Embed Size (px)
Citation preview

Strategic Plan II
2010/11 – 2014/15
Federal HIV/AIDS Prevention and Control Office | Federal Ministry of HealthAddis Ababa, Ethiopia, February 2010
For Intensifying Multisectoral HIV and AIDS Response in Ethiopia


Strategic Plan II
2010/11 – 2014/15
For Intensifying Multisectoral HIV and AIDS Response in Ethiopia

AIDS Acquired Immune Deficiency SyndromeANC Antenatal CareARC AIDS Resource CentreART Anti-Retroviral TherapyARV Anti-Retroviral BCC Behavioural Change CommunicationBSS Behavioural Surveillance SurveyCBO Community-Based Organization
CC Community ConversationCCM Country Coordination MechanismCSO Civil Society Organizations
CSW Commercial Sex WorkersDA Development Army
DHS Demographic and Health SurveyEIFDDA Ethiopian Inter-faith Forum for Development, Dialogue and Action
EHNRI Ethiopian Health and Nutrition Research InstituteEMSAP Ethiopian Multi‐Sectoral HIV/AIDS Program
ERCS Ethiopian Red cross SocietyFBO Faith-Based Organization
FMOH Federal Ministry of HealthGBV Gender-Based Violence
GFATM Global Fund to Fight AIDS, Tuberculosis and MalariaGIPA Greater Involvement of People Living with HIV/AIDS
HAPCO HIV/AIDS Prevention and Control OfficeHB Health Bureau
HCT HIV Counselling and TestingHEWs Health Extension Workers
HIV Human Immunodeficiency VirusHMIS Health Management Information System
HR Human ResourceHSDP Health Sector Development ProgramICASA International conference on AIDS and STI in Africa
IEC Information Education CommunicationIGAs Income Generating Activities
IP Infection PreventionMAC-E Millennium AIDS Campaign-Ethiopia
MARPs Most At Risk Populations
Acronyms

MC Male CircumcisionMDGs Millennium Development Goals
M and E Monitoring and EvaluationMIS Management Information System
MNCH Maternal,Neonatal,and Child HealthMOE Ministry Of EducationMOH Ministry Of Health
MOLSA Ministry of Labour and Social AffairsMTCT Mother-To-Child Transmission of HIV
MWCYA Ministry of Women,Children and Youth AffairsNAC National AIDS Council
NEP+ Network of Networks of HIV Positive in EthiopiaNGO Nongovernmental Organization
OC Organisational ConversationOI Opportunistic Infections
OVC Orphans and Vulnerable ChildrenPASDE Plan for Accelerated and Sustainable Development to End Poverty
PEP Post-Exposure ProphylaxisPFSA Pharmaceuticals Fund and Supply Agency
PIHCT Provider-Initiated HIV Counselling and TestingPLHIV People Living With HIV/AIDS
PMTCT Prevention of Mother-To-Child Transmission of HIVRAC Regional AIDS CouncilREB Regional Education Bureau
RHAPCO Regional HIV/AIDS Prevention and Control OfficeRHB Regional Health Bureau
SNNPR Region of Southern People Nations and NationalitiesSPM Strategic Plan Management
STI Sexually Transmitted InfectionTB Tuberculosis
TVET Technical and Vocational education and trainingTWG Technical Working Group
UNGASS United Nations General Assembly Special Session on HIV/AIDSVCAP Volunteer Community Anti AIDS Promoters
VCT Voluntary Counselling and TestingWrHO Woreda Health Office
WA Women AssociationsYA Youth Associations

Contents
Acronyms iiPreface viExecutiveSummary viii
Part One: Introduction 11.1. SituationAnalysis 21.2. ResponseAnalysis 6
Part Two: Vision,Mission,Goal,StrategicResults,andGuidingPrinciples 11
Part Three: ThematicAreas 153.1. ThematicAreaOne:CreatinganEnabling
Environment 163.2. ThematicAreaTwo:IntensifyingHIV
Prevention 203.3. ThematicAreaThree:IncreaseAccess
toandImproveQualityofChronicCareandTreatment 28
3.4. ThematicAreaFour:StrengthenCareandSupportServicestoMitigatetheImpactofAIDS 31
3.5. ThematicAreaFive:StrengthenGenerationandUtilizationofStrategicInformation 32

Part Four: Five-yearProgrammaticTargetsandResultsMatrix 354.1.Five-yearProgrammaticTargets 364.2.ResultsMatrix 38
Part Five: ImplementationModalityandInstitutionalArrangements 705.1.MultisectoralHIV/AIDSresponsegoverningandcoordinatingbodies 71
5.2.ImplementationofthemultisectoralHIV/AIDSresponse 71
Part Six: MonitoringandEvaluation 72

vi
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
The multisectoral response to HIV/AIDS in Ethiopia is guided by the National HIV/AIDS Policy, 1998; the Strategic Plan for Intensifying Multisectoral HIV/AIDS Response, SPM I (2004-2008); the Plan for Accelerated and Sustained Development to End Poverty, PASDEP (2007-2010); the Road Map for accelerated access to HIV prevention, treatment and care in Ethiopia, (2007-2010); and the Plan of Action for Universal Access to HIV prevention, treatment, care and support in Ethiopia, (2007-2010).
This strategic plan (SPM II) is developed as a guide towards universal access to HIV/AIDS services in the country. Various documents have been used as inputs to prepare SPM II. These include:
• Final Evaluation report of SPM I, 2004-2008;• Evaluation documents including Impact Evaluation Report of the Global Fund to Fight AIDS, TB
and Malaria, Mid-term Evaluation Report of HSDP III, Aide memoire and Mid-term review report of EMSAP I;
• Survey reports such as BSS 2005, DHS 2005 , ANC 2005, single point HIV prevalence estimate 2005, HIV/AIDS Epidemiological Synthesis Report, 2008;
• Global Fund project proposals from Round 4 (2005-2010) and Round 7 grants (2008-12) and the Rolling Continuation Channel (2009-2014);
• Road Map for HIV Prevention, Care, and Treatment (2007-2010) and Costed Universal Access Plan for HIV/AIDS Prevention, Care and Treatment (2007-2012);
• Annual Report of 2008 and 2009, proceedings from various review meetings, UNGASS report of 2008 and proceeding and consensus statement of the National Prevention Summit.
• HSDP IV and • Other strategic plans from key sectors.
Preface

2010/11-2014/15
vii
The SPM II has six major parts. Part one covers a synoptic overview of the HIV/AIDS epidemic and the response analysis. Part two consists of the vision, mission, goal and guiding principles of the national response. Part three elaborates on the five thematic areas (along with their objectives and key strategies) including: (1) creating enabling environment; (2) intensifying HIV preventions; (3) increasing access to and improving quality of chronic care and treatment; (4) intensifying mitigation efforts against the epidemic; and (5) strengthening the generation and utilization of strategic information. Part four of the SPM II is about the programmatic targets and result matrix, which outlines selected strategies, major interventions, targets, indicators, means of verification and lead responsible bodies. Part five covers the implementation modality and institutional arrangements for the SPM. Part six covers the monitoring and evaluation of the SPM.
The SPM II has been developed through a collective effort and active participation of key government sectors, faith-based organizations, community-based organizations, civil societies and associations of people living with HIV, the private sector, multilateral and bilateral donors and individuals. The SPM is fully costed and will have a consolidated road map and operational annual plans, facilitating the SPM into action. The implementation process and achievements will be closely monitored and evaluated based on a costed M and E framework that will be developed shortly. Multisectoral actors will have shared responsibilities and accountability in harmony with the “three ones” principles.

viii
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
1.EpidemicSituationAnalysisTrend of the epidemicSince the detection of the first two AIDS cases in Ethiopia in 1986, the epidemic has rapidly spread throughout the country. According to the single point estimate, the national adult HIV prevalence is 2.3% in 2009 with an estimated 1.1 million people living with HIV in the country. The epidemic which started in the mid-1980’s, expanded rapidly reaching a plateau around the mid-1990s. Although the epidemic is on the decline in major urban settings and stabilizing in rural areas, there is significant variation in the epidemic among geographic areas and population groups.
Heterogeneity of the Epidemic Across the country, the epidemic is generalized. However, urban areas and females are more affected than rural areas and males. Urban HIV prevalence was 7.7% in 2009 and this accounted for 62% of the total PLHIV in the country, while rural HIV prevalence was 0.9% in 2009, which accounted for 38% of total PLHIV population in the country. The estimated national adult HIV incidence of 0.28% in 2009 translates to over 131,000 new HIV infections. There is variation in the prevalence among regions both by urban and rural settings. The HIV prevalence in urban areas ranges from 2.3% in Somali region to 10.8% in Afar region. There is also variation in the urban HIV prevalence among big regions: Oromia (6.1%), SNNPR (7.2%), Amhara (9.9%), and Tigray (10.7%); whereas the rural HIV prevalence ranges from 0.4% in Somali region to 1.4% in Amhara region. Small towns are becoming hot-spots and can potentially bridge further spread of HIV epidemic to rural settings. Addis Ababa and four regions: Amhara, Tigray, Oromia, and SNNPR account for 93.4% of the total PLHIV population in the country.
In all regions, females are more affected than males in both urban and rural areas. In 2009, female HIV prevalence was 2.8% while male HIV prevalence was 1.8%. Females accounted for 59% of the total PLHIV in the country. According to DHS 2005, females are twice more affected than males.
Executive Summary

2010/11-2014/15
ix
Most- at- Risk Population GroupsBased on the current available information, the most-at-risk populations (MARPs) in the country includes female sex workers, uniformed forces, long distance drivers, discordant couples, refugees, and migrant labourers, including cross-border and mobile populations. However, there are data gaps to show the full picture of MARPs, their magnitude and sexual behaviours as well as their potential in further spreading the epidemic to the general population.
Knowledge and Sexual Behaviour PatternsDespite high awareness about HIV/AIDS, comprehensive knowledge on transmission routes and prevention methods is low. According to BSS 2005, only 57% of the studied population knew all three prevention methods and major misconception was high in the general population. There is an encouraging trend of consistent condom use with over 90% condom use among Commercial Sex Workers and uniformed forces. However, consistent condom use in casual sex with non-regular partner among the sexually active population is low. Only 60% of out-of-school youth who had sex with a non-regular partner used condom. Although there has been a slight decrease in individuals who have had sex with two or more non-regular partners, sexual practices such as premarital and extra-marital sex exist in the society. Never married sexually active young women are at greater risk of HIV due to sexual mixing with older and high risk men.
Determinant Factors of the EpidemicDeterminant factors that drive the epidemic and sexual behaviours among different population groups are not adequately explored. Limited studies and anecdotal evidences indicate that low level of comprehensive knowledge about HIV/AIDS, low level of perceived risk and threat of HIV/AIDS, increased population migration, high prevalence of unprotected sex through concurrent multiple partnerships, intergenerational transactional sex, high prevalence of STIs, alcohol and substance abuse, gender inequality and poverty could be cited as some of the drivers of the epidemic. In addition, as PMTCT service uptake and ANC coverage are low, there is considerably high vertical transmission from mother to child.

x
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
2.ResponseAnalysisThe multisectoral response to HIV/AIDS in Ethiopia was expanded dramatically during the implementation of SPM I (2004-2008). Capacity in the community and in the health sector significantly increased. Over 30,000 health extension workers were deployed into rural Kebeles all over the country. This has ignited public movement against HIV/AIDS through community conversation, which has enabled community members to perceive the problem of HIV/AIDS, create consensus on what fuels the epidemic in their own settings and how to prevent it, by developing plan of actions and passing relevant community bylaws. These have resulted in social transformation and increased demand for & utilization of HIV/AIDS services by communities. Many religious organizations and community groups across the country have instituted the culture of premarital HIV counselling and testing into their by-laws.
The accelerated expansion of primary health care facilities, the decentralization of HIV/AIDS services, and the innovative millennium AIDS campaign- Ethiopia, launched in November 2006 at the eve of the new Ethiopian Millennium, have increased HCT service uptake by nine folds. Individuals counselled and tested for HIV increased from less than half a million per year in 2004, to 4.6 million per year in 2008. The accelerated expansion of free ART program by the government of Ethiopia improved the survival and quality of life for AIDS patients. Patients ever started on ART increased from 8,226 in 2005 to 180,455 by the end of 2008. Although Ethiopia has seen a marked improvement in a number of HIV/AIDS related areas, the performance of the PMTCT program has been below the target for universal access.
Moreover, the capacity of PLHIV associations was also strengthened by empowering them to have a decisive role in the governance, management and service delivery of the HIV/AIDS response. The Network of Networks of HIV Positive in Ethiopia is a member of the National AIDS Council, national management board, Country Coordinating Mechanism for GFATM and review board, as well as the principal recipient of the GFATM Round 7 at national level with decentralized involvement at regional and sub-regional levels. The Ethiopian Inter-faith Forum for Development, Dialogue and Action has become the principal recipient of Round 7 GFATM, along with public sector and NEP+, to enhance the faith-based HIV/AIDS response in the country.
Many public sectors, non-government and private sector organizations have initiated mainstreaming of HIV/AIDS into their core activities during this period. The education sector has integrated HIV/AIDS into the curriculum, initiating peer education, life skills and school community conversation in a considerable number of schools.

2010/11-2014/15
xi
Other initiatives were also undertaken to enhance behaviour change among most-at-risk population groups as evidenced by high consistent condom use by traditional MARPs such as CSWs and uniformed forces. Access to AIDS information increased through the expansion of AIDS resource centres, hotlines for the general population, and the Fetun warm-line for health care service providers. Behaviour Change Communication messages were transmitted using print and radio serial dramas and condoms were supplied principally through social marketing with a limited supply distributed through health care facilities.
However, there were a number of limitations and challenges during the SPM I period. The major challenges included: (1) inadequate capacity in the key strategic sectors, (2) shortage of human resource and rapid turnover of staff, (3) low coverage and poor uptake of PMTCT services, (4) inadequate HIV mainstreaming, (5) weak STI services, (6) low coverage of care and support services, (7) limited coverage of services for MARPs, (8) inadequate strategic information, and (9) weak non-health management information system (MIS).
3.ThematicAreasofSPMIIFive thematic areas were identified after a thorough analysis of the epidemic and the response during the SPM I (its major achievements, gaps and challenges). These include (1) creating enabling environment; (2) intensifying HIV prevention; (3) increasing access to and improving quality of chronic care and treatment; (4) intensifying mitigation efforts against the epidemic; and (5) strengthening the generation and utilization of strategic information
3.1. Creating Enabling EnvironmentThis thematic area has five components: (1) capacity building, (2) community mobilization and empowerment, (3) leadership and governance, (4) mainstreaming, and (5) coordination and partnership.
3.1.1. Capacity BuildingBuilding capacity is of utmost importance to sustain the gains in the fight against HIV/AIDS and accelerate the move towards universal access. Efforts of capacity building during SPM II (2010/11-2014/15) will focus on consolidating the capacity in the health sector and in the community to achieve universal access to HIV/AIDS services and MDG 6. Moreover, emphasis will be given to building the capacity of key strategic sectors, PLHIV associations, CSOs, and vulnerable and at-risk groups including youth and women, along with building the capacity of multisectoral response coordinating & governing bodies.

xii
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
3.1.2. Community Mobilization and EmpowermentConcerted efforts will be made to intensify and sustain the anti-HIV/AIDS community movement, engage and empower communities. Furthermore, due attention will be given to bring social transformation and create community ownership. All key actors at community level should be involved in the movement, and institutional support should be strengthened to meet the demands that follow intensified community mobilization.
3.1.3. Leadership and GovernanceLeadership and governance will be strengthened to create responsiveness and accountability in the multisectoral response against HIV/AIDS. The response to HIV/AIDS will be taken as a strategic development issue by all sectors at various levels.
3.1.4. MainstreamingMainstreaming of HIV/AIDS into core mandate of all sectors will be strengthened to prevent HIV epidemic and mitigate its impacts. The focus will be conducting an assessment of sectoral vulnerabilities, existing response capacity, and the impact of HIV/AIDS on the sector and to come up with sectoral polices, strategies, and action plans to mainstream HIV/AIDS using each sector’s own resources. During SPM II period, mainstreaming should be expanded to the private sector, Non Governmental Organisations and civil society organizations.
3.1.5. Coordination and partnershipCoordination of a multi-sectoral response against HIV/AIDS will be guided by this SPM in line with the principle of the “Three Ones”. “One country plan” and “one monitoring and evaluation system” will be taken as key tools to harmonize and coordinate the multisectoral efforts at all levels.
Partnerships will be strengthened to ensure an effective response against HIV/AIDS, create synergy and enhance efficient use of resources. Partnership guidelines will be developed to strengthen partnerships and networking.
3.2. Intensifying HIV PreventionThe fight against HIV/AIDS cannot be successful unless further spread of the epidemic is reversed and ultimately halted. This requires social transformation to reduce social, cultural and economic factors that make people individually or collectively vulnerable to HIV infection, as well as creating comprehensive knowledge and behavioural change on a mass basis among the population with particular focus on MARPS. Prevention of new HIV infection among young people and the adult population must be intensified using a combination prevention approach to address structural, behavioural, and biomedical issues in HIV prevention. A package of HIV prevention services for MARPs and PLHIV will be developed, implemented and scaled-up towards universal access.

2010/11-2014/15
xiii
3.3. Increasing access to and improving quality of chronic care & treatmentAs a result of improved ART services, HIV/AIDS is becoming a manageable chronic disease. Chronic care and treatment services will be further decentralized through the expansion of services, task shifting and improving service integration, linkages and referral systems.
Barriers to service delivery will be addressed by increasing the number and quality of human resources, availing treatment for opportunistic infection and ARV drugs, as well as strengthening logistic, laboratory and health management information system. Special emphasis will be given to improve adherence and retention of patients on treatment.
3.4. Strengthening care and support services to mitigate the impact of AIDSMitigating the devastating impacts of HIV/AIDS is essential to improve the livelihoods of those infected and affected. Care and support services will be provided to orphans and vulnerable children (OVC) and PLHIV in their familial network through a sustainable approach. Efforts will be made to reduce dependency by scaling-up income generation activities to the needy OVCs and PLHIVs.
3.5. Enhancing generation and utilization of strategic informationTo institute evidence based/informed policy making, program planning and management of HIV/AIDS response, generation and utilization of strategic information will be improved. Efforts will be enhanced to match the response to the epidemic by continuous generation and use of strategic information. Capacity to generate and use strategic information will be strengthened in key sectors by integrating of HIV strategic information into sectors’ management information system.
4.MonitoringandEvaluationMonitoring and evaluation of the multi-sectoral response to HIV/AIDS will be strengthened at all levels. Response inputs, processes, outputs, outcomes, and impacts will be monitored and evaluated using routine reports, surveillances, surveys, and studies. A functional M and E system will be instituted by developing an appropriate system and strengthening M and E capacities at all levels. Appropriate indicators are identified in order to verify the achievement of the set targets for SPM II. Mid-term and final evaluations of the SPM will be conducted.

5.8 millionpeople were tested for HIV just in one year (in 2009)
200,000 students received life skills trainings
millionsof people were reached by CC
condoms were distributed during 2004-2008286 million
self-help groups were established49,147PLHIV ever started ART73%

IntroductionPart One

2
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
1.1. Situation Analysis
1.1.1. General Background Ethiopia has a population of 79.8 million. The country is a Federal Democratic Republic and administratively composed of nine National Regional States and two city administrations, with 750 Woredas (districts). The major health problems of the country are communicable diseases, most of which are preventable. In 2007/2008 potential access to primary health care had reached 89.6%.
1.1.2. Trends and Status of the HIV EpidemicEthiopia is among the countries most affected by HIV and AIDS. The existence of HIV infection in Ethiopia was recognized in the early 1980s with the first two AIDS cases reported in 1986. Since then, the epidemic has rapidly spread throughout the country. The epidemic peaked in the mid-1990s. Since 2000 the epidemic has declined in major urban areas and stabilized in rural settings. According to projections based on the single point estimate the national adult HIV prevalence for 2009 was estimated at 2.3% with 1,116,216 People Living With HIV/AIDS (PLHIV) and 855,720 orphans due to AIDS. For the same period the total number of Orphans and Vulnerable Children (OVCs) in the country was estimated at 5.4 million. There were an estimated 44,751 deaths due to AIDS in 2009. The number of AIDS-related deaths would have been much higher had it not been for the free Anti-Retroviral Therapy (ART) program which has been scaled-up in an accelerated manner since 2005. The estimated national adult HIV incidence of 0.28% in 2009 translates to over 131,000 new HIV infections. With the current status, it is evident that HIV and AIDS remains a formidable development challenge to the country.
1.1.3. Heterogeneity of the EpidemicThe HIV epidemic in Ethiopia is heterogeneous between different geographic areas and population groups. Five regions: Amhara, Tigray, Oromia, Region of Southern People Nations and Nationalities (SNNPR) and Addis Ababa account for 93.4% of total PLHIV population in the country. Across all the regions, urban and female populations are more affected than rural and male population.
Part One:Introduction

2010/11-2014/15
3
In 2009, the national urban HIV prevalence was 7.7% and an estimated 695,413 people living with HIV (PLHIV) resided in urban areas, which accounted for 62.3% of the total HIV positive population in the country. While the urban HIV epidemic presents a declining trend in major urban settings, small towns are emerging as hot-spots, according to findings of Demographic and Health Survey (DHS) 2005. There is considerable variation in urban epidemics from region to region with urban HIV prevalence ranging from 2.3% in Somali region to 10.9% in Afar region in 2009, and urban HIV incidence ranging from 3.52% and 3.0% in Afar and Amhara to 0.56% and 0.71% in Somali and Gambella regions respectively. There is also variation in the urban HIV prevalence among big regions: Oromia (6.1%), SNNPR (7.2%), Amhara (9.9%), and Tigray (10.7%).
The national rural HIV prevalence was 0.9% in 2009. The number of PLHIV living in rural areas estimated to be 420,802, accounts for 37.7% of the total population of PLHIV in the nation. The epidemic in rural settings is generalized but varies significantly from region to region with rural HIV prevalence ranging from 0.4% in Somali region to 1.4% in Amhara.
The likelihood of the further spread of HIV to rural settings is increasing as small towns are becoming hot-spots and bridging the urban epidemic with rural settings. As a result, it is necessary for combination prevention packages be intensified and scaled up to the hot-spots.
According to various surveys and studies, women are more affected than men. DHS 2005 found that HIV prevalence among the female population to be twice that of the male population. In 2009, national HIV prevalence was 2.8% among women and 1.8% among men. An estimated 658,843 women were living with HIV in 2009, which accounted for 59% of total HIV positive population in the country.
Further look into age-specific HIV prevalence has indicated that young females aged 15-24 years are three times more affected than males in the same age group. HIV prevalence peaks at age group 15-24 years in females as opposed to 25-29 years in males.

4
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
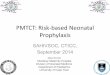
Table 1: HIV prevalence region, residence and sex in 2009
Region
AdultHIVprevalence(%)in2009
HIVprevalencebyResidencein2009
AdultHIVincidence(%)in2009
HIVincidencebyResidencein2009
HIVprevalencebysexin2009
Urban(%)
Rural(%)
Urban(%)
Rural(%)
Females(%)
Males(%)
Tigray 2.9 10.8 0.9 0.35 2.95 0.13 3.5 2.4Afar 2.1 10.9 0.9 0.27 3.52 0.25 2.5 1.7Amhara 2.8 9.8 1.4 0.34 3 0.36 3.4 2.2Oromia 1.5 6.1 0.6 0.17 1.82 0.11 1.8 1.2Somali 0.8 2.3 0.4 0.1 0.56 0.11 1 0.7Benshangul Gumuz 2 5.5 1.3 0.26 1.35 0.38 2.4 1.6
SNNPR 1.6 7 0.8 0.22 1.91 0.29 1.9 1.3Gambela 2.4 6.6 1.1 0.2 0.71 0.33 2.8 1.9Harari 3.5 5.2 0.3 0.51 1.51 0.06 4.2 2.8Addis Ababa 8.5 8.5 1.53 1.53 10.1 6.8Dire Dawa 4.6 5.9 0.5 0.68 1.74 0.16 5.5 3.7National 2.3 7.7 0.9 0.28 1.91 0.19 2.8 1.8
1.1.4. Most-at-Risk Population GroupsPopulation groups with most-at-risk of HIV infection include female sex workers, migrant workers, long distance drivers, uniformed forces, and discordant couples. Common settings with most-at-risk populations (MARPs) include economic and infrastructure development schemes, brothels, high transport corridors, refugee camps and surrounding populations.
1.1.5. Risk Factors Driving HIV Epidemic in EthiopiaThe two primary modes of HIV transmission in Ethiopia are heterosexual intercourse (87%) and vertical transmission from mother to child (10%) during pregnancy, delivery and breast-feeding.
The behaviour related risk factors for the epidemic in the country include:
• Practice of multiple concurrent sexual partnerships • Early initiation of sexual practices: The proportion with sexual debut before age 15 among the
15-19 years old boys and girls is high, and significantly higher among girls (11.1%) than boys (1.7%).
• Low and inconsistent condom use: Although there is a remarkable improvement in consistent condom use among female sex workers and uniformed forces, which reached as high as 90%, condom use among sexually active young people is still low. For instance, the 2005 DHS showed that only 40% of sexually active out-of-school youth aged 15-24 used condoms while having sex with a non-regular partner.
• Intergenerational and transactional sex. • Repeated episodes of Sexually Transmitted Infection (STIs) and low treatment seeking behaviours
for STIs.• Mobility/migration of population: Due to the current development investments, there are a
number of seasonal and migrant labourers in different parts of the country. Separation from their families for a prolonged time increases the likelihood of risky sexual practices.

2010/11-2014/15
5
• Unprotected sexual practices among discordant couples and HIV positives: The DHS 2005 showed that HIV prevalence among cohabitating individuals in urban areas was 10.9% of whom 72% were discordant.
• PMTCT and vertical transmission: The emerging epidemic pattern among couples of reproductive age, together with low prevention of mother-to-child transmission of HIV (PMTCT) service up take, means that vertical transmission continues to contribute significantly to the spread of HIV.
• Emerging behaviours: There are a number of emerging behaviours that make individuals and communities more at risk of acquiring and transmitting HIV infection in the country. These are injection drug use, substance abuse/dependency, anal sex and men having sex with men.
1.1.6. Vulnerability Factors and Drivers of the EpidemicThere are individual, socio-cultural, structural and institutional factors that influence and contribute to the spread of HIV in the country. These are:
• Lack of adequate knowledge and skills to protect one-self: According to the DHS 2005, only 55.3% of the in-school youth knew the three HIV prevention methods for sexual transmission of HIV and 26.6% had comprehensive knowledge about HIV and AIDS. In addition to the low level of the comprehensive knowledge, there is knowledge variation by sex.
• Socio-cultural norms: Harmful traditional practices such as female genital mutilation, abduction, women inheritance, acceptance of premarital and extramarital sexual practices, etc... are some of the beliefs and practices that may be fuelling the spread of the epidemic.
• Inaccessible and inadequate basic HIV service coverage, including information and education: PMTCT services and STI control and prevention services are not widely available in all health facilities.
• Poverty: Women disproportionately bear the burden of poverty due to low control over resources. Due to extreme poverty, young women engage in transactional sex with older men, while many women are forced to support their family by selling sex, putting them at greater risk of HIV infection.
• Gender inequality: Women are at greater risk of HIV infection as they are often not in a position to make decisions on matters affecting their own health including, sexual relations due to their socio-cultural and economic positions. Women increasingly bear the burden of AIDS resulting in higher stigma, discrimination and poorer access to services.
1.1.7. Impacts of AIDS There has been a noticeable decline in the estimated number of total annual deaths due to HIV/AIDS. The estimated death was 99,360 in 2005 while in 2009 it was 44,751. The decline in AIDS related deaths is mostly due to the wide availability of the free ART program in the country since 2005, initiated by the government in collaboration with development partners.
As the most sexually and economically active segment of population, 15-49 years old are highly affected by HIV/AIDS. Infection with HIV often results in considerable productivity loss due to recurrent illnesses and deaths with loss of skilled labour across the sectors and as a result, posing a challenge to the socio-economic development of Ethiopia. AIDS disrupts families and increases orphans and vulnerable children. It is estimated that the number of orphans due to HIV/AIDS in 2009 was 885,720.

6
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
1.2. Response AnalysisThe response to the HIV/AIDS epidemic in Ethiopia is a collective effort by the government, communities, faith-based organizations, community-based organizations, civil societies, associations of PLHIV, national and international non-governmental organizations, the private sector, and multilateral and bilateral donors and individuals. The response was guided by the national policy issued in 1998 and Strategic Plan for Intensifying Multi-Sectoral HIV/AIDS Response for the period 2004-2008 (SPM I).
The National AIDS Council was established in 2000, and was charged with directing and overseeing the multi-sectoral response. The Council, chaired by the President of the country and comprising members from government, NGOs, religious bodies, civil society, and PLHIV, has declared HIV/AIDS a national emergency. In June 2002, the National HIV/AIDS Prevention and Control Office (HAPCO) was established by proclamation to coordinate and lead the multi-sectoral response.
1.2.1. Major Achievements of the Response The major thematic areas in the SPM I (2004-2008) were capacity building, community mobilization and empowerment, integration with health programs, leadership and mainstreaming, coordination and networking and targeted responses. The major achievements, challenges and gaps are as follows.
1.2.1.1. CapacityBuildingThe major achievements under the capacity building efforts are: expanding and equipping of health facilities, technical and financial capacity building of public sectors, NGOs, faith-based and PLHIV associations and training of human resources.
The expansion of health infrastructure from 2004 to 2008 included an increase in number of health centres from 600 to 1,500 and a 20 percent increase in the number of hospitals from 119 to 143.
During the SPM-I period the number of service providers has increased, numerous HIV-related in-service and pre-service trainings were offered, new categories of health workers were added at the grass roots level (Health Extension Workers), and task shifting was introduced, to overcome the staff turnover and attrition.
• Short term trainings were provided to a large number of services providers. Intensive trainings have been given on various components of HIV programs by all partners.
• HIV was integrated in school curricula and in multi-purpose educational TV programs.• A number of teacher-training institutions, colleges and universities have incorporated life skills-
based HIV education into their curricula. • Investments were made on strengthening life-skills programs nationwide and in capacitating the
education sector, resulting in the development of education sector’s HIV policy and guidelines.• The capacity of PLHIV organizations has increased considerably and as a result, they have
started to become service providers. Associations of PLHIV are represented at governance and leadership structures of HAPCO, from Federal to Woreda level and are involved in the decision making processes and forums such as the Global Fund County Coordination Mechanism (CCM). In addition, several civil society organizations have been dynamic players in the HIV field.

2010/11-2014/15
7
1.2.1.2. SocialMobilizationandCommunityConversationSocial mobilization efforts, especially the Community Conversations (CCs), were successful in reaching millions of people and creating awareness about HIV and available services. CCs were used to advocate against harmful traditions and mobilize the community to mitigate the impact of HIV and AIDS.
• Better involvement of communities, mass organizations, faith based and civil society organizations in prevention, care, support, and impact mitigation services for PLHIV and OVC were observed.
• Awareness creation through social mobilization, especially during Millennium AIDS Campaign-Ethiopia (MACs), resulted in increased demand for and utilization of Voluntary Counselling and Testing (VCT), ART and other health services.
• Systematic involvement of community based organizations was observed. • Cultural and normative practices around marriage were challenged and are changing. Many
communities are encouraging or demanding mandatory premarital HIV testing and advocating to outlaw widow inheritance and abduction marriage.
• Income Generating Activities (IGAs) and other social support mechanisms are becoming more available.
1.2.1.3. IntegrationwithHealthProgramsSPM I had greater emphasis on the health sector to HIV/AIDS, and made great progress towards the strategic objective of “integration with health programs”. The Federal Ministry of Health spearheaded the implementation of integration. During this period considerable achievements have been made in expanding health facilities and services to the general population as well as to PLHIVs. Most achievements of health facility based HIV interventions can be attested to this fact. The accomplishments in this regard are highly creditable. However, the period has been criticized for putting insufficient emphasis on primarily prevention and non-health sector responses.
Availability and accessibility of health facility-based HIV services have increased from 658 and 129 in 2005 to 1596 and 843 in 2009, respectively, while free ART sites increased from 3 to 483 during the same period.
• Annual HIV Counselling and Testing (HCT) uptake has increased from 0.4 million in 2005 to 5.8 million in 2009. As a result 37 percent of the adult population know their HIV status. Millennium AIDS Campaign-Ethiopia (MAC-E) has made a significant contribution to this achievement.
• 73 percent of the PLHIV in need of treatment have been enrolled for ART as of 2009.• TB /HIV collaborative work, which started in six hospitals and three health centres in 2004, now
covers more than 330 health facilities in total. • The percentage of Tuberculosis (TB) patients counselled and tested for HIV increased from 10
percent to 80 percent.• Noteworthy investments have been made in infrastructure, including upgrading of health
facilities and procurement of equipment and supplies.

8
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
1.2.1.4. LeadershipandMainstreamingImproved leadership commitments and mainstreaming HIV in the workplace were observed at both national, regional and woreda levels. Most sectoral public agencies have recognized HIV as one of their core activities and some have gone as far as establishing a coordination office and allocating funding for HIV and AIDS activities. Noticeable strides have been made in involving leadership to actively guide HIV activities at all levels.
• Allocation of up to two percent of their budget for HIV has been initiated in many sectoral offices; additional funds are also raised through voluntary individual contributions of 0.5% to 1% of staff salaries, mainly to augment care and support activities.
• The level of commitment and active involvement of leaders from federal to woreda level has increased.
• The involvement of the First Lady in HIV work nationally and globally is a testimony to the leadership’s commitment to fight HIV.
• Provision of active leadership was evidenced by formation of AIDS councils at all levels, management and technical boards and Kebele AIDS committees broadly.
• Parliamentarians were trained to incorporate and monitor HIV activities in their respective constituencies.
• The involvement of religious and community leaders, as well as eminent Ethiopian personalities, in advocacy of HIV issues was greater than before.
• Some sectors developed workplace HIV policies and guidelines.
1.2.1.5. CoordinationandNetworkingTo ensure synergy of HIV programs in order to yield maximum impact and to increase efficient use of resources, it is necessary to work in coordination and through networking
• Responses guided by one agreed national action framework and use of one monitoring and evaluation system.
• Plan of action for Universal Access to HIV Treatment, Care and Support, 2007-2010 and a Road Map for Accelerated Access to HIV Prevention, Treatment, Care and Support, 2004-2006, and 2007-2010 were developed.
• Coordination and networking was achieved through regular joint review meetings and joint integrated support supervisions.
• Various task forces, and technical working groups comprising of stakeholders were established.• Efficient resource utilization was noted. • The national partnership forum was formed and hosted at federal level.
1.2.1.6. SpecialTargetGroupsHIV responses were generally targeting the whole community with some specific attention to certain groups like the urban population, military, OVC, PLHIV, in-and out-of-school youth, long distance track drivers, and commercial sex workers. These activities are the main areas for involvement of Nongovernmental Organization (NGOs), Community-Based Organization (CBOs) and Faith-Based Organization (FBOs).

2010/11-2014/15
9
• Over 400 school-based anti-AIDS clubs, more than 200 out-of-school anti-AIDS clubs, and 206 youth and recreational centres were established.
• 200,000 students received life skills trainings.• Over 286 million condoms were distributed during 2004-2008.• Over 450,000 orphans received various support services.• 92,537 PLHIV received basic social and financial services.• 195,000 benefited from free health care and education services. • 49,147 self-help groups were created.• 40,521 people were provided with short training on small business management and
employment.• Successful high risk corridor initiative focusing on prevention activities for long distance drivers.
1.2.1.7. MonitoringandEvaluation,SurveillanceandResearchIn addition to producing the routine monthly, quarterly, biannual and annual performance reports, Ethiopia has been conducting many researches and surveillances. The key ones are:
• ANC-based sentinel surveillances, 2005 and 2007• Behavioural surveillance surveys, 2005• Demographic health surveys, 2005• UNGASS report, 2006 and 2008. • Epidemiological synthesis, and • Health facility survey, 2005
1.2.2. Major challenges and gaps of the response • Lack of adequately trained and experienced human resources both in technical and administrative
areas.• Frequent turnover and attrition of skilled human resources.• Capacity building efforts for non-health sectors and the private sector appears to be limited.• Health centres in rural areas and hospitals are under equipped and understaffed.• Shortage of Opportunistic Infections (OI) drugs, test kits, laboratory reagents, Infection Prevention
(IP) materials and limited capacity in equipment maintenance were among the challenges. • The inadequate coverage and targeting of primary prevention programs and services, especially
those addressing most-at-risk populations and vulnerable groups.• The insufficient coverage of impact mitigating programs. • Continual inadequate performance in PMTCT and STI programs. • The referral system from primary health care units up to the tertiary level is frail, which creates
problems for ART compliance.• The response did not address the MARPs well.• Limited strategic information on HIV/AIDS • Delay in dissemination of results of surveys and surveillances.• The inadequacy of the monitoring and evaluation system for non-health HIV/AIDS activities.

”“The fight against HIV/
AIDS needs enhanced multisectoral and gender sensitive response, which empowers communities, and moves with shared sense of urgency, stronger partnership, greater involvement of PLHIV, and best use of resources...

Vision, Mission, Goal, Strategic Results, and Guiding Principles
Part Two

12
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Vision:To see Ethiopia free of HIV/AIDS
Mission:To prevent and control HIV/AIDS epidemic and mitigate its impacts by creating universal access to HIV prevention, treatment, care and support services through intensified community mobilization and empowerment, by building capacity and ensuring the active involvement and ownership across sectors, enhancing partnership under the principle of the “three ones”, and mobilizing and ensuring appropriate use of resources.
Goal:To reduce new HIV infections, AIDS related morbidity and mortality and mitigate its impacts.
Strategic Results:• Comprehensive knowledge and behavioural change created on individual and mass bases,• Reduced new HIV infection, and• Improved quality of lives of infected and affected people.
Guiding Principles
Multisectoralism: The HIV/AIDS epidemic is posing a formidable challenge to the development of all sectors as illnesses and deaths from AIDS reduce productivity of their labour force. Responding effectively to the behavioural, social, cultural, and economic factors that make individuals and communities vulnerable to HIV infection and mitigating the associated crises of AIDS requires organized and concerted efforts from all actors in the public and private sector, NGOs, FBOs, PLHIV and communities at large. All sectors should mainstream HIV/AIDS prevention and control into their core mandates, plans and programmes. Hence, multi-sectoralism remains to be the core guiding principle of comprehensive and expanded response against HIV/AIDS.
Part Two: Vision,Mission,Goal,StrategicResults,andGuidingPrinciples

2010/11-2014/15
13
Empowerment: Families and communities should be empowered and own the HIV programs so as to halt and reverse the epidemic.
Shared sense of urgency: HIV/AIDS needs to be combated with a shared sense of urgency by all actors to reverse and stop further spread of the epidemic, mitigate its impacts and succeed in our fight against poverty.
Partnership: All sectors of the society have to be involved in order to effectively respond to the epidemic by minimizing duplication of efforts, pooling resources together, creating synergy and maximizing impact. Effective scale up of the HIV services requires a coalition approach, which accommodates all partners working within the national HIV strategic plan framework.
Gender sensitivity: The fight against HIV/AIDS cannot be successful unless it effectively addresses the social, cultural, and economic causes of gender inequality in our society. Women should be actively involved in the fight against HIV/AIDS and gender sensitive HIV/AIDS prevention and control programs should be ensured by all actors.
Together with PLHIV: Greater involvement of people living with HIV (GIPA) should be ensured in all programs of HIV/AIDS prevention and control at all levels.
Result Oriented: The investment on HIV/AIDS prevention and control programs should yield the expected results in averting new infections and improving quality of life of the infected and affected population. The response should be led by evidence based/informed planning and programming.
Best use of resources: Resources mobilized from external development partners, the government and communities should be utilized in an effective and efficient manner with accountability.

”“In order to effectively
progress towards achieving MDG 6 by 2015, there is a pressing need to intensify HIV Prevention, increase access to quality chronic care and treatment, and strengthen care and support services by creating enabling environment, and establishing system for an effective strategic information...

Thematic AreasPart Three

16
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
3.1. Thematic Area One: Creating an Enabling EnvironmentGeneral Objective: To create an enabling environment for scaled up and comprehensive HIV/AIDS multisectoral response.
This thematic area has five sub-thematic areas: (1) capacity building, (2) community mobilization and empowerment, (3) leadership and governance, (4) mainstreaming, and (5) coordination and partnership.
3.1.1. Capacity Building Specific Objectives:• To ensure the capacity of the health sector to achieve Millennium Development Goals 6 (MDG
6) by 2015. • To build the capacity of key and strategic sectors, civil society organizations (CSOs) and private
sectors to contribute to the achievement of MDG 6 by 2015.Strategies:• Strengthen the capacity of the health sector.• Build the capacity of key sectors, CSOs and the private sector
Strengthening the health sector is indispensable to ensure effective HIV/AIDS multisectoral response. The expansion and equipping of health facilities together with availing adequate skilled human resource in the health facilities as well as at different levels of management of the health system is an important component of building the capacity of the health sector.
Building the capacity of key sectors and communities is also of utmost importance to intensify the fight against HIV/AIDS. In order to move towards the achievements of MDG 6 by 2015 (“to halt and reverse the spread of HIV”), there is a real and pressing need for creating adequate capacity at community and institution levels.
Capacities of key sectors that can have significant effect on the fight against HIV/AIDS such as, Education, Health, Mining, Defence, Industry, Communication , Culture and Tourism, Transport, Women, Children and Youth , Labour and Social, Water and Energy, Trade, Agriculture, Civil service, Urban Development and Construction, Federal affairs and Ministry of Finance and Economic Development, need to be
Part Three:ThematicAreas

2010/11-2014/15
17
strengthened. In addition, the building of leadership across sectors and communities and strengthening the capacity among stakeholders such as Most At Risk Populations (MARPs), Network of Networks of HIV Positive in Ethiopia (NEP+), Ethiopian Inter-faith Forum for Development, Dialogue and Action (EIFDDA) and other Civil Society Organizations (CSOs) is crucial to synchronize and harmonize efforts towards a common goal.
Interventions:• Support the expansion of health centres.• Support universities and colleges to provide pre-service training for health science students.• Train health workers on HIV/AIDS.• Staff key sectors with experts on prevention and impact mitigation.• Provide support to federal sectors to build the capacity of regional sectors on HIV. • Prepare health facilities for people with disability.• Build the capacity of networks of associations of PLHIV, OVC, elderly people, people with
disability, CSOs and FBOs.• Provide support to associations of PLHIV, OVC, the elderly, people with disability, CSOs and FBOs.
3.1.2. Community mobilization and empowermentSpecific objective: • To sustain community movement and attain social change by 2015.
Strategies:• Ensure community ownership and leadership of HIV/AIDS.• Augment community mobilization with behavioural change interventions.• Strengthen institutional support to community anti-AIDS movement.
Community mobilization and empowerment is crucial to attain success in the fight against HIV/AIDS. The anti-HIV/AIDS community movement should be anchored with the development and implementation of a concrete action plan. The community must own the movement and integrate an HIV/AIDS response into the existing socio-cultural and economic activities. Anti-AIDS community movement was intensified and over 80% of Kebeles across the nation covered with community conversation by the end of 2009.

18
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
However, social transformation, which can bring the required level of changes in behaviour and social norms, has not been fully realized in the community at large. Hence, there is a need to consolidate and intensify the anti-HIV/AIDS community movement to bring social transformation.
The movement should engage key players in the community including the youth, women, farmers through their associations, kebele administrations, health extension workers (HEWs), teachers and agricultural development agents, Iddirs, faith-based organizations, NGOs and PLHIV. The overall movement should be led by the Kebele administration with technical leadership provided by the HEWs.
Interventions:• Train community leaders. • Conduct community conversation.• Enforce relevant community by-laws.• Train Health Extension Workers (HEW) on Behavioural Change Communication (BCC).• Train community anti-AIDS promoters from model households.• Train health development armies (DA) on BCC.• Strengthen Kebeles to provide support to community anti-AIDS movement. • Document, share and scale-up best practices.
3.1.3. Leadership and Governance Specific objective: • To ensure responsiveness and accountability in the leadership and governance of the
Multisectoral HIV/AIDS response. Strategies:• Build the capacity of leadership and governing bodies at various levels.• Avail regular updates on the HIV/AIDS epidemic situation and response to leadership and
governance.• Ensure inclusion of HIV plans in the overall sector plan and oversight sector performance.
Strengthening leadership and governance is essential to create transparency, responsiveness and accountability in the multisectoral response against HIV/AIDS. Setting the response to HIV/AIDS as a national priority and strategic development issue by different sectors and enforcing its implementation requires a sustained leadership commitment from the executives and governing bodies at various levels.
Interventions:• Provide training on strategic leadership on the fight against HIV/AIDS to leadership and
governing bodies.• Select and document best practices.• Arrange experience sharing visits for leadership and governing bodies from the regions.• Disseminate annual performance reports and analytical reports on the epidemic and response.

2010/11-2014/15
19
• Establish AIDS Resource Centres (ARC) in the federal and regional parliament. • Provide oversight in the inclusion of HIV/AIDS plans in the overall sectors’ plans. • Conduct periodic review by the parliament and other governing bodies.
3.1.4. MainstreamingSpecific objective: • To enhance the HIV/AIDS response across sectors.
Strategies:• Strengthen ownership of HIV/AIDS programs across sectors.• Ensure the inclusion of HIV M and E into sectors’ management information system (MIS).
Mainstreaming HIV/AIDS prevention and control into core mandates and activities of various sectors (public, private and CSOs) is crucial to prevent further spread of the epidemic and mitigate its impacts. As HIV/AIDS is a development problem affecting all sectors, mainstreaming HIV/AIDS should be taken as a strategic issue to attain the development goals at all levels.
Interventions:• Conduct assessment on vulnerability and impact of HIV/AIDS and the capacity of the existing
response.• Develop sector specific policies, strategies and plans on HIV/AIDS.• Establish a unit for mainstreaming HIV/AIDS in both public and non-public sectors.• Ensure allocation of resources by all sectors for HIV/AIDS mainstreaming. • Incorporate monitoring and evaluation of HIV/AIDS into sectors’ MIS.
3.1.5. Coordination and Partnership Specific objective:• To ensure synergy of multisectoral HIV/AIDS response at all levels.
Strategies:• Build the capacity of HIV/AIDS response coordination of HAPCOs/ Health Bureau (HBs) at all
levels. • Strengthen partnerships at all levels.• Strengthen networking among service providers.
Strong leadership and broader coordination is required to translate the strategic plan into a viable annual plan of action. Adherence of a wide range of actors to the ‘Three Ones’ principles will anchor the production of a synchronized and harmonized annual plan and report. HAPCO will ensure coherence and close collaboration among development partners, CSOs, FBOs and the private sector with the aim of further aligning and harmonizing HIV activities in the country. Strengthening partnership forums and sub-forums is essential for effective coordination of the Multisectoral response.
Interventions:• Provide training on coordination.• Develop a joint annual plan guided by SPM II.• Institute one national multisectoral monitoring and evaluation system.• Develop partnership guidelines.

20
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
• Establish/ strengthen partnership forums at national, regional and woreda levels.• Strengthen partnerships for cross-boarder interventions. • Map HIV/AIDS service providers and stakeholders at all levels.• Establish/ strengthen linkages and networking of HIV/AIDS services.
3.2. Thematic Area Two: Intensifying HIV PreventionGeneral Objective: To reduce the rate of new HIV infections by 50 percent (from 0.28% in 2009 to 0.14% by 2014/15).
Specific Objectives:• To increase comprehensive knowledge on HIV among the adult population aged 15-49 from
22.6 percent in 2005 to 80 percent by 2014/15.• To reduce the percentage of young people, aged 15-19 years, who start sexual debut at age of
15 years from 8.4 percent in 2005 to 1.7 percent (Female from 11.1 percent to 2.2 percent and male from 1.7 percent to 0.34 percent) by 2014/15.
• To increase the percentage of young people aged 15-24 years, who use condoms consistently while having sex with non-regular partners from 59 percent in 2005 to 80 percent by 2014/15.
• To increase percentage of female sex workers reporting consistent use of condom from 93.4 percent in 2005 to 98 percent in 2014/15.
There were enormous efforts by the Government of Ethiopia to increase the availability and accessibility of HIV prevention services during the SPM I period. However, the evaluation of SPM I revealed that the scale of primary HIV prevention efforts was insufficient to stop the progress of the HIV epidemic. Moreover, primary HIV prevention efforts must target non-infected individuals that are vulnerable and at risk to HIV infection.
In general, all preventive services need to be expanded and made available to the broader population in both urban and rural areas. These services should also be expanded to specific population groups, including sex workers, in-school and out-of-school youth, uniformed services, migrants, residents of small market towns and new business opportunity sites (large scale farms, construction sites, mining, etc...) refugees and displaced populations including cross-border populations and populations with special needs like people with disability and the elderly.
Even though there is a need to expand treatment, care and support services further, prevention of new HIV infections needs to remain the cornerstone of the national HIV response in Ethiopia. Creating comprehensive HIV knowledge, increasing self-risk perception and promoting behavioural changes at a population level must be intensified, targeting highly vulnerable and at- risk populations to maximize the yield of efforts. The universal access targets can be achieved only if primary prevention is intensified to the level that can enable a reduction of new infections.
To achieve maximum impact, prevention of new HIV infection should utilize a combination of proven behavioural, structural and biomedical approaches. HIV prevention strategies and interventions need to be evidence based and should work in a concerted manner towards shared prevention goals. Knowing the epidemic and matching the response to the epidemic is the key guiding principle in developing successful prevention interventions. Under this thematic area, there are three sub-thematic areas: behavioural, structural and biomedical HIV prevention approaches.

2010/11-2014/15
21
3.2.1. Behavioural HIV Prevention Approach Expansion of behavioural change programs addressing the general population and MARPs is a key component of the combination prevention intervention strategy. The behaviour change intervention approaches need to be refined, re-focused, intensified and scaled-up in all communities to result in increased comprehensive knowledge on HIV/AIDS, delay of onset of initiation of sexual intercourse, increased self-risk perception, decrease in the number of unprotected sexual acts, reduce the number of sexual partners, increase demand for biomedical HIV prevention services like counselling and testing, STI treatment and use of condom. Behavioural intervention should be combined with interventions that address structural issues and the provision of biomedical HIV prevention services.
Strategies:• Strengthen community based HIV prevention interventions to address the general population.• Strengthen workplace HIV prevention interventions.• Strengthen school based HIV prevention interventions.• Scale-up comprehensive prevention interventions addressing MARPs.• Strengthen out-of-school youth HIV prevention programs.• Intensify secondary prevention. • Intensify HIV prevention in development schemes including new business opportunity locations.• Scale-up HIV prevention among population groups with special needs.
3.2.1.1. StrengthencommunitybasedHIVpreventioninterventionstoaddressthegeneralpopulation
Community Conversation has evolved as one of the key tools for community capacity enhancement to bring about sustained social change at individual, family and community level. CC is used for diagnosis, priority setting and community level response to fight against HIV/ AIDS in the country. In addition, CC was recently taken as a best practice by the health sector and adopted as a way to strengthen health promotion and prevention of other communicable diseases such as malaria and TB.
Interventions:• Ensure the scale-up of quality CC and integrate with existing community structures.• Review existing CC guidelines and training manuals.• Conduct training for volunteer community anti-AIDS promoters (VCAP) or model families.• Develop and disseminate HIV prevention messages using print and electronic media.
3.2.1.2. StrengthenWorkPlaceHIVpreventioninterventionMainstreaming HIV/AIDS is a process of analysing how HIV/AIDS impacts on all sectors now and in the future, both internally and externally. It entails sectors to conduct risk assessment and design appropriate work place interventions accordingly.
Interventions:• Develop Organisational Conversation (OC) guidelines and training manual. • Provide training on OC.• Conduct OC in work places.• Conduct condom promotion and distribution in the work place.

22
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
3.2.1.3. Strengthenschool-basedHIVpreventioninterventions.Preventive interventions must start at a younger age in order to create behaviour change and generate far-reaching knowledge on HIV/AIDS. School interventions must be age-appropriate and particular emphasis should be given to rural areas, secondary schools and tertiary education. Gender sensitive HIV and reproductive health interventions, which are expected to enhance life skills, including negotiation, decision making and adoption of safer sexual behaviours, will be implemented in all primary and secondary schools, as well as in public and private tertiary education institutes.
Interventions:• Conduct peer education programs in schools, higher education institutes and Technical and
Vocational education and training (TVET).• Conduct life-skill education in schools, higher education institutes and TVET.• Conduct school based CC in high schools, higher education institutes and TVET. • Integrate HIV/AIDS into school curriculum.• Train teachers on management of school HIV/AIDS programs.• Develop and disseminate targeted BCC message in schools, higher education institutes and
TVET. • Strengthen youth leadership development programs.• Develop an HIV intervention strategy for school and higher education. • Strengthen anti-AIDS clubs in schools, and higher education institutes and TVETs.• Ensure active participation/ membership of students in anti-AIDS clubs of schools in higher
education institutes and TVET.• Expand ARC in schools, higher education institutes and TVET.
3.2.1.4. HIVpreventionprogramsforout-of-schoolyouthHIV prevention programs are important to young people who are out of the school system. The coverage and quality of the existing HIV prevention services needs to be further intensified. These include peer education, outreach HIV education and youth friendly HIV services. HIV prevention interventions focusing on young women, including domestic workers and expansion of edutainment centres to all Woredas will be given due attention.
Interventions:• Expand/strengthen educational entertainment (edutainment) in youth centres in district towns. • Train Peer educators on HIV.• Implement outreach youth interventions.• Conduct youth dialogue.
3.2.1.5. CombinationPreventioninterventionsaddressingMARPsImproving the effectiveness of efforts to contain and reverse the spread of HIV requires identification of populations at risk of HIV infection, define what prevention measures are essential for these populations, and ensure adequate delivery of essential prevention measures to the identified populations. Prevention strategies and activities will be tailored and delivered as a package to address

2010/11-2014/15
23
the needs of the MARPs. Regions must have specific intervention plans based on evidence on the regional situation and their respective response analysis to give special attention to risk groups existing in their respective areas.
Interventions:• Determine the identity, size, behavioural characteristics and HIV prevalence among MARPs.• Map MARPs service providers.• Develop a package of HIV behavioural services for MARPs.• Develop comprehensive communication strategy for MARPs.• Build the capacity of CSOs to provide outreach HIV education to MARPS.• Provide comprehensive HIV prevention services to MARPs.
3.2.1.6. IntensifyingHIVpreventioninthedevelopmentschemesIt is important to focus on newly created development opportunities and commercial activities that can provide fertile ground for the spread of HIV due to increased vulnerability and/ or lack of access to HIV prevention services. Construction sites (dam and road), large-scale farms (flowers and sugar cane), mining, and the likes will be given due attention and will be targeted by HIV prevention programs. Assessment of the response capacity in development schemes of public and private sectors will be taken as the initial step to either revitalize or scale-up HIV prevention interventions. Based on the assessment of vulnerability and response capacity, development schemes/ projects will create workplace interventions and guidelines, integrating HIV prevention into their overall development program/ projects. HIV/AIDS activities will be included in the appraisal criteria of projects of development schemes. Ensuring implementation of HIV/AIDS activities will be among the duties and responsibilities of project coordinators.
Interventions:• Target business opportunity locations, industries and private development schemes. • Integrate HIV prevention in the project proposals of development schemes. • Develop and disseminate targeted HIV/AIDS messages.• Conduct peer education. • Referral and linkages with health facilities for VCT, STI and ART services. • Ensure HIV prevention among development schemes/projects areas communities.
3.2.1.7. Scale-upHIVpreventionamongpopulationgroupswithspecialneedsTailored HIV prevention programs will be scaled-up to reach population groups with special needs such as people with disability and elderly. Interventions to such groups will be designed in a manner that addresses and fits the groups’ special need.
Interventions:• Conduct risk and vulnerability assessment.• Develop prevention strategy for people with special needs.• Customize HIV intervention guidelines and implementation manuals.• Integrate BCC interventions in ARC of youth centres for people with disability. • Develop and disseminate BCC materials for people with special needs.

24
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
3.2.2. Structural HIV Prevention Approach Reduction of vulnerability factors that impair the ability of individuals and communities to avoid HIV infection will have great contribution to curb the spread of HIV in the country. Structural interventions that address factors such as gender inequality, poverty, socio-cultural norms, stigma and discrimination need to be intensified.
Strategies:• Address gender inequality.• Reduce economic vulnerability.• Address socio-cultural factors.• Protect human rights and provide legal support.
3.2.2.1. AddressgenderinequalityAddressing gender inequality, including gender-based violence (GBV) will be promoted. HIV programs will be encouraged to systematically mainstream gender, including integration into sectoral policies and programs. Awareness creation and punitive approaches must be implemented on perpetrators of GBV. HIV post exposure prophylaxis will be available to victims of rape.
Interventions:• Mainstream gender into sectoral policies. • Avail PEP to victims of rape.• Advocate for punitive measures on perpetrators of GBV.• Ensure inclusion of gender dimension in HIV programs.
3.2.2.2. ReduceeconomicvulnerabilityPoverty is one of the driving factors that increase individual’s vulnerability to HIV infection. Women with low income, unemployed youth and orphans are such groups who need support to enhance their ability to avoid HIV infection.
Interventions:• Provide IGA support to vulnerable women.• Integrate HIV/AIDS services with safety-net programs.
3.2.2.3. Addresssocio-culturalfactorsSocio-cultural norms and deep rooted beliefs and practices are fuelling factors that increase people’s vulnerability to HIV/AIDS. Addressing socio-cultural issues that contribute to the spread of the epidemic such as harmful practices and GBV need to be intensified.
Interventions:-• Address harmful traditional practices that fuel HIV/AIDS.

2010/11-2014/15
25
3.2.2.4. ProtecthumanrightsandprovidelegalsupportInterventions targeting stigma and discrimination, and protection of human rights will be given due consideration during SPM II.
Interventions:• Implement the principles of the “greater involvement of people living with HIV/AIDS (GIPA)”.• Conduct the national stigma index study.
3.2.3. Biomedical HIV Prevention Approach Biomedical HIV prevention consists of strategies and interventions implemented as part of the health sector response to HIV/AIDS. The services need to be accessible and meet the demands of the general population, MARPs and population groups with special needs.
Strategies:• Ensure access and enhance uptake of HIV counselling and testing services.• Ensure access and enhance uptake of PMTCT services. • Increase availability and utilization of STI services.• Increase supply, distribution and utilization of male and female condoms.• Ensure infection prevention and safe blood supplies in health system. • Avail post exposure prophylaxis (PEP).• Accelerate male circumcision, in areas needed.• Provide user-friendly biomedical services to people with special needs and MARPs.• Intensify positive prevention.
3.2.3.1. EnsureaccessandenhanceuptakeofHIVcounsellingandtestingservicesThis strategy aims at enabling knowledge of one’s HIV status and linking those who test positive to HIV to relevant chronic care services.
Interventions:• Promote HIV testing using CC and health extension workers as well as mobile, outreach services. • Promote HCT by the development armies.• Educate households on HCT by health development armies.• Promote HIV testing through religious leaders, local community leaders.• Educate the general public on HIV testing though mass media campaigns.• Provide training to HCT service providers.• Provide HCT to people with disability.• Ensure uninterrupted supply of test kits and other accessories. • Rollout HCT services into private health facilities.
3.2.3.2. EnsureaccessandenhanceuptakeofPMTCTservicesPMTCT is one of the weakest programs that requires multiple and combined strategies to address the current challenges and improve service utilization.

26
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Interventions:• Strengthen the integration of PMTCT with MNCH in all health facilities.• Mobilize the community to be actively involved in PMTCT. • Promote PIHCT for all pregnant women attending ANC and delivery services.• Ensure male involvement in PMTCT service.• Train health extension workers on PMTCT and delivery service provision.• Promote PMTCT by the health development armies.• Provide training to health development armies on PMTCT.• Provide education to households on PMTCT by health development armies.• Expand PMTCT services.• Equip health facilities with ANC and delivery equipment.• Train health workers on basic and emergency obstetric care and PMTCT service provision. • Deploy mother support mentors in each PMTCT site.• Provide PMTCT training for service providers to people with disability.• Build capacities of private health facilities to rollout PMTCT service.• Involve private health facilities to provide PMTCT services.
3.2.3.3. IncreaseavailabilityandutilizationofSTIservicesSTI services need to be revitalized in all health facilities through implementation of syndromic case management.
Interventions:• Create strong leadership for STI programs.• Expand STI services to all health facilities. • Intensify health education to improve treatment seeking behaviour and utilization of STI services. • Promote partner notification during STI case detection.• Ensure availability of drugs and reagents in all public health facilities.• Train heath care workers on syndromic STI case diagnosis and management. • Train laboratory technicians to perform various bacteriological and serological tests.• Develop STI follow-up and data validation system.• Provide STI training for service providers to provide user-friendly services to people with
disability.
3.2.3.4. Increasesupply,distributionandutilizationofmaleandfemalecondomsAdequate supply and distribution of male and female condoms to distribution points that are easily accessible is among one of the important HIV prevention strategies for which a number of interventions are designed.
Interventions:• Develop national condom strategy. • Promote and conduct campaigns on correct and consistent use of condom.

2010/11-2014/15
27
• Expand peripheral outlets of condom distribution.• Conduct targeted condom distribution, particularly to MARPs.• Ensure adequate supplies of condoms.• Distribute male and female condoms.
3.2.3.5. EnsureinfectionpreventionandsafebloodsuppliesinHealthsystemInfection prevention (IP) and safe blood supply are important strategies to ensure safe environment of the health facilities with regard to HIV transmission, and HIV free blood supply.
Interventions:• Ensure the availability of adequate infection protective materials. • Improve waste disposal management in health facilities. • Provide IP trainings to staff.• Implement national blood transfusion services strategy.
3.2.3.6. Availpostexposureprophylaxis(PEP)treatmentAccessible post exposure prophylaxis is an important strategy that needs to be ensured for all eligible individuals, according to the National guideline.
Interventions:• Conduct assessment on prevalence needle pierce/ prick & other sharp materials in health
facilities.• Avail PEP at health facilities.
3.2.3.7. AcceleratemalecircumcisioninareasneededRecent studies conducted in three African countries show that male circumcision has about a 60 percent protective effect to male. The evidence suggests that it is a highly cost-effective strategy in preventing HIV among non-circumcised adolescent and adult male population. In some parts of the country, such as in Gambella, the reported male circumcision prevalence is less than 50 percent while the male HIV prevalence in the region is high. Cognizant of this fact, male circumcision is proposed as one HIV prevention strategy in selected areas.
Interventions:• Promote male circumcision.• Provide trainings on male circumcision.• Avail male circumcision kits.• Provide safe male circumcision services.
3.2.3.8. EnsureuserfriendlybiomedicalservicestospecialpopulationgroupsInterventions:• Conduct consultative meetings to identify modalities of providing biomedical HIV/AIDS services
for people with disability and the elderly.

28
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
• Conduct assessment of health facilities to evaluate user friendliness to the elderly and people with disability.
• Develop strategic documents to define package of HIV /AIDS services and modalities of delivering the services for People with disability and the elderly.
• Customize and disseminate HIV/AIDS-related training manuals for people with disability and the elderly.
3.2.3.9. IntensifyingpositivepreventionEffective positive prevention requires information, training and support for HIV positive people and their partners. It is important to ensure that HIV positive people have access to information, education, commodities and services they need so that they are better able to exercise positive living that helps in preventing transmission of HIV to others.
Interventions:• Provide HIV information, education and risk reduction education and counselling.• Strengthen couple counselling and testing.• Conduct family-based HIV counselling and testing.• Develop a special package on HIV counselling, Reproductive Health, and related issues for
adolescents on chronic care and treatment. • Provide services to HIV positive adolescents based on the package.• Establish/ strengthen post-test clubs and other peer support groups.• Distribute condom sand provide education on correct and consistent condom use. • Provide STI services.• Provide family planning services.
3.3. Thematic Area Three: Increase Access to and Improve Quality of Chronic Care and Treatment
General Objective: To reduce HIV-related morbidity and mortality and improve quality of life of PLHIV.
Specific Objectives:• To increase ART enrolment from 73 percent in 2009 to 95 percent in 2014/15.• To increase survival rate among those who started ART to 85 percent in 2014/15.• To increase patient retention rate among those who started ART from 73 percent to 85 percent
in 2014/15.• To improve paediatric ART coverage from 66 percent in 2010/11 to 90 percent in 2014/15.• To increase percentage of pre-ART patients eligible for and taking cotrimoxazole prophylaxis
from 68 percent in 2009 to 95 percent in 2014/15. Strategies:• Expand treatment and care services with strengthened service linkage and integration.• Strengthen laboratory and referral systems.• Improve TB/HIV collaborative activities.• Ensure availability of essential OI and ARV drugs and reagents.

2010/11-2014/15
29
• Enhance treatment literacy and adherence counselling.• Strengthen provision of chronic care and treatment services in the private sector.• Address human resource issues.
3.3.1. Expand chronic care and treatment services Provision of chronic care and treatment is an indispensable strategy for the effective prevention and control of HIV/AIDS. The services need to be accessible in all hospitals and health centres, and adherence to the treatment needs to be improved.
Interventions:• Provide training of health personnel on chronic care and treatment.• Strengthen intra-and inter-facility service linkages by developing standard operating procedures
(SOP).• Increase number of health facilities providing ART.• Develop and disseminate ART-related service package and training manual for people with
disability.• Integrate ART-related service package for people with disability in the existing health facilities.
3.3.2. Strengthen TB/HIV Collaborative activitiesThis is an important strategy to reduce the burden of TB and HIV in patients affected by both diseases.
Interventions:• Screen all diagnosed TB patients for HIV.• Link HIV positive TB cases to HIV services.• Screen all HIV positive cases for TB.• Provide INH prophylaxis for eligible patients.• Strengthen TB-HIV co-infection management.
3.3.3. Strengthen laboratory and referral system Chronic care and treatment sites require access to laboratory services directly or through an effective laboratory referral system.
Interventions:• Avail minimum laboratory services at chronic care sites.• Strengthen preventive and curative maintenance (training, workshop and spare parts).• Strengthen quality assurance system. • Strengthen laboratory information system.• Build capacity of laboratory personnel.• Strengthen HIV laboratory services.
3.3.4. Ensure supply management system in relation to availability of essential OI, ARV drugs and reagents
The availability of essential OI and ARV drugs and reagents must be ensured all the time in the sites that provide the services. This requires ensuring the existence of strong supply management system.

30
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Interventions:• Forecast the need for OI, ARVs and reagents.• Ensure timely procurement and distribution of OI and ARV drugs and reagents.• Expand warehouses.• Strengthen logistics management information system.• Equip the supply management system with transportation services.
3.3.5. Enhance treatment literacy and adherence counsellingTreatment literacy and adherence are very important strategies to ensure effective provision of chronic care and treatment services. This includes interventions that will help to reduce patients who discontinue treatment, as well as interventions that will help to trace lost to follow up patients.
Interventions:• Develop and enforce guidelines on treatment literacy and adherence.• Strengthen adherence counselling by health care workers, case managers and adherence
supporters.• Disseminate treatment literacy education through mass media.• Institute periodic monitoring and follow-up of lost to follow-up patients.• Provide ART training for service providers on user friendly service provision to people with
disability.• Rollout ART services into private health facilities.• Strengthen clinical mentoring. • Increase number of adult and paediatric service beneficiaries receiving ART.
3.3.6. Strengthen provision of chronic care and treatment in the private Health sector
The number of private health facilities is growing with time. Private health facilities are mainly found in urban areas. Availing HIV/AIDS services in these facilities is very important to increase access, reduce the burden on public health facilities, as well as provide alternatives to patients so they access services wherever it is convenient for them. Considerable number of the urban population utilizes private health facilities. There is a clear indication of the need to strengthen the ongoing public-private partnership in order to improve access and utilization of HIV/AIDS services.
Interventions:• Map and create directory of private health facilities.• Organize public-private partnership forum.• Develop and avail guidelines, which direct the process of providing chronic care and treatment
service.
3.3.7. Address human resource issuesEnsuring availability of adequately trained human resource is among the major strategic issues to achieve universal access to HIV/AIDS services.

2010/11-2014/15
31
Interventions:• Support higher learning institutions to provide pre-service HIV/AIDS training to all health science
students.• Provide in-service training on HIV/AIDS in health sector.• Strengthen task-shifting, clinical mentoring and supportive supervision.• Train health facility leaders on HIV/AIDS program management and integration of services.• Promote involvement of staff in health facilities to conduct operational research.
3.4. Thematic Area Four: Strengthen Care and Support Services to Mitigate the Impact of AIDS
General Objective: To improve the livelihood of the needy OVC and PLHIV.
Specific objectives: • To increase care and support to needy OVC from 30 percent in 2009 to 50 percent by 2014/15.• To increase care and support to needy PLHIV from 60,000 in 2009 to 100,000 in 2014/15.
Strategies:• Strengthen the involvement of local communities in care and support.• Enforce the provision of standardized care and support to OVC and PLHIV. • Enhance school based OVC support.• Strengthen income generation activities to sustain the program.
3.4.1. Strengthen the involvement of local communities in care and supportThe involvement of the community and growing ownership of care and support services to OVCs is the basis for sustainable provision of the services.
Interventions:• Strengthen and use existing community structures.• Map care and support needs in each Kebele with existing care and support projects and identify
gaps.• Provide care and support to OVC in their familial networks.
3.4.2. Enforce the provision of standardized care and support to OVC and PLHIVThere is a need to have appropriate standards for the provision of care and support services to OVCs as well as to PLHIV. This helps to ensure efficient use of resources in providing effective care and support services in terms of HIV prevention and control.
Interventions:• Develop OVC care and support standard and service delivery guidelines. • Conduct OVC situational analysis and map OVC services. • Develop referral networks among service providers. • Strengthen school-based OVC support activities.• Provide home-based care services for PLHIV.

32
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
3.4.3. Strengthen income generating activities to sustain the program Income generation activities will be strengthened to ensure productivity of the beneficiaries thereby ensuring self-reliance which in turn significantly contributes to the sustainability of the care and support services.
Interventions:• Provide IGA support.• Follow and support IGA beneficiaries and create links to markets.
3.5. Thematic Area Five: Strengthen Generation and Utilization of Strategic Information
General Objective: To ensure timely generation and utilization of strategic information and thus enhance evidence-based decision making for the multisectoral HIV/AIDS response.
Specific Objectives:• To ensure the generation of quality data from routine program monitoring, surveys, surveillances
and studies. • To disseminate and utilize strategic information to guide policy formulation, program planning
and improvement. Strategies:• Build the capacity for monitoring and evaluation.• Institute a culture of evidence-based/informed decision-making.• Strengthen timely generation of strategic information.• Enhance dissemination and utilization of strategic information.
3.5.1. Build the capacity for Monitoring and Evaluation (M & E)Building M and E capacity at all levels requires due attention. This includes developing various manuals and ensuring availability of skilled human resource at various levels of implementation.
Interventions:• Ensure availability of HIV/AIDS M and E HR capacity at multilevel. • Develop M and E implementation manual and training manual.• Conduct training for M and E officers.• Establish/strengthen regional HIV M and E Technical Working Groups.
3.5.2. Institute culture of evidence-based/ informed decision makingThe monitoring and evaluation of HIV /AIDS multisectoral response at various levels, as well as the planning process need to be based on evidence for which it is important to institute culture of informed decision making. This helps to ensure timely and progressive achievements.

2010/11-2014/15
33
Interventions:• Establish framework for generation and utilization of strategic information. • Enforce evidenced-based planning and prioritization.• Conduct regular review of HIV programs performance.• Establish database for HIV/AIDS M and E• Conduct advocacy workshops on M and E at all levels.
3.5.3. Strengthen timely generation of strategic informationThe timeliness of information that will be generated for use is very important to ensure an appropriate response during an appropriate period of time.
Interventions:• Work with sectors to include HIV/AIDS indicators within their own monitoring and evaluation
systems. • Conduct HIV surveillance.• Conduct effectiveness study on interventions.• Identify priority research agendas and conduct research. • Develop and implement community based information system to be used at all levels.
3.5.4. Enhance dissemination and utilization of strategic informationIt is important to take into account that the strategic evidence/information generated should be disseminated and utilized for practical purposes. It also helps to disseminate best practices which will help to strengthen the overall response to the epidemic.
Interventions:• Disseminate research and evaluation findings regularly. • Prepare, print and distribute HIV/AIDS M and E reports regularly.• Prepare summary of key HIV evaluation and research findings and post reports on web sites.• Document and disseminate best practices.

By the end of 2014/15:
384health centers will be constructed and equipped
3,303health centers will provide ART service
85%of HIV positive women will receive ARV prophylaxis
9.27 millionpeople will be tested for HIV annually
condoms will be distributed1.967 billion
students will receive HIV education each year13 millionpeople will receive BCC community outreach60 million
MARPs will be reached with HIV prevention programs1 million
will be ever started on ART484,966 PLHIV
will receive IGA support75,000 OVC and PLHIV

Five-year Programmatic Targets and Results Matrix
Part Four

36
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
4.1 Five-year Programmatic Targets
Ser. No Programs Indicators
Targets by yearBaseline(2009) 2010/11 2011/12 2012/13 2013/14 2014/15
1. Prevention1.1 BCC:
community outreach
Number of people reached through outreach with at least one HIV IEC/BCC
35M 50M 52M 55M 58M 60M
1.2 BCC: School Percentage of schools that provide life skills-based HIV education in the last academic year
38% 60% 75% 90% 95% 98%
Number of students ( 10 years& above) who received HIV education per academic year
11.7 M 12M 12M 13M 13M 13M
1.3 BCC: MARPs Number of most-at –risk population reached with HIV prevention programs
200,000 400,000 700,000 1,000,000 1,000,000 1,000,000
1.4 Testing and counselling
Number of adult people who received testing and counselling in the last 12 months
5.8M 9.271M 9.271M 9.271M 9.271M 9.271M
1.5 Condom Number of condoms distributed during the last 12 months
93M 367M 400M 400M 400M 400M
1.6 PMTCT Percentage of HIV positive pregnant women who received ART to reduce the risk of MTCT.
10% 80% 80% 82% 82% 85%
1.7 Treatment of STI
Number of cases of STI treated
39,267 180,000 180,000 180,000 180,000 180,000
Part Four:Five-yearProgrammaticTargetsandResultsMatrix

2010/11-2014/15
37
Ser. No Programs Indicators
Targets by yearBaseline(2009) 2010/11 2011/12 2012/13 2013/14 2014/15
1.8 IGA: Vulnerable women and FSWs
Number of vulnerable women and FSWs supported to engage in IGA
34,661 48,789 56,920 55,000 50,630 37,000
1.9 Post-exposure prophylaxis
Number of health facilities with PEP available
NA 1,355 1,842 2,329 2,816 3,303
1.10 Blood safety & universal precaution
Percentage of donated blood units screened for HIV in Quality assured manner
100% 100% 100% 100% 100% 100%
2. Treatment2.1 Antiretroviral
therapy and monitoring
Number of adults and children with advanced HIV infection receiving antiretroviral therapy
241,250 397,539 429,384 453,134 471,189 484,966
Number of health facilities that offer ART
481 1355 1842 2329 2816 3303
2.2 Prophylaxis for opportunistic infections
Percentage of pre-ART patients eligible for and taking cotrimoxazole prophylaxis
68% 75% 80% 85% 90% 95%
3. Impact Mitigation: Care & Support3.1 Support for
OVCPercentage of orphan and vulnerable children aged 0-17 years whose households received free basic external support in caring for the child
30% 35% 40% 43% 45% 50%
3.2 Care and support for PLHIV
Number of People living with HIV who receive support( financial or IGA)
60,000 70,000 80,000 85,000 95,000 100,000

38
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
4.2
Resu
lts M
atri
x
Them
atic
Are
a O
ne: CreatingEnablingEnvironment
GeneralObjective:T
o cr
eate
an
enab
ling
envi
ronm
ent f
or sc
aled
up
and
com
preh
ensiv
e H
IV/A
IDS
mul
tisec
tora
l res
pons
e
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsSo
urce
of V
erifi
catio
nLe
ad A
genc
y
CapacityBuilding:
Spec
ific
Obj
ectiv
e 1:
To
ens
ure
the
heal
th se
ctor
cap
acity
to a
chie
ve M
DG 6
by
2015
Spec
ific
Obj
ectiv
e 2:
To
bui
ld th
e ca
paci
ty o
f key
and
stra
tegi
c se
ctor
s, ci
vil s
ocie
ty o
rgan
izat
ions
(CSO
s) a
nd p
rivat
e se
ctor
s to
cont
ribut
e to
the
achi
evem
ent o
f MDG
6 b
y 20
15St
reng
then
the
Hea
lth S
ecto
r Ca
paci
ty
Supp
ort t
he e
xpan
sion/
cons
truc
tion
of h
ealth
cen
tres
384
heal
th c
entr
es
cons
truc
ted
Num
ber o
f hea
lth
cent
res c
onst
ruct
ed
Repo
rts,
supp
ortiv
e su
perv
ision
s M
oE/ M
oHM
oH
Regi
onal
HB
& M
oHSu
ppor
t equ
ippi
ng o
f hea
lth
cent
res
384
heal
th c
entr
es
equi
pped
N
umbe
r of h
ealth
ce
ntre
s equ
ippe
d Su
ppor
t uni
vers
ities
and
co
llege
s to
prov
ide
pre-
serv
ice
trai
ning
for h
ealth
scie
nce
stud
ents
40 u
nive
rsiti
es a
nd
colle
ges w
ill p
rovi
de
pre-
serv
ice
trai
ning
fo
r hea
lth sc
ienc
e st
uden
ts
Num
ber o
f hig
her
lear
ning
inst
itutio
ns
prov
ided
pre
-ser
vice
tr
aini
ng fo
r hea
lth
scie
nce
stud
ents
Trai
n he
alth
wor
kers
on
HIV
/AI
DS
23,1
21 h
ealth
wor
kers
w
ill b
e tr
aine
dN
umbe
r of H
ealth
w
orke
rs tr
aine
dD
evel
op st
anda
rd fo
r Hea
lth
faci
lity
prep
ared
ness
for P
eopl
e w
ith d
isabi
lity
Pack
age
will
be
deve
lope
dD
evel
oped
pac
kage
Doc
umen
t of
deve
lope
d pa
ckag
esM
OH
Prep
are
heal
th fa
cilit
ies t
o pr
ovid
e us
er fr
iend
ly se
rvic
es in
H
ealth
faci
litie
s for
Peo
ple
with
di
sabi
lity
and
the
elde
rly
All H
ealth
faci
litie
s will
pr
ovid
e us
er fr
iend
ly
serv
ices
to p
eopl
e w
ith d
isabi
lity
Num
ber o
f Hea
lth
faci
litie
s pro
vidi
ng u
ser
frien
dly
serv
ices
to
peop
le w
ith d
isabi
lity
Repo
rts,
surv
eys
supp
ortiv
e su
perv
ision
s
MO
H
Stre
ngth
en
inst
itutio
nal
capa
city
of k
ey
sect
ors,
CSO
s and
pr
ivat
e se
ctor
s
Staff
key
sect
ors w
ith e
xper
ts o
n pr
even
tion
& im
pact
miti
gatio
n17
key
fede
ral s
ecto
rs
will
ass
ign
expe
rts
Num
ber o
f key
sect
ors
that
ass
igne
d ex
pert
sRe
port
s and
su
ppor
tive
supe
rvisi
ons
Key
Sect
ors
cont
inue
d...

2010/11-2014/15
39
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsSo
urce
of V
erifi
catio
nLe
ad A
genc
ySt
reng
then
in
stitu
tiona
l ca
paci
ty o
f key
se
ctor
s, CS
Os a
nd
priv
ate
sect
ors
Supp
ort f
eder
al se
ctor
s to
build
th
e ca
paci
ty o
f reg
iona
l sec
tors
on
HIV
(gui
delin
es, t
rain
ings
, lo
gist
ics)
17
key
Fede
ral s
ecto
rs
will
supp
ort t
heir
resp
ectiv
e bu
reau
s in
all
regi
on a
nd c
ity
adm
inist
ratio
ns
Num
ber o
f Fed
eral
se
ctor
s sup
port
ing
thei
r re
spec
tive
bure
aus i
n al
l reg
ions
and
2 c
ity
adm
inist
ratio
ns
Repo
rts a
nd
supp
ortiv
e su
perv
ision
s
Key
Sect
ors
Build
the
capa
city
of n
etw
orks
of
ass
ocia
tions
of P
LHIV
, OVC
, th
e el
derly
peo
ple,
peo
ple
with
di
sabi
lity,
CSO
s FBO
s
All
netw
orks
of
asso
ciat
ions
will
be
stre
ngth
ened
Num
ber o
f net
wor
ks
of a
ssoc
iatio
ns
stre
ngth
ened
Repo
rts a
nd
supp
ortiv
e su
perv
ision
s
Net
wor
k of
ne
twor
ks o
f as
soci
atio
ns,
netw
orks
of
asso
ciat
ions
, FH
APCO
Prov
ide
supp
ort t
o 50
0 as
soci
atio
ns o
f PLH
IV,O
VC, t
he
elde
rly, p
eopl
e w
ith d
isabi
lity,
CS
Os,
FBO
s
500
asso
ciat
ions
will
be
supp
orte
d N
umbe
r of a
ssoc
iatio
ns
supp
orte
dRe
port
s, su
ppor
tive
supe
rvisi
ons
Net
wor
k of
ne
twor
ks o
f as
soci
atio
ns,
netw
orks
of
asso
ciat
ions
, FH
APCO
Communitymobilizationandempowerment:
Spec
ific
Obj
ectiv
e 3:
To
sust
ain
com
mun
ity m
ovem
ent a
nd to
atta
in so
cial
cha
nge
by 2
014/
15En
sure
com
mun
ity
owne
rshi
p an
d le
ader
ship
of H
IV/
AID
S
Trai
n co
mm
unity
lead
ers (
4 pe
r ke
bele
/yea
r)35
0,00
0 Co
mm
unity
le
ader
s will
be
trai
ned
Num
ber o
f com
mun
ity
lead
ers t
rain
edSu
rvey
s, Re
port
s, su
ppor
tive
supe
rvisi
onRH
B/RH
APCO
Cond
uct c
omm
unity
co
nver
satio
n10
0% a
dult
popu
latio
n w
ill p
artic
ipat
e in
CC
% o
f adu
lt po
pula
tion
part
icip
ated
in C
CD
evel
op c
oncr
ete
plan
of a
ctio
n17
,500
Keb
eles
(s
mal
lest
adm
inist
rativ
e un
its o
f the
cou
ntry
) w
ill h
ave
conc
rete
pla
n
Num
ber o
f keb
eles
with
co
ncre
te p
lan
follo
win
g CC
Enfo
rce
rele
vant
com
mun
ity
byla
ws
17,5
00 K
ebel
es w
ill
enfo
rce
byla
ws
Num
ber o
f keb
eles
en
forc
ed b
ylaw
sAu
gmen
t co
mm
unity
m
obili
zatio
n w
ith
BCC
inte
rven
tion
Trai
n H
EW o
n BC
C34
,000
HEW
will
be
trai
ned
Num
ber o
f HEW
s tr
aine
d on
BCC
cont
inue
d...

40
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsSo
urce
of V
erifi
catio
nLe
ad A
genc
yAu
gmen
t co
mm
unity
m
obili
zatio
n w
ith
BCC
inte
rven
tion
Trai
n co
mm
unity
ant
i-AID
S pr
omot
ers f
rom
mod
el
hous
ehol
ds
770,
000
anti-
AID
S pr
omot
ers w
ill b
e tr
aine
d fro
m m
odel
ho
useh
olds
Num
ber o
f com
mun
ity
anti-
AID
S pr
omot
ers
trai
ned
Repo
rts,
supp
ortiv
e su
perv
ision
, sur
veys
RHB/
RHAP
CO
Trai
n H
ealth
dev
elop
men
t ar
mie
s (D
A) o
n BC
C34
,000
Hea
lth
deve
lopm
ent a
rmie
s w
ill b
e tr
aine
d on
BCC
Num
ber o
f Hea
lth
deve
lopm
ent a
rmie
s tr
aine
d on
BCC
Repo
rts
Stre
ngth
en
inst
itutio
nal
supp
ort t
o co
mm
unity
ant
i-AI
DS
mov
emen
t
Stre
ngth
en K
ebel
es to
pro
vide
su
ppor
t to
com
mun
ity a
nti-
AID
S m
ovem
ent
100%
of K
ebel
es
will
stre
ngth
ened
to
prov
ide
supp
ort t
o co
mm
unity
ant
i-AID
S m
ovem
ent
Perc
enta
ge o
f Keb
eles
st
reng
then
ed to
pr
ovid
e in
stitu
tiona
l su
ppor
t
Repo
rts,
supp
ortiv
e su
perv
ision
, sur
veys
RHB/
HAP
CO
Doc
umen
t, sh
are
and
scal
e up
be
st p
ract
ices
Best
pra
ctic
es w
ill b
e do
cum
ente
d, sh
ared
, &
scal
ed u
p
List
of b
est p
ract
ices
do
cum
ente
d, sh
ared
, &
scal
ed u
p
Repo
rts,
supp
ortiv
e su
perv
ision
, sur
veys
LeadershipandGovernance:
Spec
ific
Obj
ectiv
e 4:
To
ensu
re, r
espo
nsiv
enes
s and
acc
ount
abili
ty o
f the
lead
ersh
ip a
t all
leve
ls in
the
HIV
/AID
S m
ultis
pect
ral r
espo
nse
Build
cap
acity
of
lead
ersh
ip a
nd
gove
rnin
g bo
dies
at
var
ious
leve
ls
Prov
ide
trai
ning
on
stra
tegi
c le
ader
ship
in th
e fig
ht a
gain
st
HIV
/AID
S to
lead
ersh
ip a
nd
gove
rnin
g bo
dies
10,0
00 le
ader
s fro
m
the
gove
rnin
g bo
dies
of
all
regi
ons w
ill b
e tr
aine
d
Num
ber o
f lea
ders
tr
aine
dRe
port
sH
APCO
s
Sele
ct a
nd d
ocum
ent b
est
prac
tices
of r
egio
ns55
bes
t pra
ctic
e do
cum
enta
tions
will
be
pre
pare
d (5
by
each
Reg
ion
)
Num
ber o
f be
st p
ract
ices
do
cum
enta
tions
pr
epar
ed (
by e
ach
regi
on)
Doc
umen
tatio
ns,
Repo
rts
Arra
nge
expe
rienc
e sh
arin
g vi
sits f
or le
ader
ship
and
go
vern
ing
bodi
es fr
om re
gion
s
All L
eade
rshi
p an
d go
vern
ing
bodi
es
in th
e 11
regi
ons
will
par
ticip
ate
in
expe
rienc
e sh
arin
g vi
sits
Num
ber o
f gov
erni
ng
bodi
es fr
om e
ach
regi
on p
artic
ipat
ed
in e
xper
ienc
e sh
arin
g vi
sits
Repo
rts
cont
inue
d...

2010/11-2014/15
41
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsSo
urce
of V
erifi
catio
nLe
ad A
genc
yAv
ail r
egul
ar
upda
te o
n H
IV/
AID
S ep
idem
ic
situa
tion
and
resp
onse
to
lead
ersh
ip a
nd
gove
rnan
ce
Publ
ish a
nd d
issem
inat
e an
nual
per
form
ance
repo
rt
and
anal
ytic
al re
port
on
the
epid
emic
and
resp
onse
1 an
nual
per
form
ance
re
port
and
1
anal
ytic
al re
port
w
ill b
e pr
oduc
ed a
nd
diss
emin
ated
yea
rly
Num
ber o
f pe
rform
ance
and
an
alyt
ical
repo
rt
publ
ished
&
diss
emin
ated
Repo
rts
HAP
CO/ M
OH
Esta
blish
AID
S re
sour
ce C
entr
es
in th
e fe
dera
l and
regi
onal
pa
rliam
ents
12 A
IDS
Info
rmat
ion
cent
res w
ill b
e es
tabl
ished
Num
ber o
f AID
S re
sour
ce c
entr
es
esta
blish
ed
Repo
rts,
site
visit
sPa
rliam
ent
and
coun
cils
Ensu
re in
clus
ion
of H
IV p
lans
in
the
over
all s
ecto
r pl
an a
nd o
vers
ight
se
ctor
per
form
ance
Ove
rsig
ht th
e in
clus
ion
of H
IV/
AID
S pl
an in
the
over
all s
ecto
rs’
plan
All s
ecto
rs a
t eac
h le
vel w
ill in
clud
e pl
an
in th
e se
ctor
s pla
n
Num
ber o
f Sec
tors
de
velo
ped
plan
s on
HIV
/A
IDS
Repo
rts,
site
visit
sPa
rliam
ent
and
coun
cils
Cond
uct p
erio
dic
revi
ew b
y th
e pa
rliam
ent a
nd o
ther
gov
erni
ng
bodi
es
Bian
nual
revi
ews w
ill
be c
ondu
cted
by
gove
rnin
g bo
dies
at
each
leve
l
Num
ber o
f rev
iew
se
ssio
ns c
ondu
cted
by
gove
rnin
g bo
dies
Repo
rts,
site
visit
sPa
rliam
ent,
NAC
, RAC
s, W
ACs
Cond
uct r
egul
ar H
IV/A
IDS
boar
d m
eetin
gs a
t eac
h le
vel
Regu
lar b
oard
m
eetin
gs w
ill b
e co
nduc
ted
at e
ach
leve
l as p
er th
e gu
idel
ines
Num
ber o
f Reg
ular
bo
ard
mee
tings
co
nduc
ted
at e
ach
leve
l
Min
utes
, Rep
orts
,H
APCO
s
Mainstreaming:
Spec
ific
Obj
ectiv
e 5:
To
enha
nce
the
HIV
/AID
S re
spon
se a
cros
s sec
tors
Stre
ngth
en
owne
rshi
p of
HIV
/AI
DS
prog
ram
s ac
ross
the
sect
ors
Cond
uct a
sses
smen
t on
vuln
erab
ility
and
impa
ct o
f HIV
/AI
DS
and
exist
ing
resp
onse
ca
paci
ty
All s
ecto
rs w
ill
cond
uct a
sses
smen
t on
vul
nera
bilit
y &
impa
ct o
f HIV
and
th
e ex
istin
g re
spon
se
capa
city
Num
ber o
f sec
tors
co
nduc
ted
impa
ct
asse
ssm
ent /
Num
ber
of se
ctor
s doc
umen
ted
impa
ct a
sses
smen
t fin
ding
s.
Repo
rts,
site
visit
All S
ecto
rs
Dev
elop
sect
or sp
ecifi
c po
licie
s, st
rate
gies
and
pla
ns o
n H
IV/
AID
S
All s
ecto
rs w
ill d
evel
op
sect
or sp
ecifi
c po
licy,
pl
an &
stra
tegy
on
HIV
/AID
S
Num
ber o
f key
sect
ors
with
sect
or sp
ecifi
c po
licy,
pla
n an
d st
rate
gy o
n H
IV/A
IDS
Polic
ies,
plan
do
cum
ents
All s
ecto
rs
cont
inue
d...

42
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsSo
urce
of V
erifi
catio
nLe
ad A
genc
ySt
reng
then
ow
ners
hip
of H
IV/
AID
S pr
ogra
ms
acro
ss th
e se
ctor
s
Esta
blish
a u
nit f
or H
IV/A
IDS
mai
nstr
eam
ing
in p
ublic
& n
on-
publ
ic se
ctor
s
80%
Pub
lic a
nd 6
0%
non-
publ
ic se
ctor
s w
ill e
stab
lish
unit
or
assig
n fo
cal p
erso
n to
m
ains
trea
m H
IV
Num
ber o
f pub
lic &
no
n-pu
blic
sect
ors w
ith
units
or a
ssig
ned
foca
l pe
rson
to m
ains
trea
m
HIV
/AID
S
Repo
rts,
site
visit
sAl
l sec
tors
Ensu
re a
lloca
tion
of re
sour
ces
by a
ll se
ctor
s for
HIV
/AID
S m
ains
trea
min
g
100%
of s
ecto
rs
will
use
thei
r ow
n re
sour
ces
Perc
enta
ge o
f sec
tors
al
loca
ted
budg
et fo
r H
IV m
ains
trea
min
g
Repo
rts
Ensu
re th
e in
clus
ion
of H
IV M
an
d E
into
sect
ors’
man
agem
ent
info
rmat
ion
syst
em
Inco
rpor
ate
M a
nd E
of H
IV/
AID
S in
to se
ctor
s’ m
anag
emen
t in
form
atio
n sy
stem
17 k
ey se
ctor
s will
in
corp
orat
e H
IV/
AID
S M
and
E in
to
sect
ors’
MIS
& re
view
m
echa
nism
Num
ber o
f key
sect
ors
inco
rpor
ated
HIV
/AI
DS
M a
nd E
into
se
ctor
al M
IS a
nd re
view
m
echa
nism
Repo
rts,
site
visit
sKe
y se
ctor
s
CoordinationandPartnership:
Spec
ific
Obj
ectiv
e 6:
To
ensu
re sy
nerg
y of
mul
tisec
tora
l HIV
/AID
S re
spon
se a
t all
leve
lsBu
ild H
IV/
AID
S re
spon
se
coor
dina
tion
capa
city
of H
APCO
s an
d H
Bs a
t all
leve
ls
Prov
ide
trai
ning
on
HIV
/AI
DS
Mul
tisec
tora
l res
pons
e co
ordi
natio
n an
d pa
rtne
rshi
p
2,00
0 re
gion
al
heal
th a
nd H
IV st
aff
will
be
trai
ned
on
coor
dina
tion
and
part
ners
hip
Num
ber o
f sta
ff tr
aine
d on
Mul
tisec
tora
l re
spon
se c
oord
inat
ion
and
part
ners
hip
Repo
rtRH
APCO
s
Dev
elop
join
t ann
ual p
lan
guid
ed b
y SP
M II
Al
l reg
ions
and
w
ered
as w
ill p
rodu
ce
harm
oniz
ed a
nd
sync
hron
ized
pla
ns
Exist
ence
of
harm
oniz
ed a
nd
sync
hron
ized
ann
ual
plan
s at e
ach
leve
l
Repo
rts,
on si
te v
isits
HAP
COs
Inst
itute
one
nat
iona
l M
ultis
ecto
ral M
and
E sy
stem
O
ne n
atio
nal m
ulti-
sect
oral
M a
nd
E sy
stem
will
be
adop
ted
by a
ll ac
tors
in
the
natio
n
% o
f mul
ti-se
ctor
al
acto
rs u
tiliz
ing
one
natio
nal m
ulti-
sect
oral
M
and
E sy
stem
Repo
rts,
site
visit
s
Stre
ngth
en
part
ners
hip
at a
ll le
vels
Dev
elop
par
tner
ship
gui
delin
esPa
rtne
rshi
p gu
idel
ine
will
be
deve
lope
d E
xist
ence
of
part
ners
hip
guid
elin
e D
ocum
ent
HAP
CO
cont
inue
d...

2010/11-2014/15
43
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsSo
urce
of V
erifi
catio
nLe
ad A
genc
ySt
reng
then
pa
rtne
rshi
p at
all
leve
ls
Esta
blish
/str
engt
hen
part
ners
hip
foru
ms a
t nat
iona
l, re
gion
al a
nd w
ored
a le
vels
11 re
gion
al
part
ners
hip
foru
ms
will
be
esta
blish
ed
or st
reng
then
ed; 7
50
wor
eda
part
ners
hip
foru
ms e
stab
lishe
d.
Num
ber o
f par
tner
ship
fo
rum
s est
ablis
hed
or st
reng
then
ed a
t re
gion
s and
wor
edas
Repo
rts,
Site
visi
ts
HAP
CO
Regu
lar p
artn
ersh
ip
mee
tings
will
be
cond
ucte
d
Num
ber o
f reg
ular
pa
rtne
rshi
p m
eetin
gs
cond
ucte
d
Repo
rts,
min
utes
, pr
ocee
ding
s
Stre
ngth
en p
artn
ersh
ip fo
r cro
ss
boar
der i
nter
vent
ions
. Bi
annu
al c
ross
boa
rder
pa
rtne
rshi
p m
eetin
gs
will
be
cond
ucte
d w
ith e
ach
of th
ree
coun
trie
s
Num
ber o
f cro
ss
boar
der p
artn
ersh
ip
mee
tings
con
duct
ed
Repo
rt, S
ite v
isit
HAP
CO
Stre
ngth
en
netw
orki
ng a
mon
g se
rvic
e pr
ovid
ers
Map
HIV
/AID
S se
rvic
es,
prov
ider
s and
stak
ehol
ders
at a
ll le
vels
Dire
ctor
y of
HIV
/AID
S se
rvic
es p
rovi
ders
, &
stak
ehol
ders
will
be
deve
lope
d
Prod
uced
dire
ctor
y on
HIV
/AID
S se
rvic
e pr
ovid
ers &
st
akeh
olde
rs
Doc
umen
tH
APCO
s
Esta
blish
/str
engt
hen
linka
ges
and
netw
orki
ng o
f HIV
/AID
S se
rvic
es
Impr
oved
Net
wor
k am
ong
all m
appe
d se
rvic
e pr
ovid
ers w
ill
impr
ove
Num
ber o
f ser
vice
pr
ovid
ers n
etw
orke
dSi
te v
erifi
catio
n,
repo
rt, s
urve
y

44
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Them
atic
Are
a Tw
o:IntensifyingHIVPrevention
Generalobjective:
To
redu
ce th
e ra
te o
f nat
iona
l HIV
new
infe
ctio
ns in
cide
nce
by 5
0% (f
rom
0.2
8% in
200
9) b
y 20
14/1
5. Specificobjectives:
•To
incr
ease
HIV
com
preh
ensi
ve k
now
ledg
e am
ong
adul
t pop
ulat
ion
aged
15-
49 fr
om 2
2.6%
in 2
005
to 8
0% b
y 20
14/1
5.•
To re
duce
per
cent
age
of y
oung
peo
ple
aged
15-
19 y
ears
who
sta
rt s
exua
l deb
ut a
t age
of 1
5 ye
ars
from
8.4
% in
200
5 to
1.7
% (F
emal
e fr
om
11.1
% to
2.2
% a
nd m
ale
from
1.7
% to
0.3
4%) b
y 20
14/1
5.•
To in
crea
se p
erce
ntag
e of
you
ng p
eopl
e ag
ed 1
5-24
who
use
con
dom
con
sist
ently
whi
le h
avin
g se
x fr
om 5
9% in
200
5 to
80%
by
2014
/15.
•To
incr
ease
per
cent
age
of fe
mal
e se
x w
orke
rs r
epor
ting
cons
iste
nt u
se o
f con
dom
from
93.
4% in
200
5 to
98%
in 2
014/
15
BehaviouralapproachesforHIVPreventionapproaches
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
ySt
reng
then
co
mm
unity
ba
sed
prev
entio
n in
terv
entio
n to
add
ress
the
gene
ral p
opul
atio
n
Ensu
re S
cale
up
of c
omm
unity
co
nver
satio
n an
d in
tegr
ate
with
ex
istin
g co
mm
unity
stru
ctur
e
All k
ebel
es w
ill
cond
uct C
C on
HIV
in
tegr
atin
g w
ith
exist
ing
com
mun
ity
stru
ctur
es
Num
ber o
f keb
eles
in
tegr
ated
and
co
nduc
ted
com
mun
ity
conv
ersa
tion
on H
IV/
AID
S
Repo
rts,
Site
visi
tsM
OH
/RH
Bs/
HAP
COs
Revi
ew e
xist
ing
CC g
uide
line
and
trai
ning
man
uals
CC g
uide
line
and
trai
ning
man
uals
will
be
revi
ewed
Revi
ewed
CC
guid
elin
e an
d tr
aini
ng m
anua
ls pr
oduc
ed
Doc
umen
ts p
repa
red
MO
H/H
APCO
Cond
uct t
rain
ing
for v
olun
tary
co
mm
unity
ant
i-AID
S pr
omot
ers (
VCAP
) or m
odel
fa
mili
es
100%
of m
odel
ho
useh
olds
rece
ived
VC
AP tr
aini
ng
Perc
enta
ge o
f VCA
P/m
odel
fam
ilies
trai
ned
Repo
rt, s
urve
yM
OH
, HAP
CO
Dev
elop
HIV
pre
vent
ion
mes
sage
s5
mes
sage
s on
HIV
pr
even
tion
will
be
deve
lope
d an
d di
ssem
inat
ed to
all
leve
ls
Num
ber o
f mes
sage
s de
velo
ped
and
diss
emin
ated
Repo
rt, d
ocum
ent
HAP
COs/
RH
Bs
Diss
emin
ate
HIV
BCC
mes
sage
s on
prin
t, an
d el
ectr
onic
med
ia
1,25
0,00
0 pr
int
mat
eria
ls w
ill b
e di
ssem
inat
ed
Num
ber o
f prin
t BCC
m
ater
ials
diss
emin
ated
Stre
ngth
en H
IV
prev
entio
n ac
ross
se
ctor
s
Dev
elop
org
anisa
tiona
l co
nver
satio
n gu
idel
ine
and
trai
ning
man
ual
Org
anisa
tiona
l co
nver
satio
n gu
idel
ine
and
trai
ning
man
ual
will
be
deve
lope
d
Dev
elop
ed
orga
nisa
tiona
l co
nver
satio
n gu
idel
ine
and
trai
ning
man
ual
Doc
umen
ts
HAP
COs/
Sect
ors
HAP
CO
cont
inue
d...

2010/11-2014/15
45
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
ySt
reng
then
HIV
pr
even
tion
acro
ss
sect
ors
Cond
uct T
OT
on O
rgan
isatio
nal
conv
ersa
tion
for f
acili
tato
rs
sele
cted
from
sect
ors
200
trai
ners
will
re
ceiv
e TO
T on
or
gani
satio
nal
conv
ersa
tion
Num
ber o
f tra
iner
s th
at to
ok T
OT
on
orga
nisa
tiona
l co
nver
satio
n
Doc
umen
tsH
APCO
s/Se
ctor
sH
APCO
Cond
uct o
rgan
isatio
nal
Conv
ersa
tion
in w
ork
plac
esAl
l sec
tors
w
ill C
ondu
ct
orga
nisa
tiona
l Co
nver
satio
n
Num
ber o
f sec
tors
th
at C
ondu
cted
or
gani
satio
nal
Conv
ersa
tion
Prov
ide
trai
ning
to p
rogr
am
man
ager
s of s
ecto
rs o
n H
IV
prev
entio
n pr
ogra
ms
8,00
0 pr
ogra
m
man
ager
s will
be
trai
ned
on H
IV
prev
entio
n
Num
ber o
f pro
gram
s m
anag
ers o
f sec
tors
’ tr
aine
d on
HIV
pr
even
tion
Repo
rts
Sect
ors/
HAP
COs
Cond
uct c
ondo
m p
rom
otio
n an
d di
strib
utio
n in
all
sect
ors
All s
ecto
rs w
ill
cond
uct c
ondo
m
prom
otio
n an
d di
strib
utio
n
Num
ber o
f sec
tors
th
at c
ondu
ct c
ondo
m
prom
otio
n an
d di
strib
utio
n
Repo
rts,
surv
eys,
site
visit
s
Stre
ngth
en
scho
ol b
ased
HIV
in
terv
entio
ns
Prov
ide
trai
ning
on
peer
ed
ucat
ion
500,
000
peer
ed
ucat
ors w
ill b
e tr
aine
d fro
m sc
hool
s, TV
ET, a
nd h
ighe
r ed
ucat
ion
inst
itute
s
Num
ber o
f pee
r ed
ucat
ors t
rain
edD
ocum
ents
/rep
ort
MO
E/RE
B/
Hig
her
educ
atio
n In
stitu
tes /
HAP
COCo
nduc
t pee
r edu
catio
n pr
ogra
ms i
n sc
hool
s, TV
ET a
nd
high
er e
duca
tion
inst
itute
s
Peer
edu
catio
n se
ssio
ns w
ill b
e co
nduc
ted
in 2
6,40
9 pr
imar
y co
mpl
ete
and
seco
ndar
y sc
hool
s in
, 458
TVE
T an
d 72
hi
gher
edu
catio
n in
stitu
tes a
s per
gu
idel
ine
Num
ber o
f sch
ools/
TVET
/hig
her e
duca
tion
inst
itute
s tha
t co
nduc
ted
Wee
kly
peer
ed
ucat
ion
sess
ions
Repo
rt, s
urve
yM
OE/
REB/
H
ighe
r ed
ucat
ion
Inst
itute
s /H
APCO
10 m
illio
n pu
pils
reac
hed
Num
ber o
f pup
ils
reac
hed
Repo
rt, s
urve
yM
OE/
REB/
H
ighe
r ed
ucat
ion
Inst
itute
s /H
APCO
cont
inue
d...

46
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
ySt
reng
then
sc
hool
bas
ed H
IV
inte
rven
tions
Cond
uct l
ife-s
kill
educ
atio
n in
scho
ols,
high
er e
duca
tion
inst
itute
s and
TVE
T
13 M
illio
n st
uden
ts
will
rece
ive
life
skill
ed
ucat
ion
Num
ber o
f stu
dent
s re
ache
d by
life
-ski
lls
base
d H
IV e
duca
tion
in
scho
ols.
Repo
rts
HAP
CO/M
OE/
REB
Cond
uct C
omm
unity
Co
nver
satio
n in
hig
h sc
hool
s, hi
gher
edu
catio
n in
stitu
tes a
nd
TVET
Revi
ew sc
hool
CC
guid
elin
e an
d tr
aini
ng
man
ual
Revi
ewed
scho
ol C
C gu
idel
ine
and
trai
ning
m
anua
l
Doc
umen
tsM
OE/
REB/
H
ighe
r ed
ucat
ion
Inst
itute
s /H
APCO
1,19
7 hi
gh sc
hool
s, 45
8 TV
ET, a
nd 7
2 hi
gher
ed
ucat
ion
inst
itute
s w
ill c
ondu
ct C
C
Num
ber o
f sch
ools
cond
ucte
d CC
Repo
rts,
Site
visi
ts
2.4
mill
ion
pupi
ls w
ill
part
icip
ate
in C
CN
umbe
r of p
upils
pa
rtic
ipat
ed in
CC
Repo
rts
Ensu
re in
corp
orat
ion
of H
IV in
to
scho
ol c
urric
ulum
Scho
ol C
urric
ulum
will
in
corp
orat
e H
IV
Curr
icul
um in
corp
orat
e H
IV
Doc
umen
tM
OE
Trai
n te
ache
rs o
n m
anag
emen
t of
scho
ol H
IV/A
IDS
prog
ram
s 28
,000
teac
hers
w
ill b
e tr
aine
d on
m
anag
emen
t of
scho
ol H
IV p
rogr
ams
Num
ber o
f te
ache
rs tr
aine
d on
m
anag
emen
t of s
choo
l H
IV p
rogr
ams
Repo
rts a
nd si
te v
isits
MO
E/RE
B
2,60
0 hi
gher
ed
ucat
ion
and
TVET
te
ache
rs tr
aine
d on
man
agem
ent o
f sc
hool
HIV
pro
gram
s
Num
ber o
f te
ache
rs tr
aine
d on
m
anag
emen
t of s
choo
l H
IV p
rogr
ams
Repo
rts a
nd si
te v
isits
Dev
elop
and
diss
emin
ate
targ
eted
BCC
mes
sage
for
Uni
vers
ity/c
olle
ges a
nd h
igh
scho
ols
5 ty
pes o
f tar
gete
d BC
C m
essa
ges w
ill
be d
evel
oped
and
di
ssem
inat
ed
Type
s of t
arge
ted
BCC
mes
sage
s dev
elop
ed
and
diss
emin
ated
BCC
mat
eria
l, re
port
s, su
rvey
sM
OE/
REB
2 m
illio
n pu
pils
reac
hed
thro
ugh
scho
ol B
CC c
ampa
igns
Num
ber o
f pup
ils
reac
hed
thro
ugh
scho
ol
BCC
cam
paig
ns
Repo
rts &
site
visi
tsM
OE/
REBs
/H
APCO
s
600,
000
mill
ion
pupi
ls in
hig
her e
duca
tion
inst
itute
s and
TVE
T re
ache
d th
roug
h sc
hool
BCC
cam
paig
ns
Num
ber o
f pup
ils
reac
hed
thro
ugh
scho
ol
BCC
cam
paig
ns
Repo
rts &
site
visi
tsH
ighe
r ed
ucat
ion
Inst
itute
s /M
OE/
REB
cont
inue
d...

2010/11-2014/15
47
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
ySt
reng
then
sc
hool
bas
ed H
IV
inte
rven
tions
Stre
ngth
en y
outh
lead
ersh
ip
deve
lopm
ent p
rogr
ams
Stud
ent c
ounc
ils in
1,
197
high
scho
ols w
ill
be st
reng
then
ed
Num
ber o
f hig
h sc
hool
s w
ith fu
nctio
nal y
outh
le
ader
ship
pro
gram
s
Repo
rts
MO
E/RE
B/H
ighe
r ed
ucat
ion
inst
itute
sSt
reng
then
HIV
rela
ted
scho
ol
club
s1,
197
seco
ndar
y sc
hool
s will
hav
e at
le
ast 4
stre
ngth
ened
cl
ubs e
ach
Num
ber o
f sch
ools
with
at l
east
4 c
lubs
st
reng
then
ed
Repo
rts
Stre
ngth
en a
t lea
st 4
HIV
re
late
d cl
ubs o
f uni
vers
ities
and
co
llege
s
72 h
ighe
r edu
catio
n in
stitu
tes a
nd 4
58
TVET
will
hav
e at
leas
t 4
club
s str
engt
hene
d
Num
ber o
f hig
her
educ
atio
n in
stitu
tes
and
TVET
with
at l
east
4
club
s str
engt
hene
d
Repo
rts
Ensu
re a
ctiv
e pa
rtic
ipat
ion/
Mem
bers
hip
in c
lubs
of s
choo
ls,
high
er e
duca
tion
inst
itute
s and
TV
ET
598,
500
pupi
ls of
sc
hool
s will
par
ticip
ate
in c
lubs
Num
ber o
f pup
ils
of h
igh
scho
ols
part
icip
atin
g in
clu
bs
Repo
rt, s
ite v
isit,
surv
ey
229,
000
stud
ents
will
pa
rtic
ipat
e in
clu
bs
of h
ighe
r edu
catio
n in
stitu
tes
Num
ber o
f pup
ils o
f TV
ET p
artic
ipat
ing
in
club
s
36,0
00 p
upils
will
pa
rtic
ipat
e in
clu
bs
of h
ighe
r edu
catio
n in
stitu
tes
Num
ber o
f pup
ils
of h
ighe
r edu
catio
n in
stitu
tes p
artic
ipat
ing
in c
lubs
Expa
nd A
RC in
scho
ols,
high
er
educ
atio
n in
stitu
tes a
nd T
VET
1,19
7 hi
gh sc
hool
s; 72
hig
her e
duca
tion
inst
itute
s and
458
TV
ETs w
ill h
ave
ARC
Num
ber o
f hig
h sc
hool
s ha
ving
ARC
Repo
rts,
Surv
eys
MO
E/RE
B/H
ighe
r ed
ucat
ion
inst
itute
sN
umbe
r of h
ighe
r ed
ucat
ion
inst
itute
s ha
ving
ARC
Num
ber o
f TVE
T ha
ving
AR
CM
OE/
REB
2.1
Mill
ion
pupi
ls w
ill
utili
ze sc
hool
bas
ed
ARCs
Num
ber o
f pup
ils
utili
zed
scho
ol b
ased
AR
Cs
cont
inue
d...

48
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
ySc
ale
up
com
preh
ensiv
e H
IV p
reve
ntio
n in
terv
entio
ns
addr
essin
g m
ost
at ri
sk p
opul
atio
n (M
ARPs
)
Det
erm
ine
the
iden
tity,
size
, be
havi
oura
l cha
ract
erist
ics a
nd
HIV
pre
vale
nce
amon
g M
ARPs
A na
tiona
l MAR
Ps
surv
ey w
ill b
e co
nduc
ted
Prod
uced
nat
iona
l M
ARPS
surv
ey re
port
Doc
umen
t pro
duce
dEH
NRI
/MO
H/
HAP
CO
Map
MAR
Ps se
rvic
e pr
ovid
ers
Serv
ice
prov
ider
s will
be
map
ped
Serv
ice
dire
ctor
y pr
oduc
edRe
port
s & si
te v
isits
HAP
CO
Dev
elop
pac
kage
of H
IV se
rvic
es
for M
ARPs
Min
imum
pac
kage
of
serv
ices
will
be
deve
lope
d fo
r MAR
Ps
Dev
elop
ed p
acka
ge o
f se
rvic
e Re
port
s & si
te v
isits
HAP
CO
Dev
elop
com
preh
ensiv
e co
mm
unic
atio
n st
rate
gy fo
r M
ARPs
A co
mm
unic
atio
n st
rate
gy w
ill b
e de
velo
ped
Dev
elop
ed
com
mun
icat
ion
stra
tegy
The
stra
tegy
do
cum
ent a
nd re
port
sH
APCO
Build
the
capa
city
of C
SOs t
o pr
ovid
e ou
trea
ch H
IV e
duca
tion
to M
ARPS
200
CSO
s will
be
trai
ned
to p
rovi
de H
IV
educ
atio
n to
MAR
Ps
Num
ber o
f CSO
s tr
aine
d to
pro
vide
HIV
ed
ucat
ion
to M
ARPs
Repo
rts,
Surv
eyH
APCO
Prov
ide
trai
ning
to p
eer
educ
ator
s am
ong
MAR
PS
100,
000
peer
ed
ucat
ors w
ill b
e tr
aine
d am
ong
MAR
Ps
Num
ber o
f mem
ber o
f M
ARPs
trai
ned
as p
eer
educ
ator
s
repo
rt, S
urve
yH
APCO
,CSO
s
Prov
ide
com
preh
ensiv
e H
IV
prev
entio
n se
rvic
es to
MAR
Ps1
mill
ion
MAR
PS w
ill
be re
ache
dN
umbe
r of M
ARPS
re
ache
d w
ith H
IV
prev
entio
n pr
ogra
ms
Repo
rt, S
urve
yH
APCO
,CSO
s
Stre
ngth
en o
ut
of sc
hool
you
th
HIV
pre
vent
ion
prog
ram
s
Esta
blish
200
new
you
th c
entr
es20
0 ne
w A
RCs w
ill b
e es
tabl
ished
N
umbe
r of A
RCs
esta
blish
edRe
port
MoW
CYA/
HAP
COD
evel
op m
inim
um se
rvic
e pa
ckag
e fo
r you
th c
entr
esM
inim
um p
acka
ge o
f H
IV se
rvic
es w
ill b
e de
velo
ped
for y
outh
ce
ntre
s
Doc
umen
t dev
elop
ed
with
min
imum
pac
kage
of
HIV
serv
ices
for
yout
h ce
ntre
s
Repo
rtM
oWCY
A/H
APCO
Stre
ngth
en y
outh
cen
tres
to
pro
vide
use
r frie
ndly
HIV
/AI
DS
serv
ices
at y
outh
cen
tre
acco
rdin
g to
the
pack
age
100%
of y
outh
cen
tres
w
ill p
rovi
de u
ser
frien
dly
HIV
/AID
S se
rvic
es
Perc
enta
ge o
f you
th
cent
res p
rovi
ding
us
er fr
iend
ly H
IV/A
IDS
serv
ices
Repo
rt, s
urve
ysM
oWCY
A/H
APCO
Expa
nd/s
tren
gthe
n ed
ucat
iona
l en
tert
ainm
ent (
edut
ainm
ent)
yout
h ce
ntre
s in
dist
rict t
owns
60%
of y
outh
cen
tres
w
ill b
e st
reng
then
ed
Perc
enta
ge o
f you
th
cent
res s
tren
gthe
ned
Repo
rts
MoW
CYA
Trai
n Pe
er e
duca
tors
on
HIV
175,
000
peer
ed
ucat
ors w
ill b
e tr
aine
d on
HIV
Num
ber o
f pee
r ed
ucat
ors t
rain
ed o
n H
IV
Repo
rts,
surv
ey
cont
inue
d...

2010/11-2014/15
49
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
ySt
reng
then
out
of
scho
ol y
outh
H
IV p
reve
ntio
n pr
ogra
ms
Prov
ide
Peer
edu
catio
n 80
% o
f out
of s
choo
l yo
uth
will
be
reac
hed
Num
ber o
f out
of
scho
ol y
outh
reac
hed
with
HIV
& A
IDS
educ
atio
n
Surv
ey, r
epor
tsM
oWCY
AIm
plem
ent O
utre
ach
Yout
h in
terv
entio
ns
Cond
uct y
outh
dia
logu
e 60
% y
outh
cen
tres
w
ill c
ondu
ct y
outh
di
alog
ue
Num
ber o
f You
th
cent
res c
ondu
ctin
g yo
uth
dial
ogue
Repo
rts,
surv
ey
Inte
nsify
HIV
pr
even
tion
in
deve
lopm
ent
sche
mes
Targ
et b
usin
ess o
ppor
tuni
ty
loca
tions
, ind
ustr
ies a
nd p
rivat
e de
velo
pmen
t sch
emes
150
busin
ess
oppo
rtun
ity lo
catio
ns,
indu
strie
s and
priv
ate
deve
lopm
ent s
chem
es
will
be
targ
eted
Num
ber o
f bus
ines
s op
port
unity
loca
tions
, in
dust
ries a
nd p
rivat
e de
velo
pmen
t sch
emes
be
targ
eted
Repo
rts,
HAP
CO
Inte
grat
e H
IV p
reve
ntio
n in
de
velo
pmen
t sch
emes
’ pro
ject
pr
opos
als
100%
of d
evel
opm
ent
sche
mes
/pro
ject
s w
ill in
tegr
ate
HIV
pr
even
tion
Perc
enta
ge o
f de
velo
pmen
t sch
emes
/pr
ojec
ts in
tegr
ated
HIV
pr
even
tion
Surv
eys,
Repo
rts,
Doc
umen
tsRe
spon
sible
se
ctor
s
Dev
elop
and
diss
emin
ate
targ
eted
HIV
mes
sage
on
5 iss
ues
5 m
essa
ge w
ill b
e de
velo
ped
and
diss
emin
ated
on
HIV
iss
ues
Num
ber o
f mes
sage
de
velo
ped
and
diss
emin
ated
on
HIV
iss
ues
Surv
eys,
Repo
rts,
Doc
umen
tsH
APCO
Con
duct
Pee
r edu
catio
n 10
0 %
of d
evel
opm
ent
sche
me/
proj
ect
will
con
duct
pee
r ed
ucat
ion
Perc
enta
ge o
f de
velo
pmen
t sch
emes
/pr
ojec
ts c
ondu
cted
pe
er e
duca
tion
Repo
rts,
site
supe
rvisi
ons,
surv
eys
Resp
ectiv
e se
ctor
s and
In
vest
men
t Ag
ency
M
ap d
evel
opm
ent s
chem
es fo
r ou
trea
ch se
rvic
esD
evel
opm
ent
sche
mes
will
be
iden
tified
for o
utre
ach
serv
ices
Num
ber o
f de
velo
pmen
t sch
emes
id
entifi
ed fo
r out
reac
h se
rvic
es
Repo
rts,
surv
eys
Cond
uct o
utre
ach
prog
ram
s for
de
velo
pmen
t sch
emes
All d
evel
opm
ent
sche
mes
will
be
netw
orke
d fo
r ou
trea
ch se
rvic
es
Num
ber o
f de
velo
pmen
t sch
emes
re
ceiv
ed o
utre
ach
HIV
/AI
DS
serv
ices
Repo
rts,
surv
eys
Ref
erra
l lin
kage
with
hea
lth
faci
litie
s for
VCT
, man
agem
ent
of S
TI a
nd A
RT fo
r the
HIV
po
sitiv
e
100%
of d
evel
opm
ent
sche
mes
/pro
ject
s will
cr
eate
refe
rral
link
ages
w
ith h
ealth
faci
litie
s fo
r HIV
serv
ices
Perc
enta
ge o
f de
velo
pmen
t sch
emes
cr
eate
d re
ferr
al
linka
ges w
ith h
ealth
fa
cilit
ies
Repo
rt
cont
inue
d...

50
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
yIn
tens
ify H
IV
prev
entio
n in
de
velo
pmen
t sc
hem
es
Ensu
re H
IV P
reve
ntio
n am
ong
com
mun
ities
in a
reas
of
deve
lopm
ent s
chem
es/p
roje
cts
100%
of d
evel
opm
ent
sche
mes
/pro
ject
s will
co
nduc
t pre
vent
ion
inte
rven
tions
am
ong
com
mun
ities
in th
e pr
ojec
t are
as
Perc
enta
ge o
f de
velo
pmen
t sch
emes
/pr
ojec
ts c
ondu
cted
pr
even
tion
amon
g co
mm
uniti
es in
the
proj
ect a
reas
Repo
rt
Resp
ectiv
e se
ctor
s and
In
vest
men
t Ag
ency
Expa
nd H
IV
prev
entio
n am
ong
popu
latio
n gr
oups
w
ith sp
ecia
l nee
ds
(eld
erly
and
peo
ple
with
disa
bilit
y)
Cond
uct r
isk a
nd v
ulne
rabi
lity
asse
ssm
ent
One
ass
essm
ent
addr
essin
g th
e di
ffere
nt fo
rms o
f pe
ople
with
spec
ial
need
s will
be
cond
ucte
d
Asse
ssm
ent c
ondu
cted
Doc
umen
t with
As
sess
men
t res
ult
HAP
CO/
MO
LSA
Dev
elop
pre
vent
ion
stra
tegy
for
peop
le w
ith sp
ecia
l nee
dsPr
even
tion
stra
tegy
w
ill b
e de
velo
ped
Stra
tegi
c do
cum
ent
deve
lope
dD
ocum
ent
Cust
omiz
e H
IV in
terv
entio
n gu
idel
ines
, im
plem
enta
tion
man
uals,
and
BCC
inte
rven
tions
BCC
guid
elin
e an
d im
plem
enta
tion
man
ual w
ill b
e pr
oduc
ed
Prod
uced
BCC
gu
idel
ine
and
impl
emen
tatio
n m
anua
l doc
umen
ts
Doc
umen
ts
Inte
grat
e BC
C in
terv
entio
ns in
AR
C of
you
th c
entr
es fo
r peo
ple
with
disa
bilit
y
All y
outh
cen
tres
of
ARC
will
inte
grat
e BC
C in
terv
entio
ns fo
r pe
ople
with
disa
bilit
y
Num
ber o
f you
th
cent
res w
ith A
RC
that
inte
grat
ed B
CC
inte
rven
tion
for p
eopl
e w
ith d
isabi
lity
Repo
rts,
site
visit
s, su
rvey
s
Dev
elop
and
diss
emin
ate
BCC
mat
eria
ls fo
r peo
ple
with
spec
ial
need
s
5 ty
pes o
f mes
sage
s on
HIV
will
be
deve
lope
d to
peo
ple
with
spec
ial n
eeds
Type
of m
essa
ges
deve
lope
d D
ocum
ents
80,0
00 c
opie
s BCC
pr
int m
ater
ials
will
be
dev
elop
ed a
nd
diss
emin
ated
for
peop
le w
ith d
isabi
lity
Num
ber o
f BCC
prin
t m
ater
ials
deve
lope
d an
d di
ssem
inat
ed fo
r pe
ople
with
disa
bilit
y
Doc
umen
ts
cont
inue
d...

2010/11-2014/15
51
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
yEx
pand
HIV
pr
even
tion
amon
g po
pula
tion
grou
ps
with
spec
ial n
eeds
(e
lder
ly a
nd p
eopl
e w
ith d
isabi
lity)
Dev
elop
and
diss
emin
ate
BCC
mat
eria
ls fo
r peo
ple
with
spec
ial
need
s
120,
000
BCC
prin
t m
ater
ials
will
be
diss
emin
ated
for
elde
rly
Num
ber o
f BCC
prin
t m
ater
ials
deve
lope
d an
d di
ssem
inat
ed fo
r el
derly
Doc
umen
tsH
APCO
/ M
OLS
A
Dev
elop
and
diss
emin
ate
BCC
mat
eria
ls fo
r peo
ple
with
spec
ial
need
s
2,50
0 BC
C au
dio/
visu
al m
ater
ials
will
be
diss
emin
ated
for
peop
le w
ith d
isabi
lity
and
elde
rs
Num
ber o
f BCC
aud
io/
visu
al m
ater
ials
deve
lope
d an
d di
ssem
inat
ed fo
r pe
ople
with
disa
bilit
y
Doc
umen
tsH
APCO
/ M
OLS
A
StructuralHIVpreventionapproach
Addr
ess g
ende
r in
equa
lity
Mai
nstr
eam
gen
der i
nto
sect
oral
pol
icie
s Al
l sec
tora
l pol
icie
s w
ill in
tegr
ate
gend
er
issue
s
Num
ber o
f sec
tors
in
tegr
ated
gen
der i
n to
th
eir p
olic
ies
Repo
rts
MoW
CYA
Addr
ess g
ende
r in
equa
lity
Avai
l PEP
to v
ictim
s of r
ape
3,30
3 he
alth
faci
litie
s w
ill p
rovi
de P
EPN
umbe
r hea
lth fa
cilit
ies
prov
idin
g se
rvic
eRe
port
s & su
perv
ision
MO
H
Advo
cate
for p
uniti
ve m
easu
res
on p
erpe
trat
ors o
f GBV
.Si
x ro
und
advo
cacy
ca
mpa
igns
will
be
held
Num
ber o
f cam
paig
ns
by w
omen
gro
ups
Repo
rts
MoW
CYA
Ensu
re in
clus
ion
of g
ende
r di
men
sion
in H
IV p
rogr
ams
All H
IV p
reve
ntio
n pr
ogra
ms w
ill
inte
grat
e ge
nder
co
mpo
nent
Num
ber o
f HIV
pr
even
tion
prog
ram
s w
ith g
ende
r dim
ensio
n
Repo
rts
HAP
CO
Redu
ce e
cono
mic
vu
lner
abili
ty
Prov
ide
trai
ning
on
IGA
to
vuln
erab
le g
roup
s24
8,33
9 vu
lner
able
an
d w
omen
and
FSW
w
ill re
ceiv
e vo
catio
nal
trai
ning
s
Num
ber o
f vul
nera
ble
wom
en a
nd F
SW w
ho
rece
ived
trai
ning
Repo
rts
Regi
ons/
w
omen
as
soci
atio
ns./
Mic
ro &
smal
l en
terp
rise
Prov
ide
seed
mon
ey su
ppor
t to
vuln
erab
le in
divi
dual
s24
8,33
9 W
omen
&
FSW
will
be
supp
orte
d w
ith se
ed m
oney
Num
ber o
f wom
en &
FS
W su
ppor
ted
with
se
ed m
oney
Repo
rts a
nd si
te v
isits
Esta
blish
inte
grat
ion
of H
IV/
AID
S se
rvic
es w
ith sa
fety
-net
pr
ogra
ms
HIV
serv
ices
will
be
inte
grat
ed in
to a
ll re
gion
al sa
fety
-net
pr
ogra
ms
Num
ber o
f saf
ety-
net
prog
ram
s int
egra
ting
HIV
/AID
S se
rvic
es
Repo
rts
RAD
cont
inue
d...

52
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
yAd
dres
s soc
io-
cultu
ral f
acto
rs
fuel
ling
HIV
tr
ansm
issio
n
Prov
ide
sens
itiza
tion
and
educ
atio
n on
avo
idin
g ha
rmfu
l tr
aditi
onal
pra
ctic
es
All k
ebel
es w
here
FG
M is
pra
ctic
ed
shal
l enf
orce
byl
aws
agai
nst F
GM
Num
ber o
f keb
eles
(w
here
FG
M is
pr
actic
ed) e
nfor
ced
byla
ws a
gain
st F
GM
Repo
rts
MO
H/
MoW
CYA
Prot
ect h
uman
rig
hts a
nd p
rovi
de
lega
l sup
port
Cond
uct t
he n
atio
nal s
tigm
a in
dex
stud
y2
natio
nal s
tigm
a in
dex
stud
ies
cond
ucte
d
Num
ber o
f stig
ma
inde
x st
udie
s co
nduc
ted
Repo
rts
NEP
+/ H
APCO
Impl
emen
t GIP
A O
pera
tiona
lize
GIP
A (i.
e . P
LHIV
will
be
invo
lved
in p
olic
y an
d st
rate
gy d
evel
opm
ent,
serv
ice
deliv
ery
and
M
and
E)
Invo
lvem
ent o
f PLH
A in
pol
icy
and
stra
tegy
, se
rvic
e de
liver
y an
d M
an
d E
Surv
eyN
EP+
Enha
nce
impl
emen
tatio
n of
yo
uth
and
wom
en
deve
lopm
ent
pack
ages
hum
an
right
s and
lega
l su
ppor
t
Expa
nd y
outh
and
wom
en
lead
ersh
ip d
evel
opm
ent
prog
ram
s
70,0
00 y
outh
and
w
omen
lead
ers
trai
ned
Num
ber o
f you
th a
nd
wom
en tr
aine
d on
le
ader
ship
Repo
rts
MoW
YSA/
YS
A an
d W
A
Rollo
ut th
e im
plem
enta
tion
of
yout
h an
d w
omen
pac
kage
s to
all d
istric
ts
750
Wor
edas
Num
ber o
f Wor
edas
im
plem
entin
g yo
uth
& w
omen
dev
elop
men
t pa
ckag
es
Repo
rts
BiomedicalHIVpreventionservices
Ensu
re a
cces
s and
en
hanc
e up
take
of
HCT
serv
ices
46.3
5 m
illio
n of
pe
ople
will
rece
ive
HIV
te
stin
g
Num
ber o
f peo
ple
rece
ived
HIV
test
ing
Repo
rts
MO
H /
RHB
Prom
ote
HIV
test
ing
usin
g CC
an
d he
alth
ext
ensio
n w
orke
rs,
mob
ile, o
utre
ach
serv
ice
100%
of C
C gr
oups
w
ill a
ddre
ss H
CT
serv
ice
Perc
enta
ge o
f CC
grou
ps th
at a
ddre
ssed
H
CT se
rvic
e
Repo
rts/
Surv
eys
MO
H /
RHB
Inte
grat
e H
CT P
rom
otio
nal
activ
ities
in th
e pa
ckag
e of
H
ealth
dev
elop
men
t arm
ies
HCT
pro
mot
iona
l ac
tiviti
es w
ill b
e in
tegr
ated
in th
e pa
ckag
e of
Hea
lth
deve
lopm
ent a
rmie
s
Doc
umen
t of
deve
lopm
ent
arm
ies w
ith p
acka
ge
inte
grat
ing
HCT
Repo
rts,
surv
eyM
OH
/HAP
CO/
RHB
Educ
ate
hous
ehol
ds o
n H
CT b
y H
ealth
dev
elop
men
t arm
ies
100%
of h
ouse
hold
s vi
sited
by
Hea
lth
deve
lopm
ent a
rmy
mem
bers
will
rece
ive
HIV
edu
catio
n
Perc
enta
ge th
at
rece
ived
HIV
edu
catio
n ou
t of h
ouse
hold
s vi
sited
by
deve
lopm
ent
arm
y m
embe
rs
Repo
rts,
surv
eyM
OH
/HAP
CO/
RHB
cont
inue
d...

2010/11-2014/15
53
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
yEn
sure
acc
ess a
nd
enha
nce
up ta
ke o
f H
CT se
rvic
es
Prom
ote
HIV
test
ing
thro
ugh
relig
ious
lead
ers,
loca
l co
mm
unity
lead
ers
80%
Rel
igio
us le
ader
s w
ill re
ceiv
e or
ient
atio
n on
HCT
pro
mot
ion
Perc
enta
ge o
f rel
igio
us
lead
ers r
ecei
ved
orie
ntat
ion
on H
CT
prom
otio
n
Repo
rt, s
urve
yH
APCO
/Re
ligio
us
grou
ps
Educ
ate
Publ
ic o
n H
IV
test
ing
thou
gh m
ass m
edia
ca
mpa
igni
ng
Mas
s med
ia c
ampa
ign
on c
ouns
ellin
g an
d te
stin
g w
ill b
e co
nduc
ted
Cam
paig
n co
nduc
ted
Repo
rts
MO
H/R
HB/
H
APCO
s/
Prov
ide
trai
ning
to H
CT se
rvic
e pr
ovid
ers
200
HCT
serv
ice
prov
ider
s will
be
trai
ned
on H
CT fo
r pe
ople
with
disa
bilit
y an
d el
derly
Num
ber o
f HCT
serv
ice
prov
ider
s tra
ined
on
HCT
for p
eopl
e w
ith
disa
bilit
y an
d th
e el
derly
Repo
rt
Prov
ide
HCT
to P
eopl
e w
ith
disa
bilit
y an
d el
derly
50%
of p
eopl
e w
ith
disa
bilit
y an
d el
derly
w
ill re
ceiv
e H
CT
Perc
enta
ge o
f peo
ple
with
disa
bilit
y an
d th
e el
derly
who
rece
ived
H
CT
Repo
rts,
surv
eys
Ensu
re u
nint
erru
pted
supp
lies
of te
st k
its a
nd o
ther
acc
esso
ries
100%
of S
ervi
ce
rend
erin
g fa
cilit
ies w
ill
get a
dequ
ate
test
kits
an
d ot
her i
tem
s all
the
time
Perc
enta
ge o
f Ser
vice
re
nder
ing
faci
litie
s ge
ttin
g ad
equa
te te
st
kits
and
oth
er it
ems a
ll th
e tim
e
Repo
rts a
nd si
te v
isits
MO
H/P
FSA/
RH
B/
Build
cap
aciti
es o
f priv
ate
heal
th
faci
litie
s to
rollo
ut H
CT se
rvic
eCa
paci
ty b
uild
ing
to
400
Priv
ate
Hea
lth
faci
litie
s will
be
cond
ucte
d to
pro
vide
H
CT se
rvic
es
Num
ber o
f priv
ate
Hea
lth fa
cilit
ies w
ith
ensu
red
capa
city
to
prov
ide
HCT
Repo
rts a
nd v
isits
MO
H/ R
HB
Rollo
ut H
CT se
rvic
es in
to p
rivat
e he
alth
faci
litie
s40
0 pr
ivat
e he
alth
fa
cilit
ies w
ill p
rovi
de
HCT
serv
ices
Num
ber o
f priv
ate
heal
th fa
cilit
ies s
igne
d an
MO
U a
nd p
rovi
de
HCT
serv
ices
Repo
rts a
nd v
isits
cont
inue
d...

54
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
yEn
sure
acc
ess a
nd
enha
nce
upta
ke o
f PM
TCT
serv
ices
85%
of H
IV p
ositi
ve
preg
nant
wom
en w
ill
rece
ive
com
plet
e AR
V pr
ophy
laxi
s)
Perc
enta
ge o
f HIV
po
sitiv
e pr
egna
nt
wom
en re
ceiv
ed
antir
etro
vira
l pr
ophy
laxi
s
Repo
rts,
Surv
eys
MO
H/ R
HB
Stre
ngth
en th
e in
tegr
atio
n of
PM
TCT
with
MN
CH in
all
heal
th
faci
litie
s
3,30
3 H
ealth
faci
litie
s w
ill h
ave
effec
tive
inte
grat
ion
of P
MTC
T an
d M
NCH
Num
ber o
f Hea
lth
faci
litie
s with
effe
ctiv
e in
tegr
atio
n of
PM
TCT
and
MN
CH
Repo
rts
MoH
/ RH
B
Mob
ilize
the
com
mun
ity to
be
activ
ely
invo
lved
in P
MTC
T 10
0% o
f Keb
eles
will
co
nduc
t sch
edul
ed
com
mun
ity
mob
iliza
tion
rega
rdin
g PM
TCT
Perc
enta
ge o
f Keb
eles
th
at c
ondu
cted
CC
sess
ions
that
add
ress
ed
PMTC
T iss
ues
Surv
eys
MoH
/ HAP
CO/
RHB
Prom
ote
PIH
CT fo
r all
preg
nant
w
omen
att
endi
ng A
NC
and
deliv
ery
serv
ices
usin
g op
t out
ap
proa
ch
Hea
lth fa
cilit
ies w
ill
Prom
ote
PIH
CT to
all
Preg
nant
wom
en
Num
ber o
f Hea
lth
faci
litie
s Pro
mot
ing
PIH
CT to
all
Preg
nant
w
omen
Surv
eys
MoH
/RH
B
Ensu
re m
ale
invo
lvem
ent i
n PM
TCT
serv
ice
50%
of p
artn
ers o
f HIV
po
sitiv
e PM
TCT
clie
nts
will
be
test
ed fo
r HIV
an
d pr
ovid
e su
ppor
t to
thei
r fam
ily
Perc
enta
ge o
f pre
gnan
t w
omen
who
se p
artn
ers
rece
ived
test
ing
and
prov
ided
supp
ort t
o fa
mily
Surv
eys
MoH
/HAP
CO/
RHB
Trai
n he
alth
ext
ensio
n w
orke
rs
on P
MTC
T an
d de
liver
y se
rvic
e pr
ovisi
on
34,0
00 H
EWs w
ill b
e tr
aine
d on
PM
TCT
and
deliv
ery
serv
ice
prov
ision
Num
ber o
f HEW
trai
ned
& en
gage
d in
PM
TCT
and
deliv
ery
serv
ice
prov
ision
serv
ices
Repo
rts
MoH
/ H
APCO
s/ R
HB
Inte
grat
e PM
TCT
into
the
pack
age
of H
ealth
dev
elop
men
t ar
mie
s
Doc
umen
t of
deve
lopm
ent a
rmie
s in
tegr
atin
g PM
TCT
will
be
pro
duce
d
Doc
umen
t of H
ealth
de
velo
pmen
t ar
mie
s with
pac
kage
in
tegr
atin
g PM
TCT
Repo
rts,
surv
eyM
oH /
HAP
COs/
RH
B
Prom
ote
PMTC
T by
the
heal
th
deve
lopm
ent a
rmie
sPM
TCT
prom
otio
nal
activ
ities
will
be
inte
grat
ed in
the
pack
age
of h
ealth
de
velo
pmen
t arm
ies
Doc
umen
t of
heal
th d
evel
opm
ent
arm
ies w
ith p
acka
ge
inte
grat
ing
PMTC
T
Doc
umen
t, Re
port
s M
oH/ R
HB
cont
inue
d...

2010/11-2014/15
55
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
yEn
sure
acc
ess a
nd
enha
nce
upta
ke o
f PM
TCT
serv
ices
Prov
ide
trai
ning
to
deve
lopm
ent a
rmie
s on
PMTC
T10
0% o
f hea
lth
deve
lopm
ent a
rmie
s tr
aine
d on
PM
TCT
Num
ber o
f hea
lth
deve
lopm
ent a
rmie
s tr
aine
d on
PM
TCT
Repo
rts
MoH
/ RH
B
Prov
ide
educ
atio
n to
ho
useh
olds
on
PMTC
T by
de
velo
pmen
t arm
ies
100%
of h
ouse
hold
s vi
sited
by
heal
th
deve
lopm
ent
arm
ies r
ecei
ved
HIV
ed
ucat
ion
Perc
enta
ge o
f ho
useh
olds
visi
ted
by
deve
lopm
ent a
rmy
mem
bers
rece
ived
HIV
ed
ucat
ion
Repo
rts
MoH
/RH
B
Expa
nd P
MTC
T se
rvic
es3,
303
publ
ic h
ealth
fa
cilit
ies w
ill p
rovi
de
PMTC
T
Num
ber o
f pub
lic
heal
th fa
cilit
ies
prov
idin
g PM
TCT
Repo
rts &
site
visi
tsM
oH /
RHB
Equi
p he
alth
faci
litie
s with
AN
C an
d de
liver
y eq
uipm
ent
3,30
3 H
ealth
faci
litie
s w
ill b
e eq
uipp
ed w
ith
ANC
and
deliv
ery
equi
pmen
t
Num
ber o
f hea
lth
faci
litie
s equ
ippe
d w
ith A
NC
and
deliv
ery
equi
pmen
t
MoH
/ RH
B
Trai
n he
alth
wor
kers
on
basic
an
d em
erge
ncy
obst
etric
car
e an
d PM
TCT
serv
ice
prov
ision
13,2
12 h
ealth
car
e w
orke
rs w
ill b
e tr
aine
d on
bas
ic a
nd
emer
genc
y ob
stet
ric
care
and
PM
TCT
serv
ice
prov
ision
Num
ber o
f hea
lth c
are
wor
kers
trai
ned
to
prov
ide
PMTC
T se
rvic
es
MoH
/ RH
B
Dep
loy
mot
her s
uppo
rt m
ento
rs
in e
ach
PMTC
T sit
e6,
606
mot
her s
uppo
rt
grou
p m
ento
rs (i
.e. 2
pe
r Hea
lth fa
cilit
y )w
ill
be d
eplo
yed
Num
ber o
f mot
her
supp
ort g
roup
men
tors
de
ploy
ed
MO
H /
RHB/
PLH
IV
Prov
ide
PMTC
T tr
aini
ng fo
r se
rvic
e pr
ovid
ers t
o pe
ople
with
di
sabi
lity
600
serv
ice
prov
ider
s w
ill b
e tr
aine
dN
umbe
r of s
ervi
ce
prov
ider
s tra
ined
Re
port
, Site
as
sess
men
tM
OH
/ RH
B/PL
HIV
Build
cap
aciti
es o
f priv
ate
heal
th fa
cilit
ies t
o ro
llout
PM
TCT
serv
ice
Capa
city
of p
rivat
e he
alth
faci
litie
s will
be
stre
ngth
ened
to
prov
ide
PMTC
T
Num
ber o
f priv
ate
Hea
lth fa
cilit
ies w
ith
stre
ngth
ened
cap
acity
to
pro
vide
PM
TCT
Repo
rt, S
ite
asse
ssm
ent
MO
H/R
HB
Invo
lve
priv
ate
heal
th fa
cilit
ies
to p
rovi
de P
MTC
T se
rvic
esAl
l priv
ate
heal
th
faci
litie
s tha
t pro
vide
M
ater
nal H
ealth
se
rvic
es w
ill p
rovi
de
PMTC
T
Num
ber o
f priv
ate
heal
th fa
cilit
ies
prov
idin
g PM
TCT
Repo
rt, S
ite
asse
ssm
ent
cont
inue
d...

56
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
yIn
crea
se a
vaila
bilit
y an
d ut
iliza
tion
of
STI s
ervi
ces
900,
000
case
s will
be
trea
ted
Repo
rts
Repo
rts
MoH
/RH
B/EH
NRI
Crea
te st
rong
lead
ersh
ip fo
r STI
pr
ogra
ms
1,60
0 pr
ogra
m
man
ager
s will
be
trai
ned
Num
ber o
f pro
gram
m
anag
ers t
rain
edRe
port
s & si
te v
isits
MO
H/R
HB
Expa
nd S
TI se
rvic
es to
all
heal
th
faci
litie
s 3,
703
Hea
lth fa
cilit
ies
will
pro
vide
STI
serv
ice
Num
ber o
f hea
lth
faci
litie
s pro
vidi
ng S
TI
serv
ice
Repo
rts
Inte
nsify
hea
lth e
duca
tion
to
impr
ove
STI t
reat
men
t see
king
be
havi
our &
util
izat
ion
of
serv
ices
All K
ebel
es w
ill
cond
uct c
omm
unity
m
obili
zatio
n on
STI
Num
ber o
f CC
sess
ions
th
at a
ddre
ssed
STI
iss
ues
Surv
eys
Prom
ote
part
ner n
otifi
catio
n du
ring
STI c
ase
dete
ctio
n50
% o
f STI
clie
nts w
ill
refe
r the
ir cl
ient
s for
ST
I scr
eeni
ng
Perc
enta
ge o
f STI
ca
ses w
ho su
cces
sful
ly
refe
rred
thei
r par
tner
s fo
r STI
scre
enin
g
Surv
eys
Ensu
re a
vaila
bilit
y of
dru
gs a
nd
reag
ents
in a
ll pu
blic
hea
lth
faci
litie
s
STI d
rugs
and
reag
ents
w
ill b
e av
aila
ble
all
time
in 3
,703
Hea
lth
faci
litie
s
Num
ber o
f Hea
lth
faci
litie
s with
ava
ilabl
e ST
I dru
gs a
nd re
agen
ts
all t
he ti
me
Repo
rts a
nd si
te v
isits
MO
H/P
FSA/
RHB
Trai
n he
ath
care
wor
kers
on
synd
rom
ic S
TI c
ase
diag
nosis
an
d m
anag
emen
t
7,40
6 he
alth
car
e pr
ovid
ers w
ill b
e tr
aine
d on
STI
m
anag
emen
t
Num
ber o
f hea
lth c
are
prov
ider
s tra
ined
on
STI
Repo
rts
MO
H /
RHB
Trai
n 37
03 la
bora
tory
te
chni
cian
s to
perfo
rm v
ario
us
bact
erio
logi
cal a
nd se
rolo
gica
l te
sts
3,70
3 la
bora
tory
te
chni
cian
s will
be
trai
ned
Num
ber o
f lab
orat
ory
tech
nici
ans t
rain
edRe
port
s and
site
visi
tsEH
NRI
Dev
elop
STI
follo
w u
p an
d da
ta
valid
atio
n sy
stem
Func
tiona
l STI
follo
w
up &
val
idat
ion
syst
em
will
be
ensu
red
Esta
blish
men
t of S
TI
follo
w u
p &
valid
atio
n sy
stem
Doc
umen
ts p
rodu
ced
& sit
e vi
sits
MoH
/RH
B/EH
NRI
Prov
ide
STI t
rain
ing
for s
ervi
ce
prov
ider
s to
peop
le w
ith sp
ecia
l ne
eds
200
serv
ice
prov
ider
s w
ill b
e tr
aine
dN
umbe
r of s
ervi
ce
prov
ider
s tra
ined
Re
port
, Site
as
sess
men
tM
oH/R
HB
cont
inue
d...

2010/11-2014/15
57
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
yIn
crea
se su
pply
, di
strib
utio
n an
d ut
iliza
tion
of
mal
e an
d fe
mal
e co
ndom
s
Dev
elop
Nat
iona
l con
dom
st
rate
gySt
rate
gic
docu
men
t on
con
dom
will
be
deve
lope
d
Doc
umen
t pro
duce
dRe
port
MO
H/
FHAP
CO//
Pa
rtne
rs
Prom
ote
and
cond
uct
cam
paig
ns o
n pr
oper
&
cons
isten
t use
of c
ondo
m
Six
cond
om
prom
otio
n ca
mpa
igns
w
ill b
e co
nduc
ted
Num
ber o
f con
dom
pr
omot
ion
cam
paig
ns
cond
ucte
d
Repo
rts
MO
H/R
HB/
CSO
Expa
nd p
erip
hera
l out
lets
of
cond
om d
istrib
utio
n30
,000
out
lets
cre
ated
N
umbe
r of c
ondo
m
outle
ts c
reat
ed
Repo
rts
Targ
eted
con
dom
dist
ribut
ion,
pa
rtic
ular
ly to
MAR
Ps88
8 m
illio
n co
ndom
s be
dist
ribut
ed to
M
ARPs
(acc
ount
s fo
r 50%
of o
vera
ll di
strib
utio
n)
Num
ber o
f con
dom
s di
strib
uted
to M
ARPs
Repo
rts
Ensu
re a
dequ
ate
supp
ly o
f co
ndom
1.96
7 bi
llion
con
dom
s w
ill b
e pr
ocur
ed o
ver
5 ye
ars
Num
ber o
f mal
e an
d fe
mal
e co
ndom
s av
aila
ble
for
dist
ribut
ion
natio
nwid
e du
ring
the
last
12
mon
ths
Repo
rts
MO
HPF
SA /
RHB/
CSO
s
Dist
ribut
e m
ale
cond
om1.
7703
bill
ion
mal
e co
ndom
s will
be
dist
ribut
ed
Num
ber o
f mal
e co
ndom
s dist
ribut
edRe
port
sM
OH
/RH
B/CS
Os
Dist
ribut
e fe
mal
e co
ndom
196.
7 m
illio
n fe
mal
e co
ndom
s will
be
dist
ribut
ed
Num
ber o
f fem
ale
cond
oms d
istrib
uted
Repo
rts
MO
H/R
HB/
CSO
s
Stre
ngth
en
infe
ctio
n pr
even
tion
and
bloo
d sa
fety
se
rvic
es
Ensu
re th
e av
aila
bilit
y of
ad
equa
te in
fect
ion
prot
ectiv
e m
ater
ials
All f
acili
ties w
ill
be su
pplie
d w
ith
min
imum
requ
ired
IP m
ater
ials
as p
er
serv
ice
stan
dard
Num
ber o
f fac
ilitie
s su
pplie
d w
ith
min
imum
IP m
ater
ials
Repo
rts,
site
visit
sM
oH, R
HB
s
Impr
ove
was
te d
ispos
al
man
agem
ent i
n he
alth
faci
litie
s. W
aste
disp
osal
will
be
impr
oved
in a
ll he
alth
fa
cilit
ies
Hea
lth fa
cilit
ies w
ith
impr
oved
Was
te
disp
osal
Repo
rts,
site
visit
sM
oH
Prov
ide
IP tr
aini
ngs t
o st
aff7,
000
staff
will
be
trai
ned
on IP
Num
ber o
f tra
ined
staff
on
IPRe
port
s
cont
inue
d...

58
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
ySt
reng
then
in
fect
ion
prev
entio
n an
d bl
ood
safe
ty
serv
ices
Impl
emen
t nat
iona
l blo
od
tran
sfus
ion
serv
ices
stra
tegy
Nat
iona
l blo
od
tran
sfus
ion
serv
ices
st
rate
gy w
ill b
e im
plem
ente
d
Impl
emen
tatio
n of
st
rate
gyRe
port
sM
oH/E
RCS
Cond
uct a
sses
smen
t on
prev
alen
ce n
eedl
e pi
erce
/ pr
ick
& ot
her s
harp
mat
eria
ls in
he
alth
faci
litie
s
An a
sses
smen
t will
be
cond
ucte
dAs
sess
men
t doc
umen
t pr
oduc
edD
ocum
ent
MoH
Avai
l pos
t exp
osur
e pr
ophy
laxi
s (PE
P)
trea
tmen
t
Avai
l PEP
in a
ll he
alth
faci
litie
s3,
303
heal
th fa
cilit
ies
will
pro
vide
PEP
tr
eatm
ent
Num
ber o
f hea
lth
faci
litie
s pro
vidi
ng P
EP
Repo
rts,
site
asse
ssm
ent
MoH
Cond
uct b
asel
ine
asse
ssm
ent
on P
EPBa
selin
e as
sess
men
t w
ill b
e co
nduc
ted
Asse
ssm
ent r
epor
t pr
oduc
edRe
port
sM
OH
/RH
B
Prov
ide
PEP
for a
ll el
igib
le
clie
nts
100%
of c
lient
s el
igib
le fo
r PEP
am
ong
clie
nts c
laim
ing
the
serv
ice
will
rece
ive
PEP
Perc
enta
ge o
f elig
ible
cl
ient
s am
ong
thos
e cl
aim
ing
the
serv
ice
rece
ived
PEP
Surv
eys
MO
H/R
HB
Acce
lera
te m
ale
circ
umci
sion
in
area
s nee
ded
Cond
uct f
easib
ility
ass
essm
ent
on m
ale
circ
umci
sion
in th
e co
mm
unity
and
ass
ess t
he
capa
citie
s of h
ealth
faci
litie
s
Feas
ibili
ty a
nd h
ealth
fa
cilit
y ca
paci
ty
asse
ssm
ent w
ill b
e co
nduc
ted
Asse
ssm
ent r
epor
t pr
oduc
edRe
port
sM
oH/R
HB
Prom
ote
mal
e ci
rcum
cisio
n (M
C)Ad
voca
cy, c
omm
unity
m
obili
zatio
n on
MC
will
be
cond
ucte
d
Advo
cacy
repo
rts
Repo
rts
RHB
Prov
ide
trai
ning
s on
MC
180
heal
th c
are
wor
kers
will
be
trai
ned
on M
C
Num
ber o
f hea
lth c
are
wor
kers
trai
ned
on M
CRe
port
sM
OH
Avai
l mal
e ci
rcum
cisio
n ki
ts10
0,00
0 M
C ki
ts w
ill b
e m
ade
avai
labl
e N
umbe
r of M
C ki
ts
avai
led
Repo
rts
MoH
Prov
ide
safe
mal
e ci
rcum
cisio
n se
rvic
es10
0,00
0 yo
ung
mal
e ag
ed 1
0 to
24
year
s will
get
safe
ci
rcum
cisio
n se
rvic
e
Num
ber o
f mal
es
circ
umci
sed
Repo
rts
MO
H
cont
inue
d...

2010/11-2014/15
59
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
yEn
sure
pro
visio
n of
use
r frie
ndly
bi
omed
ical
HIV
Pr
even
tion
serv
ices
to
peo
ple
with
sp
ecia
l nee
ds
Cond
uct a
sses
smen
t of H
ealth
fa
cilit
ies t
o ev
alua
te st
atus
in
prov
idin
g us
er-fr
iend
ly se
rvic
es
to e
lder
ly a
nd p
eopl
e w
ith
disa
bilit
y
Asse
ssm
ent o
f Hea
lth
faci
litie
s to
eval
uate
st
atus
in p
rovi
ding
us
er-fr
iend
ly se
rvic
es
to e
lder
ly a
nd p
eopl
e w
ith d
isabi
lity
will
be
done
Asse
ssm
ent c
ondu
cted
Repo
rts
MO
H
Cond
uct c
onsu
ltativ
e m
eetin
gs
to id
entif
y m
odal
ities
of
prov
idin
g bi
omed
ical
HIV
/AI
DS
serv
ices
for p
eopl
e w
ith
disa
bilit
y an
d th
e el
derly
2 Co
nsul
tativ
e m
eetin
gs w
ill b
e co
nduc
ted
Num
ber o
f con
sulta
tive
mee
tings
con
duct
ed
Proc
eedi
ngs
MO
H /R
HB
Dev
elop
stra
tegi
c do
cum
ent
to d
efine
pac
kage
of H
IV /
AID
S se
rvic
es a
nd m
odal
ities
of
del
iver
ing
the
serv
ices
for
Peop
le w
ith d
isabi
lity
and
the
elde
rly
Stra
tegi
c do
cum
ent
will
be
deve
lope
d St
rate
gic
docu
men
t de
velo
ped
Doc
umen
t
Cust
omiz
e an
d di
ssem
inat
e tr
aini
ng m
anua
ls on
HIV
/AID
S bi
omed
ical
serv
ices
for p
eopl
e w
ith d
isabi
lity
and
the
elde
rly
Man
ual w
ill b
e cu
stom
ized
and
di
ssem
inat
ed
Num
ber o
f tra
inin
g m
ater
ials
deve
lope
d on
bio
med
ical
serv
ices
fo
r peo
ple
with
spec
ial
need
s
Doc
umen
t
Inte
nsify
pos
itive
pr
even
tion
Prov
ide
HIV
info
rmat
ion,
ed
ucat
ion
and
risk
redu
ctio
n ed
ucat
ion
and
coun
selli
ng
450,
000
PLH
IV w
ill
rece
ive
HIV
edu
catio
n an
d co
unse
lling
Num
ber o
f HIV
+
peop
le re
ceiv
ed fr
om
HIV
edu
catio
n an
d co
unse
lling
.
Repo
rts a
nd S
urve
yM
OH
/RH
Bs
Stre
ngth
en c
oupl
e co
unse
lling
an
d te
stin
g45
,000
cou
ples
will
re
ceiv
e co
unse
lling
Num
ber o
f cou
ples
re
ceiv
ed c
ouns
ellin
g Re
port
s, su
rvey
M
OH
/RH
Bs
Cond
uct F
amily
bas
ed H
IV
coun
selli
ng a
nd te
stin
g50
% o
f fam
ilies
of H
IV
posit
ive
clie
nts w
ill
have
all t
heir
fam
ily
mem
bers
test
ed fo
r HIV
Perc
enta
ge o
f fam
ilies
of
HIV
pos
itive
clie
nts
who
hav
e al
l the
ir fa
mily
m
embe
rs te
sted
for H
IV
Surv
ey, R
epor
ts a
nd
site
supe
rvisi
ons
Dev
elop
spec
ial p
acka
ge fo
r ad
oles
cent
s on
ART
on H
IV
coun
selli
ng, R
epro
duct
ive
Hea
lth, a
nd re
late
d iss
ues
Pack
age
on H
IV
coun
selli
ng,
Repr
oduc
tive
Hea
lth,
and
rela
ted
issue
s w
ill b
e de
velo
ped
for
adol
esce
nts o
n AR
T
Doc
umen
t with
pac
kage
on
HIV
cou
nsel
ling,
Re
prod
uctiv
e H
ealth
, an
d re
late
d iss
ues
Repo
rts
MO
H /
HAP
COs/
RHBs
cont
inue
d...

60
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Indi
cato
rVe
rific
atio
n Le
ad A
genc
yIn
tens
ify p
ositi
ve
prev
entio
nPr
ovid
e se
rvic
e to
the
HIV
po
sitiv
e ad
oles
cent
s bas
ed o
n th
e pa
ckag
e
100%
of H
IV p
ositi
ve
adol
esce
nts w
ill b
e pr
ovid
ed w
ith se
rvic
e ba
sed
on th
e pa
ckag
e
Perc
enta
ge o
f tee
ns
prov
ided
with
serv
ice
base
d on
the
pack
age
Repo
rts
MO
H /
HAP
COs/
RHBs
Esta
blish
/str
engt
hen
post
test
cl
ubs a
nd o
ther
pee
r sup
port
gr
oups
100%
of H
CT si
tes w
ill
have
pos
t tes
t clu
bs
and
othe
r pee
r sup
port
gr
oups
Perc
enta
ge o
f HCT
site
s w
ith p
ost t
est c
lubs
an
d ot
her p
eer s
uppo
rt
grou
ps
Repo
rts a
nd su
rvey
s
Prov
ide
Educ
atio
n on
con
siste
nt
cond
om u
se to
PLH
IV10
0% P
LHAs
will
be
edu
cate
d on
ap
prop
riate
and
co
nsist
ent u
se o
f co
ndom
Perc
enta
ge o
f PLH
As
who
rece
ived
edu
catio
n on
con
siste
nt u
se o
f co
ndom
Cond
om p
rovi
sion
and
dist
ribut
ion
89.4
mill
ion
cond
oms
will
be
dist
ribut
ed
Num
ber o
f con
dom
s di
strib
uted
Pr
ovid
e ST
I ser
vice
s10
0% o
f HIV
/AID
S pa
tient
s on
chro
nic
care
will
rece
ive
STI
serv
ices
Perc
enta
ge o
f HIV
/AID
S pa
tient
s on
chro
nic
care
re
ceiv
ed S
TI se
rvic
es
Repo
rts a
nd su
rvey
s
Prov
ide
fam
ily p
lann
ing
serv
ices
100%
of H
IV/A
IDS
patie
nts o
n ch
roni
c ca
re w
ill re
ceiv
e fa
mily
pl
anni
ng se
rvic
es
Perc
enta
ge o
f HIV
/AID
S pa
tient
s on
chro
nic
care
who
rece
ive
fam
ily
plan
ning
serv
ices
Repo
rts,
site
visit
s and
su
rvey
s
Them
atic
Are
a Th
ree:IncreaseAccesstoandImproveQualityofChronicCareandTreatment
Generalobjective:
To
redu
ce H
IV re
late
d m
orbi
dity
and
mor
talit
y an
d im
prov
e qu
ality
of l
ife o
f PLH
IVSpecificobjectives:
•To
incr
ease
ART
enr
olm
ent f
rom
73%
in 2
009
to 9
5% b
y 20
14/1
5•
To in
crea
se s
urvi
val a
mon
g th
ose
who
hav
e st
arte
d AR
T to
from
73%
in 2
009
to 8
5% b
y 20
14/1
5.•
To in
crea
se p
atie
nt r
eten
tion
rate
am
ong
thos
e w
ho s
tart
ed A
RT to
85%
by
201/
15•
To in
crea
se p
aedi
atri
c AR
T co
vera
ge fr
om 6
6% in
201
0 to
90%
in 2
014/
15•
To in
crea
se p
erce
ntag
e of
pre
-ART
pat
ient
s on
cot
rim
oxaz
ole
prop
hyla
xis
from
68%
to 9
5% in
201
4/15
cont
inue
d...

2010/11-2014/15
61
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsVe
rific
atio
n Le
ad A
genc
yEn
sure
acc
ess a
nd
enha
nce
up ta
ke o
f AR
T se
rvic
es
455,
190
adul
t PLH
IV
will
rece
ive
ART
Num
ber o
f adu
lt PL
HIV
re
ceiv
ing
antir
etro
vira
l th
erap
y
Repo
rts
MO
H/F
HAP
CO
29,7
76 P
aedi
atric
s PL
HIV
will
rece
ive
ART
Num
ber o
f Pae
diat
rics
PLH
IV re
ceiv
ing
antir
etro
vira
l the
rapy
Repo
rts
MO
H/F
HAP
CO
Expa
nd a
cces
s to
care
and
trea
tmen
t at
prim
ary
heal
th
care
faci
litie
s with
st
reng
then
ed
serv
ice
linka
ges
and
inte
grat
ion
Prov
ide
trai
ning
of h
ealth
pe
rson
nel
5368
hea
lth p
rovi
ders
w
ill b
e tr
aine
d on
ca
re a
nd tr
eatm
ent
man
agem
ent
Num
ber o
f hea
lth c
are
prov
ider
s tra
ined
.Re
port
sM
oH/ R
HBs
/H
APCO
Incr
ease
num
ber o
f Hea
lth
faci
litie
s pro
vidi
ng A
RTAR
T se
rvic
es w
ill b
e pr
ovid
ed in
3,3
03
heal
th fa
cilit
ies
Num
ber o
f Hea
lth
faci
litie
s pro
vidi
ng
antir
etro
vira
l the
rapy
.
Repo
rts
Dev
elop
and
diss
emin
ate
serv
ice
pack
age
and
trai
ning
m
anua
l on
ART
for p
eopl
e w
ith
disa
bilit
y
Man
ual w
ill b
e de
velo
ped
Dev
elop
ed m
anua
lD
ocum
ent
Dev
elop
SO
P an
d st
anda
rdiz
e in
tra
and
inte
r fac
ility
refe
rral
fo
rmat
s
SoP
and
form
ats w
ill
be d
evel
oped
and
st
anda
rdiz
ed
SOP
and
refe
rral
fo
rmat
s dev
elop
ed/
stan
dard
ized
Doc
umen
ts
Mon
itor e
ffect
iven
ess o
f the
re
ferr
al sy
stem
3,30
3 fa
cilit
ies w
ill
have
effe
ctiv
e In
ter-
faci
lity
serv
ice
linka
ge
Num
ber o
f Hea
lth
faci
litie
s with
effe
ctiv
e In
ter-
faci
lity
serv
ice
linka
ge
Repo
rts a
nd si
te v
isits
Inte
grat
e AR
T se
rvic
e pa
ckag
e of
peo
ple
with
disa
bilit
y in
the
exist
ing
Hea
lth fa
cilit
ies
100%
of t
he H
ealth
fa
cilit
ies w
ill in
tegr
ate
the
pack
age
Perc
enta
ge o
f Hea
lth
faci
litie
s int
egra
ting
the
pack
age
Repo
rt, S
ite
asse
ssm
ent
MoH
/ RH
Bs/
HAP
CO
Stre
ngth
en
labo
rato
ry se
rvic
es
and
refe
rral
syst
em
Avai
l min
imum
labo
rato
ry
serv
ices
at c
hron
ic c
are
sites
80%
chr
onic
car
e sit
es
will
be
cove
red
with
m
inim
um la
bora
tory
se
rvic
es
Num
ber o
f chr
onic
ca
re si
tes c
over
ed w
ith
min
imum
labo
rato
ry
serv
ices
Repo
rts a
nd si
te v
isits
EHN
RI
Stre
ngth
en p
reve
ntiv
e an
d cu
rativ
e m
aint
enan
ce (t
rain
ing,
w
orks
hop
and
spar
e pa
rts)
Prev
entiv
e m
aint
enan
ce se
rvic
e w
ill b
e un
dert
aken
by
all l
abor
ator
ies
Num
ber o
f la
bora
torie
s with
fu
nctio
nal p
reve
ntiv
e m
aint
enan
ce se
rvic
e
Repo
rts
Cura
tive
mai
nten
ance
se
rvic
e w
ill b
e pr
ovid
ed a
t reg
iona
l an
d fe
dera
l lev
el
Regi
ons w
ith
mai
nten
ance
cen
tres
Repo
rts
cont
inue
d...

62
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsVe
rific
atio
n Le
ad A
genc
ySt
reng
then
la
bora
tory
serv
ices
an
d re
ferr
al sy
stem
Stre
ngth
en q
ualit
y as
sura
nce
syst
em
Func
tiona
l Qua
lity
assu
ranc
e sy
stem
will
be
put
in p
lace
Exist
ence
of q
ualit
y as
sura
nce
syst
emRe
port
sEH
NRI
Stre
ngth
en la
bora
tory
in
form
atio
n sy
stem
Func
tiona
l LIS
syst
em
will
be
put i
n pl
ace
Exist
ence
of L
ISSu
perv
ision
Build
cap
acity
of l
abor
ator
y pe
rson
nel
Capa
ble
labo
rato
ry
pers
onne
l in
runn
ing
HIV
inve
stig
atio
ns a
nd
QA
will
be
avai
labl
e
Impr
oved
cap
acity
of
Labo
rato
ry p
erso
nnel
Supe
rvisi
on
Ensu
re a
vaila
bilit
y of
Ess
entia
l OI,
ARV
drug
s and
reag
ents
Fore
cast
the
need
for O
I, AR
Vs
and
reag
ents
Adeq
uate
am
ount
of
OI,
and
ARV
drug
s will
be
ava
iled
Repo
rted
num
ber o
f st
ock
outs
in th
e la
st
one
mon
th
Repo
rts
PFSA
Ensu
re ti
mel
y pr
ocur
emen
t and
di
strib
utio
n of
OIs
, ARV
dru
gs
and
, rea
gent
s
All s
ervi
ce re
nder
ing
sites
will
hav
e ad
equa
te A
RV/O
I su
pplie
s all
times
Num
ber o
f Hea
lth
faci
litie
s with
un
inte
rrup
ted
supp
ly o
f AR
V an
d O
IsEx
pand
war
ehou
ses
Cons
truc
tion
of 1
2 w
areh
ouse
s will
be
Supp
orte
d
Num
ber o
f war
ehou
ses
cons
truc
ted
Repo
rts &
site
visi
ts
Stre
ngth
en lo
gist
ics
man
agem
ent i
nfor
mat
ion
syst
em
Inve
ntor
y m
echa
nism
/LM
IS w
ill b
e es
tabl
ished
Exist
ence
of f
unct
iona
l In
vent
ory/
LM
IS a
t all
leve
ls
Perio
dic
asse
ss &
re
port
s
Equi
p th
e su
pply
man
agem
ent
syst
em w
ith tr
ansp
orta
tion
mea
ns
12 V
ehic
les w
ill b
e pr
ocur
edN
umbe
r of v
ehic
les
purc
hase
d to
supp
ort
SM sy
stem
Repo
rts a
nd si
te v
isits
Stre
ngth
en T
B/H
IV c
olla
bora
tive
activ
ities
Scre
en a
ll di
agno
sed
TB p
atie
nts
for H
IV90
% o
f TB
patie
nts w
ill
be c
ouns
elle
d &
test
ed
for H
IV
% o
f TB
patie
nts
coun
selle
d &
test
ed fo
r H
IV
Repo
rts
MoH
/RH
B
Link
HIV
pos
itive
TB
case
s to
HIV
se
rvic
es80
% o
f HIV
pos
itive
TB
case
s will
be
linke
d to
H
IV c
are
& tr
eatm
ent
% o
f HIV
pos
itive
TB
patie
nts l
inke
d to
HIV
ca
re &
trea
tmen
t
Repo
rts
Scre
en a
ll H
IV p
ositi
ve c
ases
for
TB10
0% o
f HIV
pos
itive
ca
ses w
ill b
e sc
reen
ed
for T
B ca
se d
etec
tion
% o
f HIV
pos
itive
cas
es
scre
ened
for T
B Re
port
s
cont
inue
d...

2010/11-2014/15
63
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsVe
rific
atio
n Le
ad A
genc
ySt
reng
then
TB/
HIV
col
labo
rativ
e ac
tiviti
es
Prov
ide
INH
pro
phyl
axis
for
elig
ible
pat
ient
s80
% o
f elig
ible
clie
nts
will
rece
ive
INH
pr
ophy
laxi
s
Perc
ent o
f HIV
pos
itive
ca
ses r
ecei
ving
INH
pr
ophy
laxi
s
Repo
rts
MoH
/RH
B
Stre
ngth
en T
B-H
IV c
o-in
fect
ion
man
agem
ent
5368
hea
lth c
are
prov
ider
s will
be
trai
ned
Num
ber h
ealth
car
e pr
ovid
ers t
rain
ed o
n TB
-HIV
co-
infe
ctio
n m
anag
emen
t
Repo
rts
Enha
nce
trea
tmen
t lit
erac
y an
d ad
here
nce
to
trea
tmen
t
Dev
elop
and
enf
orce
gui
delin
es
on tr
eatm
ent l
itera
cy a
nd
adhe
renc
e
Trea
tmen
t lite
racy
gu
idel
ine
will
be
deve
lope
d
A gu
idel
ine
on
trea
tmen
t lite
racy
de
velo
ped
and
enfo
rced
Repo
rts &
dev
elop
ed
guid
elin
eM
oH/R
HB
Stre
ngth
en a
dher
ence
co
unse
lling
by
heal
th c
are
wor
kers
, cas
e m
anag
ers a
nd
adhe
renc
e su
ppor
ters
Adhe
renc
e ed
ucat
ion
/cou
nsel
ling
will
be
stre
ngth
ened
Avai
labi
lity
of
adhe
renc
e co
unse
lling
/ed
ucat
ion
Repo
rts
Prov
ide
trai
ning
on
adhe
renc
e co
unse
lling
to h
ealth
wor
kers
, ca
se m
anag
ers a
nd a
dher
ence
su
ppor
ters
1,34
2 pe
ople
will
be
trai
ned
on a
dher
ence
co
unse
lling
Num
ber o
f peo
ple
trai
ned
on a
dher
ence
co
unse
lling
Repo
rts
Diss
emin
ate
trea
tmen
t lite
racy
ed
ucat
ion
thro
ugh
mas
s med
ia12
mas
s med
ia
cam
paig
ns o
n tr
eatm
ent l
itera
cy
and
adhe
renc
e w
ill b
e ca
rrie
d ou
t
Num
ber o
f mas
s med
ia
cam
paig
ns c
ondu
cted
Re
port
s
Inst
itute
per
iodi
c m
onito
ring
and
follo
w u
p of
lost
to fo
llow
up
pat
ient
s
All A
RT re
nder
ing
faci
litie
s will
est
ablis
h Fa
cilit
y ba
sed
func
tiona
l tra
cing
m
echa
nism
Num
ber o
f fac
ilitie
s w
ith F
unct
iona
l tra
cing
sy
stem
Repo
rts a
nd si
te v
isits
Prov
ide
ART
trai
ning
for
serv
ice
prov
ider
s on
iden
tified
m
odal
ities
of s
ervi
ce p
rovi
sion
to p
eopl
e w
ith d
isabi
lity
600
serv
ice
prov
ider
s w
ill b
e tr
aine
dN
umbe
r of s
ervi
ce
prov
ider
s tra
ined
Re
port
, Site
as
sess
men
t
Dev
elop
and
ava
il gu
idel
ine
whi
ch d
irect
s the
pro
cess
of
prov
idin
g ch
roni
c ca
re a
nd
trea
tmen
t ser
vice
in p
rivat
e he
alth
faci
litie
s.
Gui
delin
e fo
r pro
visio
n of
Chr
onic
car
e an
d tr
eatm
ent i
n pr
ivat
e he
alth
faci
litie
s will
be
deve
lope
d an
d av
aile
d
Dev
elop
ed g
uide
line
whi
ch d
irect
s the
pr
oces
s of p
rovi
ding
ch
roni
c ca
re se
rvic
e tr
eatm
ent i
n pr
ivat
e he
alth
faci
litie
s.
Repo
rts a
nd v
isits
cont
inue
d...

64
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsVe
rific
atio
n Le
ad A
genc
yEn
hanc
e tr
eatm
ent
liter
acy
and
adhe
renc
e to
tr
eatm
ent
Cond
uct a
sses
smen
t in
priv
ate
heal
th fa
cilit
ies
Asse
ssm
ent o
n pr
ivat
e he
alth
faci
litie
s will
be
Cond
ucte
d
Resu
lt of
ass
essm
ent
cond
ucte
d on
priv
ate
heal
th fa
cilit
ies
Repo
rts
MoH
/RH
B
Build
cap
aciti
es o
f priv
ate
heal
th fa
cilit
ies t
o ro
llout
HIV
/AI
DS
chro
nic
care
serv
ices
101
Priv
ate
Hea
lth
faci
litie
s will
hav
e ca
paci
ty to
pro
vide
ch
roni
c ca
re se
rvic
es
Num
ber o
f priv
ate
Hea
lth fa
cilit
ies w
ith
ensu
red
capa
city
to
prov
ide
Chro
nic
HIV
ca
re
Repo
rts a
nd v
isits
Rollo
ut A
RT se
rvic
es in
to p
rivat
e he
alth
faci
litie
s10
1 pr
ivat
e he
alth
fa
cilit
ies s
igne
d an
M
OU
and
pro
vide
ART
se
rvic
es
Num
ber o
f priv
ate
heal
th fa
cilit
ies s
igne
d an
MO
U a
nd p
rovi
de
ART
/PM
TCT
serv
ices
Repo
rts a
nd v
isits
Stre
ngth
en c
linic
al m
ento
ring
Hea
lth fa
cilit
ies w
ill
rece
ive
regu
lar c
linic
al
men
torin
g
Num
ber o
f Hea
lth
faci
litie
s rec
eivi
ng
regu
lar c
linic
al
men
torin
g
Repo
rts a
nd si
te v
isits
Stre
ngth
en p
ublic
-pr
ivat
e pa
rtne
rshi
pM
ap a
nd c
reat
e di
rect
ory
of
priv
ate
heal
th fa
cilit
ies
Dire
ctor
y of
priv
ate
heal
th fa
cilit
ies w
ill b
e de
velo
ped
Dire
ctor
y of
priv
ate
heal
th fa
cilit
ies
prod
uced
Repo
rts a
nd d
irect
ory
MO
H/ H
APCO
Org
aniz
e pu
blic
-priv
ate
part
ners
hip
foru
m.
Func
tiona
l pub
lic
priv
ate
part
ners
hip
foru
m w
ill b
e es
tabl
ished
Exist
ence
of f
unct
iona
l pu
blic
priv
ate
part
ners
hip
foru
ms
Repo
rts
MoH
/ RH
B
Addr
ess h
uman
re
sour
ce is
sues
Supp
ort h
ighe
r lea
rnin
g in
stitu
tions
to p
rovi
de p
re-
serv
ice
HIV
trai
ning
to a
ll he
alth
sc
ienc
e st
uden
ts
All n
ew g
radu
ates
will
be
equ
ippe
d w
ith H
IV
prog
ram
s and
serv
ice
prot
ocol
s prio
r to
grad
uatio
n
Inte
grat
ion
of H
IV in
un
iver
sitie
s cur
ricul
um
Repo
rts
Uni
vers
ities
Prov
ide
in-s
ervi
ce tr
aini
ng o
n H
IV a
nd A
IDS
in h
ealth
sect
or23
,121
hea
lth w
orke
rs
will
be
trai
ned
on H
IV/
AID
S
Num
ber o
f hea
lth
wor
kers
trai
ned
Repo
rts
Stre
ngth
en ta
sk-s
hifti
ng, c
linic
al
men
torin
g an
d su
ppor
tive
supe
rvisi
on
task
-shi
fting
and
cl
inic
al m
ento
ring
will
be
stre
ngth
ened
Avai
labi
lity
of c
linic
al
men
torin
g an
d ta
sk
shift
ing
Repo
rts a
nd si
te v
isits
MoH
/Reg
ions
cont
inue
d...

2010/11-2014/15
65
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsVe
rific
atio
n Le
ad A
genc
yAd
dres
s hum
an
reso
urce
issu
esSt
reng
then
task
-shi
fting
, clin
ical
m
ento
ring
and
supp
ortiv
e su
perv
ision
4 su
ppor
tive
supe
rvisi
ons p
er y
ear
will
be
cond
ucte
d to
he
alth
faci
litie
s
Num
ber o
f sup
port
ive
supe
rvisi
ons c
ondu
cted
pe
r hea
lth fa
cilit
y pe
r ye
ar
Repo
rts
MoH
/Reg
ions
Trai
n he
alth
faci
lity
lead
ers o
n H
IV/A
IDS
prog
ram
man
agem
ent
& in
tegr
atio
n of
serv
ices
3,30
3 he
alth
faci
lity
lead
ers w
ill b
e tr
aine
d on
HIV
/AID
S pr
ogra
m
man
agem
ent
Num
ber o
f hea
lth
faci
lity
lead
ers t
rain
edRe
port
sM
oH /R
egio
ns
Prom
ote
Invo
lvem
ent o
f sta
ff in
hea
lth fa
cilit
ies o
pera
tiona
l re
sear
ch
55 o
pera
tiona
l re
sear
ches
/stu
dies
will
be
con
duct
ed
Num
ber o
f ope
ratio
nal
stud
ies c
ondu
cted
Pu
blish
ed st
udie
sM
OH
/HAP
CO/
Regi
ons
Them
atic
Are
a Fo
ur:StrengthenCareandSupporttoMitigatetheImpactofHIV/AIDS
Generalobjective:
To
impr
ove
the
livel
ihoo
d of
the
need
y aff
ecte
d an
d in
fect
ed p
eopl
eSpecificobjectives:
•To
incr
ease
car
e an
d su
ppor
t to
OVC
from
30%
in 2
008
to 5
0% b
y 20
14/1
5•
To in
crea
se c
are
and
supp
ort t
o ne
edy
PLH
IV fr
om 6
0,00
0 in
200
9 to
100
,000
in 2
014/
15
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsVe
rific
atio
n Le
ad A
genc
ySt
reng
then
the
invo
lvem
ent o
f lo
cal c
omm
uniti
es
in c
are
and
supp
ort
Iden
tify
care
and
supp
ort n
eeds
an
d ga
ps in
eac
h Ke
bele
s Al
l Keb
eles
will
id
entif
y ca
re a
nd
supp
ort n
eeds
and
ga
ps
Num
ber o
f Keb
eles
w
ith id
entifi
ed c
are
and
supp
ort g
aps
Repo
rts &
site
visi
tsM
oWYC
/ N
EP+
/
Stre
ngth
en a
nd u
se e
xist
ing
com
mun
ity st
ruct
ure
to p
rovi
de
care
/sup
port
in th
e O
VCs’
fam
ilial
env
ironm
ent
Com
mun
ities
in
17,5
00 k
ebel
es w
ill b
e m
obili
zed
to su
ppor
t an
d ca
re fo
r OVC
Num
ber o
f keb
eles
with
ca
re a
nd su
ppor
t pla
nRe
port
s and
site
visi
ts
Enha
nce
the
prov
ision
of
stan
dard
ized
car
e an
d su
ppor
t to
OVC
50%
of t
he O
VC w
ill
get c
are
& su
ppor
t ba
sed
on p
acka
ge
Repo
rts
MoW
YCA
/ H
APCO
cont
inue
d...

66
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsVe
rific
atio
n Le
ad A
genc
yEn
hanc
e th
e pr
ovisi
on o
f st
anda
rdiz
ed c
are
and
supp
ort t
o O
VC
Dev
elop
an
OVC
car
e an
d su
ppor
t sta
ndar
d an
d se
rvic
e de
liver
y pa
ckag
e
An O
VC c
are
and
supp
ort s
tand
ard
and
serv
ice
deliv
ery
pack
age
will
be
deve
lope
d
Exist
ence
of a
n O
VC
care
/sup
port
stan
dard
&
serv
ice
deliv
ery
guid
elin
e
Repo
rts
MoW
YCA
/ H
APCO
Cond
uct O
VC si
tuat
iona
l as
sess
men
tSi
tuat
ion
anal
ysis
will
be
con
duct
edSi
tuat
iona
l ana
lysis
do
cum
ent p
rodu
ced
Doc
umen
t
Map
OVC
serv
ices
and
dev
elop
re
ferr
al n
etw
ork
amon
g se
rvic
e pr
ovid
ers
Refe
rral
net
wor
k w
ill
be c
reat
edAv
aila
bilit
y of
fu
nctio
nal r
efer
ral
netw
orks
Doc
umen
t and
site
su
perv
ision
MoW
YCA/
HAP
CO
Build
the
capa
city
of
orga
niza
tions
eng
aged
in
serv
ice
prov
ision
and
ass
istan
ce
to im
plem
entin
g ag
enci
es
1000
Impl
emen
ting
agen
cies
and
or
gani
zatio
ns w
ill b
e su
ppor
ted
Num
ber o
f Im
plem
entin
g ag
enci
es
and
orga
niza
tions
su
ppor
ted
Repo
rts
Scho
ol-b
ased
su
ppor
t for
OVC
Prov
ide
supp
ort t
o sc
hool
bas
ed
OVC
pro
gram
sSc
hool
s will
pro
vide
O
VC su
ppor
tN
umbe
r of S
choo
ls pr
ovid
ing
OVC
supp
ort
Repo
rts
MoE
Stre
ngth
en
hous
ehol
d ec
onom
ic c
apac
ity
Build
the
capa
city
of o
lder
OVC
, gu
ardi
ans o
f OVC
and
PLH
IV o
n IG
A
50,0
00 O
VC a
nd th
eir
guar
dian
will
rece
ive
trai
ning
on
IGA
Num
ber o
f OVC
an
d th
eir g
uard
ians
su
ppor
ted
thro
ugh
IGA
Repo
rts
MoW
YCA/
CSO
s/H
APCO
25,0
00 P
LHIV
will
re
ceiv
e tr
aini
ng o
n IG
AN
umbe
r of P
LHIV
su
ppor
ted
thro
ugh
IGA
Repo
rts a
nd si
te v
isits
Prov
ide
seed
mon
ey75
,000
of b
enefi
ciar
ies
will
rece
ive
seed
m
oney
to st
art I
GA
Num
ber o
f ben
efici
arie
s re
ceiv
ed se
ed m
oney
Site
s and
site
visi
ts
Follo
w u
p an
d su
ppor
t to
crea
te
links
to m
arke
ts
Num
ber o
f ben
efici
arie
s m
ento
red
for I
GA
Repo
rts a
nd si
te v
isits

2010/11-2014/15
67
Them
atic
Are
a Fi
ve: StrengthenGenerationandUtilizationofStrategicInformation
Generalobjective:
To
ensu
re th
e tim
ely
gene
ratio
n an
d ut
iliza
tion
of s
trat
egic
info
rmat
ion
to e
nhan
ce e
vide
nced
-bas
ed d
ecisi
on m
akin
g of
Mul
tisec
tora
l H
IV/A
IDS
resp
onse
Specificobjectives:
•To
ens
ure
the
gene
ratio
n of
qua
lity
data
from
rou
tine
prog
ram
mon
itori
ng, s
urve
ys, s
urve
illan
ces
and
stud
ies.
•To
dis
sem
inat
e an
d ut
ilize
dat
a fr
om th
e M
& E
sys
tem
to g
uide
pol
icy
form
ulat
ion
and
prog
ram
pla
nnin
g an
d im
prov
emen
t
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsVe
rific
atio
n Le
ad A
genc
yCa
paci
ty B
uild
ing
for M
& E
Ensu
re a
vaila
bilit
y of
M a
nd
E offi
cer o
r HIV
/AID
S M
and
E
capa
city
at r
egio
nal,
key
sect
ors
and
CSO
s
All r
egio
ns, C
SOs,
sect
ors w
ill e
nsur
e av
aila
bilit
y of
hum
an
reso
urce
with
M a
nd E
ca
paci
ty
Num
ber o
f reg
ions
, CS
Os,
sect
ors w
ith
avai
labl
e tr
aine
d H
uman
reso
urce
on
M
and
E
Site
visi
t, Re
port
sRe
gion
s, Se
ctor
s, CS
Os
Dev
elop
M a
nd E
im
plem
enta
tion
man
ual
M a
nd E
im
plem
enta
tion
man
ual w
ill b
e de
velo
ped
Dev
elop
ed M
and
E
impl
emen
tatio
n m
anua
l
Doc
umen
t pro
duce
dH
APCO
Dev
elop
M a
nd E
trai
ning
cu
rric
ulum
M a
nd E
trai
ning
cu
rric
ulum
will
be
deve
lope
d
Dev
elop
ed M
and
E
trai
ning
cur
ricul
aD
ocum
ent p
rodu
ced
HAP
CO
Cond
uct t
rain
ing
for M
and
E
office
rs10
,000
trai
ned
(800
0 M
and
E st
aff &
200
0 pr
ogra
m m
anag
ers)
w
ill b
e tr
aine
d
Num
ber o
f M a
nd E
offi
cers
trai
ned
Repo
rt
Esta
blish
/str
engt
hen
and
mee
tings
of f
eder
al a
nd
regi
onal
HIV
M a
nd E
Tec
hnic
al
Wor
king
Gro
ups
Cond
uct T
WG
mee
ting
will
be
cond
ucte
d in
al
l reg
ions
Regi
ons w
ith fu
nctio
nal
TWG
Min
utes
RHAP
CO/R
HB
Esta
blish
/str
engt
hen
and
cond
uct f
eder
al a
nd re
gion
al
HIV
M a
nd E
adv
isory
com
mitt
ee
mee
tings
FHAP
CO a
nd A
ll re
gion
s will
con
duct
Re
gula
r mee
tings
of
M a
nd E
adv
isory
Co
mm
ittee
Num
ber o
f reg
ions
co
nduc
ting
M a
nd E
Ad
viso
ry C
omm
ittee
m
eetin
gs re
gula
rly
Repo
rts,
Min
utes
of
the
mee
ting
HAP
CO
Inst
itute
cul
ture
of
evi
denc
e ba
sed
info
rmed
dec
ision
m
akin
g
Ensu
re o
ne n
atio
nal M
and
E
syst
emO
ne fu
nctio
nal M
an
d E
syst
em w
ill b
e es
tabl
ished
One
M a
nd E
syst
em
info
rmat
ion
Repo
rts,
site
visit
sPr
ocee
ding
repo
rts
Key
stra
tegi
c se
ctor
s, H
APCO
, MoH
H
APCO
cont
inue
d...

68
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsVe
rific
atio
n Le
ad A
genc
yIn
stitu
te c
ultu
re
of e
vide
nce
base
d in
form
ed d
ecisi
on
mak
ing
Esta
blish
fram
ewor
k fo
r ge
nera
tion
and
utili
zatio
n of
st
rate
gic
info
rmat
ion
Fram
ewor
k fo
r ge
nera
tion
& us
e of
st
rate
gic
info
rmat
ion
will
be
esta
blish
ed
Doc
umen
t dev
elop
ed
on fr
amew
ork
for
gene
ratio
n &
use
of
stra
tegi
c in
form
atio
n
Repo
rts,
site
visit
sPr
ocee
ding
repo
rts
Key
stra
tegi
c se
ctor
s, H
APCO
, MoH
H
APCO
Enfo
rce
evid
ence
d ba
sed
plan
ning
and
prio
ritiz
atio
nAl
l reg
ions
, sec
tors
, CS
Os w
ill p
repa
re
plan
s and
prio
ritiz
e ac
tiviti
es b
ased
on
curr
ent i
nfor
mat
ion
Num
ber o
f reg
ions
, se
ctor
s, CS
Os t
hat
use
info
rmat
ion
for p
lann
ing
and
prio
ritiz
atio
n
Surv
eys,
Site
visi
tsKe
y st
rate
gic
sect
ors,
HAP
CO, M
oHH
APCO
Cond
uct r
egul
ar re
view
of H
IV
prog
ram
s per
form
ance
40 re
gula
r rev
iew
of
HIV
Pro
gram
s pe
rform
ance
at
Fede
ral l
evel
Num
ber o
f Rev
iew
of
HIV
Pro
gram
s pe
rform
ance
Repo
rts,
site
visit
s Pr
ocee
ding
repo
rts
Key
stra
tegi
c se
ctor
s, H
APCO
, MoH
H
APCO
Esta
blish
men
t of d
atab
ase
One
dat
abas
e es
tabl
ished
Esta
blish
ed d
atab
ase
syst
emCo
nduc
t adv
ocac
y w
orks
hop
on M
and
E a
nd S
trat
egic
In
form
atio
n at
all
leve
l
24 a
dvoc
acy
wor
ksho
ps w
ill b
e co
nduc
ted
at a
ll le
vels
on M
and
E a
nd
Stra
tegi
c In
form
atio
n
Num
ber o
f wor
ksho
ps
cond
ucte
d Re
port
s, pr
ocee
ding
sH
APCO
Wor
k w
ith se
ctor
s to
incl
ude
HIV
/AID
S in
dica
tors
with
in th
eir
own
M a
nd E
syst
ems
All s
ecto
rs w
ill in
clud
e H
IV/A
IDS
indi
cato
rs
with
in th
eir o
wn
M
and
E sy
stem
s
Num
ber s
ecto
rs
incl
uded
HIV
/AID
S in
dica
tors
in th
eir
own
M a
nd E
syst
ems
surv
eilla
nce
Repo
rts,
repo
rts
FHAP
CO/
RHAP
COs/
RHBs
Stre
ngth
en
timel
y ge
nera
tion
of st
rate
gic
info
rmat
ion
Cond
uct H
IV su
rvei
llanc
e 5
HIV
surv
eilla
nce
stud
ies c
ondu
cted
N
umbe
r of S
urve
illan
ce
stud
ies c
ondu
cted
Su
rvei
llanc
e re
sults
Se
ctor
s, EH
NRI
Cond
uct e
ffect
iven
ess s
tudy
on
inte
rven
tions
Inte
rven
tion
Effec
tiven
ess s
tudi
es
will
be
cond
ucte
d
Effec
tiven
ess s
tudi
es
com
plet
edSt
udy,
Rep
orts
and
su
perv
ision
EHN
RI, S
ecto
rs
Iden
tify
prio
rity
rese
arch
ag
enda
s and
con
duct
re
sear
ches
Rese
arch
es o
n pr
iorit
y ar
ea c
ondu
cted
Pr
oduc
ed re
sear
ch
resu
ltsRe
sear
ches
con
duct
ed
FHAP
CO/
FMO
H/
Uni
vers
ities
Allo
cate
5-1
0% o
f the
SPM
fin
anci
ng to
stre
ngth
en
stra
tegi
c in
form
atio
n ge
nera
tion
5-10
% 0
f the
SPM
fin
anci
ng w
ill b
e al
loca
ted
for M
and
E
Allo
cate
d bu
dget
for M
an
d Es
Repo
rts,
site
visit
s U
nive
rsiti
es
cont
inue
d...

2010/11-2014/15
69
Sele
cted
Str
ateg
ies
Inte
rven
tions
Targ
ets
Key
Indi
cato
rsVe
rific
atio
n Le
ad A
genc
ySt
reng
then
tim
ely
gene
ratio
n of
stra
tegi
c in
form
atio
n
Dev
elop
and
impl
emen
t co
mm
unity
bas
ed in
form
atio
n sy
stem
to b
e us
ed a
t all
leve
ls
Com
mun
ity
Info
rmat
ion
syst
em
will
be
deve
lope
d an
d im
plem
ente
d
Dev
elop
ed a
nd
impl
emen
ted
Com
mun
ity
Info
rmat
ion
syst
em
Doc
umen
ts, S
urve
ys,
Site
visi
tsH
APCO
Diss
emin
ate
rese
arch
and
ev
alua
tion
findi
ngs r
egul
arly
1
BSS,
2 A
NC,
po
pula
tion
base
d su
rvey
, blo
od d
onor
s su
rvey
, dru
g re
sista
nce
surv
ey re
sults
di
ssem
inat
ed
Beha
viou
ral,
biol
ogic
al &
pro
gram
eff
ectiv
enes
s stu
dies
re
leas
ed a
t nat
iona
l &
sub-
natio
nal l
evel
s
Repo
rts
HAP
COs,
CSO
s
Enha
nce
diss
emin
atio
n an
d ut
iliza
tion
of st
rate
gic
info
rmat
ion
Prep
are,
prin
t and
dist
ribut
e H
IV/A
IDS
M a
nd E
repo
rts
regu
larly
Five
Ann
ual r
epor
t an
d fiv
e bi
ann
ual
repo
rts a
nd U
NG
ASS
repo
rt p
rinte
d an
d di
strib
uted
Num
ber o
f rep
orts
pr
epar
ed a
nd
dist
ribut
ed
Repo
rts H
APCO
/ EH
NRI
HAP
CO
HAP
CO/E
HN
RI
Prep
are
key
HIV
eva
luat
ion
and
rese
arch
find
ings
sum
mar
y an
d po
st re
port
s on
web
site
s
20 k
ey H
IV e
valu
atio
n an
d re
sear
ch fi
ndin
gs
sum
mar
ized
and
po
sted
repo
rts o
n w
eb
sites
Num
ber o
f key
HIV
ev
alua
tion
and
rese
arch
fin
ding
s sum
mar
y an
d po
sted
repo
rts o
n w
eb
sites
O
rgan
ize
inte
rnat
iona
l HIV
/AID
S re
late
d co
nfer
ence
s suc
h as
IC
ASA
2011
ICAS
A 20
11 w
ill b
e eff
ectiv
ely
orga
nize
d an
d co
nduc
ted
ICAS
A m
eetin
g co
nduc
ted
Cond
uct b
est p
ract
ice
docu
men
tatio
n &
diss
emin
atio
n20
Bes
t pra
ctic
es
docu
men
ted
& di
ssem
inat
ed
Num
ber o
f bes
t pr
actic
e do
cum
ente
d an
d di
strib
uted
Doc
umen
t, re
port
sH
APCO

Implementation Modality and Institutional Arrangements
Part Five

2010/11-2014/15
71
5.1. Multisectoral HIV/AIDS response governing and coordinating bodies HIV/AIDS councils and management boards will govern the multisectoral HIV/AIDS response at their respective levels. The councils at all levels will be composed of government, private, non-governmental, religious and civic society representatives and people living with HIV. The duties of the councils and management boards at all levels will be stipulated by the legislations of the respective governments. The Minister of Health and health officials at regional & sub-regional levels will be chairpersons of the management boards.
HIV/AIDS prevention and control offices at all levels will coordinate the multisectoral response. The House of Representatives at each level will oversight and enforce multisectoral response to HIV/AIDS to ensure effective mainstreaming, responsiveness and accountability.
5.2. Implementation of the multisectoral HIV/AIDS responseMultisectoral response to HIV/AIDS will be implemented in a decentralized and synchronized manner. Implementing bodies at Federal level will focus on capacity building, coordination, resource mobilization and monitoring evaluation. They will also develop and provide directives such as policy, strategy, guidelines, and frameworks while implementers at Regional level will further cascade these efforts to facilitate implementation of the multisectoral response at Woredas in a planned and organized manner.
Part Five: ImplementationModalityandInstitutionalArrangements

Monitoring and Evaluation
Part Six

2010/11-2014/15
73
Monitoring and Evaluation of HIV/AIDS multisectoral response will focus on tracking the progress on attaining results. A multisectoral HIV/AIDS monitoring and evaluation system will be strengthened to improve program performance. During SPM II, a community information system will be established and strengthened to track the progress of the non-health response. Outcomes and impacts of the multisectoral response will be monitored and evaluated by conducting surveillances, surveys, and studies. Emphasis will be given to monitor the epidemic trends and driving behavioral, socio-cultural and socio-economic factors to match the response to the epidemic. Moreover, appropriate indicators will be selected with clear targets for each thematic area for whole period of SPM II and annually.
A multisectoral response monitoring and evaluation plan will be developed and implemented through joint efforts in a coordinated manner, in line with the principle of “three ones”. Federal HAPCO, in collaboration with federal level stakeholders, is responsible for the coordination of the multi-sectoral monitoring and evaluation, and will convene semi-annual and annual joint review meetings and conduct semi-annual and annual joint support supervision at national level. Similarly, regional and sub-regional HAPCOs will coordinate the multisectoral M and E in their respective administrative levels. They will conduct quarterly support supervision, semi-annual and annual joint review meetings. A mid-term review and final evaluation of SPM II will also be conducted.
Data collection and reporting formats will be harmonized to facilitate data summarization and analysis. A multisectoral response database will be established at the federal and regional levels to enhance data storage and retrieval. Information dissemination will be strengthened through web postings, report publications and review meetings.
Part Six:MonitoringandEvaluation

Note


76
Strategic Plan II for Intensifying Multisectoral HIV and AIDS Response in Ethiopia