-
SPONDYLITISPLUSspring 2007
MICHAEL WARD, MDAT ACR
CELEBRATINGTHE KAUTZ FAMILY'S
LONGSTANDINGSUPPORT
HOW YOU CANHELP ADVANCE
GENETIC RESEARCH
-
UPFRONT
SPONDYLITIS
ASSOCIATIONOFAMER
ICA
SPONDYLITIS ASSOCIATIONOF AMERICAP.O. Box 5872Sherman Oaks, CA
91413Phone (818) 981-1616Fax (818) 981-9826e-mail:
[email protected]
SAA MISSION
To be a leader in the quest to cure
ankylosing spondylitis and related
diseases, and to empower those
affected to live life to the fullest.
BOARD OF DIRECTORS
David Hallegua, MD, ChairBrian MacKenzie, Vice ChairJeff Horn,
TreasurerHon. Ellen Carroll, SecretaryKimberly CooperLeslie Kautz,
CFACharlotte HowardAnn Kittell HowatMichael Supancich, MDRobert
Ulrich, PharmD
HONORARY BOARD MEMBERS
Rico BrognaVal HalamandarisMimi Kennedy
EXECUTIVE DIRECTOR
Katherine Culpepper
ASSOCIATE EXECUTIVE DIRECTORAND PROGRAMS DIRECTOR
Laurie M. Savage
DIRECTOR OF DEVELOPMENT
Susan L. Jones
SPONDYLITISPLUSPublished four times a year
Laurie M. Savage, Editor-in-Chief
Kristina Anderson, Contributing Writer
Susan Jones, Contributing Writer
Diann Peterson, Contributing Writer
Design by Cause Communications
Printing by PMF Productions, Inc.
Content is for informational purposesonly. The SAA does not
endorse orrecommend any medications or productsfor spondylitis, and
always advises thatyou seek the counsel of a physicianbefore
initiating any treatment forspondylitis. Annual subscriptions
areavailable with a membership.
MY FIRST SIX MONTHS AT SAA HAVE BEEN VERY BUSY.SAA’s calendar of
scientific meetings, Patient EducationSymposiums and support
groupmeetings has provided several oppor-tunities for me to observe
and participate in the various programs.
In November, the SAA staff and I traveled to Washington DC to
participate inthe annual scientific meeting of the American College
of Rheumatology. Thisyear’s meeting brought together more than
10,000 clinicians and researchersfrom around the globe to share
information and foster advances in rheumatology.
While in the DC area, we presented a Patient Education Symposium
that broughttogether more than 100 SAAmembers who spent the day
interacting with some ofthe leading specialists in the field of
spondylitis. That same week, we held ourannual Medical &
ScientificAdvisory BoardMeeting. It was very inspiring to meetand
interact with the many talented physicians and researchers
dedicated to findingthe cure and advancing the treatment of AS and
related diseases.
Later in November, I had the opportunity to visit San Diego and
attend a SupportGroup Meeting led by Mike Supancich, one of SAA’s
National Board members.I was impressed by the amount of helpful
information and tips shared among themembers of the group.
As I indicated in my first column, in addition to SAA’s focus on
key researchprojects, we plan an aggressive calendar of Patient
Education Symposiumsthroughout the year. Arrangements have been
finalized for a presentation inChicago on March 10th, and we’re now
confirming plans for a symposium inLos Angeles in May. The Los
Angeles meeting will coincide with SAA’s firsttraining session for
group leaders from among our network of support groupsacross the
country. In addition, later this summer, we will be releasing
addit-ional Fall and Winter dates for meetings in other key
metropolitan areas.
I hope you find this issue of Spondylitis Plus informative and
useful.
Katherine CulpepperEXECUTIVE DIRECTOR
2 spring 2007 SPONDYLITIS PLUS
-
4 | TASC INTRODUCESNEW COORDINATOR
6 | IN FOCUSREPORTING HIGHLIGHTSFROM ACR
10 | IN FOCUS
UPDATE FROM THE SOCIAL
SECURITY ADMINISTRATION
FEATURES
FOCUS
FOCUS
RESEARCH
ARTICLES
5 | CIGARETTES & ANKYLOSING SPONDYLITISMAKING THE
CASEAGAINST SMOKING
8 | CELEBRATING SAAsFORMER EXECUTIVE DIRECTOR
9 | CELEBRATING THE KAUTZ FAMILY'SLONGSTANDING SUPPORT
12 | CAR DRIVING WITH ASHOW SAFE IS IT?
ALSO IN THIS ISSUE
5 | HOW YOU CAN HELP ADVANCEGENETIC RESEARCH
Dear SAA,I really enjoyed reading Dr. Maksymowych’sarticle
regarding bisphosphonates. It is veryinteresting. Several months
ago, I receiveda newsletter for men who have prostratecancer, in
which it recently warned of a rareside effect of using IV
bisphosphonates.Could Dr. Maksymowych please shed somelight on this
issue?
JAKE SIMMONSLake Placid, NY
Dr. Maksymowych responds: (reprinted from2006) the issue raised
by this reader describesa report of 63 patients with bone
malignancythat developed aseptic necrosis of the jaw –essentially
death of the bone. It should beborne in mind that additional
factors such aschemotherapy, recent dental surgery, steroids,and
oral infections could have been a factorand were present in most of
these patients.No similar cases have been identified in otherlarge
scale and long-term studies of bisphos-phonates. Furthermore, this
complication wasnot observed in pre-clinical studies wherehigher
doses were used than currently used forosteoporosis. There is now
safety data on anestimated 20 million patient-years for one
bis-phosphonate, alendronate. It is important tocontinue to observe
and carefully evaluate anddistinguish chance associations and
causalrelationships.
Dear SAA,I am pleased to send you this donation,though I know
that it is small, I hope that itwill help in someway. I raised this
money
by playing my violin and by singing in thetown square of
Chautauqua, New York thissummer. Because my dad has spondylitis,
Iwanted to help find a cure, and since my BatMitzvah is coming up,
I decided to do thisfor one of my mini community projects. Ireally
worked very hard to earn this moneyand I hope that it will
help.
JAINIE WINTER(address withheld)
Editor’s note: we received this wonderfulnote by mail along with
an accompanyingdonation check in the amount of $54.25Thank you,
Jainie.
Dear SAA,I really appreciate the information I receivethrough
your magazine and web site. I’m a62 year old male who has had
ankylosingspondylitis more than half my life (the onsetwas in about
1972). I’ve suffered much painover all those years, and during the
past5-6 years have become increasingly bentforward. I learn to cope
as it progresses anddon't let it stop me, but it does get
frustratingat times (particularly now as I can’t do manysimple
things I always did in the past – likelook up to put something on a
shelf or dosome maintenance project around my house).
Having just moved halfway across the US(from Washington, DC to
Kansas City, MO),I now have to find a new doctor to assist me.I’m
using your online list/recommendationsin attempting to select one.
Please keephelping us with all relevant information. It
may not straighten my spine, but sometimesit helps to know I'm
not alone, and to findout the latest information.
I believe it’s important for everyone to keepa positive
attitude. I hope others who sufferfrom ankylosing spondylitis or
any otherserious ailment also can learn to accept that,no matter
how bad it may seem, there areothers who suffer from even much
worseailments. Over the years I’ve watched closefamily and personal
friends die from thoseworse ailments. Mine's not nearly that
bad.
To all of the SAA staff and volunteers,thanks for being there.
And thanks for pro-viding a source of information about what'sgoing
on. It’s very important. Folks like mecan use whatever support and
informationyou can give us.
Take care,
KENT HOWERTONKansas City, MO
REA
DER
S’FO
RUM
REA
DER
S’FO
RUM
LETTERS TO THE EDITORDear Readers: We want to hear from
you,whether it be informative, uplifting, or agripe you need to
express. Include your fullname, address and daytime phone
number.
We reserve the right to edit for space and clarity.
Please send letters to:[email protected] to
Editor/SAAP.O. Box 5872, Sherman Oaks, CA 91413
LIVING WITH SPONDYLITISLIVING WITH SPONDYLITIS
www.spondylitis.org 3
-
In recent years, a great deal of progress has been made in
shedding light on the potential causes of AS and in seeing the
advent of improvedtreatments that show tremendous hope for people
with AS and related diseases. Much of this is due to the work of
dedicated researchers, butalso to people like you who have
participated in the NASC study, (The North American Spondylitis
Consortium), which evolved from the ASFamily Genetic Project. Data
generated in that project include the discovery of regions on
chromosomes that further our understanding ofsusceptibility toward
AS. In addition, the data suggest that genes may play a significant
role in severity and outcomes of the disease. New and
moreestablished theories are being explored in regard to the
potential relationship between microbes, genes--particularly
B27--and inflammatorymechanisms in the gut/blood barrier that might
be involved in triggering AS and enteropathic arthritis.
Introducing Omolade Ogun,the SAA’s study Coordinator for
TASC
Omolade Ogun was born and raised in Lagos, Nigeria. Sheattended
the College of Medicine, University of Lagos, whereshe completed a
six-year combined Bachelors of Medicine/Bachelors of Surgery
degree. Subsequently, she trained as an intern atthe Lagos
University Teaching Hospital in 2001. In 2002, she moved toLos
Angeles. She has volunteered at various healthcare facilitiesin
Southern California. She works part time as a Health
Screener,performing screening activities at health fairs, where she
has been ableto use her medical knowledge to educate people on
health issues. Herpassion is to educate patients and treat them
with the respect and individ-uality that allows them to make some
of the most important decisions intheir lives.
Omolade worked at the David Geffen School of Medicine at UCLA
inWestwood, California, as Clinical Research Associate in a major
multi-center, double blind, placebo controlled study to assess Lung
Function
Decline in Chronic Obstructive Pulmonary Disease patients taking
the trial medication. She credits her mentor, Donald Tashkin, MD,
and the timeshe spent at the David Geffen School of Medicine for
inspiring her to dedicate her time to clinical research. She also
strongly believes thatenergetic and creative dedication to clinical
research leads to outstanding biomedical achievement that
translates to significant changes in clinicalsettings. This is what
led her to join the Spondylitis Association of America as Study
Research Coordinator in October 2006.
The Interrelated Projects of the Grant1. To identify the genes
that cause AS(Matthew Brown MD, John D. Reveille MD)
2. To identify the genes that predict severityand
outcomes(Michael Weisman MD)
3. To identify the spectrum of related diseasesin family members
of people with AS(John C. Davis MD MPH)
4. To determine how the genes interact witheach other(Momiao
Zhong PhD, Xioudong Zhou MD)
4 spring 2007 SPONDYLITIS PLUS
CALL TO ACTION: GENETIC RESEARCH NEEDS YOU!
Update on TASC (“Triple A” Spondylitis Consortium)
WE NEED YOUR HELP!A Call for Research Participants
� People who have been diagnosed with AS� Non affected spouses
of people with AS� Non affected friends of people with AS
If this describes you, and you would like to help, andhave not
already participated in an AS Genetic Study,please call: Omolade
Ogun (800) 777-8189 x224 oremail [email protected]
The SAA is grateful to close to 100 people with aconfirmed
diagnosis of AS who have contacted us sinceNovember to find out how
to enroll in the study.
RESEARCHPhoto:ChrisMiller
-
www.spondylitis.org 5
Many people, most of them smokers,will not read this article
furtherthan this because they thinkthey’ve heard it all before.
Patience please! Ifyou have AS and smoke, you really need tothink
hard about giving up, even more thanpeople without AS. The reason
is becausethere are many factors peculiar to AS thatsmoking
detrimentally affects.
Why write this article now? Because we havejust analyzed the
data from the first 6 monthsof our AS Specialist Clinic in
Brisbane, andthe standout finding was that AS patients whosmoke had
far worse disease activity thanthose that do not, with a mean
BathAnkylosing Spondylitis Disease ActivityIndex which was 50%
worse than non-smokers. That’s a huge difference.
What are the effects of smoking in AS?
• Smokers are more likely to develop AS.
• AS is associated with a 50% increase inmortality rate compared
with age- andgender- matched people without AS,mostly due to
cardiovascular disease.Smoking will exacerbate this.
• AS is commonly associated with lungdisease. In a recent study
40% of ASpatients were found to have significantlung abnormalities
on close examina-tion. Also, because AS leads torestriction of
chest wall movement dueto fusion of the thoracic spine and
ribjoints. AS patients have less res-piratory “reserve” than those
withoutAS. So if you smoke and do even moreharm to your lungs, then
you willdevelop respiratory failure much fasterthan people without
AS.
• AS commonly causes osteoporosis.People who smoke are twice as
likelyto develop hip fractures than those whodon’t, so why add
another risk on topof the risk you have with your ASanyway?
• Smoking is associated with stomach
ulcers. AS patients are at increased riskanyway of stomach
ulceration throughNSAID usage. So smoking just addsanother
risk.
• If you get smoking-induced chronicbronchitis, you may be
excluded fromreceiving TNF-blocker treatments,which are extremely
effective in AS.
There are lots of other reasons why youshouldn’t smoke which
apply generally andare not specific to AS, such as:
• It causes a wide range of cancers
• It causes heart attacks, strokes andperipheral vascular
disease (leadingsometimes to the need for amputations)
• It costs a lot of money
• It makes you smell bad
So what can you do to stop smoking? Here aresome tips to help
you quit successfully.
• Set a date to quit. Choose a date whenthere will be a low
amount of pressureon you, two to three weeks from now.
• Plan for the most risky times. Planactivities that will not
expose you tosituations where you will be tempted tosmoke.
• Enlist the support of your friends andfamily.
• Hold a clean up ritual. Clean cigarettesout of your car,
handbag, briefcase andhouse. Get rid of ashtrays and lighters.
• Think of yourself as a non-smokerfrom the moment you quit.
• Understand withdrawal symptoms.These are reactions that your
body mayexperience as it flushes itself ofnicotine and other
chemicals. Think ofthese as recovery symptoms. Somerecovery
symptoms will come and goover a period of a few days, and mostare
gone within two to three weeks.Emotional symptoms, such as
anxietyand irritability, are closely tied to thephysical reaction
of your body as thenicotine leaves your system.
• Remember the 4 ‘D’s.’�Delay acting on the urge to smoke.After
five minutes, the urge tosmoke weakens and your resolve toquit will
come back.
�Deep breathe. Take a long slowbreath in and slowly out
again.Repeat three times.
�Drink water.
�Do something else. Take your mindoff smoking by taking
action.
• Reward yourself. Put aside the moneyyou would have spent on
cigarettes in ajar – you may be surprised by theamount of money you
can save.
• Remember, having “just one” will hurt.This is the way that
most people goback to smoking.
• If you have a relapse, don’t despair anddon’t give up on your
plans to quit.Most people who have successfullyquit smoking for
good have madeseveral serious attempts. Every daythat you have
spent smoke-free makesyour body healthier and helps to breakyour
habit and weaken your addiction.
Do something to help yourself. Stop smoking!
CIGARETTE SMOKING AND ANKYLOSINGSPONDYLITIS By Professor Matthew
Brown, Princess Alexandra Hospital, Brisbane
LIVING WITH SPONDYLITISLIVING WITH SPONDYLITIS
-
The annual ACR scientific meeting provides an opportunity for
pre-publication examination and review of work conducted by
researchers over thecourse of the previous year. Over 100 studies
presented at this year’s ACR were related to ankylosing spondylitis
and other forms ofspondyloarthritis. The abstracts from the meeting
provide us a unique opportunity to report on the considerable work
that is being done, both in theU.S. and worldwide, to develop
better treatment options and, ultimately, to find the cure.
On the Saturday prior to the opening of the scientific meeting,
SAA sponsored a Patient Educational Symposium that brought together
160 patients,family members, friends and SAA supporters with some
of the leading experts in the field of spondylitis. Drs. John
Reveille and Michael Ward andPhysical Therapist, Ms. Victoria Gall
presented lectures on advancesin research, workplace and disability
issues, and disease management.In the convention center’s
exhibition area, SAA’s booth welcomedhundreds of physicians and
researchers who eagerly signed up toreceive information about our
programs and services, as well asbrochures and educational
materials to assist them with theirspondylitis patients
6 spring 2007 SPONDYLITIS PLUS
IN FOCUS
The 71st Annual Meeting of the American College ofRheumatology
(ACR), the professional association ofrheumatologists in the United
States, was held in ournation’s beautiful capital city of
Washington, D.C. fromNovember 8th through November 11th, 2006.
Thecombined attendance of the ACR and AlliedRheumatology Health
Professional (ARHP) members wasover 13,000, making it a
record-breaking year for
participation in this important scientific meeting devoted to
the rheumatic diseases.
Reporting from the
American College of
Rheumatology Scientific
Meetings, 2006
Authors:Walter P. Maksymowych and colleaguesfrom Europe and
Canada
Objective: Researchers in this study sought to identify
bloodserum biomarkers as predictors of patients at risk
forstructural damage progression in AS.
Results: Serum matrix metalloproteinase-3 (MMP-3) – anenzyme,
was found to be elevated in two-thirds of patients whowent on to
further radiographic damage in AS.
Conclusion:Dr. Maksymowych and his colleagues strongly sug-gest
that the results of the study demonstrate that testing for
thisenzyme could be a useful and inexpensive screening tool
forpatients with AS to determine their likelihood of going on
tomore severe disease.
Serum Matrix Metalloproteinase 3 is an IndependentPredictor of
Structural Damage Progression in Patients
with Ankylosing Spondylitis (AS)
Authors: Hildrun Haibel and colleagues, Germany
Objective: There has been an ongoing debate among some
clini-cians for many years with regard to the use of
Methotrexate(MTX) in AS patients. The goal of this study was to
examine thepotential therapeutic effect of MTX 20 mg given weekly
byinjection under the skin in active AS.
Method: 20 patients were enrolled in the study for a total of
16weeks. All of the patients were experiencing active disease
asso-ciated with spinal pain and 7 of whom also had peripheral
jointinvolvement.
Results: The researchers reported that 35% of the patients
hadsome response to the treatment, but none achieved
partialremission of the disease using the ASAS scoring system.
Sevenpatients experienced a non-significant decrease in the number
ofswollen joints.
Conclusion: The researchers of this study concluded that MTXdid
not demonstrate a benefit for the axial (spinal) symptoms
inpatients with active AS beyond an expected placebo-response.Thus,
in spite of current practice, they recommended that MTXnot be used
for this indication.
Methotrexate 20 mg (injected under the skin) in AS –No Efficacy
Over 4 Months Treatment in an Open
Label Pilot Study
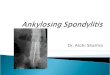
A PRIMER ON HLA-B27 IN ANKYLOSING SPONDYLITIS A group of genes
on chromosome 6 codes for the HLA (human leukocyte
antigens)antigens play a majorrole in susceptibility and resistance
to disease. Specific HLA antigens influence the development of many
common disorders. Some of these disorders, whichinclude ankylosing
spondylitis (AS), are autoimmune related and inherited in a
multifactorial manner. When a person has the specific HLA antigen
type associ-ated with the disease, he/she is thought to have an
increased chance to develop the disorder. The HLA antigen
associated with AS is called B27. People with theHLA-B27 antigen
are thought to have an increased chance (or "genetic
susceptibility") to develop AS; however, it is important to
understand that a person with-out this antigen may also develop AS.
This means HLA antigen testing is not diagnostic or accurate for
prediction of the condition.
-
www.spondylitis.org 7
Serum Retinol (vitamin A) levels are Decreasedin Ankylosing
Spondylitis and are Independent
of Disease Activity
Authors: Finbar D. O’Shea, Robert D.Inman and
colleagues,Toronto, Canada
Purpose: Vitamin A (retinol) plays an important role in
bonestructure and function, and treatment with retinoids has
beenassociated with bone abnormalities that mimic certain
diseasesthat include spondyloarthritis. In addition, in mice, the
lack ofthe gene CYP26A1 has shown to cause symptoms that mimicthose
of retinol over-dosing.
The specific aims of this study were: 1. to compare serum(blood)
levels of retinol betweenAS patients and unaffected con-trols; 2.
to correlate retinol levels with disease activity in AS; 3.to
identify any genetic association with the CYP26A1 gene.
Methods: The researchers tested for the genetic marker,
andmeasured serum levels of retinol in both AS patients and
con-trols. They also administered tests to the AS group in order
toassess disease activity.
Conclusion: The results of this study suggested that contrary
toexpectations, the serum level of retinol in the AS patient
waslower, as a group, than that of the unaffected control group.
Theresearchers also uncovered the fact that retinol did not
impactdisease activity. Furthermore, although genome-wide scans
haveimplicated p450 genes, such as CYP26A1, in the genetic
suscep-tibility to AS, the researchers caution that, to date, no
biologicalbasis for such an association has been resolved. This
study wasnot able to yield a distinct genetic association of
CYP26A1 withAS, although researchers believe that that further
analysis of thegenetic determinants of retinol metabolism in AS are
warranted.
Purpose:TNF inhibitor therapy exposes a person to a higher
riskof contracting a mycobacterial infection. Hence, the reason
thatTuberculin Skin Tests (TST) are recommended prior to
startingTNF Inhibitor therapy to screen for latent tuberculosis
infection(LTBI). The researchers who conducted this study reviewed
theresults of yearly TST testing at one institution to
evaluatewhether annual testing of patients on TNF Inhibitor therapy
canbe recommended.
Conclusion: Retesting of 379 patients receiving TNF
Inhibitortherapy revealed LTBI in 3.5%. One patient who previously
hadtested negative for a mycobacterial infection (MAI)
developedsymptoms and cultures led to a new diagnosis of MAI.
Hence,the researchers who conducted the analysis of the data for
thestudy, suggested that annual TST is warranted in order to
catchprevious false negatives as well as new infections in
patientswho are receiving TNF Inhibitor therapy.
Screening and Prevention of Mycobacterial Infectionsin Patients
taking TNF Inhibitors; the Value of Annual
Tuberculin Skin Testing
Juvenile-Onset Ankylosing Spondylitis versus Adult-Onset
Ankylosing Spondylitis for the PSOAS Cohort
The Study: It is recognized by rheumatology professionals
thatannual influenza shots are recommended for individuals
(adults)who have immuno-deficiencies, which include those that
aredrug-induced, such as TNF Inhibitor therapies. The aim of
thestudy was to evaluate whether and to what extent SID
patientssought vaccination.
Conclusion: The study results suggested that there is a low
vac-cination rate in SID patients. Two primary reasons were
associ-ated with non-compliance: 1. failure to bring it up (by the
healthcare professional) 2. patient’s fear of side-effects.
The study concluded the importance of improving patient
andphysician awareness with respect to the vaccination of patients
athigh risk of influenza complications.
Low Influenza Vaccination Rate among AdultsReceiving
Immunosuppressive Therapy for Systemic
Inflammatory Diseases
Authors: Lianne Gensler, Michael Ward, John D. Reveille,Thomas
Learch, Michael H. Weisman, John C. Davis,
Houston, Tx; San Francisco, CA; Los Angeles, CA; Bethesda,MD.
(Editor’s note: Dr. Ward is featured on the cover of thisissue of
Spondylitis Plus. He presented at a concurrent SAApatient
educational symposium, highlights of which will be
featured in the summer issue of this magazine.)
Purpose: Previous studies have suggested that patients
withchildhood onset of AS have in general more severe disease
andpoorer outcomes than people with adult onset. In this
studyresearchers evaluated the clinical and radiographic
differencesbetween the two groups. Patients in the study had
approximately20 years of disease duration.
Methods: 402 patients with a confirmed diagnosis of AS
wereenrolled in the study.
Conclusion: The researchers found that in general when
patientswith childhood onset of AS are compared to those with later
onsetin adulthood, those with childhood onset demonstrated less
spinaldisease, more hip involvement that required a hip
replacement, andthat the juvenile onset group was comprised of more
women.
Editor’s Note: Each of these studies was published in
abstractformat and presented at the ACR Scientific Meetings. These
data andconclusions should be considered to be preliminary as they
have notyet been reviewed and published in a peer-reviewed
publication suchas the ACR official journal, which is entitled
Arthritis & Rheumatism.
IN FOCUS
-
8 spring 2007 SPONDYLITIS PLUS
Tribute Dinner HonoringJane Bruckel
Once in a lifetime, an organization has the opportunity to honor
its Co-founderand retiring Executive Director, the person whose
dreams gave the organizationlife, purpose and vitality. The
Spondylitis Association of America had thatopportunity this year –
to honor Jane Bruckel and celebrate her 23 years of dedicationto
improving the lives of spondylitis patients everywhere.
This last September, SAA hosted the Jane Bruckel Tribute Dinner
at the Jonathan BeachClub in Santa Monica, California. This gala
event brought the spondylitis communitytogether to pay tribute to
the woman who changed the face of spondylitis in this country.
When diagnosed as a young nurse there was not a single patient
resource available forpatients to learn about the disease. Jane
Bruckel was determined to change that. Today,SAA publishes
thousands of educational materials for patients and physicians
alike,holds local and national symposiums and provides seed money
for the most challengingarea of all – spondylitis research – which
has brought about multi-million dollarfunding from the prestigious
National Institutes of Health.
Masters of Ceremonies and SAA Board Members David Hallegua and
Brian MacKenziepresided over an evening of tributes, testimonials
and reminiscences in honor of Jane’s bodyof achievements. Guest
speakers and presenters included Drs. John Reveille,Asim Khan
and
David Yu of SAA’s Medical andScientificAdvisory Board; Former
BoardPresidents Steve Saltzman and TomWest; and Board Members Ann
Howatand Bob Ulrich.
L.A. City Council Member Jack Weisswas on hand to present Jane
with aCertificate of Appreciation from the cityof Los Angeles in
recognition of her life-time of dedication to the
spondylitiscommunity. The evening also featured amusical
performance by Gravity and asong written especially for Jane by
inter-national singer and songwriter, HaroldPayne.
Thanks to the commitment of onewoman, supported by thousands of
SAAmembers and friends, many spondylitispatients now live more
active, morerewarding lives. The Jane Bruckel TributeDinner
provided a small opportunity forthe spondylitis community to show
herour appreciation.Top: Los Angeles City Councilmember Jack Weiss
presents Jane with
a Certificate of Appreciation from the City of Los
Angeles.Center: Jane and Harry Bruckel with loyal SAA supporters,
Jean, Floydand Damon Kvamme.Bottom: International singer/songwriter
Harold Payne performing atribute song he wrote especially for
Jane.
FUNDRAISING
-
www.spondylitis.org 9
We recently received a generous gift to the Jane BruckelResearch
Fund from the Kautz Family Foundation. TheKautz Family Foundation
has been a long-time contributor tothe Spondylitis Association of
America (SAA). Through the years, theKautz Family has provided
significant funding in the areas of advocacy,research and
organizational expansion. In 1998, the Kautz Family’s sup-port was
instrumental in helping SAA gain funding from the
NationalInstitutes of Health (NIH) to co-sponsor a major two-day
scientific sym-posium – the first symposium onAS at the NIH. The
symposium broughtscientists and researchers from related fields for
a cross fertilization ofknowledge and ideas with AS researchers. It
was an important catalyst forSAAreceiving funding from the NIH for
the Family Genetic Study and pro-viding SAA with the opportunity to
recruit key researchers to join theNorth American Spondylitis
Consortium and participate in the Study.
In 2004, Leslie Kautz, daughter of Carol and James Kautz, joined
SAA’sBoard of Directors because she “wanted to join in its passion
andcreativity for making lifebetter for people with AS."Leslie has
seen first-handthe effect that AS can haveon a person’s life. In
the1970s, she remembers theconfusion and uncertaintyher family
experiencedwhen her brother Danielsuffered the pain of ASwithout
knowing what itwas. If the SpondylitisAssociation had existedthen,
Leslie believes thatthe anguish of not knowingand the delay in
herbrother’s diagnosis couldhave been avoided. She alsoremembers
how informationfrom the SAAnewsletter gother brother started on
hispath to controlling thedisease.
Today, the entire Kautzfamily is committed to theSpondylitis
Associationand we extend our heartfeltgratitude to them for
theirgenerous support and dedication to helping SAA advance
research whileremaining the largest single source for people
affected by AS and relat-ed diseases.
Thank you!
Kautz Family Foundation
Through the years, the
Kautz Family has provided
significant funding in the
areas of advocacy, research
and organizational
expansion.
The extended Kautz Family gathers in Los Angeles.
FUNDRAISING
-
IN FOCUS
10 spring 2007 SPONDYLITIS PLUS
Social Security Cost ofLiving Adjustment (COLA)Update By
Attorney Richard I. FeingoldNew Ruling Means Changesin the
Assessment of Disability Claims
The Cost of Living Adjustment (COLA) for 2007,released by the
Social Security Administration(SSA), will be 3.3 percent. This
means that forthe more than 53 million Americans whoreceive monthly
benefits from the SSA, thosebenefits will increase 3.3 percent in
2007.
By the NumbersIn 2007, the 3.3 percent COLA increase means
that:
• Supplemental Security Income (SSI) benefits will increase
to$623/month for individuals, while the average Social
SecurityDisability Insurance (SSDI) benefit amount for a
disabledworker, spouse and one or more children will be $1,646/
month.Remember, SSI benefits are for a disabled individual
only,whereas SSDI benefits may also apply to the spouse and
childrenof a disabled worker.
• The Substantial Gainful Activity (SGA) amount will
increasefrom $860 to $900 gross earnings per month. Earning over
thisamount may prevent one from filing for disability benefits or
resultin a loss of some or all benefits.
• The Trial Work Period (TWP) amount will increase from $620
to$640 gross earnings per month. During a TWP, a person
receivingSSDI benefits is able to return to work, to test their
ability to dowork, on a trial basis for nine months.
IntroductionBy far, the most important evidence that SSA
examines in a disabilityclaim is the medical evidence. This is
somewhat obvious, because thedefinition of disability requires that
there exist a “medically deter-minable impairment.”
Medical evidence not only includes objective medical evidence,
such asmedical signs and laboratory findings, but also other
evidence frommedical sources, such as the medical history,
opinions, and statementsabout treatment received. Statements that a
disabled individual makesabout his or her impairments are also
considered, but they must becorroborated by the medical evidence in
order for them to be foundcredible and be given weight.
To help interpret the medicalevidence, and to give
bindingguidance on disability andother benefit programs,
SSApublishes several Rulings eachyear. In 2006, SSA published
aRuling entitled, “ConsideringOpinions and Other EvidenceFrom
Sources Who Are Not‘Acceptable Medical Sources’in Disability
Claims;Considering Decisions onDisability by OtherGovernmental and
Non-governmental Agencies.”
In part, this Ruling clarifies howSSA considers opinions
fromsources who are not considered
“acceptable medical sources.” The Ruling recognizes that with
the growthof managed health care and the emphasis on containing
medical costs,many people get much of their care from health care
practitioners who arenot doctors. These sources include nurse
practitioners, physician assistantsand licensed clinical social
workers. This Ruling gives guidance on howmuch weight SSAwill give
to their opinions.
Q & AQuestion:Who does SSA consider to be an
“acceptablemedical source”?
Editor’s Note:
In the November/
December 2005 issue
of Spondylitis Plus,
we published the Social
Security Administration’s
2006 Cost of Living
Adjustment figures.
Here are some updated
numbers for 2007
-
Answer: In general, “acceptable medical sources” include, for
example,licensed physicians (medical or osteopathic doctors);
licensed or certi-fied psychologists (including school
psychologists); and licensedoptometrists, although SSA may need a
report from a physician todetermine other aspects of eye
diseases.
Question:What categories of non-acceptable medicalsources are
there?
Answer: There are three categories of sources besides
“acceptablemedical sources” considered under the new Ruling:
1. “Medical sources who are not acceptable medical sources”
(forexample, nurse practitioners, physicians’ assistants,
therapists,psychiatric social workers and chiropractors);
2. “Non-medical sources” such as teachers, counselors and
socialwelfare agency staff acting in their professional capacity.
Thesesources often have close contact with the individual and
personalknowledge and expertise to make judgments about the
impairment,activities, and level of functioning over a period of
time.
3. “Non-medical sources” such as spouses, other relatives,
friends,employers, and neighbors.
Question:Why does SSA draw a distinction between“acceptable
medical sources” and other health careproviders who are not
“acceptable medical sources”?
Answer: One reason is that only “acceptable medical sources” can
give“medical opinions,” a judgment about the nature and severity of
theimpairments and the mental and physical restrictions they cause.
Inaddition, if a patient has had an ongoing treating relationship
with amedical doctor, for example, that doctor’s medical opinion
can be given“controlling weight,” which can result in a favorable
disability determi-nation by SSA.
Question:What factors does SSA consider in deciding howmuch
weight to give the opinions of medical sources whoare not
“acceptable medical sources”?
Answer: The same factors that are used to evaluate the medical
opin-ions of “acceptable medical sources” can be applied to
consider otheropinions.
As stated in the Ruling, “These factors include:
• How long the source has known the individual and how
frequentlythe source has seen the individual;
• How consistent the opinion is with other evidence;
• The degree to which the source presents relevant evidence to
supportan opinion;
• How well the source explains the opinion;• Whether the source
has a specialty or area of expertise related to theindividual's
impairment(s), and
• Any other factors that tend to support or refute the
opinion.”
Question: Is there ever a situation where the opinion of anurse
practitioner or licensed clinical social worker couldoutweigh the
opinion of a medical doctor?
Answer: It is important to keep in mind that although
information fromthese “other sources” cannot establish the
existence of a medicaldisease or illness, the information may be
based on special knowledgeand provide insight into the impairment’s
severity and how it affects anindividual's ability to function.
Under the new Ruling, it is possible for the opinion from a
medicalsource who is not an “acceptable medical source” to outweigh
the opin-ion of an “acceptable medical source,” if, for example, he
or she has hadgreater contact with the patient and can provide
better supportingevidence and an explanation of the opinion. This
can be a great boon topatients who have limited contact with a
medical doctor.
Editor’s Note We are grateful to Mr. Feingold forhis ongoing
support via the SAA website www.spondylitis.org,where he graciously
answers visitor questions on a dedicatedmessage board. Since 1986,
he has been representing dis-abled persons in their Social Security
disability claimsthroughout the United States. He a sustaining
member of theNational Organization of Social Security
Claimants’Representatives (NOSSCR) as well as a past Chair of
theChicago Bar Association's Social Security LawCommit tee. He can
be contacted by email at:Rich@FeingoldLawOff ices .com and through
hiswebsi te at www.FeingoldLawOffices.com, or by phone
at773.989.9899.
Disclaimer The information contained in this articleis provided
as a public service, is general in nature, and doesnot constitute
the rendering of legal advice or legal services.One should consult
an attorney before making any decisioninvolving a legal matter,
such as a Social Securitydisability claim.
www.spondylitis.org 11
New Social Security Ruling Means More EmphasisWill be Placedon
Medical ProvidersWho are Not “Acceptable Medical Sources”
IN FOCUS
IN FOCUS
-
12 spring 2007 SPONDYLITIS PLUS
Ask someone with AS what their biggest fear is and many
willanswer, “Getting into an automobile accident.”While there’s
always been an emphasis on driving-safety features –good brakes,
tires, seat belts, and air bags – when you start to factor in
ankylosing spondylitis, all is notequal. There is a lot at stake
withfragile ankylosed spines and necksand that raises many
questions.Should seatbelts be worn? Howshould headrests be best
used?Airbags?.Dr. Nortin Hadler, a member of theSAA Medical
Advisory Board, Pro-fessor of Medicine and Micro-b io logy / Immuno
logy a t theUniversity of North Carolina andattending
rheumatologist at UNCHospitals, graciously offeredSpondylitis Plus
the input of Dr.Barry Myers, an expert on whiplash
and the biomechanics of the spine, on the use of seatbelts,
headrests andairbags by drivers with AS.
THE ANKYLOSED SPINE IS INJURY PRONE
“These are not simple questions,” Dr. Myers thoughtfully said in
e-mail.“The severely ankylosed spine is injury prone on very modest
exposure.”
Dr. Myers, Senior Associate Dean for industrial partnerships
andresearch commercialization at Duke University’s Pratt School
ofEngineering, has extensively reviewed injury statistics and
medicalliterature. He has concluded that aside from driving
defensively andpurchasing the biggest, safest car possible, AS
patients would be bestserved by not doing anything too out of the
ordinary in their drivinghabits. “These will do more to decrease
injury rates than other interven-tions,” he observed.
SEATBELTS AND THE “AIRBAG DILEMMA”
Dr. Myers said he “strongly recommended” the use of seatbelts
despiteconcerns that an AS spine might not be able to withstand the
sheering
force the belts might create in a crash. He warned that relying
on anairbag to prevent injury, however, was way too risky. “Airbags
have avery limited range of accidents that they are effective in,
and headimpact with an ankylosed spine is devastating,” he
cautioned. “Keepingthe vulnerable kyphosed spine out of the
deploying bag is especiallyimportant.”
Dr. Myers also recommended that the headrest be set in a
position thatminimizes the gap between the head and the rest, and
also allows anadequate field of vision for the driver.
“I would not advocate retrofitting the design,” Dr. Myers
said.
Finally, there are natural concerns among AS patients that if
they wereto get into an accident serious enough to cause injuries,
they could beat risk by emergency rescuers who do not understand
the fragile natureof their backs and necks.
The SAA has done a yeoman’s job in advocating better training
foremergency medical technicians,* although Dr. Myers noted that
spinalprecautions were nonetheless pretty much standard procedure
ataccident scenes.
ALL DRIVERS SHOULD WEAR SEATBELTS
Dr. Hadler also kindly provided Spondylitis Plus with the
expertise ofanother friend and colleague, Dr. Gunnar Andersson, MD,
PhD., aninternationally recognized expert in musculoskeletal
disease and injurywho is also credited with designing the unique
seats in Volvoautomobiles.
Dr. Andersson, Professor and Chairman, Department of
OrthopedicSurgery at Rush University Medical Center, says that
education isprimary for the AS community “because of the rigidity
of their spines.”
He says that everyone should be wearing their seatbelts
“includingpatients with AS.” Dr. Andersson agrees with Dr. Myers
that dependingon an airbag for protection in an accident can be
problematic: “Whilethey provide additional protection, they do
create a problem when thespine is kyphotic because of the forces
created. Thus the seat beltclearly is the preferred protection in
this respect.”
And as for the headrest, Dr. Andersson says that is the one
feature thatwill afford you the most protection if your head is
thrown backwards,
Collective fear of a car accident
The bestcar safetydevice is arear-viewmirror witha cop in
it.
~Dudley Moore
LIVING WITH SPONDYLITISLIVING WITH SPONDYLITIS
Driving Safely With AS
-
such as in the case of a rear-end collision. He suggests using
headrestraints as opposed to stock headrests, however. “Head
restraints areactually better than headrests and can be retrofitted
if necessary.Basically, the idea is to prevent the cervical spine
from extending,which it cannot do in patients withAS very easily;
for those reasons, theheadrests may have to be flexed slightly
forward to accommodate thetypical forward flexion of an AS
patient.
DRIVING WHEN YOU HAVE AS
So keeping all these vehicle-safety caveats in mind, should the
fear ofgetting into an accident keep those with AS – with its
inherentphysical limitations – from slipping behind the wheel? Not
at all. Sincepeople with AS still need to get to where they have to
go, driving canbe a necessity – regardless of any physical
limitations.
Granted, the unique problems faced by AS patients that could
con-tribute to an increased risk in traffic include limited
range-of-motionissues, such as stiffness in the neck or other parts
of the spine and hipsthat can make it tough to maneuver a vehicle
into a parking space orthrough an intersection where the driver
needs to look around foroncoming traffic. There may also be
peripheral joint involvement thatdoesn’t allow free movement within
the confines of a car.
But studies have concluded that people with even advancedAS can
stilldrive safely by making simple modifications to their vehicle
or to theirdriving techniques. Some intrepid AS patients have used
their owningenuity to come up with devices that help
mobility-restricted driversoperate their motor vehicles.
NECESSITY IS THE MOTHER OF INVENTION
James Hall Jr. suffers from kyphosis of the spine – all
vertebrae arefused except for C1 and C3. He says he has precious
little movement inhis neck and spine, but driving is a breeze for
him due to his owningenuity.
The 58-year-old San Diego support-group member who was
diagnosedwith AS in 1975 says that he uses a “device” that he saw
mentioned inan arthritis magazine. He describes it as a
“lazy-Susan” type piece ofwood covered in foam padding and cloth
that he parks himself uponwhen he drives.
“I use it for short-distance driving where it is perfectly
tolerable,” hetells Spondylitis Plus. “It swivels my hips and
allows me to sit morecomfortably and gives me a bit of ‘extra turn’
when I come to anintersection.”
James says he also wears a cervical brace with added foam –
back-wards. He takes comfort in the fact that it provides him with
a cushionat the base of his skull and top of his shoulders.
“I’m only looking for ways to be safer while hurtling through
space ina steel box at 30 to 60 miles per hour,” he says with a
chuckle.
MIRROR EXPANDS WORLDVIEW
And then there’s Brad Sawyer, a Viet Nam-era vet with long-term
AS.His spine, neck and ribcage have fused, leaving him unable to
turn hisneck and robbing him of nearly a foot in height. Out of
dire necessity,he designed a 260-degree true-reflective mirror that
allows him toclearly see all sides coming, completely eliminating
the troublesomeblind spots. “What you see in the mirror is actually
coming, too,” hesays, “it’s a true reflection; nothing is smaller
or larger in the vision.”“It was out of absolute necessity for me
or I wouldn’t be driving,” Brad,who lives Cape Cod, recalls. “I
used to always have to have my passen-gers look around to see if
other cars were coming; my wife worriedabout me driving alone. And
one time I had a horrific near miss – and Ican tell you that the
sound of screeching brakes can be terrifying.”
The “MultiFlex Adjust-A-View Safety Mirror” (U.S. Patent
No.6926416)** actually provides for a tool-free simple attachment
to thedriver’s side sun visor giving the driver a distortion-free
imagereflection in both the left side’s and the right side’s blind
spots, and youcan easily see the passengers in the backseat,
too.
Sawyer says he has approached various carmakers with his
invention,but admits that they are proving to be a tough nut to
crack. “But if it’shelping someone drive who otherwise could not,
that’s all I care about,”he says with pride.
SOME TIPS FROM EXPERTS:
The following suggestions have been culled from many
drivingreferences sites and studies:
*Seatbelts:Always use your seatbelts with a shoulder harness:
The seat-belt is the single most important lifesaver in a crash.
Studies by theInsurance Institute for Highway Safety (IIHS),
industry group, recom-mends seat belts that are easier on fragile
shoulders and ribs. Researchby the Dept. of Transportation has
shown that lap/shoulder belts, whenused properly, reduce the risk
of fatal injury to front-seat passenger caroccupants by 45 percent
and the risk of moderate to critical injury by50 percent.
www.spondylitis.org 13
Everything in life is somewhere else,and you get there in a
car.
~E.B. White, One Man's Meat, 1943
LIVING WITH SPONDYLITISLIVING WITH SPONDYLITIS
-
14 spring 2007 SPONDYLITIS PLUS
*Brake lights: Extra high-mounted brake light to alert drivers
behindyou: Rae Tyson, a spokesperson for the National Highway
TrafficSafety Administration (NHTSA) points to a 1986 NHTSA law
changethat mandated that all new passenger cars include a center
highmounted stop lamp, or “CHMSL” – a third stop lamp, or brake
light,mounted on the rear of a vehicle. “We saw a safety benefit– a
declinein crashes,” he said. “Anything you can do to raise
visibility of avehicle is good.”
*Special mirrors: Special mirrors that offer a wider view of
what’sbehind you could be fitted onto your car. These mirrors
reduce the needto turn the head to check for cars in the driver’s
“blind spot.” Many ofthese types of mirrors are on the market;
however it is important to taketime to practice parking using these
new attachments.
*Safe car:Own a car that is known to absorb the impact of a
crash. Seethe additional research at the end of this story and
research vehicles tofit your particular needs.
*Headrests: The best seat and headrest are designed as one
system;fixed head restraints reduce the risk of neck injuries by
25%; whereasadjustable head restraints only reduce the risk by 15%.
Head restraintgeometry explained: The necessary first attribute of
an effective headrestraint is good geometry. According to the IIHS,
if a head restraintisn't behind and close to the back of an
occupant’s head, it can't preventa “whiplash” injury in a rear-end
collision. Headrests are also advisedto avoid sudden injuries to
the neck as the stiff neck of an AS patient ismore easily injured
than a normal neck.
*Cushions:A small cushion behind the back or under the buttocks
canhelp maintain good posture when driving a car.
EACH SITUATION IS UNIQUE
The above suggestions are just the beginning. There is a wealth
of richmaterial out there for drivers to consider for themselves;
what worksfor one may not work for everyone. Each safety feature
must be seri-ously considered for each individual circumstance.
And one more thing: Always do your best to avoid the jarring
potholeswhen driving. Avoiding potholes is more than just a
metaphor about life.
*See Bryan E. Bledsoe, DO, FACEP, “Ankylosing Spondylitis
PatientsNeed Special Care,” Spondylitis Plus, July-August, 2006
issue and onwww.spondylitis.org/; the article originally appeared
in the Journal ofEmergency Medical Services (JEMS); July 2006 •
Volume 31• Number 7, plus the article appears on SAA’s
website:www.spondylitis.org/
**The mirror sells for $19.99; to learn more about this safety
mirror visitwww.multiflexmirror.com
REFERENCES
SAA would like to thank The Ankylosing Spondylitis
InternationalFederation (ASIF) and The National Ankylosing
SpondylitisSociety of Great Britain (NASS), along with the late
NASSdirector, Fergus Rogers, for his kind help with this story.
Wereferred to their publication “Car Driving with
AnkylosingSpondylitis” for assistance with research. The booklet
was writtenby Dr. Jon Erlendsson, a rheumatologist based in
Denmark.
British Society for Rheumatology;1991, Driving and
ArthritisJones, J.G. and Lassere, M.N.
British Society for Rheumatology;1986, A Review of 100 Patients
with Ankylosing SpondylitisWordsworth, B.P and Mowat, A.G.
Journal of Emergency Medical Services (JEMS); July 2006Volume 31
• Number 7
The Insurance Institute for Highway Safety – IIHS
The National Highway Traffic Safety Administration
ADDING INFORMATION FOR IMPORTANTFURTHER READING AND RESEARCH
Resources for user-friendly vehicleswhere you can evaluate
options for your particular
needs:http://www.arthritis.org/resources/travel/Car_Guide/Features_love.asp
Insurance Institute for Highway Safety(for top safety picks in
vehicles)See: http://www.iihs.org/ratings/And:
http://www.iihs.org/research/bibliography/rear_crashes.html
The IIHS scores its frontal-crash results as Good,
Acceptable,Marginal, or Poor. You can find ratings for all tested
vehicles onthe IIHS Web site, at:www.hwysafety.org.
Dynamically Tested Seat/Head
Restraintshttp://www.consumerreports.org/cro/cars/safety-recalls/consumer-reports-suvs-pickup-rear-collision-and-whiplash-protection-106/index.htm
10 Safety
Checkshttp://autos.yahoo.com/consumerreports/article/safety_checks.html
LIVING WITH SPONDYLITISLIVING WITH SPONDYLITIS
-
www.spondylitis.org 15
Education & Support Meeting Facilitators
Chair:Dr. Robert Colbert, MD, PhD . . Cincinnati, OH
Bruce Clark, PT . . . . . . . . . . . . . . Vancouver, BC
Daniel Clegg, MD . . . . . . . . . . . . Salt Lake City, UT
JohnDavis, Jr., MD, MPH . . . . . San Francisco, CA
Atul Deodhar, MD . . . . . . . . . . . . Portland, OR
NortinHadler, MD. . . . . . . . . . . . Chapel Hill, NC
Robert Harris, MD. . . . . . . . . . . . Whittier, CA
Robert Inman, MD . . . . . . . . . . . Toronto, ON
MuhammadAsim
Khan, MD. . . . . . . . . . . . . . . . . . Cleveland, OH
WalterMaksymowych, MD . . . . Edmonton, AB
AllanMetzger, MD . . . . . . . . . . . Los Angeles, CA
DavidNeustadt, MD . . . . . . . . . . Louisville, KY
JohnReveille, MD. . . . . . . . . . . . Houston, TX
James Rosenbaum, MD. . . . . . . . Portland, OR
Millicent Stone,
MB, MRCP(UK) MSc . . . . . . . Bath, UK
Joel Taurog, MD. . . . . . . . . . . . . . Dallas, TX
RubenBurgos Vargas, MD . . . . . Mexico City, MX
RobertWarren, MD, PhD . . . . . . Houston, TX
Michael Weisman, MD . . . . . . . . Los Angeles, CA
DavidYu, MD . . . . . . . . . . . . . . . West LA, CA
Medical and ScientificAdvisory Board
Online Poll
You can find this new Instant Poll on ourwebsite at
www.spondylitis.org.
new pollAre you receiving Social Security DisabilityInsurance
(SSDI) benefits?
� Yes� No� Yes, however, my co-pay is too high for me to
afford the medication
� I currently am applying for SSDI.� I receive other disability
benefits.
old poll resultsDoes your insurance cover TNF-blocker therapyfor
your spondylitis?
Yes, my co-pay is within my family’s means.......56%Yes,
however, my co-pay results in a hardshipfor my family
......................................................15%No, my
current medical insurance doesnot cover TNF-blocker therapy
......................14%Yes, however, my co-pay is too high forme
to afford the medication ..........................11%I receive
assistance from a foundation,such as the Chronic Disease Fund
toreceive TNF-blocker therapy ............................ 4%Yes,
even though my form of spondylitisdoes not have an FDA indication
(off-label) ........0%No, since my form of spondylitis does nothave
an FDA indication (off-label) .................... 0%
The people listed below are a vital part of our support system.
They havevolunteered to lead support groups across the US because
they want tohelp. If you’d like to find out more about support
groups and onlinemeetings, pick up the phone or send an e-mail
to:
• Teen Athletes with AS located in Orange County - contact
[email protected] for more info.
• Little Rock, AR, Boise, ID and Portland, ME now have
Spondylitis Educational Support Groups!
• Support online from NY, NY with Michael T. Smith,
[email protected].
Little Rock, AR
Phoenix, AZ
Long Beach, CA
Long Beach, CA
Orange County, CA
San Diego, CA
San Francisco, CA
Boise, ID
Boise, ID
FortWayne, IN
Indianapolis, IN
Kansas City, MO
Augusta, ME
Portland, ME
Detroit, MI
Holland, MI
Portland, OR
Philadelphia, PA
Myrtle Beach, SC
Dallas, TX
Houston, TX
Houston, TX
Washington, DC
Seattle, WA
Mindy Hunter
John Kornfeind
Barbara Crofut
Frances Tomich
Kyle Brownfield
Mike Supancich
Eric Passmore
Tim Schaap
Cindy Salo
Ken Prather
Ken Prather
Linea Cooley
Michelle Andrews
Penny McAuley
Laura Russell
Scott May
Ken Henschel
Howard Tevelson
Alex Best
Elizabeth Smith
Richard Powell
Stephen Haskew
RogerStead
Paul Stevenson
(501) 351-6374
(623) 910-4742
(562) 421-9698
(562) 429-9685
(949) 367-0430
(760) 438-2962
(510) 644-0864
(208) 453-5006
(208) 850-3313
(260) 637-1705
(260) 637-1705
(913) 384-0728
(207) 445-2885
(207) 878-9414
(586) 530-9988
(616) 610-9130
(503) 579-8375
(215) 844-6075
(843) 655-9762
(972) 860-7179
(409) 883-7822
(281) 337-3997
(703) 455-6005
(206) 524-2186
[email protected]
[email protected]
[email protected]
not available
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
[email protected]
SAA’s Annual SpringOnline Auction
SAA’s annual Spring online auction is just a few months away.
The 7-dayE-Bay event will spread awareness of AS and related
diseases as wellas raise funds for furthering SAA’s mission to
improve the lives ofspondylitis patient throughout the country.
Auction items will include hotel packages to exotic locales,
jewelry,artwork, and autographed collectibles from famous
musicians,entertainers, sports stars, cartoonists, authors and
more!
All proceeds from the auction will go to continuing SAA’s
importantwork in advancing spondylitis research, treatment and
education.Remember – bid early and often!
LIVING WITH SPONDYLITISLIVING WITH SPONDYLITIS
-
NON-PROFITU.S. POSTAGE
PAIDWHITTIER, CAPERMIT NO.1
SpondylitisAssociationof America ™
Donate a Car today and helpadvance research tomorrow!
The process is quick and easy,includes free pick-up or
towing,and best of all the proceeds goto a cause near and dear to
yourheart—The Spondylitis Associationof America. The vehicle
doesn'teven have to run for you to donateit. Consult with your tax
advisorprior to donating a vehicle. CallHelene Hart at 800-777-8189
X 229for more information.
LOG INSAA members can now accessexclusive content in the
memberarea. Login with your email addressand ZIP code at
www.spondylitis.org
P.O. Box 5872Sherman Oaks, CA 91403
research
Save
theDate!
Are you interested in receivingmore information about
ANKYLOSING SPONDYLITIS RESEARCH?
Do you or a relative haveAnkylosing Spondylitis?
If so, you can help a research effortto develop and validate a
screening
tool for potential AS patients.
. . . . . .If you are interested, please contact:
Study [email protected]
310-423-3032
SAA Educational SymposiaChicagoMarch 10, 2007
Los AngelesMay 5, 2007
Watch for our new website S.W.I.F.T.
(Spondylitis Web Info for Teens),
launching in early 2007! This website
has information specifically for teens,
ages 13-19, including stories from
teens living with spondylitis, tips for
school and sports and activities, and
information from the doc about living
with spondylitis as a teenager. Visit
S.W.I.F.T. at http://teen.spondylitis.org
The SAA wants to help people withspondyloarthritis (AS or a
relateddisease) connect with others inlocations across the U.S.
where asupport group has not yet beenestablished.
These people would liketo connect with othersin their area:
Robert Sauls, Modesto, CA
Kelly Riedesel, Weaverville, NC
Kerry Krow, Mountain View, MO
If would like to “reach out” to any ofthese people, please
contact MelissaVelez, Programs Coordinator,
[email protected]
Reach Out andTouch Someone!