Embed Size (px)
Citation preview
1
Sports Injuries Unique to the Pediatric Population
Scott Escher MD
Gundersen Health System
Disclosures
� None
� I do have a dog
� Been married for 27 years

2
Objectives
� Review the growth plate and overuse injuries that can occur to them.
� Review growth plate fractures
� Review osteochondritis dissecans
Anatomy- Terms often used interchangeably
� Epiphysis- End of a long bone, secondary center of ossification
� Physis- Epiphyseal growth plate
� Apophysis- aka traction epiphysis
� Metaphysis- Flared area of long between physis and diaphysis
� Diaphysis- Cancellous bone in middle of long bone

3
Growth Plate Injuries
� Overuse injuries occur at the weakest part of the musculotendinous junction, the physis.
� Hypertrophic zone is weakest area of physis.
Growth Plate Injuries
� Repetitive trauma weakens the physis and subsequent trauma may fracture the involved physis.
� Physis can be weaker than ligaments and muscle-tendon junctions.
� Problems often occur during growth spurt.� Pain often ceases when growth ceases.� Anatomic variants may predispose to overuse
injuries

4
Fractures in Children, Rockwood et al 1991
Secondary Ossification Centers
Tibial Apophysitis (Osgood-Schlatters Disease)
� Presentation– Pain with activity
over the tibial tuberosity in males ages 10-15 and females ages 8-13.
– Increased size and pain with palpation of the tibial tuberosity.
– Bilateral 25-50%

5
Tibial Apophysitis (Osgood-Schlatters Disease)
� Treatment– Must differentiate from tibial tubercle
avulsion.– Quadriceps/ hamstring stretching.– Activity limited by symptoms. Padding may
help.– After maturation, separate bony ossicle may
be removed if chronically painful.
Tibial Apophysitis (Osgood-Schlatters Disease)
� Avulsion– Acute- etiology
usually resisted knee extension
– Immediate pain and swelling
– Nondisplaced-Extension cast ~4 weeks (controversial)
– Displaced- ORIF

6
Distal Patellar Apophysitis (Sinding-Larsen-Johansson
Syndrome)� Apophysitis of the
distal pole of the patella.
� Treat similar to tibial apophysitis
� X-ray Osgood-Schlatters and SLJ
Multipartite Patella
� 0.2-6% of population
� Male predominance 9:1
� Etiology not clear– Poor blood flow to superolateral patella
– Traction from vastus lateralis
– Old trauma
– Separate ossification center- can begin to ossify as early as 2 yo. Usually ossifies at 5-6

7
Bilateral Bipartite Patella
Same Knees 3 years later

8
Multipartite Patella- Treatment� If traumatic may be fracture
� If traumatic, usually treat with brief immobilization for 3-4 weeks
� If overuse can try relative rest for 3-4 weeks and if not successful, immobilization
� Some may need surgical excision
from DeLee J, Drez D (Ed). Pediatric and Adolescent Sports Medicine.
Philadelphia.Saunders, 1994
Medial Epicondylar Traction Apophysitis (Little Leaguer's
Elbow)� Presentation
– Ages 9-12– Pitchers lose control– Medial epicondylar pain and swelling– Medial elbow pain with valgus stress or
resisted wrist flexion or pronation– Limited elbow extension– Most common cause is pitching while
fatigued

9
Medial Epicondylar Apophysitis
� Radiographic findings– Medial epicondylar
enlargement, cortical thickening, fragmentation, or separation.
– May see osteochondritis of capitellum
– May need comparison x-rays
Medial Epicondylar Apophysitis

10
Medial Epicondylar Apophysitis
� Treatment– 2 to 3 weeks of rest and ROM with gradual
return to throwing at about 6 weeks.– ROM/Strengthening of flexor/pronator
group– ORIF if displaced
Pitching
� Survey conducted by Joe Chandler MD (2000) of 101 Atlanta Braves pitchers
� Average age started– Fastball 10 years– Curveball 14– Change-Up 17– Slider 18
� Average age would allow son to start– Change-Up 12– Curveball 15– Slider 17

11
Calcaneal Apophysitis (Sever's Disease)
� Present with pain at the insertion of the achilles tendon or calcaneus and limp.
� Ages 7-12� High association with foot and ankle
abnormalities including varus deformities of the foot and ankle and tight heel cords.
� Pain with medial/ lateral compression of calcaneus
Calcaneal Apophysitis
� X-ray shows dense calcaneal apophysis.
� Treat conservatively with relative rest, stretching, heel cups/lifts, and correction of biomechanical abnormalities.

12
Traction Apophysitis about the Pelvis
� Can occur at the ASIS (sartorius), AIIS (rectus femoris), iliac crest (gluteus medius and abdominals anteriorly and the gluteus maximus and latissimus posteriorly), greater trochanter (gluteus medius and minimus), lesser trochanter (iliopsoas), or the ischial tuberosity (hamstring).
Traction Apophysitis about the Pelvis
� Pain with resisted motion and palpation
� X-ray may show widening of the apophysis or an avulsion fracture
� Look for leg length inequality

13
Iliac Crest Apophysitis
Traction Apophysitis about the Pelvis
� Treatment– Relative rest 2-4 weeks– Range of Motion– Full activity usually in 4-6 weeks

14
Traction Apophysitis about the Pelvis
� Treatment- Avulsion Injuries– Usually treated
conservatively (Snyder Sling) Rest-O-Flex
– Full activity in 3-4 months
– Some advocate ORIF
Traction Apophysitis about the Pelvis
� Rest-O-Flex brace– Make sure brace
does not rub on injured area

15
Iliac Crest Avulsion
Iliac Crest Avulsion

16
ASIS Avulsion
ASIS Avulsion 6 weeks later

17
AIIS Avulsion
AIIS Avulsion

18
Ischial Tuberosity Avulsion
Proximal Humeral Apophysitis (Little Leaguer's Shoulder)
� Overuse injury of the proximal humeral physis
� Pain at deltoid insertion with throwing
� X-ray: widened humeral physis- get comparison views
� Complete throwing cessation for 6 weeks

19
Little Leaguers Shoulder-comparison views
Little Leaguers Shoulder-comparison views 6 weeks later

20
Proximal Humeral Physis
Proximal Humeral Physis normal variant

21
Slipped Capital Femoral Epiphysis
� Epidemiology– 0.7-3.4/100,000– Male > Female– 11-15 years old– 10-20 (41)% bilateral
� Etiology unclear- genetic, hormonal (thyroid), mechanical
� Presentation– Hip (groin) pain– Pain may refer to knee– Decreased internal rotation
Slipped Capital Femoral Epiphysis
� Bilateral AP pelvis and frog lateral will show slip
� Treatment is surgical

22
Slipped Capital Femoral Epiphysis
Slipped Capital Femoral Epiphysis

23
Slipped Capital Femoral Epiphysis
Slipped Capital Femoral Epiphysis- Treatment
24
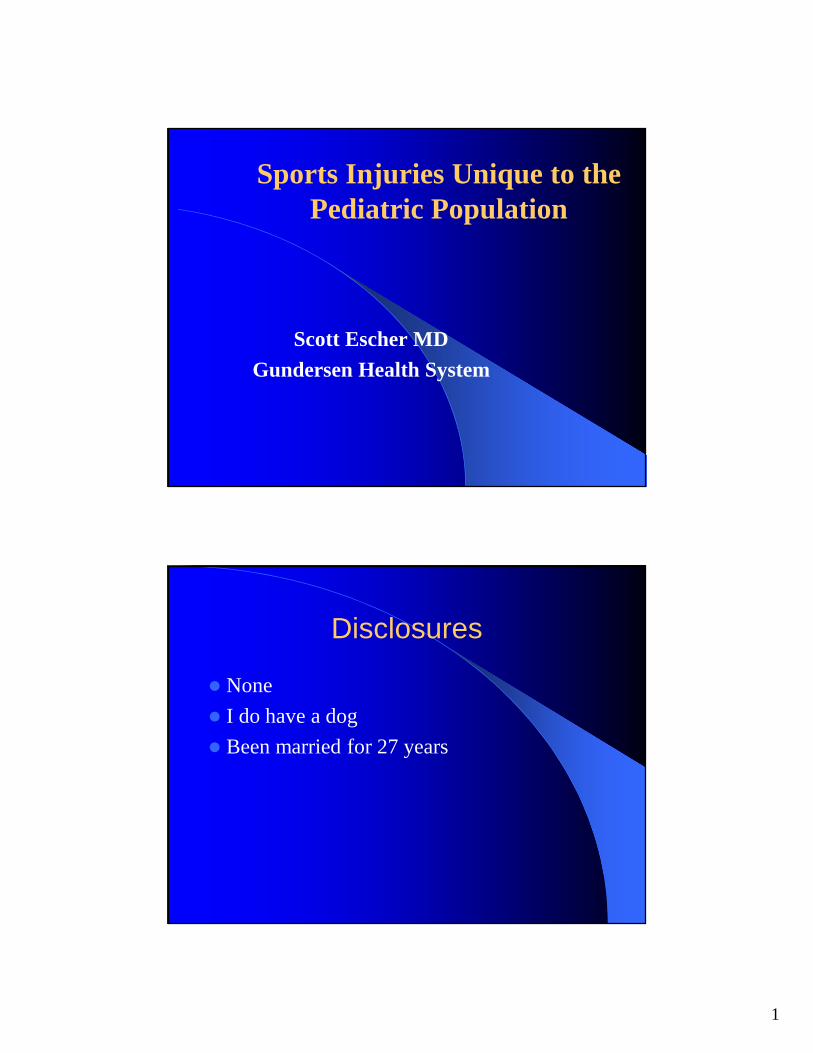
Fifth metatarsal (Iselin's disease), accessory navicular
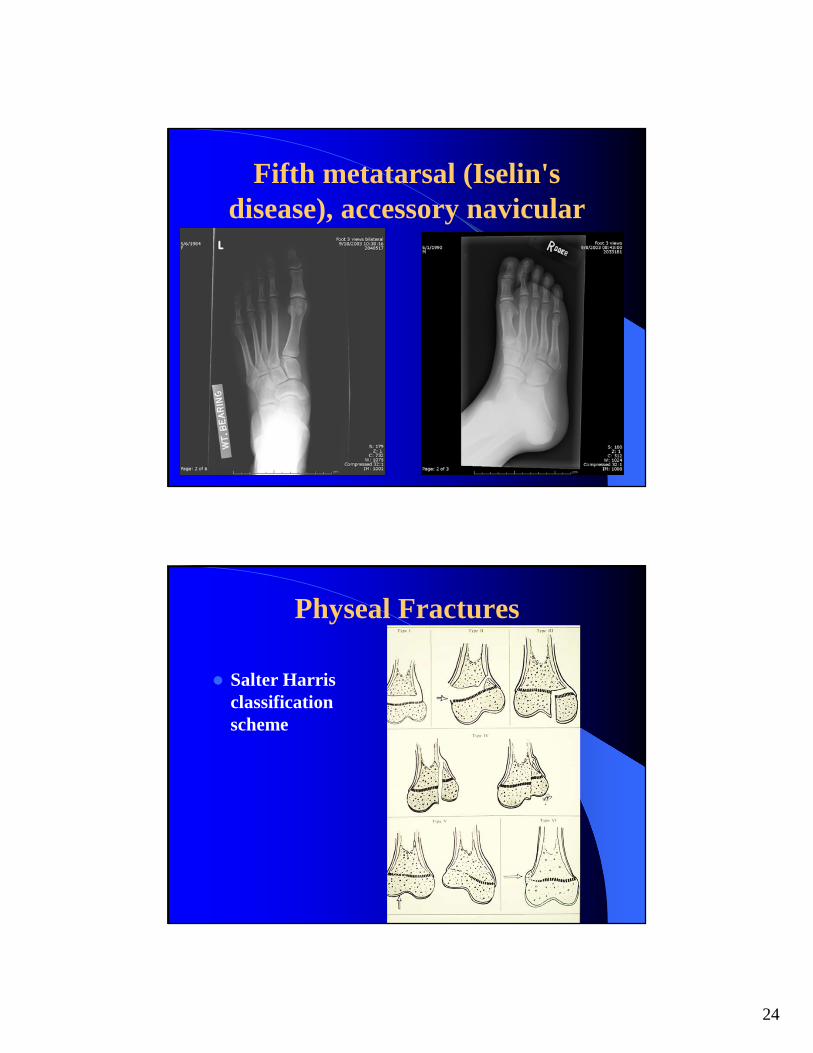
Physeal Fractures
� Salter Harris classification scheme

25
Physeal Fractures
� Salter 1 Fracture– I f physis locally tender, treat as fracture
even with normal x-ray- most common is distal fibula and distal radius
� Salter III-V– Can affect epiphyseal blood supply
Salter 1 Distal Radius

26
Salter 1 Distal Radius 4 weeks later
Salter 1 Proximal Phalanx

27
Salter 1 Distal Fibula
Salter 1 Proximal Humerus

28
Greenstick (Torus) Fracture
Osteochondritis Dissecans
� Avascular segment of subchondral bone causing involution of bone and collapse overlying articular cartilage– Articular surface may remain completely
attached (stable), partially attached or become loose (unstable)
– Patients with OCD with closed physis (adult OCD) usually have poorer results than those with open physis (juvenile OCD).

29
Osteochondritis Dissecans
� Most common area is knee; also elbow and ankle– 80% on lateral aspect of medial femoral condyle– Prevalence- 30-60/100,000– Juvenile form usually presents in teens– Bilateral in 20-40%– M:F-3:1
� Etiology multifactorial- trauma, avascular necrosis, endocrine, familial
Osteochondritis Dissecans
� Presentation– Poorly localized, aching knee pain with activity ±
swelling– May progress to mechanical symptoms– PE
� Full ROM
� Effusion
� Wilson test- Seated position- pain during active knee extension with the tibia internally rotated. Should have no pain with active extension with tibia externally rotated

30
Osteochondritis Dissecans
� X-ray– Tunnel view usually
best at visualizing OCD fragment
– Radiolucent semicircle around fragment of bone
– May show healing after 3-6 months of treatment
Osteochondritis Dissecans-X-ray
11 months later

31
Osteochondritis Dissecans
� MRI– Images articular
surface– Can give information
on stability of fragment and healing
– Bone scan activity shows ability to heal
Osteochondritis Dissecans MRI

32
Osteochondritis Dissecans
Osteochondritis Dissecans

33
Elbow OCD
Osteochondritis Dissecans-Treatment
� Conservative Treatment in juvenile OCD– Use in patient with physis with no mechanical
symptoms (stable)– Activity modification for 6-12 weeks
� Limited immobilization and minimal weight bearing for 1-2 weeks
� Limit rapid, strenuous activities e.g.. running
– Full activity when:� No complaints� Normal exam� Radiographic evidence of healing
– I f no improvement after ~6 weeks- MRI or bone scan

34
Osteochondritis Dissecans-Treatment
� Patients with open physes have better chance of healing
� OCD of lateral femoral condyle usually do poorer than medial condyle.
Osteochondritis Dissecans-Treatment
� Surgery after failed conservative management or patients with unstable fragment– Need to have smooth articular surface and
promote vascular ingrowth– Procedures include transarticular drilling,
fragment fixation, and bone grafting– Loose body removal

35
Discoid meniscus
� Enlarged meniscus covering tibial condyle� Congenital -v- Acquired� Usually lateral� See snapping in knee and tears� Intermittent effusion� May lack full extension even between episodes� Treatment of symptomatic discoid meniscus is
surgical
Discoid Meniscus

36
Avascular Necrosis
� Tarsal Navicular (Koehler's Disease)– Epidemiology
� Ages 3-8
� Male/Female- 6/1
� 30% bilateral
– Presentation� Antalgic gait
� Pain along longitudinal arch and over navicular
AVN Tarsal Navicular
� X-ray– Avascular necrosis of navicular– Will usually have normal navicular after
several months

37
AVN Tarsal Navicular-comparison x-ray
AVN Tarsal Navicular-comparison x-ray

38
AVN Tarsal Navicular
� Treatment– Aim is to maintain bony contour
– Well molded cast for 4-6 weeks
– Medial arch supports
– Activity modification
– Treatment failure sometime leads to surgery
AVN 2nd or 3rd metatarsal (Freiberg's Infarction)
� Epidemiology– Female > Male– Teens– Morton’s toe more common– Etiology unclear

39
AVN 2nd or 3rd metatarsal (Freiberg's Infarction)
� X-ray– AVN with flattening of metatarsal head
� Treatment– May cast initially– Metatarsal pads/ low heels– Surgery for refractory cases