-
[CANCER RESEARCH 45, 4206-4214, September 1985]
Steroid Receptors in Human Lung Cancer1
Craig W. Seattle, Nancy W. Hansen, and Paul A. Thomas2
Division of Surgical Oncology, College of Medicine, University
of Illinois at Chicago [C. W. B.¡,and Division of Cardio-Thoracic
Surgery, Department of Surgery, West
Side Veterans Administration Hospital, Chicago, Illinois 60612
[N. W. H., P. A. T.]
ABSTRACT
We have determined that a significant incidence of specifichigh
affinity receptors for androgen (AR), estrogen (ER),
andglucocorticoid (GR) is present in normal adult human lung
andbronchogenic carcinoma cytosols. In contrast, a limited numberof
tumor cytosols bound progesterone. Binding characteristicsfor each
class of steroid hormones were similar to those reportedfor other
steroid-responsive normal and neoplastic tissues. ERwas evenly
distributed between squamous cell and adenocarci-
noma cytosols with a slightly lower affinity, but higher
contentthan normal lung. In normal lung, GR resolved into two
distinctbinding components based on affinity using a
dextran-coated
charcoal assay. AR in squamous cell carcinomas behaved in
asimilar manner. This was not observed when hydroxyapatite wasused
to separate bound from free ligand. When AR affinity andcontent
were stratified on the basis of tumor grade in squamouscell
carcinoma, the most undifferentiated tumors had a lower ARcontent
and higher affinity. In contrast, there was no differentiation of
AR content or affinity based on tumor grade in adenocar-
cinoma where AR also did not resolve into two distinct
groupsbased on binding affinity. Although related to tumor grade,
ARincidence and content were not related to stage of disease.
Inadenocarcinoma, initial results suggest GR affinity and
contentwere inversely related to degree of tumor differentiation,
whileGR content was slightly lower in poorly differentiated
squamouscell carcinomas. GR content in squamous cell carcinoma
increased slightly between Stages I and II and declined
significantlyin Stage II patients. This was not observed in
adenocarcinoma,where GR content appeared to increase with stage of
disease.Our results suggest that a significant incidence of
specific, highaffinity receptors for estrogen, androgen, and
glucocorticoid ispresent in nonsmall cell carcinomas of the lung,
which couldprovide a useful starting point for examining whether
steroidsinfluence the natural history of selected bronchogenic
carcinomas.
INTRODUCTION
Steroids, particularly glucocorticoids and estrogens,
regulatemammalian lung differentiation and maturation (1-4).
Glucocor
ticoids accelerate the maturation of type II alveolar epithelial
cellswhich produce surfactant (5) and induce protein synthesis (6,
7)in rabbit lung. The effects of glucocorticoids in rat and
rabbitappear mediated by specific, high affinity, cytoplasmic and
nuclear receptors, particularly in pulmonary type II cells (8, 9).
Inhumans, glucocorticoids also stimulate fetal surfactant
production (10), possibly via specific glucocorticoid receptors on
type IIpneumocytes (11).
Estrogens also directly alter fetal lung differentiation and
maturation (12). In the presence of maximal stimulatory amounts
ofglucocorticoid, low doses of estrone and estradiol increase
pulmonary surfactant production, while higher doses are
inhibitory(2). Estradiol binds to fetal guinea pig (13) and adult
rat lungcytosols (14), sedimenting as a 4S species (15). Human
fetal andadult lung also bind estradiol (10, 16, 17), albeit with a
slightlylower affinity.
Like estrogen, androgens bind to cytosols from fetal and
adultrat lung (14, 18) with no apparent sex difference in
androgenbinding.
In addition to promoting surfactant production and cell
growth,hormones also strikingly alter the ultrastructural
morphology ofhuman lung expiants. Addition of cortisol, prolactin,
and insulinin vitro induces the formation of lamellar bodies in
type II pneumocytes (3).
These studies suggest that bronchogenic carcinomas arisingfrom
hormone-responsive cells could retain, and perhaps magnify, some of
the characteristics of the hormone-responsive
state.One potential mechanism for the action of steroids on
primary
bronchogenic carcinoma is receptor mediation. Receptors
forestrogen (16,19, 20), androgen (16, 20), and glucocorticoid
(16,21) are present in histologically diverse primary and
metastaticbronchogenic carcinomas. Tumor receptor incidence is
variable,however, and may be dependent on either the histogenetic
originof the lesion or method of assay. To date, no systematic
attempthas been made to characterize steroid binding in normal
lungand primary bronchogenic carcinoma cytosols in a large seriesof
patients under different assay conditions. The present studyreports
that a significant incidence of specific, high affinity receptors
for androgen, estrogen, and glucocorticoid is present innormal and
bronchogenic carcinoma cytosols.
MATERIALS AND METHODS
Materials. [1,2-3H]DEX3 (20.8 Ci/mmol), [2,4,6,7-3H]estradiol
(96 Ci/mmol), [3H]R5020 (promogestone), a synthetic progestin
(70-87 Ci/mmol), and [3H]R1881, a synthetic androgen (70-87
Ci/mmol) were
purchased from New England Nuclear (Cambridge, MA) and
repunfiedprior to use. Radioinert steroids were purchased from New
EnglandNuclear and Sigma Chemical Co. (St. Louis, MO). Trizma base,
EDTA,HAP, molybdic acid sodium salt, crystalline bovine serum
albumin, -
monothioglycerol, dithiothreitol, glycerol, phospholipase A,
DNase,Rnase, and trypsin were also purchased from Sigma. Activated
charcoal,ammonium sulfate, and additional reagents were purchased
from J. T.Baker Co. (Phillipsburg, NJ), and RNase-free sucrose was
from
1Supported by the Veterans Administration Research and
Development Service.2To whom requests for reprints should be
addressed, at the Division of Cardio-
Thoracic Surgery, Department of Surgery, West Side Veterans
AdministrationHospital, 900 S. Damen, Chicago, IL 60612.
Received 1/22/85; revised 5/23/85; accepted 6/5/85.
3The abbreviations used are; DEX, dexamethasone acetate
(9-fluoro-11,17-dihydroxy-16-methylpregna-1,4-diene-3,20-dione
diacciate); DCC, dextran-coatedcharcoal; R5020,17,21
-dimethyl-19-norpregna-4,9-diene-3-one;
R1881,17«-meth-yltrienolone; HAP, hydroxyapatite; DTT,
dithiothreitol; ER, estrogen receptor; PGR,progesterone receptor;
AR, androgen receptor; GR, glucocorticoid receptor;
DES,diethylstilbestrol; DHT, dihydrotestosterone.
CANCER RESEARCH VOL. 45 SEPTEMBER 1985
4206
on July 10, 2021. © 1985 American Association for Cancer
Research. cancerres.aacrjournals.org Downloaded from
http://cancerres.aacrjournals.org/
-
RECEPTORS IN LUNG CANCER
Schwartz-Mann (Orangeburg, NY). Dextran T-70 was obtained
fromPharmacia (Piscataway, NJ). ACS scintillation cocktail was from
Amer-sham-Searle Corp. (Arlington Heights, IL).
Methods (Tumor and Normal Lung Specimens). Fifty-five lung
can
cer tissue specimens were obtained from 55 adult patients
undergoingprimary surgery for lung cancer: 52 were obtained from
male patientsand 3 from female patients. Thirty (56%) were squamous
cell carcinomas,21 (38%) were adenocarcinomas, and 4 (7%) were
anaplastic large celltumors. All tumros were verified
histologically and staged using thecriteria established by the
American Joint Committee for Cancer Staging(22). Twenty-seven
specimens of histologically normal ventilating lung
were recovered from 30 of the patients with squamous cell lung
cancer,17 of the 20 patients with adenocarcinoma and all of the
patients withlarge cell anaplastic carcinomas.
All specimens were obtained during surgery when a portion of
thespecimen was sent for histopathological diagnosis (light and
electronmicroscopic examination). The remaining tumor was trimmed
of anynecrotic tissue on ice, washed with ice-cold saline, blotted
on sterile
gauze, and immediately frozen in liquid nitrogen. Normal lung
specimenswere verified histologically free of tumor prior to
receptor assay. Totalelapsed time from removal of specimen to
freezing was less than 15min. Receptor analysis was either
performed immediately or within 1 wkfollowing surgery. Storage
during this time was at -80°.
Receptor Analysis (DCC). Tumor and normal specimens were
initiallyanalyzed for cytosol receptor for ER, PGR, AR, and GR by
the standardDCC technique as previously reported (16). Specimens
for assay wereweighed while frozen and powdered in a tissue
pulverizer (ThermovacIndustries, Copiague, NY) at liquid nitrogen
temperatures. All subsequentsteps were performed at 0-4°C. The
powdered tissue was homogenized
1:6 (w/v) with two 10-s bursts in a P-10 homogenizer (Brinkman
Instruments, Westbury, NY) separated by a 30-s cooling period in
the followingbuffer systems: estrogen, 10 mw Tris-HCI:5 mw EDTA:1
mw DTT (pH7.4); androgen and glucocorticoid, 20 HIM Tris-HCI:5 rriM
EDTA:12 mM«-monothioglycerol:10% (v/v) glycerol with or without 20
mw sodiummolybdate (23) (pH 7.4); progesterone, 10 mw Tris-HCI:5 mw
EDTA:10ITIMa-monothioglycerol:10% (v/v) glycerol with or without 20
mM sodium
molybdate (pH 7.4). The homogenate was centrifugea at 105,000 x
g«,(Beckman L8-70 centrifuge; Beckman Instruments, Palo Alto, CA)
for 50
min, and the supernatant solution was defined as cytosol. All
cytosol swere diluted to 2-5 mg of protein per ml (24) with the
appropriate buffer
for receptor assay. Cytosols assayed for ER were divided into
twoportions, and one half was precipitated with (NH4)2SO4(40%
saturation)in an attempt to reduce the amount of nonspecific
binding in the DCCassay. The other half was assayed for ER using
HAP to separate boundfrom free ligand (25). Concentrations of
[3H]estradiol between 0.1 and
5.0 nw (minimum of eight points) were used in each 200-/il
cytosol assayin the presence and absence of a 100-fold excess of
radioinert DES. AllAR binding assays were carried out at 4°Cfor 16
h and incorporated a
100-fold excess of triamcinolone in addition to a 100-fold
excess ofradioinert R1881 to reduce the binding of [3H]R1881 to
PGR. Bindingwas determined over a range of 0.1-10 nw [3H]R1881
(minimum of eight
points) (26). PGR assays contained a 100-fold excess of cortisol
toreduce any potential binding of [3H]R5020 to the glucocorticoid
receptor.Binding of [3H]DEX was determined at 4°Cfor 18 h over a
concentration
range of 0.25-25 nw (minimum of eight points). Radiolabeled
cytosolswere counted in 8 ml of ACS cocktail at an efficiency of
36-38% in lowK ' glass vials and corrected to dpm automatically in
a Beckman LS-
7500 liquid scintillation counter. Specific binding (content,
measured asfmol/mg of cytosol protein) and affinity (measured as
Kd) were calculatedfor each sample according to the methods of
Scatchard (27) and Hill(28). No changes in binding content or
affinty in additional tumor ornormal lung specimens were found when
stored at -80°C over a 2-3
wk interval.HAP. The incidence of ER, AR, and GR was also
determined using
HAP to insure that DCC separation of bound from free ligand
wouldaccurately estimate high affinity, low capacity sites in the
presence of
substantial lower affinity (100 nM) binding. HAP (DNA grade) was
madeup to 60% with appropriate buffer following washing of fines,
and 200-
>ilaliquots were added to each incubation tube. The HAP
complex wascentifuged at 3000 x g for 15 min, washed 3 times with
buffer at 4°C,and extracted with 1 ml of absolute alcohol at
30°Cfor 15 min (25). The
alcohol was decanted and counted as above.Sucrose Gradients.
Frozen tumor specimens were weighed, pulver
ized at liquid nitrogen temperatures, and homogenized at 4°C in
the
appropriate buffer (1:4, w/v). Following centrifugation for 1 h
at 105,000x gm, all the supernatant solutions (cytosols) were
removed, and thepellet was discarded. Cytosol aliquots were
incubated for 4 h (AR, ER)or 20 h (GR) at 0-4°C with 5 nM
[3H]estradiol, 10 nM [3H]R1881, or 20nM [3H]DEX with or without a
100-fold excess of radioinert steroid.
Unbound ligand was removed by incubation with a 1-ml DCC pellet
for15 min at 4°Cand centrigued at 3000 x g for 15 min. A 250-//I
aliquot
was layered on top of a 4.7-ml 10-30% sucrose gradient and
centrifugea
at 250,000 x gav in a SS50.1 rotor for 16 h. Additional
gradients for ARand GR incorporated 0.4 M KCI or 20 mM sodium
molybdate. methyl-14C-labeled bovine serum albumin was used as a
4.6S reference marker
according to the method of Martin and Ames (29). Each tube
waspunctured, and 135-^1 fractions were collected under a constant
pressure
head and counted in 6 ml of ACS cocktail.Specificity and
Stability Analysis. Specificity of binding for androgen
and glucocorticoid was determined by incubating competing
radioinertligands with 10~9 M [3H]R1881 and 10"8 M [3H]DEX in
cytosols from
normal lung for 20 h at 4°Cand separating bound from free
ligand with
HAP. The degree of competition is expressed as percentage of
bound3H-ligand with the binding of 3H-ligand in the absence of
competitor taken
as 100%. Concentrations of radioinert competing ligand ranged
from10^-10"9 M. Receptor stability in the presence of phospholipase
A,
DNase, RNase, trypsin, and (NH4)2SO4(40% saturation) was
determinedin the presence and absence of 20 mM molybdate ion.
Additional stabilitystudies were carried out at 30°C and 37°C in
the presence of 20 mw
molybdate ion.Statistical Analysis. A value over 3 fmol/mg of
cytosol protein was
determined by Scatchard analysis was arbitrarily taken as
positive fortumor specimens in our earlier studies (16). No
arbitrary cutoff wasestablished for receptor binding to tumor or
normal lung cytosols in thecurrent study. The difference in
receptor incidence of any particular classof receptor among
histological groups was analyzed by Fisher's exact
test (30). Receptor content and affinity among groups were
analyzed byeither analysis of variance for multiple group
comparisons or simple ttest (30).
RESULTS
Receptor for Estrogen and Progesterone. [3H]Estradiol
bound to approximately 30% of normal lung cytosols assayedwhen
HAP was used to separate bound from free ligand (Table1). ER
incidence, content, and affinity (Ka) were similar in squamous cell
cancer cytosols when assayed by either DCC followingammonium
sulfate precipitation, DCC alone (data not shown), orHAP in the
presence of 20 mM molybdate ion (Table 1). In spiteof the limited
binding capacity, receptor affinity was generallylower than 1 nw.
There was no suggestion of multiple bindingsites on Scatchard
analysis when either DCC or HAP was usedto separate bound from free
ligand or when radioinert DES wasused as a competitive ligand. A
similar ER profile was found inadenocarcinoma cytosols assayed by
HAP. When present, binding was resistant to phospholipase A, DNase,
and RNase butsensitive to trypsin and maximal at 4 h at 4°Cin the
presenceof 5 nw [3H]estradiol (data not shown). ER prepared from
a
squamous cell carcinoma cytosol sedimented at 7-8S on a 10-
30% low salt sucrose gradient (Chart 1), suggesting the
binding
CANCER RESEARCH VOL. 45 SEPTEMBER 1985
4207
on July 10, 2021. © 1985 American Association for Cancer
Research. cancerres.aacrjournals.org Downloaded from
http://cancerres.aacrjournals.org/
-
RECEPTORS IN LUNG CANCER
Table 1Incidence of ER and PGR in normal lung and bronchogenic
carcinoma
PGR affinity and content were estimated over a concentration
range of 0.1-10 nM [3H]R5020 at 4°Cfor 16-18 h. Bound and free
ligand were separated by DCC. ER
assayed by DCC were first precipitated by (NH4)2SO
-
•-V"?
RECEPTORS IN LUNG CANCER
though apparent affinity was lower. In line with this
observation,HAP did increase the ratio of specific to nonspecific
binding inthe presence of molybdate and was therefore used to
separatebound from free ligand in specificity and saturability
studies.There was virtually no contamination of the tissue
specimens byblood proteins (as judged by hemoglobin content) due to
priorthorough washing in ice-cold saline prior to freezing. GR
binding
in four cytosols prepared from histologically normal lung
fromnoncancer patients was similar to that from normal lung
cytosolsobtained from patients with bronchogenic carcinoma (Kd 4.7
±1.9 nM, 76.1 ±34.5 fmol/mg of protein; range, 9.1-147.3; n =
4), suggesting that there was little, if any, indirect effect on
GRin normal lung tissue specimens by the primary carcinoma.
Binding of [3H]DEX to normal lung (Chart 2) and
bronchogeniccarcinoma cytosols (data not shown) was specific for
glucocor-
ticoids, saturable (Chart 3), and trypsin sensitive. Maximal
binding (fmol/mg of protein) was observed at 15 and 30 min at
37°and 30°C, respectively, with approximately 50% of apparent
receptor binding degraded after 2 h at either temperature.
At4°C,binding of [3H]DEX did not plateau until approximately
20
h (Chart 3) but was saturable at 20-25 nw (data not shown)
and
may represent equilibrium between higher and lower affinity
sitesfor glucocorticoid. Following a 20-h incubation with 20 nw
[3H]-
DEX, GR sedimented at 9.8S in low salt 10-30% sucrose
gradients, 11.28 in the presence of molybdate (Chart 4A), and4S
in the presence of 0.4 M KCI (Chart 40) when molybdate wasomitted
from the incubation buffer and gradient. GR was also
100H
90
80
i70C 60O
% 50
¡40
30
20
10
1
10-9 10-8 10-7 10-6
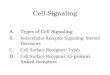
MOLAR CONCENTRATION OF COMPETITORChart 2. Specificity of [3H]DEX
(20 mM) binding to normal lung cytosols in the
presence of 20 mM MoO4. O, DEX; •,R1881; A, progesterone; A,
R5020; x,estradici; G, DHT. HAP separation bound from free
ligand.
1 2 3 4 5 6 16 18 20 22 24 26TIME(hr)
Charts. GR stability in the presence of 20 mM MoO4 at 4°C.
Binding of[3H]DEX was saturable only after 18-20 h at 20-25 HM. HAP
separation bound
from free ligand.
present in 17 of 22 (77%) squamous cell carcinoma
cytosolsassayed by DCC with a mean binding affinity and content
similarto those of normal lung cytosols assayed in the same
manner(Table 2). An additional eight specimens assayed with HAP
allexpressed a similar binding profile. Ten of 12 (83%)
adenocarci-noma cytosols bound [3H]DEX when assayed by DCC, while
8of 8 bound [3H]DEX when assayed with HAP. There was no
significant difference in GR affinity or content between
methodsor between control and tumor cytosols (Table 2). GR
contentwas significantly higher in adenocarcinoma cytosols with
anaffinity for [3H]DEX > 10 nM as determined by DCC when
compared to normal lung cytosols with the same affinity.
Thisalso appeared to be the case in four cytosols from large
cellanaplastic lesions, although the number of these latter
tumorswas small (Table 2).
Receptor for Androgen. R1881 bound with high affinity
butrelatively low capacity to 22 of 24 (92%) normal lung
cytosolsassayed by DCC (Table 3) with minimal cross-reactivity
from
other steroids (Chart 5). A similar specificity profile was
developed for squamous cell and adenocarcinoma cytosols (data
notshown). Binding of [3H]R1881 was saturable at the
temperature
tested, and like GR, it reached maximal concentrations at 15
and30 min at 37° and 30°C, respectively. Unlike GR,
however,binding plateaued at 4 h at 4°Cwith 10 HM[3H]R1881 (Chart
6)
and did not resolve into two groups with distinct
affinities.Receptor for androgen sedimented at 7S in low salt
gradients,11S in the presence of 20 mw molybdate (Chart 7), and
shiftedto a lower molecular weight 48 species in 0.4 M KCI.
[3H]R1881
also bound to a significant number of squamous cell (60%)
andadenocarcinoma cytosols (87%) specifically and with high
affinity(Table 3). In contrast to normal lung cytosols, the
relative affinityof the putative receptor for androgen in squamous
cell carcinomacytosols in the presence of 20 mM molybdate was
resolvableinto two distinct groups when assayed by DCC. Seven of
12(58%) of the squamous cell carcinoma cytosols binding [3H]-
R1881 bound the ligand in a nanomolar range, while the remaining
five (42%) expressed binding below 1 nM. Mean content was,as in the
case of GR, inversely proportional to receptor affinity.
CANCER RESEARCH VOL. 45 SEPTEMBER 1985
4209
on July 10, 2021. © 1985 American Association for Cancer
Research. cancerres.aacrjournals.org Downloaded from
http://cancerres.aacrjournals.org/
-
ce
a.
lOOO-
900-
800-
700-
500-
400 -
300-
200-
KX>-
RECEPTORS IN LUNG CANCER
BSA 4 6s
BSA 46s
3000 -
2000-
CL0 1000 -
B
BOTTOM 5 K) 15 20 25FRACTION NUMBER
30 35 TOP BOTTOM 5 10 15 20 25FRACTION NUMBER
30 35 TOP
Chart 4. A, sucrose gradient of [3H]DEX binding to normal lung
cytosols under low salt conditions. •,[3H]DEX; O, [3H]DEX:20 HIM
MoO4; A, [3H]DEX plus 100-fokJexcess unlabeled DEX. B, sucrose
gradient of [3H]DEX binding to normal lung cytosol in the presence
of 0.4 M KCI. •,[3H]DEX; O, [3H]DEX plus 100-fold excess of
labeled DEX.
Table 3
Incidence and binding characteristics of AR in normal lung
parenchyma andbronchogenic carcinoma
HistopathologyNormal
lungDCC
HAPSquamous
cellDCCHAPAdenocarcinoma
DCCHAPLarge
cellDCCN/T823/25
(92)0
14/15(93)12/18(67)
5/12 (42)"
7/12 (58f4/5(80)7/8
(88)7/8(88)2/4
(50)Affinity
Ka(nw)0.4
±0.05°
0.3 ±0.061.7
+ 0.50.2 ±0.04f
2.9 ±0.90.4 ±0.20.6
+ 0.20.4 +0.10.3
+ 0.1ARContent
(fmol/mgprotein)6.3
+ 0.8"
2.6 +0.510.1
±3.24.2 ±2.39
14.4 ±4.71.6 ±0.23.3
±0.91.9 +0.32.6
±1.68 N/T, number positive/number assayed." Numbers in
parentheses, percentage.c Mean ±SE.dP
-
RECEPTORS IN LUNG CANCER
10-9 10-8 10-7 10-6
MOLAR CONCENTRATION OF COMPETITORCharts. Specificity of
[3H]R1881 (1 nu«)binding to normal lung cytosol in the
presence of 20 mM MoO4. O, R1881; •,DHT; A, estradici;
•,progesterone; ®,DEX:cortisol. HAP separation of bound from
free ligand.
5 6 16TIME (hr)
18 20 22 24 26 28
Charte. Stability of AR in the presence of 10 nu [3H]R1881. At
4°Cbinding
was saturable at 4 h and stable for 24 h. Receptor ligand
dissociation was rapid at37°Cin the presence of 20 mM MoCv HAP
separation of bound from free ligand.
10.2 fmol/mg of protein, n = 5) and a sharp decline in Stage
IIIlesions (32.8 ±8.0 fmol/mg of protein, n = 11). When lesions
ofStages I and II were grouped, the mean GR content was greaterthan
in Stage III lesions (6.1 ±9.2 fmol/mg of protein versus32.8
±8.0, P < 0.05).
This was not observed in adenocarcinomas where there wasan
increase in mean GR content with stage of disease (Stage I,53.1
±11.8 fmol/mg of protein, n = 6; Stage II, 84.2 ±9.4 fmol/
1000
900
800
700
O 600
£ 500
o 400
300
200
100
[14c]BSA4.6s
BOTTOM 5 10 15 20 25FRACTION NUMBER
30 35 TOP
Chart?. Sucrose gradient profile of [3H]R1881 binding to normal
lung cytosols
under low salt conditions. While capacity was limited (Table 3),
suppression bindingwas demonstrable at ~7S and 4S in the absence of
MoO4 and at 11S in thepresence of 20 mM MoO. (•).A, 13H|R1881
plus 100-fold excess unlabeled R1881.
mg of protein, n = 3; Stage III, 115.8 ±29.7 fmol/mg of
protein,n = 5) in GR-positive lesions. The two AR-negative lesions
were
removed from a Stage I and Stage III patient. While the
smallnumber in each group prevents this increase from
reachingstatistical significance, it suggests that GR content of
the primarytumor increases as the disease progresses. There was no
relationship between stage of disease and the presence or
absenceofGR.
DISCUSSION
The present results suggest that a significant incidence
ofspecific receptors for androgen, estrogen, and glucocorticoidwith
an affinity for hormone similar to those in other
steroid-responsive tissues (8, 11, 13, 14, 17,18, 23, 31-35) is
present
in normal adult human lung and bronchogenic carcinoma cytosols.
The presence of a single class of high affinity (
-
RECEPTORS IN LUNG CANCER
Table 4Androgen and glucocorticoid receptor content as a
function oÃ-tumor grade
HistopathologySquamous
cellAdenocarcmomaGradel-llIII-IVl-ll
III-IVN/T*1
2/1 7 (71 f4/6(67)3/3
(100)11/13(85)ARAffinity
K«(nM)1.9±0.7°
0.25 ±0.060.3
±0.050.6 ±0.2Content
(fmol/mgprotein)9.3
±3.51.7±0.72.2
±0.53.0 ±0.7N/T19/23
6/73/3
13/13GRAffinity
Ka(nM)6.4
±1.15.0±2.515.1
±3.57.8±0.8Content
(fmol/mgprotein)47.1
±9.338.9 ±17.238.1
±15.688.6 ±13.2
* N/T, number positive/number assayed.13Numbers in
parentheses,percentage.: Mean ±SE.
squamous cell cytosols when OCC was used to separate boundfrom
free ligand in the absence of molybdate ¡on(16,20,36) andsuggest
the importance of assay conditions when attempting todetermine
small amounts of receptor in the presence of significant amounts of
nonspecific binding. In this context, Jones et al.(19) have
reported an overall ER incidence of 55% in squamouscell and
adenocarcinoma cytosols with binding characteristicsclose to the
present study using Sephadex G-25 to separate
bound from free ligand. The choice of an arbitrary cutoff
incontent as indicative of positive for receptor may also
accountfor the reported differences in ER incidence (16,36). The
numberof specimens available for assay in the present study was
toosmall to draw any correlation between degree of
histológica!differentiation and ER incidence or content. While a
significantincidence of ER in adult lung parenchyma provides
initial evidence that estrogens may continue to influence lung
function inadults, additional studies will be necessary to better
define theincidence and determine the functionality of this
estrogen bindingprotein in adult human lung.
PRG incidence, while relatively high in normal lung,
declinedsignificantly in tumor cytosols confirming earlier
observations(16, 20). There was no correlation between the presence
of ERand PGR. These observations coupled with the lack of
receptorin tumor cytosols and absence of relationship between
putativeprogesterone binding and fetal lung function (12, 37)
suggest aminor role for progesterone in lung homeostasis. Reports
ofdisplacible [3H]R5020 binding in fetal rabbit lung (18) may
reflect
a lower affinity, potentially less specific binding protein or
aspecies difference. A larger series of cytosols will have to
beassayed to resolve this question.
Androgen(s) clearly exhibit specific, high affinity, low
capacitybinding to normal adult human lung cytosols. While the
presenceof a cytosol receptor does not necessarily indicate a role
forandrogens in fetal lung development (12) and in the function
ofadult lung, the high incidence (93%) of AR and similarity to
thebinding characteristics reported for fetal and adult rabbit
lung(18) and adult rat lung (14) suggest that this is a viable
possibility(16). The presence of molybdate appears essential to
reproduc-
ibly resolving the low capacity AR sites, particularly in
tumorcytosols, as our own initial results (16) and those of others
(20)omitting MoQ»from the assay system showed a lower incidenceof
AR. AR in squamous cell carcinoma was present in twopotentially
distinct species based on receptor affinity using theDCC assay.
Cytosols assayed at the same protein concentration(1-2 mg/ml) bound
[3H]R1881 with an affinity either above or
below 1 nM. This was not observed in a smaller series of
cytosolswhen HAP was used to separate bound ligand.
Each Scatchard analysis gave a linear plot further suggestingtwo
distinct species are observable when DCC is used to separate bound
from free ligand in the presence of MoO4. This is thefirst report
of such a phenomenon in tumors of squamous cellorigin, and as yet
we have no definitive explanation for it. [3H]-
DHT does, however, bind to normal skin squamous cell cytosolsas
two distinct species (38). Alternatively the expression of ARmay be
dependent on tumor grade or stage. Although AR affinity(content)
did not appear related to tumor grade or stage ofdisease, our
series was too small to statistically evaluate properly. It should
be reiterated, however, that AR-negative lesionswere either
undrfferentiated or poorly differentiated (Grades III-IV). Previous
reports on AR in squamous cell lung cytosols showK,,s in a range of
0.1-1.0 nM (16, 20) with normal human lung
less than 1 nM (16), similar to those in the present study.
Incontrast, AR affinity in adenocarcinoma cytosols exhibited onlya
single class of high affinity sites identical to that reported
forAR in adenocarcinoma of the breast (31, 32).
GR was present in 82% of normal lung specimens assayed.Sucrose
gradient analysis and specificity studies show the binding protein
to be virtually identical with that reported for fetal andadult
rabbit, rat, and human lung (4, 6, 8, 11, 35, 39). Ourobservations
suggest that glucocorticoids may continue to influence lung
function in adult human lung, possibly via receptor-
mediated processes. When present in normal lung, GR
wasresolvable into two distinct binding moieties based on Kd
whenassayed in the presence of MoO4 using DCC. This could be
afunction of the assay system as GR-positive specimens gave a
linear Scatchard analysis with a Ka either above or below 10
nM.Alternatively this may indicate that functionally there is a
differential sensitivity to endogenous or exogenous glucocorticoids
inadult human lung. An analogous situation appears to be presentin
fetal rabbit lung. Pulmonary surfactant synthesis in fetal
rabbitlung is sensitive to lower exogenous concentrations (10~10M)
ofcortisol than cell growth (10 8 M) (5, 39) and additional
proteinsynthesis (10~7 M) (6, 7), while cultured fetal rabbit lung
bindsglucocorticoid at roughly 10~8 M (9). Adult rat and rabbit
lung
cytosols have also been reported to bind glucocorticoid in
ananomolar range as have rabbit alveolar macrophages (8, 34).When
the latter are activated by glucocorticoids, there is anincrease in
the number of binding sites (34). The slow saturationof GR at
4°C,absent in AR and ER binding but present in normal
human fetal and neonatal cytosols (11), also suggests a
multi-
component binding system of potential physiological and
pharmacological interest. Additional studies are needed to clarify
thispoint.
Squamous cell carcinomas also show a significant incidence
CANCER RESEARCH VOL. 45 SEPTEMBER 1985
4212
on July 10, 2021. © 1985 American Association for Cancer
Research. cancerres.aacrjournals.org Downloaded from
http://cancerres.aacrjournals.org/
-
RECEPTORS IN LUNG CANCER
of binding. The incidence of binding in squamous cell
carcinomais significantly higher than previously reported (16, 21)
usingDCC in the absence of molybdate. Binding affinity (nw)
wassimilar to that reported for GR in other neoplastic tissues
(21,31-33, 40). A single class of high affinity receptors for
[3H]DEX
was also present in essentially all primary adenocarcinomas
ofthe lung assayed by either DCC or HAP. These results confirmour
earlier observations (71%) (16) and suggest that GR contentis
greater in adenocarcinoma than normal lung cytosols whengroups with
similar binding constants are compared.
Demonstration of high affinity cytosol receptors for
androgensand glucocorticoids in squamous cell and adenocarcinomas
ofthe lung tempts speculation that these lesions may be manipulated
by increasing or decreasing the level of glucocorticoid.Early
studies suggest that administration of low doses of cortisone was
associated with an apparent decrease in survival inpatients with
metastatic lung carcinomas (41). In contrast, dex-
amethasone has been reported to decrease the growth of alveolar
cell carcinoma and Lewis lung carcinoma in vitro at
lowconcentrations (40, 42) and provide subjective benefit in
bron-chogenic carcinoma patients (43).
Tumor grade and stage of disease may also have to be takeninto
account in assessing the response of a particular histopath-
ological grouping. We have presented suggestive evidence for
adecrease in receptor content with increasing anaplasia and stageof
disease in squamous cell carcinoma. However, GR content
inadenocarcinoma appears to increase with dedifferentiation
andtumor burden in adenocarcinoma.
Administration of testosterone propionate had no apparenteffect
on the progress of metastatic lung carcinoma (41) but didapparently
relieve bone pain (44). Metabolism of this ester of theendogenous
steroid must be taken into account in any estimateof its efficacy.
The decrease in AR content coupled with analteration in affinity in
the more anaplastic squamous cell carcinomas suggest that only
selected lesions in this histopathologicalcategory may respond to
changes in circulating androgen.
The usefulness of ER, AR, and GR as an aid in determiningpatient
prognosis and the appropriateness of steroid manipulation as future
adjunct or palliative agents in bronchogenic carcinomas clearly
remain to be determined. While previous reportssuggest little
chance of small (oat) cell carcinomas respondingto steroids (16),
the similarity in binding characteristics betweenbronchogenic
carcinoma and other steroid-responsive tissues
suggest a potential starting point in investigating whether
steroids influence the natural history of bronchogenic
carcinomas.
REFERENCES
1. Farrell, P. M. Fetal lung development and the influence of
glucocorticoids onpulmonary surfactant. J. Steroid Biochem., 8:
453-470,1977.
2. Sarda, I. R., Hayglass, K., Corwill, R. H., and Smith, B. T.
Estrogen and lungmaturation: dual effect on rabbit fetal lung cell
carcinoma (abstract). Program62nd Annual Meeting of the Endocrine
Society. Washington, DC, 1980.
3. Snyder, J. M., Mendelson, D. R., and Johnston, J. J.
Multihormonal control ofhuman fetal lung development (abstract).
Program 62nd Annual Meeting of theEndocrine Society, Washington,
DC, 1980.
4. Torday, J. S., Smith, B. T., and Girond, C. J. P. The rabbit
fetal lung as aglucocorticoid target tissue. Endocrinology, 96:
1462-1467,1975.
5. Kikkawa, Y., Kaibara, M., Motoyama, E. K., Orzatesi, M. M.,
and Cook, C. D.Morphologic development of fetal rabbit lung and its
acceleration with cortisol.Am. J. Pathol., 64: 423-442, 1971.
6. Lombardero, M., and Nieto, A. Glucocorticoid and
developmental regulation ofuteroglobin synthesis in rabbit lung.
Biochem. J., 200: 487-494,1981.
7. Phelps, D. S., and Giannopoulos, G. Effects of dexamethasone
on protein
synthesis in fetal rabbit lung in organ culture (abstract).
Program 64th AnnualMeeting of the Endocrine Society, San Francisco,
CA, 1983.
8. Ballard, P. L, Baxter, J. D., Higgens, S. J., Rosseau, G. C.,
and Tompkins, G.M. General presence of glucocorticoid receptors in
mammalian tissues Endocrinology, 94: 998-1002,1974.
9. Ballard, P. I., Mason, R. J., and Douglas, W. H.
Glucocorticoid binding byisolated lung cells. Endocrinology, 702:
1570-1575, 1978.
10. Mendelson, C. R., MacDonald, P. C., and Johnston, J. M.
Estrogen binding inhuman fetal lung tissue. Endocrinology, 706:
368-379,1980.
11. Ballard, P. L., and Ballard, R. A. Cytoplasmic receptors for
glucocorticoids inlung of the human fetus and neonate. J. Clin.
Invest., 53: 477-486,1973.
12. Khosla, S. S., Brehier, A., Eisenfeld, A. J., Ingleson, L.
D., Parks, P. A., andRooney, S. A. Influence of sex hormones on
maturation in the fetal rabbit.Biochim. Biophys. Acta,
250:112-126,1983.
13. Pasqualini, J. R., Sumida, C., Gelly, C., and Nguyen, B. L.
Specific [3H]estradiol
binding in the fetal uterus and testes of the guinea pig.
Quantitative evolutionof [3H]estradiol receptors in different fetal
tissues (kidney, lung, uterus, testes)
during fetal development. J. Steroid Biochem.,
7:1031-1038,1976.14. Morishige, W. K., and Uetake, C. H. Receptors
for androgen and estrogen
uptake in the rat lung. Endocrinology, 702: 1827-1837, 1978.15.
Mendelson, C. R., Johnston, T. M., MacDonald, P. C., and Snyder, J.
M.
Multihormonal regulation of surfactant synthesis by human fetal
lung in vitro.J. Clin. Endocrinol. Metab., 53: 307-317,1981.
16. Chaudhuri, P. K., Thomas, P. A., Walker, M. J., Briefe, H.
A., Das Gupta, T.K., and Beattie, C. W. Steroid receptors in human
lung cancer. Cancer LettÕ6:327-332,1982.
17. Hasselquist, M. B., Goldberg, N., Schroeter, A., and
Speisburg, T. C. Isolationand characterization of estrogen receptor
in human skin. J. Clin. Endocrinol.Metab., 50:76-82,1980.
18. Giannopoulos, G., Phelps, D. S., and Sommers-Smith, S. K.
Androgen receptors in fetal rabbit lung and the effects of fetal
sex on the levels of circulatinghormones and pulmonary hormone
receptors (abstract). Program 64th AnnualMeeting of the Endocrine
Society, San Francisco, CA, 1982.
19. Jones, L. A., Blocker, S. H., Rusch, V. H., and Mountain, C.
F. Specificestrogen binding protein in human lung cancer. Proc. Am.
Assoc. Cancer Res.,25:208,1984.
20. Kobayashi, S., Mizuno, T., Tobioka, N., Ichimura, H.,
Samolo, T., Tanaka, H.,Masaoka, A., Wakabayashi, S., Umemura, S.,
Fukuoka, H., and Nagai, H. Sexsteroid receptors in diverse human
tumors. Gann, 23: 439-445,1982.
21. Liu, S. H., Otal-Brun, M., and Webb, T. E. Glucocorticoid
receptors in humantumors. Cancer Lett., 70. 269-275, 1980.
22. American Joint Committee for Staging and End Results
Reporting. Staging ofLung Cancer, 1979.
23. Nelson, C. J., Vogel, W. M., and Pratt, W. B. Inactivation
of glucocorticoidreceptor preparations of rat liver. Cancer Res.,
37: 3420-3425,1977.
24. Bradford, M. M. A rapid sensitive method for quantitation of
protein using theprinciple of protein dye binding. Anal. Biochem.,
72: 248-254, 1976.
25. Rosner, A. L., Teman, G. H., Bray, C. L., and Burstein, L.
A. Batch assaymethod evaluation of cytoplasmic estrogen receptors,
relative immunity ofhydroxyapatite method from errors of
measurements. Eur. J. Cancer, 76:1495-1502,1980.
26. Zava, D. T., Landrum, B., Horwitz, K. B., and McGuire, W. L.
Androgenreceptor assay with [3H]methyltrienolone in the presence of
progesteronereceptors. Endocrinology, 704:1007-1012,1979.
27. Scatchard, D. The attractions of proteins for small
molecules and ions. Ann.NY Acad. Sci., 87. 660-672,1949.
28. Hill, A. V. The mode of action of nicotine and curari,
determined from the formof the contraction cure and the method of
temperature coefficients. J. Physiol.,39:361-368,1909.
29. Martin, R. G., and Ames, B. N. A method for determining the
sedimentationbehavior of enzymes: application to protein mixtures.
J. Biol. Chem., 226:1372-1379,1961.
30. Sokol, R. R., and Rolf, F. J. Biometry—Principle and
Practice of Statistics inBiological Research. San Francisco: W. H.
Freeman, 1967.
31. Allegra, J. C., Lippman, M. E., Thompson, E. B., Barlock,
H., Green, L., Huff,K. K., Do, H. M. T., and Aitkan, S. C.
Distribution, frequency, and quantitativeanalysis of estrogen,
progesterone, androgen, and glucocorticoid receptors inhuman breast
cancer. Cancer Res., 39: 1447-1454,1979.
32. Horwitz, K. B., Costlow, M. E., and McGuire, W. C. MCF-7, a
human cancercell line with estrogen, androgen, progesterone, and
glucocorticoid receptor.Steroids, 26: 785-795, 1975.
33. Fazekas, A. G., and MacFariane, J. K. Glucocorticoid
receptors in humanbreast cancer tissue. In: A. C. W. Montague, G.
L. Stonesifer, and E. F.Lewison (eds.). Breast Cancer, pp. 149-154.
New York: Alan R. Liss, Inc.,1977.
34. Geroge, S. C., Gudewicz, P. W., and Jaffee, R. C.
Glucocorticoid binding tonormal and activated alveolar lung cells.
Lung, 757: 57-64, 1980.
35. Giannopoulos, G. Variation in the levels of cytoplasmic
glucocorticoid receptorsin lungs of various species at different
developmental stages. Endocrinology,94:450-458,1974.
36. Stedman, K. E.. Moore, G. E., and Morgan, R. T. Estrogen
receptor proteinsin diverse human tumors. Arch. Surg., 775:
244-248,1980.
CANCER RESEARCH VOL. 45 SEPTEMBER 1985
4213
on July 10, 2021. © 1985 American Association for Cancer
Research. cancerres.aacrjournals.org Downloaded from
http://cancerres.aacrjournals.org/
-
RECEPTORS IN LUNG CANCER
3fr. Mendelson,C. R., Snyder, J. M., Gellispy, S. E., and
Johnston, J. M. Development of humanfetal lung inorgan culture.
Effects of progesterone(abstract).Program61st Annual Meeting of the
EndocrineSociety, Anaheim,CA, 1979.
38. Keenan, B. S., and McNeel, R. L.
5-Alpha-dihydrotestosterone(DHT) bindingin skin fibroblast
sonicates: two classes of binding sites (abstract). Program64th
Annual Meeting of the EndocrineSociety, San Francisco,CA, 1982.
39. Torday, J. S. Glucocorticoid dependence of fetal lung
maturation in vitro.Endocrinology, 707: 839-844, 1980.
40. Braunschweiger, P. G., Ting, H. L., and Schiffer, L. M.
Receptor mediatedanti-proliferativeeffects of corticosteroids in
Lewis lung tumors. Eur. J. Cancer
Clin. Oncol., 20: 427-433,1984.41. Wolf, J., Spear, P., Yesner,
R., and Patno, M. E. Nitrogen mustard and the
steroid hormones in the treatment of
inoperablebronchogeniccarcinoma.Am.J. Med., 1008-1016,1961.
42. Jones, K. L., Anderson, N. S., Ill, and Addison, J.
Glucocorticoid inducedgrowth inhibition of cells from a human lung
alveolar cell carcinoma. CancerRes., 38: 1688-1693,1978.
43. Kamofsky, D. A., Meyers,W. P. L., and Phillips,R.
Treatmentof the inoperablepulmonarycancer. Primary and metastatic.
Am. J. Surg., 89: 526-537,1955.
44. Olson, K. B. A study of certain sex factors and
hormonetreatment in bronchogenic carcinoma.Am. J. Med. Sci.,
230:157-168,1955.
CANCER RESEARCH VOL. 45 SEPTEMBER 1985
4214
on July 10, 2021. © 1985 American Association for Cancer
Research. cancerres.aacrjournals.org Downloaded from
http://cancerres.aacrjournals.org/
-
1985;45:4206-4214. Cancer Res Craig W. Beattie, Nancy W. Hansen
and Paul A. Thomas Steroid Receptors in Human Lung Cancer
Updated version
http://cancerres.aacrjournals.org/content/45/9/4206
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to
receive free email-alerts
Subscriptions
Reprints and
[email protected] at
To order reprints of this article or to subscribe to the
journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take
you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/45/9/4206To request
permission to re-use all or part of this article, use this link
on July 10, 2021. © 1985 American Association for Cancer
Research. cancerres.aacrjournals.org Downloaded from
http://cancerres.aacrjournals.org/content/45/9/4206http://cancerres.aacrjournals.org/cgi/alertsmailto:[email protected]://cancerres.aacrjournals.org/content/45/9/4206http://cancerres.aacrjournals.org/