Embed Size (px)
Citation preview

3'Med Genet 1991; 28: 51-53
Spondylocostal dysplasia and neural tube defects
George P Giacoia, Burhan Say
AbstractSpondylocostal dysplasia Uarcho-Levin syndrome)comprises multiple malformations of the vertebraeand ribs coupled with a characteristic clinicalpicture of short neck, scoliosis, short trunk, anddeformity of the rib cage. We describe a patientwith the syndrome who also had spina bifida anddiastematomyelia. We surmise that this associationis not coincidental. Additional evidence is neededto support the hypothesis that spondylocostaldysplasia and neural tube defects are aetiologicailyrelated.
Spondylocostal dysplasia is a congenital disorder withmultiple abnormalities of the vertebrae and thoracic
Department of Pediatrics, The University of OklahomaCollege of Medicine, 6161 South Yale, Tulsa, Oklahoma74136, USA.G P Giacoia, B SayCorrespondence to Professor Giacoia.
Received for publication 8 February 1990.Revised version accepted for publication 4 June 1990.
cage resulting in short trunked dwarfism. It has beenvariously reported as Jarcho-Levin syndrome,'hereditary multiple hemivertebrae', 'bizarre vertebralanomalies', 'costovertebral dysplasia', and Covesdemsyndrome when associated with mesomelic shorteningof the limbs. Despite the major vertebral segmentationdefects, including spina bifida occulta, spondylocostaldysplasia is considered unrelated to neural tubedefects.'The purpose of this paper is to present a case of
spondylocostal dysplasia associated with spina bifidaand diastematomyelia and to review the pertinentpublished reports.
Case reportThe proband, a male, was born to a 28 year oldwoman after a 38 week, uncomplicated pregnancy.Apgar scores were 4 and 7 at one and five minutes,respectively. Shortly after birth, the infant hadconsiderable respiratory difficulty requiring intubationin the delivery room and subsequently neonatalintensive care. The thorax was grossly deformed withshortening of the trunk and neck and a protuberantabdomen. The occipitofrontal head circumference
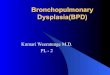
/~i7 a I .
Figure I Appearance at birthshowing diastematomyelia andopen sac ofmeningocele.
51
on Novem
ber 14, 2020 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.28.1.51 on 1 January 1991. D
ownloaded from

Giacoia, Say
was 36-2 cm (>90th centile). There was a triangularopening of the mouth with cleft palate and brevicollis.The spine was short and exhibited marked thoraco-lumbar lordosis and dextroconvex scoliosis. Spinabifida cystica was present in the thoracolumbar areaand diastematomyelia (diplomyelia) was noticed in thedefect (fig 1). There was an imperforate anus associatedwith a perineal fistula. The genitalia were normalexcept for undescended testes. His extremities werewell developed but showed paralysis of the legs. Theremainder of the physical examination was withinnormal limits. CT scan of the head showed moderatehydrocephalus owing to aqueductal stenosis. Anabdominal sonogram showed normal kidneys. X rayof the spine showed vertebral anomalies at all levels.Extensive and severe developmental anomalies of thevertebral bodies and widely open and spread neuralarches were most marked in the lower cervical spineand in the thoracolumbar area. Hemivertebrae andblock vertebrae were present, while other vertebralbodies were partially fused and irregularly deformed.The sacrum was least involved. The rib cage exhibitedbizarre features with ribs of different size, thickness,and orientation (fig 2). Fused ribs were also present.An atrial septal defect was detected by two dimen-sional echocardiography. Chromosome studies usinghigh resolution banding gave normal results (46,XY).The infant has remained dependent on a respiratorand had two episodes of pneumonia. He underwentrepair of the meningomyelocele and placement of aventriculoperitoneal shunt. The infant's parents are
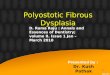
Figure 2 Anteroposterior radiograph showing shortening ofthespine and vertebral and rib abnormalities.
both American Indian, remain unmarried, and arenon-consanguineous. The mother denies knowledgeof similar cases in their respective families. There wasno history ofteratogen exposure during the pregnancy.The father is 30 years old. A 5 year old sib is normal.
DiscussionIn 1975, Wynne-Davies2 made the observation thatsibs of patients with localised multiple vertebralanomalies had an increased incidence of anencephalyor spina bifida cystica compared to the incidence inthe general population and suggested an aetiologicallink between these two conditions. Subsequendy,Naik et a13 performed a radiological necropsy study ofvertebral and rib malformations in children withmyelomeningocele. Sixty-four had anomalies, includ-ing fused vertebral arches, fused vertebral bodies,absence of vertebral bodies, and absent or fused ribs.Similarly, anomalous ribs seem to occur with increasedfrequency in patients with myelodysplasia. In theseries reported by McLennan,4 the first nine ribs wereabnormal and vertebral anomalies were found con-comitantly with abnormal ribs in about 50% ofpatients with spina bifida.Lendon et aP compared the radiological records of
patients with multiple vertebral anomalies and acomparable number of patients with spina bifidacystica. The incidence of hemivertebrae and of rib,vertebral body, and vertebral arch fusions weredetermined. The total number of bone anomalies inthe multiple vertebral anomalies group far exceededthat seen in the spina bifida cystica group; however,the distribution of these anomalies were similar inboth groups. Although the study of Lendon et a15suggests an aetiological connection, it does not provideproof of such an association.
Spina bifida occulta appears to be a commonfinding in spondylocostal dysplasia (Jarcho-Levinsyndrome). We surveyed 59 reported cases with thiscondition and found spina bifida occulta in 24(40 6%).' 6-9
Until recently, neurological abnormalities were notconsidered to be associated with the Jarcho-Levinsyndrome. Poor et al7 described a case of thissyndrome associated with cerebral polygyria. Reyes etal8 reported a case of Jarcho-Levin syndromeassociated with diastematomyelia. These authorsclaim that neurological abnormalities should be con-sidered a component of the Jarcho-Levin syndrome.This suggestion is further supported by the review ofa case published in 1976 in which thoracolumbarrachischisis accompanied the cardinal features of theJarcho-Levin syndrome.9 The infant was born to awoman who abused lysergic acid diethylamide duringpregnancy. The case reported here is unique in thatdiastomyelia and meningomyelocele occurred inassociation with findings characteristic of the Jarcho-
52
on Novem
ber 14, 2020 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.28.1.51 on 1 January 1991. D
ownloaded from

Spondylocostal dysplasia and neural tube defects
Levin syndrome. Pathological reports indicate that atnecropsy partial or complete diastematomyelia occurs
in about 30 to 35% of spinal cords involved inmeningomyelocele. '0
Our case also presented non-skeletal malformationspreviously described in patients with Jarcho-Levinsyndrome.7 They included cleft palate, triangularopening of the mouth, imperforate anus, unde-scended testes, and dextroposition of the heart withatrial septal defect. Macrocephaly was the result ofhydrocephalus accompanying aqueductal stenosis, a
feature not previously described.The Jarcho-Levin syndrome is commonly familial
but sporadic cases are well recognised. In a recentreview of 39 patients with this syndrome, 35 were
considered as having a recessive disorder and four a
dominant one.'It is possible that the Jarcho-Levin syndrome is
under-reported. The concomitant findings of neuraltube defects may preclude its recognition as a separateentity because of the well known association ofvertebral and rib anomalies with spinal dysraphism.The involvement of vertebral bodies at all levels of thespine is an important diagnostic feature in the Jarcho-Levin syndrome.The full phenotypic manifestations of a rare auto-
somal recessive gene become evident only when a
sizable number of affected patients have been evalu-ated. Although a putative association between theJarcho-Levin syndrome and malformations of the
spinal cord remains contentious, study of familialcases of the syndrome may provide evidence of anaetiological link. The concomitant presence ofspondylocostal dysplasia in some members of a familyand neural tube defects in others would prove that therelationship between the two conditions is not merelycoincidental. The genetic implications of the diagnosisof the Jarcho-Levin syndrome highlight the impor-tance of its recognition.
I Ayme S, Preus M. Spondylocostal/spondylothoracic dysostosis:the clinical basis for prognosticating and genetic counseling.Am J Med Genet 1986;24:599-606.
2 Wynne-Davies R. Congenital vertebral anomalies: aetiology andrelationship to spina bifida cystica.I Med Genet 1975;12:280-8.
3 Naik PR, Lendon RG, Barson AJ. A radiological study ofvertebral and rib malformations in children with myelo-meningocele. Clin Radiol 1978;29:427-30.
4 McLennan JE. Rib anomalies in myelodysplasia. Biol Neonate1976;29:129-41.
5 Lendon RG, Wynne-Davies R, Lendon M. Are congenitalvertebral anomalies and spina bifida cystica aetiologicallyrelated?I Med Genet 1981;18:424-7.
6 Herold HZ, Edlitz M, Barochin A. Spondylothoracic dysplasia.Spine 1988;13:478-81.
7 Poor MA, Alberti 0, Griscom T, Driscoll SG, Holmes LB.Nonskeletal malformations in one of three siblings with Jarcho-Levin syndrome of vertebral anomalies. J Pediatr 1983;103:270-2.
8 Reyes MC, Morales A, Harris V, Barreta TM, Goldbarg H.Neural defects in Jarcho-Levin syndrome. J Child Neurol1989;4:51-4.
9 Elier JL, Morton JM. Bizarre deformities in offspring of user oflysergic acid diethylamide. N Engl J Med 1976;283:395-7.
10 Emery JL, Lendon RG. The local cord lesion in neurospinaldysraphism (meningomyelocele). J7 Pathol 1973;110:83-%.
53
on Novem
ber 14, 2020 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.28.1.51 on 1 January 1991. D
ownloaded from