Embed Size (px)
Citation preview

DHS-State of Play
1
STATE OF PLAY: A REPORT ON THE SUPPORT AVAILABLE TO MEDICAL STUDENTS WITH SPECIFIC LEARNING DIFFICULTIES
AUTHOR: Duncan Shrewsbury, PGDip Med Ed, Adv Dip Clin Hyp., BMed Sc.
INSTITUTION: Medical School, College of Medical and Dental Sciences, The
University of Birmingham, Edgbaston, Birmingham, B15 2TT.
EMAIL: [email protected] / [email protected]
MOBILE: 07875499845
A report to the Higher Education Academy Subject Centre
October 2010

DHS-State of Play
2
State of Play: Support available to medical students with specific learning difficulties
INTRODUCTION
Specific learning difficulties (SpLD) are characterised by lifelong deficits in:
attention; concentration; reasoning; understanding; memory; or coordination.
An exact definition is difficult to pin down due to the varied nature of the
symptamology and deficits associated with SpLD. This umbrella term
encompasses conditions such as Dyslexia, Dyscalculia, Dyspraxia, Asperger’s
ABSTRACT: Medical schools in the United Kingdom (UK) implement
“reasonable adjustments” to some aspects of their course delivery and
assessment for students with Specific Learning Difficulties (SpLD). This is a
requirement within UK law, but creates some difficult challenges in medical
education. In order to support further research into the field of SpLD in
medical education, it is necessary to first establish a base line, or the current
‘state of play’, for the implementation of reasonable adjustments in UK
medical education. This study was conducted using structured telephone
interviews to collect data regarding the institutional implementation of
reasonable adjustments in all 32 UK medical schools. Data showed that
schools implement reasonable adjustments at a variable rate across the UK.
Further to this, data collected through the interviews and from the
applications service suggest that there is an increase in numbers of students
with declared SpLD being accepted onto medical degree programmes.
There is a need for more work to be done in investigating the impact that
SpLD have on student welfare and performance in medical education.
Furthermore, little evidence surrounding this issue exists, which must be
addressed for meaningful comparisons to be made and conclusions to be
drawn.

DHS-State of Play
3
Syndrome and Attention Deficit Hyperactivity Disorder (Wardin & Daniels,
1997; Open, 2006). Dyslexia, often incorrectly used synonymously with SpLD,
is the most common SpLD and is thought to affect an estimated 6% of the
global population (Miles, 2004).
In the UK, students enrolled on higher education (HE) courses in medicine
are given the opportunity to declare a diagnosis of SpLD during the University
and Colleges Admissions Service (UCAS) applications process. Further to
this, all UK HE institutions have a duty to provide support and opportunities for
students to be tested for SpLD, assessed for their education needs and
supported accordingly. Such processes are laid out in legislation in the
Disability Discrimination Act (DDA) (HMSO, 1995) and the Special Educational
Needs and Disability Act (SENDA) (HMSO, 2001). Support available can be
variable, and determined by many factors, such as the course that the student
is enrolled on, the learning environment and the learning needs of the student.
“Reasonable Adjustments” are legally required, and are to be made in order to
afford the students the same opportunity of success and achievement as other
students and aim to minimise the effects of their SpLD (DRC, 2006; DRC,
2007). In medical education this results in concerns and arguments
surrounding patient safety, competence and fitness to practise in later careers.
The General Medical Council (GMC) defines competency standards and
necessary requirements of practising doctors, as well as guidelines on
inclusion of those with disabilities within the profession (GMC, 2008). The true
impact of SpLD on an individual’s experience of medical education, as well as
their performance in the course and later career, remain undefined. However,
it is becoming increasingly accepted that the medical profession needs to
embrace diversity and that the inclusion of people with SpLD and other
disabilities in the education and practice of medicine would add value to the
profession and would not harm public trust or perception of standards (Roberts
et al., 2004).

DHS-State of Play
4
AIMS:
The primary objective of this project was to ascertain the level of support
currently available to medical students with SpLD at UK medical schools, in
order to provide baseline information for the implementation of reasonable
adjustments for students with SpLD. In addition, the project also aimed to
source basic data relating to numbers of applications made to undergraduate
courses in medicine and offers made to applicants with declared SpLD from
2004 to 2008.
METHODS
Data regarding the applications and number of acceptances to undergraduate
courses in medicine from 2004 until 2008 were acquired through the UCAS
Statistical Services (www.ucas.ac.uk). Two spokespeople from each of the 32
medical schools in the UK were contacted by telephone. In twenty-five cases,
both spokespeople were from within the medical school. In the remaining
seven, the second spokesperson was from the central University student
support service. Representatives were identified by their involvement in
curriculum support or student development. Where initial contacts were unable
to conduct telephone interviews, suitable alternatives were sought matching
the same criteria. Structured telephone interviews were conducted on an
individual basis, with responses being recorded immediately with expanded
interview notes. Interviews were structured by a set of fifteen questions.
Questions, or elements of questions, were routinely explained and clarified,
and the meaning of responses was consistently checked. For example, the
meaning of ‘Disability Champion’ was detailed to each spokesperson. The
interview protocol focused on three key areas of interest: attitudes regarding
SpLD; adjustments provided; and support available. This protocol (appendix 1)
was developed following background reading into educational support
guidelines and discussions with educational leaders (JCQ, 2009; Jamieson &
Morgan, 2008; DRC, 2006; DRC, 2007). The collected data was entered into a
spreadsheet (Microsoft Excel) and prepared for graphical representation.

DHS-State of Play
5
RESULTS
ADMISSIONS
The number of medical schools that actively encouraged the disclosure of a
diagnosis of SpLD was 56% (figure 1). Institutions were considered to actively
encourage disclosure of SpLD if there was written evidence suggesting the
consideration of special requirements that students may have for interview
processes, the provision of information and signposting further information.
Reasons, as reported by
respondents, for not
encouraging this disclosure
varied from logistical
difficulties to actively
avoiding it so as not to
create bias or prejudice
during the admissions
process.
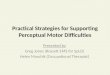
Data provided by the UCAS statistical service suggests that since 2004 the
number of students with SpLD who are applying to study medicine has
increased, from 172 (69 female, 103 male) out of a total of 15,554 applications
in 2004 to 306 (143 female, 163 male) out of 16485 applications in 2008. This
is illustrated in figure 2. The number of students that were accepted onto
courses of medicine has
concurrently increased. In
2004, 54 students (21
female, 33 male), out of
4076 students accepted
onto undergraduate
medical degree
programmes, had a
Figure 1: % of institutions that actively encourage disclosure of a diagnosis of SpLD during the admissions process
Figure 2: UCAS data showing trend in applications to the MBChB 5-year course by students with SpLD. Y-axis shows the number of students (male or female) with a learning difficulty that applied to an undergraduate medical programme.

DHS-State of Play
6
declared SpLD. This increased to 116 (66 female, 50 male) out of 6047 in
2008 (figure 3).
ADMINISTRATIVE SUPPORT
Administrative support for staff and students was considered to comprise:
student support services specifically dedicated to medical students, the
appointment of a ‘Disability Champion’ and the provision of specialised training
for academic staff to raise awareness of SpLD in medical education. Of the 32
schools, 65.6% (21) provided a student support service dedicated to the
medical students on their course, 75% (24) had a designated disability
champion and 18.8% (6) provided staff training for dealing with SpLD
specifically in medical education. 44% (14) provided both a dedicated student
support service and had a designated disability champion, 6% (2) of the
medical schools had an appointed disability champion and provided specific
staff training, whilst 1 school provided a dedicated student support service and
specific staff training. A total of 3 of schools provided all three.
WELFARE SUPPORT
Of the 32 medical schools, 87.5% (28) provided a welfare, or personal
tutoring, system dedicated to their medical students. Of the remaining 4, three
medical schools were based at institutions which had collegiate systems with
their own, individual, welfare and support systems in place. One medical
Figure 3: UCAS data showing trend in acceptance to the MBChB 5-year course by students with SpLD. Y-axis shows the number of students (male or female) with a learning difficulty that were accepted on to an undergraduate medical programme.

DHS-State of Play
7
school did not have a welfare system in place, but did provide specialised
support through one dedicated individual. Where there were tutors (or mentor),
the mean number of students in each tutor group was 16, with the number
ranging from as few as 5 and as many as 45. The modal average was 10
students per group.
REASONABLE ADJUSTMENTS
Out of a possible 11
reasonable adjustments that
are most commonly
recommended at HE
(Jamieson & Morgan, 2008;
DRC, 2007), 40% of medical
schools provided all,
depending on individual
needs assessments and
educational psychologist
reports. Figure 4 shows the
distribution of compliance with this standard across the 32 medical schools.
Figure 5 illustrates the pattern of how the 11 reasonable adjustments are
implemented, suggesting that assistance with proof reading of written work is
the least employed.
Figure 4: Proportion of medical schools providing all (11) or as few as 5 reasonable adjustments (RAs)
Figure 5: The pattern of provision of the 11 reasonable adjustments in all 32 medical schools. Y-axis show % of schools providing the specific reasonable adjustments.

DHS-State of Play
8
Five medical schools currently implement, or are experimenting with, the
implementation of reasonable adjustments in clinical placements and exams,
such as Objective Structured Clinical Exams (OSCE). Experimental
adjustments varied between the institutions. Examples include: providing extra
rest time between OSCE stations; and printing scenarios on a different
coloured paper with extra reading time during OSCE.
DISCUSSION
STRENGTHS & WEAKNESSES OF STUDY
This is the first study in the field of medical education to take a look at the
implementation of reasonable adjustments across a whole country. All medical
schools in the UK were included in this enquiry. This provides some baseline
evidence for an increasingly important debate, and can guide further work in
the area of student support in medical education.
However, whilst this study includes all UK medical schools, it is only a
preliminary investigation into what support is offered, and quite how SpLD
impact on medical education. Interpretation of the findings is limited due to the
lack of comparison with other countries, and previous studies. As the
evidence-base around the area of SpLD in medical education increases, more
such data will be available to draw upon and make such comparisons.
ADMISSIONS
As these data lack comparison with rates of diagnosis, it is not possible to infer
whether this means that more students with SpLD are actually applying and
being accepted, as it could simply mean that either the number of people with
a diagnosis of SpLD, or the rate of initial disclosure, has increased over the
last four years (figure 2). However, the data suggest that there are a greater
number of students entering medical course with a recognised and declared
diagnosis of SpLD. It would be useful to compare this to rates of diagnosis and

DHS-State of Play
9
declaration once enrolled on the course. This increase could reflect changes in
attitudes surrounding, and perceptions of, SpLD in the Health Care profession
and an increased trust in equality throughout admissions procedures (Morris &
Turnbull, 2007; Miller et al., 2009).
Active encouragement of disclosure occurred in 56% of medical schools.
However, this figure is open to interpretation. During the interviews, the
meaning of the statement was specified as an active attempt at providing
information and encouraging the confidential disclosure of a diagnosis.
Concerns were raised about the nature of such encouragement, with
representatives stating that they specifically avoided encouraging disclosure
so as to prevent “positive discrimination”. This suggests that there is still some
work to be done on refining the admissions process in terms of how and when
disclosure is sought, and the nature of the security of this information in
relation to the application process.
ADMINISTRATIVE SUPPORT
Seventy-five percent of UK medical schools had a designated member of staff
acting as a “Disability Champion”. The purpose of such a title and role is to
promote awareness of issues surrounding disability in students and staff within
their institution. This could mean that the individual is responsible for
coordinating Impact Assessments (DRC, 2006; DRC, 2007). The title ascribed
to this role was queried, with concerns raised about how it “doesn’t sound
right” and how it may have unhelpful connotations associated with it.
Institutional use of the actual term “Disability Champion” differed, with some
preferring to use the title Disability Liaison Officer or similar. The function of
the role was apparently consistent regardless of the title. However, some
individuals accepted extra responsibilities, linked to welfare and study skills
support.
Six out of the 32 schools provided specialised training for staff involved in
curriculum development and delivery, regarding students with SpLD. This
figure reflects the logistical difficulties in providing such training, and making it

DHS-State of Play
10
available and accessible to clinicians and academics, as well as others
involved in medical course. Many schools (21) provided this training on a
voluntary basis through central services. Such training was not specific to the
context of medical education, and the popularity and success of such courses
is unquantified.
WELFARE SUPPORT
Twenty-eight of the 32 UK medical schools provided a welfare support system
specifically dedicated to their medical students. Mental illness is over-
represented in medical student populations, and the study of medicine is
associated with a great number of stressors and demands (Dyrbye et al.,
2006). This highlights the need for a support system specifically tailored to the
demographic of medical students, as well as the course. Medical students with
SpLD often struggle with specific elements of the course or assessment that
overwhelm their coping strategies. Such events can prove to be highly
stressful, and deleterious to students’ welfare (Rosebraugh, 2000; Takakuwa,
1998). Further work need to be done in this area before significant
recommendations can be inferred, however it may be beneficial for those
involved in the welfare support of medical students to be able to integrate
insight into and support of SpLD with this role.
REASONABLE ADJUSTMENTS
As there is a lack of significant evidence supporting or refuting the use of
reasonable adjustments in medical education, it is impossible to comment on
how the varied institutional implementation of the 11, commonly considered
standard, adjustments relates to performance. The provision of specific
support, in the form of extra time granted in written assessments, or allowance
for the use of recording equipment is dependant on a Learning Needs
Assessment. Such assessments are conducted through University, usually
centralised, services and require a formal diagnosis of a disability or SpLD to
be initiated. Resultant reports may recommend specific adjustments to the

DHS-State of Play
11
delivery of course material, support of learning and allowance in assessments.
However, effective implementation relies heavily on logistics and practicalities
dictated by reality and specific factors associated with the course. In medicine,
for example, it would be impractical to have assistance in note taking whilst on
clinical placement.
The only conclusions that can be drawn from these results are that the
implementation of reasonable adjustments are variable across the country, but
that there are certain adjustments that are very well implemented, such as
allowing the use of audio recording equipment in lectures and the provision of
Virtual Learning Environment facilities and support. An adjustment that was
not well implemented was the facility for students to have help with proof
reading work. This may be due to the impracticalities, due to the high volume
of written work associated with the course. However, through the interviews, it
became apparent that medical students are often subject to expectations that
are incongruent with the provision of some adjustments.
RECOMMENDATIONS
This investigation highlights the need for greater communication and sharing
of examples of good practice. It would be wise to encourage an open forum for
discussion and sharing of experiences among staff and students, so as to
establish a good base of knowledge and evidence, even if anecdotal,
regarding the support of SpLD in medical education.
FURTHER WORK
Having established a baseline for support available in medical education in the
UK, it would be useful to compare this to global standards, sharing examples
of good practice and ascertaining a wider evidence and knowledge base for
the true impact of, and help required for, SpLD in medical education. There
are yet further landmarks to be achieved in defining and identifying SpLD in

DHS-State of Play
12
medical education as well as the impact that they have on performance as a
student and as a practicing clinician.
CONCLUSION
Of the 32 medical schools, 60% do not currently implement the 11 basic
reasonable adjustments investigated. Forty-four percent do not actively
encourage disclosure of a diagnosis of SpLD during the admissions process.
This demonstrates a varied following of current guidelines. However, without
an evidence base supporting the various arguments surrounding the
institutional decisions, or a comparison between this level of performance and
the effect on student’s educational experience it is not possible to suggest
whether these results reflect positively or a negatively. It became clear,
throughout the investigations, that there is still a degree of tension surrounding
the issue of SpLD in medical education and implementing adjustments for
students. Overall, institutions remain positive, encouraging diversity and
supporting students in various ways, which is exemplified by the experimental
implementation of reasonable adjustments in OSCE by 5 of the medical
schools in this study. In order to optimise student performance and to dispel
stigma and related issues surrounding SpLD and the provision of related
supporting measures, it is clear that there is much work to be done in
qualifying and quantifying the use, drawbacks and positive effects of SpLD
and reasonable adjustments in medical education.
KEY POINTS
1. Forty percent of UK medical schools provide all 11 ‘core’ reasonable adjustments.
2. The number of students, with a disclosed diagnosis of SpLD, entering medical degree programmes has increased.
3. Little evidence exists detailing the benefits and costs of reasonable adjustments in medical education.
4. Further investigation into this field should be supported, to ensure meaningful comparison.

DHS-State of Play
13
NOTES ON AUTHOR
Duncan Shrewsbury is a 5th year medical student at the University of
Birmingham and is concurrently completing a Masters in medical education at
Staffordshire University.
ACKNOWLEDGEMENTS
Many thanks are owed to Professor John Skelton, who was immensely helpful
in the preparation of this report.
REFERENCES
Disability Discrimination Act, 1995. London: HMSO.
(DRC) Disability Rights Commission. 2006.
Further and Higher Education Institutions and the Disability Equality Duty.
Do the Duty.
Accessed on 21/2/2010 via:
http://www.dotheduty.org/index.asp
Disability Rights Commission. 2007.
Code of practice (revised) for post-16 education.
The Higher Education Academy: Medicine, Dentistry and Veterinary
Accessed on 21/2/2010 via:
http://www.equalityhumanrights.com/advice-and-guidance/information-for-
advisers/codes-of-practice/
Dyrbye LN, Thomas MR, Shanafelt TD. 2006.
Systematic review of depression, anxiety, and other indicators of psychological
distress among U.S. and Canadian medical students.
Academic Medicine. 81:354e73.

DHS-State of Play
14
(GMC) General Medical Council and The Department for Innovation,
Universities and Skills. 2008.
Gateways to the Professions: advising medical schools, encouraging disabled
students.
General Medical Council, London.
Jamieson C and Morgan E. 2008.
Managing Dyslexia at University.
Routledge, Oxford.
(JCQ) Joint Council for Qualifications. 2007.
Access arrangements, reasonable adjustments and special consideration:
general and vocational qualifications. With effect from 01/09/2009.
Miles TR. 2004.
Some problems in determining the prevalence of dyslexia.
The Electronic Journal for Research in Educational Psychology, 2: 5-12.
Miller S, Ross S and Cleland J. 2009.
Medical students’ attitudes towards disability and support for disability in
medicine.
Medical Teacher, 31: e272-e377.
Morris DK Turnbull PA. 2007.
The disclosure of dyslexia in clinical practice: Experiences of student nurses in
the United Kingdom.
Nurse Education Today, 27: 35-42.
(Open) Open University. 2006.
What are specific learning difficulties?
Open University, Milton Keynes.
Accessed on 1/2/2010 via:
http://www.open.ac.uk/inclusiveteaching/pages/understanding-and-
awareness/what-are-specific-learning-difficulties.php

DHS-State of Play
15
Roberts TE, Butler A and Bouriscot KAM. 2004.
Disabled students, disabled doctors – time for a change? A study of different
societal views of disabled people’s inclusion to the study and practice of
medicine.
Higher Education Academy Subject Centre for Medicine, Dentistry and
Veterinary Medicine, Special Report: 4.
Special Educational Needs and Disability Act, 2001. London: HMSO.
Takakuwa K. 1998.
Coping with a Learning Disability in Medical School.
Journal of the American Medical Association, 298: 81.
Wardin M, Daniels C. 1997.
Definition of Specific Learning Disability.
Conference Proceedings from the Technology and Persons with Disabilities
Conference.
California State University Northridge.
Accessed on 25/2/2010 via:
http://www.csun.edu/cod/conf/1997/proceedings/120.htm

DHS-State of Play
16
APPENDIX 1
Interview Protocol:
Questions asked over the phone, of all UK Medical Schools, as directed by initial contact through general enquiry telephone numbers.
UNIVERISTY: ___________________________________
1. Do you actively encourage people to disclose diagnosis of SLD during
admissions process?
2. Do you / University provide screening for SLD?
i. Is this free, or do the students have to pay?
3. Do you provide a student support service dedicated to Medical
Students?
4. Are there dedicated staff within the Medical School that are designated
as ‘Disability Champions’?
5. Is there training or an incentive to raise awareness of dyslexia within
Medical Education within your institution?
6. Do you have a Student Welfare / Tutoring system dedicated to your
Medical Students?
7. How many students does each tutor look after?
8. Are these tutors trained in helping with study skills?
9. Is there provision for study skills workshops or training at your:
• Medical School, specific to Medical Education ☐
• University, specific to Medical Education ☐
• University, not specific to Medical Education? ☐
10. Do your dyslexic students currently get:
a. Extra 25% time in written exams?
i. If not- why

DHS-State of Play
17
ii. If more- detail
b. Advice on DSA?
c. Study Skills Support?
d. Reasonable adjustments?
(Detail.....................................................)
List of ‘Standard’ reasonable adjustments:
• Assistive Technologies ☐
• Handouts (24hs in advance?) ☐
• Virtual Learning Environment ☐
• Accessibility technology ☐
• Extended library loans ☐
• Access to dyslexia tutor ☐
• Photocopying ☐
• Printing ☐
• IT training ☐
• Note taking assistance ☐
• Dictaphone ☐
• Help with proof read ☐