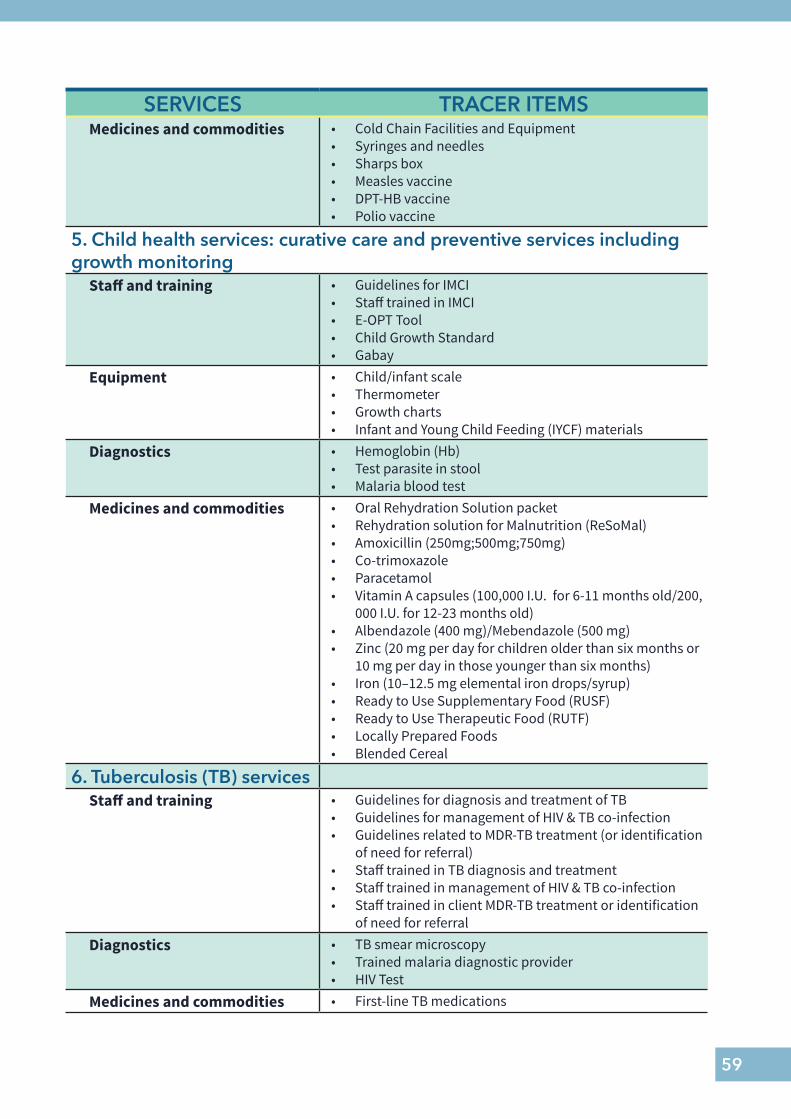
59
SERVICES TRACER ITEMSMedicines and commodities • Cold Chain Facilities and Equipment
• Syringes and needles • Sharps box • Measles vaccine • DPT-HB vaccine • Polio vaccine
5. Child health services: curative care and preventive services including growth monitoring
Staff and training • Guidelines for IMCI • Staff trained in IMCI• E-OPT Tool• Child Growth Standard • Gabay
Equipment • Child/infant scale • Thermometer • Growth charts• Infant and Young Child Feeding (IYCF) materials
Diagnostics • Hemoglobin (Hb) • Test parasite in stool • Malaria blood test
Medicines and commodities • Oral Rehydration Solution packet• Rehydration solution for Malnutrition (ReSoMal)• Amoxicillin (250mg;500mg;750mg) • Co-trimoxazole • Paracetamol • Vitamin A capsules (100,000 I.U. for 6-11 months old/200,
000 I.U. for 12-23 months old)• Albendazole (400 mg)/Mebendazole (500 mg)• Zinc (20 mg per day for children older than six months or
10 mg per day in those younger than six months)• Iron (10–12.5 mg elemental iron drops/syrup)• Ready to Use Supplementary Food (RUSF)• Ready to Use Therapeutic Food (RUTF)• Locally Prepared Foods• Blended Cereal
6. Tuberculosis (TB) servicesStaff and training • Guidelines for diagnosis and treatment of TB
• Guidelines for management of HIV & TB co-infection • Guidelines related to MDR-TB treatment (or identification
of need for referral) • Staff trained in TB diagnosis and treatment • Staff trained in management of HIV & TB co-infection • Staff trained in client MDR-TB treatment or identification
of need for referralDiagnostics • TB smear microscopy
• Trained malaria diagnostic provider • HIV Test
Medicines and commodities • First-line TB medications
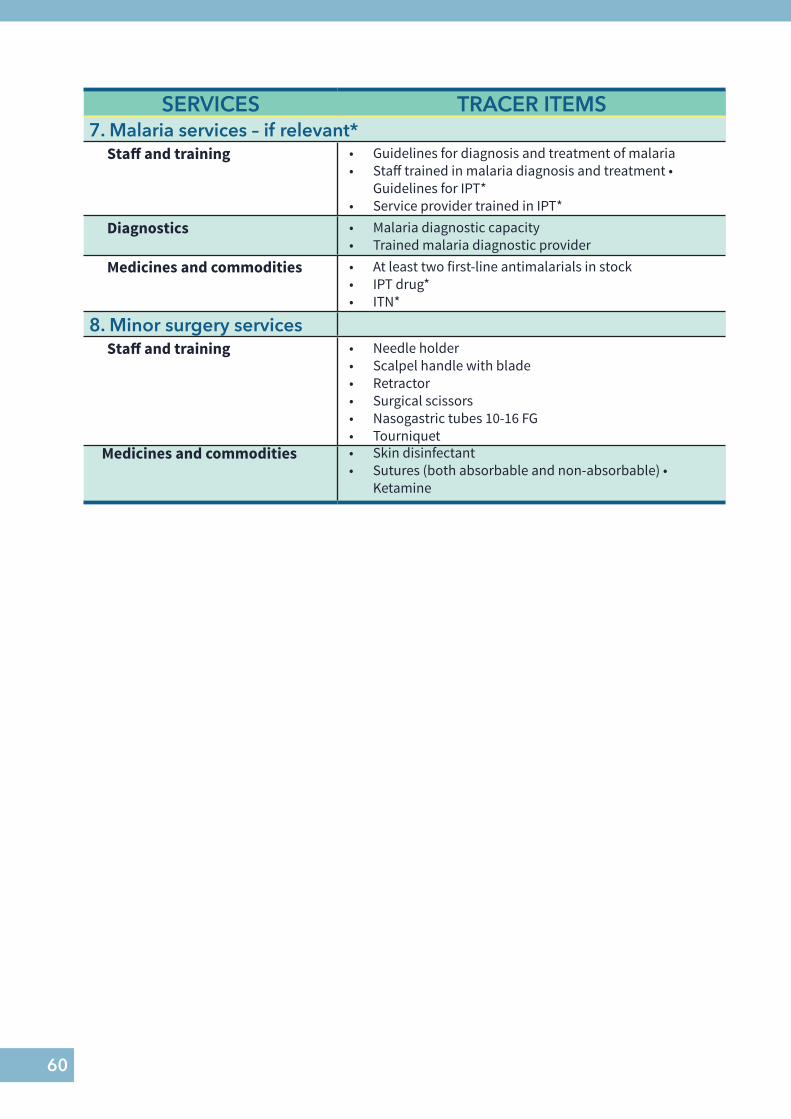
60
SERVICES TRACER ITEMS7. Malaria services – if relevant*
Staff and training • Guidelines for diagnosis and treatment of malaria • Staff trained in malaria diagnosis and treatment •
Guidelines for IPT* • Service provider trained in IPT*
Diagnostics • Malaria diagnostic capacity • Trained malaria diagnostic provider
Medicines and commodities • At least two first-line antimalarials in stock • IPT drug* • ITN*
8. Minor surgery servicesStaff and training • Needle holder
• Scalpel handle with blade • Retractor • Surgical scissors • Nasogastric tubes 10-16 FG • Tourniquet
Medicines and commodities • Skin disinfectant • Sutures (both absorbable and non-absorbable) •
Ketamine

62
APPENDIX B.EVIDENCE-BASED ACTION FOR FIRST 1000 DAYS
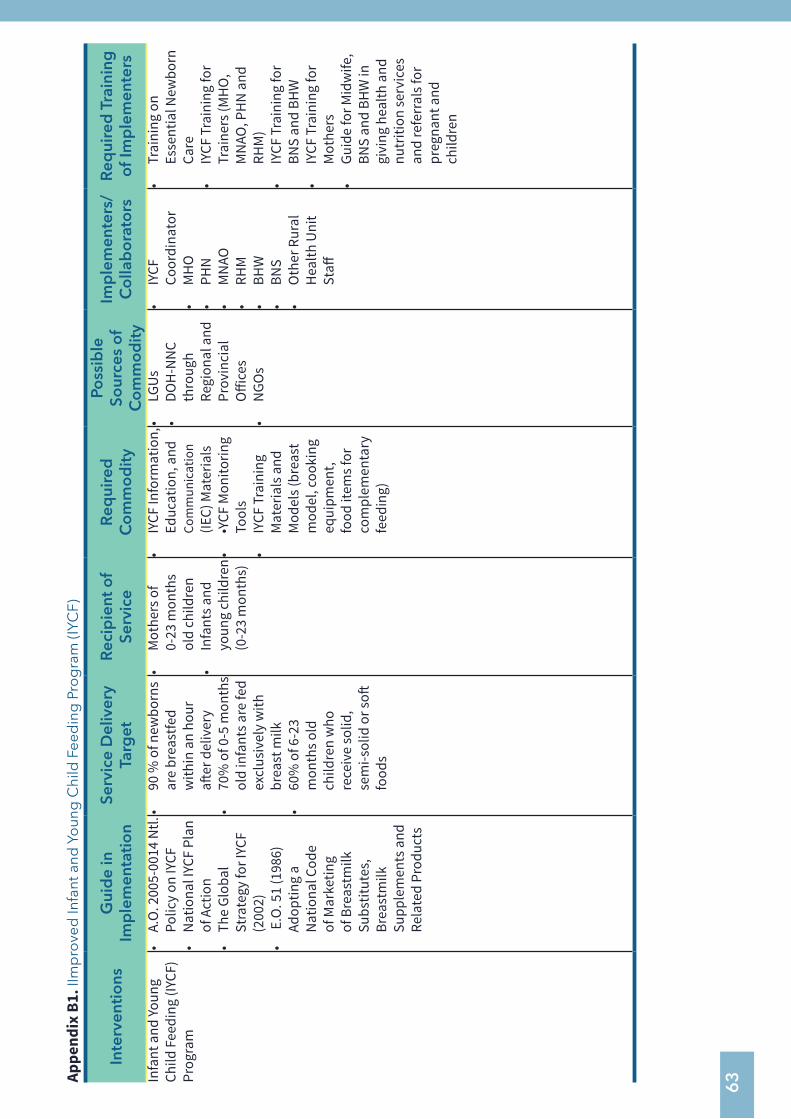
63Ap
pend
ix B
1. II
mp
rove
d In
fant
and
Yo
ung
Chi
ld F
eed
ing
Pro
gra
m (I
YCF)
Inte
rven
tio
nsG
uid
e in
Im
ple
men
tati
on
Serv
ice
Del
iver
y Ta
rget
Rec
ipie
nt o
f Se
rvic
eR
equi
red
C
om
mo
dit
y
Poss
ible
So
urce
s o
f C
om
mo
dit
y
Imp
lem
ente
rs/
Co
llab
ora
tors
Req
uire
d T
rain
ing
o
f Im
ple
men
ters
Infa
nt a
nd Yo
ung
Child
Fee
ding
(IYC
F)
Prog
ram
• A.
O. 2
005-
0014
Ntl.
Po
licy
on IY
CF•
Nat
iona
l IYC
F Pl
an
of A
ctio
n•
The
Glob
al
Stra
tegy
for I
YCF
(200
2)•
E.O
. 51
(198
6)
Adop
ting
a N
atio
nal C
ode
of M
arke
ting
of B
reas
tmilk
Su
bstit
utes
, Br
east
milk
Su
pple
men
ts a
nd
Rela
ted
Prod
ucts
• 90
% o
f new
born
s ar
e br
east
fed
with
in a
n ho
ur
after
del
iver
y•
70%
of 0
-5 m
onth
s ol
d in
fant
s are
fed
excl
usiv
ely
with
br
east
milk
• 60
% o
f 6-2
3 m
onth
s old
ch
ildre
n w
ho
rece
ive
solid
, se
mi-s
olid
or s
oft
food
s
• M
othe
rs o
f 0-
23 m
onth
s ol
d ch
ildre
n •
Infa
nts a
nd
youn
g ch
ildre
n (0
-23
mon
ths)
• IY
CF In
form
atio
n,
Educ
atio
n, a
nd
Com
mun
icat
ion
(IEC)
Mat
eria
ls•
•YCF
Mon
itorin
g To
ols
• IY
CF T
rain
ing
Mat
eria
ls a
nd
Mod
els (
brea
st
mod
el, c
ooki
ng
equi
pmen
t, fo
od it
ems f
or
com
plem
enta
ry
feed
ing)
• LG
Us•
DOH
-NN
C th
roug
h Re
gion
al a
nd
Prov
inci
al
Offi
ces
• N
GOs
• IY
CF
Coor
dina
tor
• M
HO
• PH
N•
MN
AO•
RHM
• BH
W•
BNS
• O
ther
Rur
al
Hea
lth U
nit
Staff
• Tr
aini
ng o
n Es
sent
ial N
ewbo
rn
Care
•
IYCF
Tra
inin
g fo
r Tr
aine
rs (M
HO
, M
NAO
, PH
N a
nd
RHM
) •
IYCF
Tra
inin
g fo
r BN
S an
d BH
W•
IYCF
Tra
inin
g fo
r M
othe
rs•
Guid
e fo
r Mid
wife
, BN
S an
d BH
W in
gi
ving
hea
lth a
nd
nutr
ition
serv
ices
an
d re
ferr
als f
or
preg
nant
and
ch
ildre
n
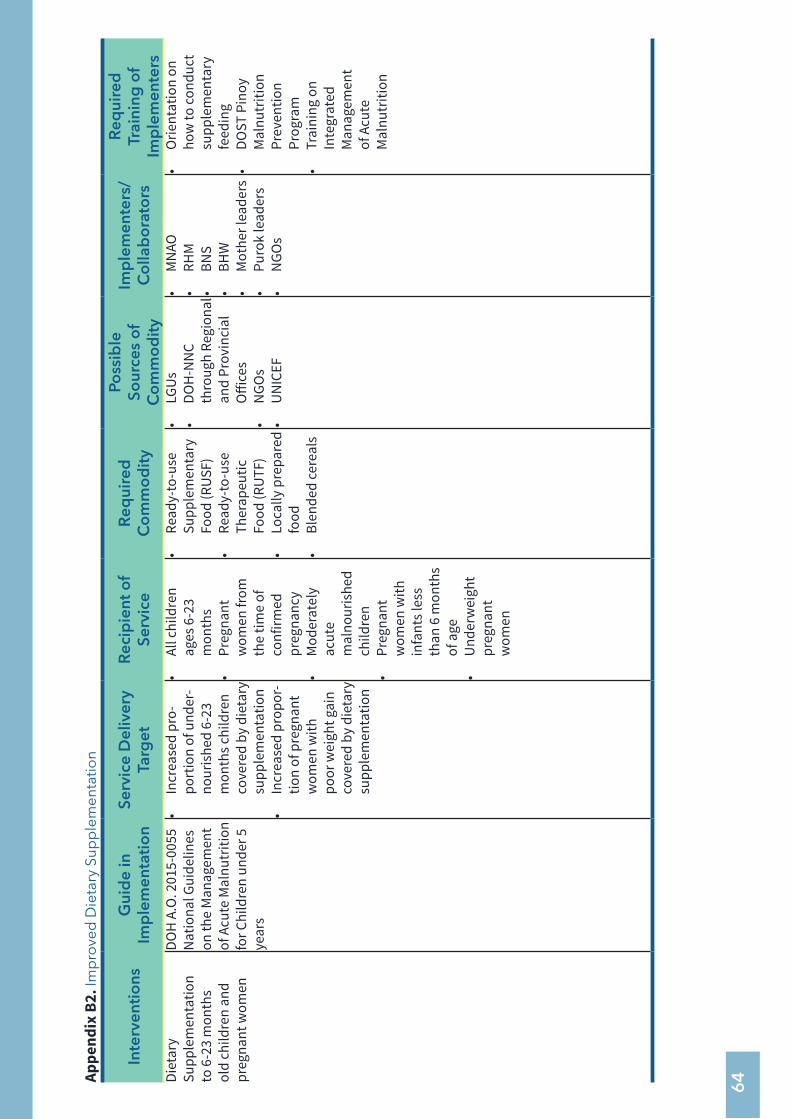
64Ap
pend
ix B
2. Im
pro
ved
Die
tary
Sup
ple
men
tatio
n
Inte
rven
tio
nsG
uid
e in
Im
ple
men
tati
on
Serv
ice
Del
iver
y Ta
rget
Rec
ipie
nt o
f Se
rvic
eR
equi
red
C
om
mo
dit
y
Poss
ible
So
urce
s o
f C
om
mo
dit
y
Imp
lem
ente
rs/
Co
llab
ora
tors
Req
uire
d
Trai
ning
of
Imp
lem
ente
rsDi
etar
y Su
pple
men
tatio
n to
6-2
3 m
onth
s ol
d ch
ildre
n an
d pr
egna
nt w
omen
DOH
A.O
. 201
5-00
55
Nat
iona
l Gui
delin
es
on th
e M
anag
emen
t of
Acu
te M
alnu
triti
on
for C
hild
ren
unde
r 5
year
s
• In
crea
sed
pro-
port
ion
of u
nder
-no
uris
hed
6-23
m
onth
s chi
ldre
n co
vere
d by
die
tary
su
pple
men
tatio
n•
Incr
ease
d pr
opor
-tio
n of
pre
gnan
t w
omen
with
po
or w
eigh
t gai
n co
vere
d by
die
tary
su
pple
men
tatio
n
• Al
l chi
ldre
n ag
es 6
-23
mon
ths
• Pr
egna
nt
wom
en fr
om
the
time
of
conf
irmed
pr
egna
ncy
• M
oder
atel
y ac
ute
mal
nour
ishe
d ch
ildre
n•
Preg
nant
w
omen
with
in
fant
s les
s th
an 6
mon
ths
of a
ge•
Und
erw
eigh
t pr
egna
nt
wom
en
• Re
ady-
to-u
se
Supp
lem
enta
ry
Food
(RUS
F)•
Read
y-to
-use
Th
erap
eutic
Fo
od (R
UTF
)•
Loca
lly p
repa
red
food
• Bl
ende
d ce
real
s
• LG
Us•
DOH
-NN
C th
roug
h Re
gion
al
and
Prov
inci
al
Offi
ces
• N
GOs
• U
NIC
EF
• M
NAO
• RH
M•
BNS
• BH
W•
Mot
her l
eade
rs•
Puro
k le
ader
s•
NGO
s
• O
rient
atio
n on
ho
w to
cond
uct
supp
lem
enta
ry
feed
ing
• DO
ST P
inoy
M
alnu
triti
on
Prev
entio
n Pr
ogra
m•
Trai
ning
on
Inte
grat
ed
Man
agem
ent
of A
cute
M
alnu
triti
on
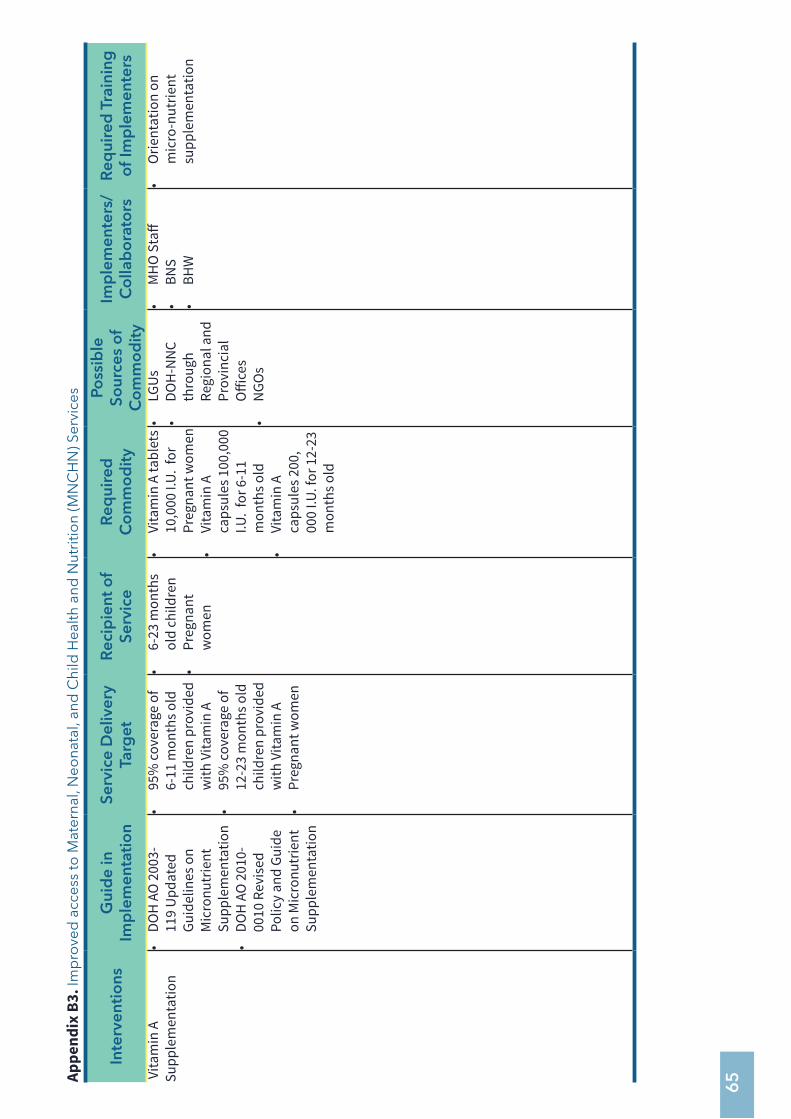
65Ap
pend
ix B
3. Im
pro
ved
acc
ess
to M
ater
nal,
Neo
nata
l, an
d C
hild
Hea
lth a
nd N
utri
tion
(MN
CH
N) S
ervi
ces
Inte
rven
tio
nsG
uid
e in
Im
ple
men
tati
on
Serv
ice
Del
iver
y Ta
rget
Rec
ipie
nt o
f Se
rvic
eR
equi
red
C
om
mo
dit
y
Poss
ible
So
urce
s o
f C
om
mo
dit
y
Imp
lem
ente
rs/
Co
llab
ora
tors
Req
uire
d T
rain
ing
o
f Im
ple
men
ters
Vita
min
A
Supp
lem
enta
tion
• DO
H A
O 2
003-
119
Upd
ated
Gu
idel
ines
on
Mic
ronu
trie
nt
Supp
lem
enta
tion
• DO
H A
O 2
010-
0010
Rev
ised
Po
licy
and
Guid
e on
Mic
ronu
trie
nt
Supp
lem
enta
tion
• 95
% co
vera
ge o
f 6-
11 m
onth
s old
ch
ildre
n pr
ovid
ed
with
Vita
min
A•
95%
cove
rage
of
12-2
3 m
onth
s old
ch
ildre
n pr
ovid
ed
with
Vita
min
A•
Preg
nant
wom
en
• 6-
23 m
onth
s ol
d ch
ildre
n•
Preg
nant
w
omen
• Vi
tam
in A
tabl
ets
10,0
00 I.
U. f
or
Preg
nant
wom
en
• Vi
tam
in A
ca
psul
es 1
00,0
00
I.U.
for 6
-11
mon
ths o
ld•
Vita
min
A
caps
ules
200
, 00
0 I.U
. for
12-
23
mon
ths o
ld
• LG
Us•
DOH
-NN
C th
roug
h Re
gion
al a
nd
Prov
inci
al
Offi
ces
• N
GOs
• M
HO
Sta
ff•
BNS
• BH
W
• O
rient
atio
n on
m
icro
-nut
rient
su
pple
men
tatio
n
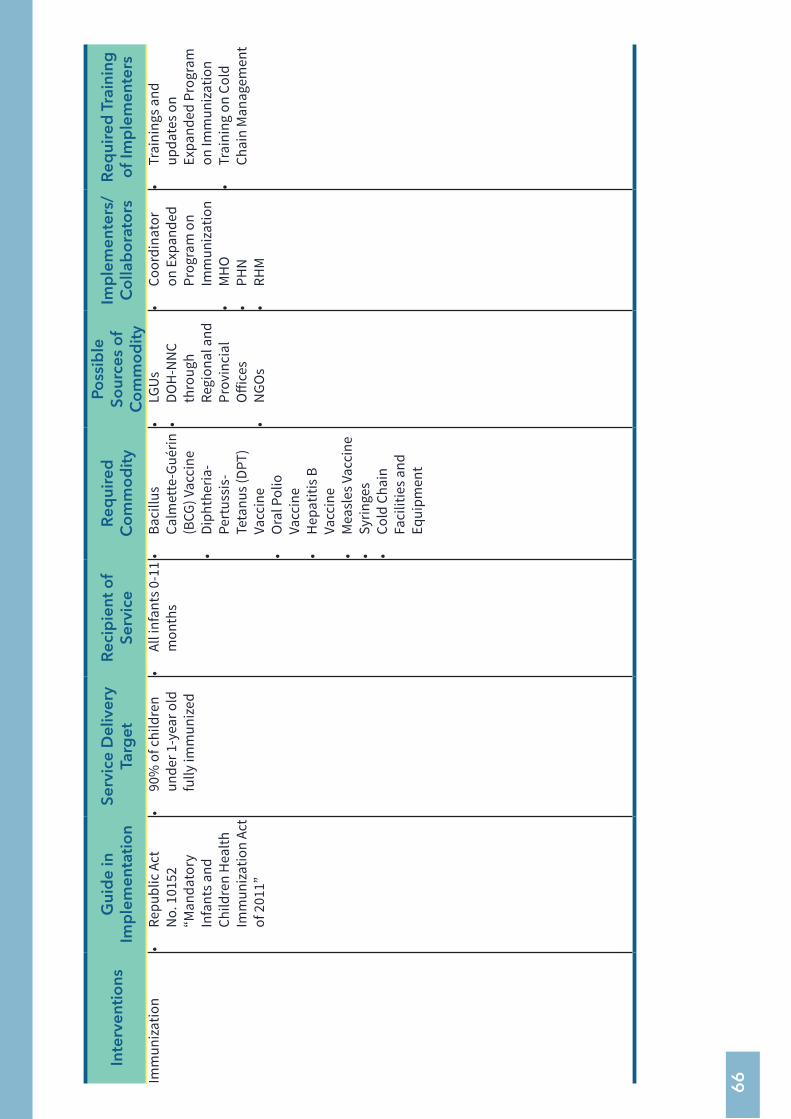
66
Inte
rven
tio
nsG
uid
e in
Im
ple
men
tati
on
Serv
ice
Del
iver
y Ta
rget
Rec
ipie
nt o
f Se
rvic
eR
equi
red
C
om
mo
dit
y
Poss
ible
So
urce
s o
f C
om
mo
dit
y
Imp
lem
ente
rs/
Co
llab
ora
tors
Req
uire
d T
rain
ing
o
f Im
ple
men
ters
Imm
uniz
atio
n•
Repu
blic
Act
N
o. 1
0152
“M
anda
tory
In
fant
s and
Ch
ildre
n H
ealth
Im
mun
izat
ion
Act
of 2
011”
• 90
% o
f chi
ldre
n un
der 1
-yea
r old
fu
lly im
mun
ized
• Al
l inf
ants
0-1
1 m
onth
s•
Baci
llus
Calm
ette
-Gué
rin
(BCG
) Vac
cine
• Di
phth
eria
-Pe
rtus
sis-
Teta
nus (
DPT)
Va
ccin
e•
Ora
l Pol
io
Vacc
ine
• H
epat
itis B
Va
ccin
e•
Mea
sles
Vac
cine
• Sy
ringe
s•
Cold
Cha
in
Faci
litie
s and
Eq
uipm
ent
• LG
Us•
DOH
-NN
C th
roug
h Re
gion
al a
nd
Prov
inci
al
Offi
ces
• N
GOs
• Co
ordi
nato
r on
Exp
ande
d Pr
ogra
m o
n Im
mun
izat
ion
• M
HO
• PH
N•
RHM
• Tr
aini
ngs a
nd
upda
tes o
n Ex
pand
ed P
rogr
am
on Im
mun
izat
ion
• Tr
aini
ng o
n Co
ld
Chai
n M
anag
emen
t
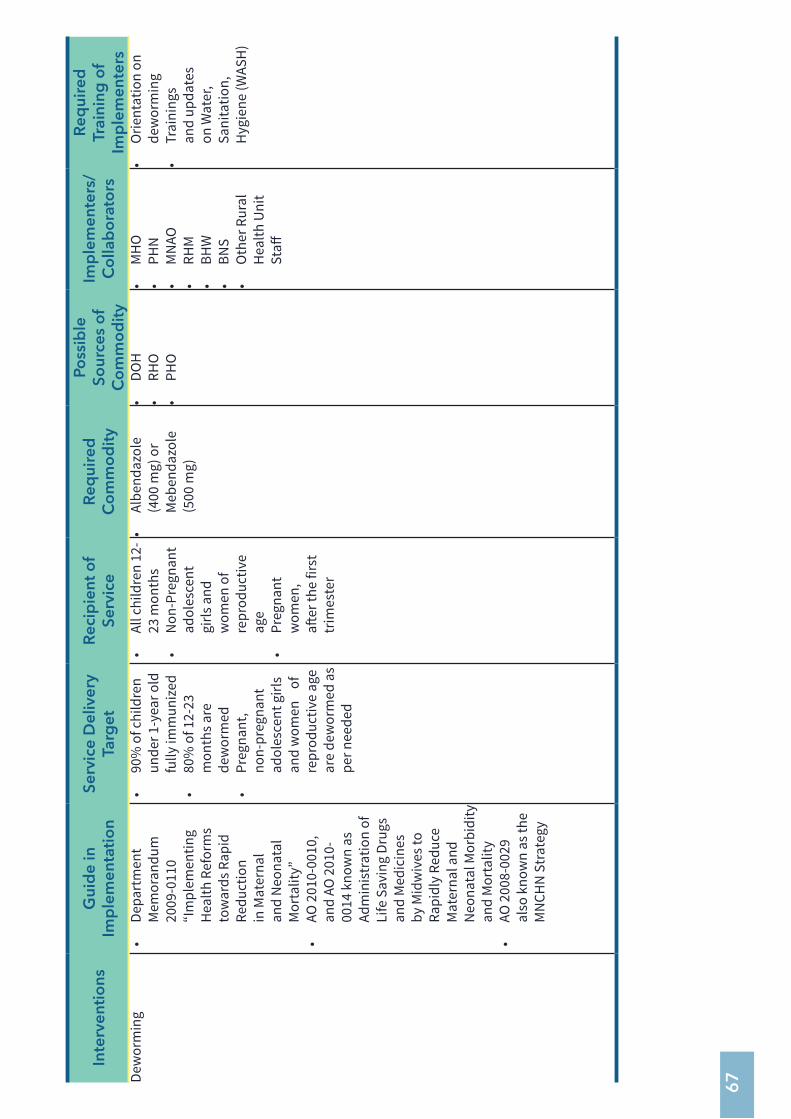
67
Inte
rven
tio
nsG
uid
e in
Im
ple
men
tati
on
Serv
ice
Del
iver
y Ta
rget
Rec
ipie
nt o
f Se
rvic
eR
equi
red
C
om
mo
dit
y
Poss
ible
So
urce
s o
f C
om
mo
dit
y
Imp
lem
ente
rs/
Co
llab
ora
tors
Req
uire
d
Trai
ning
of
Imp
lem
ente
rsDe
wor
min
g•
Depa
rtm
ent
Mem
oran
dum
20
09-0
110
“Im
plem
entin
g H
ealth
Ref
orm
s to
war
ds R
apid
Re
duct
ion
in M
ater
nal
and
Neo
nata
l M
orta
lity”
• AO
201
0-00
10,
and
AO 2
010-
0014
kno
wn
as
Adm
inis
trat
ion
of
Life
Sav
ing
Drug
s an
d M
edic
ines
by
Mid
wiv
es to
Ra
pidl
y Re
duce
M
ater
nal a
nd
Neo
nata
l Mor
bidi
ty
and
Mor
talit
y•
AO 2
008-
0029
al
so k
now
n as
the
MN
CHN
Str
ateg
y
• 90
% o
f chi
ldre
n un
der 1
-yea
r old
fu
lly im
mun
ized
• 80
% o
f 12-
23
mon
ths a
re
dew
orm
ed•
Preg
nant
, no
n-pr
egna
nt
adol
esce
nt g
irls
and
wom
en
of
repr
oduc
tive
age
are
dew
orm
ed a
s pe
r nee
ded
• Al
l chi
ldre
n 12
-23
mon
ths
• N
on-P
regn
ant
adol
esce
nt
girls
and
w
omen
of
repr
oduc
tive
age
• Pr
egna
nt
wom
en,
after
the
first
tr
imes
ter
• Al
bend
azol
e (4
00 m
g) o
r M
eben
dazo
le
(500
mg)
• DO
H•
RHO
• PH
O
• M
HO
• PH
N•
MN
AO•
RHM
• BH
W•
BNS
• O
ther
Rur
al
Hea
lth U
nit
Staff
• O
rient
atio
n on
de
wor
min
g•
Trai
ning
s an
d up
date
s on
Wat
er,
Sani
tatio
n,
Hyg
iene
(WAS
H)
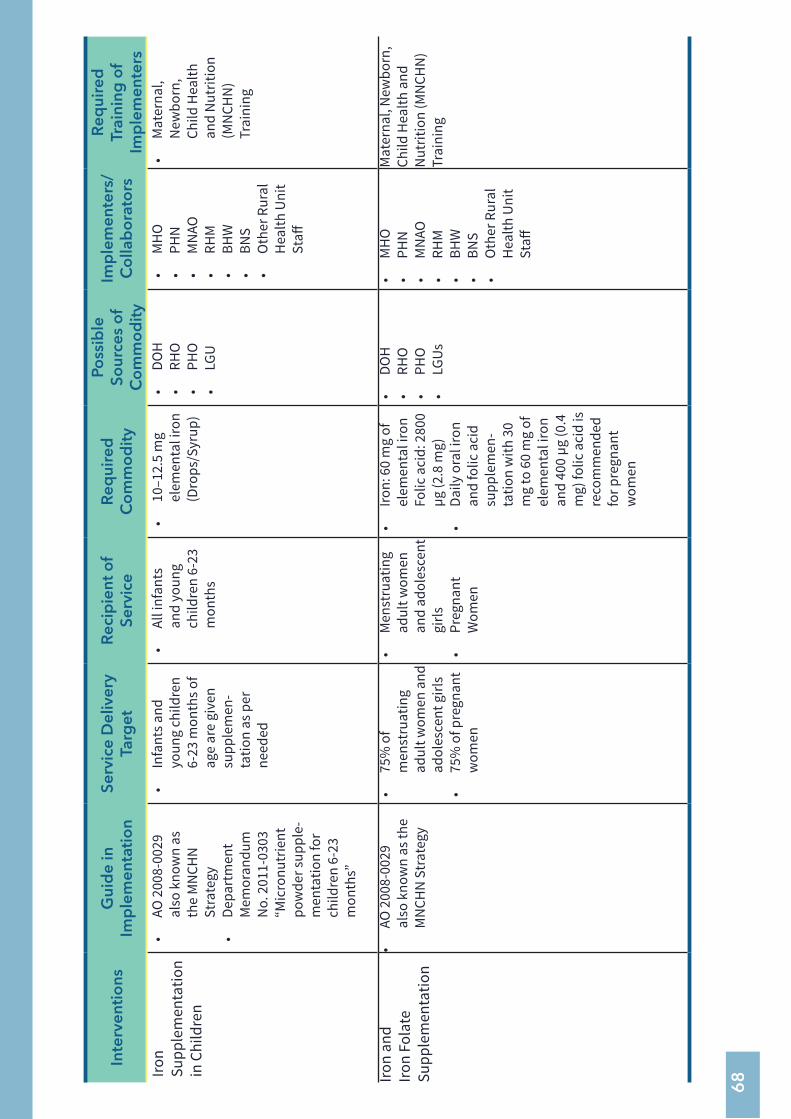
68
Inte
rven
tio
nsG
uid
e in
Im
ple
men
tati
on
Serv
ice
Del
iver
y Ta
rget
Rec
ipie
nt o
f Se
rvic
eR
equi
red
C
om
mo
dit
y
Poss
ible
So
urce
s o
f C
om
mo
dit
y
Imp
lem
ente
rs/
Co
llab
ora
tors
Req
uire
d
Trai
ning
of
Imp
lem
ente
rsIro
n Su
pple
men
tatio
n in
Chi
ldre
n
• AO
200
8-00
29
also
kno
wn
as
the
MN
CHN
St
rate
gy•
Depa
rtm
ent
Mem
oran
dum
N
o. 2
011-
0303
“M
icro
nutr
ient
po
wde
r sup
ple-
men
tatio
n fo
r ch
ildre
n 6-
23
mon
ths”
• In
fant
s and
yo
ung
child
ren
6-23
mon
ths o
f ag
e ar
e gi
ven
supp
lem
en-
tatio
n as
per
ne
eded
• Al
l inf
ants
an
d yo
ung
child
ren
6-23
m
onth
s
• 10
–12.
5 m
g el
emen
tal i
ron
(Dro
ps/S
yrup
)
• DO
H•
RHO
• PH
O•
LGU
• M
HO
• PH
N•
MN
AO•
RHM
• BH
W•
BNS
• O
ther
Rur
al
Hea
lth U
nit
Staff
• M
ater
nal,
New
born
, Ch
ild H
ealth
an
d N
utrit
ion
(MN
CHN
) Tr
aini
ng
Iron
and
Iron
Fola
te
Supp
lem
enta
tion
• AO
200
8-00
29
also
kno
wn
as th
e M
NCH
N S
trat
egy
• 75
% o
f m
enst
ruat
ing
adul
t wom
en a
nd
adol
esce
nt g
irls
• 75
% o
f pre
gnan
t w
omen
• M
enst
ruat
ing
adul
t wom
en
and
adol
esce
nt
girls
•
Preg
nant
W
omen
• Iro
n: 6
0 m
g of
el
emen
tal i
ron
Folic
aci
d: 2
800
µg (2
.8 m
g)•
Daily
ora
l iro
n an
d fo
lic a
cid
supp
lem
en-
tatio
n w
ith 3
0 m
g to
60
mg
of
elem
enta
l iro
n an
d 40
0 µg
(0.4
m
g) fo
lic a
cid
is
reco
mm
ende
d fo
r pre
gnan
t w
omen
• DO
H•
RHO
• PH
O•
LGUs
• M
HO
• PH
N•
MN
AO•
RHM
• BH
W•
BNS
• O
ther
Rur
al
Hea
lth U
nit
Staff
Mat
erna
l, N
ewbo
rn,
Child
Hea
lth a
nd
Nut
ritio
n (M
NCH
N)
Trai
ning
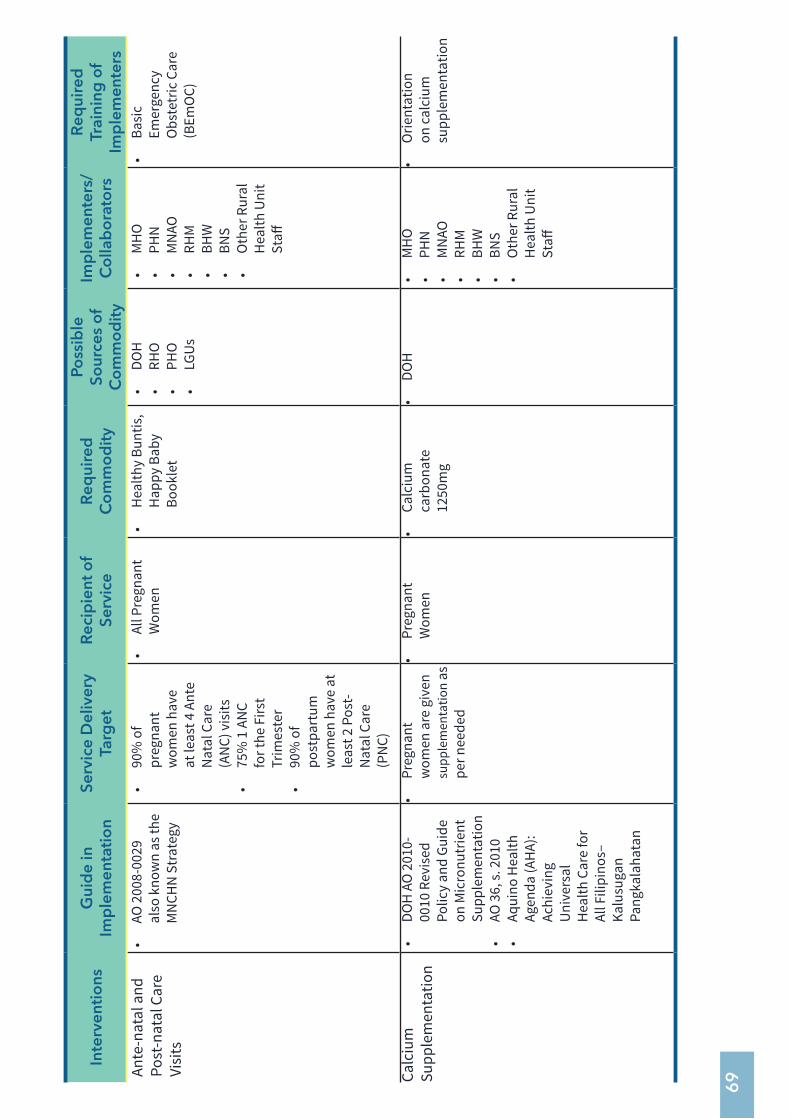
69
Inte
rven
tio
nsG
uid
e in
Im
ple
men
tati
on
Serv
ice
Del
iver
y Ta
rget
Rec
ipie
nt o
f Se
rvic
eR
equi
red
C
om
mo
dit
y
Poss
ible
So
urce
s o
f C
om
mo
dit
y
Imp
lem
ente
rs/
Co
llab
ora
tors
Req
uire
d
Trai
ning
of
Imp
lem
ente
rsAn
te-n
atal
and
Po
st-n
atal
Car
e Vi
sits
• AO
200
8-00
29
also
kno
wn
as th
e M
NCH
N S
trat
egy
• 90
% o
f pr
egna
nt
wom
en h
ave
at le
ast 4
Ant
e N
atal
Car
e (A
NC)
vis
its•
75%
1 A
NC
for t
he F
irst
Trim
este
r•
90%
of
post
part
um
wom
en h
ave
at
leas
t 2 P
ost-
Nat
al C
are
(PN
C)
• Al
l Pre
gnan
t W
omen
• H
ealth
y Bu
ntis
, H
appy
Bab
y Bo
okle
t
• DO
H•
RHO
• PH
O•
LGUs
• M
HO
• PH
N•
MN
AO•
RHM
• BH
W•
BNS
• O
ther
Rur
al
Hea
lth U
nit
Staff
• Ba
sic
Emer
genc
y O
bste
tric
Car
e (B
EmO
C)
Calc
ium
Su
pple
men
tatio
n•
DOH
AO
201
0-00
10 R
evis
ed
Polic
y an
d Gu
ide
on M
icro
nutr
ient
Su
pple
men
tatio
n•
AO 3
6, s.
201
0•
Aqui
no H
ealth
Ag
enda
(AH
A):
Achi
evin
g U
nive
rsal
H
ealth
Car
e fo
r Al
l Fili
pino
s–
Kalu
suga
n Pa
ngka
laha
tan
• Pr
egna
nt
wom
en a
re g
iven
su
pple
men
tatio
n as
pe
r nee
ded
• Pr
egna
nt
Wom
en•
Calc
ium
ca
rbon
ate
1250
mg
• DO
H•
MH
O•
PHN
• M
NAO
• RH
M•
BHW
• BN
S•
Oth
er R
ural
H
ealth
Uni
t St
aff
• O
rient
atio
n on
cal
cium
su
pple
men
tatio
n
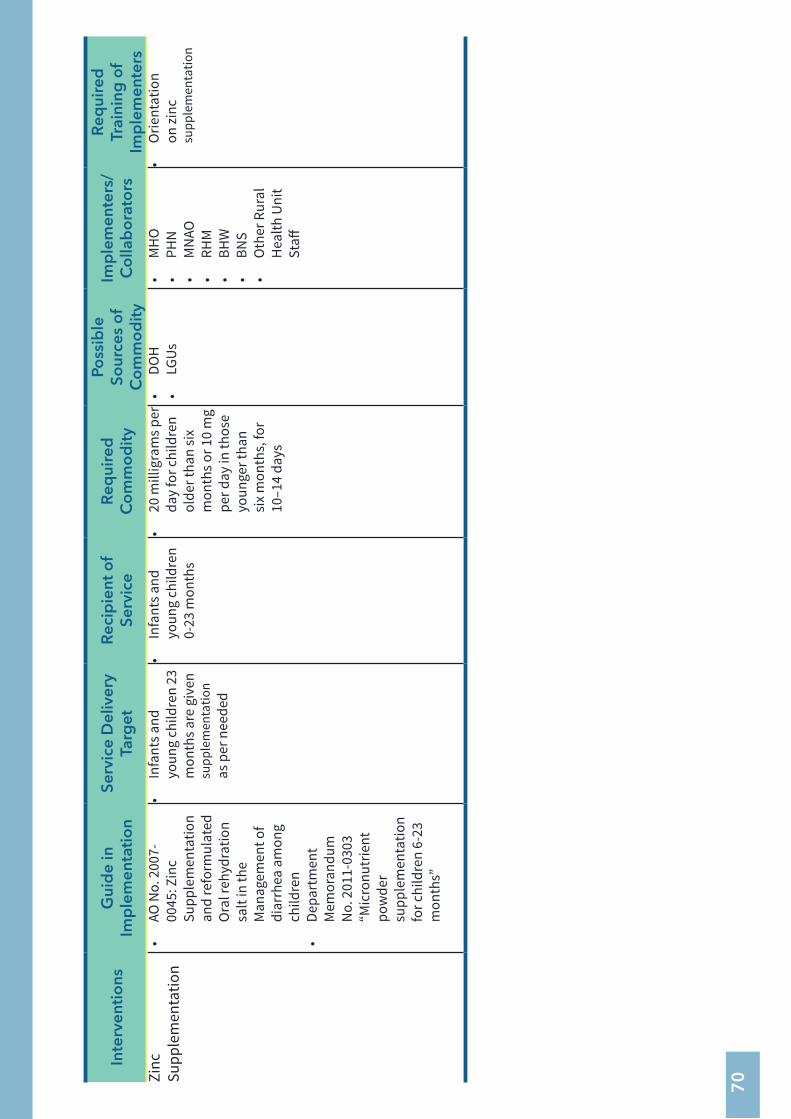
70
Inte
rven
tio
nsG
uid
e in
Im
ple
men
tati
on
Serv
ice
Del
iver
y Ta
rget
Rec
ipie
nt o
f Se
rvic
eR
equi
red
C
om
mo
dit
y
Poss
ible
So
urce
s o
f C
om
mo
dit
y
Imp
lem
ente
rs/
Co
llab
ora
tors
Req
uire
d
Trai
ning
of
Imp
lem
ente
rsZi
nc
Supp
lem
enta
tion
• AO
No.
200
7-00
45: Z
inc
Supp
lem
enta
tion
and
refo
rmul
ated
O
ral r
ehyd
ratio
n sa
lt in
the
Man
agem
ent o
f di
arrh
ea a
mon
g ch
ildre
n•
Depa
rtm
ent
Mem
oran
dum
N
o. 2
011-
0303
“M
icro
nutr
ient
po
wde
r su
pple
men
tatio
n fo
r chi
ldre
n 6-
23
mon
ths”
• In
fant
s and
yo
ung
child
ren
23
mon
ths a
re g
iven
su
pple
men
tatio
n
as
per
nee
ded
• In
fant
s and
yo
ung
child
ren
0-23
mon
ths
• 20
mill
igra
ms p
er
day
for c
hild
ren
olde
r tha
n si
x m
onth
s or 1
0 m
g pe
r day
in th
ose
youn
ger t
han
six
mon
ths,
for
10–1
4 da
ys
• DO
H•
LGUs
• M
HO
• PH
N•
MN
AO•
RHM
• BH
W•
BNS
• O
ther
Rur
al
Hea
lth U
nit
Staff
• O
rient
atio
n on
zinc
su
pple
men
tatio
n
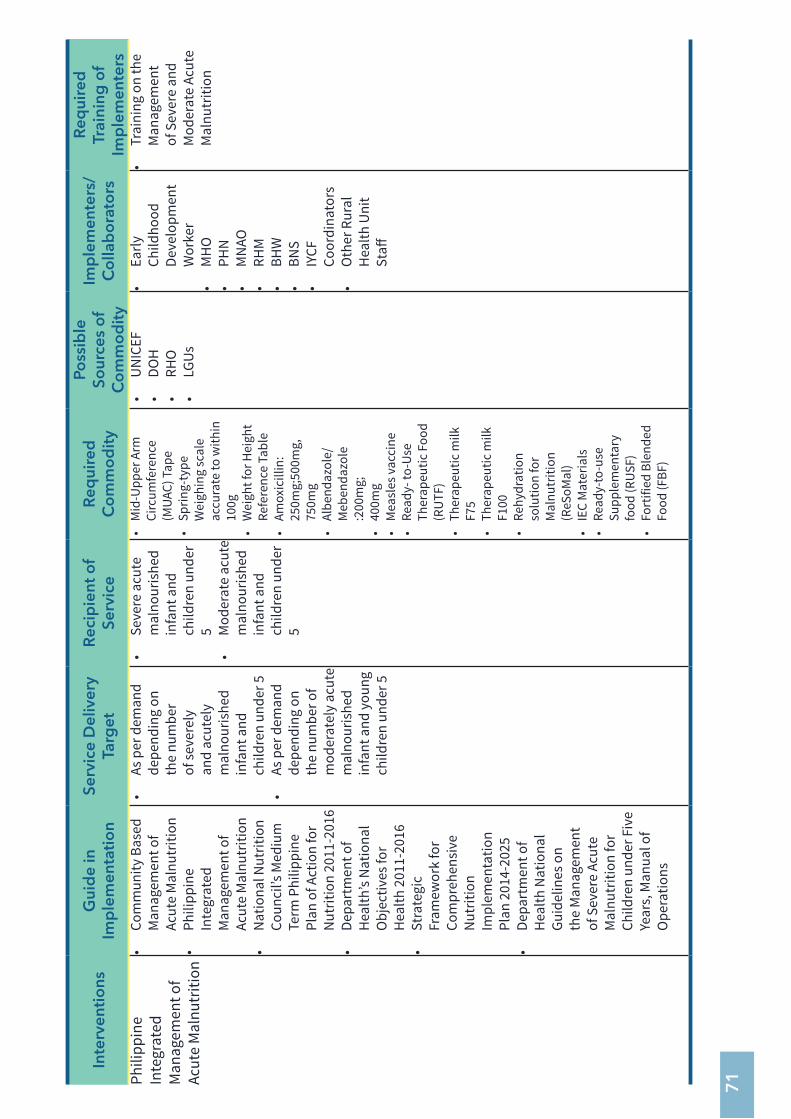
71
Inte
rven
tio
nsG
uid
e in
Im
ple
men
tati
on
Serv
ice
Del
iver
y Ta
rget
Rec
ipie
nt o
f Se
rvic
eR
equi
red
C
om
mo
dit
y
Poss
ible
So
urce
s o
f C
om
mo
dit
y
Imp
lem
ente
rs/
Co
llab
ora
tors
Req
uire
d
Trai
ning
of
Imp
lem
ente
rsPh
ilipp
ine
Inte
grat
ed
Man
agem
ent o
f Ac
ute
Mal
nutr
ition
• Co
mm
unity
Bas
ed
Man
agem
ent o
f Ac
ute
Mal
nutr
ition
• Ph
ilipp
ine
Inte
grat
ed
Man
agem
ent o
f Ac
ute
Mal
nutr
ition
• N
atio
nal N
utrit
ion
Coun
cil’s
Med
ium
Te
rm P
hilip
pine
Pl
an o
f Act
ion
for
Nut
ritio
n 20
11-2
016
• De
part
men
t of
Hea
lth’s
Nat
iona
l O
bjec
tives
for
Hea
lth 2
011-
2016
• St
rate
gic
Fram
ewor
k fo
r Co
mpr
ehen
sive
N
utrit
ion
Impl
emen
tatio
n Pl
an 2
014-
2025
• De
part
men
t of
Hea
lth N
atio
nal
Guid
elin
es o
n th
e M
anag
emen
t of
Sev
ere
Acut
e M
alnu
triti
on fo
r Ch
ildre
n un
der F
ive
Year
s, M
anua
l of
Ope
ratio
ns
• As
per
dem
and
depe
ndin
g on
th
e nu
mbe
r of
seve
rely
an
d ac
utel
y m
alno
uris
hed
infa
nt a
nd
child
ren
unde
r 5•
As p
er d
eman
d de
pend
ing
on
the
num
ber o
f m
oder
atel
y ac
ute
mal
nour
ishe
d in
fant
and
you
ng
child
ren
unde
r 5
• Se
vere
acu
te
mal
nour
ishe
d in
fant
and
ch
ildre
n un
der
5•
Mod
erat
e ac
ute
mal
nour
ishe
d in
fant
and
ch
ildre
n un
der
5
• M
id-U
pper
Arm
Ci
rcum
fere
nce
(MUA
C) T
ape
• Sp
ring-
type
W
eigh
ing
scal
e ac
cura
te to
with
in
100g
• W
eigh
t for
Hei
ght
Refe
renc
e Ta
ble
• Am
oxic
illin
: 25
0mg;
500m
g,
750m
g•
Albe
ndaz
ole/
Meb
enda
zole
:2
00m
g;•
400m
g•
Mea
sles
vac
cine
• Re
ady-
to-U
se
Ther
apeu
tic F
ood
(RU
TF)
• Th
erap
eutic
milk
F7
5•
Ther
apeu
tic m
ilk
F100
• Re
hydr
atio
n so
lutio
n fo
r M
alnu
triti
on
(ReS
oMal
)•
IEC
Mat
eria
ls•
Read
y-to
-use
Su
pple
men
tary
fo
od (R
USF)
• Fo
rtifi
ed B
lend
ed
Food
(FBF
)
• U
NIC
EF•
DOH
• RH
O•
LGUs
• Ea
rly
Child
hood
De
velo
pmen
t W
orke
r•
MH
O•
PHN
• M
NAO
• RH
M•
BHW
• BN
S•
IYCF
Co
ordi
nato
rs•
Oth
er R
ural
H
ealth
Uni
t St
aff
• Tr
aini
ng o
n th
e M
anag
emen
t of
Sev
ere
and
Mod
erat
e Ac
ute
Mal
nutr
ition
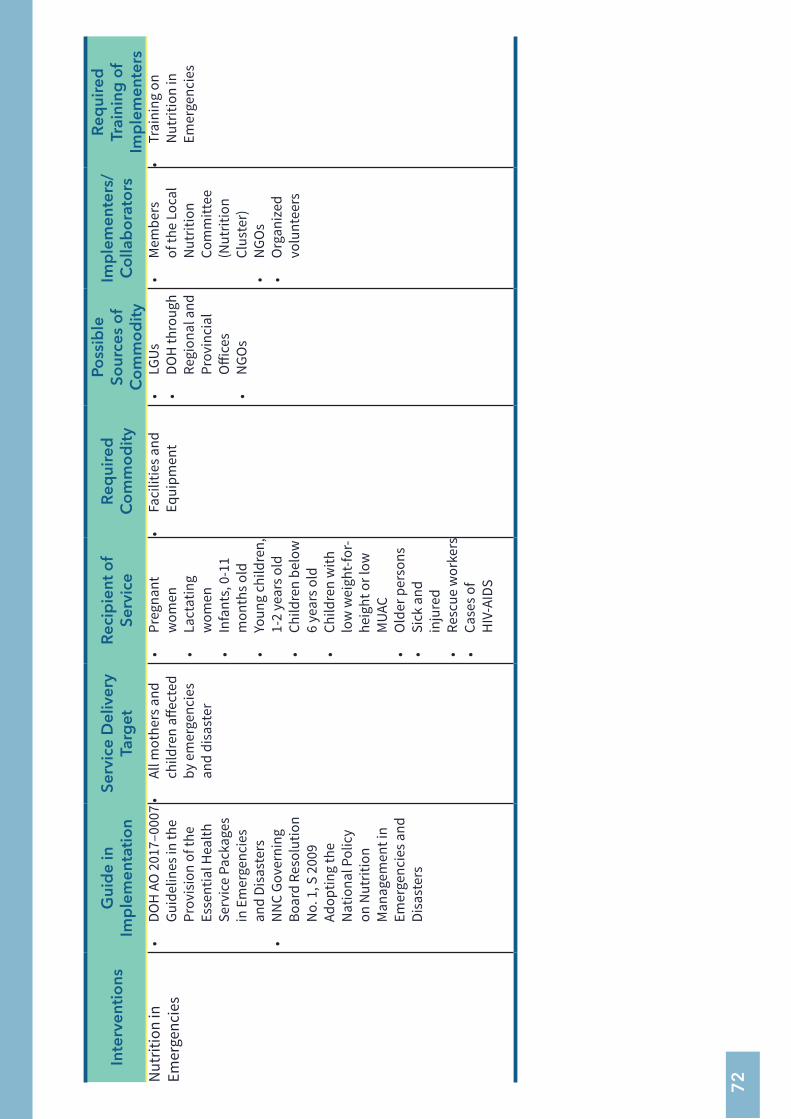
72
Inte
rven
tio
nsG
uid
e in
Im
ple
men
tati
on
Serv
ice
Del
iver
y Ta
rget
Rec
ipie
nt o
f Se
rvic
eR
equi
red
C
om
mo
dit
y
Poss
ible
So
urce
s o
f C
om
mo
dit
y
Imp
lem
ente
rs/
Co
llab
ora
tors
Req
uire
d
Trai
ning
of
Imp
lem
ente
rsN
utrit
ion
in
Emer
genc
ies
• DO
H A
O 2
017–
0007
Gu
idel
ines
in th
e Pr
ovis
ion
of th
e Es
sent
ial H
ealth
Se
rvic
e Pa
ckag
es
in E
mer
genc
ies
and
Disa
ster
s•
NN
C Go
vern
ing
Boar
d Re
solu
tion
No.
1, S
200
9 Ad
optin
g th
e N
atio
nal P
olic
y on
Nut
ritio
n M
anag
emen
t in
Emer
genc
ies a
nd
Disa
ster
s
• Al
l mot
hers
and
ch
ildre
n aff
ecte
d by
em
erge
ncie
s an
d di
sast
er
• Pr
egna
nt
wom
en•
Lact
atin
g w
omen
• In
fant
s, 0
-11
mon
ths o
ld•
Youn
g ch
ildre
n,
1-2
year
s old
• Ch
ildre
n be
low
6
year
s old
• Ch
ildre
n w
ith
low
wei
ght-f
or-
heig
ht o
r low
M
UAC
• O
lder
per
sons
• Si
ck a
nd
inju
red
• Re
scue
wor
kers
• Ca
ses o
f H
IV-A
IDS
• Fa
cilit
ies a
nd
Equi
pmen
t•
LGUs
• DO
H th
roug
h Re
gion
al a
nd
Prov
inci
al
Offi
ces
• N
GOs
• M
embe
rs
of th
e Lo
cal
Nut
ritio
n Co
mm
ittee
(N
utrit
ion
Clus
ter)
• N
GOs
• O
rgan
ized
vo
lunt
eers
• Tr
aini
ng o
n N
utrit
ion
in
Emer
genc
ies
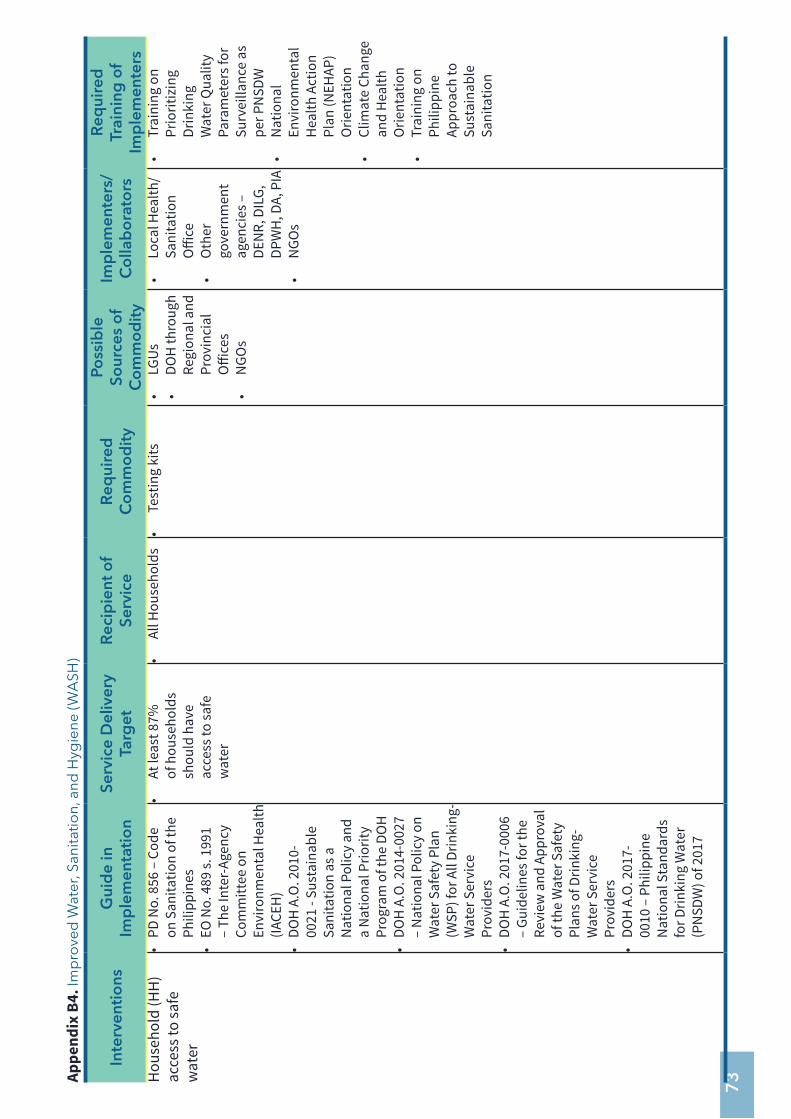
73Ap
pend
ix B
4. Im
pro
ved
Wat
er, S
anita
tion,
and
Hyg
iene
(WA
SH)
Inte
rven
tio
nsG
uid
e in
Im
ple
men
tati
on
Serv
ice
Del
iver
y Ta
rget
Rec
ipie
nt o
f Se
rvic
eR
equi
red
C
om
mo
dit
y
Poss
ible
So
urce
s o
f C
om
mo
dit
y
Imp
lem
ente
rs/
Co
llab
ora
tors
Req
uire
d
Trai
ning
of
Imp
lem
ente
rsH
ouse
hold
(HH
) ac
cess
to sa
fe
wat
er
• PD
No.
856
– C
ode
on S
anita
tion
of th
e Ph
ilipp
ines
• EO
No.
489
s. 1
991
– Th
e In
ter-A
genc
y Co
mm
ittee
on
Envi
ronm
enta
l Hea
lth
(IACE
H)
• DO
H A
.O. 2
010-
0021
- Su
stai
nabl
e Sa
nita
tion
as a
N
atio
nal P
olic
y an
d a
Nat
iona
l Prio
rity
Prog
ram
of t
he D
OH
• DO
H A
.O. 2
014-
0027
–
Nat
iona
l Pol
icy
on
Wat
er S
afet
y Pl
an
(WSP
) for
All
Drin
king
-W
ater
Ser
vice
Pr
ovid
ers
• DO
H A
.O. 2
017-
0006
–
Guid
elin
es fo
r the
Re
view
and
App
rova
l of
the
Wat
er S
afet
y Pl
ans o
f Drin
king
-W
ater
Ser
vice
Pr
ovid
ers
• DO
H A
.O. 2
017-
0010
– P
hilip
pine
N
atio
nal S
tand
ards
fo
r Drin
king
Wat
er
(PN
SDW
) of 2
017
• At
leas
t 87%
of
hou
seho
lds
shou
ld h
ave
acce
ss to
safe
w
ater
• Al
l Hou
seho
lds
• Te
stin
g ki
ts•
LGUs
• DO
H th
roug
h Re
gion
al a
nd
Prov
inci
al
Offi
ces
• N
GOs
• Lo
cal H
ealth
/ Sa
nita
tion
Offi
ce•
Oth
er
gove
rnm
ent
agen
cies
–
DEN
R, D
ILG,
DP
WH
, DA,
PIA
• N
GOs
• Tr
aini
ng o
n Pr
iorit
izin
g Dr
inki
ng
Wat
er Q
ualit
y Pa
ram
eter
s for
Su
rvei
llanc
e as
pe
r PN
SDW
• N
atio
nal
Envi
ronm
enta
l H
ealth
Act
ion
Plan
(NEH
AP)
Orie
ntat
ion
• Cl
imat
e Ch
ange
an
d H
ealth
O
rient
atio
n•
Trai
ning
on
Phili
ppin
e Ap
proa
ch to
Su
stai
nabl
e Sa
nita
tion
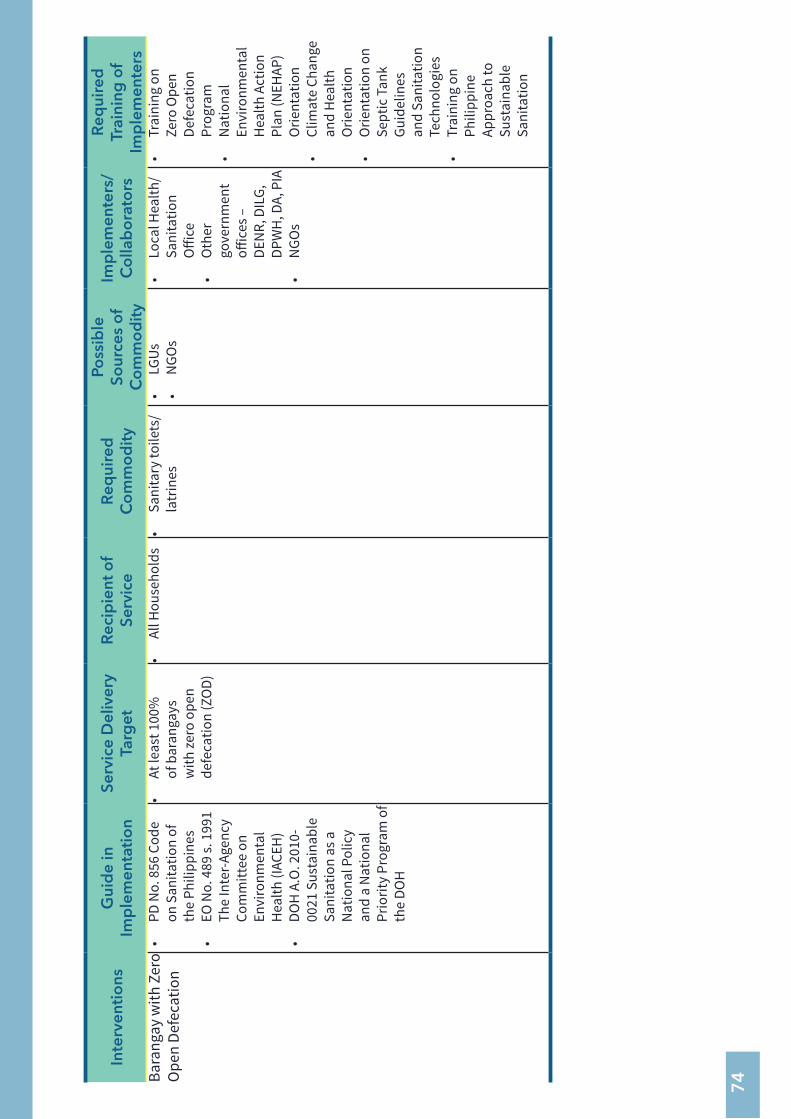
74
Inte
rven
tio
nsG
uid
e in
Im
ple
men
tati
on
Serv
ice
Del
iver
y Ta
rget
Rec
ipie
nt o
f Se
rvic
eR
equi
red
C
om
mo
dit
y
Poss
ible
So
urce
s o
f C
om
mo
dit
y
Imp
lem
ente
rs/
Co
llab
ora
tors
Req
uire
d
Trai
ning
of
Imp
lem
ente
rsBa
rang
ay w
ith Z
ero
Ope
n De
feca
tion
• PD
No.
856
Cod
e on
San
itatio
n of
th
e Ph
ilipp
ines
• EO
No.
489
s. 1
991
The
Inte
r-Age
ncy
Com
mitt
ee o
n En
viro
nmen
tal
Hea
lth (I
ACEH
)•
DOH
A.O
. 201
0-00
21 S
usta
inab
le
Sani
tatio
n as
a
Nat
iona
l Pol
icy
and
a N
atio
nal
Prio
rity
Prog
ram
of
the
DOH
• At
leas
t 100
%
of b
aran
gays
w
ith ze
ro o
pen
defe
catio
n (Z
OD)
• Al
l Hou
seho
lds
• Sa
nita
ry to
ilets
/ la
trin
es•
LGUs
• N
GOs
• Lo
cal H
ealth
/ Sa
nita
tion
Offi
ce•
Oth
er
gove
rnm
ent
offic
es –
DE
NR,
DIL
G,
DPW
H, D
A, P
IA•
NGO
s
• Tr
aini
ng o
n Ze
ro O
pen
Defe
catio
n Pr
ogra
m•
Nat
iona
l En
viro
nmen
tal
Hea
lth A
ctio
n Pl
an (N
EHAP
) O
rient
atio
n•
Clim
ate
Chan
ge
and
Hea
lth
Orie
ntat
ion
• O
rient
atio
n on
Se
ptic
Tan
k Gu
idel
ines
an
d Sa
nita
tion
Tech
nolo
gies
• Tr
aini
ng o
n Ph
ilipp
ine
Appr
oach
to
Sust
aina
ble
Sani
tatio
n
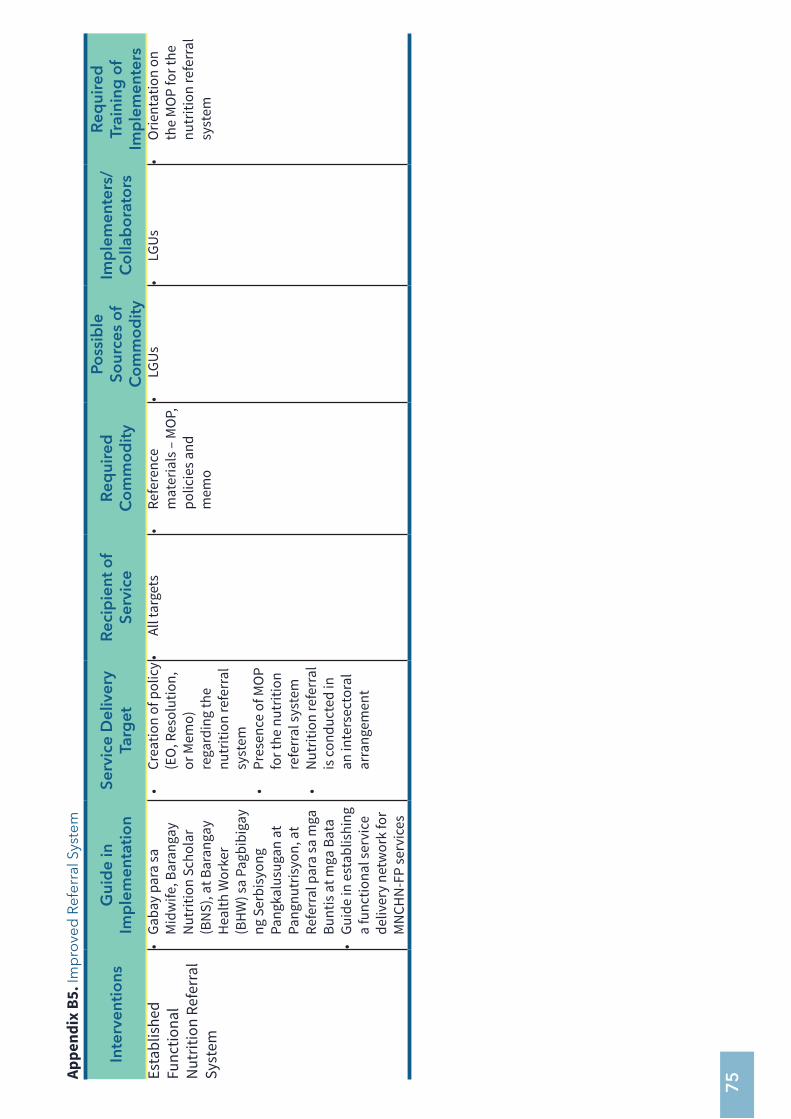
75Ap
pend
ix B
5. Im
pro
ved
Ref
erra
l Sys
tem
Inte
rven
tio
nsG
uid
e in
Im
ple
men
tati
on
Serv
ice
Del
iver
y Ta
rget
Rec
ipie
nt o
f Se
rvic
eR
equi
red
C
om
mo
dit
y
Poss
ible
So
urce
s o
f C
om
mo
dit
y
Imp
lem
ente
rs/
Co
llab
ora
tors
Req
uire
d
Trai
ning
of
Imp
lem
ente
rsEs
tabl
ishe
d Fu
nctio
nal
Nut
ritio
n Re
ferr
al
Syst
em
• Ga
bay
para
sa
Mid
wife
, Bar
anga
y N
utrit
ion
Scho
lar
(BN
S), a
t Bar
anga
y H
ealth
Wor
ker
(BH
W) s
a Pa
gbib
igay
ng
Ser
bisy
ong
Pang
kalu
suga
n at
Pa
ngnu
tris
yon,
at
Refe
rral
par
a sa
mga
Bu
ntis
at m
ga B
ata
• Gu
ide
in e
stab
lishi
ng
a fu
nctio
nal s
ervi
ce
deliv
ery
netw
ork
for
MN
CHN
-FP
serv
ices
• Cr
eatio
n of
pol
icy
(EO
, Res
olut
ion,
or
Mem
o)
rega
rdin
g th
e nu
triti
on re
ferr
al
syst
em•
Pres
ence
of M
OP
for t
he n
utrit
ion
refe
rral
syst
em•
Nut
ritio
n re
ferr
al
is co
nduc
ted
in
an in
ters
ecto
ral
arra
ngem
ent
• Al
l tar
gets
• Re
fere
nce
mat
eria
ls –
MO
P,
polic
ies a
nd
mem
o
• LG
Us•
LGUs
• O
rient
atio
n on
th
e M
OP
for t
he
nutr
ition
refe
rral
sy
stem
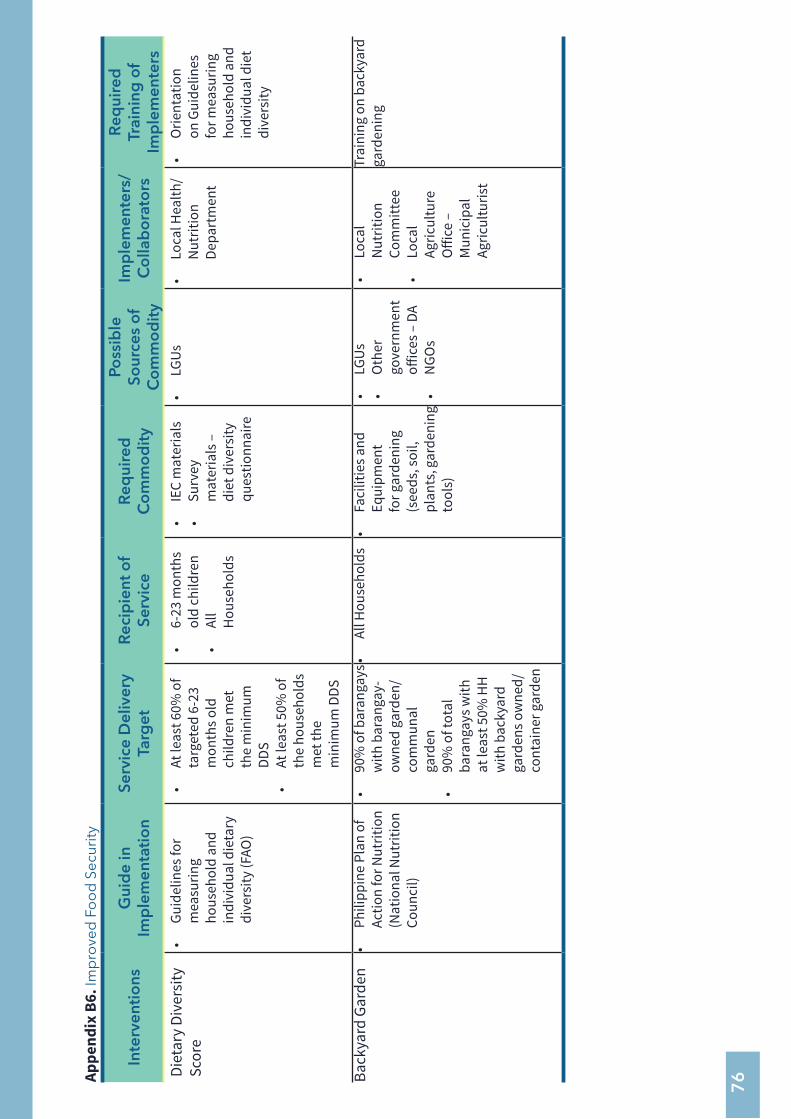
76Ap
pend
ix B
6. Im
pro
ved
Fo
od
Sec
urity
Inte
rven
tio
nsG
uid
e in
Im
ple
men
tati
on
Serv
ice
Del
iver
y Ta
rget
Rec
ipie
nt o
f Se
rvic
eR
equi
red
C
om
mo
dit
y
Poss
ible
So
urce
s o
f C
om
mo
dit
y
Imp
lem
ente
rs/
Co
llab
ora
tors
Req
uire
d
Trai
ning
of
Imp
lem
ente
rsDi
etar
y Di
vers
ity
Scor
e•
Guid
elin
es fo
r m
easu
ring
hous
ehol
d an
d in
divi
dual
die
tary
di
vers
ity (F
AO)
• At
leas
t 60%
of
targ
eted
6-2
3 m
onth
s old
ch
ildre
n m
et
the
min
imum
DD
S•
At le
ast 5
0% o
f th
e ho
useh
olds
m
et th
e m
inim
um D
DS
• 6-
23 m
onth
s ol
d ch
ildre
n•
All
Hou
seho
lds
• IE
C m
ater
ials
• Su
rvey
m
ater
ials
–
diet
div
ersi
ty
ques
tionn
aire
• LG
Us•
Loca
l Hea
lth/
Nut
ritio
n De
part
men
t
• O
rient
atio
n on
Gui
delin
es
for m
easu
ring
hous
ehol
d an
d in
divi
dual
die
t di
vers
ity
Back
yard
Gar
den
• Ph
ilipp
ine
Plan
of
Actio
n fo
r Nut
ritio
n (N
atio
nal N
utrit
ion
Coun
cil)
• 90
% o
f bar
anga
ys
with
bar
anga
y-ow
ned
gard
en/
com
mun
al
gard
en•
90%
of t
otal
ba
rang
ays w
ith
at le
ast 5
0% H
H
with
bac
kyar
d ga
rden
s ow
ned/
co
ntai
ner g
arde
n
• Al
l Hou
seho
lds
• Fa
cilit
ies a
nd
Equi
pmen
t fo
r gar
deni
ng
(see
ds, s
oil,
plan
ts, g
arde
ning
to
ols)
• LG
Us•
Oth
er
gove
rnm
ent
offic
es –
DA
• N
GOs
• Lo
cal
Nut
ritio
n Co
mm
ittee
• Lo
cal
Agric
ultu
re
Offi
ce –
M
unic
ipal
Ag
ricul
turis
t
Trai
ning
on
back
yard
ga
rden
ing













![ICDS Systems Strengthening & Nutrition Improvement Project … · 2016-07-11 · ICDS Systems Strengthening & Nutrition Improvement Project (ISSNIP) [Credit 5150-IN] Public Disclosure](https://img.pdfslide.us/doc/110x75/5e99ba8c90eddc2d407e9766/icds-systems-strengthening-nutrition-improvement-project-2016-07-11-icds.jpg)