Embed Size (px)
Citation preview

Prescription and Over-the-Counter (OTC)
Drug Misuse
© 2009 University of Sydney
Learning Objectives• What is prescription drug misuse• Substances• Extent of problem• Recognising the problem• Managing the problem• Understanding medication regulations
What is prescription drug misuse
• Variety of terms- Prescription drug misuse: use of any drug in a manner other than how it is indicated or prescribed
- Aberrant drug related behaviours: behaviours that suggest the presence of substance abuse or addiction, implying that the behaviours are pathologic
• Spectrum including excess ingestion, diversion, injection, dependence

The Medications
• Sedating• Stimulant• Performance enhancing

Sedative• Opioids-illicit, prescribed and OTC• Benzodiazepines• Non-benzodiazepine hypnotics• Antipsychotics (in some environments)• Ketamine• Barbiturates (rarely)
Performance Enhancing include:
• Diuretics• Anabolic Androgenic Steroids• Hormones EPO, hGH, Insulin,
glucocorticoids• B Agonists/ B blockers• Steroid antagonists• Stimulants• Opioids
How do we identify/monitor this?
• Anecdotal/case reports• Post marketing surveillance• WHO• National Drug Strategy Household
Survey• Illicit Drug Reporting System• DAWN (US)• User sites
Stimulant misuse in the USA• Rates of non-prescribed stimulant use
-0.5% past month use in age 12-17(1)
-0.8% adults >26 years report last year use(1)
-4.1% college students report last year use(2)
• Among college students-whites, members of fraternities and
sororities, individuals with lower grade point averages, use of immediate-release preparations, and individuals who report ADHD symptoms at highest risk for misusing and diverting stimulants(2)
(1) 2007National Survey on Drug Use and Health:National Findings at http://oas.samhsa.gov
(2) McCabe SE. Knight JR. Teter CJ. Wechsler H. Non-medical use of prescription stimulants among US college students: prevalence and correlates from a national survey Addiction. 2005; 100(1): 96-106.
Australian prescription Opioid Misuse
• 2.5% Australians report recent use of pain-killers for non-medical purposes
• 4.45 report lifetime use• 15.4% had opportunity to use pain-
killers for non-medical purposes• Jurisdictional variations
2007 Australian National Drug Strategy Household survey
Australian Tranquiliser/ Sleeping Pill Misuse
• 2007 3.3% ever used non-medically
• 2007 1.4% had used in the last year-an increase from previous surveys
2007 Australian National Drug Strategy Household survey
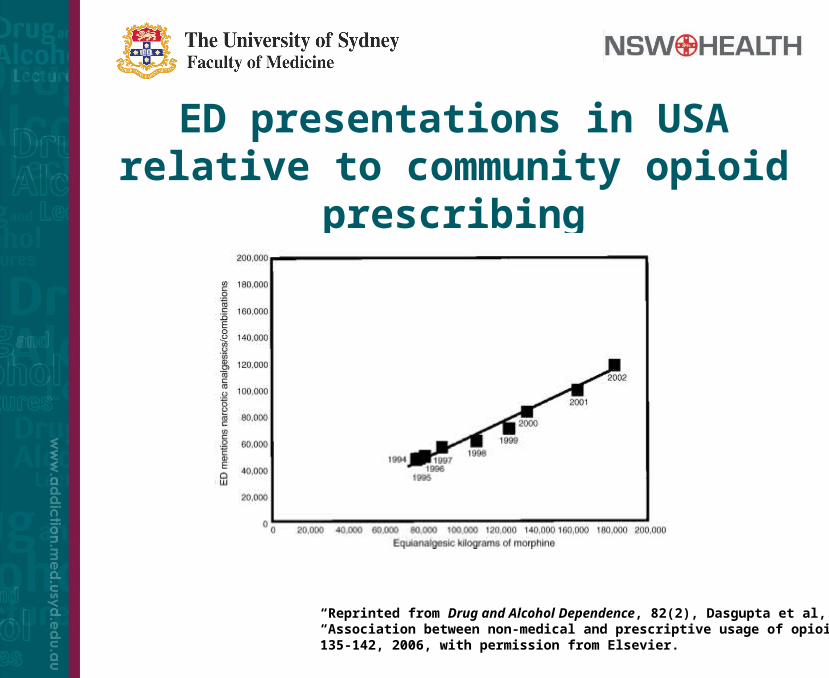
ED presentations in USA relative to community opioid
prescribing
“Reprinted from Drug and Alcohol Dependence, 82(2), Dasgupta et al, “Association between non-medical and prescriptive usage of opioids”, 135-142, 2006, with permission from Elsevier.
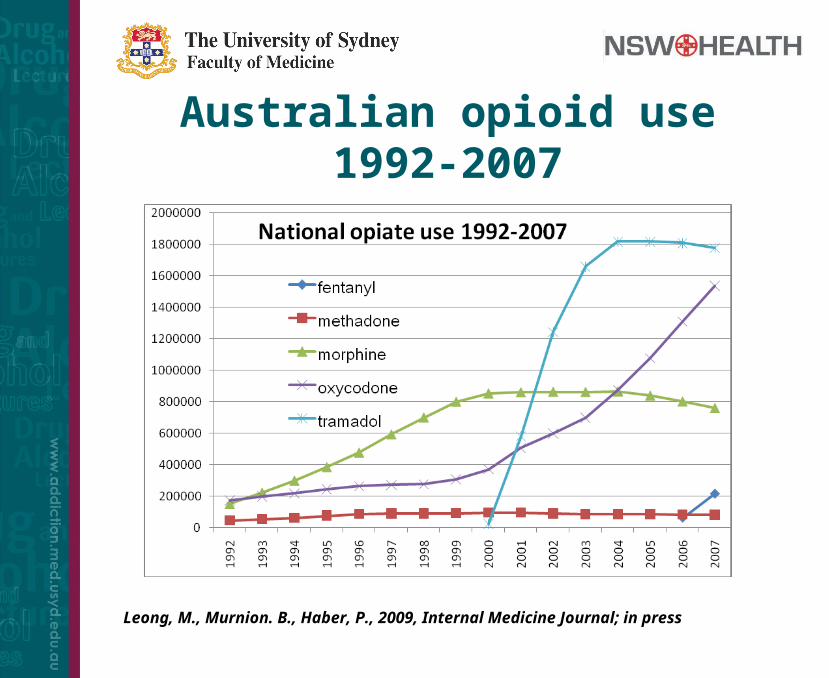
Australian opioid use 1992-2007
Leong, M., Murnion. B., Haber, P., 2009, Internal Medicine Journal; in press
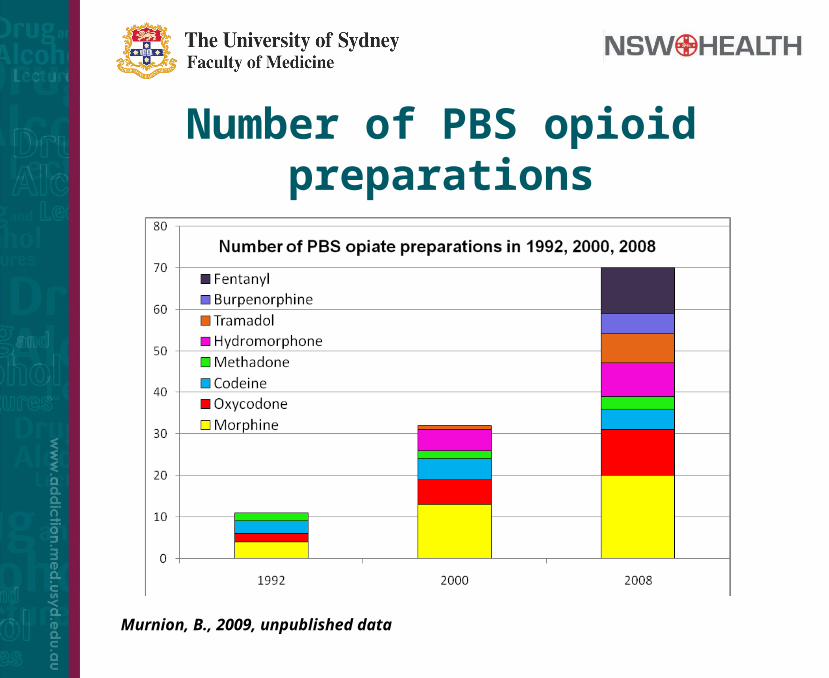
Number of PBS opioid preparations
Murnion, B., 2009, unpublished data
Over The Counter• Regulation does not easily allow
monitoring• Complex epidemiological methods• Jurisdictional variability in misuse• May vary with availability of illicits• Consider pseudoephedrine story• Is there a need for codeine containing
OTC analgesics?
Performance Enhancing• 2007- 223,898 tests undertaken by World Anti-Doping Agency• 4,402 AAF (1.97%)
Anabolic agents 2,322Stimulants 793Cannabanoids 576B2Agonists 399Diuretics and other masking agents 359Glucocorticoids 288Hormones and related substances 41B Blockers 27Narcotics 21Anti-oestrogens 18Enhancement of oxygen transfer 3
• May include TUE’s
World Anti-Doping Agency, 2007 Adverse Analytical Findings
Recognising prescription and OTC misuse
• Longitudinal observation• Corroborative history from other health
care providers• Frequent presentations with lost or
stolen scripts• Consider identified risk factors• Morbidity (e.g. Gastric erosions, CV
events )• Routine screening (e.g. elite athletes)
Strategies to prevent PDA
1. Patient
2. Drug
3. Prescriber
4. Governmental policy and legislation
5. Modification of the medication
1. Patient factors• Prior or current substance abuse
disorder places in high risk category• Environment (e.g. Prescribing
dexamphetamine to child whose parent/carers have a substance use disorder)
• Psychosocial setting may justify close monitoring
Risk of opioid misuse in chronic pain patients (CPPs)
• Adverse drug related behaviour (ADRB) in 11.5%
• Overt abuse/addiction in 3.27% • If no prior/current history of abuse,
abuse/addiction in 0.19%
• Urine toxicology showed 20% had non-prescribed or nil drug in urine and 14% had illicit drugs in urine
Structured Literature Review: Fishbain et al, 2008, Pain Med, 9
Amongst 2000+ CPPs exposed to prescribed opiates:
2. Drugs
• Drugs with abuse potential
- opioids
- hypnotics
- psychostimulants
- anticholinergics
- performance enhancing
3. Prescriber• High index of suspicion when unknown
patients present requesting repeat scripts for high risk drugs
• Screening tools• May feel isolated/threatened• Drs known to easily prescribe these
medications attract this clientele• Should report aberrant prescribing• Always ask about OTC and CAT use• Identify colleagues and report
appropriately
Managing PDA• Diagnosis
• Consider need for ongoing pharmacotherapy
• Consider cessation (gradual dose reduction)
• Harm minimisation strategy
• Patient contracts/UDS
• Doctor Shopping Agreements
• Frequent pharmacy dispensing
• Supervised dosing
• Consider need for other treatments for underlying disorder (eg anxiety/pain)
• Consult senior colleague or specialist
4. Governmental and legislative interventions• “Rogue” prescribers may be deregistered
or have prescribing limits
• Urgent NSW Medical Board inquiries to take action to protect the public rose from 22 in 2005/06 to 35 in 2006/2007
• Due in large part to increased referrals about prescribing practices from PSB
• Twelve doctors suspended, 19 had conditions imposed on registration, and two doctors removed from the Register.
New NSW medical board requirements (1/10/2008)
• Mandatory reporting to medical board if practises medicine whilst intoxicated by drugs (whether lawfully or unlawfully administered) or alcohol
• Medical Board recommends-be vigilant in identifying doctors or other
colleagues whose health, conduct, behaviour or performance may be a threat to the public;
-do your best to find out the facts, then if necessary, notify an appropriate person such as the hospital chief executive or the Medical Board. Your comments about colleagues must be honest. If you are not sure what to do, ask an experienced colleague or contact the Medical Board or your defence organisation for advice. The safety of patients must come first at all times; and
-report adverse events which reflect on the professional performance or conduct of colleagues to a hospital Chief Executive or Medical Board.
NSW Medical Board, 2009
Impaired Colleagues• If unable to deal with the matter yourself,
consult appropriate senior colleague.
• If you feel able to talk to the colleague yourself, do not take on a treating role, but
– arrange to meet with them privately,
– let them know that you are concerned and why,
– ask them to consult with an appropriate practitioner, and provide them with contact information
NSW Medical Board, 2009
Impaired Colleagues• Follow up to make sure that they have
taken your advice. Be aware that your colleague may tell you what they think you want to hear, having taken no positive steps.
• Consider the impact of their problem upon their work. If you believe that patient safety may be at risk, you should advise the doctor accordingly and seek the advice of the Medical Board
NSW Medical Board, 2009
Section 28 of the Poisons and Therapeutic Goods Act 1966
The authority of the Department of Health is required:
– to prescribe for or supply to a drug dependent person any drug of addiction (Schedule 8), or
– to prescribe for or supply to any person any preparation of dexamphetamine or methylphenidate, or
– to prescribe for or supply to any person other than a drug dependent person, for therapeutic use by that person continuously for more than two months, any of the following drugs of addiction – buprenorphine (excluding transdermal patches), flunitrazepam, hydromorphone, methadone or any injectable drug of addiction.
Governmental and legislative requirements• Vary between countries and states
• Concern internationally that rigid legislative requirements limit access to essential medications
• Separate from authority through PBS (federal)
• Prescription of methadone liquid or buprenorphine as Subutex/suboxone through OTP requires a separate authority
5. Modification of medications
• Limit scheduling of combination OTC products
• Limit to pack sizes and dose of opioid in OTC product
• Limit DTC advertising
• Reschedule substance (e.g. Ketamine)
• Remove from market e.g. pseudoephedrine
• Introduction of “abuse deterrant” formulations/combinations eg suboxone®
Case Study 1• JS• 22yr old man• Presents with agitaion, lacrimation,
rhinorrhea, yawning, abdominal pain and diarrhoea
• PMHx– Crohns Disease Rxed with Azothioprine and
prednisolone
• Acknowledges 70+ Neurofen Plus daily
What are you going to do?
What are you going to do?
• Diagnosis
What are you going to do?
• Diagnosis– opioid dependence– question diagnosis of CD
What are you going to do?
• Diagnosis– opioid dependence– question diagnosis of CD
• Investigations
What are you going to do?
• Diagnosis– opioid dependence– question diagnosis of CD
• Investigations• Treatment options
– withdrawal management– maintenance therapy
Case Study 2• Ms TD• 52 yr old woman• Presents frequently to ED with migraine• Seen neurologist-prophylactics/tryptans
ineffective• ADRs to morphine and oxycodone• Requests parenteral pethidine and has
letter form neurologist supporting this
What are you going to do?
What are you going to do?
• Diagnosis
What are you going to do?
• Diagnosis– consider rebound headaches
What are you going to do?
• Diagnosis– consider rebound headaches
• Corroborative history
What are you going to do?
• Diagnosis– consider rebound headaches
• Corroborative history• Very limited availability of pethidine in
public hospitals in NSW • Refer to appropriate local speciality
– Non-opioid management– Patient education
• Stabilise opioid use and wean
Author
Dr Bridin MurnionStaff Specialist
Drug Health Services, RPAH
All images used with permission, where applicable