Embed Size (px)
Citation preview

Staging in Cancer: Order out of Chaos
Lily L. Lai, MD, FACSChair, Clinical Cancer Committee
City of Hope

Life

The one thing that (scientists) do not and must not tolerate is disorder. The whole aim of theoretical science is to carry to the highest possible and conscious degree the perceptual reduction of chaos that began in so lowly and (in all probability) unconscious a way with the origin of life.
George Gaylord Simpson (Principles of Animal Taxonomy, 1961)

Cancer

Outline
• History• Rationale• Application• Types of Staging• Future

Cuthbert Dukes
Pierre Denoix
History
Frederic Greene
Mahul Amin

Dukes1932
A B C
+LNs

Astler & Collier1954
+ LNs
A B2B1 C1 C2

Tis T1 T2 T3 T4
TNM1968

Staging: why?
• Cancer care expectations– To aid the clinician in planning treatment– To give some indication of prognosis– To assist in evaluating the results of treatment– To facilitate the exchange of information
between treatment centers– To contribute to continuing investigations of
human malignancies
UICC, 1958AJCC Cancer Staging Manual (v. 7), 2010

Staging: Why?
• Institutional requirements– American College of Surgeons, Commission on
Cancer, Clinical Cancer Program• Standards for evaluation of cancer clinics since 1931• Accreditation of institution as providing quality
cancer care• Surveys of programs conducted every 3 years
– Standards of the ACoS, CoC specific to Staging• 90% of cases are correctly staged• Clinical staging occurs preoperatively, pre-treatment• Completed staging (Collaborative Stage) within 4
months of initiating treatment

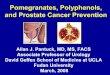
The three axes of cancer classification
Topographic site Location can change patterns of progression
Rectal v. colonHead and neck v. lung
HistologyKind of cell responds to different treatments
Nonsmall cell lung ca v. small cell lung cancerMelanoma v. basal cell cancer of the skin
Anatomic extent (Staging)
Degree of local and systemic involvement
Topographic site(disease site)
Histologic type
Anatomic extent(TNM)
Patient’s Disease

Anatomic Staging
• Based on three components
T The extent of the primary tumor
N The absence or presence and extent of regional lymph node metastasis
M The absence or presence of distant metastasis
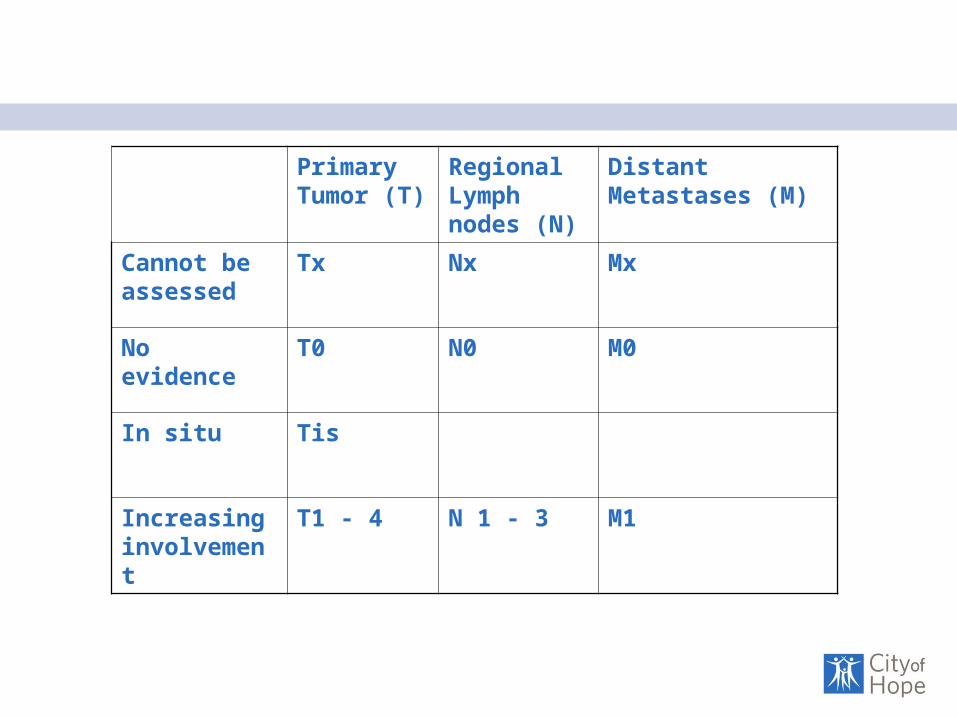
Primary Tumor (T)
Regional Lymph nodes (N)
Distant Metastases (M)
Cannot be assessed
Tx Nx Mx
No evidence
T0 N0 M0
In situ Tis
Increasing involvement
T1 - 4 N 1 - 3 M1

Tumor (T)
• cT can be based on palpation or imaging• pT requires adequate resection of tumor • If tumor is removed in pieces, an effort at reconstruction
is needed to approximate the native size prior to manipulation (add the pieces together)
• In cases with > 1 tumor in the same site, the tumor that is the highest T category is used and a parenthesis after T is used to designate multiplicity: T1 (m) or T1 (3)
• In cases with simultaneous bilateral tumors, each tumor is staged – as independent tumors (breast) – as metastasis (lung)
• Unknown primary is based on clinical suspicion of primary origin and is designated T0 (not Tx)

Tumor (T): Breast Cancer
>5 cm tumor
T1 T2 T3 T4

Tumor (T): Colorectal Cancer

Tumor (T): Lung Cancer
T1 T2
T3
T4

Accurate T-staging predicts outcome
Staging outcomes AJCC v. 6
Staging outcomes AJCC v. 7

Regional Lymph Nodes (N)
• pN entails removal of a sufficient number of LNs to ensure appropriate staging– Colon (>12)– Gastric (>16)
• If number of LNs reveals negative nodes but the total < suggested LN dissection, then N = pN0– May affect treatment
• Sentinel lymph node assessment is appropriate in some sites (breast, melanoma)
• Isolated tumor cell clusters (ITC) (< 0.2mm, less than 200 cells) are staged as N0(i+)
• Micrometastases (> 0.2 mm, <2 mm, more than 200 cells) are staged as N1mi– Breast T0-1,N1mi = St. 1B

Nodes (N)

Absolute number of positive LNs predict survival
Greene, CA Cancer J Clin 2008; 58:180-90
T1, 2, N1T3, 4, N1any T, N2

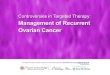
Total number of LNs removed predicts survival
Greene, CA Cancer J Clin 2008; 58:180-90

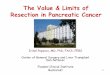
Location of lymph nodes removed predicts survival
NX Regional node cannot be addressed
N0 No regional lymph node metastases
N1 Metastasis in ipsilateral peribronchial +/- ipsilateral hilar and intrapulmonary nodes, including direct extension
N2 Metastasis in ipsilateral mediastinal +/- subcarinal nodes
N3 Metastases in contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular nodes

Metastasis (M)
• Metastasis can be staged clinically (cM) or pathologically (pM)
• cM is adequate if T and N have meet pathologic staging – Biopsy of metastasis not absolutely needed
• If metastasis has tissue diagnosis, then pM • If metastasis identified, any T and any N is
acceptable including TX, NX, M1

Metastases

Stage Grouping
STAGE
0
T
is
N
-
M
-I + - -
II + +/- -
III +/- + -
IV +/- +/- +

Descriptors
Indication
Suffix m Presence of multiple primary T
pT(m)NM
Prefix y Post initial treatment (staging after preop treatment)
ycTNM or ypTNM
r Recurrent tumor after a disease free interval
rTNM
a Autopsy aTNM

Other factors
• Histopathologic subtype– Adenocarcinoma, SCCA
• Histology/Grade– Poor, mod, well differentiated– Undifferentiated
• Lymphovascular invasion• Residual tumor
– RX, R0 – 2 resections• Site-specific factors
– Breast: ER, PR, Her2-neu– Thyroid: Age– CRC: Microsatellite instability, MMR, K-ras status– Prostate: PSA, Gleason’s Score

Site specific factors: Prostate Cancer
STAGE
T N M PSA Gleason
I T1a-cT2aT1-2a
N0N0N0
M0M0M0
< 10< 10X
< 6< 6X
IIA T1a-cT1a-cT2aT2bT2b
N0N0N0N0N0
M0M0M0M0M0
<20< 10, <20<20<20X
7< 6< 7< 7X
IIB T2cT1-2T1-2
N0N0N0
M0M0M0
Any >20 Any
AnyAny>8
III T3a-b N0 M0 Any Any
IV T4Any TAny T
NON1Any
M0M0M1
AnyAnyAny
AnyAnyAny

Clinical, Pathologic, Collaborative Staging
• Clinical (cT, cN, cM)– Before initiation of primary treatment– Important in deciding primary treatment
• Pathologic (pT, pN, pM)– From resected tissues
• Collaborative (CS)– Clinical, pathologic staging AND nonanatomic
(site-specific) factors• Implemented by the cancer registries• Stage derived through computer algorithms

Collaborative staging: example
• 65 yo male with cT3, cN0 colon cancer• Preoperative imaging does not
demonstrate metastasis, cM0• Patient undergoes resection• Pathology is pT3N1
– Pathology cannot really decide if M0, especially when no specimen was sent for evaluation of metastases
• Collaborative stage is: T3N1M0 – Stage IIIA
• The “STAGE” is a combination of pathologic and clinical findings

NCCN Guidelines Version 3.2012Colon Cancer
PATHOLOGIC STAGE SURVEILLANCEADJUVANT THERAPY
T1-3, N1-2, M0Or T4, N1-2, MO
History and PE every 3 – 6m for 2 y, then every 6 m for a total of 5yCEA every 3 – 6m for 2 y, then every 6 m for a total of 5yChest/abdominal/pelvic CT annually x 3 -5yColonoscopy in 1y except if no preoperative colonoscopy due to obstructing lesion, colonoscopy in 3-6m; if advanced adenoma, repeat in 1y; if no advanced polyp, repeat in 3y, then every 5 yPET-CT scan is not reoutinely recommendedSee Principles of Survivorship
FOLFOX (category 1) preferredOther options include:FLOX (category 1)OrCapeOx (category 1)OrCapecitabine Or5FU/Leucovorin
COL-4

Changes in 2010
• Revision cycle = 6 – 8 years– AJCC Cancer Staging Manual (Version 7), published Nov 2009
• Applied to cancer cases from January 2010
– AJCC Cancer Staging Manual (Version 8), published in late 2015• Applied to cancer cases from January 2016
• Lung– T subcategories (T(n) a,b)– Nodes by zones (not specific nodal stations)– Contralateral disease = M1a
• Colon– N subcategories (N1a – c; N2a - b)– M subcategories (M1a – single site, M1b – multiple sites)
• Breast– Stage I subcategories (IA, 1B – includes LN with micrometastases)

Limitations of Staging
• Not used in hematologic malignancies– Ann Arbor Staging System
• Not used in pediatric cancer• Not useful in rare diseases
– Not enough cases to stratify T, N, M• Merkel Cell Cancer
– Lumping different histopathologic subtypes• Soft tissue sarcoma: multiple histologies
• Dominated by anatomic pathology and histology (size, nodes, histopathology, grade)– Gradually incorporating other prognostic variables

Future of staging
• Refined clinically– Number of lymph nodes in CRC– Ulceration in melanoma
• Molecular markers– Microarray research to determine prognosis
based on patterns– Oncotype DX in breast cancer, in CRC
• Post treatment staging vs. pretreatment staging– Rectal cancer – does pretreatment staging
matter if the patient has a complete pathological response to chemoradiation?
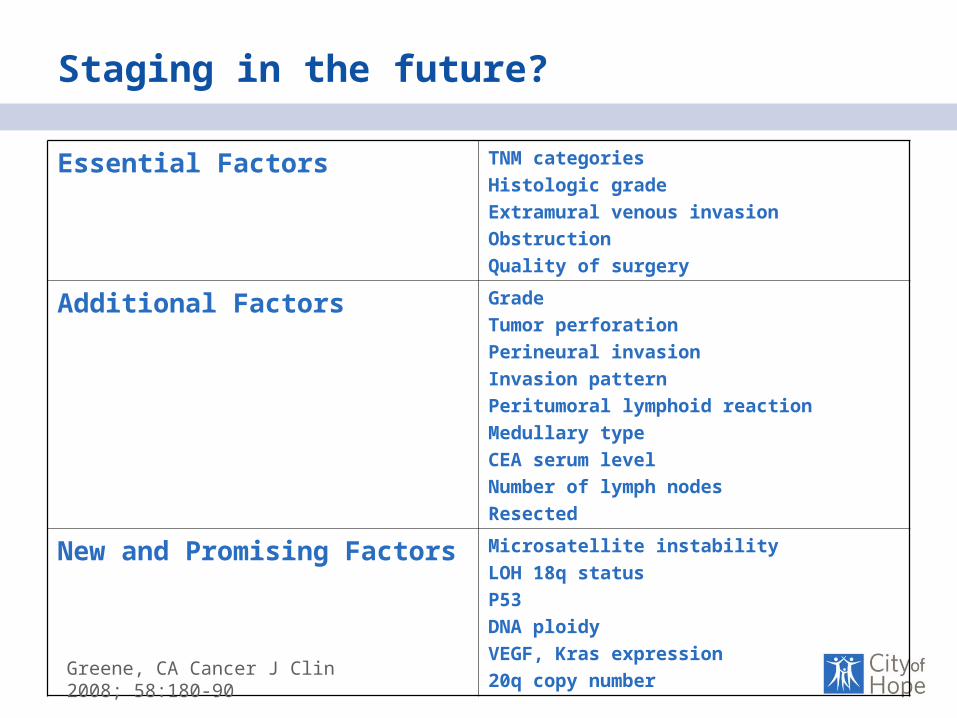
Staging in the future?
Essential Factors TNM categoriesHistologic gradeExtramural venous invasionObstruction Quality of surgery
Additional Factors GradeTumor perforationPerineural invasionInvasion patternPeritumoral lymphoid reactionMedullary typeCEA serum levelNumber of lymph nodesResected
New and Promising Factors Microsatellite instabilityLOH 18q statusP53DNA ploidyVEGF, Kras expression20q copy number
Greene, CA Cancer J Clin 2008; 58:180-90
Responsibilities
• Completion of forms – Accurate– Timely
• Completed staging within 4 months of initial treatment• Clinical staging before patient receives initial
treatment– Attendings must sign and are ultimately responsible – in
particular for the clinical staging
• Use of patient stage in notes, presentations
• Use of Stage in multidisciplinary conferences– References to NCCN guidelines in treatment
Never wonder. By means of addition, subtraction, multiplication, and division, settle everything somehow.
Charles Dickens, Hard Times, 1853

Acknowledgements
Ina Ervin, Registrar (Emeritus)Kelli Olsen, RegistrarCOH Tumor Registry
ACS, Commission on Cancer
National Comprehensive Cancer Network

References
• Gunderson LL et.al. Revised Tumor and Node Categorization for Rectal Cancer Based on Surveillance, Epidemiology, and End Results and Rectal Pooled Analysis Outcomes, JCO Jan 10, 2010:256-263; published online on November 30, 2009
• Kligerman, S. and G. Abbott (2010). "A Radiologic Review of the New TNM Classification for Lung Cancer." Am. J. Roentgenol. 194(3): 562-573.
• AJCC Committee, AJCC Staging Manual, Version 7, Springer-Verlag, 2009.
• Greene FL. The Staging of Cancer: A Retrospective and Prospective Appraisal, CA Cancer J Clin 2008;58;180-190
• http://www.nccn.org/professionals/physician_gls/f_guidelines.asp