Embed Size (px)
Citation preview

Journal of the Korean Radiologica l Society, 1994; 31(2) ; 301 -305
Staging of Advanced Gastric Cancer: Comparison of Conventional CT and Intraoperative Assessment1
Hyun Chul Rhim, M.D. , Yoon Young Choi , M.D., 0 Keun Bae, M.D.,
Jong Sung Kim, M.D., Byung Hee Koh , M.D.,
On Koo Cho, M.D. , Chang- Kok Hahm, M.D.
Purpose: We performed a retrospective study to compare the accuracy be tween conventional CT staging and intraoperative staging for advanced gastric cancer.
Materials and Methods: Sixty patients with advanced gastric cancer were included in this study during the recent 2 year-period. AII were pre- and postoperatively diagnosed as advanced gastric cancer. CTwas performed with G E 9800 and Somatom DR3 under conventional technique in 50 and with others in 10 referred patients. The CT staging for T and N category with emphasis on incurable factor , if not resected , were performed . And we compared the accuracy between conventional CT and intraoperative staging. The final histo-pathologic staging was used as a gold standard.
Results: Accuracy of CT and operation for T4(n=17) factor is 76.9 % and 86.2 % respectively. Overestimation rate for T4 was 9.3 % by CT and 6 .1 % by operation ,
and underestimation rate for was 13.8 % and 7.7 % respectively. Accuracy of CT and operation for N(n=60) factorwas 50% and 60% respectively. Overestimation rate for N factor was 18.3 % by CT and 18.3 % by operation , and underestimation rate for N factor was 31.7 % and 21.7 % respectively. Correct Tand N staging was possible only in 33% by CTand 38% by intraoperative assessment.
Conclusion: Conventional CT and intraoperative staging for incurable T/N factor in advanced gastric cancer have a potential limitations, especially for N fac tor . Therefore, more reliable modality or technique such as dynamic scanning by spiral CT, transabdominal or endoscopic ultrasonography should be preoperatively performed to complement infrequent errors in intraoperativestaging. Furthermore, a histology-oriented surgical approach seems essential in selecting the most appropriate surg ical procedure.
IndexWords: Stomach , neoplasms Stomach , CT Neoplasms, staging
INTRODUCTION
Accurate preoperative staging of gastric cancer is essential to plan appropriate treament whether it is surgical or non - surgical(1). However, accuracies of radiologic methods including computed tomography (CT) are still conflicting (2 , 6-16). Therefore , unneccessoryexpl이 aparotomy is still unavoidable.
'Department ofD iagnostic Radiology, Coll ege 01 Medicine, Hanyang University Received December8, 1993 ; Accepted June 20,1994 Address reprint requests to: Hyun Chul Rhim , M.D., Department 01 Diagnostic Radiology , College 01 Medicine, Hanyang University. 17, Haengdang-dong ,
Sungdong-ku ,Seoul , 133.792 Korea Tel. 82-2-293-2111 ,3111 Fax.82-2-291-9866
On the other hand , recent studies revealed frequent errors even in intraoperative assessment which has been considered as the most reliable and final staging method (16 -19). And Japanese Stomach Cancer Study Group is recently emphasing the importance of curative resection and proposing the criteria of incurable factor , if not resected , in gastric resection(20).
In this study , we compared the accuracy of conventional CT and intraoperative staging for advanced gastric cancer with final patholog ic staging as a gold standard.
MATERIALS and METHODS
In a 26 - month period , we retrospectively studied 60
- 301 •

Journal 01 the Korean Radiologica l Society, 1994; 31(2) : 301 - 305
patients who had pathologically proved adenocar cinoma of stomach. They consisted of 37 men and 23 women (mean age ; 54 yeras , range ; 27 - 81 years). CT scans were performed with either GE 9800 (General Electric , Milwaukee, U. S. A.) in 38 patients or Somatom DR3 (Siemens, Erlangen , Germany) in 12 patients , and with other third generation CT scanners in 10 referred patients. Scanning variables were 120 kVp , 240 mA, scanning time 2 sec for GE 9800 system and 125 kVp , 350 mA, scanning time 4 secfor Somatom DR3. Ten - millimeter thick contiguous sections with 3 mm interval were acquired from the diaphragm to the iliac crest. AII of 50 inpatients received contrast medium [a bolus 50 ml and a drip infusion 100 ml of Ultravist 300 (Schering , Germany)] intravenously. AII of 50 inpa- tients received contrast medium (500 ml water in 38 patients , 500 ml Gastrografin in 12 patients) orally before the CT procedure.
AII CT scans were reviewed in respect to depth of invasion of primary lesion and Iymph node metastasis by two radiologists (H. C. R. , Y. Y. C.). Especially we focused on the incurable T/N factor (T4 or any N) , if not resected , according to criteria of curative resection by Japanese Research Society for Gastric Cancer (20). T4 criteria on CT was defined as obliteration of fat plane between primary lesion and adjacent organ. T2 and T3 were considered as a single category because differentiation of two was very difficult by conventional technique. Total number of T lesions was 65 in 60 patients , including double T41esions in 5 patients.
Lymph node metastasis were evaluated as following criteria ; NO (No metastasis) , N1 (perigastric Iymph nodes), N2(left gastric , common hepatic, splenic , celiac artery Iymph node) , and > N2(the other intraabdominal Iymph nodes). Lymph nodes were considered positive if they exceed 10 mm in greatest diameter. The results of CT and intraoperative surgical staging for
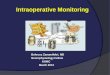
Fig .1 . Hepatic invasion Contrast-enhanced CT scan shows obliteration 01 lat plan e (white arrow) between 01 gastric mass and lateral segment 01 liver with adjacent locallow-attenuation lesion (b lack arrow); true positive on CT and operation
T/N factor were compared with final histo -pathologic staging.
RESULTS
Accurate estimate for T4 factor was possible in 76.9 % by CT and 86.2 % by intraoperative staging(Fig. 1) Overestimation rate for T4 was 9.3 % by CT and 6.1 % by operation , and underestimation rate was 13.8 % and 7.7 % respectively (Table 1 )(Fig. 2, 3) . Pathologically proven T4 factors were invasion to pancreas(n= 10) , transverse colon(n= 5) , and liver(n = 2)(Fig. 2, 3) . Estimation of N status was accurate in 50 % by CT and 60 % by intraoperative staging. Overestimation rate for N was 18.3 % and 18.3 %, and underestimation rate was 31 .7 % and 21.7 % respectively (Table 2)(Fig. 4). Correct T and N staging was possible in 33 % by CT and 38% by intraoperative assessment (Table 3).
DISCUSSION
An accurate preoperative staging of the most important prognostic factor of gastric cancer , such as depth of
invasion(T) and Iymph node metastasis(~ιfor pl anning of appropriate treatment(1) , because over
estimation may result in an unduly conservative operation and reduce the likel ihood of cure, whereas underestimation may lead to inappropriate radical surgery with risk(13)
The previous reports on the accuracy of conventional CT staging is somewhat conflicting(6 -16). Five out of twelve papers revealed pessimistic conclusions for CT’s role(2 , 13 -16) , while seven found CTto be useful(6 -12). Major limitations of these optimistic data lie in retrospective evaluation with small sized materials and comparison with intraoperative surgical assessment as a gold standard. But recent prospective studies using pathologic staging as a gold standard has shown the low accuracy of conventional CT and intraopertive staging(19). Our data has shown the agreement with recent pessimistic views for the role of pre operative conventional CT staging(2 , 13 -16). Their accuracies for T and/or N categories ranged from 45 % to 56 %, which were comparable with ours.
Accuracy for T in our study seems to be higher than
Table 1 . Staging lor T Factor : CT versus Operation
CT
T2 /3 T4
42 6
9 8
76.9 9.3
13.8
4 10
86.2
6.1
7.7
OPERATION
T2 /3 T4
PATHOLOGY (n) T2 / 3(48)
T4 (17)
Accurate( %)
Overstage( %)
Understage( %)
46 5
U 「j

Hyun Chul Rhim, et al : Stagin g of Advanced Gastric Cancer
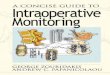
a b Fig. 2 . Pancreatic invasion
a. Contrast-enhanced CT scan shows obliteration 01 lat plane (arrows) between gastric wall and pancreatic head ; lalse positive on CT and true negative on operation
b. Contrast-enhanced CT scan shows ob literation 01 lat plane (arrows) between gastric wall and pancreatic head ; true positive on CT
and lalse negative on operation
a b Fig. 3 . Transverse colon invasion
a. Contrast-enhanced CT scan shows suspicious colonic wall thickening (arrowheads) without signilicant adjacemt omental inliltration
probably due to collapsed bowel ; lalse negative on CT and true positive on operation
b. Contrast-enhanced CT scan shows suspicious colonic wall thickening (arrows) with prominent adjacemt omental inli ltration prob-
ably du e to colonic invasion ; lalse positive on CT and true negative on operation
those of previous studies , because we excluded early Table 2 . Staging for N Factor: CT versus Operation
gastric cancer and considered T2 and T3 as single CT OPERATION category due to difficulty of differentiation between T2
NO N1 N2 ) N2 NO N1 N2 ) N2 and T3 by conventional C T. The criteria for T4 factor by
CT is not reliable because the source of errors is un- PATHOLOGY (n)
avoidable ifthe patients is emaciated or the perigastric NO( 6) 5 0 0 2 2 o 2
inflammation around tumor is present. Endoscopic N1 (24) 7 8 7 2 3 16 4
ultrasonography for T4 factor by Ziegler et al(19) N2(17) 0 5 11 4 10 2
revealed high sensitity(89%) , compared with conven- N3(13) 0 6 6 0 3 2 8
tional CT(44%) and intraoperative surgical assess- Accu rate( %) 50.0 60.0 ment(22 % ). Overstage( %) 18.3 18.3
Accuracy of conventional CT for overall N staging ac-Understage( %) 31.7 21 .7
cording to NO, N1 , N2, and ) N2 was 50 % , which was
m
ω
X 」

Journal of the Korean Radiological Society, 1994 : 31(2) : 301 - 305
a b Fig. 4. Lymph node metastasis a. Contrast-enhanced CT scan shows equivocallow - attenuation lesion(arrow) , considered as partial volume effect of pancreas ; false negative celiac nodes on CT and true positive on operation b. Contrast-enhanced CT scan shows 1.5 cm sized , ovoid low - attenuation lesion adjacent to portal vein(arrow) ,suggested as hepatoduodenallymph node ; true positive hepatoduodenal node on CT and false negative on operation
similar to other results. But our results revealed high underestimation rate in contrast to other reports(12 , 19). It is suggested that the criteria of Iymph node involvement could have influenced on the difference. It deems neccessary to define more sophisticated criteria other than size category , including shape, multiplicity , inter- nal texture , or relation to the tumor mass.
Another purpose of this study is to assess the re-liability of intraoperative surgical assessment. Intraoperative estimation of tumor infiltration and Iymph node metastases usually serve as major guidelines for decision about which operation should be performed in patients with gastric carcinoma. Type and magnitude of errors of intraoperative surgical staging in gastric cancer might be negligible if preoperatively conventional diagnostic procedures such as UGI , endoscopy, ultrasonography, CT were able to give a reliable information on extent of tumors(17). Recent studies by Rhode , Madden , or Ziegler pointed outthe possibility of errors in intraoperative staging by comparing with histo - pathologic staging as a gold standard (16 -19). Rhode described that su rgical errors in staging depended on innumerable factors ; 1) . surgeon ’s attitude towards staging 2) type of standardization or methods 3) difficulty to differentiate not advanced from more advanced at laparotomy and to ascertain the degree of invasiveness of advanced tumors 4) difficulty or, rather impossibility of differention between invaded and non - invaded structures , especially ifthere is a lot of inflammatory tissue surrounding the primary tumor (1?). Our data, which showed low accuracy with considerable over - or underestimation rates of intraoperative staging , support their opinion . Therefore , intraoperative staging alone could be insufficient in selecting the best surgical procedure for i ndividual patient(19)
Table 3. Staging for T and N Factor
T + N
CT Operation
Accurate (%) 32.0 % 38.5 %
Overstage (%) 26.0 % 20.0 %
Understage (%) 42.0 % 41 .5 %
This study showed two points; 1) the significant limitations were found in accurate T/N staging for gastric cancer by conventional CT, similar to recent pessimistic results , 2) the considerable errors are possible by intraoperative assessment without standardized frozen section
In conclusion , conventional CT staging in advanced gastric cancer has potential limitations as well as intraoperative surgical assessment. Therefore , more reliable modalities or techniques such as dynamic scanning by spiral CT, high - resolution transabdominal , or endoscopic ultrasonography are required to complement a possible errors in intraoperative macrospcopic staging. Furthermore , histology - oriented surgical approach with standardized frozen sections ofT/N factor during operation seems essential for selecting the most appropriate surgical procedure , whether the aim of operation is curative or pall iative
REFERENCES
1. BoddieAJr ‘ McBride CM , Balch CM. Gastric cancer. Am J Surg
1989 : 1 57 : 595-606 2. Andaker L, Morales 0 , Hojer H, Backstrand 8, 80rch K,Larsson
J. Evaulation of preoperative computed tomography in gastric mal ignancy. Surgery 1991 : 1 09: 132-135
304 -

Hyun Chu l Rhim, et al : Staging of Advanced Gastric Cancer
3. Meyers WG, Daniano RJ, Postlethwant RW. Adenocarcinoma 01 12 손경명, 하현권, 차은축, 박조련 , 김인철 , 심경섭, 박용후| 위암의 림프
the stomach: changing patterns over the last lour decades. Ann 절 병기 평가에 있어서 CT의 유용성 대한방사선의학회지 1992 ;28
Surg 1987 ; 205: 1-8 728-732
4. Bozetti F, Bonlanti G, Audisio Ra, etal. Prognosis 01 patients after 13. Cook AO‘ Levine BA, Si rinek KR , Gaskill HV. Evaluation 01 gastric
palliative surgical procedures lor carcinoma 01 stomach. Surg adenocarcinoma. Arch Surg 1986 ; 121 : 603-606
Gynecol Obstet 1987 ; 164 : 151-154 14. Sussaman SK , Halvorsen RA, IIlescas FF, et al. Gastric adeno-
5. Nalen B, Viste A, Haugstvedt T, Eide GE, Soereide O. Treatment carcinoma: CT versus surgical staging. Radiology 1988 ; 167
01 stomach cancer‘ national experience. Br J Surg 1988 ; 75: 335-340
708-712 15. Komaki S, Toyshima S. CT’5 capability in detecting advanced
6. Moss AA , Schnyder P, Marks W, Marg비 is AR. Gastric adeno- gastriccancer. Gastrointest radio/1983 ; 8: 307-313
carcinoma: a comparison 01 the accuracy and economics 01 16. Fraser 1, Nasch R, James DC. Computed tomography in gastric
staging by computed tomography and surgery. Gastroentero- cancer. Br J Surg 1985 ;72 ’ 248-250
logy 1981 ; 80: 45-50 17. Rohde H, Köster R, Gebbensleben B, Stützer H, Rau E Errors 01
7. Balle DM , Koehler RE, Karlstaedt N, Stanley RJ , Sagel SS. surgical staging in patients with cancer 01 the stomach. Scand J
Computed tomography 01 gastric neoplasm. Radiology 1981 Gastroentero/1987 ; 22: 27-30
140:431-436 18. Madden MV, Price SK, Learmonth GM , Dent DM. Surgical
8. Dehn TCB ‘ Rezek IB , White FE. The pre-operative assessment 01 staging 01 gastric carcinoma: sources and consequence 01
advanced gastric cancer by computed tomography. Br J Surg errors. Br J Surg 1987 ; 74 : 119-121
1984 ;71 :413-417 19. Ziegler K, Snaft C, Zimmer T, et al. Comparison 01 computed-
9 서형심 , 이재섭 , 이종진 등 위암환자에 있어서 전산화 단층촬영술의 tomography, endosonography, and intraoperative assessment
진단적 으|의 대한방사선의학회지 1985 ; 21 : 105-113 in TN staging olgastric carcinoma. Gut1993 ; 34: 604-61 0
10 신지열, 심전섭 , 김병영 등 전산화단층촬영술에 의한·우|암의 수술전 20. Japanese Research Society lor Gastric Cancer. The general
병기결정의 의의 대한방사선의학회지 1989 ;25:741-747 rules 01 gastric cancer study 12th ed 金原出版械합會社 1993 ;
11 노병석 , 임 덕 , 김기환등 CT를이용한위암의훼장침습에대한판정 32-33
대한방사선의학회지 1990 ; 26 : 1 02-1 06
대한방사선의학회지 1994; 31(2): 301-305
진행성 위암에 대한 병기결정 :고식적 CT와 수술상 병기결정의 벼교
한양대학교 의과대학 진단방사선과학교실
임현철·최윤엉·배오근·김종성·고병희·조온구·합창곡
목 적:진행성 위암의 병기결정에 있어서 비절제시 치유불가인자로 알려진 T4및 N을중심으로 고식적 CT 및 수술상의 병
기결정의 성적을 후향적으로 비교하여 술전 및 술중 병기결정의 유용성 및 문제점을 알아보고자 하였다.
방 법 . 최근 2년동안 진행성 위암으로 진단받아 위절제술을 받았던 60명의 환자를 대상으로 하여 고식적 CT검사상 및 수
술중 육안적으로 평가한 병변의 침윤도(T)와 임파선 전이 정도(N)에 대하여 후향적으로 평가하여 이를 최종병리학적 병기
를 기준으로 각각의 정확도를 비교분석하였다.
결 과 : 병변의 침윤도에 대한 즉, 인접장기 침범 (T4)에 대한 CT 및 술중진단의 정확도는 각각 76.9 % , 86.2 % 였으며, 과
대평가는 9.3 %. 6.1 % 였고 과소평가는 13.8 %. 7.7 % 였다. 임파선 전이정도(N)에 대하여 CT 및 술중진단의 정확도는 각
각 50 %와 60 %였고 과대평가는 공히 18.3 % 과소평가는 각각 3 1.7 % 와 2 1.7 % 였다. 한편 병변의 침윤도 및 임파섣 전이
정도를 모두 정확히 평가가 가능했던 경우는 CT로는 33%에서 술중에서는 38%에서 가능하였다.
결 론:고식적 CT어| 의한 진행성위암의 병기결정은 비절제시 치유불능인자로 여겨지는 주변장기로의 침범유무(T4)에 대
해서는 어느정도의 유용성을 견지하고 있으나 임파섣 전이의 평가에 있어서는 낮은 정확도를 보였고, 이러한 문제점은 최종
병기결정 방법인 술중 병기 평가상에서도 내재되어 있음이 확인되었다. 따라서 현행의 고식적 CTOI상의 보다 신뢰도 높은
술전 방사선학적 진단법으로의 전향이 필요하며,술중 병기결정의 정확도의 향상을위한다각적인 노력도이어져야 할것으
로판단한다.
%

1994년도 춘계학술대회 증례퀴즈( III )
Case 4. F/30 C.C. ; intermittent neck pain since
2 months ago
Answer ; neurenteric cyst of C-spine
- 306