Embed Size (px)
Citation preview
Straumann® Emdogain
May 25, 2011
STRAUMANN®
All trademarks from Straumann mentioned herein are the trademarks of Straumann Holding AG and/or its affiliates.
2
Please note that this Straumann® Scientific Evidence Presentation File (“File”) contains a selection of studies and makes no claim to be a complete study list. Articles were selected on merit from the results of a literature search.
By using this File, in whole or in part, the customer who has received the File from Institut Straumann AG (“User”), implicitly agrees to the following terms and conditions (“Terms and Conditions”):
1. The studies contained in this File were made by independent researchers. Whenever the User uses information from this File, the User shall cite the references in a clear and appropriate manner. Furthermore, the User shall comply with all applicable laws and regulations.
2. The User is allowed to use the File for the sole and limited purpose of holding presentations (“Presentation”) to inform the public of new data, findings, results, studies predominantly on Straumann® Emdogain or other Straumann products (“Straumann Products”).
3. The User shall not use the File for any purpose other than the Presentation, and the User agrees that any such use shall be consistent with all applicable laws and regulations and highest professional standards.
4. The User represents and warrants that to the best of his/her knowledge the content of the Presentation is true and correct and does not include any illegal, unethical or offensive contents and that all statements made in the Presentation are within indications of the Straumann Products (refer to Instructions for Use) and the User shall refrain from promoting any off-label use.
5. The User may take separate slides from this File, but shall not alter the content of a slide.
6. The User agrees that Institut Straumann AG shall have the right to terminate this agreement (Terms and Conditions) at any time upon five (5) days written notice, for any reason or no reason whatsoever, and the User agrees that upon receiving such notice, he/she shall cease the distribution of and destroy any materials containing information from this File.
7. While Institut Straumann AG is making great efforts to include accurate and up-to-date information in the File, Institut Sraumann AG makes no representations or warranties, express or implied, as to the accuracy or completeness of the information provided in this File. Institut Straumann AG and its affiliates and subsidiaries disclaim any liability for the use of the File and shall not be liable in any manner for any direct, incidental, consequential, indirect or punitive damages arising out of the use of the File or any errors or omissions in the content thereof. The User agrees that he/she shall not be entitled to recover any costs, fees, damages, or other sums from Institut Straumann AG and / or its affiliates and / or subsidiaries for any claim relating to or arising out of the permission granted in these Terms and Conditions.
8. The User agrees that he/she will not permit the use of the File, in full or in part, by any third party without the prior written consent of Institut Straumann AG, and that doing so will be deemed a violation of these Terms and Conditions.
9. The User is not permitted to assign the rights and obligations under these Terms and Conditions to any other party without the prior written consent of Institut Straumann AG.
Terms and Conditions of Institut Straumann AG regarding the use of the presentations contained in this Emdogain Scientific Evidence Presentation File
Straumann®
Emdogain
Recession Defects Intrabony DefectsFurcation DefectsLong-term Data
Recession defectsMay 25, 2011
Straumann® Emdogain
STRAUMANN® 5Miller PD Jr.Int J Periodontics Restorative Dent. 1985;5(2):8-13.A classification of marginal tissue recession
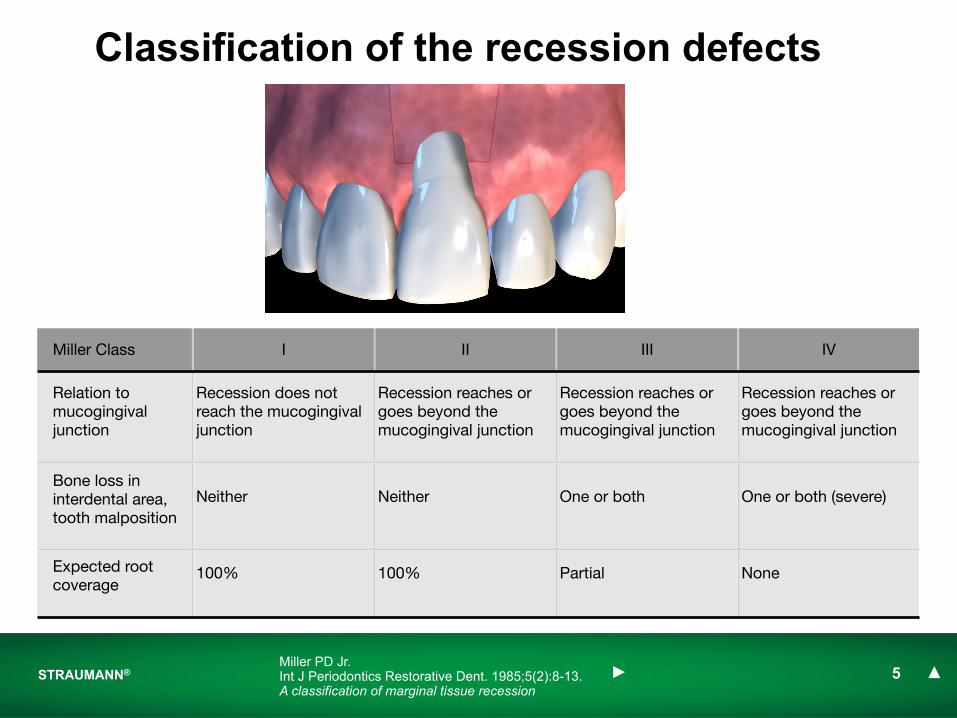
Classification of the recession defects
Miller Class I II III IV
Relation to mucogingival junction
Recession does not reach the mucogingival junction
Recession reaches or goes beyond the mucogingival junction
Recession reaches or goes beyond the mucogingival junction
Recession reaches or goes beyond the mucogingival junction
Bone loss in interdental area, tooth malposition
Neither Neither One or both One or both (severe)
Expected root coverage
100% 100% Partial None

STRAUMANN® 6
Straumann® EmdogainPublication First AuthorFirst Author Full Author List Full Title Reference
1 McGuire MK McGuire MK, Nunn M.Evaluation of human recession defects treated with coronally advanced flaps and either enamel matrix derivative or connective tissue. Part 1: Comparison of clinical parameters
J Periodontol. 2003 Aug;74(8):1110-25.
2 Cueva MACueva MA, Boltchi FE, Hallmon WW, Nunn ME, Rivera-Hidalgo F, Rees T.
A comparative study of coronally advanced flaps with and without the addition of enamel matrix derivative in the treatment of marginal tissue recession
J Periodontol. 2004 Jul;75(7):949-56.
3 Spahr A
Spahr A, Haegewald S, Tsoulfidou F, Rompola E, Heijl L, Bernimoulin JP, Ring C, Sander S, Haller B.
Coverage of Miller class I and II recession defects using enamel matrix proteins versus coronally advanced flap technique: a 2-year report.
J Periodontol. 2005 Nov;76(11):1871-80.
4 Castellanos A Castellanos A, de la Rosa M, de la Garza M, Caffesse RG.
Enamel matrix derivative and coronal flaps to cover marginal tissue recessions J Periodontol. 2006 Jan;77(1):7-14
jump to Study ! jump to Ref !
Evaluation of human recession defects treated with coronally advanced flaps and either enamel matrix
derivative or connective tissue. Part 1: Comparison of clinical parameters
McGuire MK, Nunn M.J Periodontol. 2003 Aug;74(8):1110-25.
STRAUMANN® 8McGuire MK, Nunn M.J Periodontol. 2003 Aug;74(8):1110-25.
Goal• To compare the clinical outcome of recession defects treated with the
coronally advanced flap technique (CAF) and either Emdogain or subepithelial connective tissue graft (CTG)
Methodology• Randomized, controlled clinical trial
• 20 patients
• Miller’s Class II buccal gingival recession of ≥ 4mm and width ≥ 3mm
• Incisors or premolars in contralateral quadrants of the same jaw
• Treatments sites were randomized in the control (coronally advanced flap with subepithelial connective tissue graft) or test group (coronally advanced flap with Emdogain) according to a split mouth design
Evaluation of human recession defects: comparison of clinical parameters
STRAUMANN® 9
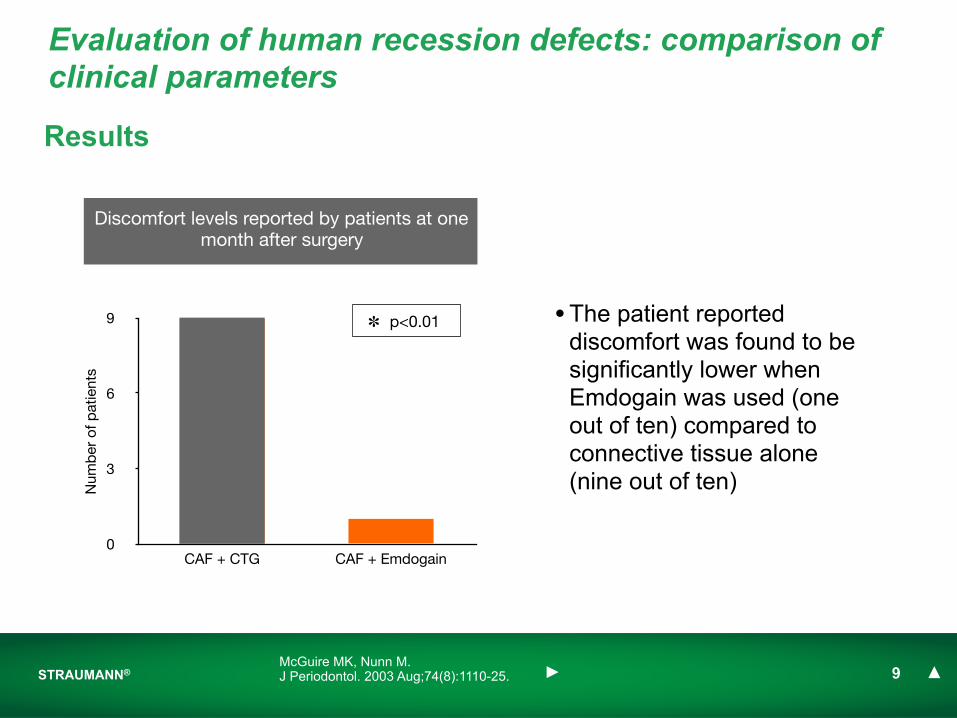
Results
• The patient reported discomfort was found to be significantly lower when Emdogain was used (one out of ten) compared to connective tissue alone (nine out of ten)
Evaluation of human recession defects: comparison of clinical parameters
0
3
6
9
CAF + CTG CAF + Emdogain
Num
ber
of p
atie
nts
Discomfort levels reported by patients at one month after surgery
✽ p<0.01
McGuire MK, Nunn M.J Periodontol. 2003 Aug;74(8):1110-25.
STRAUMANN® 10
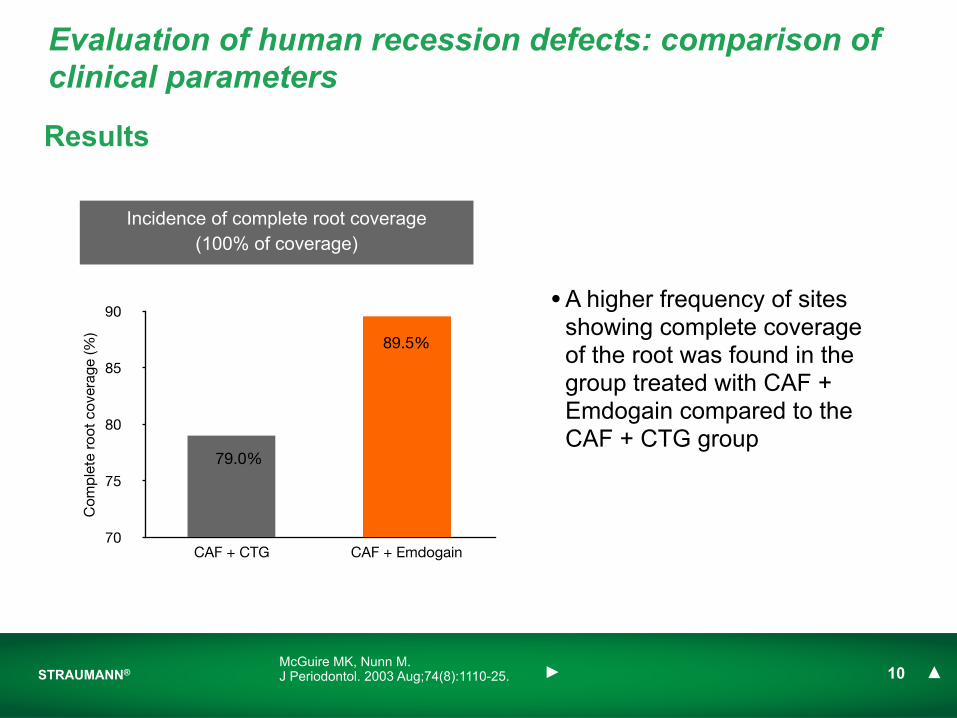
Results
Evaluation of human recession defects: comparison of clinical parameters
McGuire MK, Nunn M.J Periodontol. 2003 Aug;74(8):1110-25.
• A higher frequency of sites showing complete coverage of the root was found in the group treated with CAF + Emdogain compared to the CAF + CTG group
70
75
80
85
90
CAF + CTG CAF + Emdogain
Com
ple
te r
oot
cove
rage
(%)
Incidence of complete root coverage (100% of coverage)
79.0%
89.5%
STRAUMANN® 11
• The addition of Emdogain to the coronally advanced flap resulted in a root coverage similar to the subepithelial connective tissue graft, but without the morbidity due to potential clinical difficulties associated with the donor site surgery
Conclusion
Evaluation of human recession defects: comparison of clinical parameters
McGuire MK, Nunn M.J Periodontol. 2003 Aug;74(8):1110-25.
A comparative study of coronally advanced flaps with and without the addition of Enamel matrix derivative in
the treatment of marginal tissue recession
Cueva MA, Boltchi FE, Hallmon WW, Nunn ME, Rivera-Hidalgo F, Rees T.J Periodontol. 2004 Jul;75(7):949-56.
STRAUMANN® 13Cueva MA, Boltchi FE, Hallmon WW, Nunn ME, Rivera-Hidalgo F, Rees T.J Periodontol. 2004 Jul;75(7):949-56.
A comparative study of coronally advanced flaps in the treatment of marginal tissue recession
Goal
• To compare the clinical outcomes of root coverage procedures using the coronally advanced flap (CAF) technique with and without Emdogain
• To evaluate the influence of Emdogain on tissue keratinization
Methodology
• Randomized, controlled clinical trial
• 17 patients
• Miller’s Class I,II and III buccal marginal tissue recession ≥ 2mm
• 58 contralateral sites treated in total (29 sites per treatment modus)
• Treatment sites were randomized in the control (CAF alone) or test group (CAF in combination with Emdogain) according to a split mouth design
STRAUMANN® 14
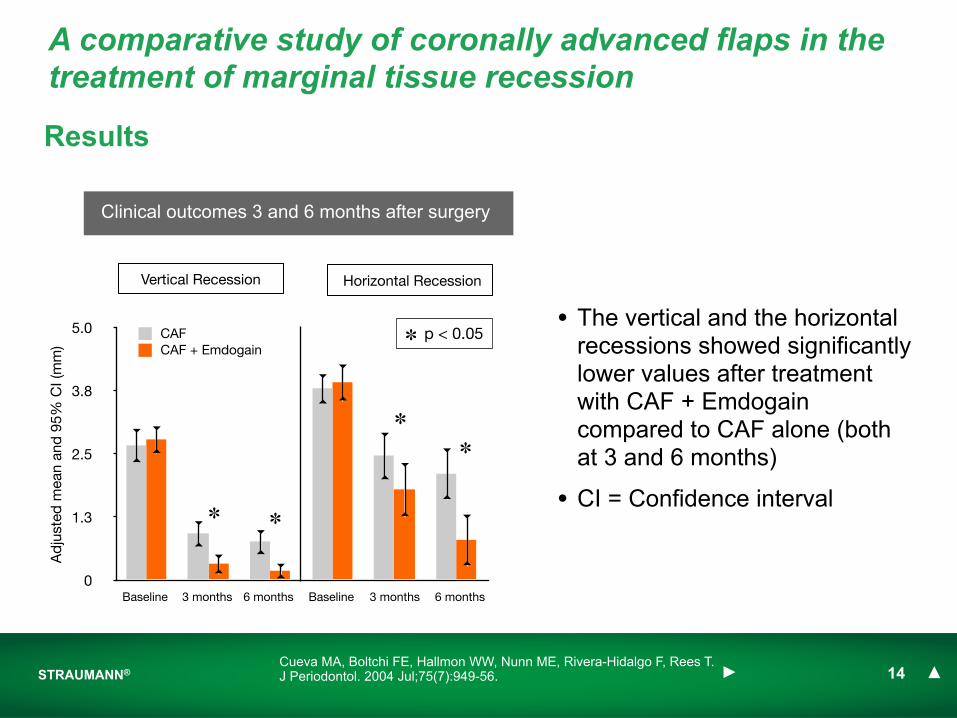
Results
• The vertical and the horizontal recessions showed significantly lower values after treatment with CAF + Emdogain compared to CAF alone (both at 3 and 6 months)
• CI = Confidence interval
0
1.3
2.5
3.8
5.0
Ad
just
ed m
ean
and
95%
CI (
mm
)
CAFCAF + Emdogain
Horizontal RecessionVertical Recession
✽ ✽
✽
✽
Clinical outcomes 3 and 6 months after surgery
✽ p < 0.05
Cueva MA, Boltchi FE, Hallmon WW, Nunn ME, Rivera-Hidalgo F, Rees T.J Periodontol. 2004 Jul;75(7):949-56.
A comparative study of coronally advanced flaps in the treatment of marginal tissue recession
Baseline 3 months 6 months Baseline 3 months 6 months

0
2.5
5.0
7.5
10.0
Baseline 3 months 6 months
STRAUMANN® 15
Results
✽ p < 0.05
• The analysis of the root exposure showed a significantly higher coverage in the CAF + Emdogain group compared to CAF alone
Cueva MA, Boltchi FE, Hallmon WW, Nunn ME, Rivera-Hidalgo F, Rees T.J Periodontol. 2004 Jul;75(7):949-56.
A comparative study of coronally advanced flaps in the treatment of marginal tissue recession
Clinical outcomes at 3 and 6 months after surgery
✽
✽
✽ p < 0.05
Exp
osed
roo
t su
rfac
e ar
ea (a
dju
sted
m
ean
and
95%
CI,
mm
2 )
0
25
50
75
100
3 months 6 months
CAFCAF + Emdogain
✽✽
✽ p < 0.05
% R
oot
cove
rage
(ad
just
ed m
ean
and
95%
CI,
mm
)
CAFCAF + Emdogain
0
0.8
1.5
2.3
3.0
Baseline 6 months
CAFCAF + Emdogain
STRAUMANN® 16
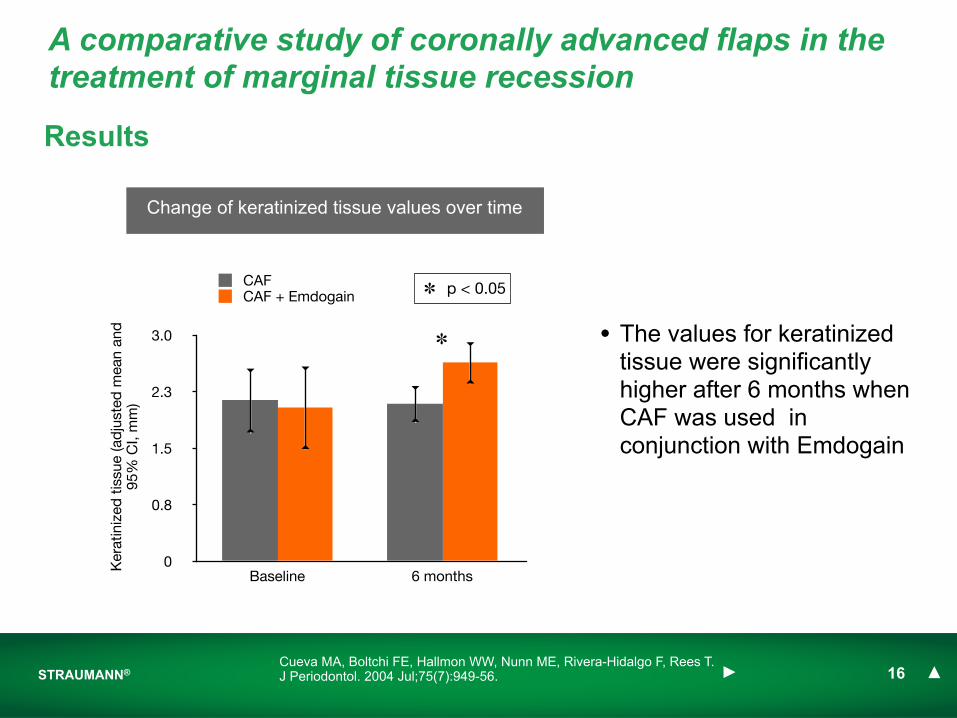
Results
Change of keratinized tissue values over time
✽
✽ p < 0.05
Cueva MA, Boltchi FE, Hallmon WW, Nunn ME, Rivera-Hidalgo F, Rees T.J Periodontol. 2004 Jul;75(7):949-56.
A comparative study of coronally advanced flaps in the treatment of marginal tissue recession
• The values for keratinized tissue were significantly higher after 6 months when CAF was used in conjunction with Emdogain
Ker
atin
ized
tis
sue
(ad
just
ed m
ean
and
95
% C
I, m
m)
STRAUMANN® 17
Conclusions
• The application of Emdogain to denuded root surfaces treated with the CAF technique increased significantly the percentage of root coverage compared to CAF alone
• The application of Emdogain was accompanied by a significant increase in keratinized tissue six months after surgery
Cueva MA, Boltchi FE, Hallmon WW, Nunn ME, Rivera-Hidalgo F, Rees T.J Periodontol. 2004 Jul;75(7):949-56.
A comparative study of coronally advanced flaps in the treatment of marginal tissue recession
Coverage of Miller class I and II recession defects using enamel matrix proteins versus coronally advanced flap
technique: a 2 year report
Spahr A, Haegewald S, Tsoulfidou F, Rompola E, Heijl L, Bernimoulin JP, Ring C, Sander S, Haller B.
J Periodontol. 2005 Nov;76(11):1871-80.
STRAUMANN® 19
Coverage of Miller class I and II recession defects using enamel matrix proteins versus coronally advanced flap technique
Spahr A, Haegewald S, Tsoulfidou F, Rompola E, Heijl L, Bernimoulin JP, Ring C, Sander S, Haller B.J Periodontol. 2005 Nov;76(11):1871-80.
Goal
• To compare the coronally advanced flap procedure used in the treatment of recession defects with or without the addition of Emdogain
Methodology
• Randomized, placebo-controlled, blinded clinical study
• 30 patients
• Miller Class I and II buccal recession defects ≥ 3mm in contralateral quadrants of the same jaw
• Surgical recession coverage was performed according to the coronally advanced flap technique
• Emdogain (test) or placebo (propylene glycol alginate, control) were randomly assigned to the sites according to a split-mouth design
STRAUMANN® 20
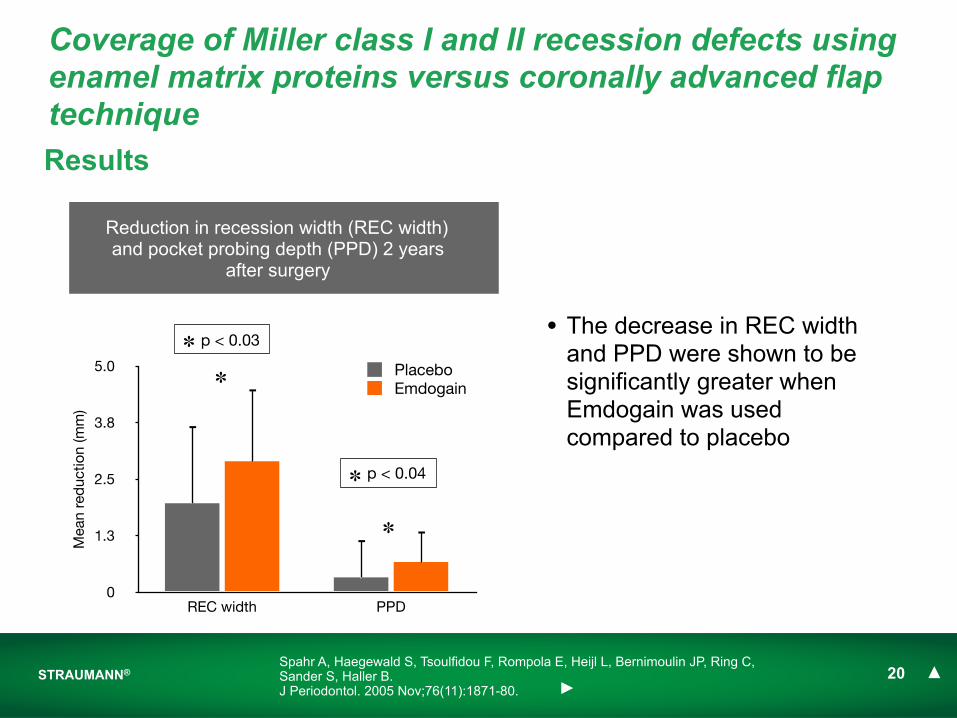
Results
• The decrease in REC width and PPD were shown to be significantly greater when Emdogain was used compared to placebo
✽
✽
Reduction in recession width (REC width) and pocket probing depth (PPD) 2 years
after surgery
Spahr A, Haegewald S, Tsoulfidou F, Rompola E, Heijl L, Bernimoulin JP, Ring C, Sander S, Haller B.J Periodontol. 2005 Nov;76(11):1871-80.
Coverage of Miller class I and II recession defects using enamel matrix proteins versus coronally advanced flap technique
0
1.3
2.5
3.8
5.0
REC width PPD
Mea
n re
duc
tion
(mm
)
PlaceboEmdogain
✽ p < 0.03
✽ p < 0.04
STRAUMANN® 21
Results
0
15
30
45
60
Emdogain Placebo
Com
ple
te r
oot
cove
rage
(%)
0
13
25
38
50
Emdogain Placebo
Det
erio
rate
d t
reat
ed r
eces
sion
s (%
)
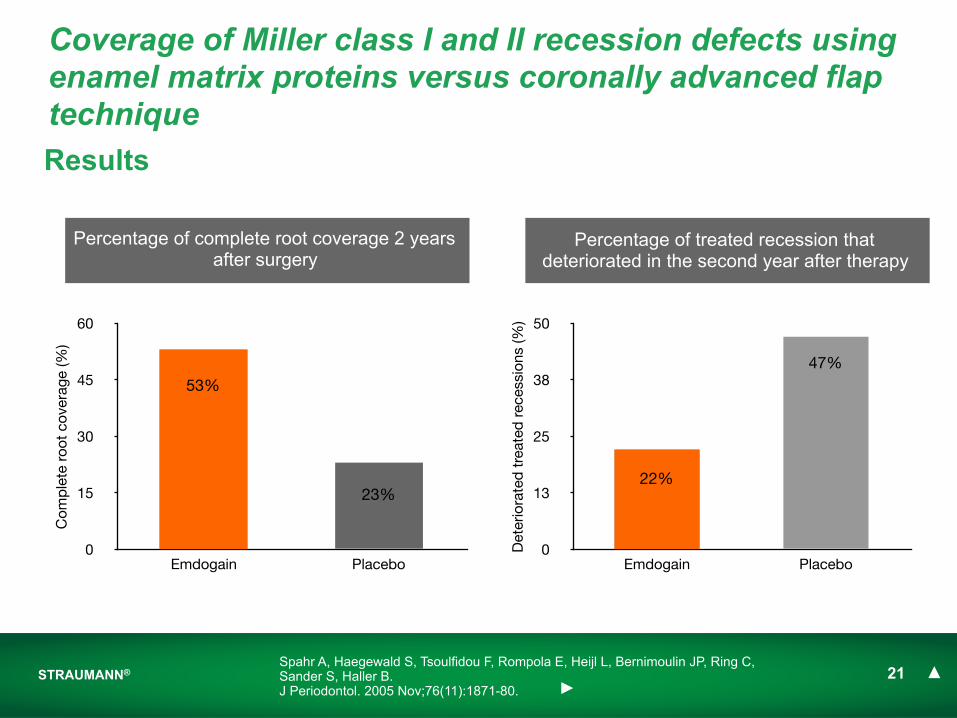
Percentage of complete root coverage 2 years after surgery
Percentage of treated recession that deteriorated in the second year after therapy
Spahr A, Haegewald S, Tsoulfidou F, Rompola E, Heijl L, Bernimoulin JP, Ring C, Sander S, Haller B.J Periodontol. 2005 Nov;76(11):1871-80.
Coverage of Miller class I and II recession defects using enamel matrix proteins versus coronally advanced flap technique
53%
23%22%
47%

STRAUMANN® 22
Conclusion
There is indication that the addition of Emdogain to the CAF technique...• provides better long-term results concerning the stability of the treatment• increases the amount of complete root coverage 2 years after surgery• reduces the amount of deteriorated recessions in the second year after therapy...in comparison to the CAF technique alone
Spahr A, Haegewald S, Tsoulfidou F, Rompola E, Heijl L, Bernimoulin JP, Ring C, Sander S, Haller B.J Periodontol. 2005 Nov;76(11):1871-80.
Coverage of Miller class I and II recession defects using enamel matrix proteins versus coronally advanced flap technique
Enamel matrix derivative and coronal flaps to cover marginal tissue recessions
Castellanos A, de la Rosa M, de la Garza M, Caffesse RG.J Periodontol. 2006 Jan;77(1):7-14.
STRAUMANN® 24
Enamel matrix derivative and coronal flaps to cover marginal tissue recessions
Goal
• To clinically evaluate the use of Emdogain in association with coronally positioned flap (CPF) technique to cover localized gingival recessions compared to CPF alone
Methodology
• Randomized, controlled clinical study
• 22 patients
• Miller Class I and II gingival recession defects > 2mm
• Control group: CPF alone; test group: CPF in combination with Emdogain
• Surgical recession coverage was performed according to the “coronally positioned flap” (CPF) technique
Castellanos A, de la Rosa M, de la Garza M, Caffesse RG.J Periodontol. 2006 Jan;77(1):7-14.
Results
STRAUMANN® 25
0
1.3
2.5
3.8
5.0
Baseline 6 months 12 months
Vert
ical
rec
essi
on (m
m)
Emdogain + CPFCPF
0
1.8
3.5
5.3
7.0
Baseline 6 months 12 monthsH
oriz
onta
l rec
essi
on (m
m)
Emdogain + CPFCPF
✽ ✽✽ ✽
✽ p < 0.05✽ p < 0.05
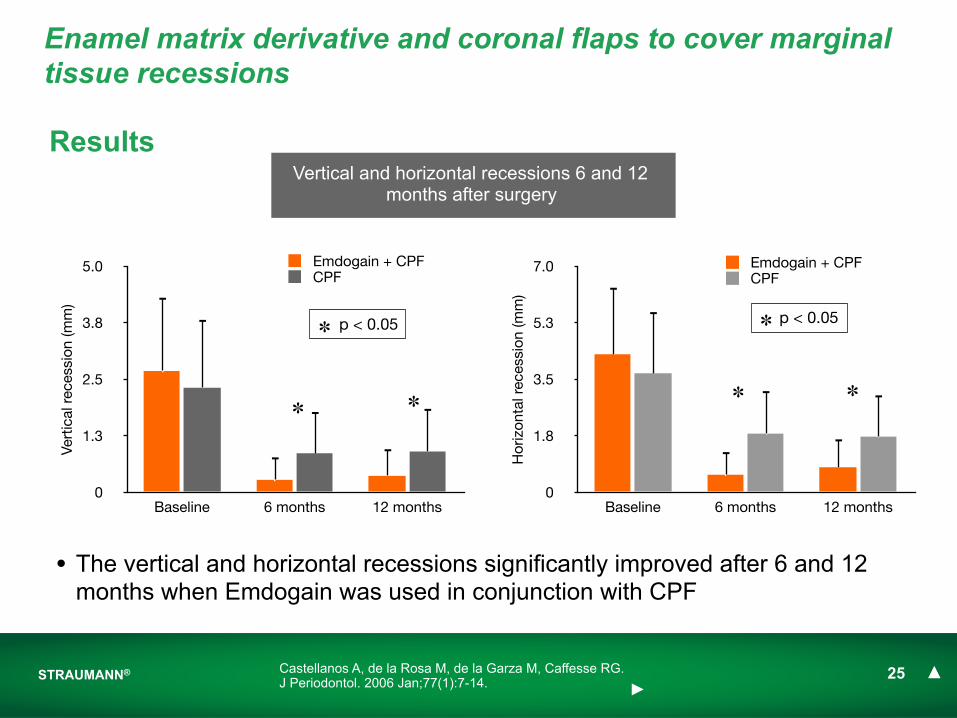
Castellanos A, de la Rosa M, de la Garza M, Caffesse RG.J Periodontol. 2006 Jan;77(1):7-14.
Enamel matrix derivative and coronal flaps to cover marginal tissue recessions
Vertical and horizontal recessions 6 and 12 months after surgery
• The vertical and horizontal recessions significantly improved after 6 and 12 months when Emdogain was used in conjunction with CPF

STRAUMANN® 26
Results
Emdogain + CPFCPF
0
1.8
3.5
5.3
7.0
Baseline 12 months
Ker
atin
ized
gin
giva
(mm
)
✽
✽ p < 0.05
Castellanos A, de la Rosa M, de la Garza M, Caffesse RG.J Periodontol. 2006 Jan;77(1):7-14.
Enamel matrix derivative and coronal flaps to cover marginal tissue recessions
• The addition of Emdogain resulted in a statistically significantly higher value after 12 months for the keratinized gingiva
Keratinized gingiva 12 months after surgery

STRAUMANN® 27
The addition of Emdogain to the CPF technique...
• significantly improved the amount of root coverage of localized gingival recessions
• resulted in a statistically significantly higher keratinized gingiva value after 12 months
...in comparison to the CPF technique alone
Conclusion
Castellanos A, de la Rosa M, de la Garza M, Caffesse RG.J Periodontol. 2006 Jan;77(1):7-14.
Enamel matrix derivative and coronal flaps to cover marginal tissue recessions
Intrabony defectsMay 25, 2011
Straumann® Emdogain
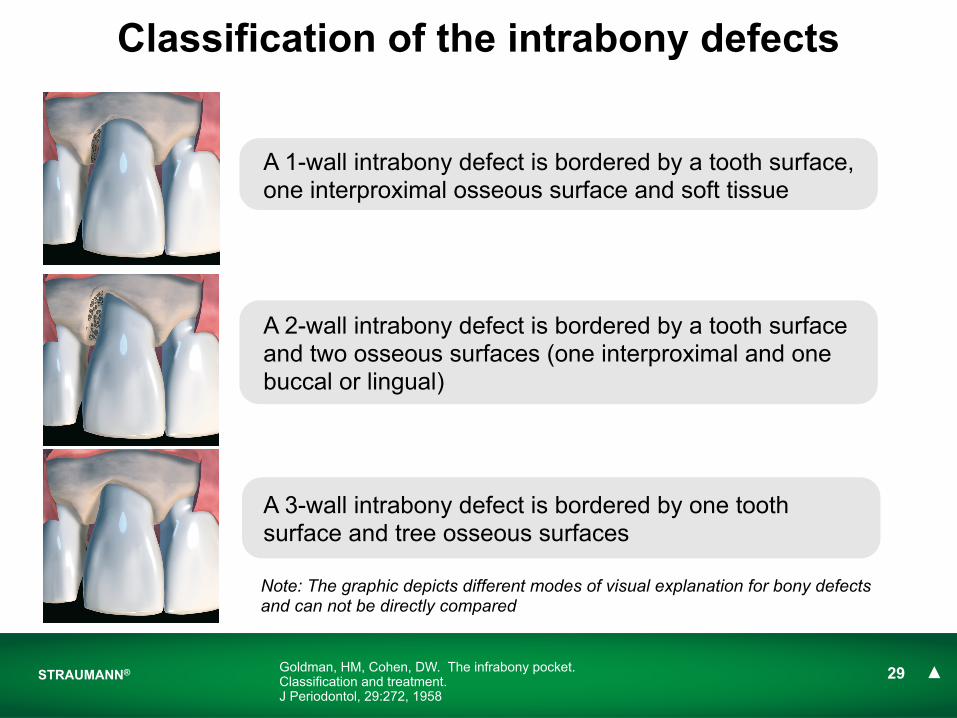
STRAUMANN® 29Goldman, HM, Cohen, DW. The infrabony pocket. Classification and treatment. J Periodontol, 29:272, 1958
Classification of the intrabony defects
A 1-wall intrabony defect is bordered by a tooth surface, one interproximal osseous surface and soft tissue
A 2-wall intrabony defect is bordered by a tooth surface and two osseous surfaces (one interproximal and one buccal or lingual)
A 3-wall intrabony defect is bordered by one tooth surface and tree osseous surfaces
Note: The graphic depicts different modes of visual explanation for bony defects and can not be directly compared

STRAUMANN® 30
Straumann® EmdogainPublication First AuthorFirst Author Full Author List Full Title Reference
1 Froum SJ Froum SJ, Weinberg MA, Rosenberg E, Tarnow D.
A comparative study utilizing open flap debridement with and without enamel matrix derivative in the treatment of periodontal intrabony defects: a 12-month re-entry study
J Periodontol. 2001 Jan;72(1):25-34.
2 Tonetti MS
Tonetti MS, Lang NP, Cortellini P, Suvan JE, Adriaens P, Dubravec D, Fonzar A, Fourmousis I, Mayfield L, Rossi R, Silvestri M, Tiedemann C, Topoll H, Vangsted T, Wallkamm B.
Enamel matrix proteins in the regenerative therapy of deep intrabony defects J Clin Periodontol. 2002 Apr;29(4):317-25.
3 Sanz M
Sanz M, Tonetti MS, Zabalegui I, Sicilia A, Blanco J, Rebelo H, Rasperini G, Merli M, Cortellini P, Suvan JE.
Treatment of intrabony defects with enamel matrix proteins or barrier membranes: results from a multicenter practice-based clinical trial. J Periodontol. 2004 May;75(5):726-33.
4 Francetti LFrancetti L, Trombelli L, Lombardo G, Guida L, Cafiero C, Roccuzzo M, Carusi G, Del Fabbro M.
Evaluation of efficacy of enamel matrix derivative in the treatment of intrabony defects: a 24-month multicenter study.
Int J Periodontics Restorative Dent. 2005 Oct;25(5):461-73.
5 Crea A Crea A, Dassatti L, Hoffmann O, Zafiropoulos GG, Deli G.
Treatment of intrabony defects using guided tissue regeneration or enamel matrix derivative: a 3-year prospective randomized clinical study J Periodontol. 2008 Dec;79(12):2281-9
jump to Study ! jump to Ref !
A comparative study utilizing open flap debridment with and without enamel matrix derivative in the treatment of
periodontal intrabony defects: a 12-months re-entry study
Froum SJ, Weinberg MA, Rosenberg E, Tarnow D.J Periodontol. 2001 Jan;72(1):25-34.
STRAUMANN® 32Froum SJ, Weinberg MA, Rosenberg E, Tarnow D.J Periodontol. 2001 Jan;72(1):25-34.
Goal
• To compare at 12 months post surgery sites treated with open flap debridement (OFD) alone to those treated with OFD and Emdogain
Methodology
• Randomized, controlled clinical trial
• 23 patients with at least 2 intrabony defects
• 53 defects were treated with OFD and Emdogain, 31 defects were treated with Emdogain alone
•The defects were randomly assigned to the treatment groups according to a split mouth design
A comparative study utilizing open flap debridement with and without enamel matrix derivative: a 12-month re-entry study
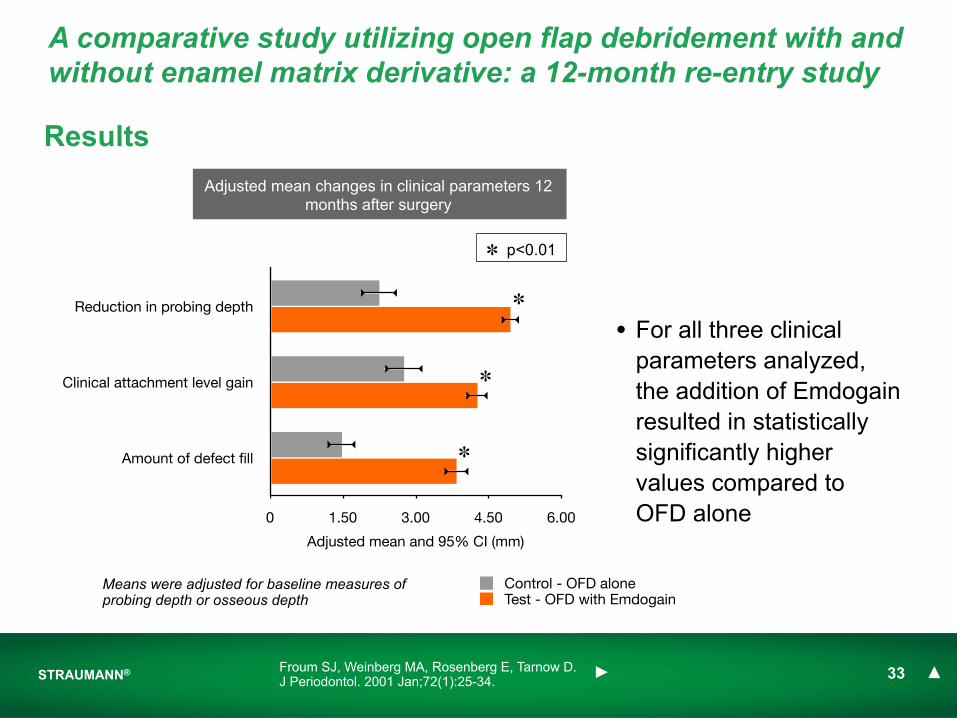
Reduction in probing depth
Clinical attachment level gain
Amount of defect fill
0 1.50 3.00 4.50 6.00
Adjusted mean and 95% CI (mm)
Control - OFD aloneTest - OFD with Emdogain
Means were adjusted for baseline measures of probing depth or osseous depth
STRAUMANN® 33
Results
• For all three clinical parameters analyzed, the addition of Emdogain resulted in statistically significantly higher values compared to OFD alone
Adjusted mean changes in clinical parameters 12 months after surgery
Froum SJ, Weinberg MA, Rosenberg E, Tarnow D.J Periodontol. 2001 Jan;72(1):25-34.
A comparative study utilizing open flap debridement with and without enamel matrix derivative: a 12-month re-entry study
✽ p<0.01
✽
✽
✽
STRAUMANN® 34
Results
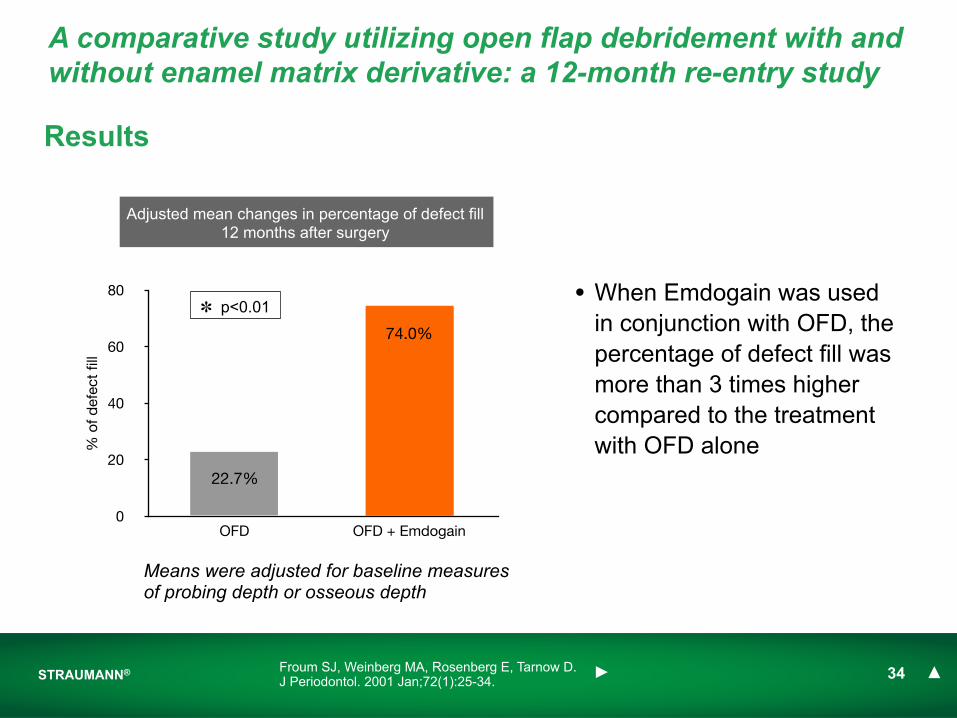
• When Emdogain was used in conjunction with OFD, the percentage of defect fill was more than 3 times higher compared to the treatment with OFD alone
Adjusted mean changes in percentage of defect fill 12 months after surgery
Froum SJ, Weinberg MA, Rosenberg E, Tarnow D.J Periodontol. 2001 Jan;72(1):25-34.
A comparative study utilizing open flap debridement with and without enamel matrix derivative: a 12-month re-entry study
Means were adjusted for baseline measures of probing depth or osseous depth
0
20
40
60
80
OFD OFD + Emdogain
% o
f def
ect
fill
✽ p<0.01
22.7%
74.0%

STRAUMANN® 35
• The study indicated that the treatment of periodontal intraosseous defects with OFD in combination with Emdogain is clinically superior to the treatment with OFD alone when considering the reduction in probing depth, the clinical attachment level gain and the amount of defect fill
•
Conclusion
Froum SJ, Weinberg MA, Rosenberg E, Tarnow D.J Periodontol. 2001 Jan;72(1):25-34.
A comparative study utilizing open flap debridement with and without enamel matrix derivative: a 12-month re-entry study
Enamel matrix proteins in the regenerative therapy of deep intrabony defects
Tonetti MS, Lang NP, Cortellini P, Suvan JE, Adriaens P, Dubravec D, Fonzar A, Fourmousis I, Mayfield L, Rossi R, Silvestri M, Tiedemann C,
Topoll H, Vangsted T, Wallkamm B.J Clin Periodontol. 2002 Apr;29(4):317-25.
STRAUMANN® 37Tonetti MS, Lang NP, Cortellini P, Suvan JE, Adriaens P, Dubravec D, Fonzar A, Fourmousis I, Mayfield L, Rossi R, Silvestri M, Tiedemann C, Topoll H, Vangsted T, Wallkamm B.J Clin Periodontol. 2002 Apr;29(4):317-25.
Enamel matrix proteins in the regenerative therapy of deep intrabony defects
Goal• To compare the clinical outcome of the papilla preservation flap technique with or
without the application of Emdogain
Methodology• Randomized, controlled, multicenter clinical trial (12 centers in 7 countries)
• 172 patients with chronic periodontitis were enrolled in the study. Data from 166 patients were collected at the one year follow-up
• Patients had at least one intrabony defect ≥ 3mm
• The surgical procedures included either the Simplified Papilla Preservation Flap (SPPF, if the interproximal space measured at the interproximal soft tissue had a mesio-distal width ≤ 2mm ) or the Modified Papilla Preservation Flap (MPPF, if the space was >2 mm ) techniques
• Patients in the control group were treated with the SPPF or MPPF technique only, while in the test group the surgeries were performed in conjunction with Emdogain

STRAUMANN® 38
Results
Enamel matrix proteins in the regenerative therapy of deep intrabony defects
The additional use of Emdogain • led to a significantly higher gain
in CAL • a greater decrease in PPD
compared to the treatment with SPPF/MPPF alone
Tonetti MS, Lang NP, Cortellini P, Suvan JE, Adriaens P, Dubravec D, Fonzar A, Fourmousis I, Mayfield L, Rossi R, Silvestri M, Tiedemann C, Topoll H, Vangsted T, Wallkamm B.J Clin Periodontol. 2002 Apr;29(4):317-25.
Clinical outcomes 1 year after treatment for the two treatment groups
0
2
4
6
SPPF/MPPF + Emdogain (n=83)
SPPF/MPPF (n=83)
Gain in clinical attachment level
(CAL)
Decrease in pocket probing depth
(PPD)
mm
✽
✽
✽ p < 0.05
STRAUMANN® 39
Results
Enamel matrix proteins in the regenerative therapy of deep intrabony defects
Tonetti MS, Lang NP, Cortellini P, Suvan JE, Adriaens P, Dubravec D, Fonzar A, Fourmousis I, Mayfield L, Rossi R, Silvestri M, Tiedemann C, Topoll H, Vangsted T, Wallkamm B.J Clin Periodontol. 2002 Apr;29(4):317-25.
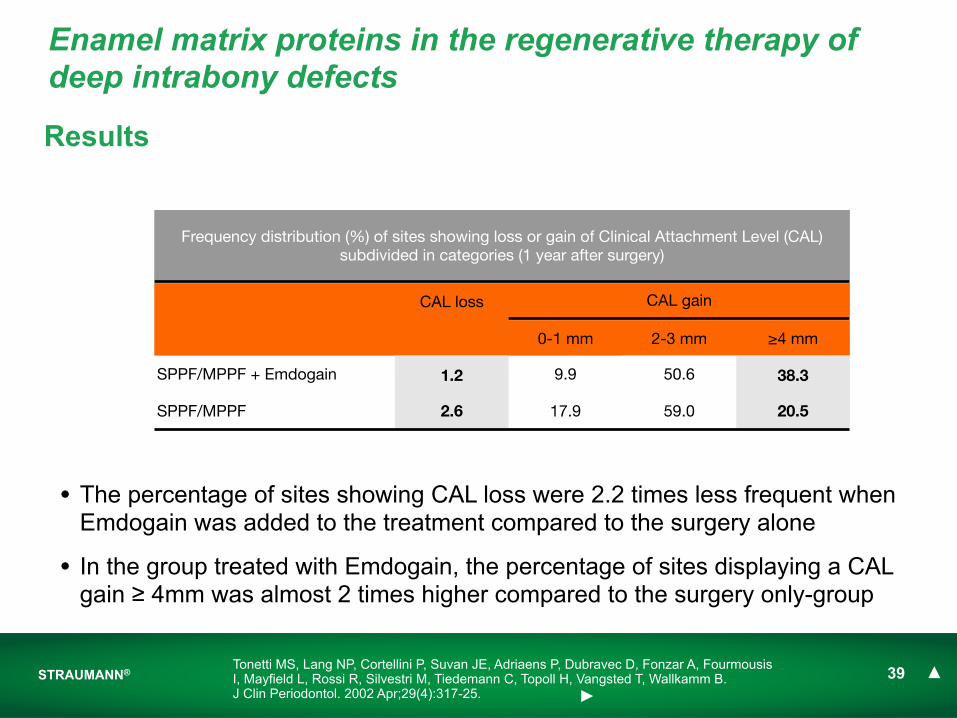
Frequency distribution (%) of sites showing loss or gain of Clinical Attachment Level (CAL) subdivided in categories (1 year after surgery)
Frequency distribution (%) of sites showing loss or gain of Clinical Attachment Level (CAL) subdivided in categories (1 year after surgery)
Frequency distribution (%) of sites showing loss or gain of Clinical Attachment Level (CAL) subdivided in categories (1 year after surgery)
Frequency distribution (%) of sites showing loss or gain of Clinical Attachment Level (CAL) subdivided in categories (1 year after surgery)
Frequency distribution (%) of sites showing loss or gain of Clinical Attachment Level (CAL) subdivided in categories (1 year after surgery)
CAL loss CAL gain
0-1 mm 2-3 mm ≥4 mm
SPPF/MPPF + Emdogain 1.2 9.9 50.6 38.3
SPPF/MPPF 2.6 17.9 59.0 20.5
• The percentage of sites showing CAL loss were 2.2 times less frequent when Emdogain was added to the treatment compared to the surgery alone
• In the group treated with Emdogain, the percentage of sites displaying a CAL gain ≥ 4mm was almost 2 times higher compared to the surgery only-group
STRAUMANN® 40
• The regenerative periodontal surgery (papilla preservation technique) used in combination with Emdogain offers an additional benefit in terms of CAL gain and PPD reduction compared with the surgical technique alone
Conclusions
Enamel matrix proteins in the regenerative therapy of deep intrabony defects
Tonetti MS, Lang NP, Cortellini P, Suvan JE, Adriaens P, Dubravec D, Fonzar A, Fourmousis I, Mayfield L, Rossi R, Silvestri M, Tiedemann C, Topoll H, Vangsted T, Wallkamm B.J Clin Periodontol. 2002 Apr;29(4):317-25.
Treatment of intrabony defects with enamel matrix proteins or barrier membranes: results from a
multicenter practice-based clinical trial
Sanz M, Tonetti MS, Zabalegui I, Sicilia A, Blanco J, Rebelo H, Rasperini G, Merli M, Cortellini P, Suvan JE.
J Periodontol. 2004 May;75(5):726-33.
STRAUMANN® 42
Treatment of intrabony defects with enamel matrix proteins or barrier membranes: results from a multicenter clinical trial
Sanz M, Tonetti MS, Zabalegui I, Sicilia A, Blanco J, Rebelo H, Rasperini G, Merli M, Cortellini P, Suvan JE.J Periodontol. 2004 May;75(5):726-33.
Goal
• To compare the clinical outcomes of Emdogain versus placement of bioabsorbable membrane in conjunction with guided tissue regeneration (GTR)
Methodology
• Randomized, controlled, multicenter clinical trial
• 7 centres in 3 countries
• 75 patients with advanced chronic periodontitis
• Patients displayed intrabony defect of ≥ 3mm located in the anterior and premolar region
• One defect per patient was treated using the simplified papilla preservation flap (PPF) and either the application of Emdogin (test) or the placement of a membrane according to GTR (control)
0
25
50
75
100
Emdogain GTR
% p
atie
nts
rep
ortin
g co
mp
licat
ions
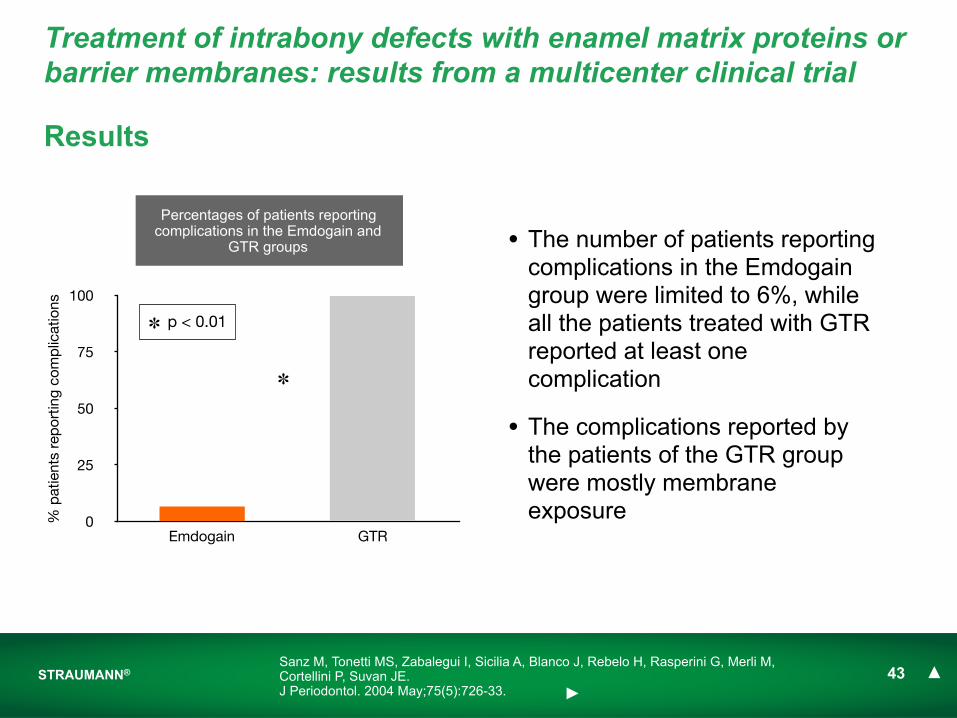
Percentages of patients reporting complications in the Emdogain and
GTR groups
✽ p < 0.01
✽
STRAUMANN® 43
Results
• The number of patients reporting complications in the Emdogain group were limited to 6%, while all the patients treated with GTR reported at least one complication
• The complications reported by the patients of the GTR group were mostly membrane exposure
Sanz M, Tonetti MS, Zabalegui I, Sicilia A, Blanco J, Rebelo H, Rasperini G, Merli M, Cortellini P, Suvan JE.J Periodontol. 2004 May;75(5):726-33.
Treatment of intrabony defects with enamel matrix proteins or barrier membranes: results from a multicenter clinical trial
STRAUMANN® 44
Results
0
1
2
3
4
5
CA
L ga
in (m
m)
Emdogain GTR
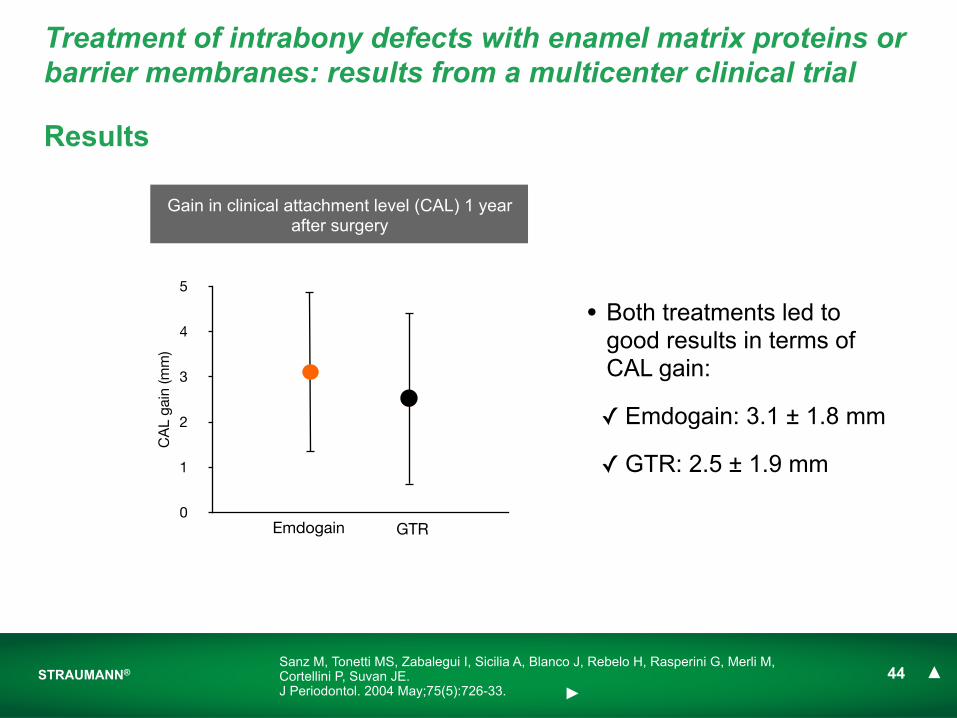
Gain in clinical attachment level (CAL) 1 year after surgery
Sanz M, Tonetti MS, Zabalegui I, Sicilia A, Blanco J, Rebelo H, Rasperini G, Merli M, Cortellini P, Suvan JE.J Periodontol. 2004 May;75(5):726-33.
Treatment of intrabony defects with enamel matrix proteins or barrier membranes: results from a multicenter clinical trial
• Both treatments led to good results in terms of CAL gain:
✓ Emdogain: 3.1 ± 1.8 mm
✓ GTR: 2.5 ± 1.9 mm
STRAUMANN® 45
• Emdogain and GTR in conjunction with the papilla preservation flap technique led to significant improvements after one year
• Patients treated with GTR showed a higher frequency of postoperative complications (mostly membrane exposure) compared with the treatment using Emdogain
Conclusion
Sanz M, Tonetti MS, Zabalegui I, Sicilia A, Blanco J, Rebelo H, Rasperini G, Merli M, Cortellini P, Suvan JE.J Periodontol. 2004 May;75(5):726-33.
Treatment of intrabony defects with enamel matrix proteins or barrier membranes: results from a multicenter clinical trial

Evaluation of efficacy of enamel matrix derivative in the treatment of intrabony defects: a 24-month multicenter
study
Francetti L, Trombelli L, Lombardo G, Guida L, Cafiero C, Roccuzzo M, Carusi G, Del Fabbro M.
Int J Periodontics Restorative Dent. 2005 Oct;25(5):461-73.

STRAUMANN® 47Francetti L, Trombelli L, Lombardo G, Guida L, Cafiero C, Roccuzzo M, Carusi G, Del Fabbro M.Int J Periodontics Restorative Dent. 2005 Oct;25(5):461-73.
Evaluation of efficacy of enamel matrix derivative in the treatment of intrabony defects
Goal• To evaluate the efficacy of Emdogain when combined with surgical treatment of
periodontal angular defects as compared to surgery alone
Methodology• Randomized, controlled, multicenter clinical trial
• 17 centers in Italy
• 153 patients enrolled, accounting for 195 defects
• One-, two- and three-wall angular defects were included
• Intrabony defect depth was ≥ 4mm and probing procket depth was ≥ 6mm
• Surgical technique: simplified papilla preservation flap (SPPF), used in combination with Emdogain (test) or alone (control)
STRAUMANN® 48
Results
12 41
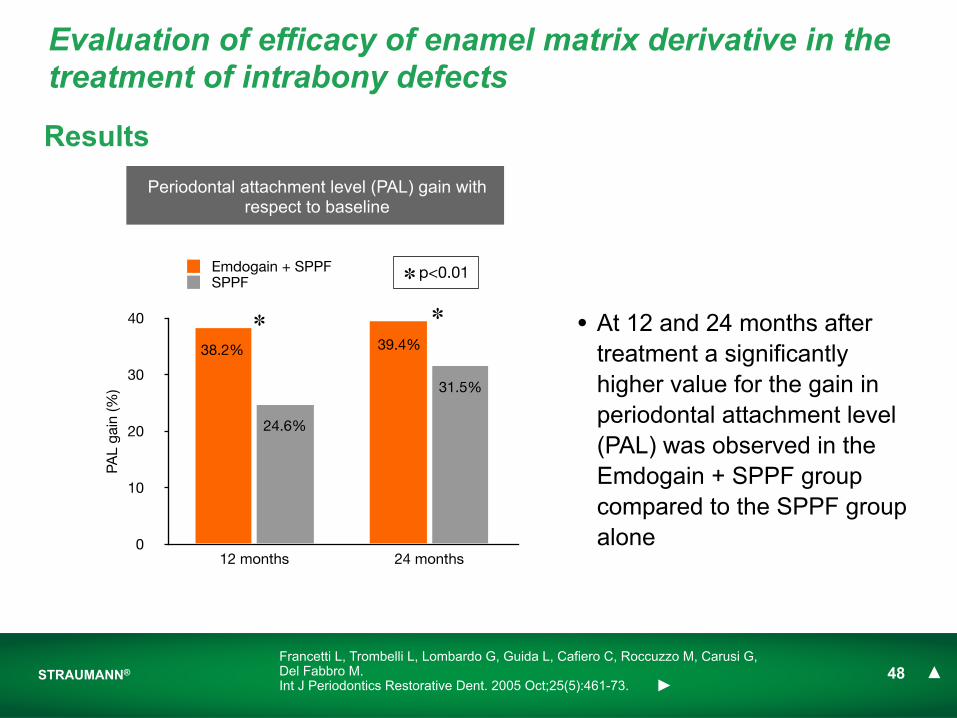
• At 12 and 24 months after treatment a significantly higher value for the gain in periodontal attachment level (PAL) was observed in the Emdogain + SPPF group compared to the SPPF group alone
Francetti L, Trombelli L, Lombardo G, Guida L, Cafiero C, Roccuzzo M, Carusi G, Del Fabbro M.Int J Periodontics Restorative Dent. 2005 Oct;25(5):461-73.
Evaluation of efficacy of enamel matrix derivative in the treatment of intrabony defects
0
10
20
30
40
12 months 24 months
PAL
gain
(%)
Emdogain + SPPFSPPF
Periodontal attachment level (PAL) gain with respect to baseline
✽ ✽
✽ p<0.01
38.2% 39.4%
24.6%
31.5%
STRAUMANN® 49
Results
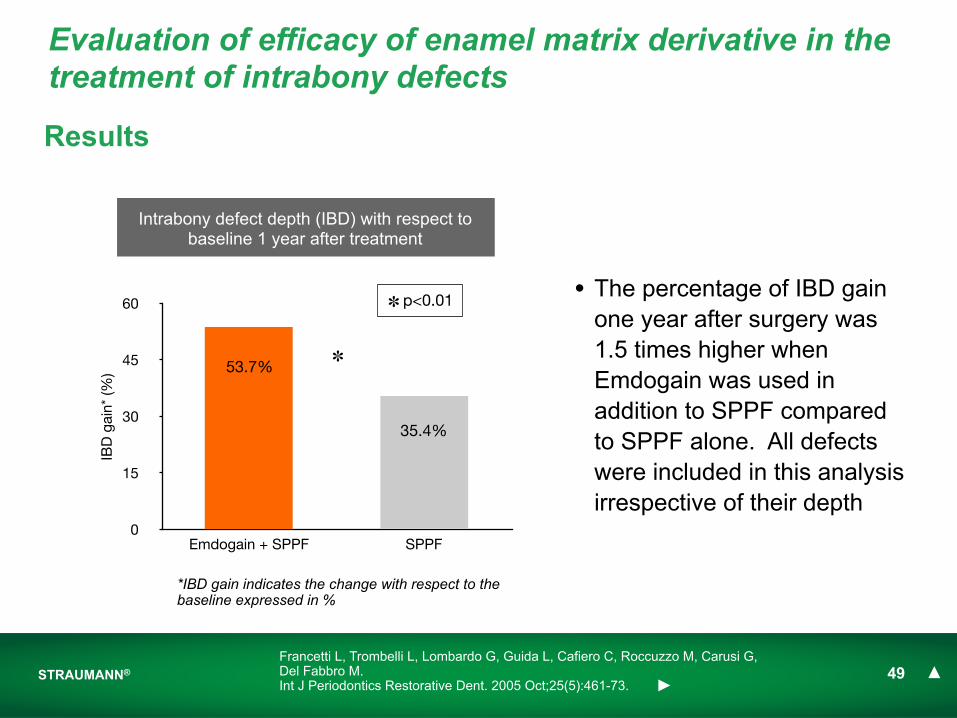
• The percentage of IBD gain one year after surgery was 1.5 times higher when Emdogain was used in addition to SPPF compared to SPPF alone. All defects were included in this analysis irrespective of their depth
Intrabony defect depth (IBD) with respect to baseline 1 year after treatment
0
15
30
45
60
Emdogain + SPPF SPPF
IBD
gai
n* (%
) 53.7%
35.4%
✽
✽ p<0.01
Francetti L, Trombelli L, Lombardo G, Guida L, Cafiero C, Roccuzzo M, Carusi G, Del Fabbro M.Int J Periodontics Restorative Dent. 2005 Oct;25(5):461-73.
Evaluation of efficacy of enamel matrix derivative in the treatment of intrabony defects
*IBD gain indicates the change with respect to the baseline expressed in %

STRAUMANN® 50
Results
• Also in case of deep defects (> 6mm) the addition of Emdogain leads to a greater (1.65 times) percentage of IBD gain compared to SPPF alone
Francetti L, Trombelli L, Lombardo G, Guida L, Cafiero C, Roccuzzo M, Carusi G, Del Fabbro M.Int J Periodontics Restorative Dent. 2005 Oct;25(5):461-73.
Evaluation of efficacy of enamel matrix derivative in the treatment of intrabony defects
0
14
28
42
56
70
Emdogain + SPPF SPPF
IBD
gai
n* (%
)
Intrabony defect depth (IBD) with respect to baseline 1 year after treatment for deep defects (> 6mm)
✽
✽ p<0.05
60.1%
36.4%
*IBD gain indicates the change with respect to the baseline expressed in %
STRAUMANN® 51
• The use of Emdogain significantly improved the periodontal attachment level (PAL) gain with respect to baseline as well as the gain in intrabony defect depth (IBD) with respect to baseline one year after treatment as compared to the use of the surgical technique alone
• Emdogain demonstrated better results in terms of improvement in intrabony defect depth (IBD) with respect to baseline one year after treatment when it was used in the subgroup of deeper defects (> 6mm) compared to the results obtained with the surgery alone
Conclusions
Francetti L, Trombelli L, Lombardo G, Guida L, Cafiero C, Roccuzzo M, Carusi G, Del Fabbro M.Int J Periodontics Restorative Dent. 2005 Oct;25(5):461-73.
Evaluation of efficacy of enamel matrix derivative in the treatment of intrabony defects
Treatment of intrabony defects using guided tissue regeneration or enamel matrix derivative: a 3-year
prospective randomized clinical study
Crea A, Dassatti L, Hoffmann O, Zafiropoulos GG, Deli G.J Periodontol. 2008 Dec;79(12):2281-9.
STRAUMANN® 53
Treatment of intrabony defects using guided tissue regeneration or enamel matrix derivative
Crea A, Dassatti L, Hoffmann O, Zafiropoulos GG, Deli G.J Periodontol. 2008 Dec;79(12):2281-9.
Goal
• To compare the clinical results obtained with guided tissue regeneration (GTR) to the ones obtained with Emdogain in the treatment of intrabony defects
Methodology
• Randomized, controlled clinical trial
• 40 patients with advanced chronic periodontitis
• 40 defect, exclusively 3-wall defects, each with a depth ≥4mm
• Surgical technique: simplified papilla preservation flap (SPPF), used in combination with Emdogain (test) or non-resorbable membranes (control)
STRAUMANN® 54
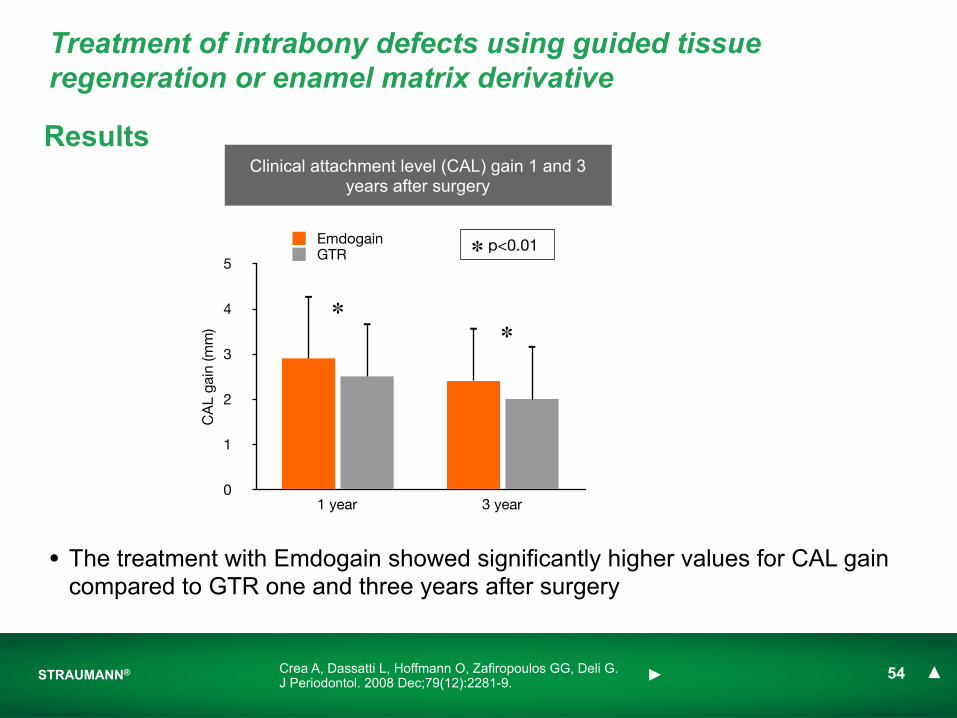
Results
• The treatment with Emdogain showed significantly higher values for CAL gain compared to GTR one and three years after surgery
0
1
2
3
4
5
1 year 3 year
CA
L ga
in (m
m)
EmdogainGTR
Clinical attachment level (CAL) gain 1 and 3 years after surgery
✽ p<0.01
✽
✽
Crea A, Dassatti L, Hoffmann O, Zafiropoulos GG, Deli G.J Periodontol. 2008 Dec;79(12):2281-9.
Treatment of intrabony defects using guided tissue regeneration or enamel matrix derivative
STRAUMANN® 55
• The gain of clinical attachment level at 12 and 36 months after surgery was significantly higher when the defects were treated with Emdogain compared to the treatment with GTR
Conclusion
Crea A, Dassatti L, Hoffmann O, Zafiropoulos GG, Deli G.J Periodontol. 2008 Dec;79(12):2281-9.
Treatment of intrabony defects using guided tissue regeneration or enamel matrix derivative

Furcation defectsMay 25, 2011
Straumann® Emdogain
STRAUMANN® 57Hamp SE, Nyman S, Lindhe J. Periodontal treatment of multirooted teeth. Results after 5 years. J Clin Periodontol. 1975;2:126-35
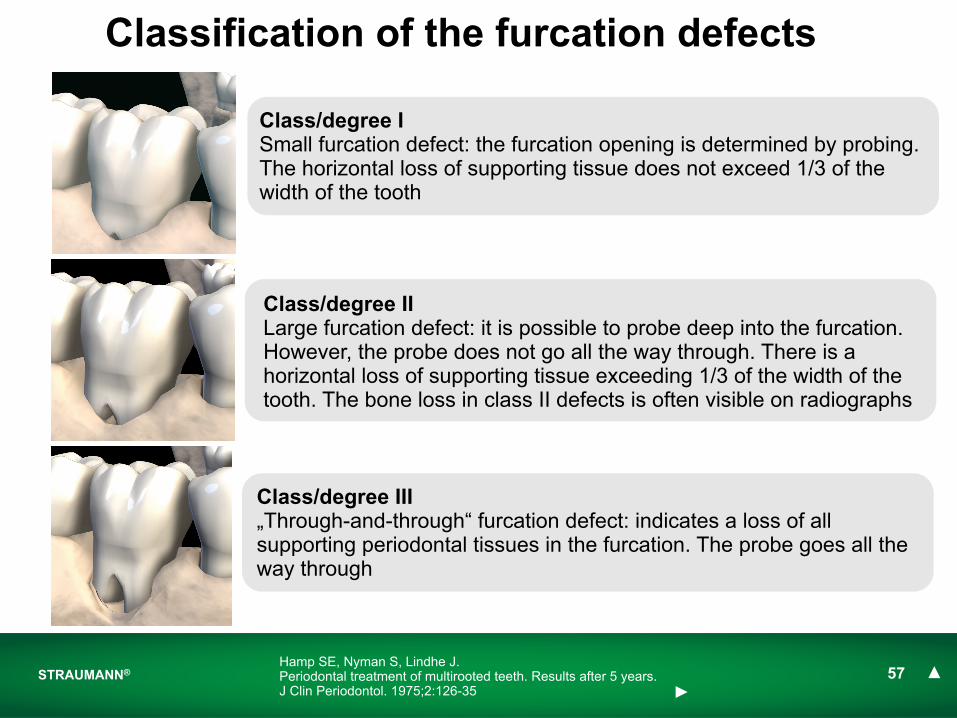
Classification of the furcation defects
Class/degree ISmall furcation defect: the furcation opening is determined by probing. The horizontal loss of supporting tissue does not exceed 1/3 of the width of the tooth
Class/degree IILarge furcation defect: it is possible to probe deep into the furcation. However, the probe does not go all the way through. There is a horizontal loss of supporting tissue exceeding 1/3 of the width of the tooth. The bone loss in class II defects is often visible on radiographs
Class/degree III „Through-and-through“ furcation defect: indicates a loss of all supporting periodontal tissues in the furcation. The probe goes all the way through

STRAUMANN® 58
Straumann® EmdogainPublication First AuthorFirst Author Full Author List Full Title Reference
1 Jepsen S
Jepsen S, Heinz B, Jepsen K, Arjomand M, Hoffmann T, Richter S, Reich E, Sculean A, Gonzales JR, Bödeker RH, Meyle J.
A randomized clinical trial comparing enamel matrix derivative and membrane treatment of buccal Class II furcation involvement in mandibular molars. Part I: Study design and results for primary outcomes
J Periodontol. 2004 Aug;75(8):1150-60.
jump to Study ! jump to Ref !

A randomized clinical trial comparing Enamel Matrix Derivative and membrane treatment of buccal class II
furcation involvement in madibular molars. Part I: study design and results for primary outcome
Jepsen S, Heinz B, Jepsen K, Arjomand M, Hoffmann T, Richter S, Reich E, Sculean A, Gonzales JR, Bödeker RH, Meyle J.
J Periodontol. 2004 Aug;75(8):1150-60.
STRAUMANN® 60Jepsen S, Heinz B, Jepsen K, Arjomand M, Hoffmann T, Richter S, Reich E, Sculean A, Gonzales JR, Bödeker RH, Meyle J.J Periodontol. 2004 Aug;75(8):1150-60.
Goal• To compare Emdogain with bioabsorbable barrier membranes for the treatment
of mandibular buccal class II furcation defects
Methodology• Randomized, controlled, multicenter clinical trial
• 45 patients
• 90 buccal Class II furcation defects on contralateral molars
• Horizontal probing depth >3mm
• Defects were randomly assigned to the Emdogain or the guided tissue regeneration (GTR) group according to a split-mouth design
Enamel matrix derivative and membrane treatment of buccal Class II furcation involvement in mandibular molars
STRAUMANN® 61
Results
0
5
10
15
20
Emdogain GTR
% d
efec
ts
18%
7%
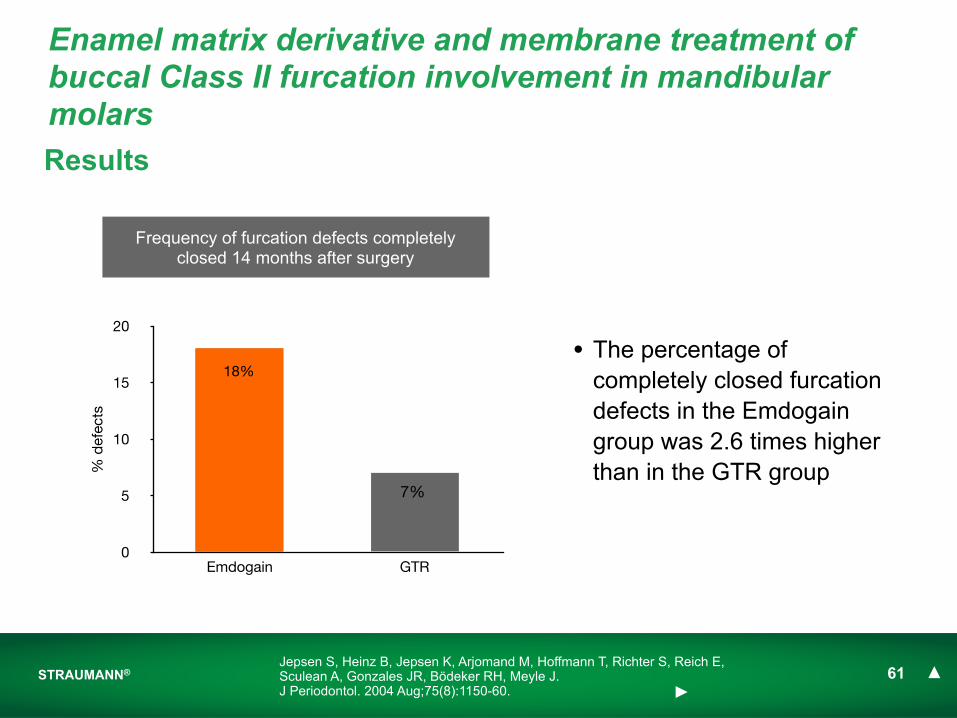
Frequency of furcation defects completely closed 14 months after surgery
Jepsen S, Heinz B, Jepsen K, Arjomand M, Hoffmann T, Richter S, Reich E, Sculean A, Gonzales JR, Bödeker RH, Meyle J.J Periodontol. 2004 Aug;75(8):1150-60.
Enamel matrix derivative and membrane treatment of buccal Class II furcation involvement in mandibular molars
• The percentage of completely closed furcation defects in the Emdogain group was 2.6 times higher than in the GTR group
STRAUMANN® 62
Results
Jepsen S, Heinz B, Jepsen K, Arjomand M, Hoffmann T, Richter S, Reich E, Sculean A, Gonzales JR, Bödeker RH, Meyle J.J Periodontol. 2004 Aug;75(8):1150-60.
Enamel matrix derivative and membrane treatment of buccal Class II furcation involvement in mandibular molars
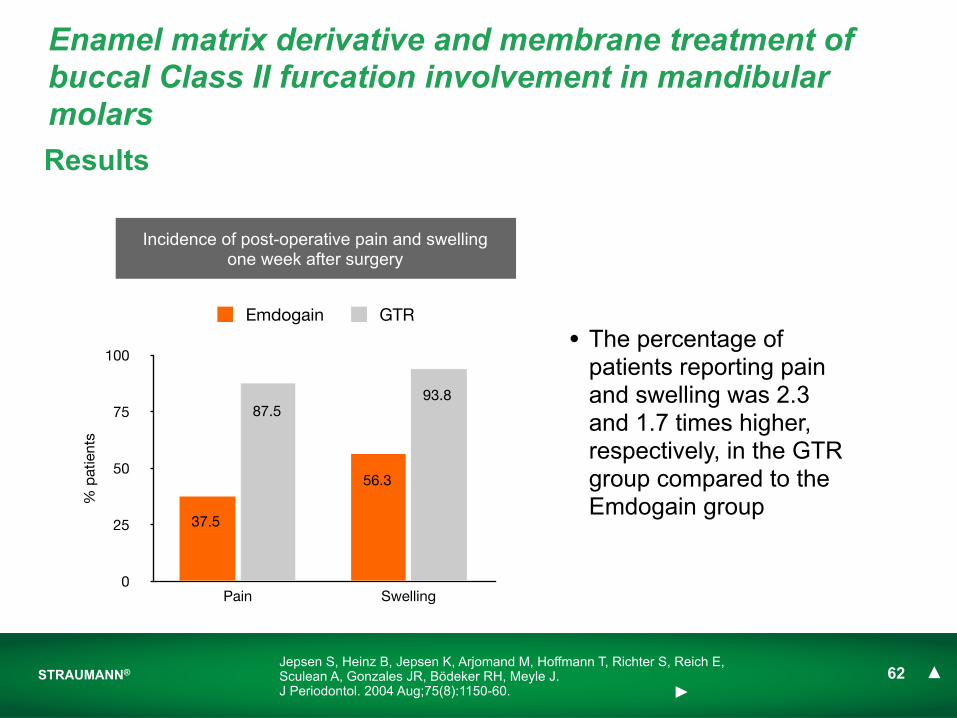
Incidence of post-operative pain and swelling one week after surgery
0
25
50
75
100
Pain Swelling
% p
atie
nts
Emdogain GTR
87.5
56.3
93.8
37.5
• The percentage of patients reporting pain and swelling was 2.3 and 1.7 times higher, respectively, in the GTR group compared to the Emdogain group
STRAUMANN® 63
• The application of Emdogain resulted in a significantly higher percentage of completely closed furcation defects compared to the use of standard membrane in the treatment of buccal mandibular Class II defects
• The study showed that fewer adverse events and postoperative complications during the early healing period were found with the use of Emdogain resulting in less discomfort for the patient
Conclusions
Jepsen S, Heinz B, Jepsen K, Arjomand M, Hoffmann T, Richter S, Reich E, Sculean A, Gonzales JR, Bödeker RH, Meyle J.J Periodontol. 2004 Aug;75(8):1150-60.
Enamel matrix derivative and membrane treatment of buccal Class II furcation involvement in mandibular molars
Long-term data May 25, 2011
Straumann® Emdogain
Sun
January, 2011January, 2011January, 2011
Mon Tue Wed Thu Fri Sat
2
9
16
23
27 28 29 30 31 1
3 4 5 6 7 8
10 11 12 13 14 15
17 18 19 20 21 22
24 25 26 27 28 29
STRAUMANN® 65
Straumann® EmdogainPublication First AuthorFirst Author Full Author List Full Title Reference
1 Heden G Heden G, Wennström JL Five-year follow-up of regenerative periodontal therapy with enamel matrix derivative at sites with angular bone defects. J Periodontol. 2006 Feb;77(2):295-301.
2 Sculean ASculean A, Kiss A, Miliauskaite A, Schwarz F, Arweiler NB, Hannig M.
Ten-year results following treatment of intra-bony defects with enamel matrix proteins and guided tissue regeneration
J Clin Periodontol. 2008 Sep;35(9):817-24
jump to Study ! jump to Ref !
Five-year follow-up of regenerative periodontal therapy with enamel matrix derivative at sites with angular bony
defects
Heden G, Wennström JLJ Periodontol. 2006 Feb;77(2):295-301.
STRAUMANN® 67Heden G, Wennström JLJ Periodontol. 2006 Feb;77(2):295-301.
Goal• To analyze the long-term stability of clinical attachment level gain following
regenerative therapy with the use of Emdogain in intrabony defects
Methodology• Case series report
• 82 patients with at least one deep proximal intrabony defect
• 102 defects included in the analysis
• Defect probing depth ≥5mm, clinical attachment loss ≥6mm, radiographic intrabony component ≥3mm
Five-year follow-up of regenerative periodontal therapy with enamel matrix derivative at sites with angular bone defects
-6.0
-4.5
-3.0
-1.5
0
Mea
n an
d 9
5% C
I (m
m)
Probing depth (PD)Clinical attachment level (CAL)
STRAUMANN® 68
Results
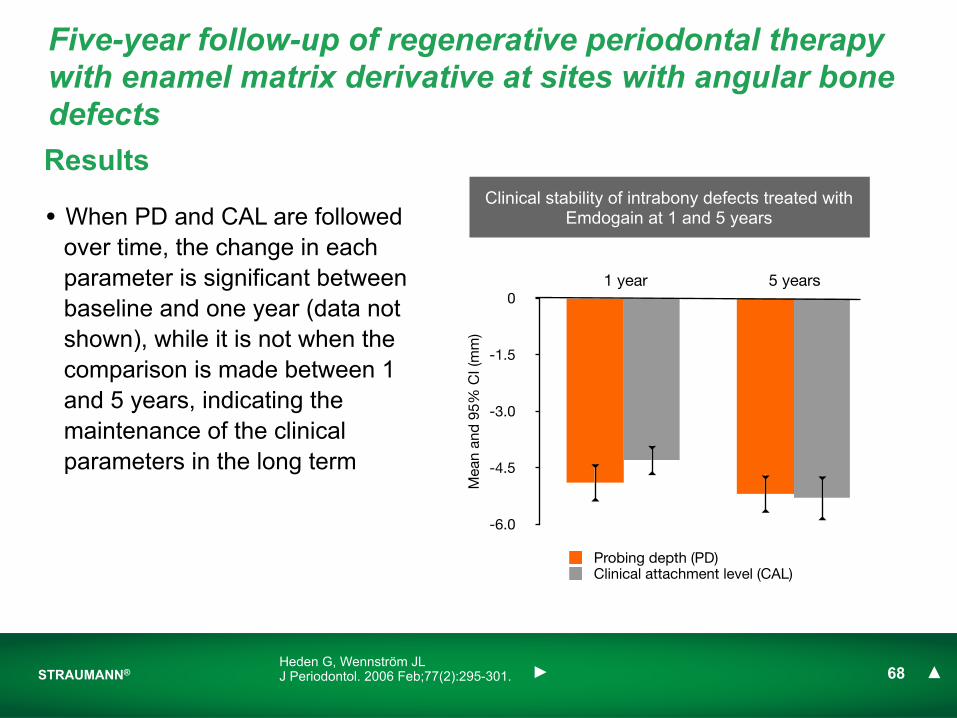
• When PD and CAL are followed over time, the change in each parameter is significant between baseline and one year (data not shown), while it is not when the comparison is made between 1 and 5 years, indicating the maintenance of the clinical parameters in the long term
1 year 5 years
Clinical stability of intrabony defects treated with Emdogain at 1 and 5 years
Heden G, Wennström JLJ Periodontol. 2006 Feb;77(2):295-301.
Five-year follow-up of regenerative periodontal therapy with enamel matrix derivative at sites with angular bone defects
STRAUMANN® 69
• The use of Emdogain intrabony defects demonstrated 5-years-stability of clinical attachment level (CAL) gain and probing depth (PD) recession following regenerative therapy
Conclusion
Heden G, Wennström JLJ Periodontol. 2006 Feb;77(2):295-301.
Five-year follow-up of regenerative periodontal therapy with enamel matrix derivative at sites with angular bone defects
Ten-year results following treatment of intrabony defects with enamel matrix proteins and guided tissue
regeneration
Sculean A, Kiss A, Miliauskaite A, Schwarz F, Arweiler NB, Hannig M.J Clin Periodontol. 2008 Sep;35(9):817-24.
STRAUMANN® 71Sculean A, Kiss A, Miliauskaite A, Schwarz F, Arweiler NB, Hannig M.J Clin Periodontol. 2008 Sep;35(9):817-24.
Goal• To evaluate the 10-year results of intrabony defects treated with:
i) Emdogainii) guided tissue regeneration (GTR)iii) the combination of Emdogain and GTRiv) the open flap debridment (OFD) technique
Methodology• Randomized, controlled clinical trial
• 38 patients displaying one intrabony defect
• Probing depth of the defects was ≥6mm
• Randomized assignment of the patients to one of the 4 treatment group
• The patients included in this study were those who regularly attended the maintenance care program (four visits a year, including oral hygiene reinforcement and professional tooth cleaning)
Ten-year results following treatment of intra-bony defects with enamel matrix proteins and guided tissue regeneration
STRAUMANN® 72
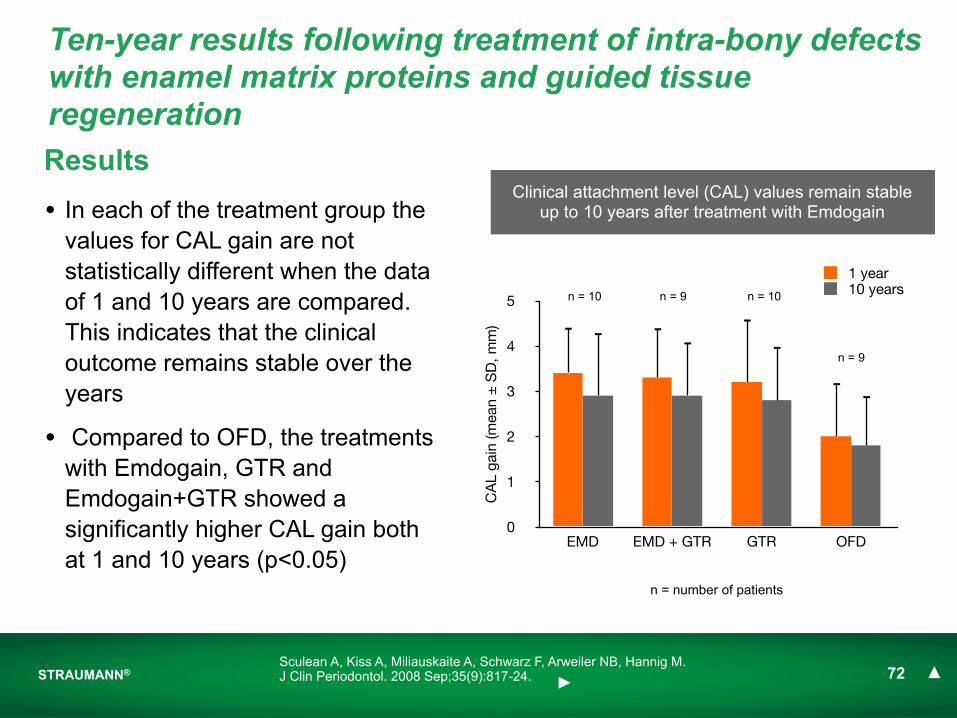
Results
0
1
2
3
4
5
EMD EMD + GTR GTR OFD
CA
L ga
in (m
ean
± S
D, m
m)
1 year10 years
Clinical attachment level (CAL) values remain stable up to 10 years after treatment with Emdogain• In each of the treatment group the
values for CAL gain are not statistically different when the data of 1 and 10 years are compared. This indicates that the clinical outcome remains stable over the years
• Compared to OFD, the treatments with Emdogain, GTR and Emdogain+GTR showed a significantly higher CAL gain both at 1 and 10 years (p<0.05)
Sculean A, Kiss A, Miliauskaite A, Schwarz F, Arweiler NB, Hannig M.J Clin Periodontol. 2008 Sep;35(9):817-24.
Ten-year results following treatment of intra-bony defects with enamel matrix proteins and guided tissue regeneration
n = 10 n = 10n = 9
n = 9
n = number of patients
STRAUMANN® 73
• The results of this long-term study indicate that the good clinical results obtained with Emdogain are stable and can be maintained over a period of 10 years
Conclusion
Sculean A, Kiss A, Miliauskaite A, Schwarz F, Arweiler NB, Hannig M.J Clin Periodontol. 2008 Sep;35(9):817-24.
Ten-year results following treatment of intra-bony defects with enamel matrix proteins and guided tissue regeneration





























