Embed Size (px)
Citation preview

Leukemia Research Vol. 10, No. 12, pp. 1469-1475, 1986. 0145-2126/86 $3.00 + .00 Printed in Great Britain. © 1986 Pergamon Journals Ltd.
STANDARD CONDITIONING REGIMEN AND T-DEPLETED DONOR BONE MARROW FOR
TRANSPLANTATION IN CHRONIC MYELOID LEUKEMIA*
GIUSEPPE PAPA,~ WILLIAM ARCESE,t FRANCESCA ROMANA MAURO,t ALESSANDRA BIANCHI,t GIULIANA ALIMENA,t LIDIA DE FELICE,t
GIANCARLO ISACCHI,t DANIELA PASQUALE'I~rI,t FRANCO MALAGNINO,t MARIA PURPURA,§ GABRIELLA GIRELLIt and FRANCO MANDELLIt
tInstitute of Hematology, University "La Sapienza" and ~University "Tor Vergata', Rome, and §Laboratory of Histocompatibility, CNTS, Rome, Italy
(Received 6 March 1986. Revision accepted 9 July 1986)
Abstract--Between January 1984 to June 1985, 18 Ph 1 positive chronic myeloid leukemia (CML) patients in chronic phase (CP) underwent allogeneic bone marrow transplantation (BMT) from HLA identical and MLC negative siblings. The median age was 32.5 yr and median disease duration of CML at time of BMT was 19.3 months. The pretransplant conditioning regimen consisted of cyclophosphamide (CTX) (120 mg/kg) and 10.20 Gy total body irradiation (TBI) at 6 doses of 1.7 Gy each, administered in 3 daily fractions over 2 days at a dose rate of 15-20 cGy/ min. To prevent graft-vs-host disease (GvHD) we used methotrexate (MTX) in one patient and cyclosporin-A (CYA) in the other 17 patients, In addition to CYA, given until day +365, l0 patients received donor marrow depleted of T cells with CAMPATH-1. The residual marrow lymphocytes were always <1%. The rate of engraftment was significantly correlated with the number of nucleated cells infused. Neither GvHD nor graft failure were observed among CAMPATH-1 patients. In this group one cytogenetic and one hematologic relapse occurred. The overall actuarial survival at 24 months is 78%. Of the 10 patients treated with donor marrow depleted of T cells, 9 are alive after a median follow-up of 9 months (range 5-18), with an actuarial survival of 90%.
Of the other 8 patients transplanted with untreated marrow, 5 are alive after a median follow- up of 19.3 months (range 3.7-24) and the actuarial survival is 63.8%. This pilot study seems to demonstrate that T-cell depletion of donor bone marrow with CAMPATH-1 is effective to prevent GvHD, while the risk of graft failure can be avoided using a "standard" conditioning regimen including a fractionated TBI with a fast dose rate and a prolonged administration of CYA at the maximum tolerable dosage. While the high frequency of relapses suggests the employ of more aggressive anti-leukemic conditioning regimens in CAMPATH-I treated marrow recipients.
Key words: Bone marrow transplantation in chronic myeloid leukemia, T-cell depletion in bone marrow transplantation, GvHD prophylaxis with CAMPATH-1 and cyclosporin-A.
INTRODUCTION
ALLOGENEIC bone marrow transplantation (BMT) is an effective treatment for chronic myeloid leukemia (CML) in chronic phase (CP) [1-3]. Graft-vs-host dis-
* Supported by a grant of the Italian National Research Council, Special Project "Oncology", contract No. 85.02287.44.
Abbreviations: CML, chronic myeloid leukemia; CP, chronic phase; BMT, bone marrow transplantation; CTX, cyclophosphamide; TBI, total body irradiation; GvHD, graft- vs-host disease; MTX, methotrexate; CYA, cyclosporin-A; IP, interstitial pneumonitis.
Correspondence to: Giuseppe Papa, Cattedra di Ematologia, via Benevento, 6, 00161 Rome, Italy.
ease (GvHD) and associated complications are still major obstacles to successful transplantation despite HLA identical and MLC negative donor/recipient con- dition. A controlled randomized study from Seattle has shown no difference of cyclosporin-A (CYA) vs methotrexate (MTX) to reduce the incidence of GvHD and to improve the overall survival of transplanted CML patients [4].
However, standard prophylaxis with CYA seems to reduce the severity, but not the incidence, of GvHD and to promote the hemopoietic engraftment in leu- kemic and aplastic patients [5-7]. Several experiences with animal models [8-10] and, more recently, clinical trials [11-14] have demonstrated that T-cell depletion from the donor bone marrow protects recipient from GvHD. However several centres report an increase in
1469

1470 GIUSEPPE PAPA et al.
incidence of graft failure as an unexpected consequence of T-cell deplet ion, irrespectively of the methods employed. To ci rcumvent this severe inconvenience, more intensive condit ioning regimens have been used successfully in l imited series [15-17]. Nevertheless this approach can expose the patients to an increasing risk of infectious complicat ions, Particularly interstitial pneumonit is (IP).
This repor t presents the results of allogeneic B M T per formed during CP of p h i + C M L patients, con- dit ioned with a standard regimen and receiving T- depleted donor bone marrow plus C Y A to prevent G v H D . Analysis of these data have been compared with the results obta ined in a similar group of patients given C Y A alone.
M A T E R I A L S A N D M E T H O D S
Patients From January 1984 to June 1985 18 pH 1 positive CML
patients, 17 in first and 1 in second CP, received allogeneic BMT from HLA identical and MLC negative siblings. The age range was 16-44 yr (median 32.5 yr); disease duration of CML at time of BMT ranged from 6 to 123 months (median 19.7 months). All patients were previously treated with hydroxy- urea and/or busulfan, only one patient was splenectomized. One patient underwent allogeneic BMT during second CP of CML obtained by intensive chemotherapy (BAVC regimen) and infusion of cryopreserved autologous peripheral blood stem-cells [18]. Median age of the donors was 29.5 yr (range 13-44). Donor/recipient ABO-Rh status was incompatible in 6 cases.
Conditioning regimen The conditioning regimen consisted of cyclophosphamide
(CTX) (120 mg/kg b.w.) followed by 10.20 Gy fractionated TBI (F-TBI) at 6 doses of 1.7 Gy each, administered by linear accelerator in 3 daily fractions over 2 days at a dose rate of 15-20 cGy/min.
GoHD prophylaxis To prevent GvHD we used MTX in one patient, according
to the Seattle protocol, and CYA in the other 17 patients. CYA was given at the dose of 5 mg/kg intravenously from day -1 to day +5 and then at 12.5 mg/kg orally from day +6. The oral dose was continued at the maximum dosage, according to the renal function, until day +365.
In addition to CYA, the 10 most recently transplanted patients including the patient in second CP, received donor marrow in vitro incubated with a monoclonal rat anti-human lymphocyte antibody (CAMPATH-1) and autologous human complement to obtain T-cell depletion. Harvested bone marrow, containing 3.15-7.27 (mean 4.67 ± 1.39) nucleated cells x 108/kg recipient weight was suspended in RPMI 1640 liquid culture. A buffy-coat fraction of 240-250 ml was pre- pared by centrifugation using Haemonetics 30. The number of nucleated cells ranged from 1.37-3.7 x 108/kg (mean 2.46---0.72). Buffy-coat was treated with CAMPATH-1 100 Ixg/ml for 10 min at room temperature. As complement source, fresh donor serum was added to a final concentration of 20-25% v/v and incubated for an additional 30 min at 37°C. The treated marrow, containing 0.46--3.7 nucleated cells x 108/ kg (mean 2.03 ± 1), was infused into the recipient without any further procedure over 3 h. Lymphocyte depletion was evaluated using E-Rosette technique and indirect immuno- fluorescence with a panel of monoclonal antibodies: OKT3, OKT4, OKT8, LEU-7, LEU-9. The effect of CAMPATH-1 on bone marrow stem cells was tested by CFU-GM in agar cultures according to the Pike and Robinson technique.
Infection prophylaxis Reverse barrier isolation, gut decontamination with sterile
food and non-absorbable antibiotics, oral acyclovir, high dose intravenous immunoglobulins (sandoglobulin) and oral cotri- moxazole, were employed for prophylaxis against infections.
Statistical analysis Actuarial survival was calculated using the Kaplan and Meier
method and patient groups were compared using the long rank test. Chi-square test was used for comparison of groups of data. The incidence of the number of cells infused on the rate of engraftment was analysed using a standard linear regression model and the correlation coefficient between the two variables.
R E S U L T S
The analysis of data is repor ted comparing retro- spectively patients receiving bone marrow treated with C A M P A T H - 1 and patients given C Y A only for G v H D prophylaxis.
Effectiveness of lymphocyte depletion Table 1 shows the lymphocyte subpopulat ion analysis
of donor bone marrow treated with C A M P A T H - 1 and
TABLE 1. LYMPHOCYTE SUBPOPULATION ANALYSIS OF DONOR BM-TREATED WITH CAMPATH-1
Lymphocyte *Pre-CAMPATH-1 *Post-CAMPATH-1 markers Abs. No. x 10S/kg % Abs. No. x 108/kg %
E-Rosette 0.12 ± 0.03 28.4 ± 10.2 0.0013 --- 0.0023 0.25 ± 0.35 OKT3 0.14 ± 0.04 33.6 ± 14.9 0.0019 ± 0.0034 0.34 ± 0.48 OKT4 0.076 ± 0.02 17.2 +- 5.9 0.0008 ± 0.002 0.14 ± 0.3 OKT8 0.06 ± 0.02 14.5 ± 9.5 0.001 ± 0.0013 0.21 ± 0.21 LEU-7 0.02 ± 0.01 6.2 ± 3.9 0.0001 ± 0.0004 0.03 ± 0.1 LEU-9 0.1 ± 0.03 23.6 ± 9.2 0.0031 ± 0.003 0.57 ± 0.47
* Mean - S.D.; Abs. No. = absolute number.

T-cell depleted BMT in chronic myeloid leukemia 1471
the absolute number of T-cell subsets infused x 108/kg b.w. Lymphocyte depletion was documented in all cases and the percentage of residual lymphocytes was always <1%.
Engraftment Engraftment was assessed by increasing bone marrow
cellularity and rising peripheral blood counts. Cyto- genetic analysis showed a Ph 1 negative karyotype for all transplanted patients. Sex chromosome or red cell antigen differences confirmed the donor origin of engraftment in all 18 patients. The rate of engraftment was calculated as a number of days post-transplant to reach a neutrophil count of 0.5 x 109/1 or a platelet count of 50 × 109/1. The mean number of nucleated marrow cells infused was 2.26 - 0.9 x 10S/kg patient weight, without significant difference between recip- ients bone marrow treated or untreated with CAMP- ATH-I : 2.03 -+ 1 vs 2.56 --- 0.8 (p > 0.2).
Similarly, no difference was observed between the two patient groups for the mean number of CFU-GM x 105 infused/kg recipient weight: 0.86 -+ 0.8 vs 1.1 - 1.97 (p > 0.2). For all patients the rate of engraftment was 2 0 . 8 - 7.8 days (range, 11--41) for neutrophils and 22.3 - 10.8 days (range, 12-56) for platelets. Although CAMPATH-1 patients showed later engraftment than the other patient group, the difference was not stat- istically significant: neutrophils 23.3 --- 9.2 vs 17.1 - 3.8 days (p > 0.1); platelets 24.7 _+ 11.9 vs 19.5 --- 9.1 days @ > 0.2).
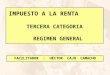
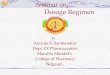
The number of nucleated bone marrow cells infused was significantly correlated to the rate of engraftment of both neutrophils (p < 0.01) (Fig. 1) and platelets (p < 0.05) (Fig. 2). No correlation between the number of CFU-GM infused and the rate of neutrophil (p > 0.1) and platelet (p > 0.1) engraftment was found. Finally no graft failure has been observed in all patients whose median follow-up is now 302 days (range 111-719).
Graft-vs-host disease GvHD was classified according to the Seattle criteria
[19]. Table 2 summarizes the incidence of acute and
TABLE 2. INCIDENCE OF GRAFT-VS-HOST DISEASE
CAMPATH-1 Yes No Total
GvHD Number patients 10 8 18
Acute-GvHD 0-I I0 4 14 (77.8%) II-IV 0 4 4 (22.2%)
*Number patients 6 7 13
Chronic-GvHD Limited 0 1 1 (7.6%) Extensive 0 2 2 (15%)
* Patients at risk to develop chronic-GvHD (>150 days).
40
i-
Z LU
It.
cr ~D
u~20 LU I
O
~0 10 >-
r~
~ O O
O •
O • • ~ O
o o
O Q •
I 2 3
N ° 8M CELLS x 10~Kg
FIG. 1. The relationship between the rate of neutrophil engraftment and the number of nucleated bone marrow cells infused. Correlation coefficient R =-0.627. Slope of line (-5.224) significant (p < 0.01). (C)) CAMPATH-1, yes. (0)
CAMPATH-1, No.

1472 GIUSEPPE PAPA et al.
50
I--
Z LU 3r
I'-- LL
(3E
(-9
Z i i i
LU T I'--
0 I - -
> -
40
30
20
10
o o
O O
o • .o •
1 2 3
N* BM CELLSxlO~/Kg
FIG. 2. The relationship between the rate of platelet engraftment and the number of nucleated bone marrow cells infused. Correlation coefficient R = -0.522. Slope of line (-5.97) significant (p < 0.05). (O) CAMPATH-1, yes. (0)
CAMPATH-1, no.
chronic GvHD. Neither advanced grade of acute-GvHD and chronic-GvHD were observed among recipients bone marrow previously treated with CAMPATH-1, while 4 out of 8 patients, given only CYA or MTX, presented I I - IV grade of acute-GvHD and 3 out of 7 developed chronic-GvHD. The difference between the two groups was not statistically significant but it becomes important considering that the CAMPATH-1 patients were significantly older than the others (median age: 35.5 vs 28 yr; p < 0.01).
CYA toxicity The most significant adverse side effect of CYA was
impairment of renal function, a complication that was usually transient and that occurred with a comparable frequency in both groups of patients.
We have observed also transient impairment of liver function, mild hypertension, neurologic abnormalities with no significant difference between the two groups.
Incidence of infections No significant difference between the two groups was
observed in regard to the incidence of bacterial, fungal and viral infections. Lethal IP related to cytomegalo-
virus infection occurred only in the patient on MTX prophylaxis and was associated with grade III acute- GvHD.
Leukemia relapse One hematological and one cytogenetic relapse have
been observed among the CAMPATH-1 patients. The first occurred in a male patient transplanted from his ABO incompatible sister. A day-20 post-BMT a 50% mixed chimerism was documented in the marrow and peripheral blood. Such condition was maintained until day-240 when CYA was discontinued. The following cytogenetic analysis at day-270 showed 100% Ph a posi- tive metaphases in the marrow with increasing per- ipheral blood counts. The second relapse, detected as 38% Ph 1 positive ceils in the marrow, was observed at day-175 in the patient transplanted with the lowest number of bone marrow nucleated cells (0.46 × 108/kg) and engrafted very late (day +51).
In this patient, at the appearance of the cytogenetic relapse, CYA was discontinued.
Mortality and survival Only one patient in the CAMPATH-1 group died of

T-cell depleted BMT in chronic myeloid leukemia 1473
%
1 0 0
_J ,¢¢
=>
LL O
5O >- p-
ro
m o
o.
C A M P A T H - 1 + C Y A I 10 pts
A L L P A T I E N T S 18 pts
C Y A 8 pts
_ 9 0 %
P = 0.2
. . . . 7 8 %
6 3 , 8 %
0 3 6 9 1; ) 15 le, 21 24
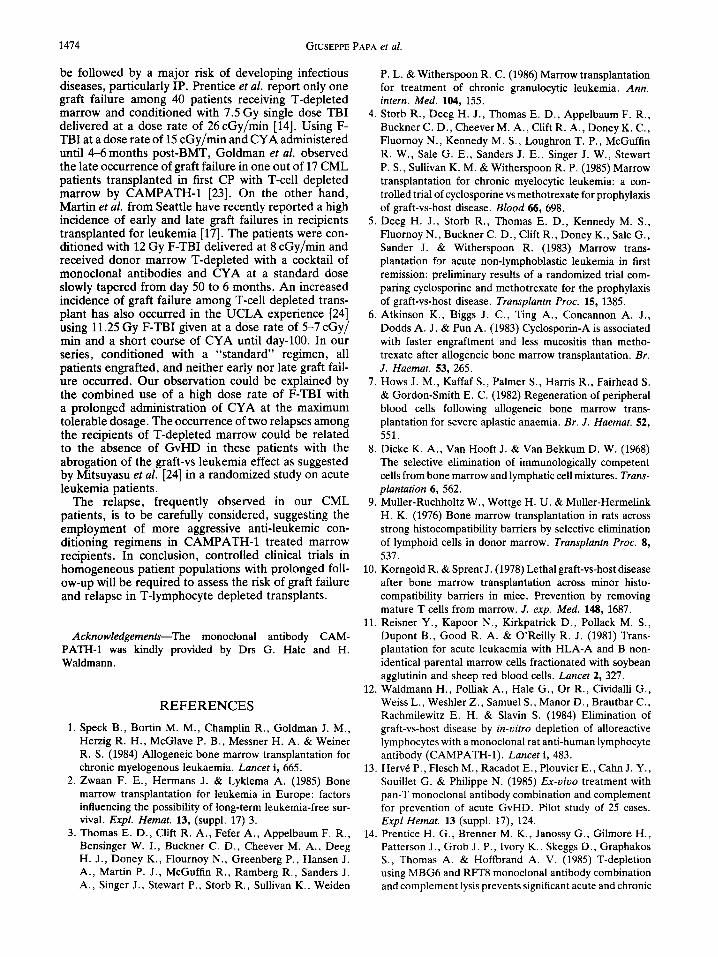
FIG. 3. Actuarial survival of 18 transplanted CML patients according to GvHD prophylaxis.
heart failure at day-153. In the other group the deaths occurred in 3 patients: 1 CMV related I.P. + A-GvHD (day-I l l ) , 1 Aspergillosis+ A-GvHD (day-168), 1 heart failure (day-210). 14 out of 18 patients are sur- viving at a median follow-up of 10 months (range 3.7- 24) with a Karnofsky score of 90-100%. The overall actuarial survival at 18 months is 78% (Fig. 3).
The median follow-up of patients receiving treated and untreated marrow is 9 months (range 5-18) and 19.3 months (range 3.7-24) respectively, with a cor- responding actuarial survival of 90 vs 63.8%.
The actuarial survival curves of the two patient groups are not strictly comparable, because the study is not randomized and the patients have been transplated during different time periods. However, at present the difference is not statistically significant (p = 0.2).
D I S C U S S I O N
This pilot study confirms the efficacy in vitro of CAMPATH-1 to induce lymphocyte depletion from bone marrow without any damage of stem-cells. In all cases a percentage of residual T lymphocyte less than 1% was obtained, a level considered crucial to prevent GvHD [20]. The use of autologous serum as comp- lement source and the short consuming time are two other advantages of this procedure. The analysis of engraftment showed that a late (but not significantly so) recovery of neutrophils and platelets is observed in the
CAMPATH-1 patients, although the mean number of nucleated cells infused was almost the same between the two patient groups. Such behaviour suggests that manipulation in vitro for T depletion could influence itself the rate of engraftment.
According to the data of Atkinson et al. [21] in leukemic patients, the lack of correlation between mar- row CFU-GM infused and neutrophil and platelet recovery in our CML patients confirms that CFU-GM assay is not a satisfactory method to assess the likelihood of engraftment. However, contrary to the authors above, we found that the number of nucleated cells infused is significantly correlated with the rate of engraftment.
No patients receiving T-depleted donor bone marrow in addition to CYA showed any sign of GvHD, while 4 out of 8 patients, treated with CYA or MTX alone, presented advanced grade of GvHD. This result is mostly relevant considering that CAMPATH-1 patients were significantly older than the others and thus at high risk of GvHD. Therefore we conclude that the depletion of T lymphocytes from donor bone marrow is effective to prevent GvHD, independently of recipient age. An increasing rate of graft failure represents a recent obser- vation in leukemic patients transplanted with T-lym- phocyte depleted marrow [17, 22]. This unexpected complication has led many centres to use more immu- nosuppressive conditioning regimens [15-17] based on the hypothesis that graft failure is due to host residual immunocompetent cells. However, this approach could
1474 GIUSEPPE PAPA et al.
be followed by a major risk of developing infectious diseases, particularly IP. Prentice et al. report only one graft failure among 40 patients receiving T-depleted marrow and conditioned with 7.5 Gy single dose TBI delivered at a dose rate of 26 cGy/min [14]. Using F- TBI at a dose rate of 15 cGy/min and CYA administered until 4-6 months post-BMT, Goldman et al. observed the late occurrence of graft failure in one out of 17 CML patients transplanted in first CP with T-cell depleted marrow by CAMPATH-1 [23]. On the other hand, Martin et al. from Seattle have recently reported a high incidence of early and late graft failures in recipients transplanted for leukemia [17]. The patients were con- ditioned with 12 Gy F-TBI delivered at 8 cGy/min and received donor marrow T-depleted with a cocktail of monoclonal antibodies and CYA at a standard dose slowly tapered from day 50 to 6 months. An increased incidence of graft failure among T-cell depleted trans- plant has also occurred in the UCLA experience [24] using 11.25 Gy F-TBI given at a dose rate of 5-7 cGy/ min and a short course of CYA until day-100. In our series, conditioned with a "standard" regimen, all patients engrafted, and neither early nor late graft fail- ure occurred. Our observation could be explained by the combined use of a high dose rate of F-TBI with a prolonged administration of CYA at the maximum tolerable dosage. The occurrence of two relapses among the recipients of T-depleted marrow could be related to the absence of GvHD in these patients with the abrogation of the graft-vs leukemia effect as suggested by Mitsuyasu et al. [24] in a randomized study on acute leukemia patients.
The relapse, frequently observed in our CML patients, is to be carefully considered, suggesting the employment of more aggressive anti-leukemic con- ditioning regimens in CAMPATH-1 treated marrow recipients. In conclusion, controlled clinical trials in homogeneous patient populations with prolonged foll- ow-up will be required to assess the risk of graft failure and relapse in T-lymphocyte depleted transplants.
Acknowledgements--The monoclonai antibody CAM- PATH-1 was kindly provided by Drs G. Hale and H. Waldmann.
R E F E R E N C E S
1. Speck B., Bortin M. M., Champlin R., Goldman J. M., Herzig R. H., McGlave P. B., Messner H. A. & Weiner R. S. (1984) Allogeneic bone marrow transplantation for chronic myelogenous leukaemia. Lancet i, 665.
2. Zwaan F. E., Hermans J. & Lyklema A. (1985) Bone marrow transplantation for leukemia in Europe: factors influencing the possibility of long-term leukemia-free sur- vival. Expl. Hemat. 13, (suppl. 17) 3.
3. Thomas E. D., Clift R. A., Fefer A., Appelbaum F. R., Bensinger W. I., Buckner C. D., Cheever M. A., Deeg H. J., Doney K., Flournoy N., Greenberg P., Hansen J. A., Martin P. J., McGuffin R., Ramberg R., Sanders J. A., Singer J., Stewart P., Storb R., Sullivan K., Weiden
P. L. & Witherspoon R. C. (1986) Marrow transplantation for treatment of chronic granulocytic leukemia. Ann. intern. Med. 104, 155.
4. Storb R., Deeg H. J., Thomas E. D., Appelbaum F. R., Buckner C. D., Cheever M. A., Clift R. A., Doney K. C., Fluornoy N., Kennedy M. S., Loughron T. P., McGuffin R. W., Sale G. E., Sanders J. E., Singer J. W., Stewart P. S., Sullivan K. M. & Witherspoon R. P. (1985) Marrow transplantation for chronic myelocytic leukemia: a con- trolled trial of cyclosporine vs methotrexate for prophylaxis of graft-vs-host disease. Blood 66, 698.
5. Deeg H. J., Storb R., Thomas E. D., Kennedy M. S., Fluornoy N., Buckner C. D., Clift R., Doney K., Sale G., Sander J. & Witherspoon R. (1983) Marrow trans- plantation for acute non-lymphoblastic leukemia in first remission: preliminary results of a randomized trial com- paring cyclosporine and methotrexate for the prophylaxis of graft-vs-host disease. Transplantn Proc. 15, 1385.
6. Atkinson K., Biggs J. C., Ting A., Concannon A. J., Dodds A. J. & Pun A. (1983) Cyclosporin-A is associated with faster engraftment and less mucositis than metho- trexate after allogeneic bone marrow transplantation. Br. J. Haemat. 53, 265.
7. Hows J. M., Kaffaf S., Palmer S., Harris R., Fairhead S. & Gordon-Smith E. C. (1982) Regeneration of peripheral blood cells following allogeneic bone marrow trans- plantation for severe aplastic anaemia. Br. J. Haemat. 52, 551.
8. Dicke K. A., Van Hooft J. & Van Bekkum D. W. (1968) The selective elimination of immunologically competent cells from bone marrow and lymphatic cell mixtures. Trans- plantation 6, 562.
9. Muller-Ruchholtz W., Wottge H. U. & Muller-Hermelink H. K. (1976) Bone marrow transplantation in rats across strong histocompatibility barriers by selective elimination of lymphoid cells in donor marrow. Transplantn Proc. 8, 537.
10. Korngold R. & Sprent J. (1978) Lethal graft-vs-host disease after bone marrow transplantation across minor histo- compatibility barriers in mice. Prevention by removing mature T cells from marrow. J. exp. Med. 148, 1687.
11. Reisner Y., Kapoor N., Kirkpatrick D., Pollack M. S., Dupont B., Good R. A. & O'Reilly R. J. (1981) Trans- plantation for acute leukaemia with HLA-A and B non- identical parental marrow ceils fractionated with soybean agglutinin and sheep red blood cells. Lancet 2, 327.
12. Waldmann H., Polliak A., Hale G., Or R., Cividalli G., Weiss L., Weshler Z., Samuel S., Manor D., Brautbar C., Rachmilewitz E. H. & Slavin S. (1984) Elimination of graft-vs-host disease by in-vitro depletion of alloreactive lymphocytes with a monoclonal rat anti-human lymphocyte antibody (CAMPATH-1). Lancet i, 483.
13. Herv6 P., Flesch M., Racadot E., Plouvier E., Cahn J. Y., Souillet G. & Philippe N. (1985) Ex-vivo treatment with pan-T monoclonal antibody combination and complement for prevention of acute GvHD. Pilot study of 25 cases. Expl Hemat. 13 (suppl. 17), 124.
14. Prentice H. G., Brenner M. K., Janossy G., Gilmore H., Patterson J., Grob J. P., Ivory K., Skeggs D., Graphakos S., Thomas A. & Hoffbrand A. V. (1985) T-depletion using MBG6 and RFT8 monoclonal antibody combination and complement lysis prevents significant acute and chronic

T-cell depleted BMT in chronic myeloid leukemia 1475
GvHD in HLA matched allogeneic marrow transplants. Expl Hemat. 13 (suppl. 17), 115.
15. O'Reilly R. J., Shank B., Collins N., Kernan N., Brochstein J., Keever C., Deansmore R., Kirkpatrick D., Castro-Malaspina H., Cunningham I., Flomenberg N. & Burns R. (1985) Increased total body irradiation (TBI) abrogates resistance to HLA-matched marrow grafts depleted of T cells by lectin agglutination and E-rosette depletion (SBA-E-BMT). Expl Hemat. 13, 406.
16. Or R., Weshler Z., Lugansy G., Steiner-Salz D., Galun E., Weiss L., Samuel S., Polliack A., Rachmilewitz E. A., Waldmann H. & Siavin S. (1985) Total lymphoid irradiation (TLI) as adjunct immunosuppressor for pre- venting late graft failure (LGF) associated with T-cell depleted marrow allograft. Expl Hemat. 13, 409.
17. Martin P. J., Hansen J. A., Buckner D., Sanders J. E., Deeg H. J., Stewart P., Appelbaum F. R., Cliff R., Fefer A., Witherspoon R. P., Kennedy M. S., Sullivan K. M., Flournoy N., Storb R. & Thomas E. D. (1985) Effects of in-vitro depletion of T cells in HLA-identical allogeneic marrow grafts. Blood 66, 664.
18. Papa G., Arcese W., Bianchi A., De Fabritiis P., Mauro F. R., Malagnino F., Meloni G., Pulsoni A., Sandrelli A., Amadori S. & Mandelli F. (1985) Sequential autografting and allogeneic bone marrow transplantation in a patient with chronic myeloid leukemia in blast crisis. Proc. ASCO 4, 610 (abstr.).
19. Thomas E. D., Storb R., Cliff R. A., Fefer A., Johnson F. L., Neiman P. E., Lerner K. G., Glucksberg H. &
Buckner C. D. (1975) Bone marrow transplantation. New Engl. J. Med. 292, 832, 895.
20. Hale G. (1986) personal communication. 21. Atkinson K., Norrie S., Chan P., Downs K. & Biggs J.
(1985) Lack of correlation between nucleated cell dose, marrow CFU-GM dose or marrow CFU-E dose and the rate of HLA-identical sibling marrow engraftment. Br. J. Haemat. 6, 245.
22. Slavin S., Waldmann H., Or R., Cividalli G., Naparstek E., Steiner-Salz D., Michaeli J., Galum E., Weiss L., Samuel S., Morecki S., Bar S., Brautbar C., Weshler Z., Hale G., Rachmilewitz E. A. and Reisner Y. (1985) Prevention of graft-vs-host disease in allogeneic bone marrow transplantation for leukemia by T-cell deple- tion in vitro prior to transplantation. Transplantn Proc. 1,465.
23. Goldman J. M., Apperley J. F., Jones L., Marcus R., Goolden A. W. G., Batchelor R., Hale G., Waldmann H., Reid C. D., Hows J., Gordon-Smith E., Catowsky D. & Galton D. A. G. (1986) Bone marrow transplantation for patients with chronic myeloid leukemia. New Engl. J. Med. 314, 202.
24. Mitsuyasu R. T., Champlin R. E., Ho W. G., Winston D., Feig S., Wells J., Terasaki P., Billing R., Weaver M. & Gale R. P. (1985) Prospective randomized controlled trial of ex-vivo treatment of donor bone marrow with mono- clonal anti-T cell antibody and complement for prevention of graft-vs-host disease: a preliminary report. Transplantn Proc. 1, 482.