Embed Size (px)
Citation preview
1
CAPT Webinar
Strategies to Reduce the Harm of Prescription Drug Misuse
May 30, 2017
Findings from the Research Literature
Josh Esrick, Policy Analyst, SAMHSA’s CAPT
Shai Fuxman, Senior Training and Technical Assistance Associate, SAMHSA’s CAPT
2
Facilitator
Molly LoweAssociate Director of Training and Technical Assistance
SAMHSA’s CAPT
2
3
This training was developed under the Substance Abuse and Mental Health Services Administration’s Center for the
Application of Prevention Technologies task order. Reference #HHSS283201200024I/HHSS28342002T.
The views expressed in this webinar do not necessarily represent the views, policies, and positions of the Substance Abuse and Mental Health Services Administration or the U.S.
Department of Health and Human Services.
This webinar is being recorded and archived, and will be available to all webinar participants. Please contact the
webinar facilitator if you have any concerns or questions.
4
Objectives
• Define the core components of strategies toprevent both fatal and nonfatal overdose fromprescription drugs
• Identify potential advantages and disadvantagesof strategies to reduce the harm of prescriptiondrugs
• Describe the need for developing acomprehensive approach to reducing the non-medical use of prescription drugs and preventingoverdoses

3
5
Preventing Prescription Drug Misuse: Strategies from the Research Literature
Strategies to Reduce Demand (4/13)
Strategies to Reduce Demand (4/13)
Strategies to Reduce Supply (4/27)
Strategies to Reduce Supply (4/27)
Strategies to Reduce Harm (Today)
Strategies to Reduce Harm (Today)
6
Presenters
Josh EsrickPolicy Analyst
SAMHSA’s CAPT
Shai FuxmanSenior T/TA Associate
SAMHSA’s CAPT
4
7
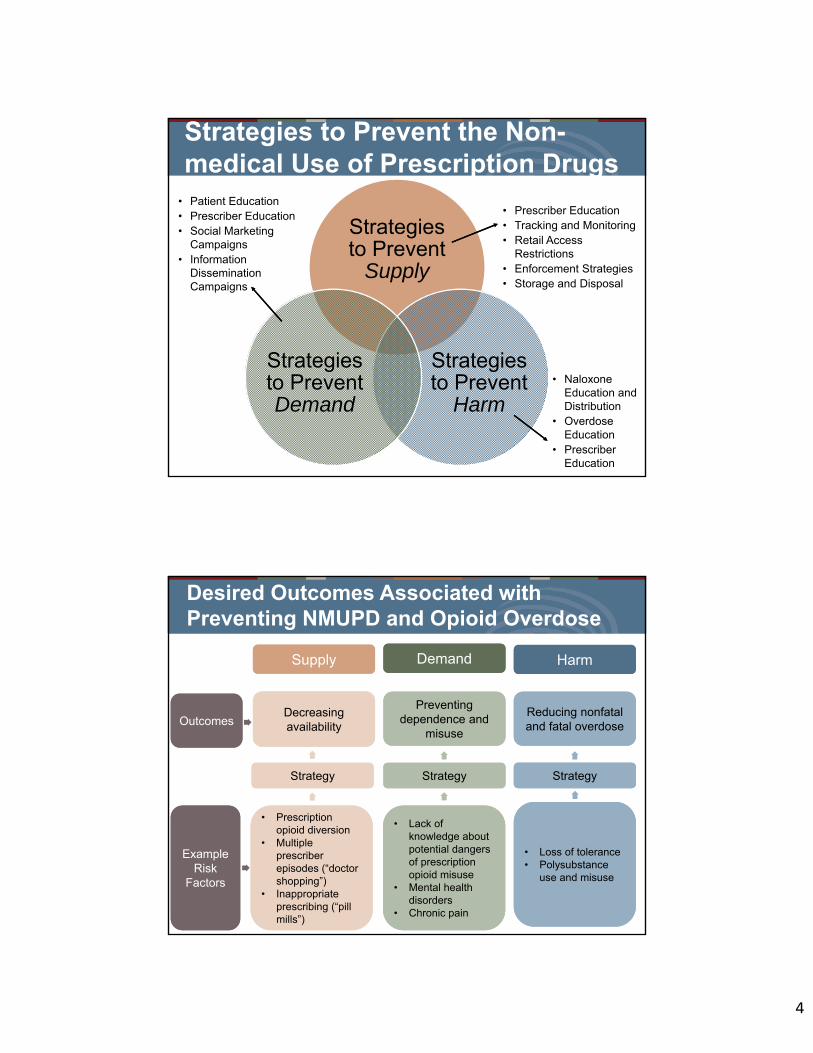
Strategies to Prevent the Non-medical Use of Prescription Drugs
Strategies to Prevent
Supply
Strategies to Prevent
Harm
Strategies to Prevent Demand
• Patient Education• Prescriber Education• Social Marketing
Campaigns• Information
DisseminationCampaigns
• Prescriber Education• Tracking and Monitoring• Retail Access
Restrictions• Enforcement Strategies• Storage and Disposal
• NaloxoneEducation andDistribution
• OverdoseEducation
• PrescriberEducation
8
Desired Outcomes Associated with Preventing NMUPD and Opioid Overdose
HarmHarmDemandDemandSupplySupply
Decreasing availabilityDecreasing availability
Preventing dependence and
misuse
Preventing dependence and
misuse
Reducing nonfatal and fatal overdoseReducing nonfatal and fatal overdose
• Prescriptionopioid diversion
• Multipleprescriberepisodes (“doctorshopping”)
• Inappropriateprescribing (“pillmills”)
• Prescriptionopioid diversion
• Multipleprescriberepisodes (“doctorshopping”)
• Inappropriateprescribing (“pillmills”)
• Lack ofknowledge aboutpotential dangersof prescriptionopioid misuse
• Mental healthdisorders
• Chronic pain
• Lack ofknowledge aboutpotential dangersof prescriptionopioid misuse
• Mental healthdisorders
• Chronic pain
• Loss of tolerance• Polysubstance
use and misuse
• Loss of tolerance• Polysubstance
use and misuse
OutcomesOutcomes
Example Risk
Factors
Example Risk
Factors
Strategy Strategy Strategy Strategy Strategy Strategy
5
9
Evidence-Based Continuum1
Promising/Emerging/
Undetermined
Promising/Emerging/
Undetermined
Supported/Well-Supported
Supported/Well-Supported
10
A Note About Evidence
• There is less evidence for NMUPDprevention strategies (compared tostrategies for preventing othersubstances).
• A lack of evidence does not mean that astrategy is ineffective.
• Practitioners should rely on experienceworking with other substances.
• It is important for practitioners to collectevaluation data to build the evidencearound strategies.
6
11
Opioid Use and Misuse
Strategies to Reduce the Harm of Prescription Drug MisuseFindings From the Research Literature
12
Defining Harm Reduction Strategies
Efforts aimed at decreasing fatal and nonfatal overdoses from both prescription and illicit opioids (such as heroin).
7
13
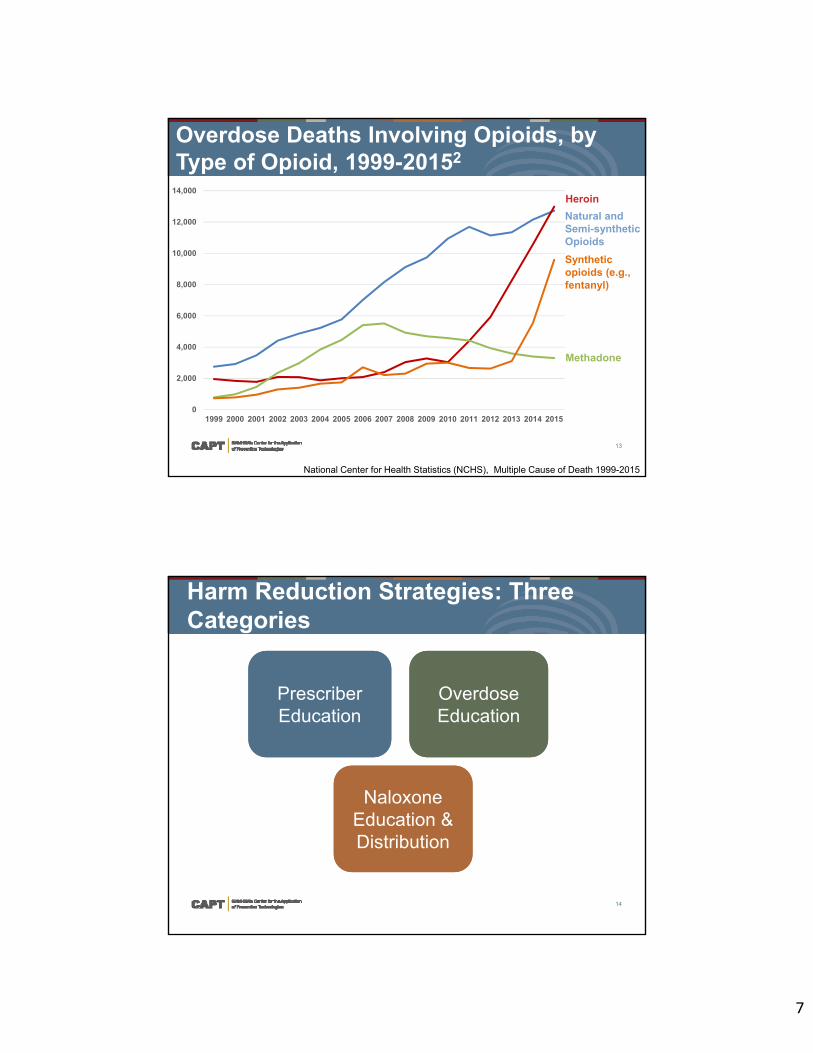
Overdose Deaths Involving Opioids, by Type of Opioid, 1999-20152
National Center for Health Statistics (NCHS), Multiple Cause of Death 1999-2015
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Heroin
Natural and Semi-synthetic Opioids
Synthetic opioids (e.g., fentanyl)
Methadone
14
Harm Reduction Strategies: Three Categories
Overdose EducationOverdose Education
Naloxone Education & Distribution
Naloxone Education & Distribution
Prescriber EducationPrescriber Education

8
15
Is your state, tribe, jurisdiction,
or community currently
implementing any harm reduction
strategies?
16
Prescriber Education3,4,5,6
Involves teaching prescribers:
• How to recognize an individual at risk
• When/how to refer a patient totreatment
• How to talk to patients about thedanger of overdose
• About using tools to identify cases ofpoly-substance use
• About strategies to prevent overdosedeaths
9
17
Overdose Prevention Strategies that Involve Prescribers7,8
• Prescribing naloxoneto patients atincreased risk ofoverdose
• Writing third-partynaloxoneprescriptions tofamily members andpeers
Prescriber EducationPrescriber Education
18
For More Information Prescriber Education
For more information on venues and delivery methods for prescriber education, visit https://captconnect.edc.org/to access the materials from the first webinar in this series.
10
19
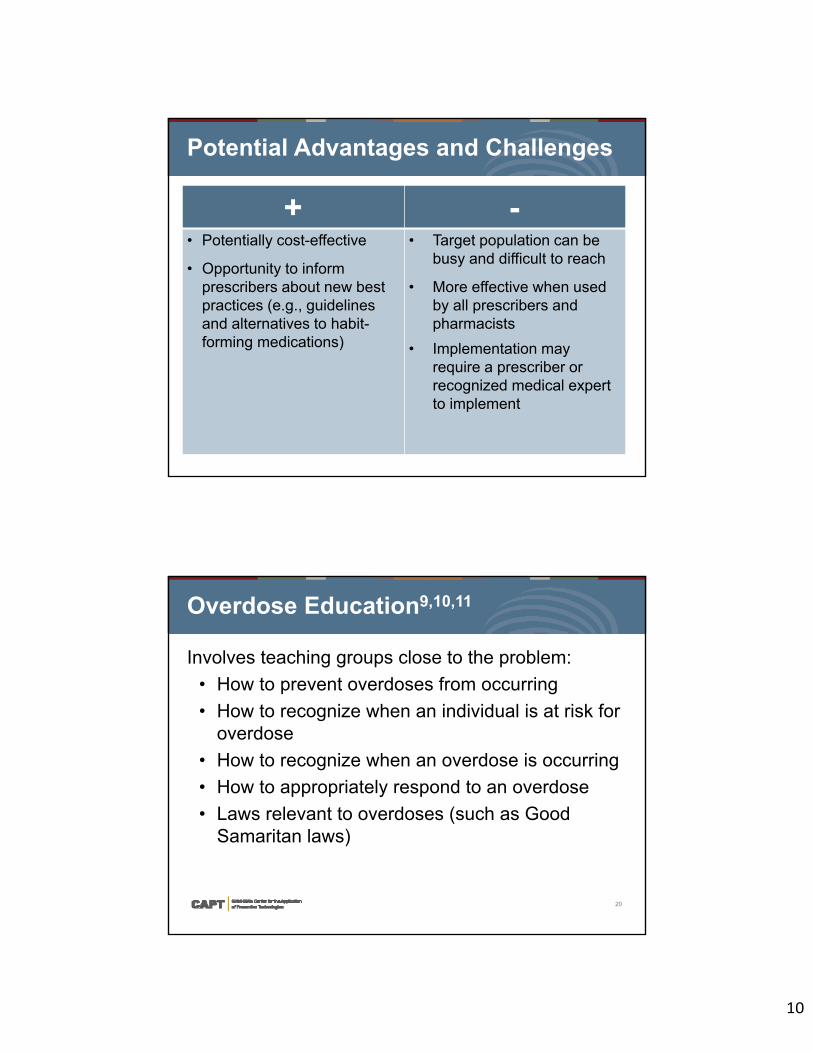
Potential Advantages and Challenges
+ -• Potentially cost-effective
• Opportunity to informprescribers about new bestpractices (e.g., guidelinesand alternatives to habit-forming medications)
• Target population can bebusy and difficult to reach
• More effective when usedby all prescribers andpharmacists
• Implementation mayrequire a prescriber orrecognized medical expertto implement
20
Overdose Education9,10,11
Involves teaching groups close to the problem:
• How to prevent overdoses from occurring
• How to recognize when an individual is at risk foroverdose
• How to recognize when an overdose is occurring
• How to appropriately respond to an overdose
• Laws relevant to overdoses (such as GoodSamaritan laws)
11
21
Potential Audiences for Overdose Education Strategies
Health Care ProfessionalsHealth Care Professionals
Professional First Responders
Professional First Responders
People Who Use Opioids Illicitly People Who Use Opioids Illicitly
People Who use Prescription Opioids
Medically
People Who use Prescription Opioids
Medically
Overdose EducationOverdose Education
Family Members of People Who Use Opioids Illicitly
Family Members of People Who Use Opioids Illicitly
22
Law Enforcement Training on Harm Reduction12,13,14,16,16,17
Involves preparing law enforcement to better respond to and prevent drug overdoses. Topics include:
• Purpose of harm-reduction training
• Foundational information on prescription drugsand other opioids
• Signs and symptoms of an overdose
• Purpose of naloxone, how it works, and how toadminister it
Overdose EducationOverdose Education
12
23
Overdose Education for People Who Use Drugs18,19,20,21,22,23 Overdose
EducationOverdose Education
Informs people who use drugs about:
• Behaviors that increaseoverdose risk (such aschange in tolerance, mixingsubstances)
• How to recognize when anoverdose is occurring
• Steps to take whenwitnessing an overdose
Photo source: http://findings.org.uk/PHP/dl.php?file=Horyniak_D_1.cab&s=d
24
Good Samaritan Education24
• Intended to raise awareness of GoodSamaritan laws and policies, and thespecific protections they provide, andbuild confidence in them.
• Audiences include:
o Law enforcement and criminaljustice professionals
o Members of the drug-usingcommunity
o Lay first responders
Overdose EducationOverdose Education
13
25
Potential Advantages and Challenges
+ -• Can raise
awareness ofdangers ofopioid misuse
• Can becombined withnaloxonedistribution
• Warning about dangerous substances onthe market can lead individuals withdependence to seek out other harmfulsubstances
• Good Samaritan laws are only effective ifboth law enforcement and potential 9-1-1callers are educated
• Good Samaritan laws and policies are notpresent in all states
• Accessing people who use drugs (andtheir friends/families) can be challenging
26
Participant Questions
14
27
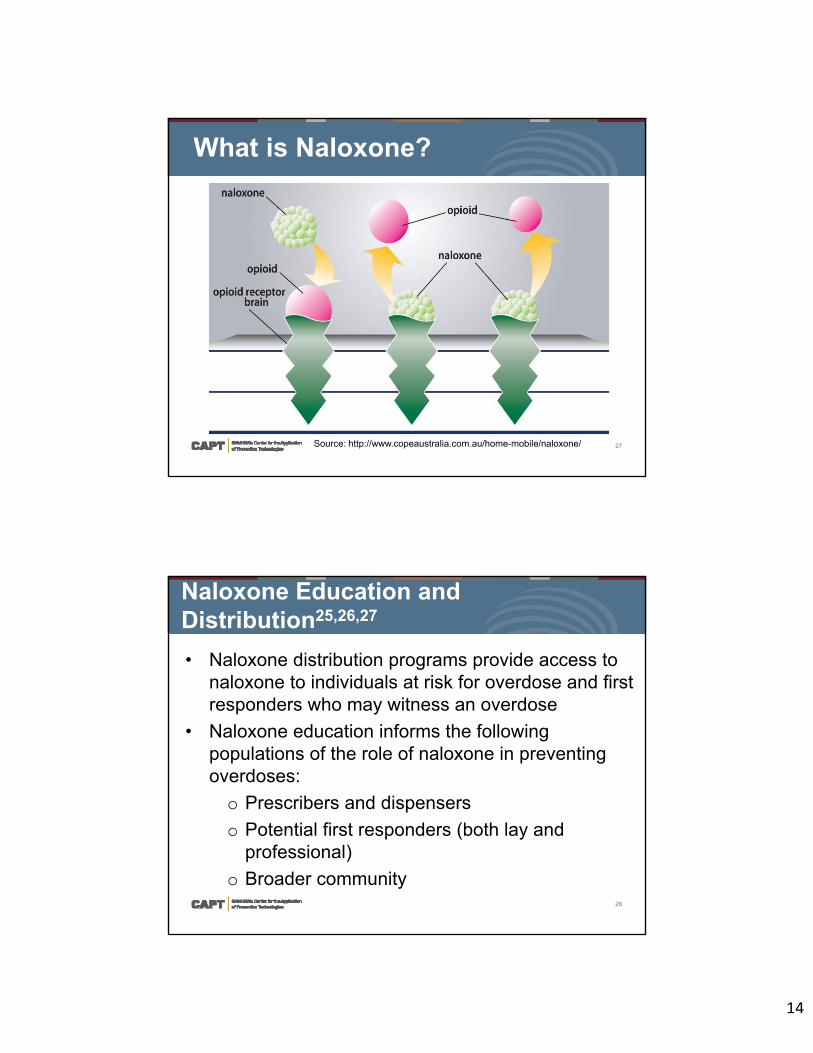
What is Naloxone?
Source: http://www.copeaustralia.com.au/home-mobile/naloxone/
28
Naloxone Education and Distribution25,26,27
• Naloxone distribution programs provide access tonaloxone to individuals at risk for overdose and firstresponders who may witness an overdose
• Naloxone education informs the followingpopulations of the role of naloxone in preventingoverdoses:
o Prescribers and dispensers
o Potential first responders (both lay andprofessional)
o Broader community
15
29
State Naloxone Access Laws28,29
• Allow naloxone to beprescribed/dispensed to:
o substance users withdocumented risk factorsfor overdose
o lay administrators(nonmedical firstresponders, potentialoverdose bystanders,family and friends ofopioid users)
Naloxone Education and
Distribution
Naloxone Education and
Distribution
30
• Traditional prescriptions
• Third-party prescriptions
• Collaborative practiceagreements
• Standing orders
• Protocol orders
Types of Naloxone Access
16
31
Overdose Education and Naloxone Distribution Programs27,29,30,31,32,33
• Overdose education andnaloxone distribution(OEND) programs providetraining on:
o recognizing andpreventing opioidoverdoses
o how to administernaloxone.
Naloxone Education and
Distribution
Naloxone Education and
Distribution
• Program participants are also provided prescriptionsfor naloxone
32
Potential Audiences for OEND Programs
Naloxone Education and
Distribution
Naloxone Education and
Distribution
• Mental health centers
• Treatment facilities(including methadoneclinics)
• Homeless shelters
• Veterans’ Affairsfacilities
• People who use opioids(and their family andfriends)
• Professional and lay firstresponders
• Broader community
17
33
Project Lazarus8,34,35,36
Project Lazarus addresses drug overdose deaths, with a focus on prescription drug overdoses. Its overdose prevention program includes:
• Community activation and coalition building
• Monitoring and epidemiological surveillance
• Prescriber, patient, and law enforcement trainingand education
• Overdose reversal medication
https://www.projectlazarus.org/
Naloxone Education and
Distribution
Naloxone Education and
Distribution
34
Potential Advantages and Challenges
+ -• Reduces rates of overdose
deaths
• When naloxone isadministered by aprofessional first responder,individuals who use drugscan be referred to services
• The education component ofthese strategies promotesproper use of naloxone
• Can reduce fatalities but notthe underlying substanceuse disorders
• Prevention practitioners mayface critiques that givingnaloxone to people who usedrugs could encouragefurther use
18
35
Additional Strategies to Note
36
Efforts to Connect Individuals to Treatment38
• Increase access and connect individuals totreatment for substance use disorders, especiallymedication-assisted treatment (MAT).
• MAT involves integrating medications (e.g.,methadone, buprenorphine, naltrexone) inconjunction with behavioral therapies and counselingto treat opioid addiction.
https://www.samhsa.gov/medication-assisted-treatment
19
37
Strategies to Reduce Non-opioid Prescription Overdoses
• Antidotes (e.g., Flumazenilfor benzodiazepineoverdoses)
• Guidance for prescribers(e.g., risks associated withmixing prescriptions)
• Safe storagerecommendations to preventaccidental poisonings
38
Participant Questions
20
39
A Comprehensive Approach to Reduce NMUPD and Opioid Overdose
40
Selection as Part of a Strategic Process
21
41
Developing a Comprehensive Approach to Reducing NMUPD and Opioid Overdose
Anytown, U.S.
42
Comprehensive Approach: Example
Risk Factors for Anytown Strategies for Anytown
Lack of knowledge about potential dangers of prescription opioid misuse
Social marketing campaign
Inappropriate prescribing Prescriber education
Polysubstance use Overdose education
Problem: Anytown experienced high rates of opioid overdose over the past five years
22
43
What NMUPD prevention
strategies are you currently
implementing or interested in
implementing?
• Patient education• Prescriber education• Social marketing campaigns• Information dissemination
campaigns• Tracking and monitoring• Retail access restrictions• Enforcement strategies• Proper storage and disposal• Overdose education• Naloxone education and
distribution
44
Where to Find Out MoreResources on Strategies to Reduce the Harm of Prescription Drug Misuse
23
45
SAMHSA Opioid Overdose Prevention Toolkit
• Facts for Community Members
• Five Essential Steps for FirstResponders
• Information for Prescribers
• Safety Advice for Patients &Family Members
• Recovery from Opioid Overdose
Available at store.samhsa.gov
46
Revised NMUPD Decision Support Tools
• Overview of Factors andStrategies
• Understanding Who is at Risk
• Programs and Strategies
Available at samhsa.gov/capt/
24
47
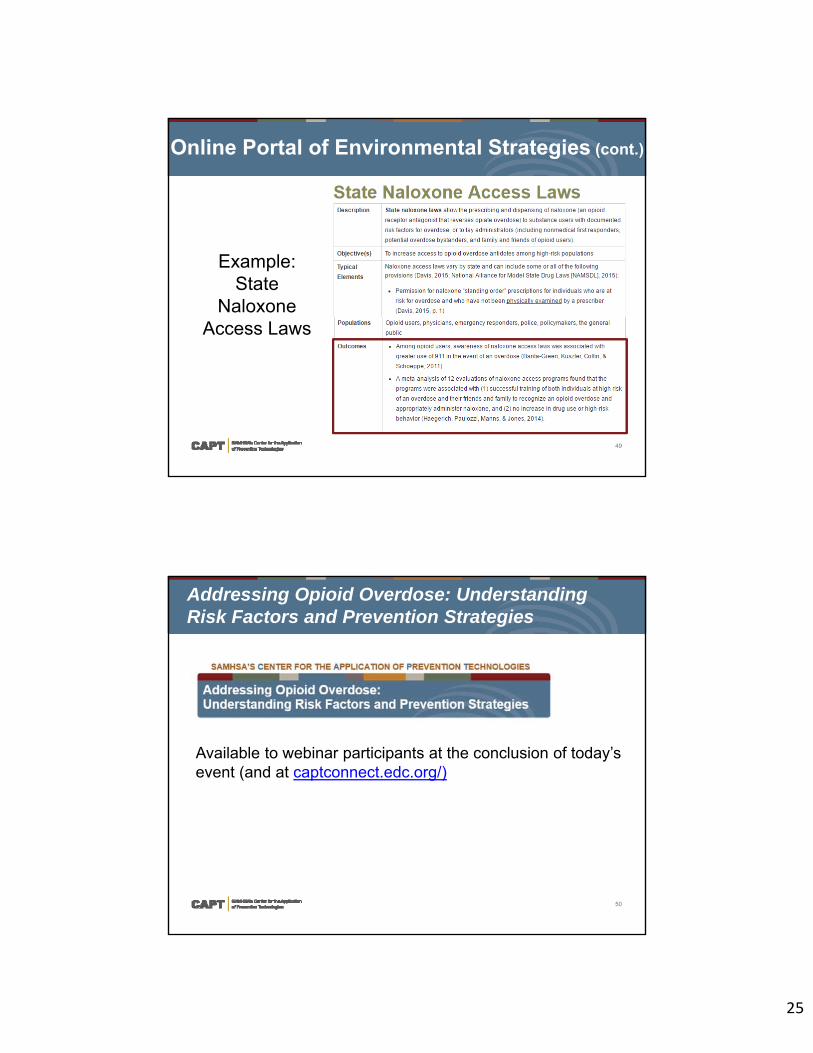
Revised NMUPD Decision Support Tools (cont.)
Example: Overdose
Education and Naloxone
Distribution Programs
48
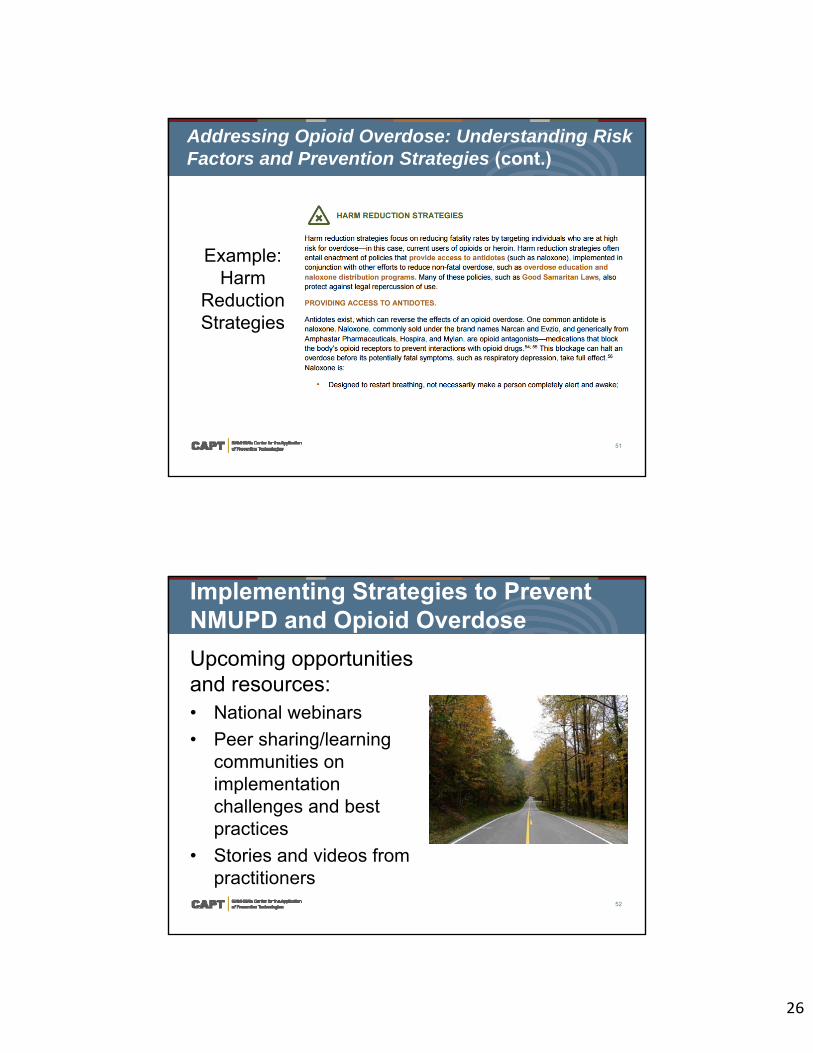
Online Portal of Environmental Strategies
Available to CSAP prevention grantees at captconnect.edc.org/
25
49
Example: State
Naloxone Access Laws
Online Portal of Environmental Strategies (cont.)
50
Addressing Opioid Overdose: Understanding Risk Factors and Prevention Strategies
Available to webinar participants at the conclusion of today’s event (and at captconnect.edc.org/)
26
51
Addressing Opioid Overdose: Understanding Risk Factors and Prevention Strategies (cont.)
Example: Harm
Reduction Strategies
52
Implementing Strategies to Prevent NMUPD and Opioid Overdose
Upcoming opportunities and resources:• National webinars
• Peer sharing/learningcommunities onimplementationchallenges and bestpractices
• Stories and videos frompractitioners
27
53
The CAPT is Here to Help
CAPT Resource Team Coordinator
Northeast Resource Team Gisela [email protected]
Central Resource Team Chuck [email protected]
Southeast Resource Team Lourdes [email protected]
Southwest Resource Team Marie [email protected]
West Resource Team Alyssa O’[email protected]
54
Contact Information
If you have questions or comments about this webinar, please don’t hesitate to contact:
Amanda DoughertyTraining and Technical Assistance Associate
312-962-4558
28
55
Evaluation
Please take the time to complete a brief feedback form:
https://www.surveymonkey.com/r/feedback-CAPT-1814
Thank you for sharing your thoughts!
56
References1. Puddy, R. W. & Wilkins, N. (2011). Understanding Evidence Part 1: Best Available Research Evidence. A Guide to the
Continuum of Evidence of Effectiveness. Atlanta, GA: Centers for Disease Control and Prevention.
2. United States Department of Health and Human Services (US DHHS), Centers for Disease Control and Prevention (CDC),National Center for Health Statistics (NCHS), Multiple Cause of Death 1999-2015 on CDC WONDER Online Database, released 2016. Data for year 2015 are compiled from the Multiple Cause of Death File 2015, Series 20, No. 2U, 2016.
3. Franklin, G. M., Mai, J., Turner, J., Sullivan, M., Wickizer, T., & Fulton-Kehoe, D. (2012). Bending the prescription opioid dosing and mortality curves: Impact of the Washington State opioid dosing guideline. American Journal of IndustrialMedicine, 55(4), 325-331.
4. American Medical Association. (2013). State Medical Licensure Requirements and Statistics (pp. 65-69): American Medical Association. Retrieved from https://www.acep.org/uploadedFiles/ACEP/CME/CME-State-CMERequirements_2013.pdf.
5. Lofwal, M. R., Wunsch, M. J., Nuzzo, P. A., & Walsh, S. L. (2011). Efficacy of continuing medical education to reduce the risk of buprenorphine diversion. Journal of Substance Abuse Treatment, 41(3), 321–329.
6. Cochella, S., & Bateman, K. (2012). Provider detailing: an intervention to decrease prescription opioid deaths in Utah. PainMedicine, 12(Suppl 2) S73–S76.
7. Albert, S., Brason II, F. W., Sanford, C. K., Dasgupta, N., Graham, J., & Lovette, B. (2011). Project Lazarus: Community-based overdose prevention in rural North Carolina. Pain Medicine, 12, S77-S85.
8. Project Lazarus. (n.d.b). Project Lazarus results for Wilkes County. Retrieved from http://projectlazarus.org/project-lazarus-results-wilkes-county
29
57
References9. Oliver, R. L., & Taylor, A. (2003). Chronic Opioid Rules: Prescribing opioids for chronic pain requires set rules, a written plan,
periodic re-evaluation, and vigilance to prevent illegal diversion of controlled substances. Practical Pain Management, 3(2), 1-8.
10. Albert, S., Brason Ii, F. W., Sanford, C. K., Dasgupta, N., Graham, J., & Lovette, B. (2011). Project Lazarus: Community-Based Overdose Prevention in Rural North Carolina. Pain Medicine, 12, S77-S85.
11. Davis, C. (2016). Legal interventions to reduce overdose mortality: Naloxone access and overdose Good Samaritan laws. Robert Wood Johnson Foundation. Retrieved from https://www.networkforphl.org/_asset/qz5pvn/naloxone-_FINAL.pdf
12. Bureau of Justice Assistance. (2014). Law enforcement naloxone toolkit. Washington, DC: U.S. Department of Justice. Retrieved from https://www.bjatraining.org/tools/naloxone/all
13. The Network for Public Health Law. (2014). Legal interventions to reduce overdose mortality: Naloxone access and overdose Good Samaritan laws. Retrieved from https://www.networkforphl.org/_asset/qz5pvn/network-naloxone-10-4.pdf
14. New York State Division of Criminal Justice Services. (2014). Opioid overdose and intranasal naloxone training for law enforcement: Trainer’s guide. Retrieved from https://www.bjatraining.org/sites/default/files/naloxone/Opioid%20Overdose%20Intranasal%20Naloxone%20Training%20-%20Trainer%20Guide.pdf
15. North Carolina Harm Reduction Coalition. (2015). Law enforcement departments carrying naloxone. Retrieved from http://www.nchrc.org/law-enforcement/us-law-enforcement-who-carry-naloxone/
16. U.S. Department of Justice. (2014). Attorney General Holder announces plans for federal law enforcement personnel to begin carrying naloxone. Retrieved from http://www.justice.gov/opa/pr/attorney-general-holder-announces-plans-federal-law-enforcement-personnel-begin-carrying
58
References17. Saucier, C. D., Zaller, N., Macmadu, A., & Green, T. C. (2016). An initial evaluation of law enforcement overdose training in
Rhode Island. Drug And Alcohol Dependence, 162, 211-218.
18. Bowser, B. P., Jenkins-Barnes, T., Dillard-Smith, C., & Lockett, G. (2010). Harm reduction for drug abusing ex-offenders: outcome of the California prevention and education project MORE project. Journal Of Evidence-Based Social Work, 7(1), 15-29.
19. Horyniak, D., Higgs, P., Lewis, J., Winter, R., Dietze, P., & Aitken, C. (2010). An evaluation of a heroin overdose prevention and education campaign. Drug And Alcohol Review, 29(1), 5-11.
20. Wagner, K. D., Valente, T. W., Casanova, M., Partovi, S. M., Mendenhall, B. M., Hundley, J. H., & ... Unger, J. B. (2010). Evaluation of an overdose prevention and response training programme for injection drug users in the Skid Row area of Los Angeles, CA. The International Journal On Drug Policy, 21(3), 186-193.
21. Maldjian, L., Siegler, A., & Kunins, H. V. (2016). Evaluation of overdose prevention trainings in New York City: Knowledge and self-efficacy among participants 12 months after training. Substance Abuse, 37(3), 459-465.
22. Winhusen, T., Theobald, J., Lewis, D., Wilder, C. M., & Lyons, M. S. (2016). Development and initial testing of a tailored telephone intervention delivered by peers to prevent recurring opioid-overdoses (TTIP-PRO). Health Education Research, 31(2),146-160.
23. Doyon, S., Klein-Schwartz, W., Anderson, B. A., & Welsh, C. (2013). A novel approach to informing the public about the risks ofoverdose and nonmedical use of prescription medications. The American Journal On Addictions, 22(2), 108-112.
24. Banta-Green, C. J., Kuszler, P. C., Coffin, P. O., & Schoeppe, J. A. (2011). Washington’s 911 Good Samaritan Drug Overdose Law - Initial Evaluation Results. Retrieved from Alcohol & Drug Abuse Institute, University of Washington: http://adai.uw.edu/pubs/infobriefs/ADAI-IB-2011-05.pdf
30
59
References25. Wheeler, E., Jones, T. S., Gilbert, M. K., & Davidson, P. J. (2015). Opioid Overdose Prevention Programs Providing
Naloxone to Laypersons — United States, 2014. Morbidity and Mortality Weekly Report (MMWR), 64(23), 631- 635.
26. Haegerich, T. M., Paulozzi, L. J., Manns, B. J., & Jones, C. M. (2014). What we know, and don’t know, about the impact ofstate policy and systems-level interventions on prescription drug overdose. Drug and Alcohol Dependence, 145, 34-47.
27. Green, T. C., Heimer, R., & Grau, L. E. (2008). Distinguishing signs of opioid overdose and indication for naloxone: an evaluation of six overdose training and naloxone distribution programs in the United States. Addiction, 103(6), 979-989.
28. Banta-Green, C. J., Kuszler, P. C., Coffin, P. O., & Schoeppe, J. A. (2011). Washington’s 911 Good Samaritan drug overdose law—Initial evaluation results. Seattle, WA: Alcohol and Drug Abuse Institute, University of Washington. Retrieved from http://adai.uw.edu/pubs/infobriefs/ADAI-IB-2011-05.pdf
29. Walley, A. Y., Doe-Simkins, M., Quinn, E., Pierce, C., Xuan, Z., & Ozonoff, A. (2013). Opioid overdose prevention with intranasal naloxone among people who take methadone. Journal of Substance Abuse Treatment, 44(2), 241–247. doi: 10.1016/j.jsat.2012.07.004
30. Bagley, S. M., Peterson, J., Cheng, D. M., Jose, C., Quinn, E., O’Connor, P. G., & Walley, A. Y. (2015). Overdose Education and Naloxone Rescue Kits for Family Members of Individuals Who Use Opioids: Characteristics, Motivations, and Naloxone Use. Substance Abuse, 36(2), 149-154.
31. Ashrafioun, L., Gamble, S., Herrmann, M., & Baciewicz, G. (2016). Evaluation of knowledge and confidence following opioid overdose prevention training: A comparison of types of training participants and naloxone administration methods. Substance Abuse, 37(1), 76-81.
60
References32. Bagley, S. M., Forman, L. S., Ruiz, S., Cranston, K., & Walley, A. Y. (2017). Expanding access to naloxone for family
members: The Massachusetts experience. Drug And Alcohol Review,
33. Williams, A. V., Marsden, J., & Strang, J. (2014). Training family members to manage heroin overdose and administer naloxone: randomized trial of effects on knowledge and attitudes. Addiction (Abingdon, England), 109(2), 250-259. doi:10.1111/add.12360
34. Albert, S., Brason II, F. W., Sanford, C. K., Dasgupta, N., Graham, J., & Lovette, B. (2011). Project Lazarus: Community-based overdose prevention in rural North Carolina. Pain Medicine, 12, S77–S85. Retrieved from http://prescribetoprevent.org/wp-content/uploads/2012/11/pm2011albert.pdf
35. Community Care of North Carolina. (n.d.). Project Lazarus: A community-wide response to managing pain. Retrieved from https://www.communitycarenc.org/population-management/chronic-pain-project/
36. Project Lazarus. (n.d.a). The Project Lazarus model. Retrieved from http://projectlazarus.org/about-lazarus/project-lazarus-model
37. Centers for Disease Control and Prevention (2016). Syringe services programs. Available at https://www.cdc.gov/hiv/risk/ssps.html
38. Schwartz, R. P., Gryczynski, J., O’Grady, K. E., Sharfstein, J. M., Warren, G., Olsen, Y., . . . Jaffe, J. H. (2013). Opioid Agonist Treatments and Heroin Overdose Deaths in Baltimore, Maryland, 1995–2009. American Journal of Public Health, 103(5), 917-922.





























