Embed Size (px)
Citation preview

Atypical Dementia �1It’s All About the Approach: A Guide to Diagnose Atypical Dementias
David F. Tang-Wai MDCM FRCPCAssociate Professor (Neurology & Geriatric Medicine), University of Toronto
10th Canadian Conference on Dementia, Quebec City QC - Friday October 4, 2019
What is an atypical dementia? • A dementia that is not typical (amnestic) Alzheimer’s dementia
Basic Outline to the Evaluation Approach
The “AcHE-I” Approach
1. Every dementia starts with a specific sign/symptom that corresponds to a specific area of the brain.
2. Over time, other signs/symptoms appear in a sequence specific to the type of dementia
3. Cognitive testing and psychiatric/physical/neurological exams determines the presence/absence of the signs/symptoms from #2.
4. The type/cause of dementia is the integration of #1, 2, and 3 above.
�
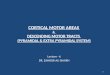
VisuospatialSimultanagnosia
Optic Ataxia
Language, CalculationsAnomia, impaired sentence
repetition, acalculia
PraxiaIdeomotor apraxia
Geographic orientationGeographic disorientation
Executive Function & Attention
Executive dysfunction
MemoryAnterograde memory
deficits
1. Ascertain the “true” chief complaint/ presenting feature 2. Chronological approach to the History & clarification of signs/symptoms 3. Attention to parts of the cognitive & neurological Examination 4. Interpretation of the entire case
�
1 2
34
Key Points 1. Each step in the evaluation & diagnostic process must
fit with each other. 2. You will be ruling in a diagnosis as opposed to ruling
out.3. Rarely does 1 component/piece alone arrive at a
diagnosis. Rather, it is all of the available information that makes the diagnosis.

Atypical Dementia �21. Ascertain the chief complaint into the following components (onset, progression, first symptom noticed & duration) as it can (1) often direct the
history, (2) inform about the diagnosis, and (3) direct investigations
ONSET PROGRESSION FIRST SYMPTOM NOTICED DURATION
Acute (seconds to days)Disorders to consider • Stroke • Infection (viral, bacterial) • Metabolic
ImprovingDisorders to consider • Stroke • Infection (viral, bacterial) • Metabolic • Delirium
• the presenting symptom often determines the type of dementia (see table below)
• not all causes of dementia present with true anterograde/short-term memory loss
Acute (seconds to days)Disorders to consider • Stroke • Infection (viral, bacterial) • Metabolic
Subacute (weeks to months)Disorders to consider • Metabolic • Infection (CJD, fungal, spirochete) • Endocrine • Paraneoplastic
StaticDisorder to consider • Stroke (fixed deficit)
Subacute (weeks to months)Disorders to consider • Metabolic • Infection (CJD, fungal, spirochete) • Endocrine • Paraneoplastic
Chronic (years)Disorders to consider • neurodegeneration • chronic cerebrovascular disease
FluctuatingDisorders to consider • Epilepsy • Paraneoplastic • Metabolic • Dementia with Lewy bodies
Chronic (years)Disorders to consider • neurodegeneration • chronic cerebrovascular disease
ProgressiveDisorders to consider • neurodegeneration • chronic cerebrovascular disease • infection (CJD)
Key Points 1. The presenting complaint may not be the first words/symptom
that the patient/collateral expresses. It may take a few minutes and/or additional examples to determine it.
2. Ask for examples of a person’s “memory” difficulties - to ascertain what their complaint/symptom really is.
3. Beware of the tendency to the “default interpretation” of anterograde memory loss and the “default”” view that every person has typical Alzheimer’s dementia.

Atypical Dementia �3Test to Consider Based on ONSET of Symptoms
Test to Consider Based on PROGRESSION of Symptoms
Definition Disorders to Consider Suggested Tests to Obtain
Acute
seconds to days •stroke•infection•metabolic
• IMMEDIATE neuroimaging (CT or MRI)Consider vascular imaging, echocardiogram, 48h+ holter monitor
• Blood tests, CSF
Subacuteweeks to months •metabolic
•endocrine•Infectious (prion)
• Blood tests, CSF• URGENT neuroimaging (CT or MRI)
Insidious/Chronic years •neurodegenerative•cerebrovascular disease
• Non-urgent blood tests• Non-urgent neuroimaging (CT or MRI)
Figure Disorders to Considers Suggested Tests to Obtain
Improving• stroke• metabolic• delirium
• Neuroimaging (CT or MRI)• Blood tests
Static • stroke• neurodegenerative*
• As above• Consider vascular imaging, echocardiogram, 48h+ holter
monitor
Progressive • neurodegenerative • infection
• Neuroimaging (CT or MRI)• Blood tests
Fluctuating
• Seizures• Metabolic• Delirium• Dementia with Lewy bodies
• As above• EEG

Atypical Dementia �4Examples of Presenting Symptoms and Potential Interpretation
Examples of Ideal Chief Complaints:
What People Really Say Interpretation & Affected Cognitive Domain Localization Disorder(s) To Consider
• repeats him/herself• rapidly forgets conversations Anterograde memory loss Temporal lobe • Alzheimer’s disease
• can’t align things• problems seeing, reading• “blurry vision”
Visuospatial Parietal and/or occipital lobes
• Alzheimer’s disease (posterior cortical atrophy)• Dementia with Lewy bodies• Corticobasal syndrome/degeneration
• can’t multitask• can’t plan• took out $20, then $50, then $20 -
instead of $90 in 1 stepExecutive function Frontal lobe
• Alzheimer’s disease• Vascular cognitive impairment• Frontotemporal dementia• Dementia with Lewy bodies• Progressive supranuclear palsy
• forgotten words• describes words, talks around
them• mixes up words, mispronounces
Language (anomia) Left hemisphere• Primary progressive aphasia• Alzheimer’s disease• Corticobasal degeneration
• cannot recall people s/he sees on the street
• does not recognize familiar people• can’t recognize his own house
Prosopagnosia (facial recognition) Right temporal (mesial) • Frontotemporal dementia
• Alzheimer’s disease
• forgotten how to fix things Apraxia Left parietal or hemisphere
• Corticobasal degeneration• Alzheimer’s disease
Chief complaint Suggestive of/Probable cause of dementia
Insidious onset for progressive anterograde (short-term) memory difficulties of 3 years in duration Alzheimer’s disease
Acute onset of anterograde memory loss, prosopagnosia (inability to recognize familiar faces), and visual hallucinations
Stroke - specifically, right posterior cerebral artery infarct
Insidious onset of fluctuating level of cognition with visual hallucinations and slowness of 2 years in duration Dementia with Lewy bodies
Acute onset of anterograde memory loss and apathy/abulia Stroke - specifically anterior cerebral artery infarct

Atypical Dementia �52. Obtain a chronological sequence of events/cognitive decline as the progression of symptoms can indicate the type of dementia and or the
presence of a secondary pathology. In all dementias, regardless of cause, there is impairment in all domains by the end. Some dementias develop additional phenotypes (see Example).
Example: Kertesz A et al. Brain. 2005;128:1996-2005
5 Tips to Help with History
Tip Rationale
1. Ask what happened to the patient if there gaps in time in the history
• Often patients are changing during these “gaps” and you will need to prompt the collateral historian or else you may interpret (incorrectly) a step-wise progression.
2. Ask for all components within a cognitive domain
• For example, for language, in addition to asking for word-finding difficulties, also ask for paraphasic errors, changes in reading/writing/comprehension
3. Ask for changes and not inability to perform tasks
• Often patients require help (prompting, assistance) before they become unable to perform a task.• The collateral historian will answer (correctly) that the patient is still able to perform a task but may not volunteer
that they require some help.
4. Clarify why a patient is not able to perform tasks - ask for additional details.
• There can be many reasons for a patient not able to perform a task and you can incorrectly attribute the inability to a cause/cognitive domain.
• For example, not being able to use a remote control can be due to visuospatial difficulties, motor weakness, language difficulties - in addition to apraxia.
5. Assign a medical term to the impairment/sign (see examples of presenting symptoms)
• For example, a person who cannot “find” the milk in the refrigerator despite intact vision is interpreted as simultanagnosia, which is a defining characteristic in posterior cortical atrophy.
• This will help with interpretation and integration of the case.
START bvFTD bvFTD bvFTD bvFTD PPA PPA PPA PSP CBD
MIDDLE PA CBD PA bvFTD CBD PSP bvFTD bvFTD
END MND MND PA CBD CBD bvFTD bvFTD PA PA
����
�
����
����
�����
�

Atypical Dementia �63. Cognitive and Neurological Examinations
Determine A Pattern on Cognitive Testing
Pattern Localization Problems Seen On Testing Disorders To Consider
Amnestic OrientationDelayed word recall
• Mild cognitive impairment (amnestic)• Alzheimer’s dementia
Executive Dysfunction/Frontosubcortical
Attention3-step commandLearningTrails BSerial 7sLetter fluencyDigit Span
• Dementia with Lewy bodies• Parkinson’s disease dementia• Vascular dementia• Normal pressure hydrocephalus
Visuospatial
DrawingTrails (searching)Inability to “see” picturesOverlapping figures (see MoCA-Basic)
• Posterior cortical atrophy• Dementia with Lewy bodies
Aphasia
NamingComprehensionReadingRepetition (Sentence, single word)Writing
• Primary progressive aphasia

Atypical Dementia �7Upper Motor Neuron (UMN) and Parkinsonism Are Common Neurological Examination Findings among the Atypical Dementias
AD Vascular FTD PSP CBD DLB PDD
Normal neurological examNormal
[If patient ONLY has fluctuations & hallucinations]
• Upper motor neuron pattern of weakness• Absolute/relative hyper-reflexia ipsilateral to the side of weakness• +/- Babinski sign ipsilateral to side of weakness• +/- Hemiparetic gait
LEGEND
AD = Alzheimer’s dementia
FTD = Frontotemporal dementia
PSP = Progressive supranuclear palsy
CBD = Corticobasal degeneration
DLB = Dementia with Lewy bodies
PDD = Parkinson’s disease dementia
Rest tremor[VERY rare] +/- Rest tremor Rest tremor
Hypophonic hypokinetic spastic dysarthria Hypophonic hypokinetic dysarthria
• Supranuclear gaze palsy
• Slow saccade velocity• Wide-eyed stare• “Surprised” look
Slow initiation of saccades
Axial > appendicular rigidity Appendicular > axial rigidity
• Narrow to broad-based gait with knee extension
• Tend to pivot on turns
• Stooped posture• Narrow-based gait with decreased stride length• Decreased to absent arm swing
Postural instability[Early]
Postural instability[LATE]
UM
NPA
RK
INSO
NIS
M

Atypical Dementia �8Features of UMN Signs and Parkinsonism
Examination Findings Disorders to Consider
Upper Motor Neuron Signs
• Minimal atrophy• Pyramidal distribution weakness (weakness pattern: arms -
extensors>flexors; legs - flexors>extensors)• Hyperreflexia• Presence of a Babinski sign (extensor plantar response)• Asymmetry
• Cerebrovascular disease (stroke)• Corticobasal degeneration• Intracranial mass lesion
Parkinsonism
• Bradykinesia (all)• Bradyphrenia (all)• Masked facies (all)• Limitation/absent of downgaze ocular movement (PSP)• Rigidity ± cogwheeling - distinguish between axial (PSP) versus
appendicular (PD, DLB, CBD) rigidity• Rest tremor (not seen in DLB, PSP, CBD)• Fatiguing
• rapid alternating movements (finger tapping, opening/closing hands)• gait (festinating)• speech - progressive hypophonic speech
• Early postural instability (PSP)
• Parkinson’s disease with dementia (PDD)• Dementia with Lewy bodies (DLB)• Corticobasal degeneration (CBD)• Progressive supranuclear palsy (PSP)• Cerebrovascular disease

Atypical Dementia �9Neuroimaging Features of the Atypical Dementias
Alzheimer Disease Dementia with Lewy Bodies
Frontotemporal Dementia
Vascular Cognitive Impairment
Corticobasal Degeneration
Progressive Supranuclear Palsy
medial temporal>parietal
atrophy
near normal, minimal atrophy
frontal and temporal knife-edge atrophy
ischemic white matter changes (white areas) and strokes (black holes)
asymmetric hemisphere atrophy, caudate, putamen atrophy
midbrain, pons, superior cerebellar peduncle atrophy
Semantic Variant PPA Non-Fluent PPA Logopenic PPA
Focal left anterior inferior temporal lobe
atrophyLeft insular atrophy Posterior temporal-
parietal atrophy
Key Point MRI of the brain detects more subtleties on neuroimaging that CT and should be obtained.

Atypical Dementia �10
4. Interpretation of the Entire Information to Determine A Diagnosis
Example of Cases:
Initial Presentation Cognitive Profile Physical Exam Neurological Examination Disorder to Consider
Rapid forgetting Amnestic Normal (including vitals) Normal Alzheimer’s Disease
Slow, executive dysfunction, inattention
• Executive dysfunction• Slow
Signs of peripheral & cardiovascular disease Upper motor neuron signs Vascular Cognitive
Impairment
Visuospatial, slow, fluctuations
• Executive dysfunction• Slow• Visuospatial
Normal Mildly asymmetric appendicular parkinsonism
• Parkinson’s Disease with Dementia
• Dementia with Lewy Bodies
2134
History - Initial Presentation Cognitive Profile Physical Exam Cranial Nerves Motor
Examination Reflexes Gait Disorder to Consider
Visuospatial, slow, fluctuations
• Executive dysfunction
• Slow• Visuospatial
Normal NormalAppendicular
rigidity ± resting tremor
NormalSlow, narrow-based, short-
strides
• Parkinson’s Disease with Dementia
• Dementia with Lewy Bodies
• Anomia• Parkinsonism• Apraxia• Visuospatial
• Executive dysfunction
• Slow• Language• Apraxia• Visuospatial
Normal
• Normal• Slow initiation
of saccades with normal velocity
Asymmetric rigidity ±
unilateral UMN signs
HyperreflexiaBabinski sign
• Slow, narrow-based, short-strides
• Hemiparetic gait
Corticobasal Degeneration (Corticobasal
syndrome)
Early falls, executive
dysfunction
• Executive dysfunction
• Slow• Language
Normal
• Downgaze limitation
• Slow saccade velocity but normal initiation
Axial rigidity Normal
Narrow-based gait with early postural instability and retropulsion
Progressive Supranuclear
Palsy

Atypical Dementia �11
History - Initial Presentation Cognitive Profile Physical Exam Cranial Nerves Motor
Examination Reflexes Gait Disorder to Consider
Rapid forgetting Amnestic Normal (including vitals) Normal Normal Normal Normal Alzheimer’s
Disease
Visuospatial Visuospatial Normal (including vitals)
• Normal• Visual field cut• Visual neglect
Normal Normal Normal Posterior Cortical Atrophy (AD)
Anomia AnomiaAcalculia Normal Normal Normal Normal Normal
Logopenic progressive
aphasia (AD)
Slow, executive dysfunction, inattention
• Executive dysfunction
• Slow
Signs of peripheral &
cardiovascular disease
Normal UMN pattern of weakness
HyperreflexiaBabinski sign
• Normal• Slow,
decreased stride length
• Hemiparetic gait
Vascular Cognitive
Impairment
Behavioural changes (apathy or disinhibition)
• Normal• Executive
dysfunctionNormal Normal
• Normal• UMN pattern of
weakness• LMN pattern of
weakness
• Normal• Hyperreflexia• Babinski sign
Normal bv-FTD ± motor neuron disease
Anomia - circumlocution Anomia Normal Normal
• Normal• UMN pattern of
weakness• LMN pattern of
weakness
• Normal• Hyperreflexia• Babinski sign
Normal
Non-Fluent Primary
Progressive Aphasia (FTD) ±
motor neuron disease
• Anomia - loss of semantic knowledge
• Prosopagnosia
Anomia Normal Normal
• Normal• UMN pattern of
weakness• LMN pattern of
weakness
• Normal• Hyperreflexia• Babinski sign
Normal
Semantic Variant Primary
Progressive Aphasia (FTD) ±
motor neuron disease