Embed Size (px)
Citation preview

4/7/15
1
The Diabe.c Foot: A Mul.disciplinary Approach
Kathy Frush, DPM Assistant Professor
Des Moines University College of Podiatric Medicine
and Surgery
Sta.s.cs
• 29.1 million affected with diabetes in the US – 9.3% of the US popula.on – 8.1 million undiagnosed
• Diabe.c foot ulcers leading cause of nontrauma.c amputa.on – 10-‐25% will develop foot ulcer during life.me
Why are we concerned with saving lower
limbs ?
Energy Cost of Amputa.on
Waters et al, “Energy Cost of Walking of Amputees: The Influence of Level of Amputa.on,” JBJS, Jan 1976, 58A, 42-‐46
“When preserva,on of
func,on is the chief concern, amputa,on should be performed at the lowest possible level.”
Energy Cost of Amputa.on
• Pinzur et al, “Energy Demands for Walking in Dysvascular Amputees as Related to the Level of Amputa.on,” Orthopedics, Sept 1992, Vol 15, p 1033-‐1037
Survival rates a`er amputa.on
• Looked at 5 yr survival rate of nontrauma.c amputa.on of Diabe.c (n 100) and Nondiabe.c (n 151) – 61% with DM died – 53.4% without died
Tentolouris et al. Diabetes Care. July 2004.
2B: PAD

4/7/15
2
Who is at risk for ulcers?
• Peripheral neuropathy • PAD • Foot deformity • Previous amputa.on
SWM • 5.07 monofilament
– exerts 10 grams of pressure
• Apply only enough pressure to just bend monofilament
• Pt eyes should be closed • Need loss of 4 of 10 areas to diagnose
• If 0/10 felt keep tes.ng up leg to knee to find level of sensa.on
PAD Risk Factors
• Diabetes • Smoking • History of CAD • Elevated cholesterol or decreased HDL
• Hypertension • Obesity
• Sedentary lifestyle • Increased plasma
homocysteine • Increased CRP • Male gender • Age • Race
– Hispanic – African American
Krajewski LP, Olin JW. Chap. 11 Peripheral Vascular Diseases 2nd ed. 1996
Marso et al. J Am Coll Cardiol. 2006.
Vascular History and Physical
Physical Exam
• Palpable Pulses • Capillary Refill Time • Cold extremity • Dependent Rubor • Absent hair growth • Hemosiderin deposits • Dry, atrophic skin • Gangrene

4/7/15
3
The Ankle-‐Brachial Index
In diabe)cs, arterial calcifica)on can lead to falsely elevated readings.
Condi.on ABI Normal Above 0.9 Mild Obstruc.on 0.8 – 0.9 Moderate Obstruc.on 0.5 – 0.8 Severe Obstruc.on Below 0.5
ABI = Lower extremity systolic pressure Brachial artery systolic pressure
Calcified Vessels
Foot deformi.es Interna.on Working Group on the Diabe.c Foot (IWGDF) Classifica.on
• Risk 0 – no recognizable risk factor • Risk 1 – neuropathy with no other risk factors • Risk 2 – PAD with or without neuropathy • Risk 3 – current foot ulcer, history of foot ulcer or prior amputa.on
Evalua.on of risk classifica.on from IWGDF
• Lavery et al, Diabetes Care, Jan 2008 – Aim: to evaluate role of risk factors to predict lower extremity complica.ons
– Evaluated 1666 consecu.ve pa.ents with DM for average of 27 months
– Lower extremity complica.on • Ulcer, infec.on, amputa.on, hospitaliza.on
Evalua.on of risk classifica.on from IWGDF
• Modified IWGDF by splilng category 2 and 3 into subsec.ons – 2A: PN with deformity – 2B: PAD – 3A: hx of ulcer – 3B: hx of amputa.on

4/7/15
4
Evalua.on of risk classifica.on from IWGDF
• Results – More complica.ons with
• 2B: PAD vs 2A: PN with deformity • 3B:amputa.on vs 3A: hx of ulcer
– No difference in risk with • Neuropathy with or without deformity
WHAT TO DO WHEN WOUNDS BECOME INFECTED
IDSA (Infec.ous Diseases Society of America) Diabe.c Foot Infec.on Classifica.on
• Infec.on present, as defined by the presence of at least 2 of the following items: – Local swelling or indura.on – Erythema – Local tenderness or pain – Local warmth – Purulent discharge (thick, opaque to white or sanguineous secre.on)
IDSA Diabe.c Foot Infec.on Classifica.on
• Uninfected – Wound without purulence or any manifesta.ons of inflamma.on
IDSA Diabe.c Foot Infec.on Classifica.on
• Mild – Celluli.s or erythema > 0.5cm to ≤2 cm around ulcer or wound
– Infec.on is limited to skin or superficial subcutaneous .ssue
– No local complica.ons or systemic illness *should exclude other causes of inflamma.on (eg, trauma, gout, acute Charcot, fracture, thrombosis, venous stasis)
IDSA Diabe.c Foot Infec.on Classifica.on
• Moderate – Erythema >2 cm, OR involving deeper structures than skin or subcutaneous .ssue (eg, abscess, osteomyeli.s, sep.c arthri.s, fascii.s)
– AND no systemic inflammatory response syndrome (SIRS)

4/7/15
5
IDSA Diabe.c Foot Infec.on Classifica.on
• Severe – Local infec.on (as described previously) with signs of SIRS as manifested by ≥2 of the following:
• Temperature > 38°C or < 36 °C • Heart rate >90 beats/min • Respiratory rate >20 breaths/min or PaCO2 <32 mm Hg • White blood cell count > 12,000 or < 4,000 cells/µL or ≥10% immature (band) forms
IDSA Valida.on Wound Depth No infec,on Mild Moderate Severe
Full thickness 88.7 76.1 30.8 22.2
Fascia -‐ tendon 7.2 21.1 25.0 11.1
Bone – joint 4.1 2.8 44.2 66.7
Bone infec.on 0 0 38.5 37.0
Lavery LA, Clinical Infec.ous Diseases. 2007.
IDSA Guideline Valida.on
Lavery LA, Clinical Infec.ous Diseases. 2007.
Obtaining Cultures • Do not culture wounds without signs of infec.on
– Wounds naturally have nonpathologic bacterial coloniza.on
• Do not culture intact skin
• If taken in clinic or at bedside – 1st cleanse and debride wound – Then take .ssue sample by using sterile cureue, 15 blade or biopsy
– Avoid doing swab cultures • May lose some of your organisms
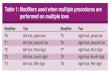
IDSA Suggested Abx for Moderate -‐ Severe Foot infec.on
Pathogen An,bio,c Comments
MSSA; Streptococcus; Enterobacteria; obligate anaerobes
Ampicillin-‐sulbactam (Unasyn)
Adequate if low suspicion of Pseudomonas
Ertapenem Once daily dosing. Rela.vely broad spectrum, not ac.ve against Pseudomonas
Imipenem-‐cilasta.n Very broad spectrum (no MRSA coverage) use only when needed
MRSA Vancomycin
Pseudomonas aeruginosa Piperacillin-‐tazobactam (zosyn)
TID/QID dosing. Good broad spectrum coverage
Main infec.ng organism
• *”Head of snake theory” – target main organism and other organisms will also be taken care of WA Joseph, J Vasc Surg Sept 2010
• Staph and strep are going to be main organism – Pseudomonas rarely main pathogen

4/7/15
6
What can PCP do to help wound healing?
• Monitor and manage nutri.on • Glycemic control • Edema control
Albumin
• Important protein in wound healing • Golinko et al. Wound Repair Regen. 2009
– Looked at clinical variables in wound healing – Amputee pa.ents had overall lower albumin than Non amputee pa.ents
– No significance in HgA1c in this study
Albumin Supplementa.on
• Armstrong et al. Diabe.c Medicine. 2014 – Looked at effects of supplement of of arginine, glutamine and β-‐hydroxy-‐β-‐methylbutyrate vs control on wound healing
• Supplement aided in wound healing – Albumin >40 g/L – ABI >1
HgA1c and healing rates
• Christman et al. J invest Derm. Oct 2011 – Hypothesized that HgA1c would correlate with wound healing rates
– 183 pa.ents • 60% had PN • 29% had PAD
– Included any diabe.c wound • 85.2% had foot or ankle ulcer
HgA1c and healing rates
• Results – For neuropathic foot wounds
• For every 1% increase in HbA1c, there was a decrease in wound area healing rate of 0.022 cm2
– In PAD pa.ents • For every 1% increase in HbA1c, there was decrease in wound healing rate of 0.030 cm2
HgA1c and healing rates

4/7/15
7
Foot management recommenda.ons
• Regular inspec.on and exam of the at risk foot • Iden.fica.on of the at risk foot • Educa.on of pa.ent and family members • Appropriate footwear • Treatment of nonulcera.ve pathology
Foot Management Recommenda.ons
• Regular inspec.on and exam of the at risk foot – All diabe.cs should have foot exam yearly – Those at risk examined every 1-‐6 months – Beware of the asymptoma.c foot
Foot Management Recommenda.ons
• Educa.on of pa.ent and family members – High risk pa.ents should inspect feet daily – Check water temperature – Don’t use hea.ng pads – No barefoot or sock foot walking – For xero.c skin “lo.on” feet daily avoiding interspaces
– Dry between toes a`er shower or bath – Don’t use medicated corn removers – Inspect inside of shoes before pulng on
Ulcer Management and Preven.on
• Proper offloading – Debridement of calluses and ulcers – Proper filng shoes
• Accomoda.ve ortho.cs and extra depth shoes for those with deformity
• Proper nail care – Management of ingrown nails – Thinning of excessively thick nails
Foot Management Recommenda.ons Ulcer Debridement

4/7/15
8
Ulcer Debridement Wound Management
Wound Management
Ques.ons?