Embed Size (px)
Citation preview

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e1
ST-Segment Monitoring
Self-Learning Package

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e2
Developed by: SBH Cardiac Sciences/Critical Care Clinical Educators
Reviewed and Revised by: The Regional Critical Care Policy and Procedure
Committee

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e3
Table of Contents:
Purpose, Objectives and Instructions 4
Normal Cardiac Cycle Review 5
Clinical Conditions for ST-Segment Monitoring 6
Lead Placement 6
Ensuring ST-Segment Accuracy 7
Considerations with ST-Segment Monitoring 7
What to do if ST-Segment Changes are Noted 8
What to Document and Where 8
In Summary 9
Reference 9
Appendix A: Philips Monitor Setup 11
Appendix B: Spacelabs Monitor Setup 13
Appendix C: Documentation Examples 15
Validation Exercise (site/program specific) See Educator

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e4
PURPOSE
The purpose of this package is to provide the nurse working in cardiac monitored areas education to care
for patients requiring ST-segment monitoring.
OBJECTIVES
After completing this package, the learner will be able to:
1. Explain the importance of ST-segment monitoring for different patient populations. 2. Identify appropriate ECG lead placement based on patient population. 3. Identify the appropriate assessment, interpretation, treatment, and documentation for ST-segment
monitoring.
INSTRUCTIONS
This package is designed to be a supplementary review to any previously acquired knowledge and experience regarding ST-segment monitoring. Prior to reading this package, review the Critical Care Clinical Practice Guideline , Cardiac Monitoring (Adults): Setup, Lead Placement, and ST-Segment Monitoring. To successfully complete this review, some sites and programs in the WRHA may require the learner to submit a completed validation exercise and display an understanding of the correct answers in discussion with the educator.

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e5
NORMAL CARDIAC CYCLE REVIEW
Review of the components of the cardiac cycle:
P wave: first wave in the cardiac cycle that represents atrial depolarization.
P-R Interval (PRI): includes P wave and PR segment, measured from the beginning of the P wave to the beginning of the QRS.
QRS: series of deflections (Q, R, S) that normally follow a P wave and represents ventricular depolarization.
ST-segment: From the end of the QRS complex to the beginning of the T wave. Represents early ventricular repolarization and is normally isoelectric.
J point: point where the QRS complex and ST-segment meet.
T wave: waveform following the QRS complex that represents ventricular repolarization.
Q-T Interval (QT): onset of QRS complex to end of the T wave that represents both ventricular depolarization and repolarization.
J point

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e6
CLINICAL CONDITIONS FOR ST-SEGMENT MONITORING
ST-segment monitoring is a recommended standard of care for patients whose clinical condition warrants ischemia monitoring (e.g. Acute Coronary Syndrome (ACS), Myocardial Infarction (MI), cardiac surgery, signs and symptoms of angina). It is reasonable to initiate ST-segment monitoring for >24-48 hours or until MI is ruled out. Myocardial ischemia causes the cells of the myocardium to become either more or less excitable. This change is most apparent in the ST-segment of the ECG. ST-segment depression or elevation reflects ischemia or injury to myocardial tissue.
Ischemia detection via ST-segment monitoring has always been an important component in managing cardiac patients. ST-segment monitoring enables the detection and documentation of potential episodes of ischemia as reflected by ST-segment changes. However, ST-segment monitoring is equally important to detect “silent ischemia” which occurs in absence of other classic symptoms for high risk patients or in patient populations unable to communicate signs and symptoms of ischemia (e.g. sedated or mechanically ventilated patients).
LEAD PLACEMENT
Lead placement will be dependent on patient population and reason for monitoring, patient specific clinical presentation or as per program/unit specific guidelines.
Recommended monitoring leads are:
1. Dysrhythmias: Leads II (supraventricular arrhythmias) & V1 (wide complex arrhythmias)
2. ST-segment fingerprint: Lead selection based on the coronary artery or surface known or
suspected to be affected by the ischemic process (identified via invasive angiography or 12 Lead
ECG).
3. ACS Leads: III & V3
4. Demand Ischemia (non-cardiac populations): V5

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e7
ENSURING ST-SEGMENT ACCURACY
Ensure lead placement is accurate according to the Cardiac Monitoring (Adults): Setup, Lead Placement, and ST-Segment Monitoring. For example, when monitoring V1, the V lead must be placed at the 4th intercostal space, right sternal border.
Optimize signal quality by ensuring electrodes are changed as per manufacturer’s recommendation and as need (PRN) with the skin prepped appropriately. If the patient is actively mobile consider taping with waterproof tape to keep in place.
Depending on the cardiac monitor software capabilities, you may need to ensure the J Point is correctly established on admission. Review with unit Clinical Educator (see Appendix A).
CONSIDERATIONS WITH ST-SEGMENT MONITORING
At times, ST-segment changes may not be representative of ischemia. Numerous conditions may mimic ischemia or make ST-segment monitoring unreliable, including the following:
Artifact
Body position changes
Arrhythmias such as atrial fibrillation/flutter (due to an irregular isoelectric line)
Continuous ventricular pacing
Left bundle branch block
Tachycardia
Drug effects (such as digitalis and diuretics)
Electrolyte imbalances (such as calcium and potassium)
Conduction disturbances (including LBBB and WPW syndrome)
Hypothermia
Left ventricular hypertrophy
Endocarditis
Pericarditis
Old infarcts

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e8
WHAT TO DO IF ST-SEGMENT CHANGES ARE NOTED
If ST-segment changes are noted, consider and assess the following:
Assess the patient:
o Perform vital signs
o Auscultate the heart and lungs
o Are they symptomatic?
o Are they moving/could this be artifact?
o Is there a change of more than 1 or 2 mm that lasts more than one minute from previous
value?
o Is the J point correctly identified (depending on the cardiac monitor software capabilities)?
o Are the electrodes intact and placed appropriately?
o Could this be expected resolution from a recent cardiac event? (e.g. STEMI)
Based on the above information, if you are concerned that this is a significant change:
Inform the MD
Call for a 12-lead ECG
Obtain bloodwork (as ordered)
WHAT TO DOCUMENT AND WHERE
Print a rhythm strip. Mount and analyze the rhythm strip on the ECG monitoring record sheet. Ensure
documentation of which lead is being monitored.
Document the ST-segment on admission and PRN. If continuous monitoring is required as per clinical
condition or per unit/program protocols or guidelines, document q4h and PRN.
Document vital signs and assessment data using unit a specific flowsheet or nursing documentation tools.
See Appendix C for unit specific examples.

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e9
IN SUMMARY
Establishing a patient specific ST-segment level, rather than an isoelectric ST-segment level, is important because the patient’s baseline ST-segment level is rarely isoelectric.
Set cardiac monitor alarms to detect changes in ST-segment elevation or depression greater than 2mm.
ST-segment elevation or depression of 1 to 2 mm that lasts for at greater than one minute can be clinically significant and warrants further patient assessment.
Supine is the optimal patient position to establish baseline ST-segments.
Key point to remember, it is about monitoring trends.
REFERENCES:
American Association of Critical Care Nurses Practice Alert: Dysrhythmia Monitoring in Adults (2016).
Retrieved from: https://www.aacn.org/clinical-resources/practice-alerts#page/1 Doi
http://dx.doi.org/10.4037/ccn2016767
American Association of Critical Care Nurses Practice Alert: Ensuring Accurate ST-segment Monitoring
(2016). Retrieved from: https://www.aacn.org/clinical-resources/practice-alerts#page/1 Doi:
http://dx.doi.org/10.4037/ccn2016935
American Association of Critical Care Nurses Practice Alert: Alarm Management (2016). Retrieved from:
https://www.aacn.org/clinical-resources/practice-alerts#page/1
Covidien (2008). Product information: Electrode selection and wear time. Point-Claire: Author.
Elsevier Mosby nursing Skills Online Resource. Cardiac monitor setup and lead placement. Retrieved from:
http://lms.elsevierperformancemanager.com/ContentArea/NursingSkills/GetNursingSkillsDetails?
skillid=CC_054&skillkeyid=66&searchTerm=cardiac%20monitor&searchContext=nursingskills
Elsevier Mosby nursing Skills Online Resource. Continuous ST-segment monitoring. Retrieved from:
http://lms.elsevierperformancemanager.com/ContentArea/NursingSkills/GetNursingSkillsDetails?
skillid=CC_056&skillkeyid=68&searchTerm=ST%20monitoring&searchContext=nursingskills

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e10
Harris. P. R. E. (2016). The normal electrocardiogram: Resting 12 lead and electrocardiogram monitoring in
the hospital. Critical Care Nursing Clinics of North America, 28(2016), 281-296. Retrieved from:
http://dx.doi.org/10.1016/j.cnc.2016.04.002
Huff, J. (2017). ECG Workout: Exercises in arrhythmia interpretation (7th ed.). Philadelphia: Wolters Kluwer.
Jevon, P. & Ewens, B. & Pooni, J. S. (2013). Monitoring cardiovascular function1: ECG monitoring.
Monitoring the Critically Ill Patient, 91-114. Wiley-Blackwell. Retrieved from:
http://onlinelibrary.wiley.com/book/10.1002/9781118702932. Doi: 10.1002/9781118702932
Lough, M. E. & Thompson, C. (2014), In Urden, L.D., Stacy, K. M., & Lough, M. E. (Eds.). Critical care
nursing: Diagnosis and Management (7th ed.), 237-337. St. Louis: Mosby.
McKinley, M. G. (2011). Electrocardiographic leads and cardiac monitoring. In Weigland, D. L. (Ed.), AACN
Procedure Manual for Critical Care, 490-500. Philadephia: Elsevier Saunders.
Philips (2006). ST-segment Monitoring. Retrieved from: http://www.mc.vanderbilt.edu/documents/
7north/files/STSegmentMonitoring%204522%20962%2020161.pdf
Philips (2007). Intellivue patient monitor manual: Patient monitoring. Germany: Philips.
Sandau, K. E., Funk, M., Auergach, A., Barsness, G. W., Blum, K., Cvach, M., … Wang, P. J. (2017). Update
to practice standards for electrocardiographic monitoring in hospital settings: A scientific
statement from the American heart association. Circulation 136(19), e273-e344.
https://doi:10.1161/CIR.0000000000000527.
Zegre-Hemsey, J. K., & Garvey, J. L., & Carey, M. G. (2016). Cardiac Monitoring in the Emergency
Department. Critical Care Nursing Clinics of North America, 28(2016), 331-345. Retrieved from:
http://dx.doi.org/10.1016/j.cnc.2016.04.009

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e11
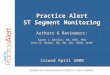
A: Lead B: ISO Point
C: Incorrect J Point D: Incorrect ST Point
Initial / Default Setup
A
B
C
D
APPENDIX A: PHILIPS MONITOR SETUP
When: Upon new patient admission, after they have been on the monitor for about one minute to
establish a baseline (e.g.: when adjusting monitor alarm limits for the first time).
1. Touch any ECG rhythm.
2. Touch “Adjust ST Points”.
3. Touch anywhere on the pop-up screen to
change the displayed Lead. Select the QRS
complex with the most distinguishable
change from QRS complex to T wave.
Use the < and > arrows to move the “ISO
Point” cursor to the ISO electric line. This is
best found - with the least amount of
artifact - between the P wave & the QRS
complex.
4. Touch “Select Point”.
5. Use the < and > arrows to move the
“J Point” cursor to the position where the
QRS complex becomes the T wave (see
Point E on the next page).
6. Touch “Apply Changes”.
2. 3.

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e12
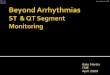
7. Note that the “ST Point” is 60 milliseconds after
the J Point. This is where ST elevation or
ST depression is measured (Point F).
8. “X” out of the pop up window.
9. Document the ST numeric for the two
appropriate leads for the patient.
Correct Setup
E: Corrected J Point F: Corrected ST Point
E
F

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e13
APPENDIX B: SPACELABS MONITOR SETUP
1. Select the ECG Menu in the main screen
2. Select Alarm Limits, then ST Alarms.
3. Monitor default alarms detect changes in ST-segment elevation or depression greater than 2mm. Select Multi ST=2.00 to adjust ST alarm limits for mulitple leads if needed. Select ST Leads to include or exclude in ST Lead alarms.

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e14
4. Monitor displays ST-segment values in the main screen.

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e15
APPENDIX C: DOCUMENTATION EXAMPLES
ICU Vital Signs Flowsheet:
1.2/0.5 0.8/.16

This self-learning package is intended to be supplementary information and is not intended to replace
Policy and Procedures, Guidelines and/or critical thinking.
Pag
e16
EPR CAAF: For the GE telemetry monitors: Click on the patient’s telemetry box then click on patient data. Click on the numeric trends option. ST-segment measurements will be displayed by time column. ST-segment measurements: I: 0mm III: +1.2mm aVR: 0mm V3: +1mm II: +1.2mm aVL: +1.2mm aVF: 0mm