Embed Size (px)
Citation preview

J. clin. Path., 1975, 28, 937-943
Spontaneous infarction of the breastJ. J. LUCEY
From the Department of Histopathology, St. Bartholomew's Hospital, London
SYNOPSIS Five cases of infarction of physiological hyperplastic breast tissue associated withpregnancy or lactation are reported. These presented clinically as lumps in the breast, two of whichwere painful. Similar cases in the literature are briefly reviewed. The demonstration of an underlyinglobular pattern in the present cases and the distribution of the infarcts support the view that the so-
called 'adenoma' of pregnancy or lactation is a myth. Organizing vascular thrombi, previouslyunrecorded in this context, were seen in three of the five cases, and it is postulated that these lesionsare the primary cause of the infarction rather than relative vascular insufficiency, as proposed byprevious authors.
Spontaneous infarction of physiologically hyper-plastic breast tissue associated with pregnancy orlactation is a recognized but rare clinical entity.Only 13 cases are recoided in the American andBritish literature (table) (Hasson and Pope, 1961;
Received for publication 9 June 1975.
Wilkinson and Green, 1964; Pambakian and Tighe,1971; Rickert and Rajan, 1974). Vascular lesionswere not demonstrated in these cases and so thepathogenesis of the infarction remains speculative.In this report, the clinical and pathological featuresof five cases are described, and evidence on theunderlying mechanism of the infarction is presented.
Author Case Race Age Breast No of Size Pain Status at DurationLumps (cm) Operation (weeks)
Hasson and Pope(1961) 1 N 33 Right 1 3-5 No 17 d pp 7
2 C 23 Right 1 3-0 No 7 d pp 43 C 26 Right 1 1-0 No 3 wk pp 2
Wilkinson andGreen (1964) 1' N 21 - 1 2-0 - 26 wk pp 40
21 LA 18 Left 3 55 - 2 wk pp 52Right 1 1-5 -
51 N 26 - 1 7-0 - 5 wk pp 861 N 21 - 1 40 - 1-2 wk -
pregnant71 N 20 - 1 2-0 - 6 wk pp 40101 N 20 - 1 3 5 - 6 wk pp 264 C 24 - 1 40 - 8 d pp 6
Pambakian andTighe (1971) 3 N 27 Left 2 5S0 each Tender I wk pp I
Rickert and 1 N 19 Left 2 2-0 No 8 wk pp 26Rajan (1974) 1-5 No
21 N 17 Right 2 1-0 No 8 wk pp 121-0 No
Present series 1 C 23 Right 1 2-0 Tender 4 wk pp 22 C 21 Left 1 2-5 No 3 wk pp 19
Right Many 0 5 each No 3 wk pp 113 N 18 Right 1 2-0 No 26 wk pp 344 N 26 Left 1 2-0 Tender 36 wk 3
pregnant5 N 28 Right 1 0-5 No 26 wk pp 32
Table Summary ofcasesN = Negro; C = Caucasian; LA = Latin American'Reported as an adenoma
937
copyright. on July 1, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.28.12.937 on 1 Decem
ber 1975. Dow
nloaded from

938
Case Reports
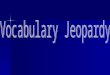
CASE IEleven days after the normal delivery of her secondchild a 23-year-old woman, gravida 2 para 2, com-plained of a tender lump in the right breast. She wasnot breast feeding and breast binders were used tosuppress lactation. There was no history of traumaor previous breast disease. Her first pregnancy threeyears previously had been normal, and shortlyafterwards she was given oral contraceptives,Minovular for four months and Gynovular for afurther six months. The mass was situated in theupper and outer quadrant of the breast, and avariety of clinical opinions were expressed regardingits nature, but infarction was not considered. Thelump was excised four weeks after delivery and herpostoperative progress was uneventful.The excised breast tissue (St B H SH 1478/74)
contained a well-circumscribed area measuring 2-0cm in diameter with a uniform grey-yellow cut sur-face. Microscopically this was an area of coagulativenecrosis of hyperplastic breast lobules (fig 1). In thenecrosis the original reticulin architecture of lobulesand acini was preserved (fig 2). The margin of thenecrotic area was formed by a narrow rim of viablebreast tissue associated with areas of haemorrhageand a moderate inflammatory cellular infiltiationcomprising lymphocytes, plasma cells, and many
J. J. Lucey
eosinophils. Many haemosiderin-laden macrophageswere also seen at the edge of the infarct. At leastthree smaller but similar discrete areas of necrosiswere observed in adjacent mammary lobules. Theresidual breast tissue was normal, exhibiting variablesecretory activity. In the interlobular collagenoustissue adjoining the infarcts, some medium-sizedarteries and 'eins showed cellular intimal fibrousthickening which partly occluded the lumen of thevessels (fig 3). Many other vessels in the same regionshowed no evidence of thrombo-occlusive or inflam-matory disease.
CASE 2A 21-year-old primigravida noticed a painless lumpin the left breast at 24 weeks' gestation. A similarlump appeared in the right breast at 32 weeks' ges-tation. There was no history of trauma or previousbreast disease. She was admitted to hospital at 25weeks' and 32 weeks' gestation with persistentvomiting which improved with bed rest. Four yearspreviously she had been treated with Duphaston forthree months and with Norlestrin for 18 months fordysmenorrhoea.On examination a solitary mass was palpable in
the left breast and at least two nodules in the rightbreast. The masses, thought to be multiple fibro-adenomata, were situated in the lower and innerquadrants. At term she was delivered of a normal
Fig 1 (Case 1)'" The sharply circum-
scribed border of theW~ ~ infarct may give an
initial impression ofadenoma(Haematoxylin and
L ~~~~ ~ eosin x 25).
copyright. on July 1, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.28.12.937 on 1 Decem
ber 1975. Dow
nloaded from

Spontaneous infarction of the breast
Fig 2 (Case>..^^ 1) Several
t-^> hyperplasticlobules comn-
>a.j posed ofclosely packedacini (Gordonand Sweet'sreticulin x150).
Fig 3 (Case]1)Partial luminalobliteration of twomedium-sized arter-iesby intimal fibroustissue (Weigert 'selastic v'an Gieson x215).
939
copyright. on July 1, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.28.12.937 on 1 Decem
ber 1975. Dow
nloaded from

J. J. Lucey
female infant which was not breast fed, lactationbeing suppressed with breast binders. Three weeksafter delivery the masses were excised.The mass from the left breast (St B H SH 2157/74)
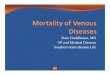
contained a central well-circumscribed soft areameasuring 2 5 cm in diameter. Pale grey and reddish-brown areas were mixed with smaller yellow areas onthe cut surface (fig 4). The tissue from the right breastmeasured 6 0 x 4 0 x 3 0 cm and contained severalgrey-white nodules which, on slicing, revealed cen-tral yellow areas, each approximately 0 5 cm indiameter.
Microscopic examination of the left breast massrevealed an almost confluent area of coagulativenecrosis of hyperplastic breast lobules. Despite theextensive necrosis the original reticulin architectureof the lobules and acini was retained. An incompleterim of viable breast acini and granulation tissueformed the margin of the infarct associated withmany haemosiderin-laden macrophages, lymphocy-tes, and plasma cells. Broad trabeculae of densefibrous tissje containing a sparse mononuclear infil-tration and areas of finely granular calcificationextended into the necrotic area from the marginalzone. Several nearby hyperplastic mammaiy lobulesshowed similar areas of coagulative necrosis whichfrequently involved only part of a lobule. The resid-ual breast lobules were normal, exhibiting variablesecretory activity. Several small veins and a fewarteries in the interlobular collagenous tissue adja-cent to the infarcts contained eccentric areas ofintimal fibrosis which partly occluded the lumen.Definite organizing venous thrombi were seen in onearea (fig 5). Many other vessels showed no evidenceof thrombo-occlusive or inflammatory disease.The right breast mass was composed of hyper-
plastic lobules, several of which showed partial
infarction (fig 6). Many foamy macrophages wereseen in the infarcted areas, and there was a slightlymphocytic infiltiation in the residual lobules. Afew small veins in the interlobular collagenous tis-sue showed cellular fibrous thickening of the intimawhich partly occluded the lumen. Several other ves-sels appeared normal.
CASE 3At 32 weeks' gestation of an otherwise normalpregnancy an 1 8-year-old negro primigravidanoticed a painless lump in the right breast. Therewas no history of trauma, oral contraceptives orprevious breast disease. On examination the mass,thought to be a fibroadenoma, was situated in theouter and lower quadrant. At term the delivery wasnormal and the infant was breast fed. The mass wasexcised six months later and postoperative progresswas uneventful.The excised breast tissue (St B H SH 2312/74)
contained a sharply circumscribed nodule 2 0 cm indiameter with grey and yellow areas on the cut sur-face. Microscopically, as in the two preceding cases,there was extensive necrosis of hyperplastic breastlobules with ghost-like acini clearly seen in a reticulinpreparation. The necrotic area was demarcated fromthe surrounding breast tissue by an irregular zone ofdense collagenous tissue containing occasional ducts.Some ducts nearest the necrosis showed squamousmetaplasia, and an incomplete layer of squamousepithelium lined a cleft-like space between thenecrotic area and the zone of collagenous tissue. Theboundary zone also contained many haemosiderin-laden macrophages, lymphocytes, and plasma cells.The surrounding breast tissue exhibited advancedpost-lactational involution. The lumina of a fewveins in the interlobular collagenous tissue near the
Fig 4 (Case 2) Cut surface of the well-circumscribed infarct from the left breast(x 2).
940
copyright. on July 1, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.28.12.937 on 1 Decem
ber 1975. Dow
nloaded from

Spontaneous infarction of the breast
Fig 5 (Case 2) Organizing thrombus partly occludingthe lumen of the vein (H and E x 175).
infarct were partly obliterated by cellular fibrousthickening of the intima. Several other vessels werenormal.
CASE 4* At 33 weeks' gestation of an otherwise normal preg-
nancy a 26-year-old negro primigravida complainedof a tender lump in the left breast. There was nohistory of trauma or previous breast disease. As shehad been a known case of homozygous sickle celldisease for 18 years, the recurrent pain in the muscles,bones, and abdomen, of which she had previouslycomplained, were attributed to episodes of infarc-tion, and the spleen which had been removed whenshe was 10 years old contained several infarcts. Onexamination the mass was situated in the upper andinner quadrant and an infaret was suspected. In viewof the underlying blood disorder, a lower segmentCaesarian section was performed at 36 weeks' gesta-tion and a healthy female infant was delivered. Thebreast mass was also excised and postoperativerecovery was satisfactory.The excised breast tissue (St B H SH 2450/60)
contained a sharply circumscribed area 2-0 cm indiameter with a yellow cut surface. Microscopicallyextensive necrosis of the lobules, sparing only anirregular rim of hyperplastic breast tissue with its
Fig 6 (Case 2)Partial infarction of
'7e;v+fi-;-%>>^;- -4A hyperplastic breastlobules (H and E x
, ~Ift 37).
941
1.
,v. t ;,I ..
.*., VI--w" f .-"
1,
:, .1t.II'r 4.
t
copyright. on July 1, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.28.12.937 on 1 Decem
ber 1975. Dow
nloaded from

942
infiltrate of lymphocytes, plasma cells, and haemo-siderin-laden macrophages, was as described in thepreceding cases. In addition, the ducts at the edge ofthe necrotic area showed patches of squamousmetaplasia. The surrounding breast lobules werenormal, exhibiting variable secretory activity. Thevessels in the interlobular collagenous tissue werenormal.
CASE 5At 34 weeks' gestation of an otherwise normal fifthpregnancy, a 28-year-old negro, gravida 5 para 2, 3abortions, noticed a painless lump in the right bieast.There was no history of trauma or previous breastdisease. On examination the mass, thought to be afibroadenoma, was situated in the upper and outerquadrant. At term she was delivered of a healthymale infant which was breast fed. The mass wasexcised six months after delivery.The excised breast tissue (St B H SH 3401/69)
measured 40 x 2 5 x 2 0 cm and contained aperipherally situated, stippled yellow area, 0 5 cm indiameter. Microscopically this area was composedof dense collagenous tissue in which several smallducts were embedded but the outline of the hyper-plastic mammary lobules was still discernible. A nar-row rim of viable breast tissue including manyhaemosiderin-laden macrophages and lymphocytesformed the boundary zone. The adjacent breast tis-sue showed advanced post-lactational involution.The vessels in the intei lobular collagenous tissuewere normal.
Discussion
Spontaneous infarction of physiologically hyper-plastic breast tissue associated with pregnancy andlactation is rare. However, it may be commoner thanis generally appreciated as three of the five cases inthe present series were detected in the surgicalmaterial received in one depaitment in a two-monthperiod. The true incidence is difficult to assess sincesome cases are reported under the title of adenomaassociated with pregnancy (Rickert and Rajan, 1974)or lactation adenoma (Wilkinson and Green, 1964).Study of the present cases leads one to believe thatthey are not true adenomata. The sharply circum-scribed infarcted masses composed of enlarged,closely packed acini give an initial impression of anadenoma when compared with the adjacent involut-ing breast tissue. However, on closer inspection,especially with the aid of reticulin preparations, theti ue hyperplastic nature of the infarcted breast tissueis reveaJed. Infarction has also been reported in fibro-adenomata of the breast (Wilkinson and Green,1964; Haagensen, 191; Pamb7akian and Tighe, 1971;
J. J. Luicey
Newman and Kahn, 1973; Majinudar and Rosales-Quintana, 1975) some of which were associatedwith pregnancy, but these neoplasms can readilybe distinguished from the hyperplastic lesionsmentioned above. The sporadic case ieports ofnecrosis of the breast from various causes, particu-larly oral anticoagulant drugs (Davis et al, 1972), andthe case of ischaemic fat necrosis in the mammaryregion (Robitaille et al, 1974) are irrelevant to thepresent study.
Infarction of physiologically hyperplastic breasttissue associated with pregnancy or lactation wasfirst reported by Hasson and Pope in 1961. Theydescribed three cases which presented clinically asbreast neoplasms. These were detected in the lastmonth of pregnancy in two cases and on the sixthpostpartum day in the third case. In 1964, Wilkinsonand Green described 10 cases of infarction of bieastlesions during pregnancy and lactation. Theyfelt thatthe background lesion was an adenoma of lactationin six cases (table) and a fibroadenoma in two. In theremaining two cases, the underlying lesion was intel-preted as lobular hyperplasia identical with thatdesciibed by Hasson and Pope. In one of thesepatients, the mass had been present for six weeks andwas removed on the eighth postpartum day. Theother case was unusual as the patient had juvenilehypertrophy of both breasts. Bilateral reductionmammaplasty was performed at 13 years and againat 15 years of age. The infarcts were found in breasttissue removed during the third mammaplasty atthree months' gestation when she was 16 years old.In view of the history of trauma, it is debatablewhether this case is comparable. In 1971, Pambakianand Tighe described three examples of mammaryinfarction. In two, the underlying lesion was interpre-ted as a fibroadenoma. The third patient noticed twomasses in the left breast on the first postpartum day.Microscopy of the resected masses revealed infarctedhyperplastic lactating breast tissue. Two cases oflocalized breast infarcts in pregnancy were recordedby Rickert and Rajan in 1974. Each patient had twonodules in the affected breast which were interpretedas adenomata. In case 4 of the present series, thepatient suffered from homozygous sickle cell disease,which may have been responsible for the infarction,but there was no clinical evidence of pre-existingdisease in the other four cases.The salient features of the reported cases, together
with those of the present series, are summarized inthe table. The infarcts usually appeared in the thirdtrimester of pregnancy or early in the puerperium.Clinically, they presented as palpable breast lumpswhich were sometimes painful. Transient tendernesswas noted by two patients in this study, and theabsence of pain may explain the long interval be-
copyright. on July 1, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.28.12.937 on 1 Decem
ber 1975. Dow
nloaded from

Spontaneotus infarction of the breast
tween the appearance and removal of the masses inthe other three. Multiple nodules are often present,but bilateral lesions, as seen in case 2, are rare. Asemphasized by previous writers, the importance ofthe lesions lies in their possible confusion with car-
cinoma, especially in rapid frozen sections. However,confusion is less likely if the possibility of infarctionis considered and the diagnosis of malignancy ismade only when viable tumour is identified.The pathogenesis of infarction has not been estab-
lished by previous authors. As vascular lesions were
not demonstrated, it was proposed that infarctionoccurred because of relative vascular insufficiencyresulting from increased metabolic demands of thebreast tissue imposed by pregnancy and lactation.However, in the collagenous tissue close to theinfarcts, obvious vascular lesions were detected inthree of the five cases of the present series. In cases
1, 2, and 3, several veins showed striking intimalfibrosis, and in cases 1 and 2 some medium-sizedarteries contained similar intimal thickening. Theseintimal thickenings were attributed to previous vas-cular thrombosis. This supposition was supportedby the finding of definite organizing venous thrombiin case 2 (fig 5). The presence of apparently normalvessels in the vicinity of those affected suggested thatthe thrombosis was primary rather than secondary tothe infarction. The most likely predisposing cause ispregnancy itself as there was no evidence of othervascular disease, and a history of trauma was notelicited. The role of the oral contraceptives in cases 1
and 2 remains speculative. It is proposed that theinfarction is due to ischaemia that resulted from the
thrombosis, rather than relative vascular insufficiencywhich was postulated by Hasson and Pope (1961)and later reiterated by others.
I wish to thank Dr. A. G. Stansfeld for helpfuladvice in the preparation of this paper and Mr. P.Crocker for the photomicrography. I am also grate-ful to surgical colleagues for access to the clinicalrecords of the patients under their care.
References
Davis, C. E., Jr., Wiley, W. B., and Faulconer, R. J. (1972).Necrosis of the female breast complicating oral anticoagu-lant treatment. Ann. Surg., 175, 647-656.
Haagensen, C. D. (Ed) (1971). Diseases of the Breast, 2nd ed.,pp. 212-226. Saunders, Philadelphia.
Hasson, J. and Pope, C. H. (1961). Mammary infarcts asso-ciated with pregnancy presenting as breast tumors. Surgery,49, 313-316.
Majinudar, B. and Rosales-Quintana, S. (1975). Infarction ofbreast fibroadenomas during pregnancy. J. Amer. med.Ass., 231, 963-964.
Newman, J. and Kahn, L. B. (1973). Infarction of fibro-adenoma of the breast. Brit. J. Surg., 60, 738-740.
Pambakian, H. and Tighe, J. R. (1971). Mammary infarction.Brit. J. Surg., 58, 601-602.
Rickert, R. R. and Rajan, S. (1974). Localised breastinfarcts associated with pregnancy. Arch. Path., 97, 159-161.
Robitaille, Y., Seemayer, T. A., Thelmo, W. L., and Cumber-lidge, M. C. (1974). Infarction of the mammary regionmimicking carcinoma of the breast. Cancer (Philad.), 33,1183-1189.
Wilkinson, L. and Green, W. O., Jr. (1964). Infarction ofbreast lesions during pregnancy and lactation. Cancer(Philad.), 17, 1567-1572.
943
copyright. on July 1, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.28.12.937 on 1 Decem
ber 1975. Dow
nloaded from


![Untitled-1 [assets-powerstores-com.s3.amazonaws.com]€¦ · 3m LITTMANN Master Classic Il Stethoscope Junior Adj Crutches Life Bedrest Back Support Reciprocal Folding Walker Life](https://img.pdfslide.us/doc/110x75/5f05b3ab7e708231d4144603/untitled-1-assets-powerstores-coms3-3m-littmann-master-classic-il-stethoscope.jpg)