Embed Size (px)
Citation preview

J Neurosurg 118:950–955, 2013
950 J Neurosurg / Volume 118 / May 2013
©AANS, 2013
Aneurysms distal to the circle of Willis represent the frontier of endovascular aneurysm treatment. Historically, MCA aneurysm treatment strategies
have favored microsurgical clipping due to the relative ease of dissection, the increased distance required for en-dovascular access, and the prevalent thought that endo-vascular treatment risks in this location may be higher than those of surgery.22 Although the ISAT (International Subarachnoid Aneurysm Trial) investigators found a similar risk of adverse events after coiling 162 MCA an-eurysms and clipping 139 MCA aneurysms, all other lo-cations trended toward fewer adverse events when using endovascular treatment, reinforcing the perception that
MCA aneurysms may be the best microsurgical candi-dates.21
Stenting has broadened the scope of endovascular aneurysm treatment in the past decade. Stenting provides scaffolding for more complete aneurysm coiling with greater protection of the parent vessel and is now used ex-tensively for large, complex, wide-necked, and fusiform aneurysms. Several stent-assisted coiling series have demonstrated a disproportionately low frequency of MCA aneurysm treatments, with only 38 (4.8%) of 796 stented aneurysms treated in this location.1–3,8–11,13–16,18–20,23,24,27,30,31 The first dedicated stent-assisted MCA aneurysm treat-ment series have been published recently with encourag-ing results.7,26,29
We present the largest case series to date for stent-assisted coiling of MCA aneurysms to further elucidate
Stent-assisted embolization of 100 middle cerebral artery aneurysms
Clinical articleAndrew K. Johnson, M.d., M.s.e.,1 dAniel M. heiferMAn, B.A. ,2 And deMetrius K. lopes, M.d.1
1Department of Neurosurgery, Rush University Medical Center, and 2Rush University Medical College, Chicago, Illinois
Object. The introduction of intracranial stents to aneurysm treatment allows endovascular repair of nearly all aneurysms, but the safety and durability of stent-assisted embolization of middle cerebral artery (MCA) aneurysms is unclear.
Methods. Ninety-one patients with 100 complex MCA aneurysms not amenable to simple coiling were treated with stent-assisted embolization as a first option. Technical and clinical results, initial follow-up imaging, and long-term annual MR angiography (MRA) were reviewed.
Results. Intracranial stents were successfully deployed in all 100 aneurysms. There was 1 case of significant neurological morbidity (1%) and 1 case of death (1%) related to treatment. Initial posttreatment angiography revealed complete occlusion of 48 aneurysms (48%), a residual neck in 21 (21%), and residual aneurysm filling in 31 (31%). Follow-up imaging performed in 85 (90.4%) of a possible 94 aneurysms showed complete occlusion of 77 aneurysms (90.6%), residual neck in 3 (3.5%), and residual filling in 5 (5.9%). Four aneurysms (4.7%) required retreatment. Long-term MRA follow-up revealed stability or progressive thrombosis in 47 (97.9%) of 48 aneurysms. In 11 patients Y-configuration stenting caused only 1 minor complication and provided durable occlusion in all cases.
Conclusions. Stent-assisted techniques increase the number of aneurysms that may be treated endovascularly and represent an acceptable alternative to craniotomy. Stents provided adequate vessel reconstruction, low complica-tion rates, and good long-term occlusion.(http://thejns.org/doi/abs/10.3171/2013.1.JNS121298)
Key words • aneurysm • endovascular • middle cerebral artery • stent • Y-configuration stent • vascular disorders • interventional neurosurgery
Abbreviations used in this paper: MCA = middle cerebral artery; MRA = MR angiography.
See the corresponding editorial in this issue, pp 947–949.

J Neurosurg / Volume 118 / May 2013
Stent embolization of MCA aneurysms
951
the safety, techniques, outcomes, and future role of endo-vascular aneurysm treatment at this anatomical site.
MethodsPatient Population
Ninety-one patients harboring 100 MCA aneurysms underwent stent-assisted aneurysm embolization per-formed by the senior author (D.K.L.) between October 2002 and June 2012. While all patients were given the options of open surgical or endovascular treatment, en-dovascular repair was recommended as the first option to patients presenting to the senior author. Informed written consent approved by the medical center’s institutional re-view board was obtained for each patient in whom stent-ing was considered. If the aneurysm could not be safely managed with coil embolization alone, stent reconstruction was performed. Indications for stent placement included 1) aneurysm neck greater than 4 mm, 2) dome-to-neck ratio less than 2, 3) coil instability or parent vessel compromise during coiling, and 4) fusiform aneurysm morphology. Up-coming surgical procedures, particularly after aneurysm rupture, hematoma mass effect requiring surgical evacua-tion, and anatomical barriers to access were contraindica-tions to stent-assisted aneurysm treatment.
Patient information, aneurysm details, and clinical course data were maintained in a database for future ret-rospective review. Patients ranged in age from 25 to 88 years (mean ± SD, 60.6 ± 12.9 years) at the time of treat-ment; patient and aneurysm characteristics are listed in Table 1. At our institution, embolization is performed in approximately 75% of unruptured and 65% of ruptured MCA aneurysms, of which stents are used in about 30% and less than 10% of cases, respectively.
Perioperative Antiplatelet ManagementWhen possible, patients took aspirin (325 mg) and
clopidogrel (75 mg) daily for 5 days prior to expected stent-ing. Those unable to complete this regimen received a 600-mg load of clopidogrel prior to the procedure and began daily aspirin therapy. Point-of-care aspirin and P2Y12 as-says (VerifyNow, Accumetrics) were routinely used begin-ning in 2005. In cases in which antiplatelet therapy was not therapeutic—that is, an aspirin reaction unit > 550 or P2Y12 reaction unit < 250 or < 30% inhibition—an intra-arterial loading dose of 0.25 mg/kg abciximab (0.25 mg/kg) was given prior to stent placement, followed by a 12-hour infusion (0.125 mg/kg/min or 10 mg/min). Abciximab was also given if thrombus developed inside the stent or when patients had a new neurological deficit after treat-ment and a CT scan showing no intracerebral hemorrhage. Clopidogrel was reloaded after the procedure if P2Y12 inhibition was inadequate. All patients continued aspirin and clopidogrel therapy daily for 3 months. Patients with multiple stents remained on antiplatelet therapy until their 6-month angiography follow-up. An ischemic event or sig-nificant in-stent stenosis on follow-up imaging led to addi-tional antiplatelet therapy on a case-by-case basis.
Eight patients in the series presented with acute sub-arachnoid hemorrhage presumably from rupture of the MCA aneurysm. Three of these aneurysms were coiled in the acute phase followed by a delayed stenting proce-dure for final aneurysm repair. These three patients were loaded with aspirin and clopidogrel in the usual fashion. Five patients with low-grade hemorrhages and without ventriculostomy were stented during the initial acute treatment. Unless a patient was already therapeutic on antiplatelet medication prior to their hemorrhage and pro-cedure, no preoperative antiplatelet therapy was adminis-tered. A loading dose of abciximab was given as soon as the ruptured aneurysm was both coiled and stented. Fol-lowing the procedure aspirin and clopidogrel were loaded and continued in similar fashion to unruptured aneurysm cases.
Stenting ProceduresIn addition to antiplatelet therapy, heparin was given
to maintain an activated clotting time of greater than 250 seconds once the procedure began. In patients with rup-tured aneurysms, heparin was given after the first coil was inserted. Heparin was not reversed following treat-ment unless postoperative CT revealed new bleeding.
Neuroform stents (Boston Scientific) were used in most patients; the open-cell design was preferred for the tight curves of the MCA complex. The closed-cell En-terprise stent (Cordis Neurovascular, Inc.) was frequently used in straighter segments or when a 0.027-inch-inner-diameter microcatheter could not navigate the distal branches. The Enterprise stent could also be partially de-ployed across the aneurysm during coiling. After coiling, a decision was made whether to fully deploy or remove the stent.17 Wingspan stents (Boston Scientific) were used in 2 patients. One had M1 segment stenosis proximal to the aneurysm; the other had a dissecting aneurysm. Table 2 details the stents used in this series.
TABLE 1: Characteristics of 100 MCA aneurysms in 91 patients
Characteristic No. of Aneurysms (n = 100)
female (n = 73) 80male (n = 18) 20single MCA aneurysm 82bilat MCA aneurysms 12multiple unilat MCA aneurysms 6small aneurysm (<10 mm) small neck (<4 mm) 37 wide neck (≥4 mm) 48large aneurysm (≥10 mm) 12giant aneurysm (≥25 mm) 3previously clipped aneurysms 1previously coiled aneurysms 4previous rupture 11 acute* 5 subacute† 3 remote 3
* Acutely ruptured aneurysms were stented on first treatment. † Subacutely ruptured aneurysms were coiled and subsequently stent-ed during a short-term follow-up procedure.

A. K. Johnson, D. M. Heiferman, and D. K. Lopes
952 J Neurosurg / Volume 118 / May 2013
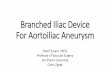
The overlapping or stent-in-stent technique was used to reinforce an existing stent or further cover the aneu-rysm neck. We used Y-configuration stenting as an option for bifurcations where both parent vessels could not be protected by a single stent (Fig. 1). In 2 patients, a single stent was placed over 2 distinct MCA aneurysms (Fig. 2).
Postoperative CourseFollowing treatment, nonenhanced CT scanning was
performed in all cases to confirm stent and coil position and to confirm the absence of hemorrhage. Patients were admitted to the ICU overnight. Patients with unruptured aneurysms were discharged on postoperative Day 1 if possible. Patients with ruptured aneurysms or complica-tions remained in the hospital as needed.
Angiography was scheduled 6 months after treat-ment. In cases of significant or increased residual filling, a decision was made whether to retreat the aneurysm. An-giography was scheduled 6 months after repeat treatment in a similar fashion. If the aneurysm showed satisfactory occlusion, the patient was followed up with yearly clinic appointments and MRI and MRA. Both MRI and MRA with and without contrast with 3D time of flight were used to evaluate evidence of ischemia, in-stent stenosis, residual treated aneurysm, and de novo aneurysms.6,28
ResultsTechnical Results
Stents were successfully placed in all patients; how-ever, one Y-configuration stent deployment was abandoned due to movement of the first stent during attempted deploy-ment of the second. The patient returned for successful staged Y-configuration stenting later. There were no intra-operative ruptures. Thrombus formation was detected in-side the stent of 1 patient prior to the end of his aneurysm treatment. Abciximab was given, and the patient remained asymptomatic. Two treatments caused small vessel occlu-sion and transient symptoms, which were treated with ab-ciximab and blood pressure augmentation.
In 4 cases, coils prolapsed despite stenting. In 3 of these cases a second overlapping stent was successful-ly deployed to plaster the coil to the vessel wall. In the fourth case, the coil stretched; it was successfully snared and subsequently released into the external carotid artery.
Clinical ResultsNine patients had new neurological symptoms fol-
lowing stent-assisted aneurysm treatment; all patients were given abciximab. Five of these patients had transient symptoms, including intermittent aphasia, contralateral weakness, and contralateral sensory symptoms, which resolved prior to discharge. Two of these patients had mi-nor residual deficits at discharge including contralateral fingertip numbness and a subtle pronator drift on exami-nation, but neither had long-term disability. Despite ag-
TABLE 2: Stent selection for 100 MCA aneurysms
Stent Selection by Aneurysm No. of Aneurysms
treatment Neuroform only 62 Enterprise only 32 Wingspan only 1 combination 5total stents placed 116stented w/out coiling 2Y-configuration stent 11*overlapping stent configuration 7*stent covering 2 aneurysms 2
* The second stent in one Y-configuration and three overlapping con-figuration cases was placed in a subsequent procedure.
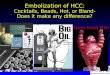
Fig. 2. Left: Anteroposterior digital subtraction angiogram show-ing an M1 segment aneurysm treated with overlapping stents and coil embolization. Right: Magnetic resonance angiogram demonstrating new filling at the site of the aneurysm 3 years after treatment. This un-usual case of either recurrence or adjacent de novo aneurysm forma-tion was treated with coil embolization delivered through the struts of the existing stents.
Fig. 1. DynaCT (Siemens) oblique axial reconstructed scan showing Y-configuration stenting of an MCA aneurysm using Neuroform stents; the anterior communicating artery aneurysm is covered by a single Neuroform stent.

J Neurosurg / Volume 118 / May 2013
Stent embolization of MCA aneurysms
953
gressive antiplatelet therapy, 1 patient developed contra-lateral hemiparesis and aphasia; symptoms improved, but the patient has permanent contralateral weakness. In 2 of the patients with persistent postoperative symptoms, MRI revealed corresponding restricted diffusion.
The ninth patient represented the single procedure-related death. This patient, who had HIV, hepatitis C vi-rus, and required hemodialysis for kidney disease, had coil compaction 4 years after initial coil embolization. She was considered a poor candidate for surgical repair, and coiling without stenting did not seem adequate given the residual dome and neck widths of 8 mm and 6 mm, respectively. The residual aneurysm was coiled after overlapping Enterprise stents were placed. The patient experienced a new contralateral hemiparesis following treatment. The patient aspirated during an MRI 5 days after treatment and died after never regaining mental sta-tus. Table 3 provides a summary of neurological compli-cations. Complications of subarachnoid hemorrhage and cancer caused 2 other patients to die before follow-up an-giography could be undertaken.
The 98 patients living beyond 1 month after stent-as-sisted aneurysm treatment were followed up clinically for a mean 1.91 ± 1.84 years (range 1 month to 6.75 years). Dur-ing the extended follow-up period, there were 4 transient events potentially related to aneurysm treatment, the latest of which occurred 27 months after treatment (Table 3).
During the follow-up period, 2 patients suffered in-tracranial hemorrhages. A de novo posterior communi-cating artery aneurysm ruptured in a patient 6 years after her MCA aneurysm was treated; she had not been compli-ant with her yearly imaging for 3 years prior to the event. A 75-year-old hypertensive, diabetic woman experienced an ipsilateral basal ganglia hemorrhage more than 1 year after her 6-mm MCA aneurysm repair; the relationship of these events is uncertain. To our knowledge, there have been no other adverse cerebrovascular events or deaths involving the patients in this series.
Three complications of femoral artery access caused morbidity but no permanent disability. Two patients de-veloped significant retroperitoneal hematomas. The other patient required surgical thrombectomy for femoral ar-tery thrombosis at the site of catheterization. One pa-tient had significant epistaxis while on dual antiplatelet therapy. There were no complications from 5 retreatment procedures or 98 follow-up diagnostic angiograms.
Radiographic ResultsInitial follow-up imaging, usually after 6 months, was
performed in 85 (90.4%) of 94 possible aneurysms (Table 4). Three patients died and 3 were treated too recently for appropriate follow-up. While only 42 of the initial 100 procedures resulted in complete occlusion, 77 (90.6%) of 85 aneurysms were completely occluded at follow-up. Four aneurysms worsened angiographically, and 4 (4.7%) required retreatment after first follow-up.
In 85 aneurysms with imaging follow-up, 8 stents (9.4%) had angiographically demonstrable in-stent steno-sis. Five were visualized on 6-month follow-up angiogra-phy; 3 additional in-stent stenoses were demonstrated on MRA. One M2 segment was completely occluded with distal reconstitution of blood flow. Only 1 other stenosis was greater than 50%, and none was symptomatic.
The mean duration of imaging follow-up for these 85 aneurysms was 2.14 ± 1.88 years (range 4 months to 6.75 years). Subsequent follow-up imaging greater than 1 year after treatment has been performed in 48 (56.5%) of 85 at this juncture. Eight aneurysms showed residual filling less than 3 mm on MRA but have remained stable and not needed treatment. One small aneurysm treated with overlapping stents and coils was completely occluded on initial and 6-month angiography, but MRA 3 years after treatment showed new residual filling adjacent to the an-eurysm. This was considered a recurrence but may actu-ally represent an unusual de novo aneurysm formed adja-cent to a previously treated aneurysm within the stented segment (Fig. 2).
Overlapping and Y-Configuration StentsOverlapping stents were placed in 7 patients; 3 of
these patients had neurological complications including the aforementioned case in which death occurred. Except for the late regrowth described above, these aneurysms remained completely occluded.
Eleven patients underwent aneurysm coiling with a Y-configuration stent. Transient contralateral upper-extremity weakness complicated 1 case, but the permanent operative morbidity and mortality rates were 0% for this subgroup. All aneurysms treated with a Y-shaped stent configuration had total occlusion on follow-up angiography; none re-quired retreatment during the follow-up period.
DiscussionStent-assisted aneurysm treatment has broadened the
range of aneurysms accessible to the neurointerventional-ist. The early aneurysm-stenting literature provides a rel-ative paucity of MCA treatment, as distal aneurysms in-cluding MCA and pericallosal locations have historically been clipped more frequently than they have been treated endovascularly. However, the complex anatomy of the MCA may be particularly amenable to stent reconstruc-tion. Our series of 100 aneurysms demonstrated 90.6% occlusion on first follow-up imaging; major morbidity and mortality rates were 1.0% each.
Vendrell et al.26 successfully deployed 50 stents, at-tempting to treat 52 MCA aneurysms in 49 patients.
TABLE 3: Neurological complications
Complication Total (%)
procedure-related transient deficits 6 (6) minor permanent morbidity 2 (2) permanent morbidity 1 (1) death 1 (1)late events transient ischemic events 4 (4.1) ipsilateral intracerebral hemorrhage 1 (1.0) permanent morbidity/mortality 0 (0)

A. K. Johnson, D. M. Heiferman, and D. K. Lopes
954 J Neurosurg / Volume 118 / May 2013
Ten total perioperative thromboembolic events resulted in permanent neurological deficits in 2 patients despite treatment with abciximab, yielding a morbidity rate of 3.8% and a mortality rate of 0% in their series. Yang et al.29 treated 16 MCA aneurysms with stents without per-manent procedure-related neurological sequelae. Fields et al.7 described the successful treatment of 22 aneurysms with 2 neurological complications.
Brinjikji et al.4 presented the composite endovascular results for MCA aneurysms in the prestenting era. Meta-analysis of 12 MCA aneurysm coiling series revealed an overall morbidity and mortality rate of 5.5% in 1030 an-eurysm treatments. Only 4 stents were included in these data. For more appropriate comparison with our results, the combined morbidity and mortality rate for unrup-tured aneurysms was 5.1%.
Horowitz et al.12 cited 6 surgical series of MCA an-eurysm treatments published in the last 30 years, demon-strating a combined morbidity and mortality rate of 10%, and a range of 3%–16%. However, direct comparison of endovascular and open surgical repair is not straightfor-ward. Surgical series did not have the luxury of exclud-ing unfavorable aneurysms prior to the advent of endo-vascular therapy, and endovascular series success rates may be overestimated secondary to selection bias. Every aneurysm carries different risks based on its architecture, location, and the anatomical variations in the access for both methods. Only a team skilled in all techniques has the appropriate judgment for selecting the best modality.
Our series demonstrated a trend of progressive thrombosis after aneurysm treatment and durability af-ter stable follow-up imaging. Six-month angiography re-vealed an increase in complete occlusion from 48% to 90.6%, while only 5 aneurysms required retreatment. One of these retreatments was needed because MRA showed new filling at 3 years, but in 47 (97.9%) of 48 patients, annual MRA revealed aneurysm stability or progressive thrombosis. There were no posttreatment ruptures during the follow-up period. The observed long-term stability of the treatment speaks to the anatomical and physiological strength of the stent and coil construct.
Limitations to the present study include but are not limited to selection bias, lack of an adequate control group, and nonblinded review of angiograms. Referral patterns may have led to a preselected aneurysm popula-tion more favorable to endovascular treatment. Because open surgical management is frequently chosen for MCA aneurysms, the population of MCA aneurysms referred to the senior author (D.K.L.) may be particularly ame-
nable to stent-assisted embolization. A control group with matching characteristics is not feasible, and historical control group comparison is limited by differences in pa-tient selection and study protocol.
The use of Y-shaped stenting may increase thrombo-embolic risks due to intraluminal struts and altered stent strut apposition, but the method can provide excellent an-eurysm repair, even in the absence of intrasaccular ther-apy.5 The success in our experience with Y-configuration stenting in all locations is similar to that of Spiotta et al.,25 showing increased complications but satisfactory angio-graphic outcomes with the technique. In this series, the very low morbidity rate with Y-configuration stenting at the MCA bifurcation may be a function of small sample size. Otherwise, the success could be related to specific anatomical features of the MCA bifurcation including the large caliber of the M1 and M2 segments or the location distal to the circle of Willis.
ConclusionsIntracranial stents allow reconstruction of the complex
anatomy of the MCA and treatment of aneurysms, many of which were previously untreatable with endovascular tech-niques. Stent-assisted embolization provides an alternative to craniotomy for these aneurysms, with an acceptable complication rate and high angiographic cure rate.
Disclosure
Demetrius Lopes discloses that he has financial and research relationships with Penumbra, Covidien, and Stryker. Drs. Johnson and Heiferman report no financial disclosures.
Author contributions to the study and manuscript preparation include the following. Conception and design: Lopes, Johnson. Acquisition of data: all authors. Analysis and interpretation of data: Lopes, Johnson. Drafting the article: all authors. Critically revising the article: all authors. Reviewed submitted version of manuscript: all authors. Statistical analysis: Johnson. Administrative/technical/material support: Lopes. Study supervision: Lopes.
References
1. Akpek S, Arat A, Morsi H, Klucznick RP, Strother CM, Mawad ME: Self-expandable stent-assisted coiling of wide-necked intracranial aneurysms: a single-center experience. AJNR Am J Neuroradiol 26:1223–1231, 2005
2. Benitez RP, Silva MT, Klem J, Veznedaroglu E, Rosenwasser RH: Endovascular occlusion of wide-necked aneurysms with a new intracranial microstent (Neuroform) and detachable coils. Neurosurgery 54:1359–1368, 2004
TABLE 4: Radiographic results*
Imaging Complete Occlusion (%) Residual Neck (%) Residual Sac (%) Retreated (%)
immediate posttreatment DSA 48 31 21 NA6-mo follow-up imaging 77 (90.6) 3 (3.5) 5 (5.9) 4 (4.7) initial complete occlusion 40 (95.2) 0 (0) 2 (4.8) 1 (2.4) initial residual neck 20 (83.3) 2 (8.3) 2 (8.3) 2 (8.3) initial residual sac 17 (89.5) 1 (5.3) 1 (5.3) 1 (5.3)
* DSA = digital subtraction angiography; NA = not applicable.

J Neurosurg / Volume 118 / May 2013
Stent embolization of MCA aneurysms
955
3. Biondi A, Janardhan V, Katz JM, Salvaggio K, Riina HA, Gobin YP: Neuroform stent-assisted coil embolization of wide-neck intracranial aneurysms: strategies in stent deployment and midterm follow-up. Neurosurgery 61:460–469, 2007
4. Brinjikji W, Lanzino G, Cloft HJ, Rabinstein A, Kallmes DF: Endovascular treatment of middle cerebral artery aneurysms: a systematic review and single-center series. Neurosurgery 68:397–402, 2011
5. Cekirge HS, Yavuz K, Geyik S, Saatci I: A novel “Y” stent flow diversion technique for the endovascular treatment of bifurcation aneurysms without endosaccular coiling. AJNR Am J Neuroradiol 32:1262–1268, 2011
6. Ferré JC, Carsin-Nicol B, Morandi X, Carsin M, de Kersaint-Gilly A, Gauvrit JY, et al: Time-of-flight MR angiography at 3T versus digital subtraction angiography in the imaging follow-up of 51 intracranial aneurysms treated with coils. Eur J Radiol 72:365–369, 2009
7. Fields JD, Brambrink L, Dogan A, Helseth EK, Liu KC, Lee DS, et al: Stent assisted coil embolization of unruptured mid-dle cerebral artery aneurysms. J Neurointerv Surg 5:15–19, 2013
8. Fiorella D, Albuquerque FC, Han P, McDougall CG: Prelimi-nary experience using the Neuroform stent for the treatment of cerebral aneurysms. Neurosurgery 54:6–17, 2004
9. Handa A, Abdo G, Yilmaz H, Lovblad KO, Lylyk P, Rüfenacht DA: Efficacy and limitations of the neuroform stent system for intracranial aneurysms. Interv Neuroradiol 10 (Suppl 2): 62–68, 2004
10. Henkes H, Bose A, Felber S, Miloslavski E, Berg-Dammer E, Kühne D: Endovascular coil occlusion of intracranial aneu-rysms assisted by a novel self-expandable nitinol microstent (neuroform). Interv Neuroradiol 8:107–119, 2002
11. Higashida RT, Halbach VV, Dowd CF, Juravsky L, Meagher S: Initial clinical experience with a new self-expanding nitinol stent for the treatment of intracranial cerebral aneurysms: the Cordis Enterprise stent. AJNR Am J Neuroradiol 26:1751–1756, 2005
12. Horowitz M, Gupta R, Gologorsky Y, Jovin T, Genevro J, Levy E, et al: Clinical and anatomic outcomes after endovas-cular coiling of middle cerebral artery aneurysms: report on 30 treated aneurysms and review of the literature. Surg Neu-rol 66:167–171, 2006
13. Kim SR, Vora N, Jovin TG, Gupta R, Thomas A, Kassam A, et al: Anatomic results and complications of stent-assisted coil embolization of intracranial aneurysms. Interv Neuroradiol 14:267–284, 2008
14. Kis B, Weber W, Berlit P, Kühne D: Elective treatment of sac-cular and broad-necked intracranial aneurysms using a closed-cell nitinol stent (Leo). Neurosurgery 58:443–450, 2006
15. Lanzino G, Wakhloo AK, Fessler RD, Hartney ML, Guterman LR, Hopkins LN: Efficacy and current limitations of intra-vascular stents for intracranial internal carotid, vertebral, and basilar artery aneurysms. J Neurosurg 91:538–546, 1999
16. Lee YJ, Kim DJ, Suh SH, Lee SK, Kim J, Kim DI: Stent-assisted coil embolization of intracranial wide-necked aneu-rysms. Neuroradiology 47:680–689, 2005
17. Lopes DK, Wells K: Stent remodeling technique for coiling of ruptured wide-neck cerebral aneurysms: case report. Neuro-surgery 65:E1007–E1008, 2009
18. Lubicz B, François O, Levivier M, Brotchi J, Balériaux D: Preliminary experience with the enterprise stent for endovas-cular treatment of complex intracranial aneurysms: potential advantages and limiting characteristics. Neurosurgery 62: 1063–1070, 2008
19. Lylyk P, Cohen JE, Ceratto R, Ferrario A, Miranda C: Endo-vascular reconstruction of intracranial arteries by stent place-ment and combined techniques. J Neurosurg 97:1306–1313, 2002
20. Mocco J, Snyder KV, Albuquerque FC, Bendok BR, Alan SB, Carpenter JS, et al: Treatment of intracranial aneurysms with the Enterprise stent: a multicenter registry. Clinical article. J Neurosurg 110:35–39, 2009
21. Molyneux AJ, Kerr RS, Yu LM, Clarke M, Sneade M, Yarnold JA, et al: International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, re-bleeding, subgroups, and aneurysm occlusion. Lancet 366: 809–817, 2005
22. Regli L, Dehdashti AR, Uske A, de Tribolet N: Endovascu-lar coiling compared with surgical clipping for the treatment of unruptured middle cerebral artery aneurysms: an update. Acta Neurochir Suppl 82:41–46, 2002
23. Sani S, Jobe KW, Lopes DK: Treatment of wide-necked cere-bral aneurysms with the Neuroform2 Treo stent. A prospec-tive 6-month study. Neurosurg Focus 18(2):E4, 2005
24. Sedat J, Chau Y, Mondot L, Vargas J, Szapiro J, Lonjon M: En-dovascular occlusion of intracranial wide-necked aneurysms with stenting (Neuroform) and coiling: mid-term and long-term results. Neuroradiology 51:401–409, 2009
25. Spiotta AM, Gupta R, Fiorella D, Gonugunta V, Lobo B, Ras-mussen PA, et al: Mid-term results of endovascular coiling of wide-necked aneurysms using double stents in a Y configura-tion. Neurosurgery 69:421–429, 2011
26. Vendrell JF, Costalat V, Brunel H, Riquelme C, Bonafe A: Stent-assisted coiling of complex middle cerebral artery aneu-rysms: initial and midterm results. AJNR Am J Neuroradiol 32:259–263, 2011
27. Wajnberg E, de Souza JM, Marchiori E, Gasparetto EL: Sin-gle-center experience with the Neuroform stent for endovas-cular treatment of wide-necked intracranial aneurysms. Surg Neurol 72:612–619, 2009
28. Weng HH, Jao SY, Yang CY, Tsai YH: Meta-analysis on diag-nostic accuracy of MR angiography in the follow-up of resid-ual intracranial aneurysms treated with guglielmi detachable coils. Interv Neuroradiol 14 Suppl 2:53–63, 2008
29. Yang P, Liu J, Huang Q, Zhao W, Hong B, Xu Y, et al: Endo-vascular treatment of wide-neck middle cerebral artery aneu-rysms with stents: a review of 16 cases. AJNR Am J Neuro-radiol 31:940–946, 2010
30. Yang X, Wu Z, Mu S, Li Y, Lv M: Endovascular treatment of giant and large intracranial aneurysms using the neuroform stent-assisted coil placement. Neurol Res 30:598–602, 2008
31. Yavuz K, Geyik S, Saatci I, Cekirge HS: WingSpan Stent Sys-tem in the endovascular treatment of intracranial aneurysms: clinical experience with midterm follow-up results. J Neuro-surg 109:445–453, 2008
Manuscript submitted July 3, 2012.Accepted January 14, 2013.Please include this information when citing this paper: pub-
lished online February 8, 2013; DOI: 10.3171/2013.1.JNS121298.Address correspondence to: Demetrius K. Lopes, M.D., Depart-
ment of Neurological Surgery, Rush University Medical Center, 1725 West Harrison Street, Suite 1115, Chicago, Illinois 60612. email: [email protected].