Embed Size (px)
Citation preview

State-Level Advocacy to Improve Health Insurance Coverage:
A Texas (Worst) Case Study
CFED Assets & Opportunity InstituteWashington, D.C.
September 24, 2009
Anne Dunkelberg, Assoc. Director, [email protected] Lydia Street - Austin, Texas 78702
Phone (512) 320-0222 (X102) – www.cppp.org


The Family Budget Estimator (FBE) Project provides a realistic picture of how much it costs Texas families in different areas of the state to meet their basic needs.
www.cppp.org/fbe

Health Care and Family Self-SufficiencyUnlike food, shelter, transportation, and education, the cost of
needed health care varies wildly across otherwise similarly-situated families
• A family with serious chronic condition, illness or injury may need hundreds of thousands in care in a year, while one with routine needs may need only thousands for basic preventive and primary care.
Current public programs:
• cover too few adults,
• end coverage abruptly at arbitrary income points (“cliffs”), creating disincentives for increased earnings
• Often present major barriers to enrolment by eligible persons
No system to fully address (in a progressive manner) the mismatch between AVERAGE costs of family coverage ($13,000-$14,000 a year) and median family incomes: e.g., ~$47,000 overall, $64,000 family of 4
No system to ensure that all can purchase coverage at or near the average cost; thus average costs are meaningless - can even be misleading

Health Care and Family Self-SufficiencySocial Security, Medicare, SSI, and Medicaid coverage of long
term care (70% of US nursing home residents) have made it possible for the generations since their creation to develop assets for home ownership, higher education, and general economic advancement.
Income and assets without them would have been devoted to the care of parents.
A progressively financed system of affordable comprehensive care for every income level will have a similar effect on enabling many more families in poverty to reach and hold middle class income and assets.
Child well-being directly improved when parents have access to physical and behavioral health care they need.

CPPP’s Texas health care work:• Educating Texans: uninsured, our lack of real
systems• Expanding public coverage eligibility
(Medicaid, CHIP)• Improving/protecting Medicaid-CHIP benefits• Reducing Barriers to Enrollment & Renewal• Private Insurance market regulation to
increase affordability• Promote National Reform: for most
comprehensive solution

Who is Uninsured in Texas?• 5.96 million total uninsured (2007)
– 4.3 million adults: 57% are below 200% FPL– 1.5 million kids (0-18): 22% of Texas children under age 19:
• 491,000 uninsured children live in families below the poverty line;• 472,000 uninsured children live in families between one and two times
the poverty line (100-200% FPL); • 339,000 uninsured children live in families between two and three times
the poverty line (200-300% FPL); and, • 208,000 uninsured children live in families above three times the poverty
line.
• Just under two-thirds of uninsured Texas children (64%) are in families below 200% FPL. – About 250,000 (roughly) uninsured Texas kids may be
undocumented and CANNOT get children’s Medicaid or CHIP.– This means 700,000-800,000⎯Half our uninsured children⎯are
eligible for Medicaid or CHIP right now, but not enrolled.• Texas HHSC estimates three-quarters are eligible for Medicaid, one-
quarter for CHIP.

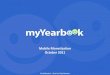
Uninsured Texans by Age Group, 200865+
0-18
19-64Rate: 32% of
19-64 are Uninsured
Rate: 20% of 0-18 are uninsured
~2/3 are below
200% FPL57% are below
200% FPL
Source: U.S. Census

0
5
10
15
Under 19 19 to 64 65 and over
Millions of Texans
Job-based coverage Medicaid Medicare Uninsured
Working-Age Texans Are Most Likely to be Uninsured
19% uninsured
3% uninsured
32% uninsured
Source: CPS Annual Social & Econ. Supplementwww.census.gov/hhes/www/hlthins/hlthins.html

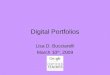
Employed65%
Unemployed7%
Not in Labor Force28%
Uninsured by Labor Force Status, 2007-08 Average
2 Out of 3 Uninsured Working-Age Texans Have a Job
Source: CPS Annual Social & Econ. Supplementwww.census.gov/hhes/www/hlthins/hlthins.html

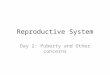
57.4 56.253 53 54 53.1 52.2 50.4 49.5
64.2 63.2 61.9 61 60.5 60.2 59.7 59.3 58.5
30
45
60
75
2000 2001 2002 2003 2004 2005 2006 2007 2008
% of Residents With Job-Based Insurance
Employer-Sponsored Coverage Declining in Texas and Nationwide, Even Before Recession
U.S. Average
Texas
Source: CPS Annual Social & Econ. Supplementwww.census.gov/hhes/www/hlthins/hlthins.html

U.S.-born citizen68%
Naturalized U.S. Citizen
6%
Not a U.S. Citizen26%
Uninsured by Citizenship Status, 2007-08 Average
Most Uninsured Texans are U.S. Citizens
Source: CPS Annual Social & Econ. Supplementwww.census.gov/hhes/www/hlthins/hlthins.html

Uninsured Problem Will Worsen Without Health Reform
Projected Uninsured Rate (%), 2010
Source: Methodist Healthcare Ministrieswww.mhm.org/advocacy/pdf/UninsuredData
ProjectionsJanuary2009.pdf
Texas average: 25.5%

Texas Medicaid: Who it Helps
Children, 1,905,520
Disabled, 391,382
Elderly, 373,686
Poor Parents, 116,141
TANF Parent, 28,059
Maternity, 92,271
April 2009, THHSC data.
Total enrolled 4/1/2009: 2.9 million
Because children account for over 2/3 of enrollment,
12-month renewals WOULD transform workload for entire
program

Income Caps for Texas Medicaid and CHIP, 2009
0%
50%
100%
150%
200%
250%
PregnantWomen
Newborns Age 1-5 Age 6-18 TANFparent of
2, noincome
WorkingParent of
2
SSI (agedor
disabled)
LongTermCare
CHIP
Mandatory Optional
$24,352/yr
$33,874/yr $33,874/yr
185% 185%
133%
$18,310
100% $2,256 $3,69612.3% 20.2%
74%
$7,884222%
$24,264$36,620
200%
Income Limit as Percentage of Federal Poverty IncomeAnnual Income is for a family of 3,
except Individual Incomes shown for SSI and Long Term Care

Why Very Few Poor Parents are Enrolled in Texas Medicaid
• Texas Medicaid income cap for poor parents, 12.8% of FPL or $188 per month for a family of 3, has not been increased by our Legislature for 24 years (last update: 1985).
• Working poor parents in Texas can get Medicaid now ONLY if they earn less than the legislatively-imposed income cap of $308 per month (e.g., for mother of two).
• Forces poor parents with high medical needs to choose between work and health care; 11 hours of work per week at minimum wage ($6.55 per hour) makes them “too wealthy” to get Medicaid.
• Texas can increase the Medicaid income limit for parents to any level it chooses, without any special federal approval. The only limiting factor is our willingness to put up our state’s share (about 40%) of the costs.
• Today, fewer than 134,000 poor Texas parents get Medicaid, though– there are about 836,000 poor parents in the state – 61% of adult Texans 18-64 below poverty are uninsured

Texas CHIP Enrollment(May 2000- August 2009)
0
200,000
400,000
600,000
May-00
Oct-00
Mar-01
Aug-01
Jan-02
Jun-0
2Nov
-02Apr
-03Sep
-03Feb
-04Ju
l-04
Dec-05
May-05
Oct-05
Mar-06
Aug-06
Jan-07
June
-07Nov
-07Apr
-08Sep
-08Feb
-09Ju
l-09
Source: Texas Health and Human Services CommissionDoes not include CHIP Perinatal program.
Highest, 5/02: 529,271
9/03: 507,259CHIP Cuts Begin
8/09: 490,603Child Medicaid
Simplified
9/07: HB 109

Texas Child Medicaid Enrollment(February 2001 – August 2009)
2006 low:1,720,025
1,000,000
1,300,000
1,600,000
1,900,000
2,200,000
Feb-01
Jul-0
1Dec
-01May
-02Oct-
02Mar-
03Aug
-03Ja
n-04Ju
n-04
Nov-04
Apr-05
Sep-05
Feb-06
Jul-0
6Dec
-06May
-07Oct-
07Mar-
08Aug
-08Ja
n-09Ju
n-09
Source: Texas Health and Human Services Commission1/2007 to present include newborn CHIP “perinates”; last month is preliminary due to lag
Simplified Enrollment begins under SB 43
12/2005 High: 1,838,239
August 2009:2,015,117

Texas Child Medicaid and CHIP Enrollment
1.5
2.0
2.5
3.0
Jan 02
Apr 02
Jul 0
2Oct
02Ja
n 03Apr
03Ju
l 03
Oct 03
Jan 04
Apr 04
Jul 0
4Oct
04Ja
n 05Apr
05Ju
l 05
Oct 05
Jan 06
Apr 06
Jul 0
6Oct
06Ja
n 07Apr
07Ju
l 07
Oct 07
Jan 08
Apr 08
Jul 0
8Oct
08Ja
n 09Apr
09Ju
l 09
Enro
llmen
t (m
illio
ns)
0.5
1.5
2.5
3.5
4.5
5.5
6.5
Chi
ld p
opul
atio
n (m
illio
ns)
Sources: Enrollment from Texas Health and Human Services Commission; Texas State Demographer's 0-17 Population Estimates
Sept. ’03: 2,150,543
August ‘09:2,505,720
Estimated child population growth is almost 70,000 per year
Combined CHIP/Child Medicaid Enrollment

Staffing Levels and Workload
0
5,000
10,000
15,000
Num
ber o
f sta
ff
01002003004005006007008009001,000
Wor
kloa
d
Eligibility Staff 9,606 9,668 9,142 8,446 7,573 6,676 5,975 6,381 6,659 7,377 8,519
Recipients per w orker 367 374 442 561 691 814 946 849 782 769
FY 00
FY 01
FY02 FY03 FY04 FY05 FY06 FY07 FY08 FY09*
FY '10**
*Estimated recipients per w orker. **Number of w orkers if additonal staff are approved under Rider 61.
Eligibility Staff Shortage: A Vicious Cycle

The Texas CHIP Coalition was formed in 1998 to work for
the establishment of a strong Children’s Health
Insurance Program in Texas. Today, our broad-based Coalition continues to work to improve access to health care for all Texas children, whether through Medicaid, CHIP, or private
insurance.www.texaschip.org

Texas CHIP Coalition Statewide Organizations, 81st SessionAARPAdvocacy Inc.AMERIGROUP Community CareAny Baby Can of TexasCatholic Health Association of TexasCenter for Public Policy PrioritiesChildren's Defense Fund of TexasChildren's Hospital Association of
Texas (CHAT)Christian Life Commission, Baptist
General Convention of TexasCoalition for Nurses in Advanced
PracticeCommunity Health Choice, IncFamily Medicaid Access ProjectLa Fe Policy Research and Education
CenterLeague of Women Voters TexasMarch of DimesMental Health America of TexasMethodist Healthcare MinistriesNational Council of Jewish Women,
Texas State Public Affairs
Superior Health PlanTeaching Hospitals of TexasTexas Association of Health PlansTexans Care For ChildrenTexas Academy of Family PhysiciansTexas American Federation of
Teachers (Texas AFT)Texas Association of Community
Action Agencies, Inc. (TACAA)Texas Association of Community
Health CentersTexas Children’s Hospital Texas Dental AssociationTexas Hospital AssociationTexas ImpactTexas Medical AssociationTexas Nurses Association Texas Network of Youth ServicesTexas Pediatric SocietyTex Protects: The Texas Association
for the Protection of ChildrenUnited Ways of Texas

100-200% FPL
300-400% FPL
<100% FPL
200-300% FPL
> 400% FPL
Uninsured Texas Children, (0-18) 2007-2008
By Family Income
Total uninsured children: 1.418
millionUS Census, March 2008 & 2009 CPS

Since 2003, Texas Kids in Moderate to High Income Families Saw the Biggest Increases in Number of Uninsured
4.3%
-5.0%
29.5%
16.4%
Below 100% 100% to below 200% 200% to below 300% 300% and above
Source: 3-year average data (2002-2004 vs. 2006-2008) for children ages 0-18, Current Population Survey, U.S. Census Bureau
Number of Uninsured Kids betw een 100-200%
poverty declined
Wor
seBe
tter

0.0
2.5
5.0
7.5
2000 2001 2002 2003 2004 2005 2006 2007 2008
Millions of Texas Children (Under 19)
Medicaid and CHIP Critical for Children’s Coverage
Uninsured
Employer-sponsored insurance
Medicaid
Medicare or Military
CHIP
Source: CPS Annual Social & Econ. Supplement, www.census.gov/hhes/www/hlthins/hlthins.htmlTexas Health and Human Services Commission, Medicaid and CHIP data

State Regulation of Health Insurance• RATES for H.I. virtually unregulated:
– Under Texas law today, small employers pay an average high premium of $22,000 a year for a single worker.
– 2003-2006 medical loss ratio averaged 72% in small employer market, 84% in large, but wide range between companies—from 22% percent to 267% share of premiums spent on medical care.
• 2009 CPPP advocacy & education on above, gains include:– First time subsidy in high-risk pool– new Healthy Texas small employer reinsurance program– Continuation reforms to extend ARRA subsidy– Damage control on default program for IV-D children– Revival of coalition work, public and lawmaker education

Texas Voice for Health Reform Principles
1. Affordable Access to Good Health Care Must be Available for All Americans. It should:
• Be affordable for people at all income levels • Remain available and affordable when family and economic circumstances change• Establish both a responsibility for the public to contribute and an assurance of cost containment
for individuals and families• Eliminate health costs as the #1 cause of bankruptcy in America.
2. A Decent Standard of Comprehensive Care Must Be Established. It should:
• Keep people healthy and treat them when they’re ill• Cover the whole person• Not be lost or reduced based on pre-existing conditions or pregnancy
• These first 2 steps will not happen by accident: Americans must choose to do this and demand it.
3. To be effective, sustainable, equitable, and balanced with our other important priorities as a nation, national health reform should also address safe and high quality care; costs and cost-effectiveness of health care; consumer choice; and eliminating non-financial barriers to care
• Just working on Step 3 will not make Steps 1 or 2 happen.

• Three bills being drafted: Senate Finance; Senate HELP; House “Tri-Committee” (E&C, W&M, Ed & Labor)
– Senate Finance: Bill to be released this week, concerns that they are cutting back by reducing affordability subsidies, protections.
– HELP: passed out of committee• Will have to be merged with Finance bill when it is passed.
– House: bill filed Tuesday July 14. Each of 3 committees made amendments which must be reconciled in September before a full House vote can happen.
• House-Senate compromise process starts as soon as Chambers vote their bills.
• If successful, bill could be voted on and signed in November, December.
• If no deal reached, large portions of (but not all of) reform can/will be passed through “Budget Reconciliation,” but this is less than ideal, both politically and from policy standpoint.
– Budget Reconciliation only requires 51 Senate votes, but limits what you can do.
Health Reform Process

• Key elements BEING CONSIDERED:– If you like what you have now, you can keep it.– Medicaid expansion (e.g., cover all up to 133% FPL: $14,404 for one; $29,327 for 4).
– Reform Private Health Insurance: standardize benefits, limits on price variation, no denial of coverage, no excluding pre-existing conditions, no annual or lifetime maximums. Changes focused on individual and small employer coverage.
– Create health insurance exchanges where participating private options can be compared and purchased (like Amazon or Travelocity for insurance).
• Will there be a Public or Non-profit plan option?
– Premium assistance up to 300% or 400% of FPL? ($66,150 to $88,200 for family of 4)
– Out-of-pocket caps, too, to ensure real affordability/end (reduce?) medical bankruptcy
– Individual mandate to have coverage: but only if affordable coverage exists!
– Requirements for employers to contribute, with exemptions for smallest employers; One idea is a requirement to help pay for only employees who use Medicaid or get premium assistance (latter approach is opposed by advocates for low-income Americans).
Health Reform Basics

• Every Texan will have new health security. You cannot lose, be denied, or priced out of coverage no matter your age, health status, or employment status.
• Annual caps on out-of-pocket costs and no annual/lifetime benefit limits mean critical financial protection at all income levels that does not exist today.
• About 4.5 million Texans would gain coverage– About 1 million uninsured Texan adults would get Medicaid—up to 133%
FPL
– About 2.3 million uninsured Texans would get premium assistance--above Medicaid and below 400% of poverty ($88,200 for family of 4)
• Small businesses and individuals can pay what large businesses do for health insurance. Under Texas law today, small employers pay an average high premium of $22,000 a year for a single worker.
• Depending on wages they pay businesses with fewer than 25 employees (67% of Texas business) can get tax credits to cover up to ½ the cost of coverage.
Benefits of Health Reform

• Medicaid expansion—up to 133% FPL.– CPPP CONSERVATIVELY estimates the Medicaid expansion alone will add $3.7 billion a year
in new federal dollars to the Texas economy ($3.3 if 90% federal share); with a multiplier effect of $10 to $12 billion a year, and
– could convert Texas from being a “donor state” that sends more to DC in taxes than we get back by covering low-income adults in Medicaid.
– What share will Texas have to pay for required Medicaid expansions & increased Medicaid provider payment rates?
• 100% federally-funded in House proposal; E&C amends to 90% from year 3 onward• But Senate may push to “phase back” over time to a state-share formula
• Premium subsidies—up to 400% FPL– even more funding will flow to Texas from premium assistance to low-to-moderate income
families
• Goal is to make the final bill 100% paid for (combo of cuts/savings and new revenues); if “pay-fors” are cut, expect to see loss of affordability and/or health benefits!
• Long list of provisions would reduce cost, improve quality of care, but MORE may be added before a bill is passed.
Cost of Health Reform

How Advocacy Landscape Changes if Reform Bill Passes
• Below/Near Poverty Income: will eligibility system bottlenecks prevent coverage?
• Low-Moderate Income: Will premium and out-of-pocket cap assistance be affordable? If not:– Financial penalties and no coverage?– Exemption from penalties, but still uninsured?
• Middle+ Income: Will market/rating reforms be adequate to assure affordability?– House & HELP limit age rating 2:1; Senate Finance 5:1 will make
premiums unaffordable for many over 40.– Need “Hard Cap” included in House bill on out-of-pocket costs (over
75% of medical bankruptcies in 2008 were to INSURED persons)• Safety Net Care: Will be needed for undocumented (possibly
LPRs, too) ; MAY be needed for low-income if coverage not affordable.

Use of This Presentation
The Center for Public Policy Priorities encourages you to reproduce and distribute these slides, which were developed for use in making public presentations.
If you reproduce these slides, please give appropriate credit to CPPP.
The data presented here may become outdated.
For the most recent information or to sign up for our free E-Mail Updates, visit www.cppp.org.
© CPPP
Center for Public Policy Priorities900 Lydia StreetAustin, TX 78702
P 512/320-0222 F 512/320-0227