Embed Size (px)
Citation preview
Straumann Emdogaintm with a ConnECtivE tiSSuE graft to trEat rECESSion dEfECtS
gingival recession is a common finding among patients and can lead to esthetic concerns and thermal sensitivity. among the most common etiologies are mechanical trauma from brushing and flossing in combination with a thin gingival biotype susceptible to recession. occlusal trauma and frenum pull are considered co-factors in the recession process.
various soft tissue grafting techniques have been developed to address this problem and have mostly included the transplantation of autogenous tissue in combination with a coronally advanced flap. other techniques included pedicle flaps, guided tissue regeneration, and the use of allograft materials.
advances in technology have improved the predictability of root coverage procedures. treatment with enamel matrix proteins in conjunction with a coronally advanced flap (Caf) has been shown to be an effective treatment modality with reduced morbidity for patients.1,3 Enamel matrix proteins have been clinically observed to enhance wound healing1 and promote regeneration of periodontal tissues on previously denuded root surfaces.2 the technique also allows clinicians to treat up to a full arch of multiple recession lesions in one appointment
and obtain predictable results.3 this procedure may be more effective when mobilizing tissues that are of adequate quality with a minimal amount of keratinized tissue, emphasizing the importance of case selection. if the tissue quality is not adequate, alternative treatment options should be considered, such as the addition of an autogenous subepithelial connective tissue graft (SCtg).
the following case report demonstrates the use of a coronally advanced flap with a subepithelial connective tissue graft and enamel matrix proteins (Straumann Emdogain).
Case Reporta healthy 28-year-old female patient presented with chief complaints of root exposure and sensitivity to thermal change in specific maxillary teeth. the patient had previous history of orthodontic treatment.
Straumann® Emdogaintm application in conjunction with subepithelial connective tissue grafting was planned to treat the patient’s gingival recession (miller Class i) of approximately 4.0 – 7.0 mm at teeth #13, 14, 23 and 24 (fdi).
Arnold Todd McClain, DDS Practice of Periodontal & Implant Surgery durham, north Carolina
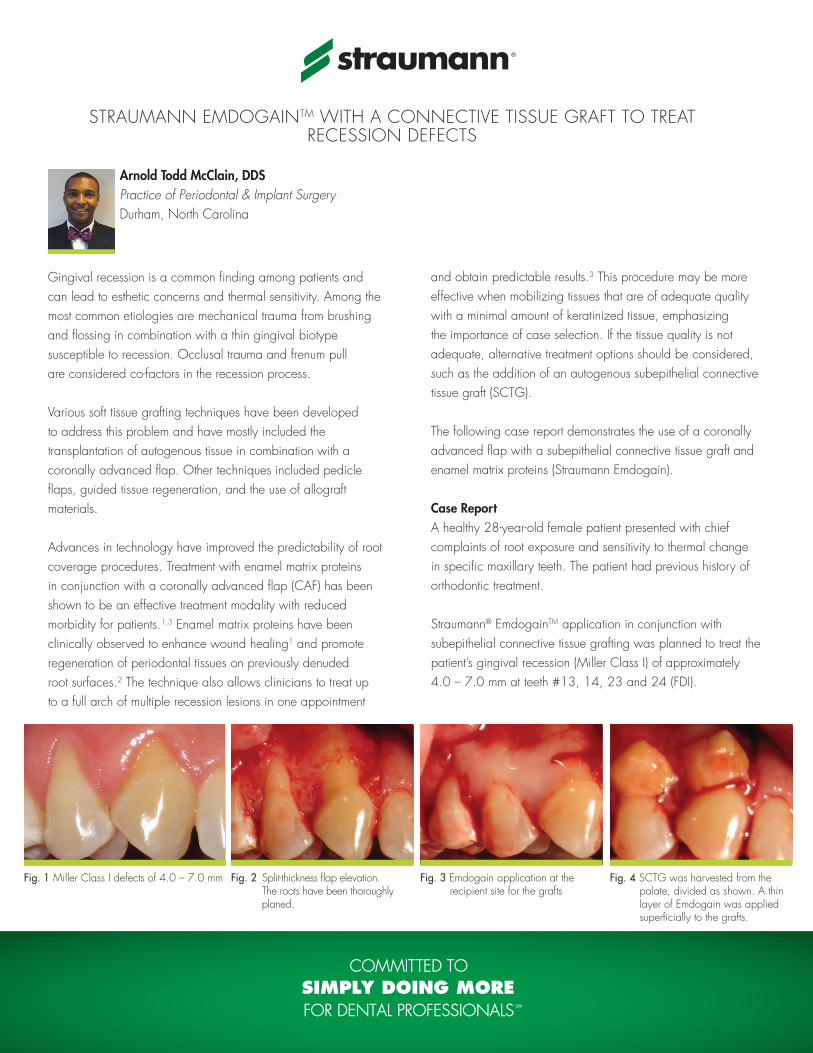
Fig. 1 miller Class i defects of 4.0 – 7.0 mm Fig. 2 Split-thickness flap elevation. the roots have been thoroughly planed.
Fig. 3 Emdogain application at the recipient site for the grafts
Fig. 4 SCtg was harvested from the palate, divided as shown. a thin layer of Emdogain was applied superficially to the grafts.
the correction of gingival defects was accomplished over two surgical visits, with teeth #13 and 14 addressed first.
Split-thickness flaps were raised at the affected areas after administration of local anesthetic. the roots of the teeth were thoroughly planed under irrigation using an ultrasonic instrument. Emdogain was applied to the recipient sites, followed by the connective tissue grafts. the grafts were then covered with a thin
layer of Emdogain. the split-thickness flaps were advanced coronally and superficially to the grafts. Chromic gut sutures (4-0 gauge) were used to secure both flaps and grafts. the flaps were secured coronally at the level of the interdental papillae.
the patient was instructed to use chlorhexidine rinse for a period of one week post-operative. the patient was monitored at three weeks, two months, and four months post-operative.
Fig. 9 a Caf with Emdogain application and SCtg was implemented
Fig. 10 Postoperative healing at 4 months
© Straumann uSa, LLC 2011. all rights reserved. Straumann® and/or other trademarks and logos from Straumann® that are mentioned herein are the trademarks or registered trademarks of Straumann holding ag and/or its affiliates.
International Headquartersinstitut Straumann ag Peter merian-weg 12Ch-4002 Basel, SwitzerlandPhone +41 (0)61 965 11 11fax +41 (0)61 965 11 01
Straumann USAStraumann uSa, LLC 60 minuteman road andover, ma 01810 Phone 800/448 8168 978/747 2500 fax 978/747 2490 www.straumannusa.com
Straumann CanadaStraumann Canada Limited 3115 harvester road, Suite 100Burlington, on L7n 3n8 Phone 800/363 4024 905/319 2900 fax 905/319 2911 www.straumann.ca
Arnold Todd McClain, DDSPractice of Periodontal & Implant Surgery (est. 2001)durham, north Carolina
Dr. Arnold Todd McClain earned his doctor of dental Surgery from howard university in washington, dC, after receiving a Bachelor of Science in Electrical Engineering from north Carolina State university. he holds a Certificate of Speciality in Periodontology as well as a master of Science from the university of north Carolina at Chapel hill. dr. mcClain currently has a practice of periodontal and implant surgery in durham, north Carolina, and is a diplomate of the american Board of Periodontology.
arnold todd mcClain, ddSPractice of Periodontal & Implant Surgery5015 Southport drive, Suite 130durham, nC 27713www.gumsandimplants.org
References1. mcguire m.K. and nunn m. J Periodontol 2003; 74:
1110-11252. mcguire mK et al. J Periodontol 2003; 74:1126-11353. Cairo et al., treatment of gingival recession with coronally
advanced flap procedures: a systematic review. J Clin Periodontol 2008; 35 (Suppl 8): 136-162.
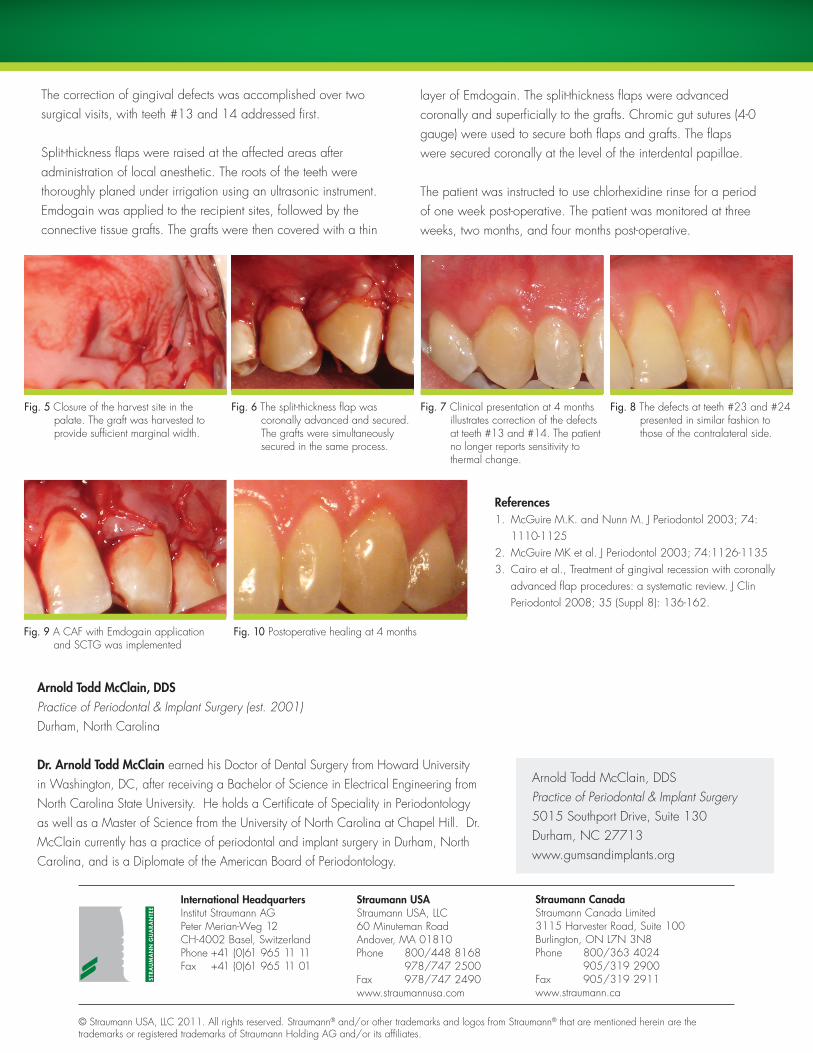
Fig. 5 Closure of the harvest site in the palate. the graft was harvested to provide sufficient marginal width.
Fig. 6 the split-thickness flap was coronally advanced and secured. the grafts were simultaneously secured in the same process.
Fig. 7 Clinical presentation at 4 months illustrates correction of the defects at teeth #13 and #14. the patient no longer reports sensitivity to thermal change.
Fig. 8 the defects at teeth #23 and #24 presented in similar fashion to those of the contralateral side.








![Enamel matrix derivative (Emdogain(R)) for periodontal ... · [Intervention Review] Enamel matrix derivative (Emdogain®) for periodontal tissue regeneration in intrabony defects](https://img.pdfslide.us/doc/110x75/5f552cf7423b6b423a7f833d/enamel-matrix-derivative-emdogainr-for-periodontal-intervention-review.jpg)
![Enamel matrix derivative [Emdogain(R)] for …...[Intervention Review] Enamel matrix derivative (Emdogain®) for periodontal tissue regeneration in intrabony defects Marco Esposito1,](https://img.pdfslide.us/doc/110x75/5e7b0259219c7e285a26632d/enamel-matrix-derivative-emdogainr-for-intervention-review-enamel-matrix.jpg)



















