Embed Size (px)
Citation preview

MEETING NOTICE AND AGENDA
AGENDA
1. Open Meeting; Roll Call
2. Public Comment
Public comment will be taken during this agenda item. No action may be taken on any matter
raised under this item unless the matter is included on a future agenda as an item on which
action may be taken. Public comments to the Board will be taken under advisement but will
not be answered during the meeting. Comments may be limited to three minutes per person
at the discretion of the chairperson. Additional three minute comment periods may be allowed
on individual agenda items at the discretion of the chairperson. These additional comment
periods shall be limited to comments relevant to the agenda item under consideration by the
Board. Persons unable to attend the meeting and persons whose comments may extend past
the three minute time limit may submit their public comment in writing to PEBP Attn: Laura
Landry 901 S. Stewart St, Suite 1001 Carson City NV 89701, Fax: (775) 684-7028 or
[email protected] at least two business days prior to the meeting. Persons making
public comment need to state and spell their name for the record at the beginning of their
testimony.
3. PEBP Board disclosures for applicable Board meeting agenda items. (Brandee Mooneyhan,
Deputy Attorney General) (Information/Discussion)
Name of Organization: Public Employees’ Benefits Program Board
Date and Time of Meeting: November 29, 2018 8:30 a.m.
Place of Meeting: The Richard H. Bryan Building
901 South Stewart Street, Suite 1002
Carson City, Nevada 89701
Video Conferencing:
Video Streaming Website:
Nevada State Business Center
3300 West Sahara Avenue
Tahoe Room, Suite 430
Las Vegas, Nevada 89102 www.pebp.state.nv.us
BRIAN SANDOVAL
Governor
PATRICK CATES
Board Chairman
DAMON HAYCOCK
Executive Officer
STATE OF NEVADA
PUBLIC EMPLOYEES’ BENEFITS PROGRAM 901 S. Stewart Street, Suite 1001 | Carson City, Nevada 89701
Telephone 775-684-7000 | 1-800-326-5496 | Fax 775-684-7028
www.pebp.state.nv.us

Public Employees’ Benefits Program Board
November 29, 2018 Agenda – Page 2
4. Consent Agenda (Patrick Cates, Board Chair) (All Items for Possible Action as specified
below)
Consent items will be considered together and acted on in one motion unless an item is
removed to be considered separately by the Board.
4.1. Approval of the Action Minutes from the September 27, 2018 PEBP Board Meeting.
4.2. Receipt of the Casey, Neilon & Associates Audited Financial Statements of PEBP for
Fiscal Year 2018.
5. Health Claim Auditors, Inc. quarterly audit of HealthSCOPE Benefits for the timeframe July
1, 2018 – September 30, 2018: (1) Report from Health Claim Auditors; (2) HealthSCOPE
Benefits response to audit report; and (3) for possible action to accept audit report findings and
assess penalties, if applicable, in accordance with the performance guarantees included in the
contract pursuant to the recommendation of Health Claim Auditors. (For Possible Action)
6. Health Claim Auditors, Inc. annual audit of Willis Towers Watson’s OneExchange for the
timeframe July 1, 2017 – June 30, 2018: (1) Report from Health Claim Auditors; (2) Willis
Towers Watson's response to audit report; and (3) for possible action to accept audit report
findings and assess penalties, if applicable, in accordance with the performance guarantees
included in the contract pursuant to the recommendation of Health Claim Auditors. (For
Possible Action)
7. Presentation on PEBP’s Fiscal Year 2020/2021 Agency Request Budget.
(Information/Discussion) (Celestena Glover, Chief Financial Officer)
8. Executive Officer Report. (Damon Haycock, Executive Officer) (Information/Discussion)
9. Discussion and possible action regarding Plan Year 2020 through 2021 Preferred Provider
Organization (PPO) network options and the potential to (1) continue the current contract with
Hometown Health Providers through 2021 or (2) issue a no-fault contract termination and join
the State on a solicitation for PPO networks. (Damon Haycock, Executive Officer) (For
Possible Action)
10. Discussion and possible action regarding the Morneau Shepell Voluntary Benefits Platform
and benefit selection for Plan Year 2020 offerings to members on the Consumer Driven Health
Plan (CDHP), PEBP Premier Plan (EPO), southern Nevada Health Maintenance Organization
plan (HPN), and Via Benefits (Medicare Exchange). Proposed benefits and providers include,
but not limited to:
Accident, Critical Illness, and Hospital Indemnity (Aflac, Allstate, MetLife, Reliance,
The Standard);
Identification (ID) Theft Protection (ID Watchdog, InfoArmor);
Legal Plan Provisions (Nationwide LegalEASE, Hyatt Legal);
Automobile, Home, and Renters Insurance (MetLife, Liberty Mutual, Travelers);
Pet Insurance (ASPCA, Nationwide);
Vision Plan Services (VSP)
(Laura Rich, Operations Officer) (For Possible Action)
11. Discussion and possible action regarding proposed plan design changes for Plan Year 2020 (July 1, 2019 – June 30, 2020), including but not limited to the following:

Public Employees’ Benefits Program Board
November 29, 2018 Agenda – Page 3
Possible disallowing pharmacy patient assistance programs (manufacturers’ coupons,
etc.) from applying to the CDHP individual/family deductibles and out-of-pocket
maximums;
Possible implementation of mandatory narrow pharmacy network for 90-day
prescriptions;
Possible implementation of a patient safety program managed by PEBP’s pharmacy
benefits manager;
Possible additional cost containment activities;
Possible increases and requirements to CDHP HSA/HRA enhanced employer
contributions;
Possible requirement for Medicare exchange participants to pay for their HRA
administration fees and life insurance premiums;
Possible elimination of the $25 copay for annual vision exams.
Possible increases to the dental benefit maximums of the CDHP, EPO, HMO, and
Medicare Exchange participants.
Possible implementation of a pilot nutrition program in southern Nevada.
Possible increase to Medicare Part B credits to retirees on the CDHP, EPO, and HMO
plans;
Possible plan design changes to the HMO/EPO copays for primary care, specialist
visits, emergency room visits, generic drugs, and specialty drug coinsurance;
Additional benefit design inclusions/exclusions/alterations to meet projected budget
needs.
(Damon Haycock, Executive Officer) (All Items for Possible Action)
12. Public Comment
Public comment will be taken during this agenda item. Comments may be limited to three
minutes per person at the discretion of the chairperson. Persons making public comment need
to state and spell their name for the record at the beginning of their testimony.
13. Adjournment
The supporting material to this agenda, also known as the Board Packet, is available, at no
charge, on the PEBP website at www.pebp.state.nv.us/board.htm (under the Board Meeting date
referenced above).
An item raised during a report or public comment may be discussed but may not be deliberated
or acted upon unless it is on the agenda as an action item.
All times are approximate. The Board reserves the right to take items in a different order or to
combine two or more agenda items for consideration to accomplish business in the most
efficient manner. The Board may remove an item from the agenda or delay discussion relating
to an item on the agenda at any time. The Board reserves the right to limit Internet broadcasting
during portions of the meeting that need to be confidential or closed.
We are pleased to make reasonable efforts to assist and accommodate persons with physical
disabilities who wish to attend the meeting. If special arrangements for the meeting are
necessary, please notify the PEBP in writing, at 901 South Stewart Street, Suite 1001, Carson
City, NV 89701, or call Laura Landry at (775) 684-7020 or (800) 326-5496, as soon as possible
so that reasonable efforts can be made to accommodate the request.

Public Employees’ Benefits Program Board
November 29, 2018 Agenda – Page 4
Copies of both the PEBP Meeting Action Minutes and Meeting Transcripts are available for
inspection, at no charge, at the PEBP Office, 901 South Stewart Street, Suite 1001, Carson City,
Nevada, 89701 or on the PEBP website at www.pebp.state.nv.us. For additional information,
contact Laura Landry at (775) 684-7020 or (800) 326-5496.
Notice of this meeting was posted on or before 9:00 a.m. on the third working day before the
meeting at the following locations: NEVADA STATE LIBRARY & ARCHIVES, 100 N.
Stewart St, Carson City; BLASDEL BUILDING, 209 East Musser Street, Carson City; PUBLIC
EMPLOYEES’ BENEFITS PROGRAM, 901 South Stewart Street, Suite 1001, Carson City;
THE GRANT SAWYER STATE OFFICE BUILDING, 555 East Washington Avenue, Las
Vegas; THE LEGISLATIVE BUILDING, 401 South Carson Street, Carson City, and on the
PEBP website at www.pebp.state.nv.us, also posted to the public notice website for meetings at
https://notice.nv.gov. In addition, the agenda was mailed to groups and individuals as requested.

1. 1. Open Meeting; Roll Call


2. 2. Public Comment


3. 3. PEBP Board disclosures for applicable Board meeting
agenda items. (Brandee Mooneyhan, Deputy Attorney General) (Information/Discussion)


4. 4. Consent Agenda (Patrick Cates, Board Chair) (All Items for
Possible Action as specified below) Consent items will be considered together and acted on in one motion unless an item is removed to be considered separately by the Board. 4.1. Approval of the Action Minutes from the September 27,
2018 PEBP Board Meeting. 4.2. Receipt of the Casey, Neilon & Associates Audited
Financial Statements of PEBP for Fiscal Year 2018.

4.1. 4. Consent Agenda (Patrick Cates, Board Chair) (All Items for
Possible Action as specified below) Consent items will be considered together and acted on in one motion unless an item is removed to be considered separately by the Board. 4.1. Approval of the Action Minutes from the September 27,
2018 PEBP Board Meeting.


STATE OF NEVADA
PUBLIC EMPLOYEES’ BENEFITS PROGRAM
BOARD MEETING
The Legislative Building 401 South Carson Street, Room #1214
Carson City NV 89701 Video conferenced to:
The Grant Sawyer State Office Building
555 East Washington Avenue, Room #4412
Las Vegas NV 89101
---------------------------------------------------------------------------------------------------------------------
ACTION MINUTES (Subject to Board Approval)
September 27, 2018
MEMBERS PRESENT
IN CARSON CITY: Mr. Patrick Cates, Board Chair
Mr. Don Bailey, Vice Chair
Ms. Jennifer Bonilla, Member
Ms. Leah Lamborn, Member
Mr. Glenn Shippey, Member
Mr. Tom Verducci, Member
MEMBERS PRESENT
IN LAS VEGAS: Ms. Linda Fox, Member
Ms. Christine Zack, Member
Mr. John Packham, Member
FOR THE BOARD: Mr. Dennis Belcourt, Deputy Attorney General
FOR STAFF: Mr. Damon Haycock, Executive Officer
Ms. Celestena Glover, Chief Financial Officer
Ms. Laura Rich, Operations Officer
Ms. Laura Landry, Executive Assistant

Public Employees’ Benefits Program Board
September 27, 2018 Action Minutes – Page 2
1. Open Meeting: Roll Call
Chair Cates opened the meeting at 9:03 a.m.
2. Public Comment
Public Comment in Carson City:
Jon Bakkedahl – PEBP Participant
Kent Ervin – Nevada Faculty Alliance
Stephanie Parker - PEBP Participant
Public Comment in Las Vegas:
There was no public comment in Las Vegas.
3. PEBP Board disclosures for applicable Board meeting agenda items. (Dennis Belcourt,
Deputy Attorney General) (Information/Discussion)
4. Consent Agenda (Patrick Cates, Board Chair) (All Items for Possible Action)
Consent items will be considered together and acted on in one motion unless an item is
removed to be considered separately by the Board.
4.1. Approval of the Action Minutes from the July 26, 2018 PEBP Board Meeting.
4.2. Receipt of PEBP Chief Financial Officer annual reports for year ending June 30, 2018:
4.2.1. Budget Report
4.2.2. Utilization Report
4.3. Receipt of annual vendor reports for timeframe July 1, 2017 - June 30, 2018:
4.3.1. HealthSCOPE Benefits – Obesity Care Management Program
4.3.2. Hometown Health Providers – Utilization and Large Case Management
4.3.3. The Standard Insurance – Basic Life and Long Term Disability Insurance
4.3.4. Willis Towers Watson - Individual Marketplace Enrollment & Performance
Report
4.4. Health Claim Auditors, Inc. quarterly audit of HealthSCOPE Benefits for the
timeframe April 1, 2018 – June 30, 2018:
4.4.1. Report from Health Claim Auditors
4.4.2. HealthSCOPE Benefits response to audit report
4.4.3. Accept audit report findings and assess penalties, if applicable, in accordance
with the performance guarantees included in the contract pursuant to the
recommendation of Health Claim Auditors.
4.5. Receipt of the PEBP Biennial Legal Compliance Review report performed by Aon.
Public Employees’ Benefits Program Board
September 27, 2018 Action Minutes – Page 3
Board Action on Item 4 -
MOTION: Motion to accept all items on the consent agenda.
BY: Vice Chair Don Bailey
SECOND: Member Leah Lamborn
VOTE: Unanimous; the motion carried.
5. Presentation on the State of PEBP. (Damon Haycock, Executive Officer)
(Information/Discussion)
6. Discussion and possible board direction regarding updating the PEBP Strategic Plan. (Damon
Haycock, Executive Officer) (For Possible Action)
Public Comment on Item 6 -
Public Comment in Carson City:
Peggy Lear Bowen - Retiree Participant (See Exhibit A for comments)
Public Comment in Las Vegas:
There was no public comment in Las Vegas.
Board Action on Item 6 -
MOTION: Motion to update the PEBP Strategic Plan as outlined today.
BY: Member Christine Zack
SECOND: Member Jennifer Bonilla
VOTE: Unanimous; the motion carried.
7. Discussion and possible action on providing PEBP staff final approval on a 2-year
amendment to the Morneau Shepell contract for eligibility and enrollment system
enhancements with a new fully integrated voluntary benefit platform. (Damon Haycock,
Executive Officer) (For Possible Action)
Board Action on Item 7 -
MOTION: Motion to provide the final approval for a two year contract extension as
recommended.
BY: Vice Chair Don Bailey
SECOND: Member Tom Verducci
VOTE: Unanimous; the motion carried.
8. Discussion and possible action regarding the Morneau Shepell Voluntary Benefits Platform
and benefit selection for Plan Year 2020 offerings to members on the Consumer Driven
Health Plan (CDHP), PEBP Premier Plan (EPO), southern Nevada Health Maintenance
Organization plan (HPN), and Via Benefits (Medicare Exchange). Proposed benefits include,
but not limited to:
Accident, Critical Illness, and Hospital Indemnity;
Identification (ID) Theft Protection;

Public Employees’ Benefits Program Board
September 27, 2018 Action Minutes – Page 4
Legal Plan Provisions;
Automobile, Home, and Renters Insurance;
Pet Insurance;
Payroll Purchasing Program;
Vision Plan Services
(Laura Rich, Operations Officer) (For Possible Action)
Public Comment on Item 8 -
Public Comment in Carson City:
Kent Ervin - Nevada Faculty Alliance
Priscilla Maloney - Representative of AFSCME retirees
Public Comment in Las Vegas:
There was no public comment in Las Vegas.
Board Action on Item 8 -
After consulting with legal counsel Chair Cates made a recommendation that this item be
reconstructed and brought back at the November 29th Board Meeting for further discussion. The
agenda item was constructed to discuss offering benefits not selecting particular providers. The
item was closed, no action taken.
9. Discussion and possible direction from the Board to staff on potential program design changes
for Plan Year 2020 (July 1, 2019 to June 30, 2020) for which the Board requests additional
information and costs to be presented at the November 29, 2018 meeting. (Damon Haycock,
Executive Officer) (For Possible Action)
Public Comment on Item 9 -
Public Comment in Carson City:
Jon Hager – Hometown Health
Terri Laird – Executive Director of RPEN
Priscilla Maloney - Representative of AFSCME retirees
Kent Ervin - Nevada Faculty Alliance
Kevin Ranft – AFSCME 4041
Peggy Lear Bowen - Retiree Participant (See Exhibit A for comments)
Public Comment in Las Vegas:
There was no public comment in Las Vegas.
Board Action on Item 9 -
MOTION: Motion to approve going forward with exploring all of the different options with
the addition of analyzing cost savings of RX coupons and how that may or may
not apply to accumulators, pricing out the cost of eliminating the $25 vision copay
and looking into increasing the dental maximum.

Public Employees’ Benefits Program Board
September 27, 2018 Action Minutes – Page 5
BY: Member Christine Zack
SECOND: Member Linda Fox
VOTE: Unanimous; the motion carried.
10. Public Comment
Public Comment in Carson City:
Peggy Lear Bowen - Retiree Participant (See Exhibit A for comments)
Public Comment in Las Vegas:
There was no public comment in Las Vegas.
11. Adjournment
Chair Cates adjourned the meeting at 1:00 p.m.


Exhibit A

These remarks are presented as transcribed by Capitol Reporters. AGENDA ITEM 6 - PUBLIC COMMENT FROM MS. BOWEN: MS. BOWEN: Good morning. My name and words for the record, my name Peggy, P-e-g-g-y Lear, L-e-a-r Bowen B-o-w-e-n. The comment I would like to make had to do with the workshop and with the survey questions. I felt and members with me felt that the survey we requested during the meeting made it very formal that when the survey was to be put together that members of the -- of us, meaning the clients of PEBP, whether they be from the University or whatever, that we members be involved in the creation of the survey questions because it's all in what you're looking for and the answers you're trying to seek in making this survey better to make the reach the need of what we need from the people from PEBP. Secondly, the survey and who was selected to receive it, both the head of RPEN and Elaine Steiner and I was one, we weren't selected to receive the survey. So we don't know who answered the questions. We don't know what the questions -- what groups were represented in the answering of questions and, therefore, we don't know if the survey -- I don't feel, Peggy Lear Bowen personally as an individual feels this survey lacked validity in terms of -- in terms of who was selected, what groups were selected. CHAIRMAN CATES: Hey, Peggy -- MS. BOWEN: And who was answering the questions. CHAIRMAN CATES: This is Agenda Item Six about the strategic plan. MS. BOWEN: And the strategic plan pertains to the strategic plan meeting that none of those people were represented in terms of sitting in on the strategic plan and setting the strategic plan records and setting what benefits and things like that would be considered. In strategic planning, you need to know what -- what you're -- and that's why I brought up the survey. You need to know what the members are asking for and what the strategic plan can include. And it was felt that within the planning and the survey that resulted thereafter that we the people were left out, and I wanted to make that point very very clear about the strategic plan. And -- and it felt like the same thing that happened about four or five years ago, well, in 2011, that things were being designed and created to benefit the insurance companies rather than to benefit the members, and that we have ended up with a virtual insurance plan. That means that you go in and find out what's wrong. You go to your eye doctor and find out you need glasses and then whether or not they are going to be included. You go to your physical, find out what you need your follow-up, but our insurance doesn't cover the actual follow-up, and those needed to be included in the plan and in the questioning and everything about the strategic plan so that PEBP is no longer a virtual insurance company, telling you what you need and then you're responsible for paying for it. And when it comes to the deductibles and things like that in the strategic plan you're working on, that it ends up -- that you end up paying over $4,000 to -- to -- in deductibles because you have several deductibles involved in what you're doing so that we don't have a realistic deductible for the individual member and so we don't utilize your plan, and that we wait until we get to the emergency room because that's what we can finally afford because we know it will incorporate that $4,000. Thank you very much for your time.

AGENDA ITEM 9 - PUBLIC COMMENT FROM MS. BOWEN: MS. BOWEN: My name and words for the record Peggy, P-e-g-g-y Lear, L-e-a-r Bowen, B-o-w-e-n. And I have a request to make of you. Since our last meeting, I have incurred a sunstroke, an actual stroke 17 because of heat and -- and -- and an ongoing situation where I received a concussion during an accident that I also had thoracic outlet which meant that oxygen is not going to the brain as well as it should. Things have been taken care of as far as my sleep goes. I had a sleep study done and my machine -- CHAIRMAN CATES: Peggy? Peggy? getting more oxygen to the brain. CHAIRMAN CATES: This is -- Peggy? MS. BOWEN: But I would request your patience. The comments I want to make pertain to -- CHAIRMAN CATES: Okay. MS. BOWEN: -- and I wrote them down so I could be very careful. Access and affordability are the two concerns here regarding the hospitals and that we have a situation under the current contract where the hospital that is offering the best care as far as the star rating goes, the national rating for hospitals, Churchill County provides the best care for certain activities but because they are not part of the current contract, people cannot access that without going outside of your insurance plan. We need to have that access affordability and quality as to healthcare. You're just not dollars and cents here but actual quality. And people who live next door to the Churchill County Hospital cannot utilize it under an exclusivity plan. They can only go to where a less qualified lower starred hospital exists, and I need you to take that in consideration while you're determining these contracts while that which is going on and while you're extending contracts. These extensions should be not just letting Hometown Health continue with same old same old, which they have been providing the whole time, and people not getting the care and closeness of care and how we need to go forward and putting out for their room rates and food rates for out of town sorts of things when they have a hospital sitting within two miles of their home that they can't access under an exclusivity clause with Renown. You're rewarding a hospital that has lied to you. You're rewarding a group that has not been up and up, who have changed back and forth, the way it's even been discussed here today, and you reward them with a continuation or extension of their contract to do these sorts of things. The RFP which you're working on is fine, but we just -- we just need that covered. As far as having those insured retirement was the only game in town that brought people to native Nevada jobs that were underpaying. We need you to know that you now don't have a reason for underpaid jobs by the State of Nevada for people to come and go to work for you for any period of time because the insurance isn't there. Three minutes has been hit. Thank you very much for your time and consideration, and I'm going to go celebrate the rest of my 69th birthday today with my family. Thank you.
AGENDA ITEM 10 - PUBLIC COMMENT FROM MS. BOWEN: MS. BOWEN: My name and words for the record P-e-g-g-y, Peggy Lear, L-e-a-r Bowen, B-o-w-e-n. Bowen is my last name, no dashes or slashes. Regarding two things that were of concern, the workshop that was held, I don't know who, what, if any, insurance companies were present during that workshop. I heard who wasn't present. I'm concerned that it was a repeat and it takes away from transparency. When you call it a workshop, you don't necessarily have to follow any other open

meeting laws to my knowledge. The try was there not to have a quorum, and Mr. Damon Haycock said there wasn't a quorum so I take the man at his word. He's always been truthful as far as I know, and he's a good person and working hard and doing the best he can, and that's from Peggy to him, thank you very much, and to this Board thank you for all of your hard work that you do. Regarding those who are uninsured after 2012, think I heard a request for a bill draft to be done by this Board in conjunction with everyone else that -- that a bill draft include that the workers who -- who cease working are hired after 2012 so that they too have retirement so Nevada maintains that benefit. The reserves, I want to remind you the reserves are still accruing. It's like it was never mentioned today and Ms. Lockard, if she mentioned earlier I don't know, but I do know that you are constantly incurring reserves and that those reserves are available for you in the future. And so when you're talking about spending down money, it's not like you're going broke, and I don't want that mindset to be left with you. You're not going broke. You have reserves that you incur at all times when premiums are being paid and not being used. I'm glad to see you can know if people exist and if they are meeting your wellness requirements without involving anything to do with computers or doctor, and I believe Mr. Haycock worked on that, but no one in order to receive their benefits or anything else with PEBP should ever ever have to go on a computer. I had to come down and physically utilize your computers to get on your program in order to receive my health benefits that I've already paid for and have earned, and I don't believe the majority of your people maybe being poor or -- or -- or elderly should have to go on a computer in order to receive their health benefits that were guaranteed through contract and belief. I shouldn't have to -- and what happens is if they don't get benefits from you, then PERS can at some point cancel their PERS check because they don't believe you exist. The way you prove existence is this, whether or not they have been to a doctor and you've received a bill, whether or not they have met your four compliances for existing, that is to get their vision checked, get their physical, get their blood work and to, there's a fourth one, Damon, I'm losing it, and your dental. If people -- if you have dental bills submitted, if you have, which you do, you have eye check bills, you have any of the bills submitted from doctors, that means those people are still alive, and I've talked with PERS about how do they check to make sure their PERS check aren't going to a dead person or otherwise being misused, and the same thing, they work interactive with you. Thank you. And they went to Damon's computer. I want to make sure that you haven't made a person lose their benefits because of some computer requirement to give you some statistic to make you happy and make your data look good. Get back to the reality of when I go to the doctor and I've met my deductibles which are $4,000 total because you have to meet them all in order to get to your first 80/20. Please make our insurance so that it's usable and people will go to the emergency -- the doctors instead of waiting until it's too late and they have to go to emergency rooms. Right now it's a virtual insurance policy that says that this is what you need but you have to meet the 80/20 before you can get one thing other than your initial benefit of being able to got to the doctor, dentist, eye doctor, that sort of thing. Get back to insuring people and not just building on reserves. Please, please make sure that happens for us and that access to the Churchill County, make it reasonable and right and accessible. CHAIRMAN CATES: Four minutes. MS. BOWEN: Thank you. Four minutes, I appreciate. It was a birthday present. Bye-bye.
4.2. 4. Consent Agenda (Patrick Cates, Board Chair) (All Items for
Possible Action as specified below) Consent items will be considered together and acted on in one motion unless an item is removed to be considered separately by the Board. 4.2 Receipt of the Casey, Neilon & Associates Audited Financial
Statements of PEBP for Fiscal Year 2018.













































5. 1. Health Claim Auditors, Inc. quarterly audit of HealthSCOPE
Benefits for the timeframe July 1, 2018 – September 30, 2018: (1) Report from Health Claim Auditors; (2) HealthSCOPE Benefits response to audit report; and (3) for possible action to accept audit report findings and assess penalties, if applicable, in accordance with the performance guarantees included in the contract pursuant to the recommendation of Health Claim Auditors. (For Possible Action)


Claims and System
Audit Report for
Audit Period: PEBP Plan Year 2019, Quarter One
July, August and September 2018
Audited Vendor:
Submitted By:
Health Claim Auditors, Inc.
October 2018

TABLE OF CONTENTS
Executive Summary 1 - 4
Procedures/Capabilities/Supporting Data 5 - 25 Introduction 5
Breakout of Claims 5
Payment/Financial Accuracy 5 - 6
History of Performance Guarantee Performance 7
Claim Payment Turnaround 8
Customer Service 8 - 9
Soft Denial Claims 10
Overpayments 11 - 12
Subrogation 12 - 13
Large Utilization 13
Dedicated Team Members 14
HSB System/Policy/Procedures 15
Eligibility 15
Deductibles, Benefit Maximums 15
Unbundling/Rebundling 16
Concurrent Care 17
Code Creeping 17
Procedure, Diagnosis, Place of Service 17
Experimental/Cosmetic Procedures 17
Medical Necessity Guidelines 17
Patterns of Care 18
Mandatory Outpatient/Inpatient Procedures 19
Duplicate Claim Edits 19
Adjusted Claims 19
Hospital Discounts 19
Hospital Bills and Audits 20
Filing Limitation 20
Unprocessed Claim Procedures 20
R&C/Maximum Allowance 20
Membership Procedures 21
COBRA 22
Provider Credentialing 22
Coordination of Benefits 22
Medicare 23
Controlling Possible Fraud/Security Access 23
Quality Control/Internal Audit 23 - 24
Internet Capabilities 24
Communication, U/R and Claims Depts. 24
Claim Repricing 25
Banking and Cash Flow 25
Reporting Capabilities 25
General System 25
General Security 25 HCA Claim Audit Procedures 26
Specific Claim Audit Results 27 – 34

HCA 10/18 Page 1 St.NV.PEBP/HSB 1st Qtr PY 19
EXECUTIVE SUMMARY
Audited Random Selection Data
Total number of claims: 500
Total Charge Value of random selection: $1,032,766.55
Total Paid Value of random selection: $ 305,108.85
Performance Guaranteed Metric Results Metric Guarantee Measurement Actual Pass/Fail
Payment Accuracy > 98% of claims audited are to be paid accurately 98.8%* Pass
Financial
Accuracy
> 99% of the dollars paid for the audited
claims is to be paid accurately
98.2%*
Fail Claim Processing
Turnaround Time - 99% of all claims are to be processed within
30 days.
99.9%
Pass
Customer Service
-Telephone Response Time: < 30 seconds.
-Telephone Abandonment Rate: < 2%.
-First Call Resolution: > 95%
21 sec.
1.49%
97.85%
Pass
Pass
Pass
Data Reporting
-100% of standard reports w/in 10 bus. days
-Annual/Regulatory Documents w/in 10
business days of Plan Year end
No
Exceptions
Noted
Pass
Disclosure of
Subcontractors
-Report access of PEBP data within 30 c. days
-Removal of PEBP member PHI within 3
business days after knowledge
No
Exceptions
Noted
Pass
* Disputed claim within the Medial Performance Guarantee Statistics
The HCA calculations for Payment and Financial Accuracies contain one (1) claim that
HealthSCOPE believes should not be calculated as an error. In situations where there is
disagreement between HCA and the Administrator as to what constitutes an error, both
sides are presented in the report and final determination of error rests with the client.
Ref. No. 348 (details on page 32) contains colonoscopy services rendered for an eleven
(11) year old participant with a diagnosis of other diseases of the intestine. HealthSCOPE
paid this claim at 100% of allowable per the MPD statement that the first colonoscopy of
the plan year will be paid under the Wellness Benefit. The MPD also states on page 29,
that PEBP plan coverage for preventative care is to be in accordance with ACA and
recommendations by the USPSTF. As this is an 11 year old with a definite non routine
DX and in addition the USPSTF recommends the colonoscopy for persons age 50 and
older, we interpreted the MPD language to not include this specific situation. HCA
requests guidance for adjudication of this unusual issue from PEBP.
Please note: Determination of this claim does not affect the Pass/Fail Performance
Guarantee results for Financial Accuracy as effect on Payment Accuracy = 0.2% and
Financial Accuracy = 0.14%.

HCA 10/18 Page 2 St.NV.PEBP/HSB 1st Qtr PY 19
The following notations within the Executive Summary section are reported as issues
considered as an “outlier” of findings typically detected within the PEBP quarterly audits
which require attention and/or acknowledgement for possible action(s).
Previous Recommendation(s)
HCA is pleased to report that all previous recommendations accepted by the PEBP
Board of Directors has been implemented and/or in the process of application.
HTH Repricing as Non PPO for Excluded Services
Multiple contractual agreements utilized for discount rates, etc. and repriced by HTH
for PEBP claims contain language, in which, the provider is considered a PPO vendor,
however, displays services that they are not authorized to provide and are excluded
for payment(s) if rendered under the HTH contract.
When the excluded services are billed from the provider and sent to HealthSCOPE for
payment by the PEBP plan (as all claims within the HTH network) they are forwarded
to HTH for repricing. These services are repriced and identified as “NON PPO” by
HTH and sent back to HealthSCOPE for adjudication. HealthSCOPE then pays these
services as NON PPO, using out of network rates including Usual & Customary
reductions and applying Out-of-Network PEBP benefits versus denying payment and
paying $0.
This audit detected example claims paid within this issue, where payment exceeded
$5,300.00 to the provider, of which, HealthSCOPE has to attempt collections and the
member will receive Explanation of Benefits (EOBs) that reflect said overpayment(s).
HCA recommends that HTH provide the repricing for services rendered by a PPO
provider for excluded services be allowed at $0 or another alternative versus
identified as NON PPO.
It is also noted but not verified, that HTH contracting department may have some
excluded services within their contracts that could be covered under “blanket” Letter
of Authorizations (LOAs) that the claims repricing personnel are not provided. HCA
recommends that PEBP request HTH verify this possibility and correct if identified.
HTH authorizations for Diplomat Pharmacy
This audit was conducted for the PEBP First Quarter of Plan Year 2019, of which, is
the first quarter period for adjudication of the PEBP EPO Premier Plan claims. This
audit detected and observed numerous EPO plan claims with authorizations provided
to PEBP participants by HTH for large dollar prescription drug claims to be
purchased through Diplomat Pharmacy (a network pharmacy), however, are to be
purchased through PEBP’s Specialty Drug vendor, Accredo to receive the negotiated
PEBP rates.
HCA recommends that HTH utilize the listing of the drugs to be purchased through
Accredo that was provided by PEBP for authorization(s) of these large dollar drugs.
Since HealthSCOPE is “holding” these claims, it is recommended that PEBP provide
advice on how to handle the current claims and future claims within this issue.

HCA 10/18 Page 3 St.NV.PEBP/HSB 1st Qtr PY 19
End Stage Renal Disease
The audit conducted two quarters ago detected an issue concerning possible errors
with the payment of participant claims with diagnosis (DX) of End Stage Renal
Disease (ESRD). Last quarter’s audit included a focus audit on this subject for the
nineteen (19) participants that were identified with an ESRD DX within the PEBP
Consumer Driven Health Plan had nineteen (19). Of the 19, one (1) was found to be
Medicare eligible and requesting $95,242.67 in overpayments and one (1) was found
to be retroactively eligible by Medicare, of which HealthSCOPE is to request
$356,704.33 in overpayments.
HCA conducted a follow-up focus audit to this issue to ensure collections of these
overpayments. It was detected, at the time of this audit, over $100,000 has been
collected for these claims on behalf of PEBP.
HCA recommends that PEBP consider language within the Plan Specific Plan
Document (SPD) that addresses the enrollment of participants Medicare eligible with
an ESRD DX.
Overpayments
The quarterly audit includes a review of the causes, volume and HealthSCOPE’s
policies and procedures for identification and collection of overpayments.
This quarter, the identified overpayment dollar volume is at the highest level in the
PEBP’s history with HealthSCOPE as its medical claims administrator. Year 2018
overpayments have increased primarily as a result of the claims sent for collections
due to network pricing adjustments from both major networks within the PEBP
Statewide Network and claims paid for participants eligible with Medicare. It is
important to note, that of the most current identified overpayments for Plan Years
2018 and 2019 (to date), 65.3% of the identified overpayment volume was found to be
caused by external sources that are not a cause of the HealthSCOPE adjudication
processes.

HCA 10/18 Page 4 St.NV.PEBP/HSB 1st Qtr PY 19
Trends/Issues
The audit revealed the following issues or trends detected from the random selection and
bias selected claims. Please note: the reference numbers in bold type are claims from the
random selection and are included within the statistical calculations. Reference numbers
in normal type were identified as issues in bias claims as defined earlier and are not
included within the statistical calculations of this audit. Specific information regarding
supporting reference numbers can be found in the Audit Results Section in numerical
sequence, which begins on page 27.
Incorrect rate due to re-pricer; Supporting reference nos. 037 and 095
Incorrect rate applied; Supporting reference nos. 262 and 372
Duplicate claim paid; Supporting reference no. 169
Lab claim associated with routine service not adjusted to pay as wellness; Supporting reference no. 035
Preventive services paid as medical; Supporting reference no. 092
Medical services paid as preventive; Supporting reference no. 348
Data entry error; Supporting reference no. 069
Deductible applied in error; Supporting reference no. 170
PPO provider paid as non-PPO; Supporting reference no. 219
Incorrect copay applied; Supporting reference no. 284
The audit revealed the following issues, which appear to be administered properly by
HSB but should be brought to client attention for proper notification or verification.
Specific information regarding supporting reference numbers can be found in the Audit
Results Section in numerical sequence, which begins on page 27.
Hospital contract changed for ER services only; Ref. No. 077, 259 and 404
PPO provider with dual contracts; Supporting ref. nos. 182 and 196
PPO provider contract with excluded services; Supporting reference no. 134
Hearing aid benefit clarification; Supporting reference no. 278
Higher of two copays applied versus applying two separate copays on
Premier Plan; Supporting reference no. 346
First EKG of plan year paid at 100% regardless of diagnosis; Ref. No. 407
HSB implant policy requires invoice for implants in excess of
$10,000.00 for non-SHO hospital; Supporting reference no. 507
Claims authorized under pharmacy other than Accredo; Ref. No. Focus 1

HCA 10/18 Page 5 St.NV.PEBP/HSB 1st Qtr PY 19
CLAIM PROCEDURES/SYSTEM CAPABILITIES/SUPPORT DATA
Introduction
In October 2018, Health Claim Auditors, Inc. (HCA) performed a Claims and System
Audit of HealthSCOPE Benefits (HealthSCOPE) located in Little Rock, Arkansas on
behalf of The State of Nevada Public Employees’ Benefits Program (PEBP).
This audit was performed by collecting information to assure that HealthSCOPE is doing
an effective job of controlling claim costs while paying claims accurately within a
reasonable period of time. This report was presented to HealthSCOPE for any additional
comments and responses on 24 October 2018.
Breakdown of Claims Audited
The individual claims audited were randomly selected from PEBP’s claims listings as
supplied by HealthSCOPE. These claims had dates of service ranging from March 2017
to September 2018 and were processed by HealthSCOPE from 01 July 2018 through 30
September 2018 (PEBP’s First Quarter Plan Year 2019). These claims were stratified by
dollar volume to assure that HCA audited all types of claims. The audit also includes
large dollar paid amounts that are considered as bias* selected claims.
*Bias claims are not part of the random selection but were audited by HCA because of
some “out of the ordinary” characteristic of the claim. There are multiple criteria to
identify the “out of the ordinary” characteristics. Examples are duplicates, CPT up
coding, exceeding benefit limits, etc.
The breakdown of the 500 random selected claims audited is as follows:
Type of Service Charge Amount Paid Amount Paid Distribution No. of Claims
Medical $ 329,073.28 $ 96,997.78 31.8% 328
Outpt. Hospital $ 447,823.33 $ 89,251.84 29.3% 54
Inpt. Hospital $ 210,642.75 $ 97,813.44 32.0% 5
Dental $ 45,227.19 $ 21,045.79 6.9% 242
TOTAL $1,032,766.55 $ 305,108.85 100% 500
Payment Accuracy
Per PEBP, the Service Performance Standards and Financial Guarantees Agreement for
the payment accuracy is to be 98% or above of claims adjudicated are to be paid correctly
or a penalty of 2.5% of Quarterly Administration Fees for each percentage (%) point, or
fraction thereof, below performance guarantee is to be applied. Payment Accuracy is
calculated by dividing the total number of claims not containing payment errors in the
audit period by the number of claims audited within the random selection.

HCA 10/18 Page 6 St.NV.PEBP/HSB 1st Qtr PY 19
The Payment Accuracy Percentage of the number of claims paid correctly from the
HealthSCOPE random selection for this audited quarter is 98.8%.
Number of claims: 500
Number of claims paid incorrectly: 6
Percentage of claims paid incorrectly: 1.2%
Number of claims paid correctly: 494
Percentage of claims paid correctly: 98.8%
Payment Accuracy for the past four quarters
Financial Accuracy
Per PEBP, the Service Performance Standards and Financial Guarantees Agreement for
the financial accuracy of the total dollars paid for claims adjudicated is to be paid
correctly at 99% or above or a penalty of 2.5% of Quarterly Administration Fees for each
percentage (%) point, or fraction thereof, below performance guarantee is to be applied.
Financial Accuracy is calculated by dividing the total audited dollars paid correctly by
the total audited dollars processed within the random selection.
The Financial Accuracy Percentage of paid dollars remitted correctly on the
HealthSCOPE claims selected randomly for this audited quarter is 98.24%. This audit
reflected ninety-seven and seven tenths percent (97.7%) of the audited errors within the
valid random selection were overpayments.
Paid dollars audited $ 305,108.85
Amount of paid dollars remitted incorrectly $ 5,345.10
Percentage of Dollars paid incorrectly 1.76%
Paid Dollars of claims paid correctly $ 299,763.75
Percentage of Dollars Paid correctly 98.24%
Financial Accuracy for the past four quarters

HCA 10/18 Page 7 St.NV.PEBP/HSB 1st Qtr PY 19
Historical Statistical Data of Performance Guarantees
The following reflects the historical statistical data since the origin of PEBP medical
claims administration by HealthSCOPE. The entries designated in bold red type are
measurable categories with underperformance of the Service Performance Guarantees
Agreement.
Period Audited Payment
Accuracy
Financial
Accuracy
Turnaround
Time Telephone
Response
Telephone Abandon Rate
First Call
Resolution
1st Qtr PY 2012 95.7% 98.6% 7.6 days :17 1.43% N/A
2nd Qtr PY 2012 93.3% 97.3% 12.7 days :12 1.16% N/A
3rd Qtr PY 2012 96.8% 98.6% 3.7 days :18 1.32% N/A
4th Qtr PY 2012 95.8% 99.5% 11.4 days :14 0.93% N/A
1st Qtr PY 2013 97.2% 99.4% 10.4 days :20 1.06% N/A
2nd Qtr PY 2013 98.5% 99.3% 7.3 days :11 0.87% N/A
3rd Qtr PY 2013 98.0% 95.7% 6.4 days :25 1.98% N/A
4th Qtr PY 2013 98.4% 99.7% 6.2 days :29 1.61% N/A
1st Qtr PY 2014 98.8% 99.6% 5.4 days :14 0.84% N/A
2nd Qtr PY 2014 99.2% 99.2% 5.9 days :29 1.96% N/A
3rd Qtr PY 2014 98.0% 98.5% 5.2 days :30.5 1.92% N/A
4th Qtr PY 2014 99.0% 99.8% 4.4 days :28 1.96% N/A
1st Qtr PY 2015 98.8% 99.27% 4.9 days :29.4 1.94% N/A
2nd Qtr PY 2015 99.0% 99.35% 8.1 days :22 1.18% N/A
3rd Qtr PY 2015 98.6% 99.8% 5.9 days :29.7 1.97% N/A
4th Qtr PY 2015 99.6% 95.6% 4.9 days :29.4 1.91% N/A
1st Qtr PY 2016 99.0% 98.9% 4.8 days :29.1 1.94% N/A
2nd Qtr PY 2016 98.6% 99.7% 3.5 days :24.0 1.14% N/A
3rd Qtr PY 2016 98.8% 98.53% 5.3 days :29.0 1.96% N/A
4th Qtr PY 2016 99.0% 99.52% 6.3 days :29.5 1.98% N/A
1st Qtr PY 2017 99.0% 99.23% 6.6 days :29.8 1.93% N/A
2nd Qtr PY 2017 99.6% 99.78% 4.3 days :29.3 1.96% N/A
3rd Qtr PY 2017 98.2% 93.83% 3.7 days :29.8 1.97% N/A
4th Qtr PY 2017 99.0% 99.66% 4.6 days :29.3 1.98% N/A
1st Qtr PY 2018 99.2% 99.83% 4.4 days :26.0 1.61% 98.79%
2nd Qtr PY 2018 99.6% 99.9% 4.3 days :12.8 1.12% 98.28%
3rd Qtr PY 2018 98.6% 99.7% 3.5 days :28.5 1.97% 98.65%
4th Qtr PY 2018 99.4% 99.5% 4.2 days :21.0 1.50% 97.65%
1st Qtr PY 2019 98.8% 98.2% 5.4 days :21.0 1.49% 97.85%

HCA 10/18 Page 8 St.NV.PEBP/HSB 1st Qtr PY 19
Turnaround Time
Per the Service Performance Standards and Financial Guarantees Agreement, the
turnaround time for payments of claims is measured in calendar days from the date
HealthSCOPE receives the claim until the date of process. Ninety nine percent (99%) of
complete claims adjudicated are to be processed within thirty (30) calendar days,
excluding federal holidays, or a penalty of two percent (2.0%) of Quarterly
Administration fees for each two and a half percent (2.5%) of non-compliance complete
claims is to be applied. HCA had requested the report that reflects the measurement of
this issue. This report reflected that 99.91% of “complete” claims were processed within
30 calendar days, in compliance with the performance guarantee. This report also
displayed the total turnaround process time for all claims at 5.4 days.
Turnaround Time Measurements
The turnaround time, measured only from the random selected claims, for Medical claims
was 12.2 calendar days, Out Patient Hospital claims was 11.5 calendar days, In Patient
Hospital claims was 17.6 calendar days and Dental claims was 2.1 calendar days.
During the audit period of 01 July 2018 to 30 September 2018, HealthSCOPE had
received 1,684 PEBP e-mail inquiries for information via the internet. The average
turnaround time for these inquiries was calculated at approximately 7.6 hours.
Customer Service Satisfaction
Per the Service Performance Standards and Financial Guarantees Agreement, the
telephone response time reflects all calls must be answered within thirty (30) seconds or a
penalty of one percent (1%) of Quarterly Administration fees for each second in non-
compliance is to be applied. HCA has reviewed the appropriate report for the PEBP first
fiscal quarter Plan Year 2019, which revealed the average incoming answer speed to be
21.0 seconds (0:21.0). The telephone response time was 31 seconds for July 2018, 12
seconds for August 2018 and 21 seconds for September 2018.
Telephone Response Time (average)

HCA 10/18 Page 9 St.NV.PEBP/HSB 1st Qtr PY 19
Per the Service Performance Standards and Financial Guarantees Agreement, the
abandonment rate must be under two percent (2%) of total calls or a penalty of one
percent (1%) of Quarterly Administration fees for each percentage point or fraction
thereof in non-compliance is to be applied. Please note: this performance measurement
was changed from 3% as the measured benchmark for previous plan years. HCA has
reviewed the appropriate report for the PEBP first fiscal quarter Plan Year 2019, which
revealed the abandoned calls ratio to be 1.49%. The telephone abandonment rate was
2.01% for July 2018, 0.93% for August 2018 and 1.53% for September 2018.
Telephone Abandonment Rate
Per the Service Performance Standards and Financial Guarantees Agreement, ninety five
percent (95%) of incoming PEBP member problems must be resolved to conclusion on
the first call or a penalty of one percent (1%) of Quarterly Administration fees for non-
compliance is to be applied. HCA has reviewed the appropriate report for the PEBP first
fiscal quarter Plan Year 2019, which revealed that HealthSCOPE documented 97.85% of
incoming calls were brought to completion on the first call.
Incoming Calls Concluded with First Call
HealthSCOPE has eighty plus (80+) Customer Service Reps (CSRs), of which, the
majority are in the Little Rock office with an average of eight (8) years experience.
Health SCOPE currently has eighteen (18) CSRs dedicated to the PEBP plan.
HealthSCOPE stated that customer service hours of operation will be applied to PEBP
direction for proper service levels.
Benefit data is supplied by electronic documentation so that the analyst may explain
benefit information to clients, members and providers by HealthSCOPE.
HealthSCOPE stated that the customer service representatives will not have the ability to
make system changes.
HealthSCOPE’s telephone conversations are documented for future reference.
HealthSCOPE does have an audit process for Customer Service Representatives.
HealthSCOPE is able to monitor trends/errors found through Customer Service.
HealthSCOPE can conduct customer service satisfaction surveys to determine employee
satisfaction of claims administration and service upon client request.

HCA 10/18 Page 10 St.NV.PEBP/HSB 1st Qtr PY 19
Soft Denied Claims
The audit identifies the volume of claims adjudicated and placed in a “soft denied” status.
HCA recognizes and respects the need to place certain claims in a soft denied status such
as claims that require additional information or special calculation of payment. It is
HCA’s opinion that these amounts are the result of HealthSCOPE conducting due
diligence and resolution of the issues and trends including those previously detected in
previous audits. It is important to include this data within this report to disclose the
outstanding unpaid claims that could create an artificial debit/savings during the time that
these claims were adjudicated. Note: The measurement of this data was provided as a
“snapshot” report. The report reflected the “soft edit” amounts as they were reported on
the specific day that the report was recorded. The report for the current claims placed in a
“soft denied” status reflect a total of 4,624 claims representing $ 24,992,938.88.
Audit Period Total Number of Claims Charge Amount Value of Soft Edits
1st Qtr PY 2012 2,607 $ 7,544,177.55
2nd Qtr PY 2012 4,068 $10,697,954.53
3rd Qtr PY 2012 1,536 $ 6,472,249.56
4th Qtr PY 2012 559 $ 2,205,318.16
1st Qtr PY 2013 1,053 $ 3,413,738.12
2nd Qtr PY 2013 1,107 $ 5,019,961.70
3rd Qtr PY 2013 1,023 $ 4,179,542.34
4th Qtr PY 2013 1,094 $ 3,049,481.74
1st Qtr PY 2014 1,389 $ 3,853,629.07
2nd Qtr PY 2014 1,157 $ 2,510,539.33
3rd Qtr PY 2014 1,621 $ 7,873,432.21
4th Qtr PY 2014 1.487 $ 4,665,197.77
1st Qtr PY 2015 1,404 $ 5,901,903.17
2nd Qtr PY 2015 1,668 $ 6,930,288.41
3rd Qtr PY 2015 2,897 $10,800,874.08
4th Qtr PY 2015 2,498 $10,685,255.24
1st Qtr PY 2016 3,071 $13,027,717.82
2nd Qtr PY 2016 2,543 $13,547,682.34
3rd Qtr PY 2016 2,871 $10,360,017.78
4th Qtr PY 2016 3,107 $15,262,995.27
1st Qtr PY 2017 2,580 $ 8,558,641.28
2nd Qtr PY 2017 3,876 $15,960,661.94
3rd Qtr PY 2017 3,696 $18,864,824.74
4th Qtr PY 2017 4,768 $20,217,736.28
1st Qtr PY 2018 3,926 $15,683,180.63
2nd Qtr PY 2018 4,073 $20,576,701.38
3rd Qtr PY 2018 4,144 $17,375,843.66
4th Qtr PY 2018 4,544 $21,591,987.11
1st Qtr PY 2019 4,624 $24,992,938.88

HCA 10/18 Page 11 St.NV.PEBP/HSB 1st Qtr PY 19
Overpayments
The previous PEBP health plan administrator (UMR) provided HealthSCOPE with
a report displaying the outstanding identified overpayments reflecting a grand total
of outstanding overpayments at $1,751,949.42. HealthSCOPE conducted much research
on these overpayments and found that 507 of these claims were deemed as no longer
valid due to providers showing items that were already paid to UMR, corrected claims
were sent to resolve the issue, etc.
HCA requested an overpayment report that reflects the identified current outstanding
overpayments incurred since the beginning of the contract period with HealthSCOPE.
This report reflected a current total of 4,482 (a decrease of 10 from the previous
report) overpayments with a potential recovery value of $2,904,144.54 (an increase of
$424,430.63) for HealthSCOPE. Detailed information regarding outstanding
overpayments can be reviewed in a separate Supplemental Report, which for
confidentiality purposes is not included in this report but is made available to PEBP staff
should they request it.
HSB’s policy is to keep all identified overpayments active for potential recoupment(s
The breakout of overpayments identified by the year paid are as follows:
Period # of Claims Due/Potential Recovery
- Fiscal Year 2012 384 $ 139,311.92*
- Fiscal Year 2013 789 $ 253,318.28*
- Fiscal Year 2014 482 $ 126,711.91*
- Fiscal Year 2015 433 $ 262,834.74*
- Fiscal Year 2016 716 $ 333,037.00*
- Fiscal Year 2017 813 $ 329,450.14
- Fiscal Year 2018 1,161 $1,019,681.74
- Fiscal Year 2019 436 $ 439,798.81
TOTAL 4,482 $2,904,144.54
* Special Note: The amounts reported for the aged overpayments in previous years
(two years +) have increased from the volume(s) reported in the previous audits.

HCA 10/18 Page 12 St.NV.PEBP/HSB 1st Qtr PY 19
Of the 1,597 most current (Plan Years 2018 + 2019) identified outstanding overpayments
(HSB only), 65.3% were found to be caused by external sources that are not a cause of
the HealthSCOPE adjudication processes. Breakout of the HealthSCOPE’s most
current (PY18 + PY19) overpayments (by claim count) are listed by reason as follows:
18.89% Provider caused, rebilled, charges billed in error, corrected EOB
15.48% No COB on file
14.15% Incorrect Benefit Applied
12.13% SHO Pricing Correction
10.23% Corrected HTH Network Pricing
9.73% Incorrect Rate Applied
5.94% Retro termination
5.62% Service not covered
2.59% COB incorrectly calculated or not applied
1.14% Eligibility
0.76% Duplicate
0.44% Industrial and/or possible Workers Compensation claim
0.44% Paid PPO provider as NON PPO
0.38% Adjusted after medical review
0.38% Pharmacy claim deductible/Co-Insurance error
0.32% Processed under the incorrect provider
0.32% Incorrect assignment applied
0.25% Processed under incorrect patient
0.19% First Health Pricing Adjustment
0.13% Subrogation error
0.13% Pre-Certification
0.06% Timely Filing
0.06% Paid NON PPO as PPO
0.06% Paid Asst. Surgeon as Surgeon
0.06% Change in Benefits
0.06% Entry Error
0.06% Stop Payment
Subrogation
HCA requested a subrogation report that can be reviewed in a separate Supplemental
Report, which for confidentiality purposes is not included in this report. It is made
available to PEBP staff should they request it.
This report reflects open subrogation claims representing a current potential recovery
amount of $4,367,780.85; an increase of $287,915.65 from the previous quarter.

HCA 10/18 Page 13 St.NV.PEBP/HSB 1st Qtr PY 19
Reports received from HealthSCOPE reflect that subrogation recoveries for the audited
period was $311,881.16. After contingency fees were paid, PEBP received $233,910.
HealthSCOPE system will apply a pursue and pay subrogation policy as directed by
PEBP. Per HealthSCOPE, subrogation is determined and pursued on all claims where the
total amount paid equals to or exceeds $1000 (one thousand).
HealthSCOPE does identify possible subrogation cases internally. HealthSCOPE utilizes
a third party vendor for recovery of monies. Vendors are paid a contingency of which the
administrator receives a portion of and disclosed within RFP 1983 for Third Party Claims
Administration.
HealthSCOPE does not conduct auditing of outstanding subrogation cases sent to
their vendors, but sends any cases not picked up by the main vendor to another
vendor for review.
HealthSCOPE depends on the external vendors to conduct the appropriate International
Classification of Diseases (ICD) sweep checks for subrogation detections. HealthSCOPE
is currently utilizing the new ICD-10 conversions and the coding has been completed
within their system.
Per HealthSCOPE, claims related to Worker’s Compensation are denied.
Recoupment and payments for subrogation claims are assigned as directed by PEBP.
High Dollar Claimants
Per the request of PEBP staff, HCA has requested a report to identify the number
of active, retiree or COBRA elected participants or dependents who have
obtained a plan paid level of $750,000.00 or greater.
This report reflected thirty-five (35) members and twenty-one (21) dependents for a total
of 56 active participants, who have obtained this level of plan payment participation
representing an accrued dollar paid amount of $78,497,922.00.

HCA 10/18 Page 14 St.NV.PEBP/HSB 1st Qtr PY 19
Personnel
The audit included a review of the HealthSCOPE personnel dedicated or assigned to
PEBP. The current Organization Chart for individuals assigned to the PEBP plan, is, with
changes, as follows:
State of Nevada Manager;
Vice President – Quality Assurance;
Sr. Vice President Operations Customer Care;
Executive Account Manager;
Client Relations Manager;
Financial Operations Director;
Provider Maintenance Specialist;
Financial Analysts, 3 individuals;
Funding Supervisor;
Claims Administration Manager; CHANGED
Claims Administration Supervisors; 2 individuals;
Claims Analysts, CHANGE, 3 individuals deleted and 3 individuals added for a total
of 12 individuals;
Eligibility Director;
Eligibility Supervisor;
Customer Service Vice President;
Customer Service Director;
Customer Service Representatives, CHANGE, 2 individuals deleted and 2 individuals
added for a total of 18 individuals;
Scanning Services Manager;
Recoveries Manager;
Recoveries Specialists, 2 individuals;
Vice President Data Services;
Senior Data Analyst;
Chief Information Officer;
Data Architect
Computer Domain Hosting (CDH) Services Manager;
Sr. Vice President-Legal and Compliance;
COBRA Service Manager;
Customer Care Supervisor;
Customer Care Representatives, total of 3 individuals, CHANGE, 1 individual
deleted and 1 added.

HCA 10/18 Page 15 St.NV.PEBP/HSB 1st Qtr PY 19
HealthSCOPE POLICY/PROCEDURES/SYSTEM CAPABILITIES
The following section displays HealthSCOPE policies, procedures and system
capabilities as they pertain to adjudication of PEBP claims. Due that system edit and
functions do not change frequently, the following section appears only in the first quarter
audit each Plan Year.
Eligibility
The HealthSCOPE system systematically denies claims for services rendered prior to or
after the effective date.
The HealthSCOPE system systematically adjudicates claims pertinent to the date of
service for those claims received prior to or after any benefit changes.
The HealthSCOPE system has the capability to load by line of coverage tiers (i.e.: single
medical/family dental, etc.).
HealthSCOPE can, if requested, request divorce decrees or court orders for those
dependents of divorced or separated parents.
The HealthSCOPE system will enforce IRS regulations if the Plan Document does not
require stricter requirements.
Disabled (handicapped) dependent status is determined by PEBP when a covered
dependent child has reached the age of 26, which would terminate his/her status as a
dependent. HealthSCOPE can determine disabled dependent status with internal medical
personnel if required.
HealthSCOPE has stated that they would not ever add a member dependent without
PEBP authorization.
HealthSCOPE stated that the turnaround time to add or delete a member’s eligibility is
within 24 hours of receipt.
If a member is terminated retroactively, HealthSCOPE will review that member’s claim
history to determine any overpayments for possible recoveries and proceed per PEBP
instructions.
Deductibles, Out-of-Pocket and Benefit Maximums
The HealthSCOPE system is capable of separate PPO and Non PPO accumulators.
All deductibles, out-of-pocket expenses and most benefit maximums are tracked by the
HealthSCOPE system.
The HealthSCOPE system contains automated carry over deductible features if
necessary.

HCA 10/18 Page 16 St.NV.PEBP/HSB 1st Qtr PY 19
HealthSCOPE system contains integrated deductibles for dental and medical claims.
HealthSCOPE does have experience of applying the Prescription Drug and Medical
claims deductibles as reflected within the PEBP SPD.
Unbundling/Rebundling
The HealthSCOPE system can systematically edit to identify laboratory, diagnostic and
radiology charges that have been unbundled and billed separately.
The HealthSCOPE system has the electronic capacity to match multiple claims in history
for application of the unbundling edit.
The HealthSCOPE system systematically soft edits for multiple surgical guidelines, for
those situations where a surgeon is billing for more than one (1) surgical procedure
during the same operative session. The HealthSCOPE system has the capacity to match
claims in history for application of the multiple procedure reduction edit.
For Network providers and Non-PPO providers where multiple surgical procedures have
been performed, the HealthSCOPE system will electronically adjudicate and apply 100%
of the Reasonable and Customary (R&C) or the provider specific fee schedule amount for
the major procedure, 50% of the R&C or network fee schedule amount for subsequent
procedures or any deviation designed by the network contract. This application is
conducted manually with HealthSCOPE. The system can calculate the claim by global or
individual allowance accounting.
For Network providers and Non-PPO providers where bilateral surgical procedures have
been performed, the HealthSCOPE system will not electronically adjudicate to allow
100% of the Reasonable and Customary (R&C) or the provider specific fee schedule
amount for the major procedure and 50% of the R&C or network fee schedule amount for
the secondary procedure. This application is manually applied.
HealthSCOPE manually breaks this issue into separate line services for adjudication.
The HealthSCOPE system is automated to identify pre/post operative care related to
surgical procedures.
The HealthSCOPE system denies incidental procedures when in relation to primary
procedures.
The HealthSCOPE system systematically identifies claims that contain a same day
procedure (procedures that are not customarily billed on the same day as a surgical
procedure) unless billed under the same provider.
HealthSCOPE will allow the doctor to bill the initial obstetrical diagnostic office visit.
The subsequent visits are paid and then manually tracked and applied to the global
obstetrical fee. Reasonable and Customary (R&C) allowance or network fee schedule
amount is applied to the global obstetrical fee. Obstetrical lab and diagnostic procedures
are allowed to be billed separately.

HCA 10/18 Page 17 St.NV.PEBP/HSB 1st Qtr PY 19
Concurrent Care
The HealthSCOPE system is not automated to identify situations where more than one
(1) physician is billing for services during the same time period for the same diagnosis.
The claims analysts rely on the system’s possible duplicate edit to detect this situation.
Code Creeping
The HealthSCOPE system is automated to identify code creeping. An example of this
occurs when a physician is consistently billing for an initial or new patient office/hospital
visit when services performed are actually rendered for a subsequent or established
patient visit.
Procedure, Diagnosis and Place of Service
The HealthSCOPE system is automated to determine the correct usage of the Current
Procedural Terminology (CPT) code. The system is automated to edit if the patient’s age
or gender does not concur with the (CPT) code.
The HealthSCOPE system edits if multiple CPT codes that are billed on the same claim
don’t belong together.
The HealthSCOPE system is automated to identify if the place of service does not concur
with the (CPT) code.
The HealthSCOPE system is also automated to edit if a diagnosis does not concur with
the (CPT) code.
The HealthSCOPE system has the capability to edit for routine/medical diagnosis’ to
determine which benefits are allowable under routine versus medical.
Experimental and Cosmetic Procedures
The HealthSCOPE system is automated to assist processors in identifying those
procedures that are or could be cosmetic. Analysts are also trained to identify these
claims. These procedures can also be identified during the pre-certification process.
The HealthSCOPE system can be programmed to systematic hold or deny these types of
claims, depending upon plan election.
Medical Necessity/Potential Abuse Guidelines and Procedures
The HealthSCOPE system is automated to determine the appropriateness of an assistant
surgeon based on the surgery performed. These claims can be pended or denied,
depending upon the plan election.

HCA 10/18 Page 18 St.NV.PEBP/HSB 1st Qtr PY 19
The HealthSCOPE system is automated to determine the appropriateness of an
anesthesiologist based on the service performed. These claims can be held or denied,
depending upon the plan election.
The HealthSCOPE system is not automated to determine if anesthesia is billed by both
the hospital and anesthesiologist under both a revenue code and separate CPT service
code.
HealthSCOPE determines medical necessity for the rental or purchase of durable medical
equipment (DME) by prescription from a physician or internal Medical Reviewers.
Rental cost of DME is tracked up to the purchase price by HealthSCOPE to assure that
PEBP will pay no more for rental than it would if this equipment had been purchased.
HealthSCOPE tracks this issue on a manual basis within their system.
HealthSCOPE investigates to determine if a prescription is a federal legend drug. They
utilize the Medi-Span database for this procedure.
Claims involving chiropractic care, physical therapy are determined for medical necessity
by HealthSCOPE. Therapeutic treatment needs to be rendered by a licensed physical
therapist. Treatment must be commonly and customarily recognized as appropriate within
the doctor’s profession.
Per HealthSCOPE, medical necessity for infusion services are usually determined by
Utilization Review but can be determined internally if necessary.
The HealthSCOPE system can comply with authorization, repricing and all requirements
as they pertain to adjudication of Mental Health claims.
HealthSCOPE does execute on a regular basis, daily exception reports, which are run for
supervisors to review edits that are overridden.
The HealthSCOPE system has the capability to identify repeat tests being done by both
primary physicians and specialists.
Patterns of Care and Treatment for Physicians
HealthSCOPE has the capability to conduct evaluations of patterns of care of physicians
on patient outcome studies (success) for various procedures and communicate facts to
physicians to eliminate unnecessary or ineffective care or disclose potential fraud or
trends of fraud.

HCA 10/18 Page 19 St.NV.PEBP/HSB 1st Qtr PY 19
Mandatory Outpatient/Inpatient Procedures
The HealthSCOPE system is not automated to determine those procedures that do not
require hospitalization. Pre-certification is required for an inpatient stay and many
surgical procedures, of which, most procedures will be identified at that time.
Duplicate Claim Edits
The HealthSCOPE system is automated to identify duplicate claims. The HealthSCOPE
system will “soft” edit a claim under partial match and a “hard” edit under exact match
circumstances. The following criteria are matches: Date of Service, CPT including
modifier and Provider tax identification number.
In the event of multiple provider submissions, the PEBP member will receive an
Explanation of Benefits (EOB) for all claims paid.
Adjusted Claims
In the event that a claim was previously paid and an adjustment is made to the original
adjudication, the HealthSCOPE system will assign a “claim identification number” to the
adjustment that reflects the original paid claim. HealthSCOPE links the original with the
adjusted claim(s) with a notation on subsequent claim screens.
Hospital and Other Discounts
HealthSCOPE can automate all PPO Provider discounts including per diem and
Diagnosis Related Group (DRG) arrangements.
HealthSCOPE stated that PPO (Preferred Provider Organization) provider rates which
can be obtained can be repriced in-house.
If a network has negotiated a prompt payment discount, the HealthSCOPE system is
programmed to apply the discount.
Attempts to negotiate non-PPO provider discounts are conducted by HealthSCOPE’s
vendors, with contingencies as reported within the response to RFP 1893. PEBP can set
this issue at as low as $0 for HealthSCOPE.
HealthSCOPE declared that they do not collect any year end settlements, rebates, etc.
other than those declared within their response(s) to RFP 1893.
HealthSCOPE stated that they would review and disclose any provider discount contracts
relative to PEBP claims for the absence of any “Hold Harmless” language as an aid in
protecting PEBP members.

HCA 10/18 Page 20 St.NV.PEBP/HSB 1st Qtr PY 19
Hospital Bills (UB-92) and Audits
HealthSCOPE requires itemized hospital bills to determine non-covered items.
Itemization for all hospital bills over $10,000.00 is required by HealthSCOPE to
determine non-covered items.
The HealthSCOPE system utilizes revenue codes when processing hospital bills.
HealthSCOPE has an internal hospital audit program in place. All non-PPO claims over
$50,000.00 are sent for audit. HealthSCOPE also stated that some claims are audited
through their external audit process. HealthSCOPE is willing to accept any amount PEBP
determines as a minimum for this issue. Contingency fees and administrator percentage
shares are disclosed within their responses to RFP 1983.
Filing Limitations
The HealthSCOPE system can systematically apply the appropriate standard filing
limitation for submitting all claims. The standard filing limitation for submitting claims
for PEBP is twelve (12) months after date of service.
Unprocessed Claims Procedures
Unprocessed claims are logged on the HealthSCOPE system for verification of receipt.
HealthSCOPE has paper claims scanned and entered into their adjudication system within
twenty four (24) hours of receipt.
HealthSCOPE stated that this process and data entry will be conducted by individuals
within the continental United States. HealthSCOPE stated that they do utilize a company
that conducts this process outside the United Sates, however, has ensured that PEBP data
stays on shore.
Reasonable/Customary and Maximum Allowances
HealthSCOPE is utilizing R&C allowances for non-network providers. HealthSCOPE is
utilizing R&C data for medical claims at the seventieth (70th) percentile. Out of Network
dental providers are paid using the same allowables as in-network dental providers,
subject to the appropriate geographic location rates.
R&C is applied utilizing the date of service and geographical location (zip code). R&C
data is updated four times per year by HealthSCOPE, last updated in August 2018.
HealthSCOPE does not have separate R&C schedules for Facilities versus Professional
services, however, HealthSCOPE uses a vendor that can apply reductions for Non PPO
facilities.

HCA 10/18 Page 21 St.NV.PEBP/HSB 1st Qtr PY 19
HealthSCOPE will pay medical claims at the appropriate network negotiated rates. Non
network providers and non- negotiated services will be paid at the lesser of the MDR rate
at the percentile chosen by the PEBP plan or the billed amount. Dental claims will be
paid at the lesser of the MDR rate at the percentile chosen by the PEBP plan or the billed
amount.
The HealthSCOPE system will pay the lower of charges or scheduled amount when
contracts allow.
The HealthSCOPE system utilizes modifiers to determine R&C for professional and
technical components for diagnostic, laboratory and radiological procedures.
Assistant surgical charges, when performed by MDs will be systematically calculated at
no more than 20% of the R&C amount (or the network fee schedule) allowable for the
surgeon’s procedure performed.
HealthSCOPE will pay all related charges of an inpatient stay at the network level if a
network hospital is utilized if the benefit plan dictates. This will be performed on a
manual basis by HealthSCOPE.
HealthSCOPE is utilizing a form of R&C for Non-PPO Durable Medical Equipment
(DME) claims when applicable.
In situations where the PEBP member has claims adjudicated under the PEBP Preferred
Provider Organization (PPO) Exception Rule (50 mile rule), HealthSCOPE will identify
these exceptions at the time of adjudication and pay within the Exception Rule per the
PEBP Master Plan Document.
Membership Procedures
HealthSCOPE has the capabilities of electronic enrollment and re-enrollments.
HealthSCOPE will add or cancel employee information onto their system within twenty
four (24) hours.
Per HealthSCOPE, claims received for newborns can be paid and history tracked under
their own name.
The HealthSCOPE system analysts have inquiry capability to view eligibility files only.
They do not have the capability to make changes to eligibility information.
If an employee is terminated, the HealthSCOPE system will deny claims as not covered.
An explanation of benefits is generated every time a claim is received after this date.
HealthSCOPE will check for claims paid after this termination date.
Current historical eligibility information is stored on the HealthSCOPE system
indefinitely.

HCA 10/18 Page 22 St.NV.PEBP/HSB 1st Qtr PY 19
COBRA Administration
COBRA administration is being done by PEBP. If elected, determination for benefits
elected by individuals under COBRA administration rules can be done by HealthSCOPE.
The HealthSCOPE system can maintain an eligibility date that coincides with the
premium “paid to” COBRA date. If the system detects an exception to the date, it forces
human intervention. If the member is found to be terminated from COBRA, the claim is
denied. The HealthSCOPE COBRA system is integrated with the claims administration
system.
Provider Credentialing
Currently, providers are monitored by the PPO for credentialing. Claims received by
providers not in the PPO network are verified as legitimate by HealthSCOPE.
HealthSCOPE will check legitimacy of the provider through the internet and alternate
resources before payments are released.
Coordination of Benefits
Coordination of Benefits (COB) information is obtained via enrollment applications and
claims displaying positive COB by HealthSCOPE.
HealthSCOPE states that all claims are investigated for COB information.
HealthSCOPE’s procedure for COB is to pursue then pay for all possible COB claims.
Claims are denied until requested information is received. If a claim form displays that a
spouse is employed, HealthSCOPE will send a COB questionnaire.
The HealthSCOPE system utilizes COB indicators, which will cause a warning edit to
alert the processor to the presence of other insurance.
The HealthSCOPE system utilizes separate COB indicators for different lines of business,
i.e. medical, dental, etc.
The HealthSCOPE system has electronic split indicators to assure the proper payment of
claims received out of sequence and multiple positive COB periods.
Per HealthSCOPE, COB processing is performed by all claim processors.
The HealthSCOPE system can process claims utilizing a COB Credit Reserve program
on a calendar year basis if required.
HealthSCOPE will utilize the primary carrier’s discount when the discount is greater than
the client’s if by Plan design.
HealthSCOPE policies are to recover overpayments of past paid claims when COB is
discovered after the fact.

HCA 10/18 Page 23 St.NV.PEBP/HSB 1st Qtr PY 19
Medicare
The HealthSCOPE system will alert the Processor when a member or dependent may be
eligible for Medicare benefits. If an individual is age sixty-five (65) or older and
Medicare may exist, active employment may be verified.
HealthSCOPE can present a report specific to active participants for verification to
eligibility files when requested.
Controlling Possible Fraudulent Claims and Security Access
HealthSCOPE claims analysts have a payment authority of $10,000.00. HealthSCOPE
Team Lead has an authority of $35,000.00 and the HealthSCOPE Claims Manager has an
authority of $75,000.00. HealthSCOPE directors review claim payments in excess of
$75,000.00.
Security logs are created and monitored by HealthSCOPE. HealthSCOPE system utilizes
passwords, is monitored to restrict the use of certain system operations and can lockout
unauthorized users.
The HealthSCOPE system can track activity by individuals to identify who handled a
claim.
HealthSCOPE does currently offer website access to be used by clients for eligibility
purposes.
Quality Control and Internal Audit
HealthSCOPE has a total of 125+ claim analysts in their Little Rock location.
HealthSCOPE has 12 claims analysts dedicated to the PEBP account.
HealthSCOPE Claims Managers and Directors were found to be knowledgeable and
possess extensive training. Discussions and tests of their working knowledge of
adjudication processes and policies and procedures were positive. They were found to
possess the ability to identify and defeat many adjudication potential “problem areas”
defined with billing practices within the nation.
HealthSCOPE does not have internal audit personnel. They utilize an outside vendor that
conducts a review of no less than 2% of their claims.
HealthSCOPE has formal training programs, where policies and procedures are taught.
HealthSCOPE stated their training lasts four (4) weeks from the start. HealthSCOPE
offers consistent ongoing training and identifies needs of specific individual training. Any
needs are identified and supplied on an ongoing basis.
HealthSCOPE conducts audits on all processors. HealthSCOPE audits new analysts at
100% during their probationary period.
HealthSCOPE stated that experienced claim analysts will have the PEBP
performance guarantee levels met for claims per person per month audited.

HCA 10/18 Page 24 St.NV.PEBP/HSB 1st Qtr PY 19
Records for all analysts are kept on a database for performance reference by
HealthSCOPE.
HealthSCOPE has internal accuracy and production standards. HealthSCOPE’s internal
financial accuracy standard is 99.2% of paid claims and payment accuracy is 98%.
The production standard for HealthSCOPE experienced claims analysts is 150 - 175
medical/dental claims per day.
Internet Capabilities
HealthSCOPE does have internet capabilities to further extend membership and
administrative service levels.
HealthSCOPE has internet sites provided for member information. These sites provide
claim information, network provider identification and contact data.
HealthSCOPE internet sites were user friendly and easy to access. HealthSCOPE’s site
was checked for security processes of data protection and was found to be protected by
member supplied passwords, etc.
HealthSCOPE has an internet site available for vendor information. These sites provide
claim and benefit information, network rates and contact data.
Communication between Utilization Review (UR) and Claims Department
HealthSCOPE can currently accept communication between the UR and the claims
department via electronic source. Information received regarding pre-certification, PCP
references and Case Management can be entered on the system when received.
Precertification penalties for non-compliance will be manually applied by HealthSCOPE.
HealthSCOPE will apply the proper cutbacks to UR authorized number of service days if
different than the number of billing days on a manual basis. HealthSCOPE verified that
they will apply authorized number of service days according to PEBP’s methodology.
HealthSCOPE analysts are trained to identify potential catastrophic cases and refer them
to a Case Management program.
The HealthSCOPE system has the ability to communicate special instructions or
negotiate arrangements/ discounts to the analysts through the notes.
PEBP’s policy allows for a three (3) Level Appeal process. HealthSCOPE stated that they
can apply this policy.

HCA 10/18 Page 25 St.NV.PEBP/HSB 1st Qtr PY 19
Claim Repricing Capabilities
HealthSCOPE is currently receiving network fee schedules and provider maintenance
data electronically for internal claims repricing. HealthSCOPE has data loaded into their
adjudication system within 24 hours of receiving.
HealthSCOPE currently is participating with multiple networks for repricing via the
Electronic Data Interface (EDI) methodology.
Banking and Cash Flow
HealthSCOPE stated that they can accommodate PEBP’s requirement for payment
release frequency. HealthSCOPE stated that they could release payment checks the same
date of final adjudication if before 10:00 AM.
HealthSCOPE is utilizing bulk checks for provider payments.
Reporting Capabilities
In addition to the standard AD HOC reporting, HealthSCOPE has the capability to
develop and produce client-requested reports based on any information captured on the
system.
HealthSCOPE stated that no additional charge would be applied for any requested report
which is in the standard reporting.
General System
HealthSCOPE has been using the current system for twenty plus (20+) years. The current
system has undergone many updates since its inception.
HealthSCOPE has the controls in place for the application of source coding enabling
them to make client specific adjustments as necessary.
HealthSCOPE has written procedures in place for a formal Disaster Recovery program.
HealthSCOPE conducts daily system data backups, which are stored in a secure location
off site.
HealthSCOPE stated that they have not experienced any significant downtime.
Security
This audit reviewed building security, the handling and security of sensitive documents
and materials and the proper disposal of data for any potential data breaches. The audit
also reviewed internal processes and potential exposure to possible fraudulent activity.
The HealthSCOPE office located in Little Rock, Arkansas was found to be secure. All
external ingress and egress locations were secured and locked. Entrance was made
available to HealthSCOPE personnel by electronic pass keys. HCA entry beyond the
reception area required assistance from official personnel. The facility work areas are
monitored and recorded twenty four hours per day.

HCA 10/18 Page 26 St.NV.PEBP/HSB 1st Qtr PY 19
Sensitive data, specifically, member Personnel Health Information (PHI) of
HealthSCOPE’s clients was reviewed for security exposure practices. Any paper was
found to be in secured areas and/or file cabinets when not in use.
Per Agreement, HealthSCOPE must provide all subcontractors that have access to PEBP
member Personal Health Information (PHI) within 30 calendar days of said access or a
penalty of 5.0% of rolling 12 months of administration fees will be applied for each
violation.
Per Agreement, HealthSCOPE must remove PEBP member PHI from
unauthorized/designated servers within 3 business days after they know or should have
known using commercial reasonable efforts or a penalty of 5.0% of rolling 3 months of
administration fees will be applied.
A review of the system server equipment for HealthSCOPE noted it was secured in a
separate area under locked environments with appropriate fire suppression protections.
Every attempt to access the adjudication system required appropriate security measures
such as passcodes, etc.
HCA CLAIM AUDIT PROCEDURES
HCA selects a valid random sampling of claims from the client's current detailed claims
listings. The third party administrator is advised of the audit and requested to provide
either limited system access or paper reproduction of the entire file associated with each
random claim.
Each random claim and file is reviewed comparing eligibility and benefits to information
provided by the client. Third party administrator personnel are questioned regarding any
discrepancies. Entire files are reviewed to assure the client that deductibles, out-of-
pockets benefit maximums and related claims are processed correctly. This allows HCA
to verify all details of the client's benefit plan.
Audit statistics involve only those claims chosen in the random selection. If a randomly
selected claim HealthSCOPE been recalculated or corrected prior to the release of the
random selection for the audit, an error was not charged for the original miscalculation.
HCA will, at its opinion, comment on any claim in the random claim history to illustrate
situations it feels the client should be aware of or specific areas requiring definition.
A payment error is charged when an error identified in claim processing results in an
under/ overpayment or a check being paid to the wrong party. Assignment errors are
considered payment errors since the plan could be liable for payment to the correct party.
In situations where there is disagreement between HCA and the third party administrator
as to what constitutes an error, both sides are presented in the report. Final determination
of error rests with the client.

HCA 10/18 Page 27 St.NV.PEBP/HSB 1st Qtr PY 19
AUDIT RESULTS Listed below are the errors or issues of discussion found by this audit while processing
the claims for PEBP.
Ref. No. 035 Medical HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
Claim originally paid 1/9/18 all going to deductible
Audited is adjusted on 7/2/18 – per trans msg “wellness labs”
Claims xxxxxx for 261.25 and xxxxxx for 343.39 also have same DX
as audited. Should these 2 claims have also been adjusted?
HSB response: Agree – xxxxxx & xxxxxx should have also been corrected
to allow as wellness.
Ref. No. 037 Medical HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
Originally claim paid 4/11/18 – 00300 chg 1400 allow 760 x 80% = 608
Audited is adjusted on 7/2/18 – HTH allow now 780 – additional $20 paid
(OOP now met)
Appears HTH repricing changed?
HSB response: Yes. Corrected pricing received from HTH and claim
adjusted. No error.
Ref. No. 069 Dental HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
Claim paid originally on 5/24/18 on claim #xxxxxx w/ADA code D7953
charge 440.00 coded as D9999
Audited is adjusted paid on 7/6/18 to use correct code of D7953 and pay
additional (maxing out cal yr max)
Why was this service originally coded incorrectly?
HSB response: Due to a data entry error D7953 was entered and paid
under D9999 originally. Claim was corrected from internal audit.
Ref. No. 077 Outpatient Hospital HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
Contract displays effective 1/1/18 a 66% discount rate is to be applied for
ER services.
Claim pd as: allow/pd 4,889.85 on 7/15/18
$13,971.00 x 35% = $4,750.14. Claim was allowed at 65% versus 66%
Shouldn’t allowable be 4,750.014 versus 4,889.85?
HSB response: See attached email where we asked about this on 10-1-18
and were told rates did not change. Two different rates. We followed up
again on 10-12-18 for more clarification. Email response 10-16-18
confirmed final clarification. We will run reports to identify any claims
with pricing issues as soon as new ACT’s received.
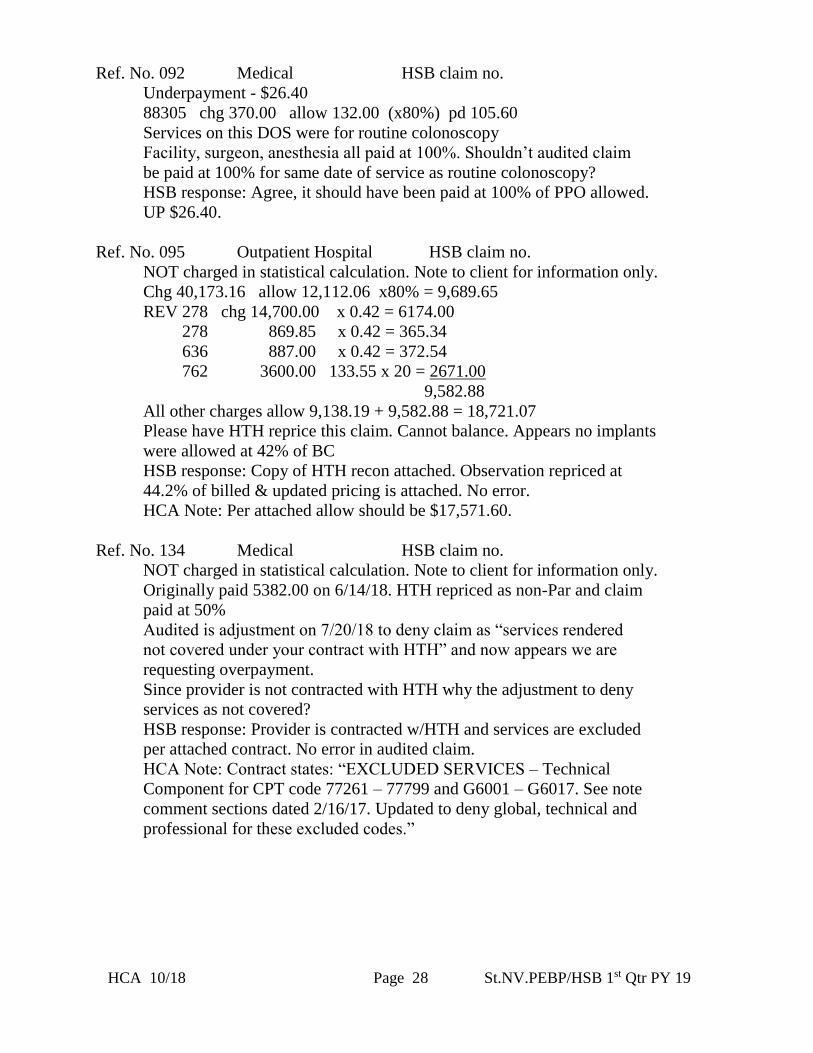
HCA 10/18 Page 28 St.NV.PEBP/HSB 1st Qtr PY 19
Ref. No. 092 Medical HSB claim no.
Underpayment - $26.40
88305 chg 370.00 allow 132.00 (x80%) pd 105.60
Services on this DOS were for routine colonoscopy
Facility, surgeon, anesthesia all paid at 100%. Shouldn’t audited claim
be paid at 100% for same date of service as routine colonoscopy?
HSB response: Agree, it should have been paid at 100% of PPO allowed.
UP $26.40.
Ref. No. 095 Outpatient Hospital HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
Chg 40,173.16 allow 12,112.06 x80% = 9,689.65
REV 278 chg 14,700.00 x 0.42 = 6174.00
278 869.85 x 0.42 = 365.34
636 887.00 x 0.42 = 372.54
762 3600.00 133.55 x 20 = 2671.00
9,582.88
All other charges allow 9,138.19 + 9,582.88 = 18,721.07
Please have HTH reprice this claim. Cannot balance. Appears no implants
were allowed at 42% of BC
HSB response: Copy of HTH recon attached. Observation repriced at
44.2% of billed & updated pricing is attached. No error.
HCA Note: Per attached allow should be $17,571.60.
Ref. No. 134 Medical HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
Originally paid 5382.00 on 6/14/18. HTH repriced as non-Par and claim
paid at 50%
Audited is adjustment on 7/20/18 to deny claim as “services rendered
not covered under your contract with HTH” and now appears we are
requesting overpayment.
Since provider is not contracted with HTH why the adjustment to deny
services as not covered?
HSB response: Provider is contracted w/HTH and services are excluded
per attached contract. No error in audited claim.
HCA Note: Contract states: “EXCLUDED SERVICES – Technical
Component for CPT code 77261 – 77799 and G6001 – G6017. See note
comment sections dated 2/16/17. Updated to deny global, technical and
professional for these excluded codes.”

HCA 10/18 Page 29 St.NV.PEBP/HSB 1st Qtr PY 19
Ref. No. 169 Medical HSB claim no.
Overpayment - $3,683.63
Audited claim paid 8/13/18 for J1569, 72 units total.
Appears audited claim is duplicate to claim xxxxxx also from Accredo
for exact same DOS, service and units paying 3683.64 on 7/23/18.
Shouldn’t audited claim have been denied as a dup?
HSB response: Agree. This is a duplicate. Analyst should have denied.
Ref. No. 170 Outpatient Hospital HSB claim no.
Underpayment - $94.24
Claim paid as: REV 255 chg 186.25 allow 94.24 ded 94.24 pd 0
611 2624.00 1327.65 copay 250 1077.65
1) Since this member has the Premier Plan which has no deductible
Shouldn’t line 1 REV 255 have paid 94.24 versus zero? (REV 255 –
related drugs to MRI)
NOT charged in statistical calculation. Note to client for information only.
2) Claim xxxxxx same DOS for reading of MRI:
70553 chg 386.00 allow/ded 140.70 pd 0.00
Shouldn’t this have paid at 100% versus zero?
HSB response: 1 & B2) Analyst error.
Ref. No. 182 Medical HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
Audited claim is original claim paid 8/7/18 allow 363.76
Claim adjusted under claim xxxxxx on 9/28/18 to now allow 330.68 and
pay 264.54. Claim overpaid 26.47.
Per trans msg HTH provider had a contract change effective 4/20/18 &
incorrect fees were loaded.
When were the correct fees received from HTH?
HSB response: Provider dual contracted – SHO discounts are overall
better than HTH & SHO is used.
Ref. No. 196 Medical HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
Audited is original claim allow/pd 354.19 on 8/9/18
Claim adjusted under xxxxxx on 10/1/18 to allow/pay 335.62. Claim now
overpaid 18.57.
Appears HTH provider had contract change 4/20/18 & incorrect fees loaded
and has now been updated.
HSB response: Provider dual contracted – SHO discounts are overall
better than HTH & SHO is used.

HCA 10/18 Page 30 St.NV.PEBP/HSB 1st Qtr PY 19
Ref. No. 219 Medical HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
Member had 11 claims for this DOS of 6/26/18, all from Health Care Prov
Labs: 8 were processed on 8/3, 2 were processed on 8/2 and 1 was
processed on 8/5
All were paid as non-PPO w/UCR applied. One claim was adjusted & paid
on 9/19/18 as PPO versus non-PPO (claim xxxxxx replaced w/xxxxxx)
chg 669.18 allow 505.24 pd 252.62
Shouldn’t all these claims have been adjusted to apply the PPO network
rates?
HSB response: HTH repriced xxxxxx on 9-12-18 and claim corrected
under xxxxxx on 9-19-18. Copy attached. HTH returned other claims
as non-par, pricing attached. We will send back to HTH to validate all
pricing.
Ref. No. 259 Outpatient Hospital HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
Per contract discount is to be 66%, effective 1/1/18 versus 65%
Claim for PT paid as:
chg 2846.00 (x35%) allow 996.10, paid 796.88 on 8/8/18
1) Should allowable be 967.64 versus 996.10?
2) Should payment be 774.11 versus 796.88?
HSB response: 66% is for ER only – claim priced correctly with 65%
discount. No error.
Ref. No. 262 Medical HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
A9276 chg 2792.97 allow 1050.00 ded 122.29 pd 742.17
Same procedure, same vendor purchased:
DOS 8/6/18 chg 2792.97 allowed 1050.00
1/22/18 2792.97 1134.00
10/22/17 2792.97 1050.00
7/18/17 2792.97 1050.00
All w/same charge but DOS 1/22/18 allowed 1134.00 versus 1050.00 as
others before & after. Please explain why the difference.
HSB response: xxxxxx processed correctly. Bias claim xxxxxx should
have paid with HSB pricing.

HCA 10/18 Page 31 St.NV.PEBP/HSB 1st Qtr PY 19
Ref. No. 278 Medical HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
Claim for 3 hearing aids paid on 8/15/18 as:
Allow 3000.00 ded 1493.10 pd 1205.52
Allowed 1500.00 for each hearing aid – Per MPD “plan pays 80% after
plan year deductible (limit $1500 per device, per each ear)”
Claim adjusted under xxxxx on 9/12/18 to pay an additional 1752.00 as:
Allow 5190.00 ded 1493.10 pd 2957.52
Per trans msg “Per recent email on hearing aids – reversed to allow
correct payment”
Please provide a copy of above referenced email.
HSB response: Processed correctly. Email attached.
HCA Note: Per attached email hearing aid benefit clarified to “not to
exceed an actual paid amount of $1500 per hearing aid (per ear, every
three years”.
Ref. No. 284 Medical HSB claim no.
Overpayment - $25.00
Claim paid as: allow 2051.73 copay 50 pd 2001.73
Claim contains CPT 96401 – chemo administration
96365 – IV infusion for prophylaxis or diagnosis
85025 – CBC
J9041 – cancer drug
J3489 – cancer drug
These charges appear to be for chemotherapy done in physician’s office.
Shouldn’t copay be $75 versus $50?
HSB response: agree, should be $75.00 copay. OP $25.00.
Ref. No. 346 Medical HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
Claim pd as: 77263 allow 508.22 copay 75 pd 433.22
77334 197.43 197.43
99243 299.85 299.85
Since 99243 is an office consultation should we have applied a specialty
copay of $45 on this service?
HSB response: Initial consult billed w/initial radiation therapy charges.
Higher of the two applicable copays applied based on direction from
PEBP. We assessed the higher of two copays, which would be $75 for
radiation therapy.

HCA 10/18 Page 32 St.NV.PEBP/HSB 1st Qtr PY 19
Ref. No. 348 Medical HSB claim no.
Overpayment - $429.00
Claim for 45380 – colonoscopy w/biopsy for child dep w/DX K6389 –
other spec diseases of intestine
Claim paid as preventive since this is first colonoscopy of plan year.
However, patient is a child & per USPSTF routine colonoscopy is
recommended for persons age 50 & older. (Per MPD pg. 29 “Plan
provides coverage for preventive care in accordance with Affordable
Care Act & other services that are recommended by the USPSTF.”
Since patient is a child & DX is medical shouldn’t this claim be paid as
medical versus preventive?
(Individual ded met 273.00, family deductible 1032.59)
NOT charged in statistical calculation. Note to client for information only.
Claim xxxxxx for anes pd 624.00 & xxxxxx for ASC pd 558.39 also paid
at 100% w/same DX. Shouldn’t these have paid as medical?
(Note: claim xxxxxx for lab 88305 same DX took 273.00 to ded)
HSB response: 1) Per MPD page 94, 1st colonoscopy of plan year pays as
preventive regardless of DX and references no age restrictions. 2) No
these would follow colonoscopy & pay at 100% also.
Ref. No. 372 Medical HSB claim no.
Overpayment - $1,086.83
Audited claim DOS 8/14/18:
J1335 units 16 chg 9709.40 allow 2173.81
S9494 8 4532.76 680.00
14,242.16 2853.81 pd 100%
Same provider claim xxxxxx exact services DOS 8/22/18:
J1335 units 16 chg 9709.40 allow 1086.98
S9494 8 4532.76 680.00
14,242.16 1766.98 pd 100%
Same provider claim xxxxxx same services DOS 9/6/18:
J1335 units 12 chg 6626.07 allow 815.23
S9494 6 3399.57 510.00
10,025.64 1325.23
Claims for DOS 8/22/18 & 9/6/18 both allowed $67.94/unit for J1335,
however audited claim allowed $135.86/unit (double). Should the
allowed for J1335 on audited claim be $1,086.98 versus 2,853.81 as
the other claims?
HSB response: Agree. Repricing error. OP 1086.83.

HCA 10/18 Page 33 St.NV.PEBP/HSB 1st Qtr PY 19
Ref. No. 404 Outpatient Hospital HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
This ER bill charged 6607.00 allowed 2246.38 pd 1797.11 on 9/17/18
Allowance of 2246.38 represents discount of 66% which matches contract
(written as 66% eff 1/1/18 on contract that displays 65% disc in typed form)
HSB response: Claim priced with 66% discount correctly. ER services –
copy of contract attached. No error.
Ref. No. 407 Outpatient Hospital HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
93000 chg 15.85 allow/pd 15.85
DX: T675 – heat exhaustion & R4182 – altered mental states
OOP not met. Please explain why this claim paid at 100% versus 80%.
HSB response: First EKG of plan year pays at 100%. No error.
HCA Note: MPD page 94 states, “the first billed procedure of the Plan
Year for a colonoscopy or a mammogram will be considered preventive
regardless of the diagnosis.” EKG is not listed as a service under this
consideration.
Ref. No. 507 Outpatient Hospital HSB claim no.
NOT charged in statistical calculation. Note to client for information only.
19357-50 allow 2397 x 150% = 3595.50 x 50% = 1797.75
19303-50 2098 x 150% = 3147.00 x 50% = 1573.50
15777-50 3335 x 150% = 5002.50
REV 278 21,304.00 x 40% = 8521.60
636 131,192.00 x 40% = 52476.80
69,372.15
1) Claim paid as: allow 60,850.55 coins 793.95 pd 60,056.60
Appears implants not paid due to lack of invoice. No language in contract
with hospital that says invoice needed for payment. Shouldn’t we have
paid the implants?
2) Is invoice required by HSB to pay implants? If so, please explain the
SOP regarding when & why invoices are required.
HSB response: 1) No per policy & procedures – implants in excess of
$10,000.00 require invoice. 2) Yes, policy & procedure attached.
HCA Note: Per attached policy & procedure for non-SHO network claims
if complete description of the implant charges is not received, “it is
permissible to deny the implant portion of the claims for that specific
information and consider the remaining charges for payment”.

HCA 10/18 Page 34 St.NV.PEBP/HSB 1st Qtr PY 19
Ref. No. Focus 1
NOT charged in statistical calculation. Note to client for information only.
J0257 2000 units chg 10,880.00 DOS 8/30/18
570 units 3,149.25 DOS 8/15, 7/25, 8/8 & 8/1/18
525 units 2,856.00 DOS 7/5, 7/12 & 7/19/18
2000 units 45,500.00 DOS 9/19/18
This member has claims for J0257 services provided by Diplomat
Pharmacy. This product should be purchased through Accredo.
HSB has pended these claims for payment, however, system reflects
Prior Authorizations from HTH for the member to participate this
service w/Diplomat.
1) DOS 8/30/18, J0257 2000 units charged $10,880.00
DOS 9/19/18, J0257 2000 units charged $45,500.00
2) $77,545.00 in charges for 10 claims with J0257 authorized w/Diplomat
which should be authorized w/Accredo
Note: 19 claims auth’d w/Diplomat

Little Rock / Columbus / El Paso / Indianapolis / Los Angeles / Nashville / St. Louis www.healthscopebenefits.com
November 2, 2018 Public Employees’ Benefits Program Board State of Nevada 901 Stewart Street, Suite 1001 Carson City, NV 89701 Subject: Audit Results July 1, 2018 – September 30, 2018 Dear Public Employees’ Benefits Program (PEBP) Board: HealthSCOPE Benefits appreciates the opportunity to respond to the audit performed by Health Claim Auditors for the first quarter of Plan Year 2019. The audit included 500 claims with paid amounts totaling $305,108.85. HealthSCOPE Benefits is very disappointed to have missed the financial accuracy percentage for this audit period. We take the quality of our work very seriously and strive for perfection. We continue to review quality improvement opportunities within our organization and our vendor partners. Based on our review, we have implemented the following quality control measures: Item (1) HealthSCOPE Benefits will conduct continued education with the Claims staff regarding our claims system edits. The initial claim was submitted as one line and the second submission received from the provider reflected four different service lines. Item (2) HealthSCOPE Benefits is pursuing system enhancements to improve the automated duplicate parameter review. We have implemented a new workflow process and created a daily QA report to review possible duplicate claims. We will continue to investigate other quality control measures from a programming perspective.
27 Corporate Hill Little Rock, AR 72205

Little Rock / Columbus / El Paso / Indianapolis / Los Angeles / Nashville / St. Louis www.healthscopebenefits.com
We continue to be pleased with the financial savings we are able to provide on the PEBP account. We saved PEBP an additional $1,593,694 through non-network negotiations, subrogation and transplant savings in the first quarter of Plan Year 2019. We appreciate the quarterly audit process and the interaction between Health Claims Auditors, PEBP, and HealthSCOPE Benefits as it provides for continuous improvement in our service. Sincerely,
Mary Catherine Person President & Co-CEO

6. 6. Health Claim Auditors, Inc. annual audit of Willis Towers
Watson’s OneExchange for the timeframe July 1, 2017 – June 30, 2018: (1) Report from Health Claim Auditors; (2) Willis Towers Watson's response to audit report; and (3) for possible action to accept audit report findings and assess penalties, if applicable, in accordance with the performance guarantees included in the contract pursuant to the recommendation of Health Claim Auditors. (For Possible Action)


Medicare Exchange Health Reimbursement Arrangement
Audit Report for
Conducted on
WTW Willis Towers Watson
Audit Period:
PEBP Plan Year 2018
Submitted By:
Health Claim Auditors, Inc.

TABLE OF CONTENTS
Page(s)
Introduction 1 - 2
Executive Summary of Findings 2 - 7
Other Customer Service Measurements 8
Overpayments 8
Explanation of Payments 9
Participant Funding 9
Participant Survey 9
Breakout of Claims Audited 10
Payment Accuracy 10
Financial Accuracy 11
Disputed Claims 11
Turnaround Times 12
Policy, Procedures and System 12 - 14
Customer Service Detail 14 - 15
Reporting 16
Specific Claim Audit Detail 17 - 25
Exhibit A –
Explanation of Payment 26 – 27

HCA 10/18 Page 1 St. NV. PEBP/WTW/PayFlex
State of NV. PEBP - Health Reimbursement Arrangement
Introduction
The State of Nevada Public Employees’ Benefits Program (PEBP) requested
Health Claim Auditors, Inc. (HCA) to conduct a Claims and System Audit on Willis
Towers Watson (WTW), contracted with PEBP as the current contracted vendor
for administration of the PEBP Medicare Exchange Health Reimbursement
Arrangement (HRA) plan. This audit is conducted per The State of Nevada
Division of Purchasing Request For Proposal (RFP) No. 1922.
WTW’s subcontractor, PayFlex*, administrates the claims adjudication function
for the Medicare Exchange HRA PEBP plan. The onsite portion of the audit was
conducted in September 2018 at the PayFlex location in Omaha, Nebraska.
* PayFlex, an Aetna company, is a benefit administrator specializing in the
administration of flexible spending accounts, health savings accounts, health
reimbursement arrangements and COBRA administration.
HCA was provided with a claim file from PayFlex of claims adjudicated for
PEBP’s Plan Year 2018 (July 2017 – June 2018). The file contained information
pertinent to 353,704 HRA claims representing $40,763,330.79 in requested
reimbursements. A claim is defined as each separate expense reimbursement
request. Requests that contain multiple expenses (such as prescriptions) are
separated and administered as separate claims.
The purpose of the audit was to assure that WTW/PayFlex is doing an effective job
of controlling claim costs while processing HRA claims accurately and within a
reasonable period of time.
The preliminary report was presented to WTW for additional comments and
responses on 18 September 2018. Additional comments/responses received from
WTW/PayFlex are included within the report and identified in bold/italicized type.
In situations where there is disagreement between HCA and the Administrator as
to what constitutes an error, both sides are presented in the report. Final
determination of error rests with the client. The statistical effect on the Financial
Accuracy measurement for each error is displayed in the HCA note immediately
after the WTW comment.
Detailed data for each of the items displayed within the results, both statistical and
non-statistical calculations, can be found in the Specific Claim Audit Details
chapter of this report, which begins on page 17.
A valid random selection of 400 claims plus no more than 200 bias* selected claims
were identified for audit as per agreement.
*Bias claims are not part of the random selection but were selected manually and
audited by HCA because of some “out of the ordinary” characteristic of the claim.

HCA 10/18 Page 2 St. NV. PEBP/WTW/PayFlex
Bias claims are not included within the statistical calculations for measurement of
Performance Guaranteed categories within the Administration Agreement.
The valid random selection included claims from all categories adjudicated by
PayFlex. These categories included, but were not limited to: 1) deductibles; 2)
dental; 3) medical; 4) orthodontia; 5) over the counter; 6) premiums; 7)
prescriptions and 8) vision claims.
The Claim Financial Precision provision in the Agreement defines the
measurement of the “Total Amount Approved”. The statistical calculations for this
category includes all payments completed for the participant’s request for the entire
history of the claim up to the date the claim is audited.
EXECUTIVE SUMMARY OF FINDINGS
Guaranteed Performance Measurements - Audit Period: 01 July 2017
through 30 June 2018 (PEBP Plan Year 2018) Metric Guarantee Measurement Actual Pass/Fail
Claim Processing
Turnaround Time
Processing will average two (2) business days
or less. Additionally, 98% of all claims will be
processed within five (5) business days.
0.91 Bus.
Days
Pass
Claim Processing
Payment Precision
Processing average precision will be at
least 98% or better.
97.0%*
Fail
Claim Financial
Payment Precision
Financial accuracy will be 98% or
better
95.59%* Fail
Customer Service
Abandon Rate
The percentage of incoming calls
abandoned by participants be 5% or less
1.526%**
Pass
Customer Service
Speed to Answer
Incoming telephone calls, on average, shall
be answered within thirty (30) seconds.
28.3 sec.**
Pass
Reports
Reports will be available within ten (10)
business days of the end of the period. No Delays
Noted
Pass
HRA Web Services
99% availability of web services for
benefit information and HRA information
exclusive of scheduled maintenance.
99.0% +
Pass
Disclosure of
Subcontractors
Contractor shall not engage additional
subcontractors to maintain PEBP data nor
change the physical locations where PEBP data
is maintained and/or stored without written
authorization by PEBP.
No
Exceptions
Detected
Pass
Unauthorized
Transfer of PEBP
Data
All PEBP data will be stored, processed and
maintained solely on currently designated servers
and storage devices identified in this contract
amendment and/or prior contract documents.
No
Exceptions
Detected
Pass
Speed to Respond
to Issue(s)
98% of incoming participant issues are to
be responded to within 48 Hours of receipt
100%
Pass
Issue Resolution 98% of incoming issues escalated are to be
resolved within 30 business days
99.0%
Pass
* Please refer to Disputed Claims section displayed on page 11.
** Please refer to Disputed Calculation Methods section displayed on page 15.
NOTE: Disputes DO NOT affect the Pass/Fail results of these categories.

HCA 10/18 Page 3 St. NV. PEBP/WTW/PayFlex
Historical Statistics
The following reflects the historical statistical data since the origin of PEBP Health
Reimbursement Arrangement (HRA) claims administration by WTW. The entries
designated in bold red type are measurable categories below the Service
Performance Guarantees Agreement.
Period Audited Payment
Accuracy
Financial
Accuracy
Turnaround
Time
Telephone Response
Telephone Abandon Rate
Plan Year 2012 91.6% NA 1.2 days 0:19 1.07%
Plan Year 2013 98.7% 99.2% 1.1 days 0:15 0.94%
Plan Year 2014 98.2% 99.3% 1.3 days 0:19 1.30%
Plan Year 2015 98.0% 98.5% 1.3 days 0:24 1.47%
Plan Year 2016 98.7% 99.58% 1.1 days 1:50 4.15%
Plan Year 2017 96.0% 96.36% 0.59 days 0:46 2.7%
Plan Year 2018 97.0% 95.59% 0.91 days 0:28 1.53%
Trends/Issues
The audit revealed the following issues or trends detected from the random
selection and bias selected claims. Please note: the reference numbers in bold type
are claims from the random selection and are included within the statistical
calculations. Reference numbers in normal type were identified as issues in bias
claims as defined earlier and are not included within the statistical calculations of
this audit. Specific information regarding supporting reference numbers can be
found in the Audit Results Section in numerical sequence, which begins on page
17.
Duplicate premium paid; Supporting ref. nos. 063, 254, 264, 268 and 374
Paid without proper documentation; Supporting ref. nos. 105 and 218
Claim incorrectly denied; Supporting reference nos. 266 and 360
Claim crossing plan years reimbursement amount split by system
versus manually; Supporting reference no. 121
Claim not paid when contribution loaded due to being stuck in
system; Supporting reference no. 179
Social Security premium deduction future dates reimbursed; Supporting reference no. 179
Non-requested amount paid; Supporting reference no. 241

HCA 10/18 Page 4 St. NV. PEBP/WTW/PayFlex
RXs for two different dates paid with same DOS on one line; Supporting reference no. 267
Multiple services not entered separately; Supporting reference no. 287
Charge for multiple months premium not broken into individual
monthly charge; Supporting reference no. 295
Incorrect date of service entered; Supporting reference no. 391
The audit revealed the following issues, which appear to be administered properly
by Willis Towers Watson/PayFlex but should be brought to client attention for
proper notification or verification. Specific information regarding supporting
reference numbers can be found in the Audit Results Section in numerical
sequence, which begins on page 17.
Dual TPD entry caused by carrier; Supporting reference nos. 220 and 306
Paid without complete documentation due to copay rule; Supporting reference nos. 276 and 334
Two months recurring claims not broken into separate months; Supporting reference no. 063
Itemized statements entered as one line using date span; Supporting reference no. 121
Member disenrolled in plan resulting in file overpayment; Supporting reference no. 155
Initial denial/overpayment notice EOP sent, then additional
overpayment EOPs sent for next three months;
Supporting reference no. 155
Recurring premium request submitted on incorrect form denied
for service not provided yet versus denying for incorrect form used; Supporting reference no. 166
Real time duplicate logic not added to system until June 2018; Supporting reference no. 187
Dental charges paid with documentation showing insurance payment
but not discounted amounts; Supporting reference no. 200
Proof of payment not required for medical claims; Supporting reference
no. 285

HCA 10/18 Page 5 St. NV. PEBP/WTW/PayFlex
Other Audit Findings/Observations
WTW, originally contracted with PEBP as Extend Health, has been the
administrator of Health Reimbursement Arrangement (HRA) claims for the PEBP
retirees since July 2011.
HCA recognizes the numerous improvements in system edits, policies and
procedures instituted this audit period with more to be applied in PEBP Plan Year
2019, however, reports the following detected issues of concern:
Overpayments
It is HCA’s opinion that overpayments have become a serious issue as new
identified overpayments are far greater than successful collections.
Overpayments were found to be $802,455.47 at the end of Plan Year 2018
representing 1,549 claims. This amount is an increase of 249 claims (19.1%)
representing an increase of $18,177.18 (2.3%) from the Plan Year 2017 totals.
Causes of overpayments vary from rescinded funding(s) from PEBP,
reimbursement errors to carrier issues as described above.
Collections for overpayments become very difficult to collect when they age
more than two (2) years. Currently, of the 1,549 claims, 1,174 (76%) claims
representing $675,143.79 in overpayments are greater than two (2) years of age.
Date of Service (DOS) Entries
An issue detected in previous audits as well as this audit, concerned the date of
service entries into the PayFlex system. It is the auditor’s opinion that the exact
date(s) of coverage should be entered into the adjudication system in order for
the system to detect issues such as possible duplicates. As example, if a carrier
bills for multiple months such as January 01 – March 30, it is entered into the
system as 01 January – 01 January, and the system cannot detect a possible
duplicate if the carrier would bill for an individual month such as 01 February
– 28 February. It is HCA’s opinion that this operational procedure has caused
the system to not detect duplicates as identified and reported within this audit.
Discussions with PayFlex reflect that they have recently applied a “real time”
duplicate edit that we believe will produce greater accuracy in detecting
possible duplicate submissions of reimbursement(s). PayFlex also stated that
they will be instituting a change in the entry of multiple month premium
requests. They stated that the current policies of breaking multiple month
premium requests into separate month entries will be expanded to include those
requested from third parties. It is our opinion that this will also greatly improve
the function of the system edits and also reduce possible duplicates as detected
in this audit.

HCA 10/18 Page 6 St. NV. PEBP/WTW/PayFlex
Focus Audits
PEBP staff provided HCA with fourteen (14) cases where the participant had
communicated that they had negative issues or concerns with WTW during the
audited period. These cases were supplied in three (3) different types”
1) Enrolled in June 2018 but carrier did not receive information
The participant provided communications and enrolled with WTW in
June 2018 for initial coverage to be effective 01 September 2018. The
participant was told by WTW that there was a problem with their file and
would have to re-submit their application.
HCA findings: It was confirmed that the participant enrolled in June
2018, however, it appears that UHC did not receive his enrollment.
Participant called in multiple times in August 2018 as followup, WTW
engaged with research of the issue and requested the participant to re-
enroll at the end of August 2018. Participant was informed on 11
September 2018 of successful enrollment and funding found to be
installed on 13 September 2018.
2) June 2018 Eligibility but not enrolled as of September 2018
This issue contained twelve (12) participants that are reported as eligible
for HRA participation in June/July 2018 but not reported as enrolled in
programs even though most has Tristar as a sponsor.
HCA findings: Of the 12 participants within this issue, HCA found one
(1) case that was subject to an error caused by WTW/PayFlex. In this
one case, the incorrect social security number was entered by
WTW/PayFlex on the original enrollment in June 2018 and created two
(2) files for this individual and unfortunately, the funding provided for
this participant was not linked to both files. WTW/PayFlex stated that
they would combine these files and a complete fix should be expected
within seven (7) days.
3) May 2018 eligibility but no funding as of September 2018
This participant became eligible for funding effective 01 May 2018. Per
PEBP eligibility vendor, this participants information was sent to WTW
on 21 May 2018 changes file and all subsequent full eligibility files of
June, July, august and September.
HCA findings: Records reflect that this participant now has his
funding reinstated. The allocations were deposited on 9/19/2018 and
pending claims were reimbursed, 9/21/2018. Their new expense period
starts as of 5/1/2018 and the participant was informed of the updates by
the CSS team.

HCA 10/18 Page 7 St. NV. PEBP/WTW/PayFlex
Validation of Carrier Commissions
During the September 17, 2015 PEBP Board of Directors meeting, the WTW
representative was quoted that the average annual amount of commission that
we receive for each individual that is enrolled is $300. It was requested that
HCA validate the commissions earned by Willis Towers Watson for each
audited period thereafter.
The statement received from Willis Towers Watson reflects that they received
a total of $3,100,273.79 in commissions for PEBP Plan Year 2018.
Conclusion
It is HCA’s unbiased opinion that metric measurements for this audited period
were equal to or better than the agreed values within the Service Performance
Standards Related to HRA Services Agreement (Agreement), Attachment N,
with the exclusion of the following;
1) Underperformance of the > 98% Claim Processing Payment Precision
Guarantee. Penalty is to be 2% of total fees for the twelve (12) month
period being audited.
2) Underperformance of the > 98% Claim Financial Precision Guarantee.
Penalty is to be 2% of total fees for the twelve (12) month period being
audited.
HCA recommends that PEBP consider the collection of the penalty for the
underperformance of these categories.
Identified overpayments have increased to $802,455.47 with a volume of 1,549
claims. HCA is recommending that WTW continue the reporting to PEBP that
displays the cause/reason for each overpayment and provide an operational
process to collect these overpayments. HCA also recommends that this process
include reporting to help quantify and/or aid in identifying the responsible party
of the overpayment.
HCA is satisfied thus far with the WTW/PayFlex current changes and promised
actions to resolve the problem of the one date entered for service dates when
multiple months or time periods are billed and looks forward to the audit of the
future resolution(s) for this issue in future audits.
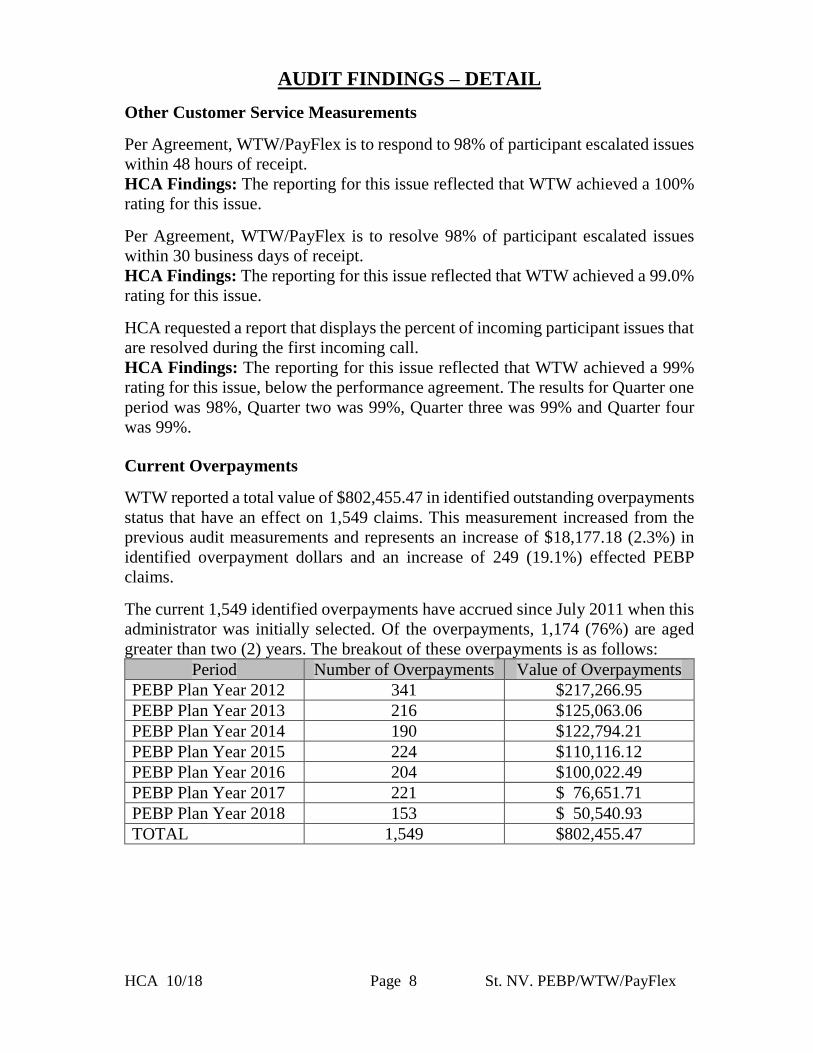
HCA 10/18 Page 8 St. NV. PEBP/WTW/PayFlex
AUDIT FINDINGS – DETAIL
Other Customer Service Measurements
Per Agreement, WTW/PayFlex is to respond to 98% of participant escalated issues
within 48 hours of receipt.
HCA Findings: The reporting for this issue reflected that WTW achieved a 100%
rating for this issue.
Per Agreement, WTW/PayFlex is to resolve 98% of participant escalated issues
within 30 business days of receipt.
HCA Findings: The reporting for this issue reflected that WTW achieved a 99.0%
rating for this issue.
HCA requested a report that displays the percent of incoming participant issues that
are resolved during the first incoming call.
HCA Findings: The reporting for this issue reflected that WTW achieved a 99%
rating for this issue, below the performance agreement. The results for Quarter one
period was 98%, Quarter two was 99%, Quarter three was 99% and Quarter four
was 99%.
Current Overpayments
WTW reported a total value of $802,455.47 in identified outstanding overpayments
status that have an effect on 1,549 claims. This measurement increased from the
previous audit measurements and represents an increase of $18,177.18 (2.3%) in
identified overpayment dollars and an increase of 249 (19.1%) effected PEBP
claims.
The current 1,549 identified overpayments have accrued since July 2011 when this
administrator was initially selected. Of the overpayments, 1,174 (76%) are aged
greater than two (2) years. The breakout of these overpayments is as follows:
Period Number of Overpayments Value of Overpayments
PEBP Plan Year 2012 341 $217,266.95
PEBP Plan Year 2013 216 $125,063.06
PEBP Plan Year 2014 190 $122,794.21
PEBP Plan Year 2015 224 $110,116.12
PEBP Plan Year 2016 204 $100,022.49
PEBP Plan Year 2017 221 $ 76,651.71
PEBP Plan Year 2018 153 $ 50,540.93
TOTAL 1,549 $802,455.47
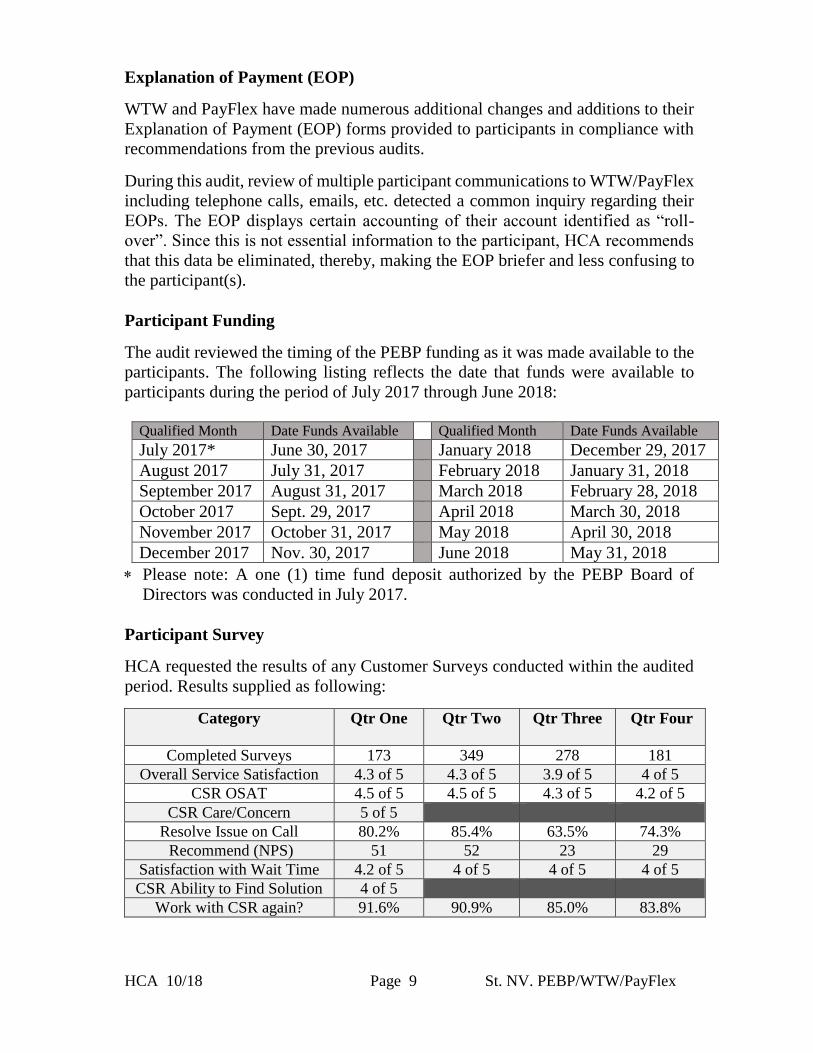
HCA 10/18 Page 9 St. NV. PEBP/WTW/PayFlex
Explanation of Payment (EOP)
WTW and PayFlex have made numerous additional changes and additions to their
Explanation of Payment (EOP) forms provided to participants in compliance with
recommendations from the previous audits.
During this audit, review of multiple participant communications to WTW/PayFlex
including telephone calls, emails, etc. detected a common inquiry regarding their
EOPs. The EOP displays certain accounting of their account identified as “roll-
over”. Since this is not essential information to the participant, HCA recommends
that this data be eliminated, thereby, making the EOP briefer and less confusing to
the participant(s).
Participant Funding
The audit reviewed the timing of the PEBP funding as it was made available to the
participants. The following listing reflects the date that funds were available to
participants during the period of July 2017 through June 2018:
Qualified Month Date Funds Available Qualified Month Date Funds Available
July 2017* June 30, 2017 January 2018 December 29, 2017
August 2017 July 31, 2017 February 2018 January 31, 2018
September 2017 August 31, 2017 March 2018 February 28, 2018
October 2017 Sept. 29, 2017 April 2018 March 30, 2018
November 2017 October 31, 2017 May 2018 April 30, 2018
December 2017 Nov. 30, 2017 June 2018 May 31, 2018
Please note: A one (1) time fund deposit authorized by the PEBP Board of
Directors was conducted in July 2017.
Participant Survey
HCA requested the results of any Customer Surveys conducted within the audited
period. Results supplied as following:
Category
Qtr One
Qtr Two Qtr Three Qtr Four
Completed Surveys 173 349 278 181
Overall Service Satisfaction 4.3 of 5 4.3 of 5 3.9 of 5 4 of 5
CSR OSAT 4.5 of 5 4.5 of 5 4.3 of 5 4.2 of 5
CSR Care/Concern 5 of 5
Resolve Issue on Call 80.2% 85.4% 63.5% 74.3%
Recommend (NPS) 51 52 23 29
Satisfaction with Wait Time 4.2 of 5 4 of 5 4 of 5 4 of 5
CSR Ability to Find Solution 4 of 5
Work with CSR again? 91.6% 90.9% 85.0% 83.8%

HCA 10/18 Page 10 St. NV. PEBP/WTW/PayFlex
Breakdown of Claims Audited
The individual claim requests audited were randomly selected from PEBP’s claims
listings as supplied by WTW. The detail claims listing supplied, reflected each
separate service as a claim. These claims were processed by WTW/PayFlex from
01 July 2017 through 30 June 2018. These claims were stratified by dollar volume
to assure that HCA audited all types of claims.
The breakdown of the 400 random selected claims is as follows:
Type of Service Requested Amount Audited (Req – Denied) Paid Amount
Medical $ 15,077.44 $ 10,832.27 $ 5,322.27
Dental $ 6,675.70 $ 6,126.70 $ 5,219.00
Vision $ 3,975.01 $ 3,407.21 $ 2,907.21
Premiums $ 35,137.57 $ 34,355.48 $ 19,311.87
Prescription $ 5,409.57 $ 5,051.57 $ 3,019.99
Deductible $ 1,630.77 $ 1,519.50 $ 1,519.50
Over The Counter $ 323.72 $ 313.02 $ 313.02
Orthodontia $ 1,749.20 $ 1,749.20 $ 1,749.20
TOTAL $ 69,978.78 $ 63,354.95 $ 39,362.06
Payment Accuracy
Per agreement, payment accuracy for the randomly selected claims should be 98%
or above. Payment accuracy is defined as a claim that was processed for payment
without a payment or non-payment error. Payment Accuracy is calculated by
dividing the total number of claims not containing payment errors in the audit
period by the number of claims audited within the random selection.
The Payment Accuracy Percentage of the number of claims paid correctly from the
WTW random selection for this audited period is 97.0%* (please refer to Disputed
Claims section, page 11, 97.5% without disputed claims calculated).
Payment Accuracy
Medical …
Vision …
Premiums 54.20%
Dental …
Prescription…
Deductible2.40%
Orthodontia2.70%
Over The Counter0.50%
Claim Audited $ Distribution MedicalVisionPremiumsDentalPrescriptionsDeductibleOrthodontiaOver The Counter
98%
97.0%
90% 92% 94% 96% 98% 100%
Payment Accuracy
Guarantee

HCA 10/18 Page 11 St. NV. PEBP/WTW/PayFlex
Financial Accuracy
Per agreement, financial accuracy for the randomly selected claims should be 98%
or above. Financial accuracy is defined as total absolute value (overpayments and
underpayments) as difference of the correct payment amount. The payment amount
is defined, by agreement, as the full requested amount minus any denied amount.
Financial Accuracy is calculated by dividing the total dollar amount of claims not
containing payment errors in the audit period by the dollar amount of claims audited
within the random selection.
The Financial Accuracy Percentage of the number of claims paid correctly from
the WTW random selection for this audited period is 95.59%* (please refer to
Disputed Claims section, below, 95.66% without disputed claims calculated).
Financial Accuracy
Statistical calculations for the metric measurement of the Performance Guarantees
are calculated of the claims adjudicated from the period of 01 July 2017 through 30
June 2018 (PEBP Plan Year 2018). Specific audit error findings and issues can be
reviewed within the Specific Claim Audit Detail section of this report, which begins
on page 17.
* Disputed claims within the Performance Guarantee Statistics
HCA conducts the audit as per standards set forth within documented agreements
between the client and administrator. HCA has received rebuttals from
WTW/PayFlex for claims charged as errors within this report that they believe
should not be calculated as an error. In situations where there is disagreement
between HCA and the Administrator as to what constitutes an error, both sides are
presented in the report. Final determination of error rests with the client. The total
effect of these two (2) disputed claims is 0.5% on Payment Accuracy and 0.06%
on Financial Accuracy. If determined that these two (2) disputed claims should not
be calculated as errors, the Payment Accuracy would be 97.5% versus 97.0% and
the Financial Accuracy would be 95.66% versus 95.59%.
1) Ref. No. 254, $38.89 overpayment. The participant requested this amount
as a dental premium reimbursement. The document received by PayFlex
did reflect the reimbursement for a medical premium, however, the
premium was for a dental plan. PayFlex processed per the display on the
received document. It is the auditor’s opinion that due to documentation
not matching the member’s reimbursement form, verification should have
been sought and found that this was for a dental premium.
98%
95.59%
90% 92% 94% 96% 98% 100%
Financial Accuracy
Guarantee

HCA 10/18 Page 12 St. NV. PEBP/WTW/PayFlex
2) Ref. No. 287, no financial error charged. The participant requested
reimbursement for three (3) items (filters, headgear and replacement
humidifier chamber). All 3 were paid as one receipt as per their
policy/process. It is the auditor’s opinion that claims such as these should
be entered as are the prescription drug claims, each item listed separately.
By entering these as one entry, the system cannot properly identify
possible duplicates if the participant resubmits partial or different number
of items on another request.
Turnaround Time
Turnaround time for claim payments is measured in business days from the date
WTW/PayFlex receives the claim to the date the claim was processed and also from
the date received to the date of payment. Per agreement, all claims in aggregate will
be processed within an average of two (2) business days and 98% of all claims will
be processed within five (5) business days.
HCA requested a lag report from PayFlex that displayed the processing turnaround
times. This report reflected that the audited period turnaround time for processing
claims was 0.91 business days and also meeting the 98% of claims processed within
5 business days guarantee. The random selection was tested for the average
turnaround with a result of 1.8 business days.
During the audited period, WTW received a total of 866 Emails from participants
to the Email team seeking information. The average time to respond to these emails
was within 30 minutes.
Policy, Procedures and System
WTW receives the funding and eligibility data directly from PEBP and relays this
information to PayFlex on a regular basis.
WTW applies received funding and eligibility data weekly, every Thursday. WTW
stated that they are moving toward updating eligibility daily. Allocations are
applied to the HRA’s by the first of the month. Participants with retroactive
qualification will receive their allocation on the next weekly file following
qualification.
Claims are received at the PayFlex facility in Omaha, Nebraska by mail, facsimile
and other third party requestors such as insurance carriers. PayFlex stated that all
claims received from PEBP participants are scanned into the PayFlex system the
date they are received and assigned a document identification number.

HCA 10/18 Page 13 St. NV. PEBP/WTW/PayFlex
Claims are transferred and archived into the PayFlex adjudication system,
Complete Benefit Administration System CBAS) within forty-eight (48) hours of
receipt. PayFlex has utilized this system since 2006 and owns the key for any
program changes.
PayFlex has a two (2) level appeal process for claims questioned by PEBP
participants. If the two appeals are exhausted with PayFlex, the participant has the
right for a third level appeal. When this level is achieved, the claim is sent to
the client for final disposition.
PayFlex stated that they have internal written Standard Operating Procedures
(SOP). HCA reviewed these SOPs during the on-site portion of the audit:
1) Standard requirements for documentation from PEBP participants for
payment of premiums, prescriptions and medical reimbursement
requests;
2) Standard operations requirements of PayFlex associates for all processes
from receipt of the request to payment.
PayFlex stated that they have over fifty (50) experienced processors for requests
received in the Omaha, Nebraska facility. PayFlex stated that PEBP has no
dedicated processors assigned to their account, however, PayFlex has designated\
27 examiners to adjudicate the WTW client claims.
Initial processor training lasts from two (2) weeks to six (6) months depending on
the individual. PayFlex stated that they conduct internal audits on all processors.
New processors have 100% audit until the supervisor is satisfied with their
performance. Experienced processors have four (4) claim lines audited per every
three hundred and fifty (350) lines processed.
WTW stated that they have over one thousand (1,000) Customer Service
Representatives that address all incoming inquiries from client participants.
PayFlex also stated that they have over eighty (80) Customer Service
Representatives to provide services to their clients. Both WTW and PayFlex stated
that no Customer Service Representatives are dedicated to the PEBP plan.

HCA 10/18 Page 14 St. NV. PEBP/WTW/PayFlex
HCA had requested a written response from WTW and/or PayFlex that any and all
PEBP Personal Health Information (PHI) is retained with secured practices within
their operating systems and that no PHI is shared, transferred or obtained to any
other entity other than WTW or PayFlex, including any subcontracted or entities
that have acquired their businesses since the authorization of their vendor contract
with PEBP. HCA redacted the names of these subcontractors for confidentiality
purposes. WTW response: Subcontractor Entity Name
Axxx
Bxxx
Cxxx
Dxxx
Ixxx
Ixxx
Lxxx
Oxxx
Pxxx
Pxxx
Pxxx
Rxxx
Txxx
Zxxx
HCA requested that WTW please verify if any of these entities were NOT
supplied to PEBP as subcontractor vendors previous to this audit report
disclosure.
WTW/PayFlex comment: Bxxx, Pxxx and Pxxx are future subcontractors and
new to this list. However, as they are new, disclosure is not needed yet.
Customer Service
Per agreement, the average incoming telephone response time should be within
thirty (30) seconds or less. The report supplied by WTW reflected that the average
answer speed for all incoming calls during the period of 01 July 2017 through 30
June 2018 was 28.3 seconds** (0:28.3) (please refer to page 15 for Disputed
Calculation Method). The average response time for Quarter One was 11.5 seconds,
77.8 seconds for Quarter Two, 5 seconds for Quarter Three and 4.9 seconds for
Quarter Four. Note: the number of calls utilized for calculation of this category
were obtained from the FCR report.
Telephone Average Response Time
30
28.3
0 10 20 30 40 50
Response (in seconds)
Performance Guarantee

HCA 10/18 Page 15 St. NV. PEBP/WTW/PayFlex
Per agreement, the abandonment rate must be under five percent (5%) of total
incoming. HCA has reviewed the appropriate report for the audited period, which
revealed the abandoned calls ratio to be 1.53%** (refer below for Disputed
Calculation Method) for the period of 01 July 2017 through 30 June 2018 (period
measurable against the Performance Agreement)*. The average abandonment rate
for Quarter One was 1.12%, 3.77% for Quarter Two, 0.35% for Quarter Three and
0.46% for Quarter Four.
Abandonment Rate
Please note: WTW utilizes an Integrated Telephone System and these customer
service performances are measurements after the participant completes the
integrated inquiries that aid in the directing of the call.
** Disputed Calculation Method
WTW has received communications, in which they disagree with the method
utilized by HCA to calculate the telephone response time and abandonment rate for
the annual metrics in comparison with the performance agreement for these
categories. The reports received by WTW/PayFlex displayed only the averages for
these categories for each quarter year so HCA requested the number of calls
received in each quarter in order to accurately calculate the annual average.
WTW/PayFlex calculations: Period No. of calls Reported Aver
Response Time
Reported Aver
Abndmnt Rate
Jul – Sep 2017 74,154 11.553661 sec 1.12%
Oct – Dec 2017 159,258 77.8 sec. 3.77%
Jan – Mar 2018 208,997 5 sec. 0.35%
Apr – Jun 2018 76,253 4.9 sec. 0.46%
Plan Year 2018 518,662 24 sec. 1.43%
HCA calculated the annual average telephone response time and abandonment rates
as follows: Period No. of
calls
Aver Response
Time
Total
Seconds
Aver Abndmnt
Rate
No. Abndmnt
Calls
Jul – Sep 2017 74,154 11.553661 sec 856,750 1.12% 830
Oct – Dec 2017 159,258 77.8 sec. 12,390,272 3.77% 6,004
Jan – Mar 2018 208,997 5 sec. 1,044,985 0.35% 731
Apr – Jun 2018 76,253 4.9 sec. 373,639 0.46% 350
Plan Yr 2018 518,662 28.3 sec. 14,665,646 1.53% 7,915
14,665,646 seconds / 518,662 calls = 28.3 seconds average telephone response.
7,915 abandonment calls / 518,662 calls = 1.53%
5
1.53
0 1 2 3 4 5 6
Percentage of Calls Abandoned
Performance Guarantee

HCA 10/18 Page 16 St. NV. PEBP/WTW/PayFlex
Reporting
Per Agreement, the following reports will be available within ten (10) business days
of the end of the reporting period if requested or scheduled by the last day of the
reporting period or later if agreed to by PEBP. Analyses of data or custom reports
are excluded.
Standard:
Ledger Summary
Production Payment Register
Deposit Summary
Payment Summary
Optional:
Employer Funding Summary
Employer Funding Detail Report
Overpaid Employees Report
Quarterly:
S.C.O.R.E. Analysis
Account utilization
Claim information
Direct Deposit
Benefit Reports (Included in the quarterly board presentation):
Retiree Enrollment Decisions
Retiree Premium Costs
Retiree Survey Results
Benefit Customer Service Matrices
Issue Resolution Summary
Quarterly board presentations will be provided fifteen (15) business days prior to
the quarterly board meeting where it is scheduled for presentation.

HCA 10/18 Page 17 St. NV. PEBP/WTW/PayFlex
SPECIFIC AUDIT RESULTS Listed below are the errors or issues of discussion found by this audit while
processing the claims for PEBP Exchange HRA Plan.
Ref. No. 063 WTW/PayFlex claim no.
Overpayment - $39.40
1) Expense is for 2 months of RX premium (39.40/mo)
Should each month have been processed on a separate line versus on
one line with a DOS span of 7/1/17-8/1/17?
2) Per claims history review appears 8/1/17 premium of $39.40 also
paid as TPD on claim ID xxxxxx on 8/31/17. Appears audited claim
is overpaid 39.40.
WTW/PayFlex response: 1) Because we received a recurring claim
form our process is to enter a date span & lump sum with a monthly
contract amount. Based on how the system works, 2 months recurring
claims do not break out into individual claimlets. The claim was
processed correctly. 2) Yes. $39.40 was overpaid. The duplicate was
not caught. I’ve denied the $39.40. The claim is now correct.
Ref. No. 105 WTW/PayFlex claim no.
NOT charged in statistical calculation. Note to client for information only.
Charge of 33.03 DOS 1/26/17 was reimbursed. Only documentation is
receipt of payment which does not list patient, DOS or type of service.
Shouldn’t we have denied this charge for more information?
WTW/PayFlex response: Yes, the $33.03 should have been denied for
more information.
Ref. No. 121 WTW/PayFlex claim no.
Over/Underpayment - $0.00
Per documentation:
5/17/17, 5/22/17, 5/30/17, 6/5/17, 6/9/17, 6/12/17, 6/16/17, 6/26/17
$35 x 8 days = $280.00, paid $133.62
7/31/17, 8/4/17, 8/11/17, 10/9/17, 10/16/17, 10/23/17, 11/3/17
$35 x 7 days = 245.00, paid $391.38
1) I understand why the dates of service were split between the plan years,
but please explain how the dollar amounts of $133.62 and $391.38 were
determined.
2) Should each DOS have been split out separately to allow for possible
dup editing?
WTW/PayFlex response: 1) The system logic prorates based on the
number of days being claimed in each plan year. 2) Our process is that we
enter itemized statements as one line using a date span & lump sum.
HCA Note: In a further discussion with WTW/PayFlex it was determined
that this claim should have been manually split versus allowing the system
to do it.
HCA 10/18 Page 18 St. NV. PEBP/WTW/PayFlex
Ref. No. 155 WTW/PayFlex claim no.
NOT charged in statistical calculation. Note to client for information only.
Claim is for RX paid 7.18 on 12/19/17. Contributions in system reflect
active (168.00 per mo.) through 2/1/2018. Appears contributions were
adjusted on 2/1/18 retro to 11/1/17 causing overpayments (360.49)
1) Please explain what happened for cause to adjust contribution back
to 11/1/17.
2) Please explain what processes have been applied for collection of
these overpayments.
WTW/PayFlex response: 1) On 1/27/18 Via Benefits received notice that
this member disenrolled effective 10/31/17. This was sent over to
Payflex via file on 2/1/18 and the account end date was changed. Claims
that had previously paid were then denied. 2) A denied EOP is sent out
when the claims are initially denied. For the next 3 months they will be
sent an additional denied EOPs asking for repayment due to the account
being in an overpaid status.
Ref. No. 166 WTW/PayFlex claim no.
NOT charged in statistical calculation. Note to client for information only.
Claim is premium request for month of 2/1/18. Member requested for
DOS 1/1//2018 to 12/31/2018 Med B at 118.00/mo. Member incorrectly
requested on a Reimbursement Request for versus Recurring form.
EOP displays that “the service must have been provided before you
submit for reimbursement. You may submit the claim for the expense
after service has been provided.”
The EOP does not instruct the member that they could submit w/the
correct docs & form. Can this be added into the EOP in this type of
case or a reach out conducted?
WTW/PayFlex response: Claims is intake only. We will take under
advisement changing the verbiage of the remark code used.

HCA 10/18 Page 19 St. NV. PEBP/WTW/PayFlex
Ref. No. 179 WTW/PayFlex claim no.
Underpayment - $114.00
Recurring premium for $114/mo. for 1/1/18-12/1/18 (Note: came in on a
Reimbursement Request form w/no proof of payment just SS letter
showing 114.00 will be deducted each month)
1) Charge for DOS 6/1/18 not paid but charges for 7/1/18-12/31/18,
which were originally denied on 2/5/18, have been paid on 6/29/18 –
$684.00 clm #xxxxxx. Why were these months (July-Dec) paid
before the June DOS?
NOT charged in statistical calculation. Note to client for information only.
3) Why was Aug-Dec paid before they had been incurred?
WTW/PayFlex response: 1) This is not a recurring claim, it’s a standard
claim. So the examiner entered 12 lines. Jul-Dec auto denied because
that plan year was not yet set up. June appears to be stuck in the system.
I can see that it’s going to pend pay but keeps going back to awaiting
contribution. We will submit a ticket to have the claim unstuck so it will
pay when the next deposit comes in.
Ref. No. 187 WTW/PayFlex claim no.
NOT charged in statistical calculation. Note to client for information only.
Clm xxxxxx for same service as audited claim. Adjudicated on 1/16/18
and denied for additional information. Since audited claim was already
in the system & paid shouldn’t this claim (xxxxxx) have been denied as
previously received & paid?
WTW/PayFlex response: This was processed prior to our Realtime
duplicate logic. So at that time the examiner would not have known there
was a duplicate claim out there & would have approved/denied solely on
the documentation received.
Ref. No. 200 WTW/PayFlex claim no.
NOT charged in statistical calculation. Note to client for information only.
Part of documentation for audited claim is claim ID xxxxxx for DOS
10/24/17 paying 109.80 for dental charges requested through Express
claim. Documentation received shows primary insurance payment but
no discounting information.
Shouldn’t we have denied this service requesting EOB from dental
insurance?
WTW/PayFlex response: Our policy is to allow itemized statements if they
have the required information and if insurance is indicated & we see the
insurance paid. If there were any insurance adjustments they should be
reflected on the statement as well.

HCA 10/18 Page 20 St. NV. PEBP/WTW/PayFlex
Ref. No. 218 WTW/PayFlex claim no.
Overpayment -$550.00
Member requested reimbursement for $550.00 paid on outpatient
services for DOS 11/27/17, 11/28/17 & 12/12/17 provider Renown
Health from Senior Care Plus. Billing for these DOSs reflect a patient
payment for $550.00 on 11/28/17. Receipt for the payment displays
date of 11/28/17.
Audited claim received on 02/04/18 & paid $550.00
2nd claim received on 12/5/17 denied for additional info but has DOS of
11/27/17 recorded & requested 550.00
3rd claim received on 12/14/17 denied for additional info but has DOS of
11/20/17 recorded & requested 550.00
1) Shouldn’t the service dates/span be utilized versus the payment date so
system can detect duplicate payments, etc.?
2) Paid on Renown Hospital itemization received however appears to have
insufficient data for payment. Shouldn’t Senior Care Plus EOB have been
obtained?
WTW/PayFlex response: 1) Yes. This should have been date span
11/28-12/12. 2) Yes. This should have been denied for an EOB.
Ref. No. 220 WTW/PayFlex claim no.
NOT charged in statistical calculation. Note to client for information only.
Claim is for Medicare Part D, DOS 1/1/18
System reflects two claims each month for Medicare Part D all for this
member. One reflects 89.80/mo. eligible & the other requested $0
reimbursed $0.
Please explain why this member has 2 entries for the entire file history.
No spouse, etc.
WTW/PayFlex response: The first file came to us for January on 2/8/18
as $0.00 from the carrier. Then on 3/7/18 a file came over with both
January & February’s premiums of $89.80.

HCA 10/18 Page 21 St. NV. PEBP/WTW/PayFlex
Ref. No. 241 WTW/PayFlex claim no.
Overpayment - $2.50
Per member’s Reimbursement Request form: “out-of-pocket drug costs
643.68”
Per documentation: out of pocket Lantus 74.75
Nexium 108.63
Victoza 187.30
Xarelto 273.00
643.68
1) Audited claim for Lisinopril DOS 8/23/17 for $2.50 which is not one
of the requested reimbursements. Overpaid $2.50
NOT charged in statistical calculation. Note to client for information only.
2) We processed & paid $755.22 total for request which is the total of the
patient prescription record. Shouldn’t we have just paid the member’s
requested amount of $643.68?
WTW/PayFlex response: 1) Agree. The $2.50 was not requested & should
not have been paid. 2) We should have only keyed and allowed the
requested amount of $643.68.
Ref. No. 254 WTW/PayFlex claim no.
Overpayment - $38.89 (Disputed claim by WTW/PayFlex)
Service coded as premium medical & paid 3/7/18. Per member
reimbursement for premium is for dental. Per history review dental
premium is TPD and 38.89 was paid on claim ID xxxxxx paid on 2/5/18.
Appears audited claim is dup payment.
WTW/PayFlex response: We enter the type of premium based on what
is listed on our documentation. This states it’s a medical plan so that is
what we used. PEBP might want to consider adjusting the wording on
the EFT statements to reflect the correct type of premium. We processed
correctly based on what is on the document. The duplicate would not
have been caught due to how the premium type was reflected on the EFT
statement.
WTW/PayFlex additional response: PayFlex does not agree with error.
EFT statement provided stated it was a medical premium and that is what
was keyed by PayFlex.
WTW/PayFlex additional response received 01 Oct 2018: As a further note
to this. PayFlex adjudicates based on documentation provided, not the
claims form.
HCA Note: The PEBP electronic fund transfer (EFT) notice does state
medical plan. At the minimum this claim should have been questioned
due to documentation not matching the member’s reimbursement form.

HCA 10/18 Page 22 St. NV. PEBP/WTW/PayFlex
Ref. No. 264 WTW/PayFlex claim no.
NOT charged in statistical calculation. Note to client for information only.
Audited claim is TPD for medical premium Anthem BC/BS of Missouri
paying 134.01 on 3/9/18.
Claim ID xxxxxx also for medical premium DOS 2/1/18 came in by
WEB & we paid 134.01 on 3/12/18.
Shouldn’t claim ID xxxxxx have been denied as a duplicate?
WTW/PayFlex response: Yes the web claim should have caught as a
duplicate & denied.
Ref. No. 266 WTW/PayFlex claim no.
NOT charged in statistical calculation. Note to client for information only.
Claim ID xxxxxx for DOS 12/3/17 denied 16.66 and claim ID xxxxxx for
DOS 1/3/18 denied 16.53 both for “amount to the provider is either not
shown or not clear.”
Please see documentation for these 2 DOS. On the right-hand side to
right of patient name it clearly shows how much patient owes.
Shouldn’t we have paid these 2 DOS from this documentation?
(Note: appears both these services have subsequently been paid)
WTW/PayFlex response: Yes I believe so. Even though the amount is
cut off we could’ve allowed based on the patient owes amount.
Ref. No. 267 WTW/PayFlex claim no.
Over/Underpayment - $0.00
Service input as one RX for DOS 2/19/18 for $111.61.
Per documentation this is actually 2 RXs – one for DOS 2/19/18 for
$11.61 and one for DOS 2/13/18 for $100.00.
Shouldn’t these have been input on 2 separate lines?
WTW/PayFlex response: Yes. These should have been split into 2
separate lines & two different dates.
Ref. No. 268 WTW/PayFlex claim no.
NOT charged in statistical calculation. Note to client for information only.
Audited claim for medical premium 2 mos. x 20.25 each mo.
Claim ID xxxxxx same DOS & requested & paid of 40.50 but shows
as dental premium submitted via USP received 3/8/18 paid 3/21/18.
Could this possibly be a dup to the audited claim?
WTW/PayFlex response: Yes it appears to be a duplicate. The bias claim
has a different premium expense type so it would not have caught. This
is due to how the member submitted. One claim form says medical and
one says dental.

HCA 10/18 Page 23 St. NV. PEBP/WTW/PayFlex
Ref. No. 276 WTW/PayFlex claim no.
NOT charged in statistical calculation. Note to client for information only.
Claim documents include 1) a bill from Southwest Medical with bill date
of 2/14/18. 2) copy of member’s check. Documents provided do not
include service, date of service or any type of payment received by the
provider. Shouldn’t these docs be received from member so service, DOS,
etc. can be entered into system correctly?
Note: Express Claim form does request these items plus amount charged.
WTW/PayFlex response: This was processed correctly based on our copay
rule (page 12 of claims manual). Copay definition: patient liability
amounts that are whole dollar amounts in increments of $5 up to $50 at
a medical facility or doctor’s office. Type of service is not required for
amounts that fall within our copay definition.
Ref. No. 285 WTW/PayFlex claim no.
NOT charged in statistical calculation. Note to client for information only.
This member submitted claim & EOB from BC/BS of TX for inpatient
stay charged 32,398.67 with 1340.00 covered expenses. EOB reflects
1340.00 applied to 2018 deductible. File reflects no member payment
of the 1340.00 to any party.
Should documentation be received for member payment before
reimbursement(s) are made?
WTW/PayFlex response: Proof of payment is not required for medical
claims. We just need to see that they have been incurred, they are
eligible and that the member owed that liability.
Ref. No. 287 WTW/PayFlex claim no.
Over/Underpayment - $0.00 (Disputed claim by WTW/PayFlex)
This claim is for three (3) items:
1) set of 12 filters 6.67
2) full face headgear 30.85
3) replacement chamber for humid 19.50
Should these three items have been entered into the system separately
versus all together so the system could identify any duplicates if the
member were to submit claim differently?
Note: Member submitted reimbursement form with each item separate
WTW/PayFlex response: Our current process is to enter by receipt so
We did enter this correctly. With our new process we will enter separately.
WTW/PayFlex additional response: PayFlex does not agree to the error.
PayFlex entered based on our current process as noted.
HCA note: It is our opinion that claims such as these should be entered as
the prescription drug claims, each item listed separately. By entering these
as one entry, the system cannot properly identify possible duplicates if the
participant resubmits partial or different number of items on another
request.

HCA 10/18 Page 24 St. NV. PEBP/WTW/PayFlex
Ref. No. 295 WTW/PayFlex claim no.
Over/Underpayment - $0.00
Claim is for TPD premium of $737.22. DOS in system reflects for DOS
4/1/18-4/1/18.
Should it be in system w/DOS 4/1/18-6/30/18 versus 4/1-4/1/18 to allow
system to detect duplicate or broken into 3 month periods?
Note: premium must be for 3 month periods as reimbursement of 737.22
conducted in 1/2018, 4/2018, 7/2018, 7/17 & 10/17
WTW/PayFlex response: We have confirmed this is a quarterly premium.
The system is not currently designed to injest end dates from TPD files.
It was designed to recognize individual months & that is how the file is
supposed to come over but this carrier is not breaking out the months.
Ref. No. 306 WTW/PayFlex claim no.
NOT charged in statistical calculation. Note to client for information only.
Per history review from DOS 12/1/16 to 2/1/18 the TPD for MEDD
premium from AARP has come in twice. First with a request of $0.00
then later with an amount for actual premium.
Was this a system glitch or a problem on the TPD end with the incoming
file?
WTW/PayFlex response: TPDs are pass through & not manipulated on our
end or Via benefits. This is how it is received by the carrier.
Ref. No. 334 WTW/PayFlex claim no.
NOT charged in statistical calculation. Note to client for information only.
Claim xxxxxx contains what appears to be 2 copays – documentation are
receipts of payment.
Copay of $45 DOS 4/19/18 was paid but copay of $90 was denied for
“itemized bill from the provider if expense is not covered under insurance
plan.” Should the $45 copay have been denied the same way?
WTW/PayFlex response: The $45 was approved based on our copay rule
(pg. 34 of manual). The $90 does not fall within the parameters of our
copay rule ($5-$50 in increments of 45) so it was denied appropriately
for more information.
Ref. No. 360 WTW/PayFlex claim no.
Underpayment - $50.00
Member requested reimbursement of $50.00 copay paid
Provided Steinberg Diag Med Imaging billing reflecting name, services,
DOS, payment of $50.00 etc. Request was denied as “this expense is not
eligible for reimbursement and has been denied. Your plan does not
allow for reimbursement of this type of expense.”
Please explain why denied as this appears as an eligible expense.
WTW/PayFlex response: The examiner chose the wrong expense type
so it system denied. I have adjusted & approved the claim.

HCA 10/18 Page 25 St. NV. PEBP/WTW/PayFlex
Ref. No. 374 WTW/PayFlex claim no.
Overpayment - $1,996.68
Claim #xxxxxx
1) Member requested $1850.56 for DOS 6/30/17-5/30/18
Appears to be premiums from 7/1/17-5/1/18. Per documentation
premiums are $166.69 for Jul 2017 through April 2018 and then premium
is $186.66.
Calculation for member request of 1850.56 would be:
10 months x 166.39 = 1663.90
1 month x 186.66 = 186.66
1850.56
Why did we pay 1996.68?
2) Claim #xxxxxx received same day for pharm & same premium request
was also paid. Claim Id xxxxxx did pay the correct amount of 1850.56
for premium. Appears claim ID xxxxxx (audited claim) is a duplicate
payment to claim ID xxxxxx.
WTW/PayFlex response: 1) I believe she took the 166.39 x 12 months
which is incorrect. 2) Yes this is a duplicate. We will deny the claim &
reach out to the member.
Ref. No. 391 WTW/PayFlex claim no.
Over/Underpayment - $0.00
DOS entered as 6/8/18. However there were 2 RXs for 6/10/18. One RX
Was entered with the correct DOS – this one on audited claim was not.
WTW/PayFlex response: Agree to date of service error. It should be
6/10/18.

HCA 10/18 Page 26 St. NV. PEBP/WTW/PayFlex
EXHIBIT A
Understanding Your Explanation of Payment (EOP) Statements

HCA 10/18 Page 27 St. NV. PEBP/WTW/PayFlex


7. 7. Presentation on PEBP’s Fiscal Year 2020/2021 Agency Request
Budget. (Information/Discussion) (Celestena Glover, Chief Financial Officer)


AGENDA ITEM
Action Item X Information Only
Date: November 29, 2018
Item Number: VII
Title: Agency Request Budget – Fiscal Year 2020-2021
Summary This report addresses the Agency Request Budget for the 2019-2021 Biennium (Fiscal Years 2020 and 2021) to include:
1. Budget Overview 2. Enrollment Projections 3. Inflation Assumptions 4. Reserves 5. State Subsidies 6. Enhancement Decision Units
Report PEBP’s budget request was submitted to the Budget Office in the Governor’s Finance Office on August 31, 2018 and totaled $1.1 billion for Fiscal Years 2020 and 2021. This represents a 15% increase from the Fiscal Years 2018 and 2019 legislatively approved budget of $953 million. The increase is a result of a projected increase in enrollment, medical inflation assumptions, and adjustments to the required reserve levels to meet the requirement of the Board’s Duties Policies and Procedures to maintain fully funded reserves.

Agency Request Budget November 29, 2018 Page 2 Budget Overview PEBP’s budget request includes the addition of $1 per year of service per month in each year of the biennium ($13 in Fiscal Year 2020 and $14 in Fiscal Year 2021) for retirees on the Medicare Exchange, the addition of one full-time legal counsel position, a 5% salary increase for executive staff and reclassifying the Financial Analyst position to an Administrative Services Officer 2. The detail for each of these requests is included in the report below. Enrollment Projections The table below represents the enrollment projections used to develop revenue and expenditure requirements. Enrollment in Fiscal Year 2018 is based on actuals, while Fiscal Years 2019 through 2021 are based on projections as of the July 1, 2018 headcount report.
Enrollment Actual Projected Agency Request FY 2018 FY 2019 FY 2020 FY 2021
State Employees 26.078 26,257 26,272 26,210 Non-Medicare Retirees 4,034 4.041 4,083 4,153 Medicare Retirees 6,739 6,295 7,150 7,519 Total State 36,852 36,593 37,504 37,882
Non-State Employees 8 8 8 8 Non-Medicare Retirees 5,221 5,142 5,373 5,457 Total Non-State 6,710 6,386 6,431 6,343 Total 43,562 42,979 43,936 44,225 Total Enrollment Growth -1.36% 2.18% 0.65%
Medical Inflation Medical inflation assumptions are based on actuarial analysis and includes expected cost per service and utilization of plan benefits for the Consumer Driven Health Plan (CDHP) and the PEBP Premier Exclusive Provider Organization (EPO), both of which are self-funded plans. Inflation assumptions for the Health Maintenance Organization (HMO) plan was held at 6% as provided for the self-funded plans. Plan experience will continue to be analyzed through March of 2019 when final Plan Year 2020 rates are approved. Finally, inflation assumptions for the various Medicare plan options was provided by Willis Towers Watson. Medical inflation assumptions are shown in the table below.

Agency Request Budget November 29, 2018 Page 3
Self-Funded Plans CDHP/EPO/Dental FY 2020 FY 2021
Medical 6% 6% Rx 8% 8% Dental 3% 3%
Fully-Insured Products FY 2020 FY 2021 HPN (HMO-South) 6% 6% Life and Long Term Disability Insurance 0% 0%
Medicare Plans FY 2020 FY 2021 Medicare Advantage 3% - 5% 3% -5% Medicap Plans 1% - 4% 1% - 4% Prescription Drug Plans 4% - 6% 4% - 6%
Reserves The Agency Request Budget includes reserves for the Health Reimbursement Arrangement account balances, Incurred but Not Reported (IBNR) claims payments for both the CDHP and EPO plans as well as a Catastrophic (CAT) reserve to ensure the plan’s solvency. The IBNR and CAT reserves were determined through actuarial analysis utilizing a 95% probability that they will be sufficient to meet the financial obligations of the plan. Reserve levels included in the Agency Request Budget are as follows:
• Incurred but Not Reported o FY 2020 - $54,400,000 o FY 2021 - $57,500,000
• Catastrophic Reserves o FY 2020 - $42,800,000 o FY 2021 - $45,800,000
• Health Reimbursement Arrangement o FY2020 - $35,435,819 o FY2021 - $37,207,610
Maintenance Decision Units Maintenance decision units make adjustments to the base budget and includes costs for enrollment projections, medical inflation assumptions, and required reserve levels based on the projections and assumptions listed in the tables above. The total costs for the maintenance decision units included in the Agency Requested Budget can be seen in the table below:

Agency Request Budget November 29, 2018 Page 4
Maintenance Decision Units FY 2020 FY 2021
M100 – Statewide Inflation $42,877 $42,877 M101 – Medical/Rx/Dental Inflation $27,973,681 $46,057,383 M102 – IBNR/Catastrophic/HRA Reserves ($17,193,750) ($3,092,626) M103 – Medicare HRA Increase $6,060,003 $8,615,301 M150 – Adjustments to the Base Budget ($67,737,084) ($67,321,279) M200 – State Enrollment Changes $66,474,177 $70,350,608 M201 – Non-State Enrollment Changes ($4,054,185) ($7,275,788) M202 – Medicare Retiree Enrollment Changes $1,839,018 $3,429,989
Total Maintenance Decision Units $13.4 M $50.8 M Subsidy The State subsidy is the employer contributions paid toward the overall plan rates on behalf of the employees and retirees and include the assessments deposited into Active Employee Group Insurance (AEGIS) and the Retired Employee Group Insurance (REGI) budget accounts. The tables below reflect the per employee/retiree request as well as the State subsidy total cost.
State Subsidy Per Employee/Retiree
Per Month
Legislatively Approved Agency Requested Budget
FY 2018 FY 2019 FY 2020 FY 2021
Employee $743.00 $740.92 $772.00 $814.00
Pre-Medicare Retiree $445.03 $451.23 $472.00 $492.00
Medicare HRA $180.00 $180.00 $195.00 $210.00 Note: Retiree subsidies are based on a 15 year retiree. An additional $1.00 per month per year of service has been included in each year of the biennium for the Medicare HRA.
State Subsidy Revenue Total
Actuals Agency Requested Budget FY 2018 FY 2019 FY 2020 FY 2021
State Total AEGIS $231,022,690 $239,027,092 $234,302,054 $257,083,423
$8,004,402 ($4,725,038) $22,781,369
% Change 3.35% -2.02% 8.86%
Total REGI $39,710,152 $43,045,079 $52,008,480 $59,314,017 $3,334,927 $8,963,401 $7,305,537
% Change 7.75% 17.23% 12.32%

Agency Request Budget November 29, 2018 Page 5 The total increase in budgeted subsidy for employees and retirees is $45.65 million more for the FY 2020-2021 biennium over the FY 2018-2019 biennium. This increase will assist PEBP with absorbing increased population and inflation (see below) of healthcare. Enhancement Decision Units Enhancement decision units are used to request additional funding for new projects and programs and the expansion or reduction of existing projects and programs. The Agency Requested Budget includes the following:
1. E225 – Addition of PEBP full time General Counsel a. This requests funds one Legal Counsel Position. This position will be in
the unclassified service of the state. PEBP is requesting a full-time legal counsel position in accordance with NRS 287.043(4): "The Board may engage the services of an attorney who specializes in health plans and health care law as necessary to assist in carrying out the Program." PEBP relies heavily on the Attorney General's office for services in response to litigation, requests for information, and personnel matters. PEBP currently shares the assigned Deputy Attorney General with several other agencies and believes it is critical to have a full-time counsel available to meet our needs. PEBP has met with members of the Attorney General's office to discuss the viability of assigning a Deputy Attorney General position to PEBP fulltime. Upon conclusion of those discussions PEBP decided a new unclassified position would be most appropriate.
2. E815 – Unclassified Staff Pay Increase
a. PEBP reported to the Board at its meeting on March 22, 2018 the disparity in executive staff pay and the greater responsibilities and complexity of their duties. PEBP compared the salaries of executive staff to other similar positions within state service and specifically reviewed positions of the Department of Health and Human Services, Directors Office (DHHS) and the Division of Health Care Financing and Policy (DHCFP). In the review it was determined that the pay for similar positions at PEBP are between 10 and 15% less than those at DHHS and DHCFP. PEBP's request includes a 5% increase to begin closing the gap in pay.
3. E816 – Reclassify Financial Analyst to an Administrative Services Officer 2
(ASO2) a. PEBP's Financial Analyst position was established in July 2003 in an
attempt to meet the need for in-house actuarial services. Over time this position has become the support role to the Chief Financial Officer (CFO) with an opportunity to succeed the CFO when the position becomes vacant. To allow for appropriate succession planning and opportunity, PEBP is requesting the reclassification of the Financial Analyst position to an ASO2, Grade 39. Many qualified staff are reluctant to leave a

Agency Request Budget November 29, 2018 Page 6
relatively secure position with the classified service where they may receive step increases as well as overtime pay for a salaried position that is perceived to be less secure. Reclassifying this position would provide PEBP additional recruitment and retention opportunities.
4. E710 – Equipment Replacement a. This request replaces computer hardware and associated software per the
EITS's recommended replacement schedule.
Enhancement Decision Units FY 2020 FY 2021 E225 – Full Time General Counsel $0 ($139,729) E815 – Unclassified Staff Pay Increase $0 ($37,356) E816 – Reclassify Financial Analyst to ASO2 $0 $24,593 E710 – Equipment Replacement $169,648 $164,694
Total Enhancement Decision Units $169,648 $12,202 Recommendations None.

8. 8. Executive Officer Report. (Damon Haycock, Executive Officer)
(Information/Discussion)


BRIAN SANDOVAL Governor
PATRICK CATES Board Chairman
DAMON HAYCOCK Executive Officer
STATE OF NEVADA
PUBLIC EMPLOYEES’ BENEFITS PROGRAM 901 S. Stewart Street, Suite 1001 | Carson City, Nevada 89701 Telephone 775-684-7000 | 1-800-326-5496 | Fax 775-684-7028
www.pebp.state.nv.us
AGENDA ITEM Action Item X Information Only
Date: November 29, 2018
Item Number: VIII
Title: Executive Officer Report
SUMMARY This report will provide the Board, participants, public, and other stakeholders information on the overall activities of PEBP.
REPORT PLAN YEAR 2019 1ST QUARTER CUSTOMER SERVICE STATISTICS PEBP provided a high level of customer service during the first quarter of Plan Year 2019. As seen below, call volume increased, walk-ins increased and emails significantly increased over the same period the previous year. PEBP attributes this increase to the new EPO plan that began July 1, 2018:
1st Quarter (July-Sept) PY19 PY18 Total Calls 11,645 10,848 Abandonment rate 1.3% 1.09% Average calls per day 187 168 Average Call Duration 5:18 4:09 Average Speed to Ans. :25 :15 Total Walk-ins 337 293 Total Emails 5534 3202
PEBP’s customer service statistics remain at or below industry standards.

Executive Officer Report July 26, 2018 Page 2 HEALTHCARE BLUEBOOK UPDATE PEBP implemented Healthcare Bluebook, an online transparency vendor beginning July 1, 2018. As of November 15, 2018:
• 2,364 participants have taken the online tour • Just over 40,000 online searches have occurred • 31 members have received rewards checks ranging from $25 to $100 (totaling $1,375) in
areas across the state (both rural and urban), as well as out-of-state in Wyoming, Idaho, Arizona, and Florida
Healthcare Bluebook informed PEBP we have exceeded engagement beyond anything they have experienced with typical clients when launching the program. Through coordinated communication and their successful marketing strategy, coupled with the Board’s decision to incentivize the utilization of this transparency tool, members and the plan are already benefiting although early in the release of this program. MULTI-STATE COLLABORATION PEBP recently attended the annual Public Sector Healthcare Roundtable in Alexandria, VA. Nevada is a member and was given an opportunity to speak on a panel of experts addressing drug costs to 17 states as well as representatives from national insurance carriers, consultants, pharmacy benefits managers, third party administrators and healthcare providers. The day prior to the event the State and Local Government Benefits Association (SALGBA) held another pre-event roundtable at the same location providing states, systems of higher education, and local jurisdictions more opportunities to discuss topics from specialty drug cost containment, plan design, wellness incentives, transparency, and contracting best practices. During the events, PEBP met with the Executive Director of the National Academy for State Health Policy (NASHP) who became very interested in setting up a multi-state collaborative to leverage purchasing power for high cost specialty drugs. Multiple conversations with multiple states occurred and a planned exploratory call is being developed in the near future. PEBP will monitor the opportunities closely and provide the Board with updates as the states look to improve their contracting through coordination and collaboration. CONCLUSION PEBP continues to provide high quality and timely customer service to our members, prioritizing transparency and providing tools that make members better consumers. PEBP constantly looks for opportunities with other states and jurisdictions to negotiate the best agreements keeping costs down for the plan, the members, and the Nevada taxpayer.

9. 9. Discussion and possible action regarding Plan Year 2020 through
2021 Preferred Provider Organization (PPO) network options and the potential to (1) continue the current contract with Hometown Health Providers through 2021 or (2) issue a no-fault contract termination and join the State on a solicitation for PPO networks. (Damon Haycock, Executive Officer) (For Possible Action)

BRIAN SANDOVAL Governor
PATRICK CATES Board Chairman
DAMON HAYCOCK Executive Officer
STATE OF NEVADA
PUBLIC EMPLOYEES’ BENEFITS PROGRAM 901 S. Stewart Street, Suite 1001 | Carson City, Nevada 89701 Telephone 775-684-7000 | 1-800-326-5496 | Fax 775-684-7028
www.pebp.state.nv.us
AGENDA ITEM X Action Item Information Only
Date: November 29, 2018
Item Number: IX
Title: PPO Network Options Report
SUMMARY This report will provide the Board multiple options to address the current and future Preferred Provider Organization (PPO) networks for both the statewide Consumer Driven Health Plan (CDHP) and PEBP’s Premier Exclusive Provider Organization (EPO) plan.
REPORT CURRENT CONTRACTED PPO NETWORKS PEBP contracts with two PPO networks today:
1. Aetna – nationwide network 2. Hometown Health Providers (HHP)/Sierra Health Options (SHO) – in-state regional joint
network The nationwide PPO network has been managed by HealthSCOPE Benefits since 2012, originally with a different network and changed per Board approval to Aetna in 2016 as part of a cost saving activity. The contract is set to expire in 2022 and recently was amended to include the EPO population in June. At this time, PEBP is recommending no change to this contract. The statewide PPO contract is currently scheduled to expire in 2021 with the most recent amendment occurring after public negotiation over hospital exclusivity and EPO member inclusion in April. Additionally, in May, HHP testified to the Board they would terminate this agreement ending June 30, 2019 (2 years early) to allow PEBP to develop a solicitation for network services for Plan Year 2020 (beginning July 1, 2019) that could disclude their exclusivity requirement. PEBP never received a termination notice in accordance with the requirements outlined in the contract (public testimony was not a valid contract termination clause) and therefore did not

PPO Network Options Report November 29, 2018 Page 2 develop a solicitation awaiting the official notice. At the September Board meeting, HHP testified to the Board they would no longer issue a termination and wanted to keep the current contract in place. REVISIT PPO NETWORK NEGOTIATIONS When PEBP heard HHP testify they were terminating the partnership in 2019, PEBP reached out to the other joint partner on the PPO network contract (SHO) to determine if they too wanted to end the relationship and agreement to provide services to PEBP members next year. SHO informed PEBP they were not privy to the termination decision and still wanted to partner with PEBP on these services. PEBP was also approached by other networks in the state asking when/if a solicitation will be coming. PEBP patiently waited for a termination notice that never came. Immediately following HHP’s change in position announced at the September Board meeting, PEBP reached out to HHP and setup a meeting to discuss the potential to move forward with HHP as the northern and rural Nevada partner within the joint PPO Network contract. PEBP shared concerns about the inconsistency of HHP’s position over the last year and reiterated the desire to provide an open competitive fair marketplace for PPO network services. PEBP asked HHP to consider the following:
1. Include the Saint Mary’s agreement PEBP negotiated already as part of HHP’s network for PEBP members. PEBP recognizes HHP wants to manage all providers associated with services provided and precedence set by PEBP to ne0gotiate and implement outside of the network has been accused of weakening the integrity of their network.
2. Honor cost controls with Renown. The original amendment in April included acceptance of Renown’s exclusivity with the caveat costs would remain flat for PEBP this current plan year and cap at 2% each year for the next two plan years (0%/2%/2%). Recognizing the loss of the exclusivity, PEBP offered 4% increases over the next two years (0% current /4% /4%) and a promise to not actively steer services away from Renown.
3. Ask Renown to match Saint Mary’s reimbursement levels for surgical implants. Saint Mary’s agreed to reimbursement at cost where Renown (and other hospitals) include a markup.
In the meantime, PEBP reached out to Saint Mary’s and asked them if they would honor the pilot program reimbursement model and allow their organization to join the HHP network next plan year. The agreement would ultimately be between HHP and Saint Mary’s, but the negotiated terms for PEBP would stand. Although Saint Mary’s expressed concern with partnering with their direct competitor in the region, they informed PEBP they would be willing to if safeguards were put in place to ensure open competition. Unfortunately, HHP came back to PEBP and informed us they were unwilling to make any changes to the existing contract and would not allow Saint Mary’s into their network.

PPO Network Options Report November 29, 2018 Page 3 IN-STATE PPO NETWORK OPTIONS Option 1: Stay the Course The PEBP Board approved an amendment in April to retain Renown exclusivity, implement cost controls on Renown, and include the EPO population on the existing statewide PPO network contract. PEBP believes this amendment was necessary to ensure thousands of EPO members had in-network services beginning July 1, 2018. PEBP also believes cost controls on Renown, PEBP’s single largest expense across the state, provides a safety net to increasing costs over the next two years. However, there is no guarantee Renown will allow cost controls beyond the current contract amendment. PEBP is also very concerned that at any time, HHP could return to the Board and testify they are canceling the contract again. Option 2: Join in the State Solicitation for PPO Network Services The State of Nevada, Department of Administration, Purchasing Division recently released and awarded contracts on a statewide healthcare provider solicitation. This solicitation was designed to allow any state (or local) government entity the ability to work directly with healthcare providers on direct negotiated contracts for the good of the state. Maximizing purchasing power (larger populations) and reducing redundant solicitations (previously every agency running a separate solicitation), this paradigm shift should increase efficiency, reduce workload, reduce costs and expedite the process to contract for care. Following this process, Purchasing has developed a solicitation for PPO network services statewide for all agencies. Currently, PEBP is joined by the Department of Health and Human Services and Department of Corrections in the need for contracted networks across the state and this solicitation will provide all state agencies the ability to assess, negotiate, and maximize cost savings for all populations. Furthermore, there are planned market checks at regular intervals to ensure optimal agreements remain and suboptimal agreements are replaced. PEBP’S RECOMMENDATION Because of the recent inconsistency and announcement to terminate a longstanding PPO network partnership mid contract, PEBP recommends the Board take Option 2 above. This means PEBP would issue HHP (and SHO) a no-fault termination notice a minimum of 180 days before June 30, 2019, negotiate with qualified networks as a result of Purchasing’s solicitation, and bring back a new contract for Board approval at the March 2019 Board meeting for implementation July 1, 2019.


10. 10. Discussion and possible action regarding the Morneau Shepell
Voluntary Benefits Platform and benefit selection for Plan Year 2020 offerings to members on the Consumer Driven Health Plan (CDHP), PEBP Premier Plan (EPO), southern Nevada Health Maintenance Organization plan (HPN), and Via Benefits (Medicare Exchange). Proposed benefits and providers include, but not limited to:
• Accident, Critical Illness, and Hospital Indemnity (Aflac, Allstate, MetLife, Reliance, The Standard);
• Identification (ID) Theft Protection (ID Watchdog, InfoArmor);
• Legal Plan Provisions (Nationwide LegalEASE, Hyatt Legal);
• Automobile, Home, and Renters Insurance (MetLife, Liberty Mutual, Travelers);
• Pet Insurance (ASPCA, Nationwide);• Vision Plan Services (VSP)
(Laura Rich, Operations Officer) (For Possible Action)

AGENDA ITEM X Action Item Information Only
Date:
November 29, 2018
Item Number: X
Title: Morneau Shepell Voluntary Benefits Platform Pilot Program and Benefits Selection Portal Update
SUMMARY This report will provide the Board, participants, public, and other stakeholders information on the Morneau Shepell Voluntary Benefits Platform and Benefits Selection Portal.
REPORT The contract amendment allowing Morneau Shepell to implement a voluntary benefits platform and upgraded benefits selection portal, approved by the Board in September was approved by the Board of Examiners on November 13, 2018. Morneau Sheppell has informed PEBP that both they and Corestream, have met the licensing requirements in 49 of the 50 states. VOLUNTARY BENEFITS At the September 27th board meeting, the Board was presented with several voluntary product offerings but was unable to take action on the specific agenda item. Attachment A provides a detailed breakdown of the products and pricing comparisons as presented at the September Board meeting. This updated version also includes a quoted premium for Hyatt Legal, which was not included in the version presented in September. The attachment also excludes Purchasing Power, which PEBP has tabled as we work through some concerns that were raised since initially presented. PEBP recommendations for each of the remaining products remain consistent with the previous recommendations:
Product PEBP Recommendation
Accident Plan Bundle AFLAC for Accident, Critical Illness and Hospital Indemnity Plans Critical Illness Plan
Hospital Indemnity Plan ID Theft Protection ID watchdog
STATE OF NEVADA
PUBLIC EMPLOYEES’ BENEFITS PROGRAM 901 S. Stewart Street, Suite 1001
Carson City, Nevada 89701 Telephone (775) 684-7000 (800) 326-5496
Fax (775) 684-7028 www.pebp.state.nv.us
PATRICK CATES Board Chairman
BRIAN SANDOVAL Governor
DAMON HAYCOCK Executive Officer

Voluntary Benefits and Benefits Selection Portal Update November 29, 2018 Page 2
Product PEBP Recommendation
Legal Plan Provisions Nationwide LegalEASE Auto, Home and Renters Insurance MetLife, Liberty Mutual and Travelers Pet Insurance ASPCA and Nationwide Voluntary Vision VSP Vision Services
VOLUNTARY DENTAL In response to member requests, PEBP has been working with Morneau Shepell and Corestream to introduce a potential “buy-up” dental option to be offered on the voluntary platform. Initial analysis concluded that a simple buy-up plan would not be beneficial as it would not provide members with any significant value. Members purchasing this type of product would be required to satisfy long waiting periods before many services would be covered. PEBP is currently working with Corestream to analyze several other options that may be available and there have been initial discussions with dental carriers that may be interested in offering expanded voluntary dental coverage. PEBP will continue to explore and analyze its options and hope to bring opportunities back to the Board in January. SUMMARY OF RECOMMENDATIONS
1. Approve AFLAC for Accident, Critical Illness and Hospital Indemnity Plans. 2. Approve ID Watchdog for ID Theft Protection 3. Approve Nationwide LegalEASE for Legal Plan 4. Approve both ASPCA and Nationwide for Pet Insurance 5. Approve VSP Vision Services for Voluntary Vision

Page 1 of 26
Attachment A

Page 2 of 26
Accident Plan
Plan Benefit or Provision Aflac Allstate MetLife Reliance Standard
On and Off Job Coverage 24 Hour 24 Hour 24 Hour 24 Hour 24 Hour
Situs State NV NV NV NV NV
Eligibility
Full time benefit eligible employees working at least 16
hours per week
Full time and/or permanent part-time Actively at Work W-
2 employees working 20 or more
hours per week
Full time benefit eligible associates
Full time benefit eligible employees
Full time benefit eligible associates
Spouse Eligible Eligible Eligible Eligible Eligible
Domestic Partner Eligible Eligible Eligible Eligible Eligible
Dependent Children up to age 26 up to age 26 up to age 26 up to age 26 up to age 26
HSA Compliant Yes Yes Yes Yes Yes
Claims Waiting Period None None None None None
Pre-Existing Conditions Limitation Waived Waived Waived Waived N/A
Portable Yes Yes Yes Yes Yes
Benefit Age Reduction None None 50% at age 70 None None

Page 3 of 26
Injuries
Fracture/Dislocation Schedule Fractures: up to
$8,000, Dislocations up to $6,000
up to $4,000 up to $6,000
Fractures: Up to $5,000,
Dislocations: Up to $3,200
up to $8,000
Burns - (2nd & 3rd degree) varies by type and severity of burn up to $20,000 up to $500 up to $20,000 up to $6,400 up to $20,000
Skin Graft (% of burn) up to $1,000 50% of burn benefit 50% of burn benefit 25% of burn benefit 50% of burn benefit
Concussion $350 $300 $300 $100 $300
Coma $10,000 $10,000 $10,000 $5,000 $15,000
Ruptured Disc up to $1000 $500 $1,000 $500 $1,000
Torn Knee Cartilage up to $1000 up to $500 up to $750 $300 up to $750
Lacerations $38-$600 $50 $50 - $600 $25 - $400 $75 - $500
Tendons/Ligaments/Rotator Cuff up to $1000 up to $500 up to $1,000 $50 up to $1,000
Dental Work $50-$200 $100 $50 - $200 $50-$150 $100-$200
Eye Injuries $300 $100 $300 $100-$200 $300
Accidental Death, Dismemberment
Accidental Death $50,000 $40,000 $50,000 $25,000 $50,000
Accidental Death - Common Carrier $150,000 $100,000 $150,000 $25,000 $200,000

Page 4 of 26
Dismemberment $8,750 - $17,500 $40,000 $10,000 $12,500 $1,000 - $15,000
Catastrophic Dismemberment $50,000 $40,000 $50,000 $25,000 $50,000
Paralysis $7,500-$12,500 $7,500-$15,000 $25,000 - $50,000 up to $10,000 $15,000 - $50,000
Medical Services and Treatment
Ambulance Ground: $300 Ground: $200 Ground: $300 Ground: $150 Ground: $300
Air: $1,000 Air: $600 Air: $1,000 Air: $500 Air: $1,000
Emergency Care (Physician Office or Urgent Care)
$100-$150 Physician Office /
Urgent Care up to $200 $100 $50 $100
Emergency Room Treatment $200-$250 $400 $200 $150 $200
CT or MRI $200 $50 $200 $100 $200
Accident Follow-Up Visit $75 $50 $75 $50 $75
Therapy Services (per day) $25 $30 Physical/ Occupational/ Speech: $25 $25 $50
Prosthesis (1 device or 2 or more devices) $2,000 $500 or $1,000 $750 or $1,500 $500 or $1,000 $1000; $2000
Medical Appliances $30-$300 $125 $100 - $200 $100 $200
Blood & Plasma $35-$400 $300 $400 $200 $400
Outpatient Surgery $400 up to $1,000 $200 up to $1,000 $500
Hospital Coverage
Rehabilitation (per day) $200/day $100/day $200/day $50/day $200/day

Page 5 of 26
Hospital Confinement (per day) $200/day $200/day $200/day $200/day $200/day
Intensive Care (per day) $400/day $400/day $400/day $400/day $400/day
Hospital Admission Benefit $1,250 $1,000 $1,000 or $2,000 for ICU
$500 or $1,000 for ICU
$1,000 or $2,000 for ICU
Family Lodging (per day) $200/day $100/day None 100/day $175/day
Monthly Premium
Employee $11.49 $9.66 $11.53 $12.49 $18.42
Employee & Spouse $17.71 $16.70 $22.11 $18.20 $28.68
Employee & Child(ren) $18.52 $21.24 $23.75 $24.81 $36.03
Employee & Family $24.74 $25.86 $29.47 $31.21 $56.06

Page 6 of 26
Critical Illness Plan
Plan Benefit or Provision Aflac Allstate MetLife Reliance Standard
Situs State NV NV NV NV NV
Guaranteed Issue Benefit Amount up to $30,000 up to $30,000 up to $30,000 up to $30,000 up to $30,000
Pre-Existing Conditions Clause Waived Waived Waived 6 month look back Waived
Portable Yes Yes Yes Yes Yes
Age Reduction None None None None None
Waiting Period None None None None None
Eligibility
Full time benefit eligible employees working at least 16
hours per week
Full time and/or permanent part-time
Actively at Work W-2 employees working 20 or more hours per week
Full time benefit eligible associates
Full time benefit eligible associates
Full time benefit eligible associates
Spouse Coverage 50% 50% 50% 100% 100%
Child(ren) Coverage 50% 50% 50% 25% 50%
Benefits
Heart Attack 100% 100% 100% 100% 100%
Heart Transplant 100% 100% 100% 100% 100%

Page 7 of 26
Stroke 100% 100% 100% 100% 100%
Coronary Artery By-Pass 50% 25% 100% 25% 25%
Major Organ Transplant 100% 100% 100% 100% 100%
End Stage Renal Failure 100% 100% 100% 100% 100%
Burns (3rd Degree or 50% coverage) N/A Not Covered N/A 100% Not covered
Coma N/A 100% N/A 100% 100%
Cancer 100% 100% 100% 100% 100%
Carcinoma in Situ 100% invasive, 25% non-invasive 25% 25% 25% 25%
Prostate Cancer 100%
Stage III or IV covered at 100%
Stage A, I or II covered at 25%
25% 100% life threatening, 25% in-situ Not covered
Skin Cancer $250 $250 per calendar year Not covered 100% life threatening, 25% in-situ Not covered
Advanced Alzheimer’s Disease 100% 100% 100% Not covered 100%
Recurrence Benefit 100% 100% 0% to 50% 100% 25%
Additional Standard Offering
Wellness $50 $50 $50 $50
Additional Included Riders/Benefits

Page 8 of 26
Additional Riders
Bone Marrow Transplant (Stem Cell Transplant) ; Sudden Cardiac
Arrest
Specified Chronic Illness Rider:Adrenal
Hypofunction (Addison's Disease):
50%*Arthritis: 50%*Huntington's Chorea: 50%*Lou Gehrig's Disease
(ALS): 50%*Multiple Sclerosis:
50%*Muscular Dystrophy:
50%*Osteomyelitis: 50%*Osteoporosis:
50%*Injury: 100%***Pays after 90 & 365 days of loss of ADLs due to Listed
Condition**Pays after 365 days of loss of ADLs due to Listed
Condition
23 Additional Conditions Occupational HIV, HEP,
ALS, MS
Monthly Premium Issue Age / Non-Tobacco
Issue Age / Non-Tobacco
Issue Age / Non-Tobacco
Attained Age / Non-Tobacco
Issue Age / Non-Tobacco
Employee $10,000 $10,000 $10,000 $10,000 $10,000
Age 30 $5.31 $9.03 $5.10 $6.40 $12.40
Age 40 $8.50 $18.01 $11.20 $11.90 $20.30
Age 50 $15.70 $31.75 $22.30 $27.20 $38.60
Employee & Spouse

Page 9 of 26
Age 30 $8.64 $14.41 $8.10 $12.80 $24.80
Age 40 $13.42 $28.12 $17.40 $23.80 $40.60
Age 50 $24.22 $49.03 $34.30 $54 $77.20
Employee & Child(ren)
Age 30 $5.31 $9.03 $6.60 $9.45 $12.40
Age 40 $8.50 $18.01 $12.70 $14.95 $20.30
Age 50 $15.70 $31.75 $23.80 $30.25 $38.60
Family
Age 30 $8.64 $14.41 $9.60 $16.30 $24.80
Age 40 $13.42 $28.12 $18.90 $26.85 $40.60
Age 50 $24.22 $49.03 $35.80 $57.45 $77.20

Page 10 of 26
Hospital Indemnity Plan
Plan Benefit or Provision Aflac Allstate MetLife Reliance Standard
Situs State NV NV NV NV NV
Eligibility Full time benefit eligible
employees working at least 16 hours per week
Full time and/or permanent part-time
Actively at Work W-2 employees working 20 or more hours per week
Full time benefit eligible associates
Full time benefit eligible associates
Full time benefit eligible associates
Spouse Eligible Eligible Eligible Eligible Eligible
Domestic Partner Eligible Eligible Eligible Eligible Eligible
Dependent Children up to age 26 up to age 26 up to age 26 up to 26 up to age 26
HSA Compliant Yes Yes Yes Yes Yes
Claims Waiting Period None 10-month Pregnancy Waiting Period None None None
Pre-Existing Conditions Limitation Waived Waived Waived Waived Waived
Portability Yes Yes Yes Yes Yes
Primary Benefits
Hospital Confinement $100 $100 $100 $100 $100
Hospital Admission $500 $1,000 $500 $500 $1,000

Page 11 of 26
Hospital Intensive Care - Admission $500 $1,000 $1,000 $500 $1,500
Hospital Intensive Care - Confinement $200 $100 $200 $100 $150
Pregnancy Covered (Normal & Complications)
Covered (Normal & Complications) - 10
Month Waiting Period
Covered (Normal & Complications)
Covered (Normal & Complications)
Covered (Normal & Complications)
Monthly Premium
Employee $11.78 $24.05 $7.89 $24.78 $13.64
Employee & Spouse $21.64 $71.11 $16.28 $52.29 $29.10
Employee & Child(ren) $17.92 $25.22 $13.02 $37.17 $26.06
Family $27.78 $74.62 $21.41 $64.68 $44.32

Page 12 of 26
ID Theft Protection
Plan Name ID Watchdog InfoArmor
Participants Input Data via Secure Website Dashboard
Confirmed Confirmed (SS#, Email Address, Drivers License, Credit Cards, Etc.)
Member Alerts Confirmed Confirmed
Program Services
Website Tips, Tools and Resources on Prevention Confirmed Confirmed
Credit Score and Report Confirmed (1 Bureau or 3 Bureau) Confirmed (1 Bureau or 3 Bureau)
Sex Offender Registration Reports Confirmed Confirmed
National Do Not Call List and No Solicitation Lists Confirmed Confirmed
Lost Wallet/Care Support Confirmed Confirmed
Online Surveillance and Alerts

Page 13 of 26
Buy, Sell, or Trade of Personal Information on Black Market (Searches for Personal Information Provided by Participant)
Confirmed Confirmed
Credit Monitoring and Alerts Confirmed (1 Bureau or 3 Bureau) Confirmed (1 Bureau or 3 Bureau)
Social Network (Facebook, Twitter, Instagram, Etc.) Confirmed Confirmed
Court Records (Bankruptcies, Criminal Records, Etc.) Confirmed Confirmed
Large Scale Data Breach Notifications Confirmed Confirmed
New or Added Wireless Accounts Confirmed Confirmed
Bank Account Changes Confirmed Confirmed
Guarantee/Insurance
Coverage for Victim of ID Theft While in Program (Such as Lawyers, Investigators, Legal Defense)
Confirmed Confirmed

Page 14 of 26
Reimbursement to Participant or Provider Hired
Yes, up to the limit of $1M per subscriber Yes, up to the limit of $1M per subscriber
Monthly Premium
One Bureau $5.00/individual, $9.50/family $7.95/individual, $13.95/family
Three Bureau $7.50/individual, $14.50/family $9.95/individual, $17.595/family

Page 15 of 26
Legal Plan
General Services for Covered Matters Nationwide LegalEASE Hyatt Legal
Office & Phone Consultations with Attorney Covered in Full Covered in Full
Document Review Covered in Full Covered in Full
DIY Online Access Confirmed - Portal Access Confirmed - Portal Access
Services for Non-Covered Matters
Discount for Non-Covered Items 25% discount 25% discount
Miscellaneous Law Services 15 hours of miscellaneous service covered 25% discount
Estate Planning
Wills & Codicil Covered in Full Covered in Full
Living Trusts Covered in Full Covered in Full
Powers of Attorney Covered in Full Covered in Full

Page 16 of 26
Complex Wills Covered under 15 hours of miscellaneous Covered in Full
Real Estate
Sale or Purchase of Real Estate Covered in Full Covered in Full
Refinancing Covered in Full Covered in Full
Tenant Negotiations Covered in Full Covered in Full
Eviction Defense Covered in Full Covered in Full
Property Tax Assessments Covered under 15 hours of miscellaneous Covered in Full
Foreclosure Covered in Full Covered in Full
Construction Disputes Covered in Full Covered in Full
Neighbor Disputes Covered in Full Covered in Full
Family Law
Adoption Covered in Full Covered in Full

Page 17 of 26
Guardianship / Conservatorship Covered in Full Covered in Full
Name Change Covered in Full Covered in Full
Premarital Agreement Covered in Full Covered in Full
Divorce Covered up to 28.5 hours of Contested, 10 hours Uncontested Covered up to 20 hours
Post Decree Child Custody/Support Covered up to 28.5 hours Covered up to 8 hours
Domestic Violence Covered up to 28.5 hours Covered in Full
Consumer Protection
Advice & Negotiations Covered in Full Covered in Full
Court Representation Covered in Full Covered in Full
Small Claims Actions Covered up to 2 hours Covered up to 2 hours
Financial Matters

Page 18 of 26
Creditor Negotiations Covered in Full Covered in Full
Debt Collection - Defense and Collection for Consumer Debts Covered in Full Covered in Full
Personal Bankruptcy Covered in Full – Chapter 7 or Chapter 13 Covered in Full – Chapter 7 or Chapter 13
Personalized Financial Planning Covered up to 10 hours N/A
Tax Preparation Covered in Full as it pertains to Legal items related to Tax Prep
Covered in Full as it pertains to Legal items related to Tax Prep
Tax Audits Covered in Full Covered in Full
IRS Collection Defense Covered in Full Covered in Full
Defense of Civil Lawsuits
Administrative Hearings Covered in Full Covered in Full
Other Civil Litigation Covered in Full Covered in Full
Incompetency Defense Covered in Full Covered in Full
Traffic Offenses

Page 19 of 26
Defense of Tickets Covered in Full - Includes DUI Covered - Excludes DUI
Driving Privilege Protection Covered in Full Covered in Full
Juvenile Court Defense Covered in Full Covered in Full
Immigration Assistance Covered for advice/consultation and document review
Covered for advice/consultation and document review
Elder Care Consultation Covered In Full - for elder matters relating to the participant
Covered In Full - for elder matters relating to the participant
Financial Counseling Services Covered up to 10 hours N/A
Debt Management Services Covered up to 10 hours N/A
Debt Consolidation Services Covered up to 10 hours N/A
Budget Analysis Services Covered up to 10 hours N/A
Credit Improvement Services Covered up to 10 hours N/A
Monthly Premium $16.85 $17.75

Page 20 of 26
Auto, Home and Renters Insurance
Auto Insurance Coverage MetLife Liberty Mutual Travelers
Automobiles, Boats, Motor Homes, Motorcycles, Snowmobiles, Trailers, Personal Watercraft Included Included Included
Personal Excess Liability Included Included Included
Multi-Car/Multi-Policy Discount Included Included Included
Anti-Theft Device Discount Included Included Included
Home Insurance Coverage
Home, Condo, Renter's, Rental, Personal Articles, Mobile Home Included Included Included
Protective Devices Discount Included Included Included
Fire Protection Included Included Included

Page 21 of 26
Multi-Home/Multi-Policy Discount Included Included Included
Group Discounts
Group Discount Yes (Up to 7%) Yes (Auto: Up to
10%; Home: Up to 5%)
Yes (Auto: Up to 5%; Home: Up to 2.5%)
Payroll Deduction Included (Up to 8%) Yes (Auto: Up to
7.5%; Home: Up to 5%)
Yes (Up to 3%)

Page 22 of 26
Pet Insurance
Program Eligibility to Enroll ASPCA Nationwide
Eligible Participants All Benefit Eligible Employees All Benefit Eligible Employees
Eligible Pets All Cats & Dogs Cats and Dogs; Avian and Exotic Pet Plans available
Pet Age Limitations Minimum 8 weeks of age N/A
Medical History Required Not at enrollment N/A
Coverage / Plan Information
Accidents and Illnesses, Including Hospitalizations and Surgeries Included Included
Prescription Medications Included Included

Page 23 of 26
Other Included Coverages X-rays, exams, alternative therapy, stem-cell therapy, behavioral conditions, etc.
My Pet Protection plans include congenital and hereditary conditions with no additional waiting
periods, prescribed therapeutic pet foods, prescribed nutritional supplements, prescribed behavioral
treatment and therapy, all dental diseases, internal and external parasite treatment, treatment for
complications of pregnancy, elective or cosmetic procedures, boarding or kennel fees for employee's
hospital stay, advertising and reward coverage, coverage for loss due to theft or straying and a
mortality benefit.
Additional Riders (Added Cost) Wellness Wellness
Cost
Annual Deductible Customized: $100, $250 or $500 (annual) $250
Co-Pays Customized: 10%, 20% or 30% 10%
Annual Maximum Starting at $2,500 up to unlimited $7,500
Maximum Per Incident N/A N/A
Covered Claims Paid Customized: 90%, 80% or 70% of covered veterinary costs. 90% of eligible conditions
Pricing Factors

Page 24 of 26
Payroll Deduction Yes Yes
Group Discount 10% 5%
Multi-Pet Discount 10% for each additional pet 5% additional for 2-3 pets; 10% additional for 4 or more pets
Factors Affecting Rates Species, breed, age, location and plan selection State and species
Sample Monthly Premium $5,000 Calendar Year Maximum $7,500 Calemdar Year Maximum
Golden Retriever - Male, 3 years old, 89101 Zip $53.60 $35.62
Golden Retriever - Male, 7 years old, 89101 Zip $85.77 $35.62
Domestic Short Hair Cat - Male, 3 years old, 89101 Zip $19.51 $21.36
Domestic Short Hair Cat - Male, 7 years old, 89101 Zip $29.26 $21.36

Page 25 of 26
Voluntary Vision Plan
Plan Benefits VSP Base VSP Buy-up
Calendar Year Benefit Yes Yes
Wellvision Exam Copay $10 $10
Prescription Glasses
Frames Copay $25 $25
Frame Allowance $120 / $140 for featured frame brands $200 / $220 for featured frame brands
Lenses Single vision, lined bifocal and lined trifocal included Single vision, lined bifocal and trifocal included
Lens Enhancements $55-$105 $0-$105
Contacts (Instead of Glasses)
Copay Up to $60 Up to $60
Contacts Allowance $110 $200

Page 26 of 26
Additional Features
Diabetic Eyecare Plus Program $20 Copay $20 Copay
Extra Savings 20% savings on additional glasses, discount on Laser Vision Correction
20% savings on additional glasses, discount on Laser Vision Correction, Retinal Screening
enhancement
Monthly Premium
Employee $5.86 $9.09
Employee & Spouse $11.75 $18.16
Employee & Child(ren) $12.57 $19.43
Family $20.09 $31.05

11. 11. Discussion and possible action regarding proposed plan design
changes for Plan Year 2020 (July 1, 2019 – June 30, 2020), including but not limited to the following: • Possible disallowing pharmacy patient assistance programs
(manufacturers’ coupons, etc.) from applying to the CDHP individual/family deductibles and out-of-pocket maximums;
• Possible implementation of mandatory narrow pharmacy network for 90-day prescriptions;
• Possible implementation of a patient safety program managed by PEBP’s pharmacy benefits manager;
• Possible additional cost containment activities; • Possible increases and requirements to CDHP HSA/HRA
enhanced employer contributions; • Possible requirement for Medicare exchange participants to
pay for their HRA administration fees and life insurance premiums;
• Possible elimination of the $25 copay for annual vision exams.
• Possible increases to the dental benefit maximums of the CDHP, EPO, HMO, and Medicare Exchange participants.
• Possible implementation of a pilot nutrition program in southern Nevada.
• Possible increase to Medicare Part B credits to retirees on the CDHP, EPO, and HMO plans;
• Possible plan design changes to the HMO/EPO copays for primary care, specialist visits, emergency room visits, generic drugs, and specialty drug coinsurance;
• Additional benefit design inclusions/exclusions/alterations to meet projected budget needs.


BRIAN SANDOVAL Governor
PATRICK CATES Board Chairman
DAMON HAYCOCK Executive Officer
STATE OF NEVADA
PUBLIC EMPLOYEES’ BENEFITS PROGRAM 901 S. Stewart Street, Suite 1001 | Carson City, Nevada 89701 Telephone 775-684-7000 | 1-800-326-5496 | Fax 775-684-7028
www.pebp.state.nv.us
AGENDA ITEM
X Action Item Information Only
Date: November 29, 2018
Item Number: XI
Title: Plan Year 2020 Plan Benefit Design
SUMMARY This report will provide the Board, participants, public, and other stakeholders information and recommendations for Plan Year 2020 Plan Benefit Design. REPORT At the September 27, 2018 Board meeting, PEBP provided the Board with opportunities for additional analysis regarding potential Plan Year 2020 (PY20) Benefit Design changes. Per the Board’s direction, PEBP has conducted analysis and has made recommendations on the following:
1. Implementing additional cost containment activities 2. Utilizing excess reserves to renew and/or implement new programs and services
EXCESS RESERVES Excess reserves are a constant moving target as projected experience and costs throughout the plan year often differ from actual results. PEBP reviews and revises excess reserve projections monthly and will continue to provide updates to the Board and public as new information becomes available. For the purposes of today’s discussion, the same reserve reconciliation provided at the September 27, 2018 Board meeting is reprinted below: Excess Reserve Reconciliation Type Amount Comments PY19 Starting Cash on Hand $143,129,727 PY18 Ending Amount PY19 HRA Reserve Budget -$31,676,056 Legislatively Approved PY19 IBNR Reserve Budget -$37,200,000 Legislatively Approved PY19 Cat Reserve Budget -$20,600,000 Legislatively Approved Increased IBNR Reserve -$14,600,000 Aon projected increased IBNR for the

Plan Year 2020 Plan Benefit Design November 29, 2018 Page 2 Excess Reserve Reconciliation
CDHP plus projected amount for new EPO plan totaling $51,800,000.
Increased Cat Reserve -$19,300,000 Aon projected increased Catastrophic for CDHP plus projected amount for new EPO plan totaling $39,900,000.
Remaining Available $19,753,671 PY 19 Approved Excess Reserve Spend
-$14,231,925 Approved by the Board in March 2018 (includes enhanced life insurance, enhanced CDHP HSA/HRA funding, Medicare Exchange life insurance premiums and HRA fees, supplemental HRA funding to Medicare retirees, and 3D mammograms)
PY 20 and PY 21 Budget Enhancements
-$376,864 Budget submission in August 2018
Remaining Balance $5,144,882 Amount available for PY20+ Cost Saving Opportunities for PY20 The following table describes cost-saving activities PEBP can implement in PY20: Benefit Design Benefit Level Projected Population Projected PY20
Savings Disallow Patient Assistance Programs from Applying to Accumulators
Drug manufacturer coupons/cash cards used to satisfy plan deductibles/out-of-pocket maximums
358 with Accredo Specialty Pharmacy copay assistance (PY18 CDHP members utilizing these services)
Variable PY18 utilization was
$1.4 million
Implement Mandatory Narrow Pharmacy Network
90 day drug fills at select retail/mail order
8,905 $347,000
TOTAL Cost Saving Opportunities $347,000+ Plus Starting Excess Reserves $5,144,882 Amount Remaining $5,491,882+ Disallow Patient Assistance from Applying to Accumulators PEBP and Express Scripts performed initial analysis on implementing a copay accumulator program to control specialty drug costs. This program is not new and many large employers have implemented it across the nation. To simplify the program, a copay "accumulator" recognizes when an employee uses a drugmaker discount card and makes sure that money does not apply toward their annual out-of-pocket spending requirement. When the copay card runs out of money, a patient must either cover the

Plan Year 2020 Plan Benefit Design November 29, 2018 Page 3 full copay cost, get a new discount card, or stop filling the prescription. The program can apply to almost any drug coupon used at a pharmacy working with the pharmacy benefit manager. Estimates show there are more than 41 million Americans in plans that use an accumulator. A recent article in U.S. News describes how two large companies (Walmart and Home Depot) are adopting these programs moving forward. (https://money.usnews.com/investing/news/articles/2018-11-13/walmart-home-depot-adopt-health-insurer-tactic-in-drug-copay-battle) PEBP had numerous conversations with both our Third Party Administrator (HealthSCOPE Benefits) and Pharmacy Benefits Manager (Express Scripts), and we concur there is significant money available by the drug manufacturers that is being left on the table because of our lower out-of-pocket maximums. Pharmacy manufacturers set drug prices accounting for copay accumulator programs like this and therefore PEBP and its members are effectively paying more for these drugs than we should. Unfortunately, there is no way today to develop a cost savings amount as changes to copay assist cards and coupons will most assuredly change between now and July 1, 2019 when this program can go live. Savvy drug manufacturers can and will circumvent these types of programs, but doing nothing ensures PEBP pays too much for these high cost drugs. PEBP Recommendation: PEBP believes we can no longer sit by and allow the plan, the members, and the Nevada taxpayer pay more for high cost drugs than most employers with these programs allow. Therefore we recommend implementing a copay accumulator program next year. If approved, PEBP will come back to the plan in March with some current savings numbers and address additional opportunities for excess reserve expenditures to offset those savings at that time. Smart90 Mandatory Network Express Scripts (ESI) is recommending Smart90 Mandatory Network for the State of Nevada beginning 7/1/2019. Through this program, ESI would proactively reach out to members through an extensive communication campaign that includes emails, letters and phone calls to notify them that they could save money by using a Smart90 participating pharmacy. Information will also be available on their website. Only clinically appropriate maintenance medications would be impacted by this program. This is a program that saves both the plan and the member money. The member will save money when they move to a Smart90 pharmacy or home delivery due to the improved pricing.
1. Approximately $282,000 savings come from channel shifts – moving from Retail 30 to either Retail 90/Mail Order allows the plan to access steeper discounts: for brands, discounts improve almost 6%; for generics, discounts improve 0.25%.
2. Approximately $65,000 savings come from pricing changes. PEBP has Voluntary Retail 90 currently, but the rates under Mandatory Smart 90 are better: brand Retail 90 rates improve around 1.25%; generic Retail 90 rates improve 0.25%.
3. Approximately $48,000 member savings is a product of channel shifts and pricing changes. While members still pay their coinsurance (on generics and preferred brands),

Plan Year 2020 Plan Benefit Design November 29, 2018 Page 4
those who move from Retail 30 to a 90-day channel will be able to fill meds with a deeper discount. • Total Projected Plan Savings: $347,000 • Total Projected Member Savings: $48,000
This network excludes Walgreens and CVS but includes most of the other chains (Walmart, Costco, Smiths and other grocery store chains) and independent pharmacies. Members are also still able to obtain a 90-day supply through ESI’s home delivery pharmacy if they so choose. 45.8% of Nevada’s subscribers currently use a preferred pharmacy in the standard network. That means that 54.2% of subscribers would have to use a different pharmacy if they wished to fill a 90 day supply at retail. Only 0.2% (18) of those members would have to travel over 4 miles to reach a preferred pharmacy.
Distance Summary
Network Participation Locations %
Locations Retail Claims
% Retail Claims
Eligible Members
% Eligible
Members Not Impacted 664 45.8% 38,923 48.2% 36,810 80.5% Impacted 785 54.2% 41,904 51.8% 8,905 19.5% Within 1 mile 540 68.8% 29,902 71.4% 6,345 71.3% 2 and 4 Miles 229 29.2% 11,915 28.4% 2,542 28.5% Over 4 Miles 16 2.0% 87 0.2% 18 0.2% Total 1,449 100% 80,827 100% 45,715 100%
PEBP Recommendation: Approve Smart90 Mandatory Network detailed above for PY20. Continuing Current / Implementing New Programs and Services Requiring Excess Reserves CDHP HSA / HRA Funding PEBP has provided a level of enhanced HSA/HRA funds to CDHP participants since the program incurred excess reserves. The following table shows current and proposed enhanced contributions to the HSA/HRA: Plan Year Individual Amount (Enhanced) Dependent
Amount (Enhanced)
2019 (Current) $200: • $100 tied to preventive program • $100 tied to Dr. on Demand and
Healthcare Bluebook enrollment
$0
2020 (Proposed) $100: • $100 tied to enrolling in Dr. on Demand
and Healthcare Bluebook
$0

Plan Year 2020 Plan Benefit Design November 29, 2018 Page 5 In Plan Year 2018, PEBP introduced enhanced HSA/HRA funding ($200) tying it to required completion of preventive activities. In Plan Year 2019, PEBP continued this incentive policy by expanding the requirements for the $200 enhanced funding to both preventive activities and enrollment in member online tools. In Plan Year 2018, some members reported difficulties in meeting the preventive activities requirements. They reported completion of these activities but the provider’s billing did not show the actions required when coding visits as diagnostic versus prevention. PEBP and HealthSCOPE staff spent significant effort and time researching and requesting rebilling from numerous providers to ensure members received credit for their actions. We believe these hurdles prevented some members from earning what was supposed to be a simple and transparent process for enhanced funding. With this history, PEBP is no longer recommending incentivizing preventive activities starting Plan Year 2020, however, there was increased utilization during the Plan Year 2018 time period. If the Board wishes to increase the HSA/HRA funding, the table below reflects the estimated costs:
Participant Count Enhanced Benefit Plan Cost 23,636 $ 400 $ 9,454,400 23,636 $ 300 $ 7,090,800 23,636 $ 200 $ 4,727,200 23,636 $ 100 $ 2,363,600 Dependent Count Enhanced Benefit Plan Cost 17,837 $ 100 $ 1,783,700
PEBP Recommendation: Since excess reserve levels are dwindling, PEBP recommends $100 be provided initially to primary participants for enrolling in Dr. on Demand and Healthcare Bluebook for PY20. Both programs saw significant increases in utilization due to the requirement in PY19, and all of the members who are already enrolled will by default receive the funding in July 2019. PEBP will keep a close eye on excess reserves and may come back to the Board in March 2019 with a recommendation to increase this funding. Medicare Exchange Life Insurance Premiums and HRA Administrative Fees Since 2011, PEBP has included the costs of Medicare Exchange retiree life insurance premiums and HRA administration fees in the administrative costs within the CDHP and HMO premiums. Enhanced life insurance premiums were paid for out of excess reserves. Conversely, dental premiums are paid directly by Medicare Exchange retirees since 2011, creating an inconsistency in who pays for certain benefits. PEBP developed the Agency Request Budget for Fiscal Year 2020/2021 which included the previously earmarked enhanced life insurance levels to become the standard amount provided

Plan Year 2020 Plan Benefit Design November 29, 2018 Page 6 regardless of excess reserves (restoration of these benefits). However, PEBP did not build into its biennial budget employees paying the costs of Medicare Exchange retiree fees and life insurance premiums. These costs will either need to be paid for out of reserves, paid for by retirees, or built into the PEBP budget in a budget amendment during session next year. The projected costs are as follows: Benefit Design Benefit Level Projected Population Projected PY19 Cost Medicare Exchange HRA Admin Fees*
$1.50 per Retiree per Month
12,523 $225,414
Life Insurance $12,500 / Retiree ($0.539/$1,000x12.5 = $6.74 per month)
12,523 $1,012,860
Total Amount $1,238,274 *HRA fees were recently negotiated from $2.74 to $1.50 per retiree per month and these cost savings are reflected above. PEBP looked up the premiums for individual life insurance utilizing the following inputs:
1. Female 2. 65 years old 3. Perfect health (never used any tobacco product) 4. Perfect family health history 5. Perfect driving record 6. $12,000 of coverage
The lowest cost that we found was $48 per month (7 times higher than PEBP’s life insurance premiums). Changing from “female” to “male” increased the costs to $66 per month (almost 10 times higher). Many members don’t have perfect health, perfect family history, or a perfect driving record, so those members’ costs would increase. Many members are older than 65. If PEBP’s Medicare Exchange retirees purchased individual life insurance plans on the commercial market, they would be subject to vigorous underwriting and may not even qualify for a life insurance policy. PEBP Recommendation: PEBP believes asking the Medicare Exchange retirees to pay for their administrative costs and life insurance premiums is fair. The market alternatives are potentially unaffordable or inaccessible, and the total costs per month are low ($8.24 combined). Additionally, PEBP included $1 per month/per year-of-service increased funding in the Agency Request Budget each year of the next biennium, so a retiree with 9 or more years of service has this cost covered by the increase year 1 and retirees with 5 years of service (minimum) or more have this cost covered completely in year 2 increased funding. The average years-of-service our Medicare retirees have is around 18. Eliminating $25 Copay for Annual Vision Exams In November 2016, the PEBP Board approved implementing a $25 copay for annual vision exams starting Plan Year 2018 to help offset the costs of other enhanced benefits. At the time,

Plan Year 2020 Plan Benefit Design November 29, 2018 Page 7 the projected savings were approximately $298,000 in PY18. The following data showcases actual savings in PY18 and projected savings/costs in PY19 and PY20: Plan Year 2017 2018 2019* 2020* Eye Exams 10,858 10,905 10,952 10,999 Copay $25 $25 $25 $25 Cost Savings $271,450 $272,625 $273,805 $274,990 *2019 and 2020 are projected based on 2017 and 2018 data (increasing 0.4% each year). Additionally, PEBP approved the implementation of a voluntary vision plan (buy-up) for members who need additional vision benefits. All voluntary vision plans evaluated and the plans the Board approved have a $10 copay for annual eye exams. PEBP Recommendation: Retain the $25 copay to maximize remaining reserves for CDHP HSA/HRA funding and other Board approved enhanced benefits for PY20/21. Increasing the Dental Benefit Annual Maximum In 2011, PEBP developed the Consumer Driven Health Plan (CDHP) and changed the dental offering from an annual $1,500 maximum per individual to $1,000. In 2014, PEBP developed a 3-year plan to spend down excess reserves which included increasing the annual maximum dental benefit back to $1,500. In 2017, PEBP was able to restore this temporary enhanced dental benefit back to the base plan moving forward. PEBP’s actuaries (Aon) analyzed the projected costs if the Board chose to increase this benefit again utilizing $100 increments to a maximum of $2,000: Plan Design Projected PY2020
Claims Cost** % Increase in
Cost $ Increase in
Claims Cost** Current Dental PPO Design $1,500 Annual Max*
$26,721,000
Increase Annual Max to $1,600 $27,065,000 1.3% $344,000 Increase Annual Max to $1,700 $27,308,000 2.2% $587,000 Increase Annual Max to $1,800 $27,478,000 2.8% $757,000 Increase Annual Max to $1,900 $27,598,000 3.3% $877,000 Increase Annual Max to $2,000 $27,654,000 3.5% $933,000 *Current projected PY2020 claims cost is based on PY2018 claims trended by 4% annually to PY2020 ** All numbers are rounded to the nearest thousand. Prior to 2011, the dental maximum had been $1,500, and PEBP has managed to restore this benefit to the pre-CDHP implementation level already. Comparing the plan benefit design with other government offerings, PEBP believes the current levels are sufficient. Additionally, PEBP

Plan Year 2020 Plan Benefit Design November 29, 2018 Page 8 is looking to offer a “buy-up” voluntary dental plan for members who desire more coverage and believe this mechanism will meet their needs. PEBP Recommendation: PEBP recommends no changes to the current benefit levels. Developing Pilot Program with UNLV for Enhanced Nutrition Services PEBP and a Board member reached out to UNLV to ascertain the feasibility and probability of a partnership with their Registered Dietician program. PEBP currently provides preventive/wellness benefits that correspond to the Affordable Care Act (ACA) and United States Preventive Services Task Force (USPSTF) recommendations. These recommendations include vaccinations, annual exams, etc. PEBP has expanded these recommendations to include a preventive drug list and 3-Dimensional Mammography in recent years. PEBP proposes a partnership among PEBP and two UNLV entities – the Dietetic Internship and Nutrition Center and the UNLV Student Health Center (SHC) and Faculty and Staff Treatment Center (FAST) which will allow the piloting of a nutrition education program targeted at high-risk PEBP members in Southern and rural Nevada, while facilitating the internship/patient experience component of UNLV dietetic students preparing for their board exam to obtain Registered Dietician Nutritionist (RDN) licensing in the State of Nevada. PEBP has received a draft proposal from UNLV and summarized key elements below:
1. Initial pilot of 500 members who have diabetes or renal disease. 2. Targeted participants will ideally live in Southern Nevada and obtain face-to-face
services on the UNLV campus, or be rural Nevadans and participate via the telemedicine model.
3. Program Launch and Duration: 12 months, launching 7/1/19 4. Initial and follow-up consultation (in-person at the UNLV Student Health
Center/FAST Center or via webcam) with UNLV dietetic internship students, supervised by a Registered Dietitian, will review members’ 3-day food journals and provide nutrition education for diabetics or renal patients, as well as provide guidance on healthy eating, including shopping tips, meal planning, and caloric intake. Members will have option to participate in program over 12 months with an initial consultation, and follow-up consultations at recommended prescribed intervals depending on diagnosis and disease stage, as follows:
a. Newly diagnosed (Day 1, Day 22, quarterly) b. Maintenance mode/well-managed (quarterly) c. High-risk/non-compliant patients (monthly)
5. Location: UNLV Student Health Center/Faculty and Staff Treatment (FAST) Center (located within Student Recreation and Wellness Center), 4505 S. Maryland Pkwy, Las Vegas, NV 89154
6. Scheduling: by appointment, Monday – Friday; 9 am- 4 pm 7. Patients are given the option to participate in sessions remotely due to rural location,
limited mobility, etc. Schedulers will send patient a web link in advance of the session and members can join from their chosen device.

Plan Year 2020 Plan Benefit Design November 29, 2018 Page 9
8. Pilot program costs estimated at $77,000. Contingency costs of $23,000 are proposed, resulting in a total annual budget for fiscal 2020 year of $100,000.
PEBP is still working out logistical details and payment methods to ensure the pilot program meets the requirements outlined above. UNLV researchers will evaluate and potentially publish the pilot data and outcome measurements and reporting to ensure a transparent program is implemented and results provided to the Board at meetings during and after the pilot ends. A successful pilot, based on positive patient and financial outcomes may initiate a proposal for expansion of services to a broader member population on a longer term basis. PEBP’s Recommendation: PEBP recommends earmarking $100,000 for this pilot with UNLV and implementing the program July 1, 2019. Increase Medicare Part B Credit for Retirees on CDHP, EPO, and HMO plans Currently, PEBP provides a $134 credit (minimum Medicare Part B premium) to retiree premiums on the CDHP, EPO, and HMO plans to save the plan under coordination of benefits rules. If the retiree’s CDHP, EPO, or HMO monthly premium is less than $134, the retiree’s monthly premium is reduced to $0 (with no additional credit). The Centers for Medicare and Medicaid Services (CMS) has announced the minimum Medicare Part B premium in 2019 is increasing $1.50 to $135.50. PEBP analyzed the enrollment and costs and as of October 2018, there are 1,113 retirees with Part B on the CDHP, EPO, and HMO plans: Type CDHP EPO HMO Total State Part A+B 281 45 23 349
Part B Only 296 41 20 357 Non-State Part A+B 31 16 27 74
Part B Only 215 36 82 333 Total 1,113 Monthly Cost $1,669.50
Annual Cost $20,034.00 PEBP Recommendation: Since the cost is minimal and PEBP benefits from Medicare paying primary on these participants, PEBP recommends paying the approximate $20,000 a year to increase the Medicare Part B premium credit to $135.50. HMO/EPO Plan Design Opportunities In 2016, PEBP signed a contract with both Health Plan of Nevada (HPN) and Hometown Health to provide a combined statewide HMO plan to eligible plan members. Last November, the Board approved the termination of the Hometown Health northern Nevada HMO plan and replaced it with a Exclusive Provider Organization (EPO) plan starting July 1, 2018. Although we have recently finished the first quarter (July – September), PEBP reached out to HPN to discuss any recommended changes to the plan design statewide. HPN proposed and PEBP analyzed the following changes:

Plan Year 2020 Plan Benefit Design November 29, 2018 Page 10 Plan Feature Benefit Design PY19 Benefit Design PY20 Primary Care Physician (PCP) Visit
$25 Copay $20 Copay
Specialist Visit $45 Copay $40 Copay Emergency Room Visit $300 Copay $500 Copay Hospital In-Patient Services $500 per Admit $500 per Admit Retail Pharmacy
1. Preferred Generic 2. Preferred Brand 3. Non-Formulary 4. Specialty
$7 Copay $40 Copay $75 Copay
30% Coinsurance
$10 Copay $40 Copay $75 Copay
20% Coinsurance Out-of-Pocket Limit $7,150 Individual
$14,300 Family $7,150 Individual $14,300 Family
PCP Referral Requirement to Specialists
No No
The shaded areas in green showcase proposed changes to copays/coinsurance. PEBP asked our actuaries (Aon) to analyze the potential impacts for both the HMO and EPO plans if the recommendations were implemented. The following projections are summarized below:
HPN Plan Design Scenarios Projected PY2020
Claims Cost** % Increase in
Cost $ Increase in
Claims Cost** HPN Current Design* $40,069,000
Enhance Specialty Coinsurance to 20% $40,311,000 0.60% $242,000 Proposed PCP, Specialist, ER, Generic Copay Changes $39,792,000 -0.69% -$277,000
EPO Plan Design Scenarios Projected PY2020
Claims Cost** % Increase in
Cost $ Increase in
Claims Cost** Premier Current Design* $63,299,000
Enhance Specialty Coinsurance to 20% $63,666,000 0.58% $367,000 Proposed PCP, Specialist, ER, Generic Copay Changes $62,862,000 -0.69% -$437,000
HPN and EPO Total Projected PY2020
Claims Cost** % Increase in
Cost $ Increase in
Claims Cost** HPN and EPO Current Design * $103,368,000
Enhance Specialty Coinsurance to 20% $103,977,000 0.59% $609,000 Proposed PCP, Specialist, ER, Generic Copay Changes $102,654,000 -0.69% -$714,000 NET TOTAL $105,000

Plan Year 2020 Plan Benefit Design November 29, 2018 Page 11 *Current projected PY2020 claims cost is based on PY2018 claims trended by 8% annually to PY2020 ** All numbers are rounded to the nearest thousand. PEBP Recommendation: With an increase to costs for lowering the specialty drug coinsurance from 30% to 20% offset by the decrease to costs adjusting copays for primary care, specialists, emergency room visits and generic drugs, the net difference is approximately a $105,000 overall savings. Therefore PEBP recommends all outlined changes to the HMO/EPO plan design above be implemented for PY 2020. Summary of Recommendation PEBP developed analysis and makes recommendations above predicated on the availability of projected excess reserves. As we get closer to the March 2019 rate setting meeting, PEBP may discover increased excess reserves and will come back to the Board to recommend additional expenditures (if appropriate). A summary of all recommendations for PY19 is below:
1. Do implement a copay accumulator cost containment program. 2. Do implement mandatory Smart90 pharmacy network cost containment program. 3. Do approve $100 CDHP HSA/HRA enhanced funding tied to Dr. on Demand and
Healthcare Bluebook enrollment, and revisit in March at rate setting for additional available funds.
4. Do require Medicare Exchange retirees directly pay for their HRA administration fees and Life Insurance premiums.
5. Do not eliminate the $25 copay for CDHP annual vision exams. 6. Do not increase the program-wide dental benefit maximum. 7. Do approve a one-year pilot nutrition program partnering with UNLV. 8. Do increase CDHP/EPO/HMO Medicare Part B premium credits from $134 to $135.50. 9. Do approve revised EPO/HMO plan design PCP, specialists, and generic drug copays and
coinsurance for specialty drugs as described above. The funding result from the above recommendations are as follows: Activity Amount Starting Excess Reserves $5,144,882 Recommended Cost Containment +$374,000* $100 CDHP HSA/HRA Funding -$2,363,600 UNLV Pilot – Enhanced Nutrition -$100,000 Increased Medicare Part B Premium Credits for CDHP/EPO/HMO Members -$20,034 Revise HMO/EPO PCP, Specialist, Generic Copays and Specialty Coinsurance
-
*Remaining for PY2021+ $3,035,248 *PEBP will revisit and make recommendations pending additional available funding at the March 2019 Board meeting (similar to the March 2018 Board meeting).


12. 12. Public Comment


13. 13. Adjournment





























