Embed Size (px)
Citation preview

Spondyloarthropathies andAnkylosing Spondylitis
Previously known as “Sero-negative arthritis”
Disease FeaturesCurrent Management
• Ankylosing (Greek ankylos)= stiffening of a joint, bent, crooked, fixed, closed
• Spondylos = vertebra.• Spondyloarthropathies: Diseases of vertebrae & joints• Ankylosing spondylitis: إلتهاب الفقرات اإللتحامي
يا قارئا تبييضا�... هل فهمت أنني... ال أحب بصم محاضرا�؟

Spondyloarthropathies (SpA)sero-negative arthritis
• A cluster of inter-related and overlapping diseases that includes 5subtypes:
– Ankylosing Spondylitis (AS)– Reactive Arthritis: Reiter’s disease– Psoriatic Arthritis (PsA)– Arthritis associated with IBD (Crohn’s disease and Ulcerative Colitis)– Undifferentiated SpAs.
• Lumbar spine is spared in which disease?– RABefore coming with a group of diseases called SpA, physicians called RA
associated with low back pain “Seronegative RA” because most it wasassociated with negative serum RF.
• SpA involves which bones in the body?– Axial spine: Spine + Pelvis
Braun J and Sieper J. Arthritis Res 2002,4:307-321
Khan MA. Ann Intern Med.2002;136:896-907
• ?What is the DDx of spondyloathropathiesسؤال راوند:

The Spondyloarthropathies
Juvenile SpA
ReactivearthritisReitersyndrome
Arthritisassociated
with Crohn’sdisease / UC
PsoriaticArthritis
Ankylosing
Spondylitis
Sacroiliitis
AAU
Undifferentiated SpA
Elyan M, Khan MA. Diagnosing ankylosing spondylitis.J Rheumatol 2006; 33 Suppl 78: 12-23.
AI+HB
AI = Aortic incompetenceHB = Heart blockAAU = Acute ant uveitis
Uvea= Uveal tract = Vascular layer of the eyeball. the vascular, pigmentary, or middle coat of the eye, comprising the choroid, ciliary body, and iris. Syn: uveal tract,
vascular tunic of eye, Haller tunica vasculosa, tunica vasculosa bulbi [TA], tunica vasculosa oculi, uvea.

Spondyloarthropathies are characterized by:• Radiographic sacroilitis with or without accompanying spondylitis:• Variable inflammatory peripheral arthritis, enthesitis, and
dactylitis• Dactylitis: inflammation of one or more fingers digits: all joints in the digit are inflamed)• Enthesitis: Condition occurring at the insertion of muscles where recurring concentration of muscle stress provokes inflammation
with a strong tendency toward fibrosis and calcification. = insertions of tendons into bones become inflamed)
– Association with chronic inflammatory bowel disease– Association with psoriasis and other mucocutaneous lesions– Tendency for anterior ocular inflammation (AAU)– Increased familial incidence– Occasional aortitis and heart block– No association with rheumatoid factor (sero-negative).– Strong association with HLA-B27 (discovered in 1973).
• RA: Synovitis• SpA: Enthesitis (the main pathology of SpA)• Joints invovled: Usually axial involvement (spine & pelvis)• Uveitis: Anterior is better than posterior

Association of Spondyloarthropathies withHLA-B27 in White Persons
Disease Approximate Prevalenceof HLA-B27, %
Ankylosing spondylitis 90Reactive arthritis 40–80Juvenile spondyloarthropathy 70Enteropathic spondyloarthritis 35–75Psoriatic spondyloarthritis 40–50Undifferentiated spondyloarthropathy 70Acute anterior uveitis (acute iritis) 50Aortic incompetence with heart block 80* Uveitis is of acute not of the chronic type and is anterior not posterior
Khan MA. Ann Intern Med.2002;136:896-907
HLA-B27 prevalence in healthy population is approximately 8%.- HLA-B27 was discovered in 1972. It is one of the important landmarks in the history of Rheumatology.

Epidemiology ofSpondyloarthropthies
• Prevalence of SpA is 0.6 – 1.9%.– Do you conclude that it is a rare disease? Not!
• Prevalence is close to Rheumatoid Arthritis.• AS prevalence is 0.1- 1.1%.• 13.6% of all individuals positive for the HLA B27 antigen had a
spondyloarthropathy.• Prevalence of HLA B27 varies between 1% (Japanese) to 40% (Eskimos and
Inuits).• The risk for spondylo-arthropathies among HLA-B27–positive persons who have
a first-degree relative with ankylosing spondylitis is increased threefold (30%instead of 10%).
Braun J and Sieper J. Arthritis Res 2002, 4:307-321Khan MA. Ann Intern Med. 2002;136:896-907
Dougados M. Joint Bone Spine 2001 ; 68 : 557-63
Risk of spondyloarthropathy % of general population
Nomral people 0.6-1.9%
Person HLA-B27 +ve 13%
HLA-B27 +ve & FH 30%
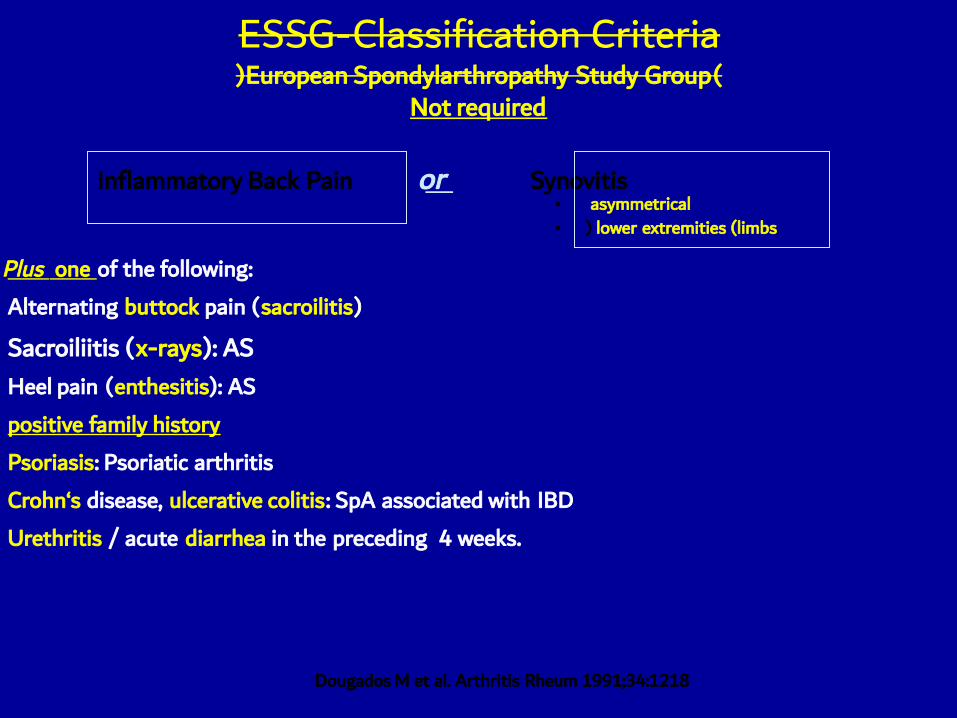
ESSG-Classification Criteria(European Spondylarthropathy Study Group)
Not required
Plus one of the following:Alternating buttock pain (sacroilitis)
Sacroiliitis (x-rays): ASHeel pain (enthesitis): ASpositive family historyPsoriasis: Psoriatic arthritisCrohn‘s disease, ulcerative colitis: SpA associated with IBDUrethritis / acute diarrhea in the preceding 4 weeks.
Inflammatory Back Pain or Synovitis• asymmetrical• ) lower extremities (limbs
Dougados M et al. Arthritis Rheum 1991;34:1218

Ankylosing Spondylitisالالصق الفقار التهاب
• Most typical and common form of SpA.• Chronic inflammatory joint disease of unknown cause that
mainly affects the spine and the joints between the base of thespine and the pelvis.
• A chronic and progressive form of sero-negative arthritis.– Most common joints affected?
• Shoulder + Hip– Any inflammation is more at which part of day? In relation to activity?
• At nigh (2nd part of night… associated with morning stiffness) + At rest
– Chest wall pain might be misdiagnosed as MI– Etiology: Genetic predisposition & infection (Klebsiella)

AS: A Complex Disease
• Chronic, systemic, and progressive inflammatory disorder1,2
• Characterized by involvement of the axial spine1
• Affects the sacroiliac (SI) joints and may also affect peripheral joints,including hips, shoulders, and ankles1
– Don’t say it is an AS without sacroilitis
– Sacroilitis is necessary to diagnose SpA
• Manifests the enthesitis typical of the spondyloarthropathies (SpAs)2
• Recurrent back pain and loss of spinal mobility may progress tospinal fusion (ankylosis)2
• May affect extra-articular sites2
References: 1. Brophy S et al. J Rheumatol 29 :1236-1243, 2002. 2. Sieper J et al. Ann Rheum Dis 61 (Suppl III):iii8-iii18, 2002.

Ankylosing spondylitis: ankylosis, lumbar spineLimited spine motion is a frequent finding ofankylosing spondylitis. The patient's attemptto touch the floor with his fingers whileholding his knees straight revealed markedlimitation of flexion. Lumbar flattening or lossof the normal lumbar curvature ischaracteristic. The flexion seen in this patientoriginates almost entirely from hip, not spine,motion.
Stiffness of the backLimited spine movementFlattening of normal lumbar curvature = Lossof lumbar lordosis

Clinical Features of AS
• Chronic inflammatory back pain.– Pain when? At night– Morning stifness & back pain
• Sacroiliitis• Ankylosis• Kyphosis• Peripheral joint affection• Uveitis• Systemic manifestations (fever,
anorexia, anemia) Name of posture? Questionmark posture

Chronic Inflammatory Back Pain• Age of onset below 40 years• Insidious onset• Duration greater than 3 months before medical attention is sought• Morning stiffness and improvement with exercise or activity.
AS should be differentiated from other causes of back pain (mechanical or degenerative –seetable below, metabolic, infectious and malignant).
Inflammatory Mechanical
Age of onset Below 40 Any ageOnset Gradual SuddenWorse pain Morning EveningMorning Stiffness Present AbsentEffect of exercise Relieves pain Aggravates pain
Inflammatory back pain is characterized by: Age of onset below 40 years, insidious onset,duration greater than 3 months before medical attention is sought, morning stiffness andimprovement with exercise or activity.

Typical joints involved:
LumbosacralHipJoints

Ankylosing spondylitis:iridocyclitis with synechiae
Acute Anterior uveitis

- Modified Shober’s test- Step:
- 10 cm from the lumbosacral joint- Ask patient to bend forward- Your hands should move appart > 5 cm
- Another method: Assessment of chest expansion. Also, itshould be > 5m. In AS, it is <5 cm.
- Patient with AS complain of chest pain due to? Enthesisits- Costosternal- Costovertebral- Costocartilage

Diagnosis of AS
Modified New York Criteria (1984):• Criteria components
1. Low back pain of at least 3 months’ duration that improved byexercise and was not relieved by rest
2. Limited lumbar spinal motion in sagittal (sideways) and frontal(forward and backward) planes
3. Chest expansion decreased relative to normal values for sex andage
4. Bilateral sacroiliitis grade 2–4 or unilateral sacroiliitis grade 3 or 4– Definite ankylosing spondylitis if criterion 4 and any one
of the other criteria is fulfilled
van der Linden S, Valkenburg HA, Cats A. Arthritis Rheum . 1984;27:361-8

Radiological Findings in AS• Early:• Sacroiliitis (closed arrow):
– Erosions– Sclerosis
• Late:• Vertebra (open arrow):
– Syndesmophytes• Syndesom: ligament• An osseous excrescence
(outgrowth) attached to aligament. Origin [syndesmo- +G. phyton, plant]
– Calcification of ligaments(tramline appearance)
– Squaring of vertebrae due toerosions of their corners.

Radiological Findings In AS
Bilateral sacroiliitis. Frontalradiograph shows bilateral sacroiliac
joint erosions and iliac sidesubchondral sclerosis.
Bilateral chronic sacroiliitis. Frontalradiograph shows complete fusion of
both sacroiliac joints.
Wilfred CG Peh. Ankylosing Spondylitis. www.emedicine.com. Updated March 2002.
- On X-ray, how does sclerosing appear?- white colored on X-Ray

Ankylosing spondylitis: earlysacroiliitis (radiograph)
Right: Pseudo-wideningLeft: Decreased space. White color indicates sclerosing.

Ankylosing spondylitis: advancedsacroiliitis (radiograph)

- Sites of ligaments insertion- Undergo? Inflammation- Next? Erosion- Finally, the shaped of the vertebra will be “square-like”- Bambo spine- Calcification = syndesmophytes- Ensethitis → Erosion → Damage → loss of angle

Radiological Findings In AS
Lateral radiograph shows anteriorcorner erosions at the T12 and L1vertebral bodies. The typical shinycorner sign (or Romanus lesion) is
present (arrows).
Vertebral body squaring. Lateralradiograph shows squaring of L3 andL4 vertebral bodies, L3-L4 anterior
syndesmophyte, and lumbar facet jointfusion.
Wilfred CG Peh. Ankylosing Spondylitis. www.emedicine.com. Updated March 2002.
- Shiny corners indicates? Squaring- Shape of vertebrae will be? Bamboo-like



Laboratory Findings in AS• No diagnostic test:
– HLA-B27 gene (90%)– High ESR, CRP– How to differentiate between elevated ESR and CRP in AS and in RA?
In AS, it is not as high as RA– Mild normocytic normochromic anemia [What is the type of this anemia?
Anemia of chronic disease]– High AP (alkaline phosphatase) (in severe cases)– High serum IgA levels– -ve RF, ANA– Synovial fluid similar to other inflammatory arthritis .– Pulmonary functions: Low VC, High FRC
• To diganose AS: X-Ray + HLA-B27 + ESR & CRP• MRI can show the presence of sacroilitis. But to appear on X-Ray, it
requires 5-7 years.

Bone Scintigraphy• Helpful in AS patient with normal or
equivocal radiograph findings.• Quantitative analysis: ratios of
sacroiliac joint to sacral uptake of 1.3:1or more are considered abnormal.
• ↑ bone scintigraphic uptake also maybe used to evaluate active disease
• What can you see in the image at theright?– Increased uptake at the sacroiliac joint
– In sacroilitis, there is increaed uptake ofisotope.
Wilfred CG Peh. Ankylosing Spondylitis. www.emedicine.com. Updated March 2002.

Magnetic Resonance Imaging (MRI)
• Best for early detection of skeletal involvement– 5 to 7 years before findings start to appear on X-Ray.
• No associated radiation; so especially valuable in adolescents & young women• Use MRI STIR technique; no need for gadolinium enhancement• Major problems: high cost & relatively restricted availability• Does MRI have advantage over X-ray?
– Yes, 7-8 years before sacrolilitis can be revealed by an X-ray, it can be seen using an MRI– Q: Pt was found to have sacroilitis using MRI, does he have ankylosing spondyloitis?
• Criteria is based on X-ray showing sacroilitis not MRI!
• In clinical practice, what do you request first: X-ray or MRI?– X-ray. If showed nothing, you can then consider requesting an MRI

Weber U, Pfirrmann CWA, Khan MA. Ankylosingspondylitis: update on imaging and therapy. Int J
Adv heumatol. 2007;5(1):2-7

• NSAIDs are recommended as the first-line drugtreatment for AS patients with pain and stiffness.
In those with increased GI risk , non-selective NSAIDs plusa gastro-protective agent, or a selective COX-2 inhibitorcould be used.
*ASessment in AS International Society
Zochling J, et al. Ann Rheum Dis . 2006;65:442-452.
ASAS*/EULAR Recommendations for theManagement of Ankylosing Spondylitis

Efficacy of NSAIDs in AS
(good or very good efficacy)
Amor B, et al. Rev Rheum Engl Ed . 1995;62:10-5.

• There is no evidence for the efficacy of thetraditional DMARDs, including MTX, for thetreatment of axial disease of AS.
• Sulfasalazine may be considered in patients withperipheral arthritis.• peripheral arthritis فقط هو الذي يستعمل من المجموعة ويستعمل إذا كان هناك
*ASessment in AS International Society
Zochling J, et al. Ann Rheum Dis . 2006;65:442-452.
ASAS*/EULAR Recommendations for theManagement of Ankylosing Spondylitis

Active AS
TNF Antagonists
Treatment Algorithm26
C/S Injections? ???
Sacroiliac Axial Entheses Periph jts
NSAIDs Exercise
Sulfasalazine
C/S Injections C/S Injections
In peripheral, if C/S (corticosteriods) injections didn’t work, you then use sulfaslazine

Psoriatic Arthritis• AGE of on set• Psoriasis usually appears in the second and third decades of life arthritis
delayed by some 2 decade.• juvenile P S A: 9-12 years• Sex Ratio: 1-1
– Percentage of population who have psoriasis? 1%– Percentage of those with psoriasis who will develop psoriatic arthritis? 20%– Can a patient have arthritis before he develops psoriasis?
• Unfortunately! You can’t execlude psoriatic arthritis!
– There may be a urethritis before skin manifestations

Psoriatic arthritis has subtypes:Group (1):Predominant involvement of DIP's: 8-16%.Nails shows? Nail pitting. This is not seen in RA. Only in psoriasis.

Group (2): Arthritis Mutilan's• - Osteolysis of the phalanges and Metacarpal's 5%.• - Often associated with sacorilities.• شكلها زي الجرس؟؟؟
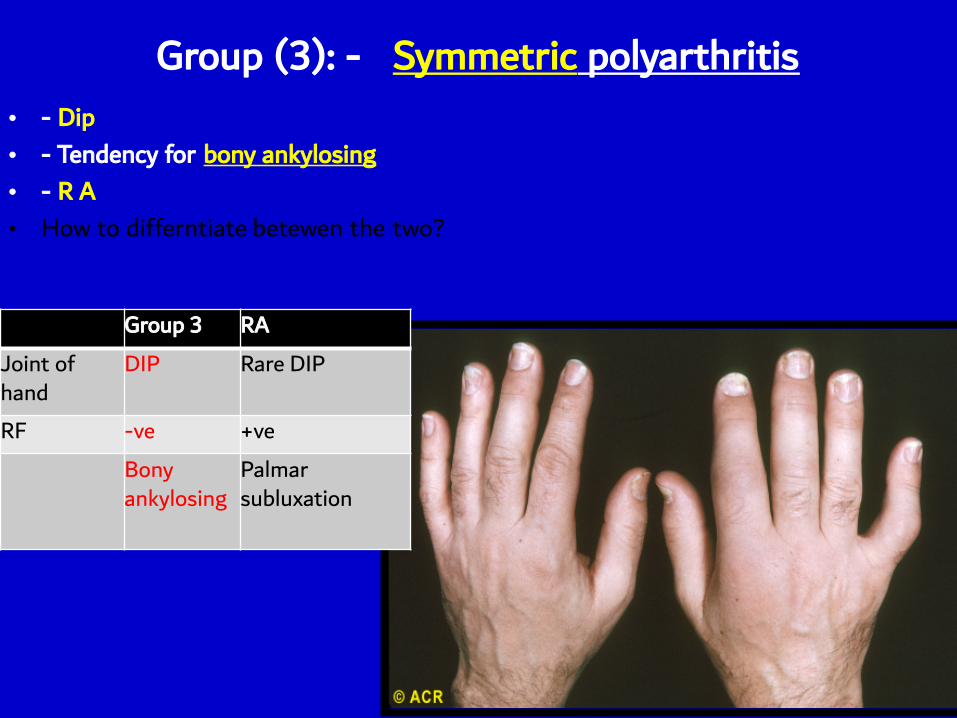
Group (3): - Symmetric polyarthritis• - Dip• - Tendency for bony ankylosing• - R A• How to differntiate betewen the two?
Group 3 RA
Joint ofhand
DIP Rare DIP
RF -ve +veBonyankylosing
Palmarsubluxation

Group (4): -Oligoarticular Arthritis
• - Asymmetric• - D I P -P I P-M C P –M I P –knee
– The most common is? Knee• 15-30%• Oligo-articular: no. of joints invovled <= 4

Knees are not symmetrical.Left knee? SwellingNormal right knee

- Identify? Dactylitis.- Most commonly caused by? Spondylitis
Psoriatic arthritis: ”sausage" digits and rashPsoriasis involving the first, third, and fourth toes is accompanied by psoriatic arthritis ofinterphalangeal joints of the third and fourth toes. The "sausage shape" of these toes is causedby soft-tissue swelling more marked than that usually seen in rheumatoid arthritis.

Group (5): Axial Involvement
• It is similar to RA.

Extra-articular manifestion ofpsoriatic arthritis
•* Eye: - conjunctivitis• - episclecitis
• - iritis•* Mitral prolapse – Aortic incompetence
•

Psoriatic arthritis: progressivejoint changes (radiographs)


Enteropathic Arthritis I B D
• peripheral arthritis• axial involvement• Flare up of IBD causes flare up of… but not of…
– Peripheral joints not axial joints– Therefore, some suggests that axial involvement
is a separate disease and should not beconsidered as part of IBD
Peripheral arthritis
• - 17-20%• Age 25-44
•Clinical: - pauci articular• - Asymmetric
• - Mono arthritis• - Migratory and transient
• - parallels the activity of bowelinvolvement .

Axial
•5-12%•M : F 3:1
•B 27: 33-70%

Extra-articular of SpA with IBD
• erythema nodosum• pyoderma gangrenosum• anterior uveitis• In late stage: amyloidosis

Therapy
•- NSAID'S•- Corticoidsteroid's
•- Sulphasalazine•- Anti TNF

Reactive arthritis
•Is a sterile synovitis which occurs following aninfection

Aetiology• salmonella , shigella, yersina enterocolitica
• N S U : chlamydia trachomatis• urea plasma urealyticum• bacterial antigen or bacterial DNA have been found in the
inflamed synovium of affected joint• Repeated infection donot necessarilly produce reactive
arthritis
• Etiology: Post venereal + Post-dysenteric

Clinical features•*arthritis –acute , lowerlimb , asymmetrical
•*enthesitis – plantar fascitis or achills tendonitis•Sacroilities or spondylitis *
-bilateral conjunctivitis 30%
•-circinate balanitis : painless superficial ulceration of theglan`s penis. heal without scarring
•-keratoderma blenorrhagica :skin of feet and hand's painlesred and raised plaques and pustules
•-Acute anterior uveitis


Reactive arthritis: balanitiscircinata

Reactive arthritis: conjunctivitis

Ankylosing spondylitis: earlysacroiliitis (radiograph)

Treatment
•-antibiotic (cultures should be taken and anyinfection treated )
•-NSAIDs•-local injection
•-sulfasalazin or MTX•-Anti TNF

Fig 163-1 Asymmetrical sacroiliitis in a patient with inflammatory bowel disease

![Ankylosing spondylitis and related conditions - NHS Wales1].pdf · Condition Ankylosing spondylitis Ankylosing spondylitis and related conditions This booklet provides information](https://img.pdfslide.us/doc/110x75/5d53eb2788c993a4728b841d/ankylosing-spondylitis-and-related-conditions-nhs-1pdf-condition-ankylosing.jpg)