Embed Size (px)
Citation preview

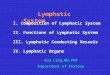
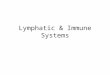
StomachStomach






Blood supplyBlood supply


Lymphatic D1Lymphatic D1
1
2
3
4
5
6

Lymphatic D2Lymphatic D2
78 9
1011









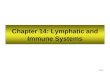
Peptic ulcerPeptic ulcer

Peptic ulcerPeptic ulcerHelicobacter pyloriHelicobacter pylori
H. PyloriH. Pylori is gram-negative spiral flagellated bacterium is gram-negative spiral flagellated bacterium Important in the etiology of peptic ulcers and gastric Important in the etiology of peptic ulcers and gastric cancer cancer Found in: Found in: – 90% patients with duodenal ulceration 90% patients with duodenal ulceration – 70% patients with gastric ulceration 70% patients with gastric ulceration – 60% patients with gastric cancer 60% patients with gastric cancer
H pylori Is located beneath the mucus layer, and H pylori Is located beneath the mucus layer, and produce various enzymes and toxinsproduce various enzymes and toxins– Endo-peptidaseEndo-peptidase that causes mucolysis that causes mucolysis – Large amounts of NH3, from ureaLarge amounts of NH3, from urea, that changes the surface pH, , that changes the surface pH,
and cellular permeability leading to back diffusion of HCL, and and cellular permeability leading to back diffusion of HCL, and also increasing serum gastrin productionalso increasing serum gastrin production
– Vacuolizing toxinVacuolizing toxin, and less importantly , and less importantly hemolysin toxinhemolysin toxin

Peptic ulcerPeptic ulcer
Helicobacter pylori (Helicobacter pylori (Investigation)Investigation)The organism can be detected by The organism can be detected by – Microscopy Microscopy – silver or Giemsa staining of antral – silver or Giemsa staining of antral
biopsies biopsies – Culture Culture – difficult and requires special culture – difficult and requires special culture
techniques techniques – Rapid urease testRapid urease test – color changes due to change in – color changes due to change in
pH pH – 13C or 14C breath test13C or 14C breath test – Ingested radioactive urea is – Ingested radioactive urea is
broken down to carbon dioxide broken down to carbon dioxide – Serology – detected immunologically using an ELISASerology – detected immunologically using an ELISA

Peptic ulcerPeptic ulcerAspirin and NSAIDSAspirin and NSAIDS. . – NSAIDs are pathogenic through their inhibition of the NSAIDs are pathogenic through their inhibition of the
cyclooxygenase-1 (COX-1) pathway, which normally cyclooxygenase-1 (COX-1) pathway, which normally produces protective prostaglandins. produces protective prostaglandins.
– Recently, the potential for decreased GI mucosal Recently, the potential for decreased GI mucosal injury with newer cyclooxygenase-2 (COX-2) selective injury with newer cyclooxygenase-2 (COX-2) selective inhibitors, celecoxib and rofecoxib, has been inhibitors, celecoxib and rofecoxib, has been emphasized. emphasized.
– These newer NSAIDs do not inhibit COX-1 and, These newer NSAIDs do not inhibit COX-1 and, therefore, do not have the disadvantage of reducing therefore, do not have the disadvantage of reducing the synthesis of protective prostaglandins.the synthesis of protective prostaglandins.
Lifestyle factors influencing development of DULifestyle factors influencing development of DU. . Increased consumption of alcohol, smoking, Increased consumption of alcohol, smoking, coffee and cola coffee and cola

Duodenal ulcerDuodenal ulcer
Hyperacidity
Defective mucosal barrier
Predisposing factorsHelicobacter pylori

Clinical pictureClinical picture
Age incidence 25- 50Age incidence 25- 50
Remitting disease with seasonal exacerbationsRemitting disease with seasonal exacerbations
Typically epigastric pain when the stomach is Typically epigastric pain when the stomach is empty, and awaken the patient from sleepempty, and awaken the patient from sleep
Back radiation indicates pancreatic penetrationBack radiation indicates pancreatic penetration
Vomiting without obstruction is rare and due to Vomiting without obstruction is rare and due to exacerbationexacerbation
Bleeding is either minor, and intermittent (pallor) Bleeding is either minor, and intermittent (pallor) or severe (hematemesis and melena) or severe (hematemesis and melena)


Gastric ulcerGastric ulcerDefective mucosal barrier dt decrease• secretion• Pg• BS• Pyloric function


Gastric ulcerGastric ulcer

Healing ulcerHealing ulcer

Pre pyloric gastric ulcerPre pyloric gastric ulcer

Clinical pictureClinical picture
Less commonLess commonTwo types, Two types, – type I (at incisura angularis)type I (at incisura angularis)– type II pyloric channel ulcer (NB prepyloric ulcer is like DU in all type II pyloric channel ulcer (NB prepyloric ulcer is like DU in all
aspects)aspects)
Type I affects middle aged and elderly patientsType I affects middle aged and elderly patientsIt is associated with hypo acidity and may come on top of It is associated with hypo acidity and may come on top of atrophic gastritisatrophic gastritisPain is induced by meals (more as discomfort)Pain is induced by meals (more as discomfort)Vomiting and nausea are commonVomiting and nausea are commonMay present also with complications (perforation, May present also with complications (perforation, obstruction or bleeding)obstruction or bleeding)

InvestigationsInvestigations
EndoscopyEndoscopy– To see the ulcer, To see the ulcer, – to take biopsy (gastric ulcers) to test for H pylori, and to take biopsy (gastric ulcers) to test for H pylori, and – to follow up treatment and healing to follow up treatment and healing
Double contrast or simple barium mealDouble contrast or simple barium meal – To delineate anatomy, the most important signs of To delineate anatomy, the most important signs of
duodenal ulcerations are deformities (linear or duodenal ulcerations are deformities (linear or trifoliate) and ulcer niche or craterstrifoliate) and ulcer niche or craters
– To detect lesions that may make endoscopy To detect lesions that may make endoscopy dangerous dangerous




Medical treatmentMedical treatmentPPI (proton pump inhibitorsPPI (proton pump inhibitors) are the most useful ) are the most useful drugsdrugsH2 blockersH2 blockers comes as number two with less cost comes as number two with less cost in long term treatment, but higher recurrence ratein long term treatment, but higher recurrence rateSucralfate, and bismuthSucralfate, and bismuth are locally acting drugs are locally acting drugs used as adjuvant to previous medications (not used as adjuvant to previous medications (not with PPI since it needs to react with HCL to form with PPI since it needs to react with HCL to form the coating membrane)the coating membrane)For H.pylori eradicationFor H.pylori eradication – three drug regimen can be used (bismuth, three drug regimen can be used (bismuth,
metronidazole, and amoxycillin) or metronidazole, and amoxycillin) or – two drug regimen (PPI &clarithromycin). two drug regimen (PPI &clarithromycin). – H pylori eradication can prevent recurrenceH pylori eradication can prevent recurrence

Surgery for peptic ulcerSurgery for peptic ulcer
Indications for surgeryIndications for surgery
Non compliance to medical treatmentNon compliance to medical treatment
Resistant DUResistant DU
GU persistent >3 months despite medical GU persistent >3 months despite medical treatment irrespective of complicationstreatment irrespective of complications
Onset of complicationsOnset of complications

Options of surgical treatment for Options of surgical treatment for DUDU
Truncal vagotomy and drainage (either Truncal vagotomy and drainage (either pyloroplasty or gastrojujenostomy)pyloroplasty or gastrojujenostomy)– Very commonly used operation, Very commonly used operation, – although the side effects are numerous,and although the side effects are numerous,and
the recurrence rate is high. the recurrence rate is high. – Used commonly for its simplicity, and less Used commonly for its simplicity, and less
surgical complications. surgical complications.

Options of surgical treatment for Options of surgical treatment for DUDU
Truncal vagotomy and anterectomyTruncal vagotomy and anterectomy– Is the operation with the least recurrence rate, Is the operation with the least recurrence rate,
and best option for pyloric channel ulcers and best option for pyloric channel ulcers – Is used as the ultimate goal for all recurrent Is used as the ultimate goal for all recurrent
ulcers after surgeryulcers after surgery– Unfortunately associated with the side effects Unfortunately associated with the side effects
of both vagotomy and resection surgeryof both vagotomy and resection surgery

Options of surgical treatment for Options of surgical treatment for DUDU
Highly selective vagotomyHighly selective vagotomy– Is the most physiologic and least side effects.Is the most physiologic and least side effects.– High recurrence rate is due to surgeon’s abilities, and High recurrence rate is due to surgeon’s abilities, and
is proportional to the completeness of the technique.is proportional to the completeness of the technique.– Not used with the presence of obstruction, and Not used with the presence of obstruction, and
prepyloric ulcers.prepyloric ulcers.– Two modifications described Two modifications described
where the posterior vagus is cut at the trunk with anterior where the posterior vagus is cut at the trunk with anterior seromyotomy (Taylor) or seromyotomy (Taylor) or
anterior HSV (Hill)anterior HSV (Hill)



Super selective vagotomySuper selective vagotomy




Surgical options for GUSurgical options for GU
Standard treatment for GU is partial gastrectomy Standard treatment for GU is partial gastrectomy with with Billroth I operationBillroth I operation (resection includes the (resection includes the lesser curve, the ulcer and antrum with lesser curve, the ulcer and antrum with gastroduodenal ananstomosis). gastroduodenal ananstomosis). Sometimes BII (gatrojujenostomy is used to Sometimes BII (gatrojujenostomy is used to reestablish the anastomosis.reestablish the anastomosis.HSV +excision of the ulcer is an alternative with HSV +excision of the ulcer is an alternative with less side effects but high recurrence rate .It is less side effects but high recurrence rate .It is the best for the rare high GU located just the best for the rare high GU located just beneath the cardiabeneath the cardia

Gastric ulcer excisionGastric ulcer excision


Side effects of gastric surgery Side effects of gastric surgery and vagotomyand vagotomy
1.1. Early dumpingEarly dumping2.2. Late dumping (reactive hypoglycemia)Late dumping (reactive hypoglycemia)3.3. Bile vomiting Bile vomiting 4.4. Diarrhea Diarrhea 5.5. Recurrence Recurrence 6.6. Enterogastric refluxEnterogastric reflux7.7. Gastroesophageal refluxGastroesophageal reflux8.8. Mechanical loops obstruction & intussusceptionMechanical loops obstruction & intussusception9.9. Nutritional complications Nutritional complications
– Weight lossWeight loss– Anemia Anemia – Bone diseaseBone disease– Small stomach syndromeSmall stomach syndrome

Dumping due to hypovolemia Dumping due to hypovolemia due to rapid gastric emptying due to rapid gastric emptying This will include This will include vasomotor systemic vasomotor systemic manifestationsmanifestations and and gastrointestinal gastrointestinal manifestationsmanifestations (after 30 -60 minutes) (after 30 -60 minutes) The vasomotor manifestations are partially due The vasomotor manifestations are partially due to to hypo-volemiahypo-volemia initiated by initiated by – the rapid gastric emptying of hypertonic food into the the rapid gastric emptying of hypertonic food into the
small bowel where much fluids are poured on it to small bowel where much fluids are poured on it to create isotonicity,create isotonicity,
– partially to the release of various vasomotor partially to the release of various vasomotor mediators initiated by the sudden confrontation of the mediators initiated by the sudden confrontation of the small bowel with hypertonic food stuff. small bowel with hypertonic food stuff.

Late Dumping (Reactive Late Dumping (Reactive hypoglycemia)hypoglycemia)
2-3 hours after meals due to increased 2-3 hours after meals due to increased release of insulin, which is again due to release of insulin, which is again due to rapid gastric evacuation of hypertonic rapid gastric evacuation of hypertonic foodstuff into the small bowelfoodstuff into the small bowelThis causing too much insulin, release This causing too much insulin, release which lag behind causing hypoglycemia. which lag behind causing hypoglycemia. This is usually associated with dumping This is usually associated with dumping and diarrhea and diarrhea

Bile vomiting Bile vomiting
Occurs early in the morning Occurs early in the morning
It is usually associated with severe It is usually associated with severe nausea and also after meals and nausea and also after meals and
It is due to low reflux or due to It is due to low reflux or due to intermittent afferent loop obstruction.intermittent afferent loop obstruction.

Diarrhea Diarrhea Usually accompanied by dumping, and initiated Usually accompanied by dumping, and initiated by foodby foodIt can be in the form ofIt can be in the form of– Frequent loose stools Frequent loose stools – Intermittent episodes of short-lived diarrhea Intermittent episodes of short-lived diarrhea – Explosive diarrhea with disabilityExplosive diarrhea with disability
May be due toMay be due to– Rapid gastric emptyingRapid gastric emptying– Fat malabosrptionFat malabosrption– Bacterial overgrowth due to decreased HCL and Bacterial overgrowth due to decreased HCL and
presence of blind loop presence of blind loop – Denervation of the gut (accelerated small bowel Denervation of the gut (accelerated small bowel
transit time transit time

RefluxRefluxEnterogastric reflux (low reflux)Enterogastric reflux (low reflux)– Causes severe erosive gastritis Causes severe erosive gastritis – Pain, nausea, vomiting, bile vomiting early in the Pain, nausea, vomiting, bile vomiting early in the
morning and early postprandialmorning and early postprandial– Pallor is due to chronic blood lossPallor is due to chronic blood loss– Prolonged gastritis will lead to atrophic gastritis, Prolonged gastritis will lead to atrophic gastritis,
intestinal metaplasia with predisposition to cancer intestinal metaplasia with predisposition to cancer
GERD (high reflux)GERD (high reflux)– Vagotomy per se does not initiate GERDVagotomy per se does not initiate GERD– Destruction of the phrenoesophageal ligaments may Destruction of the phrenoesophageal ligaments may
initiate GERDinitiate GERD– If there is bile gastritis, the refluxate will be extremely If there is bile gastritis, the refluxate will be extremely
injurious to the esophagus (BE)injurious to the esophagus (BE)

Nutritional side effectsNutritional side effectsWeight lossWeight loss– Diminished food intake (small stomach syndrome)Diminished food intake (small stomach syndrome)– Fat malabsorptionFat malabsorption– Dumping and diarrheaDumping and diarrhea
Anemia Anemia – Iron deficiency due malabsorption of iron due to lack of HCL and Iron deficiency due malabsorption of iron due to lack of HCL and
pepsinpepsin– Chronic blood loss in biliray gastritis Chronic blood loss in biliray gastritis – Macrocytic anemia due to B12 deficiency due to loss of intrinsic Macrocytic anemia due to B12 deficiency due to loss of intrinsic
factor and loss of HCL, also bacterial overgrowth can induce factor and loss of HCL, also bacterial overgrowth can induce B12 DB12 D
Bone diseaseBone disease– The exclusion of the duodenum, which is the main site of Ca The exclusion of the duodenum, which is the main site of Ca
absorption, is the cause absorption, is the cause – Also loss of HCL that helps Ca absorptionAlso loss of HCL that helps Ca absorption– It occurs many years after operation It occurs many years after operation

Mechanical side effectsMechanical side effects
Afferent loop obstructionAfferent loop obstruction– Predisposed to by long loops and antecolic Predisposed to by long loops and antecolic
anastomosis anastomosis – Kinking and adhesionsKinking and adhesions– Volvulus Volvulus – Internal herniationInternal herniation– Jejunogastric intussusceptionsJejunogastric intussusceptions

Other side effects Other side effects
Gall stonesGall stones due to vagotomy due to vagotomy
Cancer in gastric remnant due to Cancer in gastric remnant due to decreased HCL, bacterial overgrowth, and decreased HCL, bacterial overgrowth, and biliary gastritis that lead to intestinal biliary gastritis that lead to intestinal metaplasia metaplasia
Bezoars,Bezoars, of vegetable and fruit remnants of vegetable and fruit remnants due to loss of HCL and pyloric mill functiondue to loss of HCL and pyloric mill function

Recurrence rates after different Recurrence rates after different operationsoperations
Causes of recurrent ulcerationCauses of recurrent ulcerationIncomplete vagotomyIncomplete vagotomyG cell hyperplasia G cell hyperplasia Antral exclusionAntral exclusionInadequate subtotal gastrectomyInadequate subtotal gastrectomyHypercalcemia Hypercalcemia Zollinger Ellison syndrome (gastrinoma)Zollinger Ellison syndrome (gastrinoma)


Steps of management Steps of management
Start with endoscopy and barium studies Start with endoscopy and barium studies Since there is no superior method of vagal integrity Since there is no superior method of vagal integrity testing attempt accurate measurement of gastric acid testing attempt accurate measurement of gastric acid secretion in both basal and stimulated status secretion in both basal and stimulated status – BAO>2 mEq/h indicates BAO>2 mEq/h indicates inadequate vagotomyinadequate vagotomy– BAO>4 mEq/h indicates BAO>4 mEq/h indicates recurrent ulcerationrecurrent ulceration– MAO>15 mEq/h strongly MAO>15 mEq/h strongly supports the diagnosis of recurrent supports the diagnosis of recurrent
ulcer ulcer – BAO=MAO BAO=MAO indicates Zollinger Ellison or other hypersecretoryindicates Zollinger Ellison or other hypersecretory
conditions like retained antrumconditions like retained antrum
Serum gastrinSerum gastrin is characteristically responsive by is characteristically responsive by increase in ZE after secretin or calcium infusionincrease in ZE after secretin or calcium infusion



Upper GIT bleedingUpper GIT bleeding
Causes Causes Esophageal or gastric varices (almost 80% in Esophageal or gastric varices (almost 80% in our country)our country)Gastric erosionsGastric erosionsPeptic ulcer Peptic ulcer Gastric neoplasiaGastric neoplasiaMallory-Weiss tearMallory-Weiss tearReflux esophagitis Reflux esophagitis Dieulafoy malformation Dieulafoy malformation

Upper GIT bleeding Upper GIT bleeding (Management)(Management)
Start withStart with resuscitation resuscitation – I.V. lines to get blood sample for cross I.V. lines to get blood sample for cross
matching and install replenishment fluids matching and install replenishment fluids (colloids and crystalloids)(colloids and crystalloids)
– Monitor pulse and blood pressure, a central Monitor pulse and blood pressure, a central venous line for CVP is optionalvenous line for CVP is optional
– Best bedside monitor for tissue perfusion is Best bedside monitor for tissue perfusion is urinary output (insert a catheter)urinary output (insert a catheter)

Upper GIT bleeding Upper GIT bleeding (Management)(Management)
Synchronously start to lavageSynchronously start to lavage the stomach to the stomach to prepare for prepare for
Diagnostic endoscopyDiagnostic endoscopy (corner stone of (corner stone of management). Endoscopy can correctlymanagement). Endoscopy can correctly
determine the site and cause of bleeding in over 90% determine the site and cause of bleeding in over 90% of patients. of patients.
An ulcer should be accepted as the bleeding source An ulcer should be accepted as the bleeding source only if it has one of the stigmata of active or recent only if it has one of the stigmata of active or recent hemorrhage. hemorrhage.
The signs of recent hemorrhage include an The signs of recent hemorrhage include an adherent clot without oozing, adherent clot without oozing,
an adherent slough within the ulcer base, oran adherent slough within the ulcer base, or
a visible vessel within the ulcer.a visible vessel within the ulcer.



Upper GIT bleeding Upper GIT bleeding (Management)(Management)
The nasogastric tubeThe nasogastric tube is a good bleeding is a good bleeding monitormonitor until endoscopy is done until endoscopy is done
Endoscopic therapyEndoscopic therapy– Laser photocoagulation using the Nd-YAG Laser photocoagulation using the Nd-YAG
laser laser – Bipolar diathermy Bipolar diathermy – Heat probes Heat probes – Adrenaline or sclerosant injection Adrenaline or sclerosant injection – No technique is superior No technique is superior

Upper GIT bleeding Upper GIT bleeding (Management)(Management)
Management specific for ulcersManagement specific for ulcers
Drugs usedDrugs used– Sucralfate given via the nasogastric tubeSucralfate given via the nasogastric tube is for is for
stress acute ulcerations onlystress acute ulcerations only– H2 blockers and omeprazoleH2 blockers and omeprazole are used to are used to
prevent rebleeding with doubtful efficiencyprevent rebleeding with doubtful efficiency– Somatostatin infusionsSomatostatin infusions are of little help except are of little help except
if used with HCL supressor drugsif used with HCL supressor drugs– Tranexamic acid (antifibrinolytic agent)Tranexamic acid (antifibrinolytic agent) is is
proved to be efficient in reducing the rate of proved to be efficient in reducing the rate of rebleeding and need for surgeryrebleeding and need for surgery

Upper GIT bleeding Upper GIT bleeding (Management)(Management)
Indications of surgeryIndications of surgery
Endoscopic findingsEndoscopic findings– Arterial spurter &visible vesselArterial spurter &visible vessel– The presence of a clot attached is equivocal The presence of a clot attached is equivocal
signsign
Bleeding criteriaBleeding criteria – Continued bleedingContinued bleeding– Recurrent bleedingRecurrent bleeding– 4 units after the initial resuscitation especially 4 units after the initial resuscitation especially
in an elderly patient in an elderly patient

Upper GIT bleeding Upper GIT bleeding (Management)(Management)
For DUFor DU
the pylorus and duodenum are incised the pylorus and duodenum are incised longitudinally and longitudinally and
the vessel is undermined or the ulcer the vessel is undermined or the ulcer excised and excised and
the closure is transverse as in pyloroplasty, the closure is transverse as in pyloroplasty,
usually with addition of TV specially if the usually with addition of TV specially if the general condition permits.general condition permits.

Upper GIT bleeding Upper GIT bleeding (Management)(Management)
For GU: For GU: partial gastrectomypartial gastrectomy. .
A bleeding gastric ulcer is most commonly A bleeding gastric ulcer is most commonly managed by a managed by a distal gastrectomydistal gastrectomy that that includes the ulcer includes the ulcer
with a gastro-duoden-ostomy or with a gastro-duoden-ostomy or
a gastro-jejun-ostomy reconstruction.a gastro-jejun-ostomy reconstruction.

Gastric outlet obstructionGastric outlet obstruction

Gastric outlet obstructionGastric outlet obstructionThe most important causes of gastric outlet obstruction are The most important causes of gastric outlet obstruction are 1.1. the stricture caused by the stricture caused by scatrized duodenal ulcerscatrized duodenal ulcer, and , and 2.2. malignancy of the stomachmalignancy of the stomach involving the pyloric antrum. involving the pyloric antrum. 3.3. The third common cause is congenital The third common cause is congenital hypertrophic hypertrophic
pyloric stenosis.pyloric stenosis.4.4. A very common malignant cause is A very common malignant cause is pancreatic cancerpancreatic cancer
which in fact obstructs the duodenum. which in fact obstructs the duodenum. 5.5. Less important cuasesLess important cuases are: are:
– Adult pyloric hypertrophyAdult pyloric hypertrophy– Mucosal diaphragm Mucosal diaphragm – MegaduodenumMegaduodenum– Annular pancreasAnnular pancreas– Duodenal hematomaDuodenal hematoma– Arteriomesenteric compression (Wilkie’s disease Arteriomesenteric compression (Wilkie’s disease


Clinical pictureClinical picture
Ulcer pain becomes constantUlcer pain becomes constant, generalized , generalized and lose periodicityand lose periodicityVomitingVomiting is prominent, bile free, retained is prominent, bile free, retained foul odoured food residue foul odoured food residue ConstipationConstipationDehydration, loss of weightDehydration, loss of weight+Succusion splash+Succusion splash, and upper left , and upper left abdominal fullness, with possible visible abdominal fullness, with possible visible peristalsis (left to right)peristalsis (left to right)



Management Management Correct dehydration and electrolyte imbalanceCorrect dehydration and electrolyte imbalance– Use saline infusions with K supplementsUse saline infusions with K supplements– Monitor by frequent Na &K Monitor by frequent Na &K – Success is indicated by increase in urinary output and Success is indicated by increase in urinary output and
secreting alkaline urine secreting alkaline urine
Gastric lavageGastric lavage– Wide bored tube,Wide bored tube,– Use saline irrigationUse saline irrigation
SurgerySurgery– GastrojujenostomyGastrojujenostomy is ideal for bypassing the is ideal for bypassing the
obstruction, TV should be added obstruction, TV should be added – For gastric ulcers For gastric ulcers partial gastrectomypartial gastrectomy is again the is again the
solutionsolution

Perforated peptic ulcerPerforated peptic ulcer

Clinical pictureClinical picture
The moment of perforation is often The moment of perforation is often identified by the patient as an excruciating identified by the patient as an excruciating epigastric pain epigastric pain
Early there is no manifestations of shock Early there is no manifestations of shock (no hypovoleamia, no septicemia), (no hypovoleamia, no septicemia),
However, late variable degrees of However, late variable degrees of circulatory collapse may be present circulatory collapse may be present
Respiration is shallow and grunting due to Respiration is shallow and grunting due to severe abdominal rigidity severe abdominal rigidity

Clinical pictureClinical pictureThe abdomenThe abdomen is usually is usually – First,First, showing board like rigidity, tenderness and showing board like rigidity, tenderness and
rebound, with dead silent abdomen (chemical rebound, with dead silent abdomen (chemical peritonitisperitonitis
– however, this ameliorates in the however, this ameliorates in the lucid phaselucid phase by by dilution, and then the dilution, and then the
– third stagethird stage of septic peritonitis starts with toxemia and of septic peritonitis starts with toxemia and feverfever
Two common variations are causing conflictTwo common variations are causing conflict– Early sealing with less symptoms and signs Early sealing with less symptoms and signs – Leakage towards the right paracolic gutter causing Leakage towards the right paracolic gutter causing
signs and symptoms of appendicitissigns and symptoms of appendicitis

DiagnosisDiagnosisPlain standing abdomenPlain standing abdomen – Free air under the copulaFree air under the copula– (right side is more informative)(right side is more informative)– (higher and liver with no gastric air bubble)(higher and liver with no gastric air bubble)
CT scans of the abdomenCT scans of the abdomen: : – This modality can be a valuable investigative tool, This modality can be a valuable investigative tool,
providing differential morphologic information not providing differential morphologic information not obtainable with plain radiography or ultrasonography.obtainable with plain radiography or ultrasonography.
Gastrographin meal and follow throughGastrographin meal and follow through – In sealed perforations, or in minor gastric perforations In sealed perforations, or in minor gastric perforations
to differentiate from pancreatitis to differentiate from pancreatitis
Serum amylase should be doneSerum amylase should be done – It is a bit high in perforations, yet it is very high It is a bit high in perforations, yet it is very high
(around 1000 units) in pancreatitis (around 1000 units) in pancreatitis
Endoscopy is controversialEndoscopy is controversial

Management Management ResuscitationResuscitation– Nasogastric tube, Nasogastric tube, – I.V. fluids, I.V. fluids, – antibiotics, antibiotics, – PPI or H2 blockers and analgesics, PPI or H2 blockers and analgesics, – estimation of urinary outputestimation of urinary output
Operative interferenceOperative interference – Closure of the perforation (use of omental patch)Closure of the perforation (use of omental patch)– Peritoneal toilet (warm saline irrigation)Peritoneal toilet (warm saline irrigation)– Addition of a definitive operation (HSV for DU or PG Addition of a definitive operation (HSV for DU or PG
for GU) only if for GU) only if There is a long history of ulcer (chronic ulcersThere is a long history of ulcer (chronic ulcersEarly perforation (6 to 8 hours)Early perforation (6 to 8 hours)No much sepsis No much sepsis Previous or synchronous second ulcer complicationPrevious or synchronous second ulcer complication

PenetrationPenetrationPenetrated ulcer is that one that erodes Penetrated ulcer is that one that erodes the wall of the stomach or duodenum with the wall of the stomach or duodenum with sealing from surrounding visceral sealing from surrounding visceral structures with no loss of luminal contentsstructures with no loss of luminal contents
Sites of penetration:Sites of penetration:
– For DU: pancreas, biliary tree, colonFor DU: pancreas, biliary tree, colon
– For GU, gastrohepatic ligament, For GU, gastrohepatic ligament, mesocolon, liver, pancreasmesocolon, liver, pancreas


Clinical picture &ManagementClinical picture &Management
• Clinical pictureClinical pictureLoss of periodicity Loss of periodicity A new radiation of pain (to the back if pancreas is A new radiation of pain (to the back if pancreas is affected)affected)Manifestations of gastrocolic fistula Manifestations of gastrocolic fistula
Diarrhea with severe weight lossDiarrhea with severe weight lossPassage of undigested food Passage of undigested food Foul odoured breath and eructations and feculent vomiting Foul odoured breath and eructations and feculent vomiting
DiagnosisDiagnosis is by barium enema due to pressure is by barium enema due to pressure difference difference TreatmentTreatment is by the usual ways of treatment of is by the usual ways of treatment of non-complicated ulcers, with leaving the base of non-complicated ulcers, with leaving the base of the ulcer in the penetrated organ untouched the ulcer in the penetrated organ untouched

Cancer stomachCancer stomach

Cancer stomach (Etiology)Cancer stomach (Etiology)Dietary nitratesDietary nitrates: Bacteria in the stomach break down : Bacteria in the stomach break down nitrites to compounds (eg, nitrites to compounds (eg, NN-nitroso compounds) that -nitroso compounds) that are carcinogenic in animals. are carcinogenic in animals. Hypochlorhydria:Hypochlorhydria: This condition occurs in gastric atrophy This condition occurs in gastric atrophy and promotes bacterial colonization of the stomach. It and promotes bacterial colonization of the stomach. It leads to increased nitrite formation, which may have a leads to increased nitrite formation, which may have a mutagenic effect on the atrophic gastric mucosa. mutagenic effect on the atrophic gastric mucosa. Helicobacter pyloriHelicobacter pylori: Antral gastritis caused by : Antral gastritis caused by H pyloriH pylori has been lined to the development of gastric cancer. has been lined to the development of gastric cancer. Patients with Patients with H pylori gastritisH pylori gastritis are 3-6 times more likely are 3-6 times more likely to develop gastric cancer than individuals without the to develop gastric cancer than individuals without the infection. infection. Certain foodsCertain foods: Starch, pickled vegetables, salted fish and : Starch, pickled vegetables, salted fish and meat, smoked foods, and salt have all been implicated. meat, smoked foods, and salt have all been implicated.

Cancer stomach (Etiology)Cancer stomach (Etiology)
Cigarette smokingCigarette smoking: Those who smoke more than 30 : Those who smoke more than 30 cigarettes per day have a 5-fold increased risk of gastric cigarettes per day have a 5-fold increased risk of gastric carcinoma.carcinoma.Several precancerous conditions are recognized: Several precancerous conditions are recognized: – Chronic atrophic gastritis Chronic atrophic gastritis – Pernicious anemia Pernicious anemia – Previous partial gastrectomy Previous partial gastrectomy – Ménétrier disease Ménétrier disease – Gastric dysplasia Gastric dysplasia – Adenomatous polyps (20% of all gastric polyps) Adenomatous polyps (20% of all gastric polyps) – Hereditary factorsHereditary factors
Approximately 95% of all malignant gastric neoplasms Approximately 95% of all malignant gastric neoplasms are adenocarcinomas. The remaining tumors are are adenocarcinomas. The remaining tumors are lymphomas, leiomyosarcomas, carcinoids, or sarcomas. lymphomas, leiomyosarcomas, carcinoids, or sarcomas.

EtiologyEtiology (Lauren DIO (Lauren DIO classification)classification)
Diffuse gastric cancer (D) Diffuse gastric cancer (D) – Hereditary factors Hereditary factors – Proximal locatioProximal locatio– Younger, more femalesYounger, more females– No relation to intestinal metaplasia or No relation to intestinal metaplasia or
dysplasiadysplasia– Associated with pernicious anemia Associated with pernicious anemia

EtiologyEtiology (Lauren DIO (Lauren DIO classification)classification)
Intestinal type GC (I)Intestinal type GC (I)– Distally locatedDistally located– Older patients, more malesOlder patients, more males– Frequently endemic Frequently endemic – Associated with inflammatory changes Associated with inflammatory changes – Associated with H pylori infectionAssociated with H pylori infection– On top of dysplasia or intestinal metaplasia On top of dysplasia or intestinal metaplasia – On top of adenomatous polyps not hyperplastic On top of adenomatous polyps not hyperplastic
polyps (75%)polyps (75%)– On top of chronic gastritis (atrophic)On top of chronic gastritis (atrophic)
There is a mixed type (O type only 10%)There is a mixed type (O type only 10%)



Morphologic types of GCMorphologic types of GC
Morphologic types of early cancer Morphologic types of early cancer (Japanese endoscopic society JES) (Japanese endoscopic society JES) – (by definition the penetration of the tumor (by definition the penetration of the tumor
does not exceed the submucosa even if LN does not exceed the submucosa even if LN are positive )are positive )
Morphological classification of Morphological classification of advanced cancer stomach Borrmannadvanced cancer stomach Borrmann– ( ( by definition , the penetration of the tumor by definition , the penetration of the tumor
exceeds the submucosa even if LN are exceeds the submucosa even if LN are negative )negative )






Spread of cancer stomachSpread of cancer stomach
Direct extensionDirect extension– Ulcerative and polypoid type penetrates Ulcerative and polypoid type penetrates
through the wallthrough the wall– The scirrhous type spreads through the The scirrhous type spreads through the
submucosa and musculosa to encase the submucosa and musculosa to encase the stomacstomac
– Direct extension into the omenta, pancreas, Direct extension into the omenta, pancreas, diaphragm, transverse colon or mesocolon, diaphragm, transverse colon or mesocolon, and duodenum is common. and duodenum is common.

Spread of cancer stomachSpread of cancer stomach
Lymphatics Lymphatics – To perigastric LN To perigastric LN – To regional LN (along splenic, common hepatic left To regional LN (along splenic, common hepatic left
gastric and celiac arteries) gastric and celiac arteries) – Virschow (supraclavicular) or left axillary LN (Irish’s Virschow (supraclavicular) or left axillary LN (Irish’s
node)node)– Umbilical nodule (Sister Joseph nodule)Umbilical nodule (Sister Joseph nodule)
Blood borneBlood borne– Liver (40%), lung (40%)sclerotic bone metastasis Liver (40%), lung (40%)sclerotic bone metastasis
TranscelomicTranscelomic– Krukenberg (ovaries), Krukenberg (ovaries), – rectal wall (Blummer shelf) or peritoneumrectal wall (Blummer shelf) or peritoneum

Clinical pictureClinical picture
At the fundus and near the cardia At the fundus and near the cardia ( Esophegeal obstruction) The triad of ( Esophegeal obstruction) The triad of
dysphagia, dysphagia,
regurgitation, and regurgitation, and
chest infectionschest infections
At the pyloric antrum and sphincter At the pyloric antrum and sphincter (gastric outlet obstruction) The triad of (gastric outlet obstruction) The triad of
early satiety, early satiety,
vomiting of retained food, and vomiting of retained food, and
constipation and dehydrationconstipation and dehydration

Clinical pictureClinical pictureAt the midzone away from sphincters At the midzone away from sphincters – Recent dyspepsia in an old male (anorexia Recent dyspepsia in an old male (anorexia
&early satiety &distaste for meat)&early satiety &distaste for meat)– Dyspepsia above 40Dyspepsia above 40– Change nature of dyspepsiaChange nature of dyspepsia
3 A syndrome3 A syndrome– Unexplained anemia Unexplained anemia – AnorexiaAnorexia– Athena Athena
Pain (60%), weight loss (50%) vomiting Pain (60%), weight loss (50%) vomiting (40%) and mass (30%)(40%) and mass (30%)

Diagnostic studiesDiagnostic studiesEndoscopy Endoscopy – With biopsy or exfoliative cytology or brush With biopsy or exfoliative cytology or brush
biopsy to detect >95% of lesions (biopsy biopsy to detect >95% of lesions (biopsy alone is valid in 80% only)alone is valid in 80% only)
Barium mealBarium meal– The barium meal findings in case of gastric The barium meal findings in case of gastric
cancer depends on cancer depends on the location of the tumor, and also the location of the tumor, and also
on the Bormmann type of gross pathologyon the Bormmann type of gross pathology

Diagnostic studiesDiagnostic studiesA filling defectA filling defect in case of the presence of in case of the presence of nodular, polypoidal or cauliflower mass located nodular, polypoidal or cauliflower mass located in the stomach away from the inlet or outletin the stomach away from the inlet or outletPyloric obstructionPyloric obstruction with the presence of an antral with the presence of an antral filling defect and mild gastric dilatation, or if filling defect and mild gastric dilatation, or if associated with linitis plastic (Borrmann IV) it will associated with linitis plastic (Borrmann IV) it will show a very small no dilated stomachshow a very small no dilated stomachPseudoachalasia of the cardia if the tumorPseudoachalasia of the cardia if the tumor is is located just below the cardia with submucous located just below the cardia with submucous infiltration upwards in the esophagus infiltration upwards in the esophagus An ulcer niche on top of a filling defectAn ulcer niche on top of a filling defect (inside (inside the boundaries of the stomach) usually due to the boundaries of the stomach) usually due to exophytic ulcer (Bormmann II) on he lesser exophytic ulcer (Bormmann II) on he lesser curve side curve side

Diagnostic studiesDiagnostic studiesCT abdomenCT abdomen – To assess the extent of the disease, To assess the extent of the disease, – depth of infiltration, LN, and depth of infiltration, LN, and – omental cakes and ascitesomental cakes and ascites
LaparoscopyLaparoscopy– New method to assess more accurately the New method to assess more accurately the
advancement of the disease specially concerning the advancement of the disease specially concerning the peritoneal deposits and mild ascitesperitoneal deposits and mild ascites
EUSEUS– 6 times more accurate than CT in assessing the stage 6 times more accurate than CT in assessing the stage
of the disease especially for cardiac lesionsof the disease especially for cardiac lesions








Staging of cancer stomachStaging of cancer stomach
According to TNM According to TNM
TumorTumor
T1 tumor limited to the mucosa and sub-T1 tumor limited to the mucosa and sub-mucosa mucosa
T2 tumor involves the muscularis properia T2 tumor involves the muscularis properia or subserosaor subserosa
T3 tumor penetrates the serosaT3 tumor penetrates the serosa
T4 tumor involves contiguous structures T4 tumor involves contiguous structures

Staging of cancer stomachStaging of cancer stomach
NodeNodeN0 no metastases to the regional lymph nodesN0 no metastases to the regional lymph nodesN1 involvement of the perigastric lymph nodes N1 involvement of the perigastric lymph nodes – within 3 cm of the primary tumor or within 3 cm of the primary tumor or – from 1 to 6 LNfrom 1 to 6 LN
N2 involvement of the regional lymph nodes N2 involvement of the regional lymph nodes – more than 3 cm from the primary including those located along more than 3 cm from the primary including those located along
the left gastric , common hepatic , splenic and celiac arteries orthe left gastric , common hepatic , splenic and celiac arteries or– from 7 to 15 LNfrom 7 to 15 LN
N3 more than 15 LN N3 more than 15 LN MetastasesMetastases
M0 no evidence of distant metastasesM0 no evidence of distant metastasesM1 evidence of distant metastases M1 evidence of distant metastases

Staging of cancer stomachStaging of cancer stomach
Stage1 Stage1 – T1 N0 M0, T1 N0 M0, – T1 N1 M0,T1 N1 M0,– T2 N0 M0T2 N0 M0
Stage 2Stage 2– T1 N2 M0, T1 N2 M0, – T2 N1 M0, T2 N1 M0, – T3 N0 M0 T3 N0 M0
Stage 3aStage 3a– T2 N2 M0, T2 N2 M0, – T3 N1 M0, T3 N1 M0, – T4 N0 M0 T4 N0 M0
Stage 3bStage 3b– T3 N2 M0 T3 N2 M0
Stage 4Stage 4– T4 N1-3 M0, T4 N1-3 M0, – Tx N3 M0 Tx N3 M0 – Tx Nx M1 Tx Nx M1

Prognostic factorsPrognostic factors
The three The three grave signsgrave signs are are – Serosal involvement Serosal involvement – Nodal involvementNodal involvement– Tumor at the line of resectionTumor at the line of resection
StageStage– The most important determinant is the No of LN involved (up to 3 The most important determinant is the No of LN involved (up to 3
is like non)is like non)
GradeGradeNature and extent of resectionNature and extent of resection– Curative R>palliativeCurative R>palliative– Distal R>proximal RDistal R>proximal R– Subtotal R> total RSubtotal R> total R

Surgery of Cancer StomachSurgery of Cancer Stomach
GastrectomyGastrectomy– An appropriate resection with adequate An appropriate resection with adequate
tumor free margins, this margin is tumor free margins, this margin is proximal in distal tumors and should proximal in distal tumors and should never be less than 5 cm. never be less than 5 cm.
– However, in proximal tumors total However, in proximal tumors total gastrectomy is done, and no part of the gastrectomy is done, and no part of the antrum is left behind since it will be antrum is left behind since it will be denervated and will perform no function.denervated and will perform no function.
Greater and lesser omentaGreater and lesser omenta with excised with excised stomach (most commonly used typestomach (most commonly used type

Surgery of Cancer StomachSurgery of Cancer Stomach
A regional LN clearanceA regional LN clearance corresponding to corresponding to location of primary tumor location of primary tumor – R1R1 (removal of N1 lymph nodes) in (removal of N1 lymph nodes) in
practice is achieved by removal ofpractice is achieved by removal of– R2R2 (removal of N2 lymph nodes) (removal of N2 lymph nodes)
Necessitates removal of LN around Necessitates removal of LN around main arteries (left gastric, common main arteries (left gastric, common hepatic, celiac and splenic arteries)hepatic, celiac and splenic arteries)In addition, splenectomy and distal In addition, splenectomy and distal pancreatectomy may be added to pancreatectomy may be added to achieve LN clearance achieve LN clearance




Surgery of Cancer StomachSurgery of Cancer StomachSafe and well functioning reconstructionSafe and well functioning reconstruction
– In potentially curable resections try to In potentially curable resections try to restore duodenal continuity by using restore duodenal continuity by using jujenal interposition with or without a jujenal interposition with or without a
pouch or pouch or colon interposition in case of total colon interposition in case of total
gastrectomy, or gastrectomy, or BIIBII in case there is subtotal in case there is subtotal
gastrectomygastrectomy..


Surgery of Cancer StomachSurgery of Cancer StomachSafe and well functioning reconstructionSafe and well functioning reconstruction–In potentially incurable resection a In potentially incurable resection a
duodenal bypass procedure as duodenal bypass procedure as Hunt Lawrance Hunt Lawrance jujenal Roux en Y loop with or jujenal Roux en Y loop with or without a pouch is used in case of without a pouch is used in case of total gastrectomy ortotal gastrectomy or
BIIBII in case of subtotal gastrectomy in case of subtotal gastrectomy

potentially incurable resection a duodenal potentially incurable resection a duodenal bypass procedurebypass procedure

Surgery of Cancer StomachSurgery of Cancer Stomach
Potentially curable resectionPotentially curable resection Proceed with R1 or R2 and Proceed with R1 or R2 and reconstruct with reconstruct with – jujenal interpostion with or without a pouch or jujenal interpostion with or without a pouch or – with colon interposition .with colon interposition .– All should be isoperistaltic.All should be isoperistaltic.– Duodenal continuity is preferred Duodenal continuity is preferred
Much controversy exists as regards R2 types of Much controversy exists as regards R2 types of resection, because it adds little to the curability rate if resection, because it adds little to the curability rate if compared with R1 and at the same time has got much compared with R1 and at the same time has got much side effects due to denervation of the celiac axis and side effects due to denervation of the celiac axis and other arteries leading to intolerable diarrhea.other arteries leading to intolerable diarrhea.

Surgery of Cancer StomachSurgery of Cancer Stomach
Potentially incurablePotentially incurable Three main grave signs Three main grave signs
(a)(a) serosal or extraserosal involvement, serosal or extraserosal involvement, (b) extensive nodal involvement (b) extensive nodal involvement (c) suspected safety margin,(c) suspected safety margin,
proceed with R1 and proceed with R1 and reconstruct with either reconstruct with either
– BII in subtotal gastrectomy or BII in subtotal gastrectomy or – with Hunt Lawrence roux en Y jujenal loop with with Hunt Lawrence roux en Y jujenal loop with
esophagojujenostomy in total gastrectomy. esophagojujenostomy in total gastrectomy.
Duodenal continuity is not preferred as after potentially Duodenal continuity is not preferred as after potentially curable resection due to early obstruction in these type curable resection due to early obstruction in these type of reconstruction if local recurrence occurs.of reconstruction if local recurrence occurs.

Surgery of Cancer StomachSurgery of Cancer Stomach
Un-resectable cancerUn-resectable cancer
A bypass operation (gastrojujenostomy) is done A bypass operation (gastrojujenostomy) is done if there is obstruction of the pylorus, or if there is obstruction of the pylorus, or
metal prosthesis is endoscopically inserted as in metal prosthesis is endoscopically inserted as in esophageal cancer if the cardia is obstructed.esophageal cancer if the cardia is obstructed.
A terminal patient with extensive peritoneal A terminal patient with extensive peritoneal seedlings and ascites with liver deposits are seedlings and ascites with liver deposits are better to be left without any surgery if they are better to be left without any surgery if they are not obstructed or bleedingnot obstructed or bleeding

Un-resectable cancerUn-resectable cancer A bypass operation A bypass operation (gastrojujenostomy)(gastrojujenostomy)

Surgery of Cancer StomachSurgery of Cancer Stomach
The best palliation is resection, and this is The best palliation is resection, and this is helpful in patients beyond any cure like helpful in patients beyond any cure like those with liver or peritoneal seedlings but those with liver or peritoneal seedlings but is bleeding or obstructed with a is bleeding or obstructed with a respectable tumor. respectable tumor. It is done to rid the patient of infected, It is done to rid the patient of infected, bleeding, obstructed, or ulcerated gastric bleeding, obstructed, or ulcerated gastric lesions. lesions. Limited gastric resection may suffice.Limited gastric resection may suffice.