Embed Size (px)
Citation preview
Stilianos E. Kountakis
Brent A. Senior
Wolfgang Draf
Editors
The Frontal Sinus
Stilianos E. Kountakis
Brent A. Senior
Wolfgang Draf
Editors
The Frontal Sinus
With 144 Figures, 73 in Color
and 40 Tables
Stilianos E. Kountakis, MD, PhDProfessor and Vice ChairChief, Rhinology-Sinus SurgeryMedical College of Georgia1120 15th St, Ste BP-4632Augusta, GA 30912-4060, USA
Brent A. Senior, MDAssoc. Prof., Chief, Rhinology, Allergy, and Sinus SurgeryDept. of Otolaryngology/Head and Neck SurgeryUniv. of North Carolina at Chapel HillChapel Hill, NC 27599--7070, USA
Wolfgang Draf, MD, PhD, FRCS (Ed)Professor and ChairmanDept. of ENT-Diseases, Head-, Neck and Facial Plastic SurgeryCommunication Disorders, Klinikum Fulda gAGPacelliallee 4, D 36043 Fulda, Germany
Library of Congress Control Number: 2005924448
ISBN-10 3-540-21143-8 Springer Berlin Heidelberg New YorkISBN-13 978-3-540-21143-3 Springer Berlin Heidelberg New York
This work is subject to copyright. All rights are reserved, whether the whole or part of the material is con-cerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, repro-duction on microfilm or in any other way, and storage in data banks. Duplication of this publication or partsthereof is permitted only under the provisions of the German Copyright Law of September 9, 1965, in its cur-rent version, and permission for use must always be obtained from Springer. Violations are liable to prosecu-tion under the German Copyright Law.
Springer is a part of Springer Science+Business Mediaspringeronline.com© Springer-Verlag Berlin Heidelberg 2005Printed in Germany
The use of general descriptive names, registered names, trademarks, etc. in this publication does not imply,even in the absence of a specific statement, that such names are exempt from the relevant protective lawsand regulations and therefore free for general use.
Product liability: the publishers cannot guarantee the accuracy of any information about dosage and applica-tion contained in this book. In every individual case the user must check such information by consulting therelevant literature.
Editor: Marion Philipp, Heidelberg, GermanyDesk Editor: Martina Himberger, Heidelberg, GermanyProduction: ProEdit GmbH, 69126 Heidelberg, GermanyCover: Frido-Steinen-Broo, EStudio, Calamar, SpainTypesetting: K. Detzner, 67346 Speyer, Germany
Printed on acid-free paper 21/3151 ML 5 4 3 2 1 0
� Dedicated to the memory of my mother,Eftihia E. Kountakis, who with her nurturingdevotion inspired my pursue of a medicalcareer, and to my loving wife Eleni and children Eftihia, Emmanuel and Nikoleta,who bring meaning to my life.Many thanks to my assistant Aprell Edwardsfor her long hours of hard work during thisproject.
Stil Kountakis
� To my wife, Dana, and my children, Rebecca,Benjamin, Grace, and Anna. A part of you is in each of these pages. Soli Deo Gloria.
Brent Senior
� To my wife Julia, and to my childrenMaximilian and Clara for their constant patience.It is a pleasure to thank my American colleagues for excellent cooperation in editing this book.
Wolfgang Draf
Dedications and Acknowledgements

Advances in instrumentation and surgical tech-niques continue to yield improvements in the surgi-cal management of sinus disease. Rhinologists havedeveloped techniques to address disease in remoteareas along the anterior skull base so that many pro-cedures previously performed using an open ap-proach may now be performed endoscopically. De-spite these advances, the complex anatomy and re-mote location of the frontal recess continue to posechallenges in the surgical management of frontal si-nus disease. The narrow funnel-shaped aperture andimportant surrounding structures can predispose tocomplications most rhinologists hope to avoid theycan do without. Because of this, it is not uncommonto hear at rhinology meetings that it is usually bestfor the average otolaryngologist to avoid instrumen-tation in this area, especially in primary surgeries.Numerous manuscripts are published describing theanatomy, diagnostic techniques, and medical andsurgical management of frontal sinus disease. But asour residents and fellows survey the literature, theyoften wish they had a single comprehensive source ofinformation related to the anatomy and managementof frontal sinus disorders.
Preface
This project was initiated in order to fill this voidand to provide a valuable source of information notonly for academic institutions but also for the privatepractice environment. Most of the world’s leading au-thorities in rhinology were invited to participate.Chapters in the book are arranged in a logical fash-ion, providing a comprehensive body of informationbeginning with the history of frontal sinus surgeryand addressing more complex surgical concepts asthe reader progresses through the text. Each chapterwas written by authors that possess extensive experi-ence on the topic and have previously published onthe particular anatomical structure or issue thechapter addresses. The result is the first exhaustivefrontal sinus textbook that can be used as a referencesource by both academic and practicing otolaryngol-ogists worldwide.
Stilianos Kountakis, MD, PhDBrent A. Senior, MDWolfgang Draf, MD, PhD, FRCS (Ed)

1 History of Frontal Sinus Surgery . . . . . 1Hassan H. Ramadan
2 Radiologic Anatomy of the Frontal Sinus 7Ramon E. Figueroa, Joseph Sullivan
3 Surgical Anatomy and Embryology of the Frontal Sinus . . . . . . . . . . . . 21Carlos S. Duque, Roy R. Casiano
4 Acute Frontal Sinusitis . . . . . . . . . . 33Douglas Reh, Peter H. Hwang
5 Chronic Frontal Rhinosinusitis:Diagnosis and Management . . . . . . . 43Michael Sillers
6 Microbiology of Chronic Frontal Sinusitis 53Birgit Winther, Jack Gwaltney
7 Orbital Complications of Frontal Sinusitis . . . . . . . . . . . . . 59Robert T. Adelson, Bradley F. Marple
8 CNS Complications of Frontal Sinus Disease . . . . . . . . . 67Andrew P. Lane
9 Frontal-Orbital-Ethmoid Mucoceles . . 75James Palmer, Ioana Schipor
Contents
10 Pott’s Puffy Tumor . . . . . . . . . . . . . 83Richard R. Orlandi
11 The Frontal Sinus and Nasal Polyps . . . 87James A. Stankiewicz, James M. Chow
12 Allergy and the Frontal Sinus . . . . . . 95Berrylin J. Ferguson
13 The Role of Fungus in Diseases of the Frontal Sinus . . . . . . . . . . . . 101Robert T. Adelson, Bradley F. Marple
14 Frontal Headache . . . . . . . . . . . . . 115Allen M. Seiden
15 Pediatric Frontal Sinusitis . . . . . . . . 127Charles W. Gross, Joseph K. Han
16 Frontal Sinus Fractures . . . . . . . . . . 133Tanya K. Meyer, John Rhee,Timothy L. Smith
17 Frontal Sinus Cerebrospinal Fluid Leaks 143Bradford A. Woodworth,Rodney J. Schlosser
18 Benign Tumors of the Frontal Sinuses . 153Brent A. Senior, Marc G. Dubin

ContentsX
19 Frontal Sinus Malignancies . . . . . . . . 165Christine G. Gourin, David J. Terris
20 The Endoscopic Frontal Recess Approach 179Boris I. Karanfilov, Frederick A. Kuhn
21 Revision Endoscopic Frontal Sinus Surgery . . . . . . . . . . . . . . . 191Alexander G. Chiu, David W. Kennedy
22 Image-Guidance in Frontal Sinus Surgery . . . . . . . . . . . . . . . 201Ralph Metson, Feodor Ung
23 “Above and Below” FESS:Simple Trephine with Endoscopic Sinus Surgery . . . . . 211Ankit M. Patel, Winston C.Vaughan
24 Endonasal Frontal Sinus Drainage Type I–III According to Draf . . . . . . . 219Wolfgang Draf
25 Endoscopic Modified Lothrop Procedure 233Stilianos E. Kountakis
26 Frontal Sinus Rescue . . . . . . . . . . . 243Martin J. Citardi, Pete S. Batra,Frederick A. Kuhn
27 Endoscopic Trans-septal Frontal Sinusotomy . . . . . . . . . . . . 251Pete S. Batra, Donald C. Lanza
28 Frontal Sinus Stenting . . . . . . . . . . 261Seth J. Kanowitz, Joseph B. Jacobs,Richard A. Lebowitz
29 Complications of Frontal Sinus Surgery 267Scott M. Graham
30 Open Approaches . . . . . . . . . . . . . 275Mark C. Weissler
31 Osteoplastic Frontal Sinusotomy and Reconstruction of Frontal Defects . 281Ulrike Bockmühl
Subject Index . . . . . . . . . . . . . . . . . . . 291
Robert T. Adelson, MDChief Resident, Dept. of Otolaryngology Head and Neck SurgeryUniv. of Texas Southwestern Medical Ctr.5323 Harry Hines Blvd., Dallas, TX 75390–9035USA
Pete S. Batra, MD (e-mail: [email protected])Cleveland Clinic FoundationHead & Cleveland Clinic FoundationDept. of Otolaryngology9500 Euclid Ave., Desk A71, Cleveland, OH 44195USA
Ulrike Bockmühl, MD, PhD (e-mail: [email protected] Professor, Dept. of OtorhinolaryngologyHead and Neck and Facial Plastic SurgeryKlinikum Fulda gAGTeaching Hospital of the Philipps-University MarburgPacelliallee 4, 36043 FuldaGermany
Roy Casiano, MD(e-mail: [email protected] )University of Miami1475 NW 12th Ave, Suite 4025Miami, FL 33136-1002USA
Alexander G. Chiu, MD (e-mail: [email protected])Dept. of Otorhinolaryngology-Head and Neck SurgeryUniv. of Pennsylvania Health System3400 Spruce St., 5 Ravdin, Philadelphia, PA 19104USA
James M. Chow, MD (e-mail: [email protected])Dept. of Otolaryngology-Head and Neck SurgeryLoyola University Medical Center2160 S. First Ave., Maywood, IL 60153USA
Martin J. Citardi, MD (e-mail: [email protected])Cleveland Clinic FoundationHead & Cleveland Clinic FoundationDept. of Otolaryngology9500 Euclid Ave., Desk A71, Cleveland, OH 44195USA
Wolfgang Draf, MD, PhD, FRCS (Ed)(e-mail: [email protected])Professor and ChairmanDept. of ENT-DiseasesHead-, Neck and Facial Plastic SurgeryCommunication Disorders, Klinikum Fulda gAGTeaching Hospital of the Philipps-University MarburgPacelliallee 4, 36043 FuldaGermany
Marc G. Dubin, MDGeorgia Nasal and Sinus Institute4750 Waters Ave., Ste. 112, Savannah, GA 31404USA
Carlos S.Duque, MD(e-mail: [email protected])University of Miami1475 NW 12th AveSuite 4025Miami, FL 33136-1002United States of AmericaUSA
List of Contributors
Berrylin J. Ferguson, MD (e-mail: [email protected])Otolaryngology/Head and Neck SurgeryUniversity of Pittsburgh, Pittsburgh, PAUSA
Ramon E. Figueroa, MD, FACR (e-mail: [email protected])Professor of Radiology, Chief of NeuroradiologyMedical College of Georgia1120 15th St., Augusta, GA 30912USA
Christine G. Gourin, MD, FACS (e-mail: [email protected])Dept. of Otolaryngology – Head and Neck SurgeryMedical College of Georgia1120 15th St., BP 4117, Augusta, GA 30912USA
Scott M. Graham, MD (e-mail: [email protected])Professor, DirectorRhinology and Paranasal Sinus ClinicDept. of Otolaryngology – Head and Neck SurgeryUniversity of IowaIowa City, IA 52242USA
Charles W. Gross, MD (e-mail: [email protected])Dept. of Otolaryngology and Head & Neck SurgeryDivision of RhinologyUniversity of Virginia Health SystemBox 800713, Charlottesville, VA 22908-0713USA
Jack Gwaltney, MDDepts. of Otolaryngology and Internal MedicineUniversity of Virginia Health SystemCharlottesville, VA 22908USA
Joseph K. Han, MD (e-mail: [email protected])Dept. of Otolaryngology and Head & Neck SurgeryDivision of RhinologyUniversity of Virginia Health SystemBox 800713, Charlottesville, VA 22908-0713USA
Peter H. Hwang, MD (e-mail: [email protected])3181 SW Sam Jackson Pk. Rd., PV01, Dept. OTO-HNS, Portland OR 97239USA
Joseph B. Jacobs, MD (e-mail: [email protected])New York Univ. Med. Ctr., Dept. of Otolaryngology530 First Ave., Ste. 3C, New York, NY 10016-6402USA
Seth J. Kanowitz, MD(e-mail: [email protected]) Department of OtolaryngologyNew York University School of Medicine530 First Avenue, SUite 3CNew York, New York 10016USA
Boris I. Karanfilov, MD (e-mail: [email protected])Ohio Sinus Institute750 Mt. Carmel Mall, Ste. 240, Columbus, OH 43222USA
David W. Kennedy, MD (e-mail: [email protected])Dept. of Otorhinolaryngology-Head and Neck SurgeryUniversity of Pennsylvania Health System3400 Spruce St., 5 Ravdin, Philadelphia, PA 19104USA
Stilianos E. Kountakis, MD, PhD (e-mail: [email protected])Dept. of Otolaryngology–Head and Neck SurgeryMedical College of Georgia1120 15th St., Ste. BP-416, Augusta, GA 30912-4060USA
Frederick A. Kuhn, MD, FACS (e-mail: [email protected])Georgia Nasal and Sinus Institute4750 Waters Ave., Ste. 112, Savannah, GA 31410USA
List of ContributorsXII
Andrew P. Lane, MD (e-mail: [email protected])Director, Div. of RhinologyDept. of Otolaryngology – Head and Neck SurgeryJohns Hopkins Outpatient Center6th Fl., 601 N. Caroline St., Baltimore, MD 21287USA
Donald C. Lanza, MD (e-mail: [email protected])Director, Sinus & Nasal Inst. of Florida, P.A.St. Anthony’s Outpatient Ctr.900 Carillon Pkwy., Ste. 200, St. Petersburg, FL 33716USA
Richard A. Lebowitz, MD (e-mail: [email protected])Asst. Prof. of OtolaryngologyNew York Univ. School of Medicine, NYUSA
Bradley F. Marple, MD, FAAOA (e-mail: [email protected])Associate Professor and Vice-ChairmanDept. of Otolaryngology Head and Neck SurgeryUniv. of Texas Southwestern Medical Ctr.5323 Harry Hines Blvd., Dallas, TX 75390–9035USA
Ralph Metson MD (e-mail: [email protected])Zero Emerson Pl., Ste. 2D, Boston, MA 02114USA
Tanya K. Meyer, MDDept. of Otolaryngology and Communication Sciences9200 W. Wisconsin Ave., Medical College of WisconsinMilwaukee, WI 53226USA
Richard R. Orlandi, MD, FACS (e-mail: [email protected])Division of Otolaryngology – Head and Neck SurgeryThe University of Utah50 N. Medical Dr., Ste. 3C120, Salt Lake City, UT 84132USA
James Palmer, MD(e-mail: [email protected]) Hospital University of Pennsylvania3400 Spruce Street, 5th floor, Ravdin BuildingPhiladelphia, PA 19104USA
Ankit M. Patel, MD300 Pasteur Dr., R135, Stanford, CA 94305USA
Hassan H. Ramadan, MD, MSc (e-mail: [email protected])Dept. of Otolaryngology Head & Neck SurgeryWest Virginia UniversityP.O. Box 9200, Morgantown, WV 26506–9200USA
Douglas Reh, MD(e-mail: [email protected])3181 SW Sam Jackson Pk Rd PV01Dept. OTO-HNSPortland, OR 97239USA
John S. Rhee, MDDiv. of Facial Plastic and Reconstructive Surgery9200 W. Wisconsin Ave, Medical College of Wisconsin Milwaukee, WI 53226USA
Ioana Schipor, MD(e-mail: [email protected]) Hospital University of Pennsylvania3400 Spruce Street, 5th floor, Ravdin BuildingPhiladelphia, PA 19104USA
Rodney J. Schlosser, MD (e-mail: [email protected])Medical Univ. of South CarolinaDept. of OtolaryngologyPO Box 250550135 Rutledge Ave., Ste. 1130, Charleston, SC 29425USA
List of Contributors XIII
Allen M. Seiden, MD (e-mail: [email protected])Prof. of Otolaryngology, Univ. of CincinnatiCollege of Medicine, Dept. of Otolaryngology – Head and Neck SurgeryP.O. Box 670528231 Albert Sabin Way (formerly Bethesda Ave.)Rm. 6412 MSB, Cincinnati, Ohio 45267–0528USA
Brent A. Senior, MD (e-mail: [email protected])Assoc. Prof., Chief, Rhinology, Allergy,and Sinus Surgery, Dept. of Otolaryngology/Head and Neck SurgeryUniv. of North Carolina at Chapel HillChapel Hill, NC 27599–7070USA
Michael Sillers, MD (e-mail: [email protected])Assoc. Prof., Otolaryngology/Headand Neck Surgery, Univ. of Alabama at Birmingham1501 5th Ave. S., Birmingham AL 35233-1614USA
Timothy L. Smith, MD, MPH (e-mail: [email protected])Div. of Rhinology and Sinus Surgery9200 W. Wisconsin Ave.Medical College of Wisconsin, Milwaukee, WI 53226USA
James A. Stankiewicz, MD (e-mail: [email protected])Dept. of Otolaryngology-Head and Neck SurgeryLoyola Univ. Medical Ctr2160 S. First Ave., Maywood, IL 60153USA
Joseph Sullivan, MD (e-mail: [email protected])Neuroradiology Fellow, Neuroradiology ServiceMedical College of Georgia1120 15th St., Augusta, GA 30912USA
David J.Terris, MD, FACS (e-mail: [email protected])Dept. of Otolaryngology – Head and Neck SurgeryMedical College of Georgia1120 15th St., BP 4117, Augusta, GA 30912USA
Feodor Ung, MD (e-mail: [email protected])DuPage Medical Group at Lombard1801 S. Highland Ave., Ste. 220, Lombard, IL 60148USA
Winston C.Vaughan, MD (e-mail: [email protected])300 Pasteur Dr., R135, Stanford, CA 94305USA
Birgit Winther, MD (e-mail: [email protected])Dept.s of Otolaryngology and Internal MedicineUniversity of Virginia Health SystemPO Box 800713, Charlottesville,VA 22908USA
Mark C. Weissler, MD, FACS (e-mail: [email protected])G0412 Neurosciences HospitalUniv.y of North Carolina, Campus Box 7070Chapel Hill, NC 27599–7070USA
Bradford A.Woodworth, MDMedical University of South CarolinaDepartment of OtolaryngologyPO Box 250550135 Rutledge Ave., Suite 1130Charleston, SC 29425USA
List of ContributorsXIV
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . 1Trephination Era (1750) . . . . . . . . . . . . . . . . 2Radical Ablation Procedures (1895) . . . . . . . . . . 2Conservative Procedures (1905) . . . . . . . . . . . . 2External Frontoethmoidectomy (1897, 1906, 1921) . 3Osteoplastic Anterior Wall Approach to the Frontal Sinus (1958) . . . . . . . . . . . . . . . 4Microscopic/Endoscopic Intranasal Approaches (1991) . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . 5
References . . . . . . . . . . . . . . . . . . . . . . . . . 5
Introduction
The first frontal sinus procedure was described in1750 [36]. Despite more than two centuries since thedescription of the first procedure on the frontal si-nus, the optimal procedure remains unclear. Al-though frontal sinus surgery makes up only a smallportion of all paranasal sinus surgery, the literature isfilled with publications on this subject. Ellis in 1954stated that “surgical treatment of chronic frontal si-nusitis is difficult, often unsatisfactory and some-times disastrous. The many surgical techniquesavailable are expressions of our uncertainty and per-haps so our failure” [11].
The ideal treatment for diseases of the frontal si-nus is one that will provide complete relief of symp-toms, eradicate the underlying disease process, pre-serve the function of the sinus, and cause the leastmorbidity and the least cosmetic deformity. Over thelast two centuries a variety of surgical procedureshave been described for the treatment of frontal si-nus disease. Those procedures flip-flopped from ex-ternal to intranasal to external and currently to intra-nasal again. The ideal procedure has not been identi-fied yet despite 2 centuries of various techniques.
The recent advances in imaging and endoscopictechniques have resulted in the resurgence of intra-nasal procedures for the treatment of frontal sinusdisease. Frontal sinus disease, particularly chronicfrontal sinusitis, is a highly morbid and sometimeslife-threatening condition because of its potentialcomplications. Despite the fact that over the years theincidence of complications has decreased, orbitaland intracranial complications, including meningi-tis, subdural abscess, intracerebral abscess, and os-teomyelitis continue to occur.
Core Messages
� With over two centuries of scientificdescription of frontal sinus surgery, theoptimal procedure remains unclear
� Balancing concerns of eradication of dis-ease with cosmesis and restoration of fron-tal sinus function has resulted in the devel-opment of numerous procedures for treat-ment of frontal sinus disease
� Endoscopic approaches are now widelyapplied to the management of frontal sinusdisease
Chapter 1
History of Frontal Sinus SurgeryHassan H. Ramadan
1
Trephination Era (1750)
Frontal sinus surgery was first described in the 18th
century. It is noted that as early as 1750 Runge per-formed an obliteration procedure of the frontal sinus[36]. The first published report in 1870 by Wells de-scribed an external and intracranial drainage proce-dure for a frontal sinus mucocele [44].
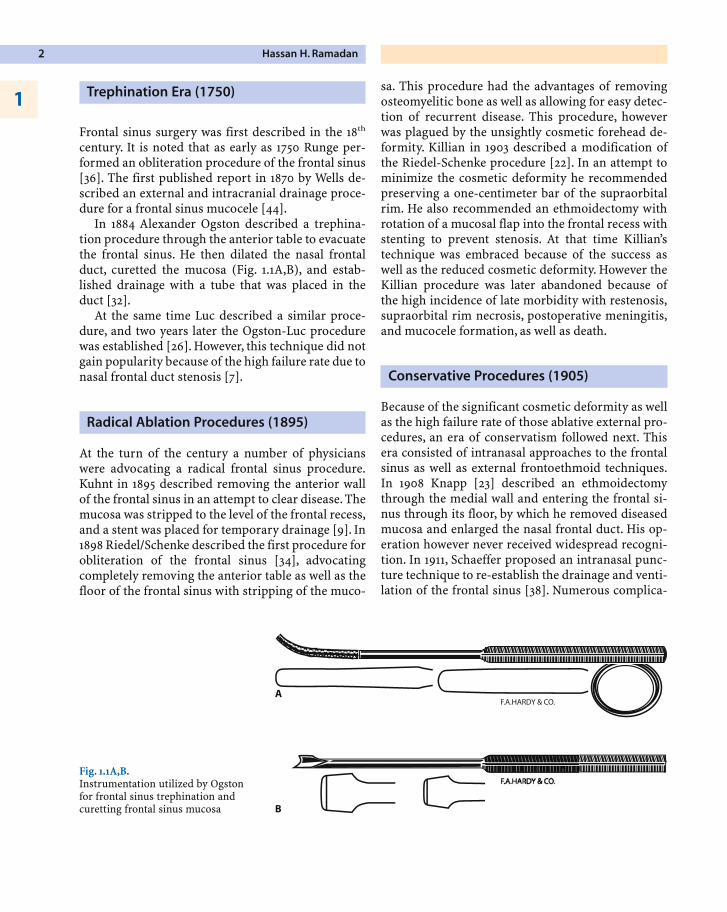
In 1884 Alexander Ogston described a trephina-tion procedure through the anterior table to evacuatethe frontal sinus. He then dilated the nasal frontalduct, curetted the mucosa (Fig. 1.1A,B), and estab-lished drainage with a tube that was placed in theduct [32].
At the same time Luc described a similar proce-dure, and two years later the Ogston-Luc procedurewas established [26]. However, this technique did notgain popularity because of the high failure rate due tonasal frontal duct stenosis [7].
Radical Ablation Procedures (1895)
At the turn of the century a number of physicianswere advocating a radical frontal sinus procedure.Kuhnt in 1895 described removing the anterior wallof the frontal sinus in an attempt to clear disease. Themucosa was stripped to the level of the frontal recess,and a stent was placed for temporary drainage [9]. In1898 Riedel/Schenke described the first procedure forobliteration of the frontal sinus [34], advocatingcompletely removing the anterior table as well as thefloor of the frontal sinus with stripping of the muco-
sa. This procedure had the advantages of removingosteomyelitic bone as well as allowing for easy detec-tion of recurrent disease. This procedure, howeverwas plagued by the unsightly cosmetic forehead de-formity. Killian in 1903 described a modification ofthe Riedel-Schenke procedure [22]. In an attempt tominimize the cosmetic deformity he recommendedpreserving a one-centimeter bar of the supraorbitalrim. He also recommended an ethmoidectomy withrotation of a mucosal flap into the frontal recess withstenting to prevent stenosis. At that time Killian’stechnique was embraced because of the success aswell as the reduced cosmetic deformity. However theKillian procedure was later abandoned because ofthe high incidence of late morbidity with restenosis,supraorbital rim necrosis, postoperative meningitis,and mucocele formation, as well as death.
Conservative Procedures (1905)
Because of the significant cosmetic deformity as wellas the high failure rate of those ablative external pro-cedures, an era of conservatism followed next. Thisera consisted of intranasal approaches to the frontalsinus as well as external frontoethmoid techniques.In 1908 Knapp [23] described an ethmoidectomythrough the medial wall and entering the frontal si-nus through its floor, by which he removed diseasedmucosa and enlarged the nasal frontal duct. His op-eration however never received widespread recogni-tion. In 1911, Schaeffer proposed an intranasal punc-ture technique to re-establish the drainage and venti-lation of the frontal sinus [38]. Numerous complica-
Hassan H. Ramadan2
1
Fig. 1.1A,B.Instrumentation utilized by Ogstonfor frontal sinus trephination andcuretting frontal sinus mucosa
tions were encountered, however, including intracra-nial penetration. Between 1901 and 1908, Ingals,Halle, Good, and Wells described several intranasalprocedures to the frontal sinus [14, 16, 19, 45]. Halledescribed a procedure in which the frontal process ofthe maxilla was chiseled out, and then a burr wasused to remove the floor of the frontal sinus [16]. Thisoperation was rarely used because it was associatedwith a high mortality rate. All of these intranasal ap-proaches were abandoned because of the high mor-tality and complication rates associated with them.This increased incidence of mortality and complica-tions was a result of the inadequate visualization ofthe frontal recess.
In 1914, Lothrop described a procedure to enlargethe frontal drainage pathway in a way that would pre-vent restenosis as well as closure as was reportedwith other procedures at the time [25]. The proceduredescribed a combined intranasal ethmoidectomyand an external ethmoid approach to create a com-mon frontal nasal communication by resecting thenasal sinus floor, the frontal sinus septum, and thesuperior nasal septum. Lothrop later admitted thatthe lack of visualization during the intranasal ap-proach made the procedure dangerous. Further fol-low-up on those patients also showed that the resec-tion of the medial orbital wall allowed the collapse oforbital soft tissue into the ethmoid area, with subse-quent stenosis of the frontal drainage pathway.
External Frontoethmoidectomy (1897, 1906, 1921)
Between 1897 (Jansen [20]) and 1906 (Ritter [35]), thedetails of frontoethmoidectomy were described inGermany. In the Anglo-American literature, Lynch(1921) [28] in the United States and Howarth [18] inthe United Kingdom popularized the principle offrontal sinus floor resection and enlargement of thefrontal sinus drainage. Therefore in those countriesfrontoethmoidectomy was known as the Lynch andHowarth operation [17].
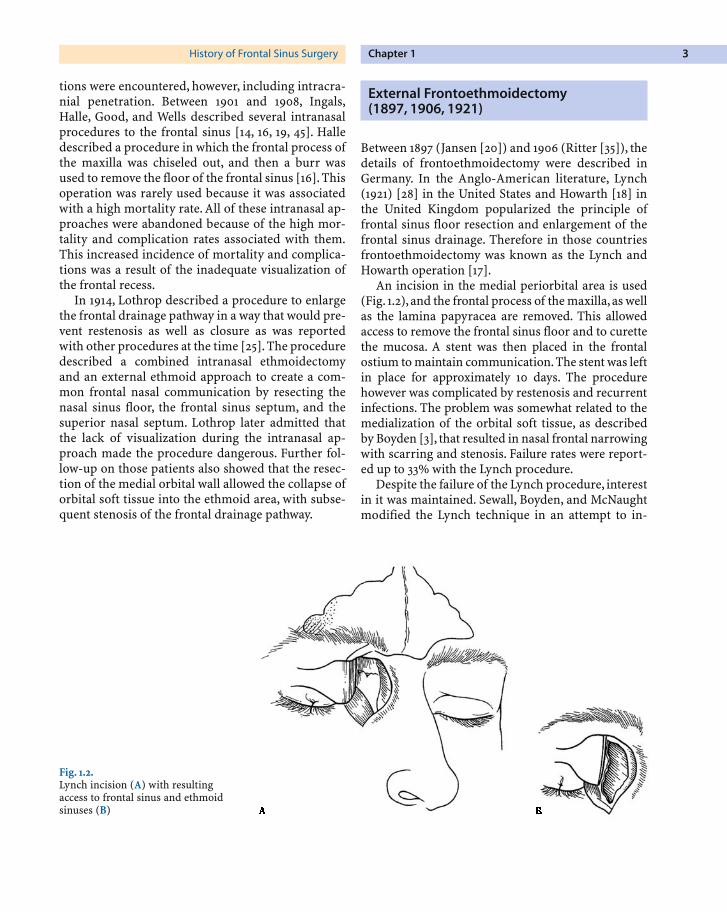
An incision in the medial periorbital area is used(Fig. 1.2), and the frontal process of the maxilla,as wellas the lamina papyracea are removed. This allowedaccess to remove the frontal sinus floor and to curettethe mucosa. A stent was then placed in the frontalostium to maintain communication.The stent was leftin place for approximately 10 days. The procedurehowever was complicated by restenosis and recurrentinfections. The problem was somewhat related to themedialization of the orbital soft tissue, as describedby Boyden [3], that resulted in nasal frontal narrowingwith scarring and stenosis. Failure rates were report-ed up to 33% with the Lynch procedure.
Despite the failure of the Lynch procedure, interestin it was maintained. Sewall, Boyden, and McNaughtmodified the Lynch technique in an attempt to in-
Chapter 1History of Frontal Sinus Surgery 3
Fig. 1.2.Lynch incision (A) with resultingaccess to frontal sinus and ethmoidsinuses (B)
crease the success rate and decrease failure and re-stenosis rates [3, 30, 40]. They described using a localmucoperiosteal flap to line and re-epithelialize thenasal frontal drainage pathway area. They also used asilicone tube to stent the frontal ostium, and they rec-ommended leaving the stent in place for 4 weeks. Lat-er several other authors lined the frontal drainagepathway with a mucoperiosteal flap to prevent re-stenosis and reported early success rates of about90% [29]. Dedo, using the Sewall/Boyden technique,reported a success and patency rate of 97% at 6 yearfollow-up [8]. This era of utilizing modifications ofthe Lynch external frontoethmoidectomy continuedto be the procedure of choice extending from its de-scription in 1921 to the 1950s. Walsh in 1943, in an at-tempt to solve the problem of restenosis and the needfor stenting, described a modification of the Lynchprocedure in which the frontal drainage pathwaymembrane was left intact [43]. He came to those ob-servations after he performed an experimental studyon three groups of dogs. Brown, in accord withWalsh’s idea, reported in 1946 a procedure to preservethe frontal drainage pathway mucosa in an attempt toreduce the failure drainage pathway and restenosisrates [5]. The problem of stenosis was significantenough that many researchers devised stents made ofdifferent materials in attempts to solve the problem[12]. Despite those modifications and stent tech-niques, long-term failure rates up to 30% were stillreported, necessitating the continued development ofbetter surgical procedures for the frontal sinus [29].
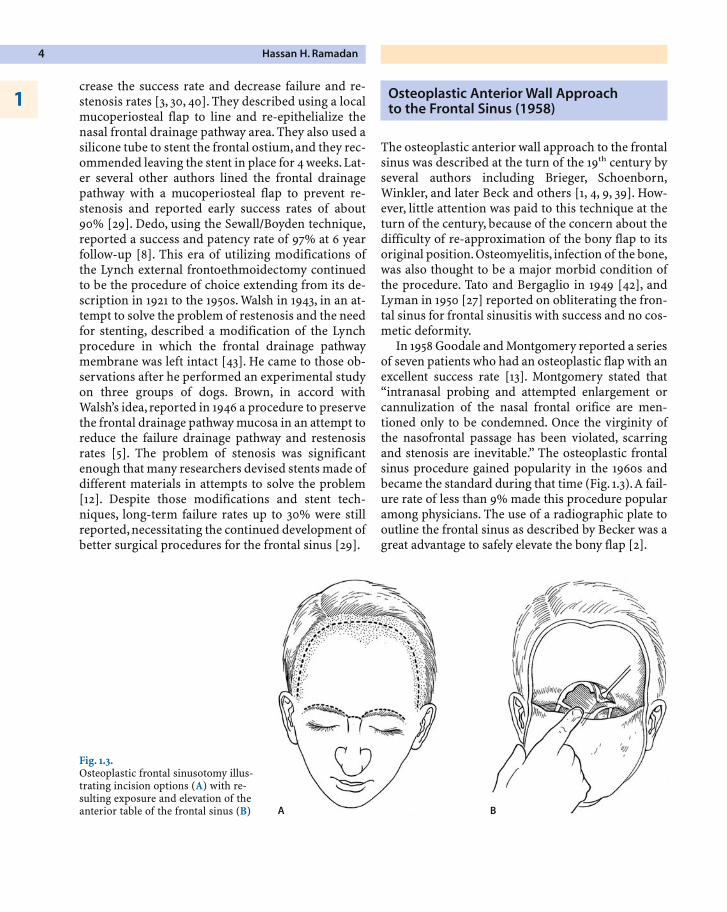
Osteoplastic Anterior Wall Approach to the Frontal Sinus (1958)
The osteoplastic anterior wall approach to the frontalsinus was described at the turn of the 19th century byseveral authors including Brieger, Schoenborn,Winkler, and later Beck and others [1, 4, 9, 39]. How-ever, little attention was paid to this technique at theturn of the century, because of the concern about thedifficulty of re-approximation of the bony flap to itsoriginal position. Osteomyelitis, infection of the bone,was also thought to be a major morbid condition ofthe procedure. Tato and Bergaglio in 1949 [42], andLyman in 1950 [27] reported on obliterating the fron-tal sinus for frontal sinusitis with success and no cos-metic deformity.
In 1958 Goodale and Montgomery reported a seriesof seven patients who had an osteoplastic flap with anexcellent success rate [13]. Montgomery stated that“intranasal probing and attempted enlargement orcannulization of the nasal frontal orifice are men-tioned only to be condemned. Once the virginity ofthe nasofrontal passage has been violated, scarringand stenosis are inevitable.” The osteoplastic frontalsinus procedure gained popularity in the 1960s andbecame the standard during that time (Fig. 1.3).A fail-ure rate of less than 9% made this procedure popularamong physicians. The use of a radiographic plate tooutline the frontal sinus as described by Becker was agreat advantage to safely elevate the bony flap [2].
Hassan H. Ramadan4
1
Fig. 1.3.Osteoplastic frontal sinusotomy illus-trating incision options (A) with re-sulting exposure and elevation of theanterior table of the frontal sinus (B) A B

A lot of experience accumulated with this tech-nique, and Hardy and Montgomery reported in 1976a 95% success rate with a median follow-up of 3 years[17]. Wide et al. in 1997 reported a 62% success ratewith an additional 21% of patients achieving successafter revision surgery [46].
Many otolaryngologists did not feel that the oste-oplastic flap with fat obliteration was the answer tofrontal sinus disease. They noted that it was an inva-sive procedure, which is technically difficult. It car-ries with it a high blood loss with potential for cos-metic deformity and poor scar formation. Many pa-tients experience frontal neuralgias with numbnessof the forehead. An additional operative site is need-ed for harvesting fat with potential morbidities.Long-term follow-up is necessary because of poten-tial mucocele formation, and the presence of fat inthe sinus makes it difficult to diagnose other frontalsinus problems [33].
Despite the popularity and the wide use of the os-teoplastic flap, many physicians were not satisfiedand did not feel that it was the ultimate procedure.
Microscopic/Endoscopic Intranasal Approaches (1991)
Earlier intranasal frontal sinus procedures had a highcomplication rate due to poor visualization. In 1990,Schaefer and Close reported on the use of the endo-scope to treat 36 patients with frontal sinus disease.They performed endoscopic frontal sinusotomy with12 patients reporting complete resolution of symp-toms and 11 reporting improvement [37]. Draf, in1991, reported on a series of 100 patients in which heused both a microscope and an endoscope to per-form intranasal frontoethmoid surgery for frontal si-nus disease. He described a concept of three proce-dures with a 90% success rate. He reported no com-plications with this endoscopic technique. All 10% ofhis failures had an open osteoplastic obliterative pro-cedure. The Draf procedures were aimed at openingthe frontal ostium intranasally and allowing the si-nus to drain. Draf I consisted of an anterior ethmoi-dectomy with opening of the nasofrontal duct (NFD).Draf II in addition consists of unilateral resection ofthe floor of the frontal sinus; Draf III is bilateral re-section of the frontal sinus floor [10].
With the advent of the endoscope, several authorshave recently reported on the use of the endoscope toopen the frontal sinus ostium and establish drainageof the frontal sinus. The advantages included lowermorbidity rates, a shorter hospital stay, a less invasiveprocedure, and no external scarring [6, 15, 21, 31].
Kountakis and Gross in 2003 reported on long-term results of the modified Lothrop procedure andnoted that with advancement of instrumentation andimproved skills of surgeons with endoscopic proce-dures, success has been similar to that of the open os-teoplastic approach with obliteration [24]. Stankie-wicz and Wachter in 2003 reported a 90% successrate with the endoscopic approach for patients whohad an osteoplastic approach and failed [41].
Conclusion
Currently, most otolaryngologists will initially per-form an endoscopic procedure in most cases ofchronic frontal sinusitis. An open procedure is usual-ly reserved for patients with absent or distortedintranasal landmarks, failed endoscopic approaches,complicated frontal sinusitis, and evidence of lateraldisease or posterior table erosion.
References
1. Beck, JC (1916) External frontal sinus operation. JAMA 67 :1811–1815
2. Becker D, Moore D, Lindsey W, et al (1995): Modified trans-nasal endoscopic Lothrop Procedure: Further considera-tions. Laryngoscope 105 : 1161
3. Boyden GL (1952) Surgical treatment of chronic frontal si-nusitis. Ann Otol Rhinol Laryngol 61 : 558
4. Brieger (1895) Ueber chronische Eiterungen der Neben-hoehlen der Nase.Arch Ohren Nasen Kehlkopfheilk 39 :213.
5. Brown, JM (1946) Frontal sinusitis. Tran Amer Laryngol,Rhinol And Otol Soc 50 : 314–317
6. Close LG, Lee NK, Leach JL, et al (1994) Endoscopic resec-tion of the intranasal frontal sinus floor. Ann Otol RhinolLaryngol 103 : 952–958
7. Coakley CG (1905) Frontal sinusitis: Diagnosis, treatment,and results. Trans Am Laryngol Rhinol Otol Soc 11 : 101
8. Dedo HH, Broberg TG, Mur AH (1998) Frontoethmoidec-tomy with Sewall-Bowden reconstruction: Alive and well, a25-year experience. Am J Rhinol 12 : 191
Chapter 1History of Frontal Sinus Surgery 5
t
9. Donald PJ (1995) Surgical management of frontal sinus in-fections. In Donald PJ, Gluckman JL, Rice DH (eds): TheSinuses. New York, Raven Press
10. Draf W (1991) Endonasal micro-endoscopic frontal sinussurgery: The Fulda concept. Oper Tech Otolaryngol HeadNeck Surg 2 : 234
11. Ellis M (1954) The treatment of frontal sinusitis. J LaryngolOtol 68 : 478–490
12. Goodale, RL (1945) The use of tantalum in radical frontalsinus surgery. Ann Otol, Rhinol And Laryngol 54 : 757–762
13. Goodale RL, Montgomery WW (1958) Experience with os-teoplastic anterior wall approach to the frontal sinus. ArchOtolaryngol 68 : 271
14. Goode RH (1908) An intranasal method for opening thefrontal sinus establishing the largest possible drainage. La-ryngoscope 18 : 266
15. Gross WE, Gross CW, Becker D, et al (1995) Modified trans-nasal endoscopic Lothrop procedure as an alternative tofrontal sinus obliteration. Otolaryngol Head Neck Surg113 : 427–434
16. Halle M (1906) Externe oder interne Operation der Neben-höhleneiterungen. Berl Klin Wochenschr 43: 1369–1372,1404–1407
17. Hardy JM, Montgomery WW (1976) Osteoplastic frontalsinusotomy: an analysis of 250 operations. Ann Otol Rhin-ol Laryngol 85 : 523–532
18. Howarth WG (1921) Operations on the frontal sinus. J La-ryngol Otol 36: 417–421
19. Ingals EF (1905) New operation and instruments for drain-ing the frontal sinus. Ann Otol Rhinol Laryngol 14 : 512
20. Jansen A (1894) Zur Eröffnung der Nebenhöhlen der Nasebei chronischer Eiterung. Arch Laryng Rhinol (Berl) 1:135–157
21. Kennedy DW, Josephson JS, Zinreich SJ, et al (1989) Endo-scopic sinus surgery for mucoceles: a viable alternative.Laryngoscope 99 : 885–895
22. Killian G (1903) Die Killianische Radicaloperation chro-nischer Stirnhoehleneiterungen: Weiteres kasuistischesMaterial and Zusammenfassung.Arch Laryngol Rhinol 13 :59.
23. Knapp A (1908) The surgical treatment of orbital compli-cations in disease of the nasal accessory sinuses. JAMA 51 :299
24. Kountakis SE, Gross CW (2003) Long-term results of theLothrop operation. Curr Opin Otolaryngol Head NeckSurg 11(1) : 37–40
25. Lothrop HA (1914) Frontal sinus suppuration. Ann Surg59 : 937
26. Luc H (1893) Empyeme latent du sinus frontal duct sanscause aparante: Traitemente par l’ouverture de los frontalet la currettage du foger guerim incomplete. Arch Int La-ryngol 6 : 216
27. Lyman EH (1950) The place of the obliterative operation infrontal sinus surgery. Laryngoscope 60 : 407
28. Lynch RC (1921) The technique of a radical frontal sinusoperation which has given me the best results. Laryngo-scope 31 : 1
29. May M, Schaitkin B (1995) Frontal sinus surgery: Endona-sal endoscopic osteoplasty rather than external osteoplas-ty. Oper Tech Otolaryngol Head Neck Surg 6 : 184
30. McNaught RC (1936) Refinement of the external frontoethmosphenoid operation: A new nasofrontal pedicle flap.Arch Otolaryngol 23 : 544
31. Metson R (1992) Endoscopic treatment of frontal sinusitis.Laryngoscope 102 : 712–716
32. Ogston A (1884) Trephining the frontal sinus for catarrhaldiseases. Men Chron Manchester 1 : 235
33. Ramadan HH (2000) History of frontal sinus surgery.Arch Otolaryngol Head Neck Surg 126 : 98–99
34. Riedel-Schenke H: Cited by Gosdale RH (1955) The radicalobliterative frontal sinus operation: A consideration oftechnical factors in difficult cases.Ann Otol Rhinol Laryn-gol 64 : 470
35. Ritter G (1906) II. Eine neue Methode zur Erhaltung dervorderen Stirnhöhlenwand bei Readikaloperationen chro-nischer Stirnhöhleneiterungen. Dtsch Med Wochenschr32: 1294–1296
36. Runge: Cited by Stevenson RS, Guthrie D: (1949) A historyof otolaryngology. Baltimore, Williams and Wilkins
37. Schaefer SD, Close LG (1990) Endoscopic management offrontal sinus disease. Laryngoscope 100 : 155–160
38. Schaeffer JP: Cited by Sier (1911) Rouillons.Arch Int Laryn-gol 31 : 709
39. Schoenborn: Cited by Wilkop A (1894) Ein Beitrag zur Ka-suistik der Erkrankungen des Sinus frontalis. Wuerzburg,F. Frome.
40. Sewall EC (1935) The operative treatment of nasal sinusdisease. Ann Otol 44 : 307
41. Stankiewicz JA, Wachter B (2003) The endoscopic modi-fied Lothrop procedure for salvage of chronic frontal si-nusitis after osteoplastic flap failure. Otolaryngol HeadNeck Surg 129(6) : 678–83
42. Tato JM, Bergaglio OE (1949) Cirurgia del frontal injertode grosa. Nueva tecnica (Surgery of frontal sinus. Fatgrafts, new technique. Otolaringologica, Oct. 1949) citedaccording Tato, Sibbald and Bergaglio. Laryngoscope(1954) 64: 504–521
43. Walsh TE (1943) Experimental surgery of the frontal sinus.The role of the ostium and nasofrontal duct in postopera-tive healing. Laryngoscope 53 : 75–92
44. Wells R (1870) Abscess of the frontal sinus. Lancet 1 : 69445. Wells WA (1901) On sounding and irrigating the frontal si-
nus through the natural opening. Laryngoscope 10 : 26246. Wide K, Sipila J, Suonpaa J (1997) Report on results of fron-
tal sinus obliterations in Turku University Central Hospi-tal, 1977–1994. Acta Otolaryngol 529(suppl) : 184–186
Hassan H. Ramadan6
1
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . 7
Embryologic and Functional Concepts . . . . . . . . . 7
Frontal Sinus Evaluation . . . . . . . . . . . . . . . . . 8
Frontal Sinus Drainage Pathway . . . . . . . . . . . . . 9
Anatomic Variants . . . . . . . . . . . . . . . . . . . . . 15Frontal Cells . . . . . . . . . . . . . . . . . . . . . . . 15Supraorbital Ethmoid Cell . . . . . . . . . . . . . . . 16Depth of Olfactory Fossa . . . . . . . . . . . . . . . . 16
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . 20
References . . . . . . . . . . . . . . . . . . . . . . . . . 20
Introduction
The frontal sinus and its drainage pathway compriseone of the most complex anatomic areas of the ante-rior skull base. Its complexity is magnified by the fre-
quency of anatomic variations which impact the di-rection of drainage, efficiency of mucociliary clear-ance, and morphology of the frontal recess. Recentsignificant advances in computed tomography (CT),especially the introduction of multidetector helicalscanning and the routine availability of computerworkstations, have made demonstration of this com-plex anatomy easier and more useful to rhinologicsurgical approach. This improvement in imagingclarity and multiplanar demonstration of frontal si-nus complex anatomy is now of even more clinicalrelevance in view of the extensive developments inpowered instruments, better endoscopic devices, andsurgical navigation with CT cross-registration.
Embryologic and Functional Concepts
The sinonasal embryologic development during thefirst trimester is characterized by the emergence ofmore than six ethmoturbinals, which progressivelycoalesce and differentiate into the final anatomy ofthe lateral nasal wall [6].
The ethmoturbinals give rise to the following struc-tures:
� The most superior remnant of the first ethmo-turbinal becomes the agger nasi mound
� The remnant of the descending portion of thefirst ethmoturbinal becomes the uncinate pro-cess
� The basal lamella of the second ethmoturbinalpneumatizes and gives origin to the bulla eth-moidalis
� The basal lamella of the third ethmoturbinal be-comes the basal lamella of the middle turbinate.
Core Messages
� The frontal sinus and its drainage pathwaycomprise one of the most complex anatom-ic areas of the anterior skull base, amplifiedby significant variability
� Improvements in radiologic imaging clar-ity along with multiplanar demonstrationof frontal sinus complex anatomy have par-alleled and augmented advances in the sur-gical management of the frontal sinuses
Chapter 2
Radiologic Anatomy of the Frontal SinusRamon E. Figueroa, Joseph Sullivan
2
The nasal mucosa invaginates at specific points in thelateral nasal wall, forming nasal pits that develop intothe anlages of maxillary, frontal sinuses, and ethmoidcells [2]. The mesenchyme resorbs around the invag-ination of the nasal pits, allowing progressive devel-opment of the sinus cavity. The embryologic point atwhich the initial invagination occurs becomes the fu-ture sinus ostium. Cilia develop and orient towardsthis ostium, allowing mucus to flow towards andthrough the ostium. The efficiency of the mucociliarydrainage is then dictated and impacted by the paten-cy, tortuosity, and/or frank narrowing of the result-ing drainage pathways, which are progressively mod-ified by the sequential ongoing pneumatization pro-cess occurring during the patient’s life. Typically theethmoid cells and the maxillary antra are pneuma-tized at birth, with the maxillary antra progressivelyexpanding into mature sinuses as the maxilla ma-tures and the teeth erupt. The frontal sinus developsand expands in late childhood to early adolescence,and continues to grow into adulthood. The rate of si-nus growth is modified by the efficiency of ventila-tion and mucociliary drainage, dictated by the sinusostium and corresponding drainage pathways. Thefrontal sinus drainage pathway is the most complex
of all sinuses, impacted by its anatomic relationshipswith the agger nasi, anterior ethmoid cells, and pat-tern of vertical insertion of the uncinate process [3].
Frontal Sinus Evaluation
CT of the paranasal sinuses classically has been per-formed with continuous coronal and axial 3-mm slic-es to provide two planes of morphologic depiction ofsinus anatomy for presurgical mapping and evalua-tion [5]. Recent advances in CT scanner designs withthe introduction of multidetector helical designs andmuch larger and faster computing processing capac-ities now allow for single-plane thin-section high-resolution databases to be acquired and postproc-essed to depict the sinus anatomy in any planar pro-jection with high definition of the underlying anato-my. This multiplanar capability has impacted theevaluation of the frontal sinus drainage pathways themost, since depiction of this region in a sagittal planehas become routine.
Typical high-resolution multidetector scanning isperformed in the axial plane (Fig. 2.1A) following thelong axis of the hard palate, using a low MA tech-
Ramon E. Figueroa, Joseph Sullivan8
2
Fig. 2.1A,B.High-resolution sinus navigation CTprotocol. A Lateral scout view showsthe typical prescription of axial thinsection slices. B An axial image at thelevel of the nasal cavity helps pre-scribe the sagittal reformatted images
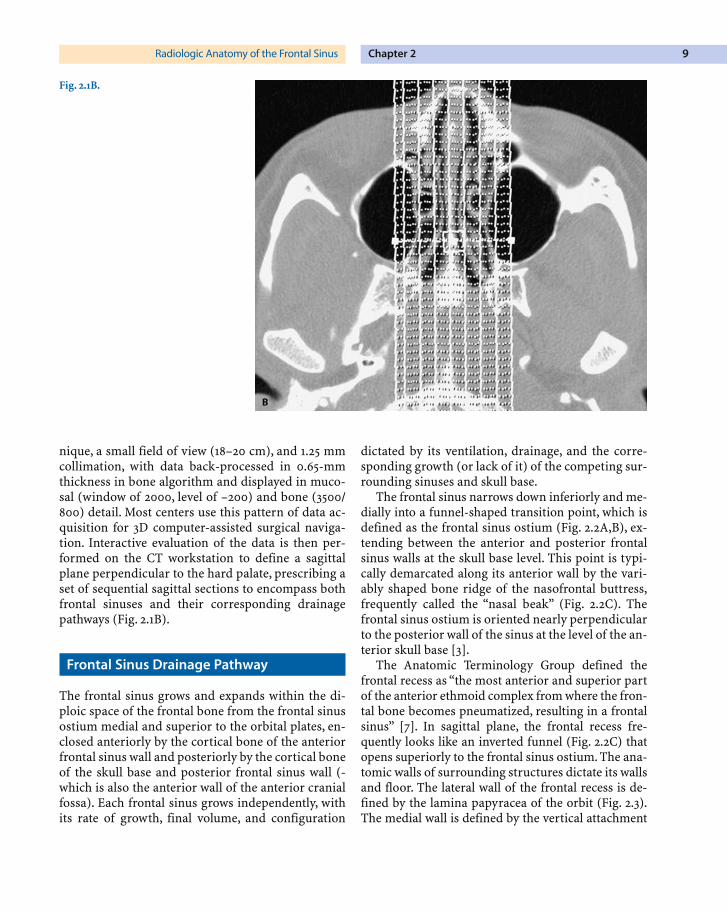
nique, a small field of view (18–20 cm), and 1.25 mmcollimation, with data back-processed in 0.65-mmthickness in bone algorithm and displayed in muco-sal (window of 2000, level of –200) and bone (3500/800) detail. Most centers use this pattern of data ac-quisition for 3D computer-assisted surgical naviga-tion. Interactive evaluation of the data is then per-formed on the CT workstation to define a sagittalplane perpendicular to the hard palate, prescribing aset of sequential sagittal sections to encompass bothfrontal sinuses and their corresponding drainagepathways (Fig. 2.1B).
Frontal Sinus Drainage Pathway
The frontal sinus grows and expands within the di-ploic space of the frontal bone from the frontal sinusostium medial and superior to the orbital plates, en-closed anteriorly by the cortical bone of the anteriorfrontal sinus wall and posteriorly by the cortical boneof the skull base and posterior frontal sinus wall (-which is also the anterior wall of the anterior cranialfossa). Each frontal sinus grows independently, withits rate of growth, final volume, and configuration
dictated by its ventilation, drainage, and the corre-sponding growth (or lack of it) of the competing sur-rounding sinuses and skull base.
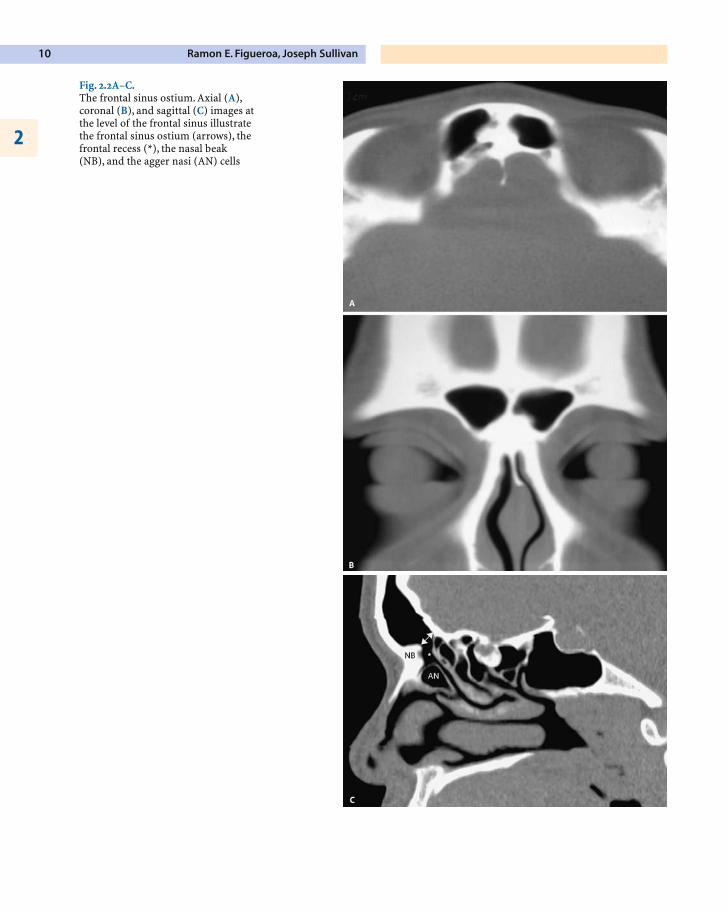
The frontal sinus narrows down inferiorly and me-dially into a funnel-shaped transition point, which isdefined as the frontal sinus ostium (Fig. 2.2A,B), ex-tending between the anterior and posterior frontalsinus walls at the skull base level. This point is typi-cally demarcated along its anterior wall by the vari-ably shaped bone ridge of the nasofrontal buttress,frequently called the “nasal beak” (Fig. 2.2C). Thefrontal sinus ostium is oriented nearly perpendicularto the posterior wall of the sinus at the level of the an-terior skull base [3].
The Anatomic Terminology Group defined thefrontal recess as “the most anterior and superior partof the anterior ethmoid complex from where the fron-tal bone becomes pneumatized, resulting in a frontalsinus” [7]. In sagittal plane, the frontal recess fre-quently looks like an inverted funnel (Fig. 2.2C) thatopens superiorly to the frontal sinus ostium. The ana-tomic walls of surrounding structures dictate its wallsand floor. The lateral wall of the frontal recess is de-fined by the lamina papyracea of the orbit (Fig. 2.3).The medial wall is defined by the vertical attachment
Chapter 2Radiologic Anatomy of the Frontal Sinus 9
Fig. 2.1B.
Ramon E. Figueroa, Joseph Sullivan10
2
Fig. 2.2A–C.The frontal sinus ostium. Axial (A),coronal (B), and sagittal (C) images atthe level of the frontal sinus illustratethe frontal sinus ostium (arrows), thefrontal recess (*), the nasal beak(NB), and the agger nasi (AN) cells

of the middle turbinate (its most anterior and superi-or part). Its posterior wall is variable, depending onthe basal lamella of the bulla ethmoidalis reaching (ornot) the skull base, if it is dehiscent allowing a com-munication with the suprabullar recess, or if it is hyp-er-pneumatized producing a secondary narrowing ofthe frontal recess from it posterior wall [2].
The agger nasi cells and the uncinate process dic-tate the floor and the pattern of drainage of the fron-tal recess. The frontal recess can be narrowed fromthe anterior-inferior direction by hyper-pneuma-tized agger nasi cells (Fig. 2.3). Its inferior drainage isdictated by the insertion of the vertical attachment ofthe uncinate process, a sagittally oriented hook-likebony leaflet (Fig. 2.4).Whenever the uncinate processattaches to the skull base or the superior-anteriorportion of the middle turbinate, the frontal recessdrains into the superior end of the ethmoidal infun-dibulum (Fig. 2.4A). If the uncinate process attaches
laterally into the lamina papyracea of the orbit(Fig. 2.4B), the frontal recess opens directly into thesuperior aspect of the middle meatus, and the eth-moidal infundibulum ends blindly into a “terminalrecess”.
The ethmoidal infundibulum is a true three-di-mensional space defined laterally by the lamina pap-yracea, anteromedially by the uncinate process, andposteriorly by the bulla ethmoidalis (Fig. 2.5A). Itopens medially into the middle meatus across thehiatus semilunaris inferior, a cleft-like openingbetween the free posterior margin of the uncinateprocess and the corresponding anterior face of thebulla ethmoidalis (Fig. 2.5B). It is the functional com-mon pathway of mucociliary drainage for the anteri-or ethmoid, agger nasi, and maxillary sinus mucus.The frontal sinus drainage can also drain through theethmoidal infundibulum if the uncinate process doesnot attach to the lamina papyracea of the orbit.
Chapter 2Radiologic Anatomy of the Frontal Sinus 11
Ramon E. Figueroa, Joseph Sullivan12
2
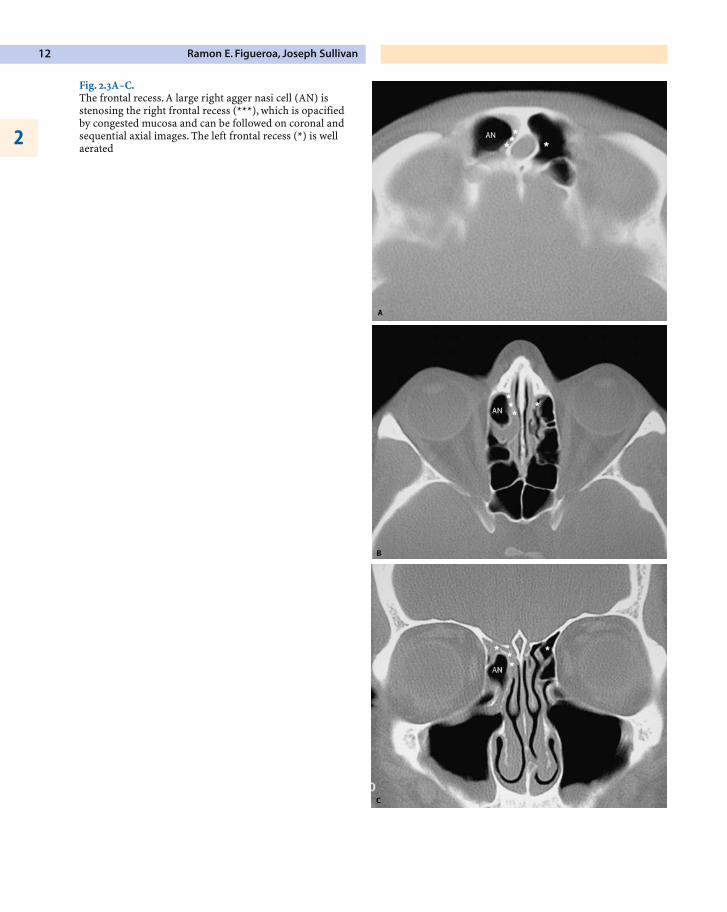
Fig. 2.3A–C.The frontal recess. A large right agger nasi cell (AN) is stenosing the right frontal recess (***), which is opacifiedby congested mucosa and can be followed on coronal andsequential axial images. The left frontal recess (*) is wellaerated
Chapter 2Radiologic Anatomy of the Frontal Sinus 13
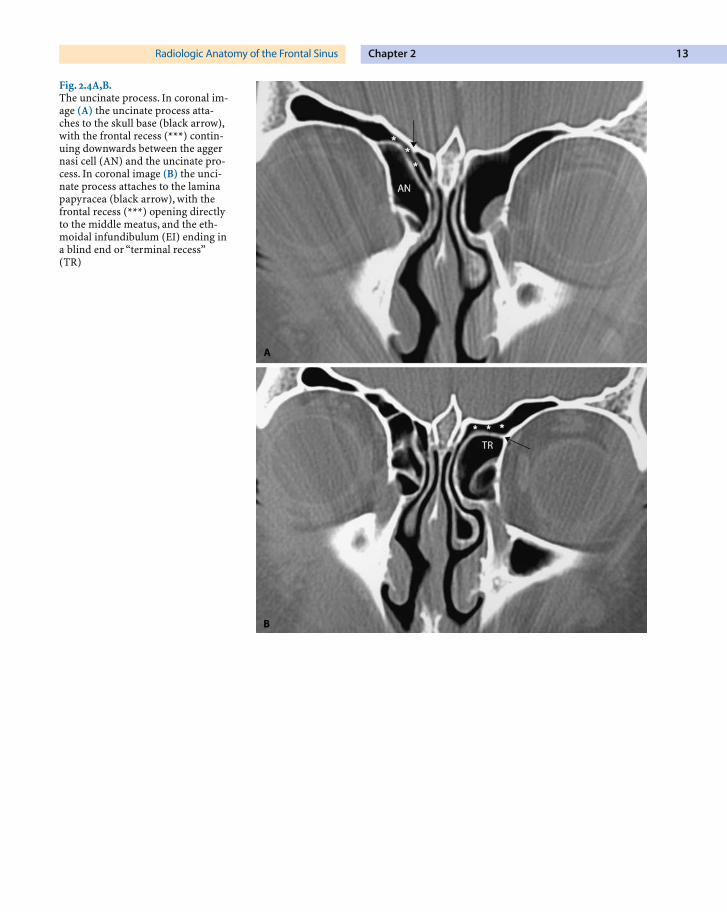
Fig. 2.4A,B.The uncinate process. In coronal im-age (A) the uncinate process atta-ches to the skull base (black arrow),with the frontal recess (***) contin-uing downwards between the aggernasi cell (AN) and the uncinate pro-cess. In coronal image (B) the unci-nate process attaches to the laminapapyracea (black arrow), with thefrontal recess (***) opening directlyto the middle meatus, and the eth-moidal infundibulum (EI) ending ina blind end or “terminal recess”(TR)
Ramon E. Figueroa, Joseph Sullivan14
2
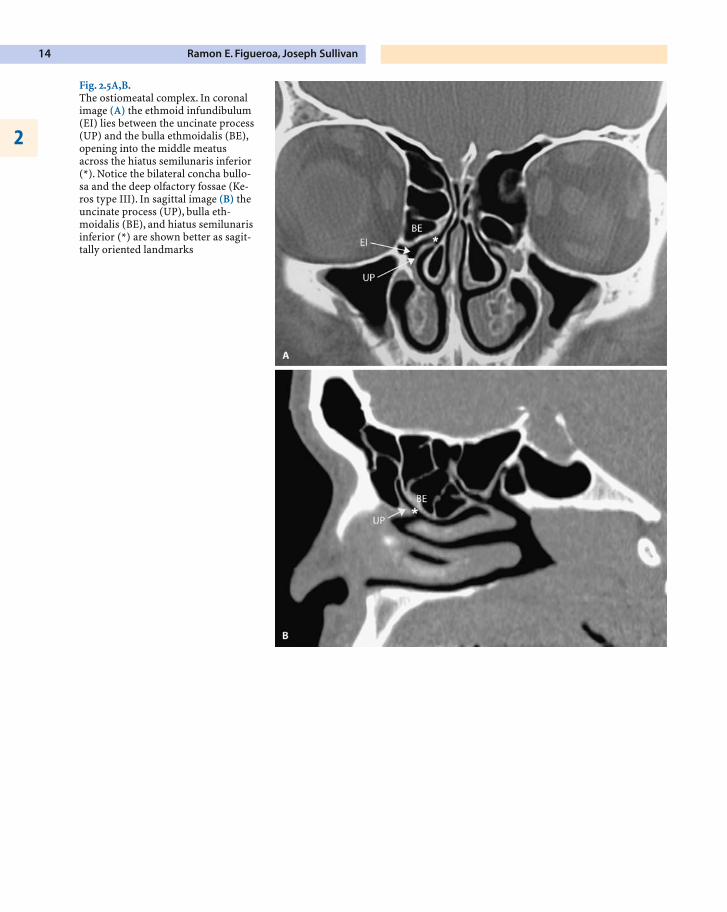
Fig. 2.5A,B.The ostiomeatal complex. In coronalimage (A) the ethmoid infundibulum(EI) lies between the uncinate process(UP) and the bulla ethmoidalis (BE),opening into the middle meatusacross the hiatus semilunaris inferior(*). Notice the bilateral concha bullo-sa and the deep olfactory fossae (Ke-ros type III). In sagittal image (B) theuncinate process (UP), bulla eth-moidalis (BE), and hiatus semilunarisinferior (*) are shown better as sagit-tally oriented landmarks
Anatomic Variants
Several important anatomic variants impact on theanatomy of the frontal sinus drainage pathways andthe anterior skull base. Familiarity with these ana-tomic variants is required for safe anterior skull baseand frontal recess surgical considerations.
Frontal Cells
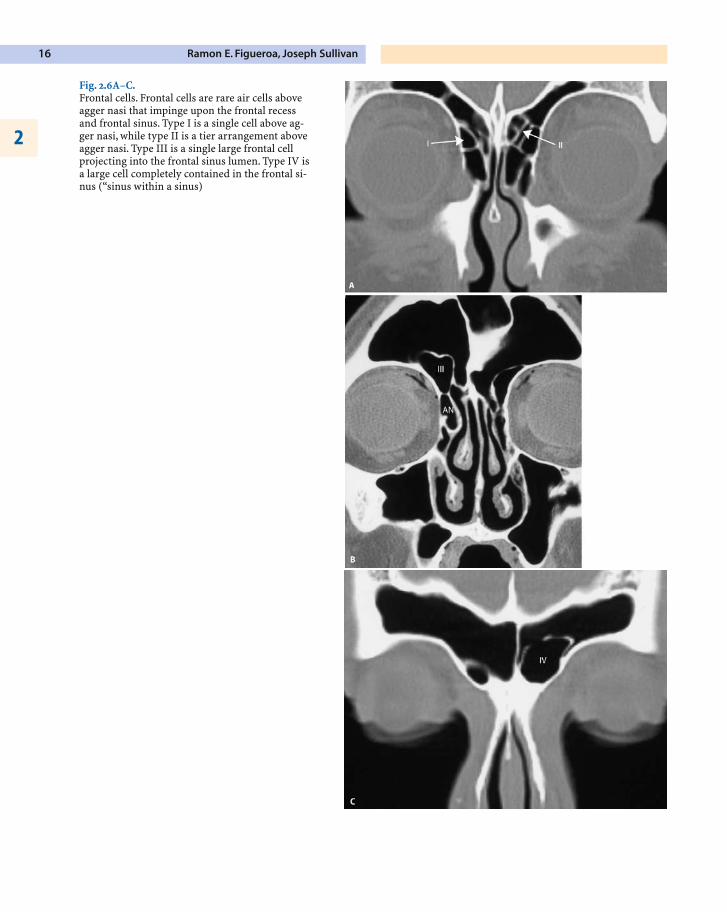
The frontal cells are rare anatomic variants of anteri-or ethmoid pneumatization that impinge upon thefrontal recess and typically extend within the lumenof the frontal ostium above the level of the agger na-si cells (Fig. 2.6). Bent and coworkers described fourtypes of frontal cells [1]. All frontal cells can be clini-cally significant if they become primarily infected orif they obstruct the frontal sinus drainage, leading tosecondary frontal rhinosinusitis.
The different types of frontal cells as described byBent are [1]:
� Type I frontal cell, a single frontal recess cellabove the agger nasi cell (Fig. 2.6A)
� Type II frontal cells, a tier of cells above theagger nasi cell, projecting within the frontalrecess
� Type III frontal cell is defined as a single mas-sive cell arising above the agger nasi, pneuma-tizing cephalad into the frontal sinus(Fig. 2.6B)
� Type IV frontal cell is a single isolated cellwithin the frontal sinus, frequently difficult tovisualize due to its thin walls (Fig. 2.6C)
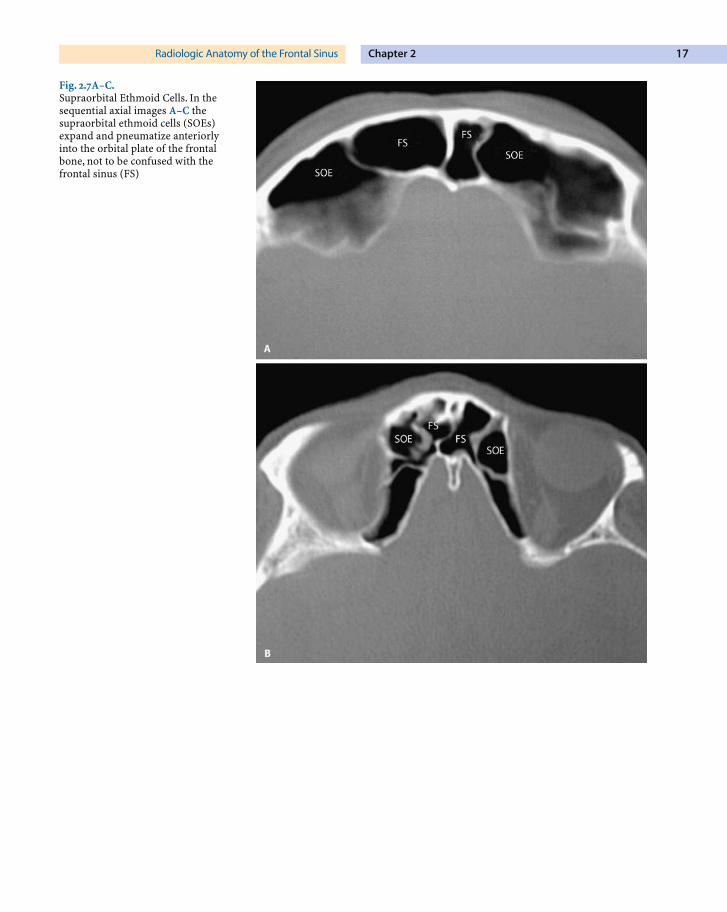
Supraorbital Ethmoid Cell
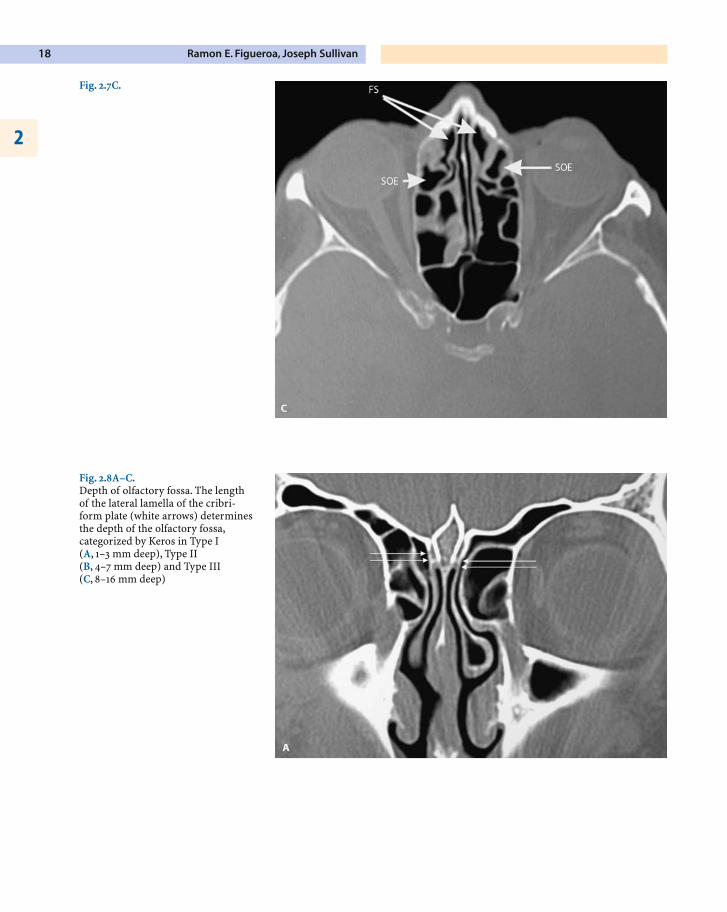
This is a pattern of pneumatization of the orbitalplate of the frontal bone posterior to the frontal re-cess and lateral to the frontal sinus (Fig. 2.7), fre-quently developing from the suprabullar recess [2].The degree of pneumatization of the supraorbitalethmoid cells can reach the anterior margin of theorbital plate and mimic a frontal sinus. Tracing backthe borders of the air cell towards the anterior eth-moid behind the frontal recess allows us to recognizethis variant better.
Depth of Olfactory Fossa
The orbital plate of the frontal bone slopes down-wards medially to constitute the roof of the ethmoidlabyrinth (foveola ethmoidalis), ending medially atthe lateral border of the olfactory fossa (Fig. 2.8). Thisconfiguration makes the olfactory fossa the lower-most point in the floor of the anterior cranial fossa,frequently projecting between the pneumatized aircells of both ethmoid labyrinths [7]. The depth of theolfactory fossa into the nasal cavity is dictated by theheight of the lateral lamella of the cribriform plate, avery thin sagittally oriented bone that defines the lat-eral wall of the olfactory fossa.
Chapter 2Radiologic Anatomy of the Frontal Sinus 15
Ramon E. Figueroa, Joseph Sullivan16
2
Fig. 2.6A–C.Frontal cells. Frontal cells are rare air cells aboveagger nasi that impinge upon the frontal recessand frontal sinus. Type I is a single cell above ag-ger nasi, while type II is a tier arrangement aboveagger nasi. Type III is a single large frontal cellprojecting into the frontal sinus lumen. Type IV isa large cell completely contained in the frontal si-nus (“sinus within a sinus)
Chapter 2Radiologic Anatomy of the Frontal Sinus 17
Fig. 2.7A–C.Supraorbital Ethmoid Cells. In thesequential axial images A–C thesupraorbital ethmoid cells (SOEs)expand and pneumatize anteriorlyinto the orbital plate of the frontalbone, not to be confused with thefrontal sinus (FS)
Ramon E. Figueroa, Joseph Sullivan18
2
Fig. 2.8A–C.Depth of olfactory fossa. The lengthof the lateral lamella of the cribri-form plate (white arrows) determinesthe depth of the olfactory fossa,categorized by Keros in Type I (A, 1–3 mm deep), Type II (B, 4–7 mm deep) and Type III (C, 8–16 mm deep)
Fig. 2.7C.