Embed Size (px)
Citation preview

8/20/2017
1
Cindy Weston, DNP, RN, CCRN, CNS‐CC, FNP‐BCAssistant ProfessorTexas A&M University College of [email protected]
Review background and definitions of hypertension with appropriate ICD‐10
Discuss evidence for diagnosis and treatment of resistant hypertension
Describe classifications of pharmacologic treatment of resistant hypertension
Apply evidence based guidelines to the treatment of resistant
No Conflicts
“I struggled with everything cardiac in nursing school.”

8/20/2017
2
• 34% US adults > 18 year old
• 6% undiagnosed
• 77% people with 1st stroke BP > 140/90
• 76% of those diagnosed are on pharmacotherapy
• 46.5% are NOT controlled
• Health disparity‐ black women• Overall Death rate: 18.8 per 1000 per year
• Cost = $46.4 Billion$274 billion
Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics—2014 update: a report from the American Heart Association. Circulation. 2014; 129(3):e28‐e292. http://circ.ahajournals.org/content/early/2013/12/18/01.cir .0000441139.02102.80. http://dx.doi.org/10.1161/01.cir.0000441139.02102.80.Benjamin et al., on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2017 update: a report from the American Heart Association [published online ahead of print January 25, 2017]. Circulation. doi: 10.1161/CIR.0000000000000485
HDS‐4 Increase the proportion of adults who have had their blood pressure measured within the preceding 2 years and can state whether their blood pressure was normal or high (GOAL = 92.6%....2014= 91.8%)
HDS‐5 Reduce the proportion of persons in the population with hypertension
HDS‐9 Increase the proportion of adults with prehypertension who meet the recommended guidelines
HDS‐10 Increase the proportion of adults with hypertension who meet the recommended guidelines
HDS‐11 Increase the proportion of adults with hypertension who are taking the prescribed medications to lower their blood pressure
HDS‐12 Increase the proportion of adults with hypertension whose blood pressure is under control (GOAL = 61.2%) 43.7%50.3%
https://www.healthypeople.gov/2020/topics‐objectives/topic/heart‐disease‐and‐stroke/objectives

8/20/2017
3
HDS‐4 Increase the proportion of adults who have had their blood pressure measured within the preceding 2 years and can state whether their blood pressure was normal or high (GOAL = 92.6%....2014= 91.8%)
HDS‐5 Reduce the proportion of persons in the population with hypertension
HDS‐9 Increase the proportion of adults with prehypertension who meet the recommended guidelines
HDS‐10 Increase the proportion of adults with hypertension who meet the recommended guidelines
HDS‐11 Increase the proportion of adults with hypertension who are taking the prescribed medications to lower their blood pressure
HDS‐12 Increase the proportion of adults with hypertension whose blood pressure is under control (GOAL = 61.2%) 43.7%50.3%
HDS‐25 Increase the proportion of patients with hypertension in clinical health systems whose blood pressure is under control (58.3%64.3%)
https://www.healthypeople.gov/2020/topics‐objectives/topic/heart‐disease‐and‐stroke/objectives
Measure Population NCQA CMS/AHIPACO/PCMH
CPC+ HEDIS
Controlling High Blood Pressure
Adult
https://www.cms.gov/regulations‐and‐guidance/legislation/ehrincentiveprograms/ecqm_library.html
CMS165v6 Percentage of patients 18‐85 years of age who had a diagnosis of hypertension and whose blood pressure was adequately controlled (<140/90mmHg) during the measurement period (exclusions: ESRD, renal transplant, pregnancy, hospice.) Patients whose blood pressure at the most recent visit is adequately controlled (systolic blood pressure < 140 mmHg and diastolic blood pressure < 90 mmHg) during the measurement period
CMS65v7 Percentage of patients aged 18‐85 years of age with a diagnosis of hypertension whose blood pressure improved during the measurement periodPatients whose follow‐up blood pressure is at least 10 mmHg less than their baseline blood pressure or is adequately controlled.

8/20/2017
4
Cuff too small = False high BP
Cuff too big = maybe ok but maybe False low
BP 10‐20 mmHg higher in legs than arms
Right Arm = standard
Bladder Width > 40% arm circumference Bladder length 80‐100% arm circumference
No caffeine or Tobacco 30 minutes before measurement
Empty bladder
Seated, Back supported, Feet flat on floor for 5 minutes before measurement
Arm at heart level resting on support‐ 2 readings 1 minute apart & average (repeat other arm)
If variation‐ always use arm with higher readings
Useful to take standing measurement to check postural effects (older adults)
If high on automated machine‐ should be repeated by
auscultation 1‐2 minutes.
Weber, M.A., Schiffrin, E.L., White, W.B., Mann, S., Lindholm, L.H., Kenerson, J.G….Harrap, S.B. (2014). Clinical practice guidelines for the management of hypertension in the community: A statement by the American Society of Hypertension and the International Society of Hypertension. Journal of Hypertension, 32: 3‐15. https://www.nhlbi.nih.gov/health/health‐topics/topics/hbp/diagnosis
BP > 140‐90 on 2 separate visitsIf 1 elevated BP reading bring patient back in 1‐4 weeks for a repeat BP
BP > 180/100 at any single visit
Be mindful of “white coat hypertension” phenomenon
Home BP readings/log (5‐7 days minimum)
Ambulatory Blood Pressure Monitoring
Weber, M.A., Schiffrin, E.L., White, W.B., Mann, S., Lindholm, L.H., Kenerson, J.G….Harrap, S.B. (2014). Clinical practice guidelines for the management of hypertension in the community: A statement by the American Society of Hypertension and the International Society of Hypertension. Journal of Hypertension, 32: 3‐15.

8/20/2017
5
Cardiovascular Events
Stroke/TIA (vascular dementia)
CAD‐MI, angina, prior stents/CABG
Heart FailureLeft Ventricular Systolic function
Chronic Kidney Disease
Peripheral Arterial Disease
Diabetes Mellitus
OSA
I Cardiac codesHTN Heart
DiseaseHeart Failure
KidneyDisease
ICD‐10 codes
Description
YES No No No I10 Essential (Primary) Hypertension
YES YES No No I11.9 Hypertensive Heart Disease without Heart Failure
YES YES YES* No I11.0 Hypertensive Heart Disease with Heart Failure
YES No No Yes** I12.9 Hypertensive Chronic Kidney Disease stages 1‐4
YES No No Yes** I12.0 Hypertensive Chronic Kidney Disease Stage 5 or end‐stage Renal Disease
YES YES No Yes** I13.10 Hypertensive Heart Disease without Heart FailureWITH Chronic Kidney Disease stages 1‐4
YES YES No Yes** I13.11 Hypertensive Heart Disease without Heart FailureWITH Chronic Kidney Disease stage 5 or end‐stageRenal Disease
YES YES Yes* Yes** I13.0 Hypertensive Heart Disease with Heart Failure and Chronic Kidney Disease stages 1‐4
YES YES Yes* Yes** I13.2 Hypertensive Heart Disease with Heart Failure and Chronic Kidney Disease stage 5 or end‐stage Renal Disease
* Requires type of Heart Failure ICD‐10 code ** Requires type of Renal Disease ICD‐10 code
Adapted from: Family Practice Management, Coding Hypertensive Diseases under ICD‐10. http://www.aafp.org/fpm/2014/0300/fpm20140300p5‐rt1.pdf
CMP
Fasting Lipids
UA‐microalbuminuria
ECG
?H/H

8/20/2017
6
Study Yr n Criteria Result Conclusion
HOTHypertension Optimization Treatment Study
1998 18,790Age 50‐80HTN‐ DBP 100‐115
3 groups:DBP < 80DBP <85 DBP < 90All received Felodipine +
Lowest CV event DBP = 82.6 mmHg, Lowest mortality DBP = 86.5 mmHg
DBP < 90 mmHg
ALLHATAntihypertensive and Lipid‐lowering Treatment to Prevent Heart Attack Trial
2002 33,357HTN + 1 risk factor (1/3 DM)
4 groups:ChlorthalidoneLisinoprilAmlodipineDoxazosin **stopped CHF/Stroke
No difference in primary outcome or mortality
No difference in CV event or stroke
ACCOMPLISHAvoiding Cardiovascular events through Combination therapy in Patients Living with Systolic Hypertension
2008 11,000HTN, High CV risk
2 groups:Benazepril + AmlodipineBenazepril + HCTZ
Less CV events (9.6 % vs 11.8%) with ACEI/CCB combo
ACEI/CCB combo in thin, high risk
HYVETHypertension in the Very Elderly Trial
2008 3,84580+ years old
2 groupsIndapamide SRPlacebo
Lower BP associated with risk reduction
ACCORDAction to Control Cardiovascular Risk in Diabetes
2010 4,73360 year oldDM II x 10 yrs with CAD or 2+ RF
2 groupsGoal SBP < 140 mmHgGoal SBP < 120 mmHg
No difference in CV events
Small decrease in stroke with intensive control group
AASKAfrican American Study of Kidney Disease and Hypertension Trial
2010 1,094Black, HTN, nephrosclerosis, NO DM
3 groupsMetoprololRamiprilAmlodipine
No difference in GFR BUT ACEI more effective in slowing decline of GFR than BB or CCB
ACEI best, Lower BP may be benefit with proteinuria
• 1977 – JNC 1 • 1980 – JNC 2 • 1984 – JNC 3 • 1988 – JNC 4 • 1993 – JNC 5 • 1997 – JNC 6 • 2003 – JNC 7 (delayed wait for ALLHAT) • 2014 – JNC 8
• AHA/ACC/CDC advisory algorithm 2013
• ASH/ISH 2013• Canadian 2011 • British 2012 • European 2013
Chopra, . & Nanda, N. (2013). Textbook of Cardiology: A Clinical and Historical Perspective. New Delhi: Jaypee Brothers Medical Publishers.
BP Goal JNC‐72004
JNC‐82014
ASH/ISH2013
ESC/ESH2013
CHEP2013
Age < 60 <140/90 <140/90 <140/90 <140/90 <140/90
Age 60‐79 <140/90 <150/90 <140/90 <140/90 <140/90
Age 80+ <140/90 <150/90 <150/90 <150/90 <150/90
Diabetes <130/80 <140/90 <140/90 <140/85 <130/80
CKD <130/80 <140/90 <140/90 <130/90 <140/90
Salvo, M. & White, C.M. (2014). Reconciling multiple hypertension guidelines to promote effective clinical practice. Annals of Pharmacotherapy, 48(9), 1242‐1248.

8/20/2017
7
Whelton, P. et al. (2003). Primary prevention of hypertension. JAMA, 288(15), 1882‐1888.
0%
5%
10%
15%
20%
25%
30%
35%
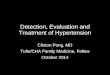
Coronary heartdisease
Stroke
Xie, X. et al. (2016). Effects of intensive blood pressure lowering on cardiovascular and renal outcomes: updated systematic review and meta‐analysis. Lancet, 387(10017), 435‐433.
BP‐ 133/76
Comparison of expected and observed effects of a 7 mm Hg systolic blood pressure decrease on coronary heart disease and stroke outcomes

8/20/2017
8
Blood Pressure Lipids
Mediterranean(low evidence)
If DM or 3 risk factors < 6‐7/2‐3 mmHgHealthy < 2‐3/1‐2 mmHg
No change
DASH(high evidence)
< 5‐6/3 mmHg < LDL 11mg/dL< HDL 4 mg/dLNo change TG
Reduce dietarySodium(high evidence)
Lowers BP
1150mg/d < 3‐4/1‐2 mmHg
No change
Exercise < 2‐5/1‐4 mmHg(high evidence)
< LDL 2.5 mg/dL< non‐HDL 6 mg/dLNo change TGNo change HDL(moderate evidence)
EXERCISE: at least 12 weeks duration, 3 to 4 sessions per week, lasting on average 40 minutes per session, and involving moderate‐ to vigorous intensity physical activity. Strength of evidence: High
Eckel, R.H.. et al. (2013). 2013 AHA/ACC Guideline on lifestyle management to reduce cardiovascular risk. Circulation.
Whelton, P. et al. (2003). Primary prevention of hypertension. JAMA, 288(15), 1882‐1888.
0%
5%
10%
15%
20%
25%
30%
35%
Coronary heartdisease
Stroke
Xie, X. et al. (2016). Effects of intensive blood pressure lowering on cardiovascular and renal outcomes: updated systematic review and meta‐analysis. Lancet, 387(10017), 435‐433.
BP‐ 133/76
Comparison of expected and observed effects of a 7 mm Hg systolic blood pressure decrease on coronary heart disease and stroke outcomes

8/20/2017
9
Diuretics
ACEI: Angiotensin Converting Enzyme Inhibitors
ARB: Angiotensin Receptor Blockers
Calcium Channel Blockers
Beta Blockers
Alpha Blockers
Central Acting
Vasodilators
Potassium Channel Activators
JNC‐72004
JNC‐82014
ASH/ISH2013
ESC/ESH2013
CHEP2013
Non‐blackNo DM/CKD
Thiazide Thiazide, ACEI, ARB, CCB
< 60 ACEI, ARB> 60 CCB, Thiazide
Thiazide,ACEI, ARB, CCB, BB
Thiazide, ACEI, ARB (BB if < 60)
BlackNo DM/CKD
Thiazide ThiazideCCB
ThiazideCCB
Thiazide, ACEI, ARB, CCB, BB
Thiazide, ARB (BB if < 60)
DiabetesWithout CKDAll races
ACEI, ARB, CCB, BB, Thiazide
Thiazide,ACEI, ARB, CCB
ACEI, ARB, CCB, Thiazide
ACEI, ARB ACEI, ARB, CCB, Thiazide
CKD ACEI, ARB ACEI, ARB ACEI, ARB ACEI, ARB ACEI, ARB
Salvo, M. & White, C.M. (2014). Reconciling multiple hypertension guidelines to promote effective clinical practice. Annals of Pharmacotherapy, 48(9), 1242‐1248.

8/20/2017
10
Diuretics
Drug Class Drug Dose Interval
Benzophenone Chlorthalidone(Hygroton)
12.5‐25mg Daily
Benzothiadiazine HCTZ 12.5‐50mg Daily
Indapamide(Lozol)
1.25‐2.5mg Daily
Quinazolinones Metolazone(Zaroxolyn)
2.5‐10mg Daily
JNC‐72004
JNC‐82014
ASH/ISH2013
ESC/ESH2013
CHEP2013
Non‐blackNo DM/CKD
Thiazide Thiazide, ACEI, ARB, CCB
< 60 ACEI, ARB> 60 CCB, Thiazide
Thiazide, ACEI, ARB, CCB, BB
Thiazide, ACEI, ARB (BB if < 60)
BlackNo DM/CKD
Thiazide ThiazideCCB
ThiazideCCB
Thiazide, ACEI, ARB, CCB, BB
Thiazide, ARB (BB if < 60)
DiabetesWithout CKD
ACEI, ARB, CCB, BB, Thiazide
Thiazide, ACEI, ARB, CCB
ACEI, ARB, CCB, Thiazide
ACEI, ARB ACEI, ARB, CCB, Thiazide
CKD ACEI, ARB ACEI, ARB ACEI, ARB ACEI, ARB ACEI, ARB
Salvo, M. & White, C.M. (2014). Reconciling multiple hypertension guidelines to promote effective clinical practice. Annals of Pharmacotherapy, 48(9), 1242‐1248.
ACEIs
ARBs
Aldosterone Antagonist
Renin Inhibitor

8/20/2017
11
Captopril (Capoten)
Lisinopril (Zestril, Prinivil)
Enalapril (Vasotec)
Ramipril (Altace)
Fosinopril (Monopril)
Benazepril (Lotensin)
Quinapril (Accupril)
Trandolapril (Mavik)
Perindopril (Aceon)
Losartan (Cozaar)
Candesartan (Atacand)
Valsartan (Diovan)
Telmisartan (Micardis)
Irbesartan (Avapro)
Omesartan (Benicar)
Eprosartan (Teveten)

8/20/2017
12
Aliskiren (Tekturna)
CYP3A4!
Avoid grapefruit juice, ‐azoles
JNC‐72004
JNC‐82014
ASH/ISH2013
ESC/ESH2013
CHEP2013
Non‐blackNo DM/CKD
Thiazide Thiazide, ACEI, ARB, CCB
< 60 ACEI, ARB> 60 CCB, Thiazide
Thiazide, ACEI, ARB, CCB, BB
Thiazide, ACEI, ARB (BB if < 60)
BlackNo DM/CKD
Thiazide ThiazideCCB
ThiazideCCB
Thiazide, ACEI, ARB, CCB, BB
Thiazide, ARB (BB if < 60)
DiabetesWithout CKD
ACEI, ARB, CCB, BB, Thiazide
Thiazide, ACEI, ARB, CCB
ACEI, ARB, CCB, Thiazide
ACEI, ARB ACEI, ARB, CCB, Thiazide
CKD ACEI, ARB ACEI, ARB ACEI, ARB ACEI, ARB ACEI, ARB
Salvo, M. & White, C.M. (2014). Reconciling multiple hypertension guidelines to promote effective clinical practice. Annals of Pharmacotherapy, 48(9), 1242‐1248.
DihydropyridinesAmlodipine (Norvasc)
Felodipine (Plendil)
Isradipine (DynaCirc)
Nifedipine (Procardia XL, Adalat CC)
Nisoldipine (Sular)
Non‐dihydropyridinesVerapamil (Isoptin, Calan)
Diltiazem (Cardizem, Dilacor)
Avoid grapefruit juice

8/20/2017
13
JNC‐72004
JNC‐82014
ASH/ISH2013
ESC/ESH2013
CHEP2013
Non‐blackNo DM/CKD
Thiazide Thiazide, ACEI, ARB, CCB
< 60 ACEI, ARB> 60 CCB, Thiazide
Thiazide, ACEI, ARB, CCB, BB
Thiazide, ACEI, ARB (BB if < 60)
BlackNo DM/CKD
Thiazide ThiazideCCB
ThiazideCCB
Thiazide, ACEI, ARB, CCB, BB
Thiazide, ARB (BB if < 60)
DiabetesWithout CKD
ACEI, ARB, CCB, BB, Thiazide
Thiazide, ACEI, ARB, CCB
ACEI, ARB, CCB, Thiazide
ACEI, ARB ACEI, ARB, CCB, Thiazide
CKD ACEI, ARB ACEI, ARB ACEI, ARB ACEI, ARB ACEI, ARB
Salvo, M. & White, C.M. (2014). Reconciling multiple hypertension guidelines to promote effective clinical practice. Annals of Pharmacotherapy, 48(9), 1242‐1248.
Beta Blocker TherapyPercentage of patients aged 18 years and older with a diagnosis of coronary artery disease or heart failure seen within a 12
month period who also have a prior MI OR a
current or prior LVEF <40% who were prescribed beta‐blocker therapy
Metoprolol (Lopressor, Toprol)
Atenolol (Tenormin)
Bisoprolol (Zebeta)
Esmolol (Brevibloc)
Carvedilol (Coreg)
Propranolol (Inderal)
Labetalol (Trandate)
Nadolol (Corgard)
Nebivolol (Bystolic)
JNC‐72004
JNC‐82014
ASH/ISH2013
ESC/ESH2013
CHEP2013
Non‐blackNo DM/CKD
Thiazide Thiazide, ACEI, ARB, CCB
< 60 ACEI, ARB> 60 CCB, Thiazide
Thiazide, ACEI, ARB, CCB, BB
Thiazide, ACEI, ARB (BB if < 60)
BlackNo DM/CKD
Thiazide ThiazideCCB
ThiazideCCB
Thiazide, ACEI, ARB, CCB, BB
Thiazide, ARB (BB if < 60)
DiabetesWithout CKD
ACEI, ARB, CCB, BB, Thiazide
Thiazide, ACEI, ARB, CCB
ACEI, ARB, CCB, Thiazide
ACEI, ARB ACEI, ARB, CCB, Thiazide
CKD ACEI, ARB ACEI, ARB ACEI, ARB ACEI, ARB ACEI, ARB
Salvo, M. & White, C.M. (2014). Reconciling multiple hypertension guidelines to promote effective clinical practice. Annals of Pharmacotherapy, 48(9), 1242‐1248.

8/20/2017
14
Terazosin (Hytrin)
Prazosin (Minipress)
Doxazosin (Cardura)
Phentolamine (Regitine)
JNC‐72004
JNC‐82014
ASH/ISH2013
ESC/ESH2013
CHEP2013
Non‐blackNo DM/CKD
Thiazide Thiazide, ACEI, ARB, CCB
< 60 ACEI, ARB> 60 CCB, Thiazide
Thiazide, ACEI, ARB, CCB, BB
Thiazide, ACEI, ARB (BB if < 60)
BlackNo DM/CKD
Thiazide ThiazideCCB
ThiazideCCB
Thiazide, ACEI, ARB, CCB, BB
Thiazide, ARB (BB if < 60)
DiabetesWithout CKD
ACEI, ARB, CCB, BB, Thiazide
Thiazide, ACEI, ARB, CCB
ACEI, ARB, CCB, Thiazide
ACEI, ARB ACEI, ARB, CCB, Thiazide
CKD ACEI, ARB ACEI, ARB ACEI, ARB ACEI, ARB ACEI, ARB
Salvo, M. & White, C.M. (2014). Reconciling multiple hypertension guidelines to promote effective clinical practice. Annals of Pharmacotherapy, 48(9), 1242‐1248.
Clonidine
Methyldopa

8/20/2017
15
Loop DiureticsFurosemide
Torsemide
Bumetanide
Ethacrynic Acid
Mineralcorticoid AntagonistSpironolactone
Eplerenone
Sodium Channel BlockerAmiloride
Hydralazine
Sodium Nitroprusside
Minoxidil (Loniten)
Diazoxide (Proglycem)
Uncontrolled blood pressure despite the use of three optimized antihypertensive medications, of which one is a diuretic.
D. A. Calhoun, D. Jones, S. Textor et al., (2008). Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension, 117(25), e510–e526.
Prevalence is unknown(Estimated 10‐30%)

8/20/2017
16
Poor adherence
Provider inertia
Inadequate doses
Inappropriate combinations of meds
Excess alcohol intake
Obstructive Sleep Apnea
D. A. Calhoun, D. Jones, S. Textor et al., (2008). Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension, 117(25), e510–e526.P. A. Sarafidis and G. L. Bakris, (2008). Resistant hypertension. An overview of evaluation and treatment. Journal of the American College of Cardiology, 52(22), 1749– 1757.
Thyroid Disease
OSA
Primary Hyperaldosteronism
Renal Artery Stenosis
Cushings Disease
Coarctation of the Aorta
Hyperparathyroidism
Pheochromocytoma
Faselis, C., Doumas, M. & Papademetriou, V. (2011). Common secondary causes of resistant hypertension and rational for treatment. International Journal of Hypertension,.

8/20/2017
17
Increase diuretic doseConsider a loop if GFR< 30mL/min/1.73m2
Add an alpha blocker
Use a combined alpha/beta blocker: carvedilol, labetalol
Add spironolactone, epleronone, OR amiloride
Add hydralazine, clonidine, guanfacine,
Consider using BOTH a nondihydropiradine CCB AND a dihydropiradine CCB
Consider minoxidil
REFER to A HYPERTENSION SPECIALIST:
Viera, A.J. 7 Hinderlier, A.L. (2009). Evaluation and management of the patient with difficult to control or resistant hypertension. American Family Physician, 79(10), 863‐869.
BP remains > 140/90
(>age 60 150‐90)
despite 3 antihypertensives
(1 being a diuretic)
Review Lifestyle Factors & Coach patient
‐Obesity, excess alcohol, high salt intake, DASH diet, physical
activity
SCREEN for SECONDARY causes of Hypertension
Stop or Minimize interfering substances
‐ NSAIDS, OCPs, Alcohol, Ephedra, etc.
Assess Adherence
Review Home BP log
Adjust Pharmacologic Treatment
Maximize Diuretic include Spironolactone
REFER to a SPECIALIST
Cardiology
Nephrology

8/20/2017
18
NSAID use
Belief System
Medication Adherence
Medication Affordability
Home Blood Pressure Monitoring
Self‐Titration
Patient Selection
BP Goals: < 140/90
Home BP monitoring
Patient Centered Care
Self Titration in select populations
Facilitate healthy lifestyle modification

8/20/2017
19
QUESTIONS??
• Beckett NS, Peters R, Fletcher AE, et al; HYVET Study Group. (2008). Treatment of hypertension in patients 80 years of age or older. NEJM;358(18):1887‐189B.
• Benjamin et al., on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2017 update: a report from the American Heart Association [published online ahead of print January 25, 2017]. Circulation. doi: 10.1161/CIR.0000000000000485
• Caboral‐Stevens, M. & Rosario‐Sim, M. (2014). Review of the Joint National Committee’s recommendations in the management of hypertension. JPN, 10(5), 325‐330.
• Calhoun, D. A. , Jones, D., Textor, S. et al., (2008). Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension, 117(25), e510–e526.
• Chobanian AV. Bakris GL. Black HR, et al; (2003). Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. JAMA, 289(19), 2560‐2572.
• Chopra, . & Nanda, N. (2013). Textbook of Cardiology: A Clinical and Historical Perspective. New Delhi: Jaypee Brothers Medical Publishers.
• Cushman WC, Evans GW, Byington RP, et al; (2010). ACCORD Study Group. Effects of intensive blood‐pressure control in type 2 diabetes mellitus. NEJM;362(17):1575‐1585.
• Eckel, RH, et al. (2013). 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk, Circulation.
• Salvo, M. & White CM (2014). Reconciling multiple hypertension guidelines to promote effective clinical practice. Annals of Pharmacotherapy, 48(9), 1242‐1248.
• Egan, B., Li, J., Hutchison, F. & Ferdinand, K. (2014). Hypertension in the United States 1999‐2012: Progress toward Healthy People 2020 Goals. Circulation.
• Faselis, C., Doumas, M. & Papademetriou, V. (2011). Common secondary causes of resistant hypertension and rational for treatment. International Journal of Hypertension.
• Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics—2014 update: a report from the American Heart Association. Circulation. 2014; 129(3):e28‐e292.
• Healthy People 2020 – Heart Disease and Stroke. https://www.healthypeople.gov/2020/topics‐objectives/topic/heart‐disease‐and‐stroke/objectives. Accessed August 16, 2016.
• James, P. et al. (2014). 2014 Evidence‐based guideline management of high blood pressure in adults: Report from the panel members appointed to the eighth Joint National Committee (JNC8). JAMA, 311(5), 507‐520.
• Wright, JT, et al. (2015). A randomized trial of intensive versus standard blood‐pressure control. NEJM 373, 2103‐2116.
• Leung AA, et al. Hypertension Canada’s 2016 CHEP Guidelines for blood pressure measurement, diagnosis, assessment of risk, prevention and treatment of hypertension. Can J Cardiol. 2016; 32:569–588.
• National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; (2003). National High Blood Pressure Education Program Coordinating Committee The JNC 7 report. JAMA. 289(19):256O‐2572.
• Sarafidis, P. A. and Bakris, G. L. (2008). Resistant hypertension. An overview of evaluation and treatment. Journal of the American College of Cardiology, 52(22), 1749– 1757.
• Viera, A.J. 7 Hinderlier, A.L. (2009). Evaluation and management of the patient with difficult to control or resistant hypertension. American Family Physician, 79(10), 863‐869.
• Weber, M.A., Schiffrin, E.L., White, W.B., Mann, S., Lindholm, L.H., Kenerson, J.G….Harrap, S.B. (2014). Clinical practice guidelines for the management of hypertension in the community: A statement by the American Society of Hypertension and the International Society of Hypertension. Journal of Hypertension, 32: 3‐15.
• Whelton, P. et al. (2003). Primary prevention of hypertension. JAMA, 288(15), 1882‐1888.