Embed Size (px)
Citation preview

Splenectomy in Hairy Cell Leukemia:
A Retrospective Mu it icen te r An a I ysis
JAN JANSEN, MD,*.t AND JO HERMANS, PHD,$ FOR THE COLLABORATIVE STUDY GROUPS
To study the effect of splenectomy in hairy cell leukemia, we initiated a retrospective multicenter analysis. A series of 391 patients, contributed by 22 centers (median: 15 cases per center, range 2-130), was analyzed. Since comparison of the data from these centers showed few significant differences, the data were pooled. Factors that proved to have prognostic value at the time of diagnosis were the hemo- globin level and the neutrophil and platelet counts. Survival after diagnosis was significantly longer in the splenectomy group (n = 225) than in the nonsplenectomy group (n = 166) (P < 0.0001). When sub- groups were analyzed, no difference in survival time was found between splenectomized and non- splenectornized patients having an age > 60 years, symptoms > 12 months, spleens < 4 cm under costal margin, hemoglobin levels > 12 g/dl, neutrophils > 500/mm3, or platelets > l00,000/mm:'. After the operation, the platelet count usually increased to acceptable values, whereas the neutrophil count in- creased less often. Patients with Hb > 11 g/dl, neutrophils > 1,000/mm:', and platelets > 100,000/mm" aftersplenectomy, survived longer than patients with a less complete response to the operation (P < 0.01). In patients with definite splenomegaly and pancytopenia, splenectomy seems to be beneficial. However, in patients without distinctly enlarged spleens, other therapeutical modalities should be considered.
Cancer 47:2066-2076, 1981.
A I R Y C E L L L E U K E M I A (HCL, leukemic reticulo- H endotheliosis) is an uncommon type of leukemia. Its reported frequency is 2-57? of all leukemias,".' which means that its incidence must be about 2-5/10"/ year. The clinical and pathologic aspects of this disease have been studied extensively, particularly in recent
Although the origin of the malignant cell of HCL has not yet been completely elucidated, most investigators believe the hairy cell (HC) to be a B-lymphocytic cell.9,33 This origin would locate HCL in the group of lymphoproliferative disorders, perhaps near chronic lymphocytic leukemia and prolymphocytic leukemia.
years .B,11.19,20,31.33
The therapy of choice in HCL is claimed to be quite different from that in other lymphoproliferative disorders. Chemotherapy in particular has often caused severe pancytopenias and until recently was considered contraindicated in HCL. Some recent case reports however, have documented a favorable response to aggressive chemotherapy,10,32 and two groups have observed beneficial effects of low-dose alkylating agents in patients with progressive disease after splenectomy.O.Ls However, the therapy of choice in most centers is splenectomy. In the majority of cases, the peripheral blood counts have shown a favorable response, and many patients have survived for years
From the "J. A . Cohen Institute for Radiopathology and Radia- tion Protection and Departments of t Hematology and $Medical Statistics, Leiden University Medical Center. Leiden. The Netherlands.
Address for reprints: Jan Jansen, MD, Isolation Ward. Building 16, Leiden University Medical Center, 2333 AA Leiden-The Net herlands.
$University of Iowa (C. P. Burns, MD, Iowa City), University of Massachusetts ( I . Katayama. MD, Worcester: H . E. Finkel, MD. Boston), University of Minnesota (R. F. Branda, MD, Minneapolis), University of Utah (A. Turner MD and C. R. Kjeldsherg, MD, Salt Lake City), Stanford University (J. S. Burke, MD, Stanford), A. Maxwell Evans Clinic, Vancouver Canada (1. H. Plenderleith, MD), Universities of Olomouc and Hradec Kralove. Czechoslovakia (B. Wiedermann, MD, I.. Chrobak, MD, R. Kodousek, MD, and K. Indrak, MD) Coventry Hospital, Coventry. England (N. K. Shinton. MD), Hammersmith Hospital,
London, England (D. Catovsky MD), HBpital St. Louis, Paris, France (G. Flandrin, MD), HBpital Edouard-Herriot, Lyon, France (D. Espinousse, MD. and P. A. Bryon, MD), Hbpital St. Antoine, Paris, France (G. Duhamel, MD), HBtel-Dieu, Paris, France IC. M. Blanc, MD, and Chr Dao, MD), Institut-d'Hematologie, Montpellier, France (P . Izarn, MD, J. M. Emberger, MD, and M . Navarro, MD), Moabit Hospital, Berlin FRG (S. Mende, MD). St. Georg Hospital, Hamburg FRG (J. Diillmann, MD, and K . Hausmann, MD), Universitit Tubingen FRG ( H . W. von Heyden, MD, and H. D. Waller. MD), Universita Ferrara. Italy ( G . L. Castoldi, MD), Meir General Hospital, Kfar-Saha, Israel (A. Gutman. MD), Universiteit Leiden. The Netherlands (J. Jansen, MD, J . Hermans. PhD, and J. t e Velde. MD), Det Norske Radiumhospitalet, Oslo. Norway (R. Langholm, MD), Uni- versitatsspital, Zurich, Switzerland ( K . Rhyner, MD, and J . Fehr, MD).
Accepted for publication April 29. 1980.
0008-S43X/81/0415/2066 $1.10 American Cancer Society
2066

No. 8 SP~ENECTOMY IN HAIRY CELI. LEUKEMIA . JUIZSC.~ crtid H ~ w z r r r z s 2067
after the operation, often without any additional ther- apy. On the other hand, some patients did not respond to the operation or showed only very transient re- sponses and died within a few months. Furthermore, splenectomy may have serious complications in patients with large spleens and severe cytopenia. In fact, the beneficial effect of splenectomy is primarily anecdotal. All studies performed were retrospective. and usually no checks could be made to be sure that the splenectomy and nonsplenectomy groups were comparable for factors with a possibly prognostic value. The decision to perform splenectomy had not been randomized in. any of these studies.
Another difficulty encountered in evaluating these studies is given by the reported survival time. Usually, the survival time after diagnosis or after the onset of symptoms is reported, but when splenectomy was not performed immediately after diagnosis, the survival time between diagnosis and the operation is generally added to the survival time after the operation. Jansen et t i / . I!’ described a retrospective study covering cases in the literature and from their own center. By applying criteria to obtain more or less comparable groups, they collected 24 splenectomy and 51 nonsplenectomy patients. Survival was longer for the splenectomy group, but the difference was not statistically signifi- cant at two years after diagnosis. For some subgroups, however, the operation seemed to be of definite bene- fit. Sebahoun or a/.:” and Golomb et a / . 1 4 , who studied large series of patients, reported a better survival for the splenectomy group, although this was not statis- tically significant. It remains questionable, however, whether the splenectomy and nonsplenectomy groups were comparable.
A prospective randomized trial would be the most desirable way to study the effect of splenectomy in HCL but seems difficult to perform. Not only do most centers see few cases of HCL but also the grave clinical condition of some of the patients and the claimed benefit of the operation virtually exclude a ”wait and see” alternative. Therefore, we performed a retrospective multicenter analysis of the effect of splenectomy. Special attention was paid to ensuring the comparability of the various centers and of the splenectomy and nonsplenectomy groups.
Materials and Methods
All centers known to be particularly interested in HCL, as shown by papers in the literature, were invited to participate in this study. The total number came to 42, of which 32 responded and 22 actually contributed patient data (Appendix 1). The intake of data took place from February 1977 to April 1979 and
included 456 patients. The number of patients per center ranged from 2-130 (median: 15). Six cases were omitted because of insufficient data. The remain- ing 450 patients were analyzed.
In this part of the collaborative study, no histologic proof of the diagnosis of hairy-cell leukemia was re- quired. Although in most patients histologic examina- tion of a bone marrow biopsy or of the splenectorny specimen would have been performed, at this stage of the study the slides had not been reviewed by the pathology panel. However, the particular interest in hairy-cell leukemia of all the participating centers suggests that the diagnosis had been established with an acceptable degree of reliability.
The questionnaire covered clinical and laboratory findings at the time of diagnosis, and for splenectomy cases before and two to three months after the opera- tion (Appendix 2). Survival was to be reported from the time of diagnosis. Finally. there were questions on the cause of death and on details of additional therapy. Statistical analysis included comparison of the splenectomy and nonsplenectomy groups by the chi- square test and Student’s t test (after transformation to obtain normal distribution). The different centers were compared by cross-tables, scattergrams. chi- square tests, and analyses of variance with multiple- comparison analyses according to Scheffe.’ Survival analyses were performed with the log rank test.”
For most of the analyses, a P value of 0.05 was considered significant, but in the log rank analyses, ;t
P value of 0.01 was used, the latter because of the size of the series and the large numbers of comparisons of survival curves.
Results
Cliiiicrrl Ferit1rrP.s t i t Di~ig.no.vis
Of the 450 patients, 59 were omitted for the fol- lowing reasons: of those diagnosed before 1965, many were long-term survivors who had been diagnosed retrospectively. To avoid the bias these long-term survivors would introduce, we excluded all patients diagnosed before 1965 ( n = 32). Second, surviving pa- tients diagnosed during the preceding six months were also omitted, because the time might have been too short for planning treatment strategy (n = 27). Since comparison of the excluded ( n = 59) and “restricted” (n = 391) groups showed no significant differences, analysis of the “restricted” group was considered acceptable. The clinical findings in the 391 patients are listed in Table I , the laboratory data in Table 2. A male preponderance of 3.4:1 was present. Liver enlargement was seldom prominent: only 2% of the patients had severe hepatomegaly ( > l o cm under the

2068 CANCER April 15 1981 Vol. 47
TARI E 1 . Clinical Findings at Diagnosis of 391 Patients with HCL
Q Patients Median Range
Age (years) 52 22-89 Duration of symptoms before
Lymphadenopathy 18.8%
~ : 4 cm (ucm) 13.6% 4-10 c m (ucm) 49.1% '.,I0 cm (ucm) 18.9%
diagnosis ( in months) 0-98
Spleen not palpable 18.4% 5.2 0-28
t,iver not palpable 50.49 0.S 0-23 1-2 cm (ucm) 15.7%' 3-4 cm (ucm) 14.8%' >4 cm (iicm) 19.1%
ucm under costal margin. Ma1e:female = 3.4:l.
TABLE 2. Laboratory Data at Diagnosis of 391 Patients with HCL
c/n Patients Median Range
Hemoglobin (ddl) 10.1 18.S 34.6% 8.5-12.0 45.9';; '12.0 1 9 . m
--'4,000 62.S% 4- 10.000 23.8% :> 10,000 13.7"r
<so0 38.SV 500- 1,000 29.1% ,' I ,000 32.4%
,:so0 50.3% 500-5,000 32.1% >5.000 17.6%
-:50.000 30.2% 50- 100.000 48.9% > 100.000 20.94
I.eukocytes (imm.') 3000
Neutrophils (imm:') 640
Hairy cells ( /mmR) 480
Platelets ( imm' ) 65.100
2.5- 16.4
500-?01.000
0-24.120
0- 150.750
10,000- 998,000
right costal margin). Splenomegaly was present in 82% of the patients: in 19% it was massive (>I0 cm under costal margin). Pancytopenia was the most frequent sign, 37% of the patients having Hb < 1 1 g/dl, platelets < 100,OOO/mm:l, and neutrophils < 1,00O/mm:'. Leuko- cytosis was observed in only 14% of the patients, and leukocyte counts higher than S0,000/mm" were extremely rare (1%). The median survival of the pa- tients was 48 months: 19% died within one year after diagnosis, and 39% survived for more than eight years. The most frequent causes of death were sepsis (469%) and pneumonia (19%)).
co n7p ( I r is0 I1 of' cc I1 t e
The comparability of the data of the 22 centers was evaluated for the various factors at diagnosis on the basis of cross-tables and scattergrams. The percentage of splenectomized patients ranged from 0 (0/11) to 100 ( 1 5 / l S ) , but the factors at diagnosis did not show many differences.
Subsequently. a more refined analysis (analysis of variance) was performed only for the IS centers con- tributing more than ten patients (Table 3). Significant differences were present for the hemoglobin level ( P =: O . O l ) , number of hairy cells ( P < 0.01), degree of splenomegaly ( P = 0.021, and degree of hepato- megaly ( P < 0.001). However, when multiple compari- son analyses according to Scheffe were performed, no two groups turned out to differ significantly at the P = 0.05 level for any factor except the degree of hepatomegaly. For this factor the data of one center, which had diagnosed hepatomegaly frequently, dif- fered from those of the four centers, which had seldom diagnosed hepatomegaly. The nine centers that had
TARLF. 3. Comparison of the 15 Centers Contributing more than Ten Patients for the Various Factors at Diagnosis (Analyses of Variance). Only the Mean Values are Given
Center Center Center Center Center Center Center Center Center Center Center Center Center Center Center 1 2 3 4 5 6 7 Y in I 1 I? I1 Ih ? I ) 2 2 P w/, ,c
Month, of \ymptom\
Age lyearc) H h (pidl1 I.eukocyle\
1 % IWmin') Neutrophil\
( x IO'lmm'l Hairy cells
1 I 10'/mm.ll Platelets I IO'imm?
Spleen \i7e (cm ucml
1.1ver size Icm ucml
Numhrr of patient<
? Y 11.4 9.2 2 0 7 6.7 11.9 119 4.5 I?.O 6.8 4.6 i? 15.7 2 O h IX.5 n . r . ( 5 52 58 53 5 2 5 5 50 51 53 49 62 5? 5 1 $ 2 5 2 n.\. 1 2 I 9.2 10.6 12.1 i n 6 9 .1 9.7 9.y 10.1 10.8 Y.? Y 1 9.2 IO I 1o.6 n.ni
2 1 2 6 .1 in.9 4.2 4 . ~ 4 . 1 5 . 2 9.9 4.6 6.9 3 .7 4 6 4.0 4 n 4.0 n 5:
14 Y I 1.5 2 3 . 2 7.9 7.4 7 6.1 n.n 9.5 12.5 h l 6.5 7.6 R.8 6.5 n.s.*
I 3 3 7.2 6 1 I 9 I . ? 6 I 2.8 3.3 2.0 6.1 1 . 6 3 2.2 n Y 1.8 ,.n.ni*
99 70 129 65 h4 71 93 h? 7 1 Y4 70 7h 5 5 8' 66 n 5 . -
6 6 n.n 6 9 4 h 7.5 9 .5 X . ? 6.4 5 . 1 6.0 3.6 7 Y Y 5 5 Y 9.5 n . w
1 9 1 . 1 1.5 I.? O ? 3.6 3.x 3 1 1.4 0 7 1.9 1.6 2 6 0 . 5 2.7 n . n w
17 29 17 I1 I 5 10 4x I 5 Ill 13 17 15 ?I I S - I1
After noiinltlizing rran\form.ition. ucm ~ under co\tltl margin. n . 5 ~ not rignificnnl 0' ' 0.051

No. 8 SPLENECTOMY I N HAIRY CELL LEUKEMIA . Jrinsrn rind Hermnns 2069
contributed approximately equal numbers of splenec- tomy and nonsplenectomy patients were analyzed for differences between these two groups at diagnosis.
Significant differences were found in four of the nine centers: for the splenectomy group, two centers had reported patients with larger spleens, one center had patients with larger spleens and lower platelet counts, and one center had patients with only lower platelet counts. The hemoglobin level, leukocyte, hairy-cell, and neutrophil counts did not differ significantly in any of the nine centers. When the data of the non- splenectomy group at diagnosis were compared with those of the splenectomy group before the operation, differences were again found in four centers. Besides spleen size and platelet count, one center now also showed significantly lower neutrophil counts in the splenectomy group. In our view, the results of this analysis gave no serious objections to pooling the data of the 22 centers.
P w g t i os tic. Fri c t or.\
Table 4 shows the prognostic value of the various factors at diagnosis. The only factors significantly correlated with survival were the hemoglobin level (Fig. I ) , the platelet count, and less strongly, the neutrophil count. The prognostic relevance of these factors was supported by the presence of a significant trend toward better survival with increasing blood cell counts. The degree of splenomegaly and the number of peripheral hairy cells had no significant prognostic value. When only nonsplenectomized patients were taken into consideration, patients without palpable spleens did significantly better ( P < 0.01).
Splellcc~tol?ly
Of the group of 391 patients, 225 underwent splenectomy. The comparability of the splenectomy
TABLE 4. Prognostic Value of the Various Factors at Diagnosis in Relation to Survival Time after Diagnosis. Tested
with the Log-Rank Test (391 Patients)
Median survival (mo.) P value
Sex male female
<45 years 45-60 >60
0 1-3 4- 12 >12
0 1-3 4- 10 > 10
no Yes
c8.5 8.5-12.0 > 12.0
14000 4- 10,000 > 10,000
< 500 500- 1000 > 1000
<500 500- 5000 > 5000
Platelets (imrn') <50,000 50- 100.000 =. 100.000
Age
Duration of symptoms (months)
Splenomegaly (cm ucm)*
Lymphadenopathy
Hemoglobin (gldl)
Leukocytes (imm
Neutrophils (imm')
Hairy cells (immJ)
ucm = under costal margin.
45 0.18 97
48 0.25 50 44
44 0.96 97 52 60
98 0.07 30 50 44
50 0.38 39
26 < 0.000 1 76 89
48 0.36 35 44
36 0.009 50
109+
65 0.06 36 44
27 <0.0001 76 89
3 " " L
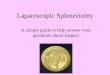
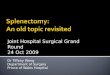
FIG. 1. Actuarial-survival curves of 384 patients 60
12LI J-
with hairy-cell leukemia according to the hemo- glohin level at the time of diagnosis. The numbers on the curves refer to patients still being followed. Patients with higher Hb levels had a significantly longer survival time ( P i 0.0001).
5 $
L- ~
0 1 I 1171 "' 4 HbDl2.O g / d i ( # 7 5 ) 0 : 8 5 c H b 6 1 2 0 g/d l I# 176)
: H b C 8 . 5 g / d i I# 1 3 3 )

2070 CANCER April 1.5 1981 Vol. 41
TABLE 5. Values of Various Factors in the Splenectorny and Nonsplenectomy Groups
Non- Splenectomy splenectomy
(n = 225) (n = 166)
mean S D mean SD P value
Age (years) Spleen (cm ucrn) Liver (cm ucm) Duration of
symptoms (months)
Hemoglobin (gidl)
Leukocytes ( x IO’irnrn:’)
Neutrophils ( x IO’irnm’)
Hairy cells ( K 10’imm’)
Platelets ( x IO’imm:’)
49.7 10.4 56.7 12.5 <O.OOI 1.8 5.6 5.1 5.8 <O.OOI* 1.8 2.4 2.2 3.3 n.s.*
9.9 15.6 13.8 19.6 n.s.*
10.2 2.5 10.0 2.1 n.s.
6.8 15.6 5.2 7.6 n.s.*
9.5 12.1 9.6 9.8 n.s.*
35.6 94.1 27.0 69.7 n.s.*
15.9 19.6 82.4 54.9 n.s.*
ucm = under costal margin; n.s. = not significant ( P > 0.05). The equality of the two groups was tested with the chi-square test and Student’s t test. Percentage of males: splenectomy, 78%: non- splenectomy, 76%. Percentage of lymphadenopathy: splenectomy. 22%: nonsplenectorny. 14%.
* After normalizing transformation.
group and the nonsplenectomy group was tested by the chi-square test and Student’s t test (Table 5) . Only the age and the degree of splenomegaly at diagnosis differed ( P < 0.001). When the preoperative data of the splenectomy group were compared with the data at diagnosis in the nonsplenectomy group (Table 6), differences were found for the numbers of platelets and hairy cells ( P < 0.001 and P = 0.03, respectively) and the size of the spleen ( P < 0.001).
TAB[ F 6. Data of the Nonsplenectomy Group at Diagnosis and of the Splenectomy Group before the Operation
Non-
(n = 166) Splenectomy splenectomy
( n : 225)
mean S D mean SD P value
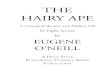
The splenectomy group had a significantly longer survival after diagnosis (Fig. 2: P < 0.0001). This dif- ference persisted when the survival of the splenectomy group was calculated from the operation onwards. Even with omission of the nonsplenectomized patients who died within four months after diagnosis (whose physical condition was possibly too poor for surgery), the postoperative survival of the splenectomy group was still better (Fig. 3: P < 0.01).
Analysis of subgroups (Table 7) showed that the beneficial effect of splenectomy was not influenced by the sex of the patient or by the leukocyte count. However, splenectomy did not lead to better results in patients with lymphadenopathy, Hb > 12.0 gidl, neutrophil counts > 5OO/mm”, hairy-cell counts < 500/ mrn:], platelet counts > 100,00O/mm”, or spleens < 4 cm under the costal margin. Furthermore, the operation did not appear beneficial in patients older than 60 years at diagnosis or in patients with a duration of the symptoms amounting to more than 12 months before diagnosis. For all other subgroups, the survival of the splenectomy group was significantly better ( P < 0.01). If, however, survival was calculated from the date of operation for the splenectomy group, the benefit of the operation for patients with leukocyte counts < 4000/mm3 or Hb > 8.5 g/dl lost its significance. In the subgroup with spleens < 4 cm under the costal margin, the influence of the Hb level, neutrophil count, and hairy-cell counts, was no longer apparent, but patients with platelet counts < 50,00O/mm:’ survived longer after splenectomy.
The effect of splenectomy on the peripheral blood counts was studied. Table 8 shows the Hb level and the neutrophil and platelet counts before and two to three months after the operation.
Almost normal levels were reached the most fre- quently by the platelet count (159/202 = 79%), the least frequently by the neutrophil count ( 1 13/197
57%). A complete response (according to Catovsky!’ with Hb > 1 I .O g/dl, neutrophils > 1,00O/mm:’, and platelets > 100,000/mm~3) was attained postoperatively by 40% of the patients (Table 9).
Spleen (cm ucm) 9.2 5.7 5.1 5.8 <0.001* Hemoglobin
(gidl) 10.0 2.4 10.0 2.1 n.s. Leukocytes
( x 1O”irnm~”) 5.7 6.1 5.2 7.6 n.s. Neutrophils
( x 10”imm’) 8.2 7.9 9.6 9.8 n.8. Hairy cells
( Y IO’imm,’’) 32.6 54.5 27.0 69.1 0.03* Platelets
( x IO’imm:’) 61.6 37.4 82.4 54.9 <0.001*
ticm = under costal margin; n.s. = not significant. -& After normalizing transformation.
Discussion
According to the present results, splenectomy is a beneficial form of therapy. When survival was cal- culated from the time of diagnosis, the splenectomy group did far better than the nonsplenectomy group (Fig. 2). Even when the splenectomy group was af- fected adversely by calculation of the survival from the date of the operation and the nonsplenectomy group was favored by the omission of patients who died within four months after diagnosis (on the grounds that

No. 8 SPLENECTOMY I N HAIRY CELL LEUKEMIA . Jansen and Hennans 207 1
the clinical condition of these patients might have prevented splenectomy), the survival of the splenec- tomy group was still longer than that of the non- splenectomized patients (Fig. 3). Since the decision to perform splenectomy was certainly not taken according to a well-designed randomized clinical trial, great care had to be taken to avoid a systematic bias in favor of the splenectomy group. For prognostic factors, the two groups did not differ significantly for the factors with prognostic value, i . e . , the Hb level and the neutrophil and platelet counts but did differ as to age and spleen size. The splenectomy patients were younger and had larger spleens. Although the patient’s age proved to lack prognostic value, the younger age of the splenec- tomy group may nevertheless have resulted in a bias in favor of this group. On the other hand, the non- splenectomy group had more patients whose spleen was not palpable, and this probably gave an advantage to this group.
In sum, we could not find a systematic bias in favor of the splenectomy group, and this makes a true beneficial effect of the operation highly probable. Other studies’ t,19m showed somewhat longer survival times for the splenectomized patients, but the dif- ferences were not statistically significant, although Sebahoun et Lil.:” found a P value of <0.05 at a single point after diagnosis. The larger number of patients in the present study, which included all of the patients reported by Sebahoun et uI.X1 and some of those re- ported by Golomb r t d . 1 4 and Jansen rt was probably responsible for the significance of the dif- ferences in survival we found between the splenectomy and the nonsplenectomy groups.
The analysis of subgroups indicated that particularly the patients with large spleens should undergo splenec- tomy; in the patients with smaller spleens (<4 cm ucm), the operation was not significantly beneficial. Even the splenectomized patients with low Hb or neutrophil levels, whose spleens had been <4 cm under the costal margin, did not do better than their nonsplenectomized counterparts. Therefore, the practice of some groups to splenectomize all patients with HCL, regardless of the size of the spleen, is not supported by this study.
In the present study, there was no advantage in survival for patients who were splenectomized in the absence of severe neutropenia, anemia, or thrombo- cytopenia. Therefore, this study does not support the finding of Jansen et that patients without severe cytopenia benefited the most from the operation. This divergence might be explained by the fact that the study of Jansen et al.I9 included many cases that were diag- nosed in the early days after the recognition of HCL as an entity,1.’2.2X when the diagnosis was usually
z 4 0 1 , , , (l; , ( I ) l r ”’ , ‘i’ 2 0
non - SX
6 12 18 2L 30 36 L I 48 5 L 60 66 72 78 81 90 96
Months
FIG. 2. Survival curves, calculated from the time of diagnosis, of 225 splenectomized (Sx) and 166 nonsplenectomized (non-Sx) patients with hairy-cell leukemia. The Sx group did significantly better ( P < 0.0001).
established in a later stage of the disease, as suggested by the shorter median survival and the preponderance of huge spleens (40%). Furthermore, the application of criteria to obtain comparable splenectomy and non- splenectomy groups meant that they omitted the pa- tients who died within four months after diagnosis. Perhaps, therefore, the survival of the nonsplenectomy group was estimated too optimistically. Finally, the numbers of splenectomized patients in the subgroups were very small.
The aim of splenectomy is primarily to remove splenic sequestration of normal peripheral blood cells and thus to alleviate pancytopenia. The removal of the huge tumor load is only a secondary aim. Pancyto- penia can, however, also be caused by bone marrow insufficiency due to infiltration of hairy cells. In pa- tients with pancytopenia primarily due to bone marrow insufficiency, splenectomy would certainly be less beneficial than in pancytopenia due to splenic sequestration. Therefore, it is crucial to know which
100
8 0 m
.? 60 C ._
L 3 Cn
4 0 -$
sx
non-SX 2 0 -
I I I I I I I I I , , ,
6 12 18 24 30 36 L 2 L8 5L 60 66 72
Months
FIG. 3. Survival curves of 225 splenectomized patients (Sx) , calculated from the date of splenectomy, and of 143 nonsplenec- tomized patients (non-Sx), calculated from the time of diagnosis. For the non-Sx group, those patients who died within four months after diagnosis have been omitted. The Sx group still shows sig- nificantly longer survival ( P < 0.01).

2072 CANCER April 15 1981 VOl. 47
TABLE 7. Survival Time after Diagnosis in the Splenectomy and the Nonsplenectomy Groups according to Several Subgroups (Log Rank Test)
Median survival months
No. No. SxINo. non-Sx Sxlnon-Sx P value
Total group Sex
males females
Age (years) <45 45-60 > 60
0 1-3 4- 12 >I2
0 1-3 4- 10 > 10
no
Duration of symptoms (months)
Splenomegaly (cu ucm)
Lymphadenopathy
yes Hemoglobin (gidl)
C8.5 8.5- 12.0 >12.0
14000 4- 10,000 > 10,000
<500 500- 1000 > 1000
<500 500-5000
Leukocytes (imrn’)
Neutrophils (lmm’)
Hairy cells (lmm’)
>5000 Platelets (imm’)
<50,000 50- 100,000 > 100.000
391
302 88
96 198 97
42 97
132 85
70 52
I87 82
315 73
133 176 75
24 1 92 53
145 110 I22
180 1 I5 63
1 I4 185 79
ucm = under costal margin; Sx = splenectomy: non-Sx = non- splenectomy; * Significance disappeared when survival of the
factor is primarily responsible for the pancytopenia in HCL.
Castro-Malaspina et ul. found hypoproduction of erythrocytes in half of their patients by ferrokinetics. The rate of erythrocyte production had prognostic value, since patients with subnormal production all died within a year, with or without splenectomy. When erythrocyte production was increased, splenec- tomized patients seemed to do better. Schafer et ~ l . ” ~ did not find splenic sequestration in three of their four patients and saw only mild sequenstration of erythro- cytes in the fourth patient. Lewis et ~ 1 . ~ : ’ found exten- sive splenic erythrocyte pooling in HCL, even more
(2251 166) 8912 1 <0.0001
(1761126) (49139)
(67129) ( 126172) (32165)
(18124) (72125) (78154) (40145)
(17153) (33119)
( 1 11/76) (64118)
(1721143) (50123)
(69164) ( I 1 1165) (40135)
(1361105) (47145) (37116)
(85160) (60150) (70152)
(94186) (6015 5 ) (44119)
89120 <0.0001 94il22 0.0009
89122 0.0004 7612 I <0.0001 601 I7 0.02
5712 1 0.03 87+112 <o. 000 1 98+121 <0.0001
60176 0.40
59+198 0.40 34116 0.04 89/19 <0.0001
<0.0001
108+/20 <o. 000 1 65122 0.05
39113 <0.0001 98+144 0.002*
89152 0.05
65137 0.003% 79+117 0.0001 69+116 1 0 ,000 1
84+115
761 18 < 0.000 1 57150 0.08
98+144 0.02
65176 0.11 <0.0001 601 18
89/ 16 < 0.000 1
(65149) 41/12 <o.ooo 1 ( I 18/67) 98+121 0.0002
(33146) 89175 0.02
splenectomy group was calculated from the date of the operation.
marked then in myeloproliferative disorders. The rela- tionship between the severity of anemia and the degree of splenic erythrocyte pooling was not close, but after splenectomy most of the patients showed an improve- ment in the hemoglobin level that was fairly well correlated with the erythrocyte volume of the spleen. This suggests that marrow failure was not the primary cause of anemia in their patients. The excellent re- covery of the platelet counts in many patients after splenectomy suggests that the spleen is the primary cause of thrombocytopenia in HCL, too.X.”26 In the patients whose platelet counts did not increase after the operation, bone marrow failure probably played a more

No. 8 SPLENECTOMY IN HAIRY CELL LEUKEMIA . Jarzsen ~ r n d Herl?ltrns 2073
important role. Yam P t ( i / . ’ j . ; believe that bone marrow failure is the most important cause of pancytopenia in HCL, because they observed an impaired granulo- cyte reserve even after splenectomy.
In the present study too, the neutrophil count at- tained acceptable levels (57%’ > l,OOO/mm:i) the least frequently. The platelet count was the factor that showed an increase most often after the operation (79% 1 100,00O/mm~’~. Conceivably, thrombocyto- penia is primarily caused by splenic sequestration, neutropenia by bone marrow failure, and anemia by a mixture of splenic pooling and erythrocyte hypopro- duction. Catovsky!’ reported a positive response to splenectomy in 90% of his patients. In 60% the re- sponse was “complete,” i.6.. , after the operation the Hb level was > 1 I .O g/dl, and the neutrophil and platelet counts were 1 1,000/mm:3 and ~100,00O/mm:’, re- spectively. Using the same criteria. Jansen c t (i/.l9
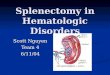
also saw a 60% “complete response” rate. In the study of Mintz and Golomb”i and in the present study, however, the “complete response” rate was only 40%. The patients who showed a “complete response” had a significantly longer survival time than the patients with only a partial response or the small group of patients (3%’) with severe pancytopenia after the opera- tion (Fig. 4).
Our findings suggest that patients with severe pancytopenia and large spleens should be splenec- tomized. There seems to be no obvious indication for splenectomy in patients with small spleens. Perhaps if it could be demonstrated that a small spleen showed extensive sequestration. an indication would be present. In this respect, ferrokinetic studies or platelet- survival studies could give important information.
FIG. 4. Survival curves (calculated from the date of the operation) of 81 splenectornized patients who had almost normal blood counts after the operation (CR; Hb > 11.0 gidl, neutrophils > lOOO/ mm’, and platelets > 100,00O/mm’), six patients who were severely pancytopenic after the opera- tion (Hb < 8.5 gidl, neutrophils < 500/rnm’, and platelets .-c SO.OOO/rnm~’O, and 118 patients not belonging to either of the former two groups (PR). The CR group had significantly longer sur- vival time ( P < 0.01).
100
TABLE 8. Influence of Splenectomy on Hemoglobin Level and Neutrophil and Platelet Counts
Post-Sx
Hb (gidl) C8.5 8.5- I I > I 1.0 Total
pre-Sx i 8 . 5 10 18 28 56 8.5- 11.0 4 29 52 85 ’11.0 3 5 57 65
Total 17 52 I37 206
Post-Sx Neutrophils
(imrn:’) 500-1000 >I000 Total
pre-Sx ‘:so0 17 26 35 78 500- 1000 8 20 37 65 > 1000 7 6 41 54
Total 32 52 113 197
Post-Sx
Platelets (irnm’) <50.000 S O - 100,000 > 100,000 Total
pre-Sx ‘: 50,000 9 18 60 87 SO- 100,000 5 9 80 94 >100,000 2 0 19 21
Total 16 27 I59 202
Furthermore, since splenectomy often results in considerable increases in platelet and neutrophil counts even in patients with only small spleens, postopera- tive cytotoxic therapy may become feasible. The pos- sible benefit of the operation should, however, be weighed against the risk, including an early postopera- tive mortality (in our study amounting to about 2%).
20 -
I I21
0 - C R ( # E l )
: pancytopenic ( # 6 ) 0 : PR ( # i i e )
-I-- I
18 2 L 30 36 L 2 La 51 6 0 66 6 12
Months

2074 CANCER April 15 1981 V O l . 47
TABLE 9. Influence of Splenectomy on the Number of Cell Lines that Attained Almost Normal Values (Hb > 11.0 gidl, Neutrophils > l.OOO/mm:J and Platelets 1 100,OOO/mm~l).* Number of Patients
with All Data Available: 192)
Post - s x Number of cell
lines under limit 3 2 I 0 Total
pre-Sx 3 10 16 28 36 90 2 5 I5 28 18 66 I 1 2 7 23 33 0 0 0 I 2 3
Total 16 33 64 79 192
I n this table only the upper limit of Table 8 is taken into consideration.
In the severely pancytopenic patients with small spleens, other therapeutic modalities, such as androgen
aetiocholanolone,' or cytotoxic ther- spy" l( l . l5.:i2 should be considered.
REFERENCES
I . Armitage P. Statistical Methods in Medical Research. Oxford: Blackwell Scientific Publications, 1971: Chapters 4, 7.
2. Besa EC, Dale DC, Wolff SM, Gardner FH. Aetiocholanolone and prednisolone therapy in patients with severe bone-marrow failure. Ltrncet 1977: 1:728-730.
3. Bezwoda WR, Derman DP, Bothwell TH, e t tr l. The diagnosis and management of hairy-cell leukaemia. S Afr Med J 1979; 55:
4. Bouroncle BA, Wiseman BK, Doan CA, Leukemic reticulo- endotheliosis. Blood 1958: 13:609-30.
5 . Branda RF. Leukemic reticuloendotheliosis and 'hairy-cells'. N Engl J M r d 1976: 295:lOlS. 6. Burke JS. The value of the bone-marrow biopsy in the diagnosis
of hairy cell leukemia. Am J Chi Ptitliol 1978: 70376-884. 7. Burns CP. Serum-murarnidase in leukaemic reticuloendothelio-
sis. Lnncrr 1974; 2:964. 8. Castro-Malaspina H, Najean Y , Flandrin G. Erythrokinetic
studies in hairy-cell leukaemia. Br J Htrumctiol 1979; 42: 189- 197. 9. Catovsky D. Hairy-cell leukaemia and prolymphocytic
leukaemia. Clin Htrrnitriol 1977; 6:145-268. 10. Davis ThE. Waterbury L , Aheloff M . Burke PJ. Leukemic
reticuloendotheliosis. Repon of a case with prolonged remission following intensive chemotherapy. Arch I n t ~ r n M1.d 1976: 136: 620-622.
I I . Duhamel G. Lymphoid myelofibrosis. About 10 further ob- servations. Ac.tri Htiemtrtol 1971; 45:89-98.
12. Diillmann J . Wulfhekel U, Drescher S, Hausmann K. Die Haarzellenhimoblastose ('hairy-cell leukemia'). Dt.scli Me i l Wschr 1974; 99:859-963.
13. Emberger JM, Navarro M. Rizkalla N. Izarn P. Etude histologique et cytologique de la moelle osseuse et de la rate au cours de I'histiolymphocytose primitive medullaire et splenique. Norri. R e i , Fr d'Hhtntirol 1972: 13:365-375.
577-583.
14. Golomb HM. Catovsky D. Golde DW. Hairy cell leukemia. A clinical review based on 71 cases. Ann Intern M r d 1978; 89:
15. Golomb HM, Mintz U. Treatment of hairy cell leukemia (Leukemic reticuloendotheliosis) 11. Chlorambucil therapy in postsplenectomy patients with progressive disease. B l o o d 1979; 54:305-309. 16. Grusovin GD, Castoldi GL, Scapoli GL. Anzanel D.
Osservazioni citomorfologiche e funzionali in sei casi di 'hairy cell leukemia'. Hrreninrokrgicrr 1977: 62:23-48. 17. Gutman A, Tatarski A, Taragan R, e i d. Splenectomy for
hairy cell leukemia. Hrrrefrrrili 1976; 91:4- 12. 18. Von Heyden HW, Waller HD, Pape GR, e t NI. Haarzell-
Leukamie. I . Klinik, Zytochemie, Phagocytose-fahigkeit von Haarzellen, Etablierung permanent wachsender Zellinien. D t d i Mcd W.rc/w 1976; 101:3-8. 19. Jansen J , Hermans J . Remme J, den Ottolander GJ, Lopes
Cardozo P. Hairy-cell leukaemia. Clinical features and effect of splenectorny. Scrintf J Hrrenirrtol 1978; 21:60-71.
20. Katayama I , Finkel HE. Leukemic reticuloendotheliosis. A clinicopathologic study with review of the literature. A m J Med
21. Langholm R, Marton PF. Leukemisk retikuloendoteliose. Tid.sskrifr Den Norde LoegyfLwening 1976; 1416- 1420. 22. Lee SL, Rosner F. Rosenthal N, Rosenthal RL. Reticulum
cell leukemia. N Y Sttire J M d 1969; 69:422-29. 23. Lewis SM, Catovsky D, Hows JM, Ardalan B. Splenic
red-cell pooling in hairy-cell leukaemia. Br J Htrrmtirol 1977; 35: 351-357. 24. Lusch ChJ, Ramsey HE, Katayama I . Leukemic Reticulo-
endotheliosis. Report of a case with peripheral blood remission on androgen therapy. Cancer 1978; 41:1964- 1966. 25. Mende S , Fiille HH, Weissenfels 1. Diagnose und Dif-
ferential-diagnose der Haarzell-Leukamie. Bhir 1975: 30: 163- 174. 26. Mintz U, Golomb HM. Splenectomy as initial therapy in
twenty-six patients with leukemic reticuloendotheliosis (hairy cell leukemia). Cfincrr Res 1979; 39:2366-2370. 27. Peto R, Pike MC. Armitage P, at d. Design and analysis
of randomized clinical trials requiring prolonged observation of each patient. Br J C~rnc.er 1977; 35:l-39. 28. Plenderleith IH. Hairy cell leukemia. Crrn Mid A.WK J
1970; 102:1056- 1060. 29. Rhyner K, Streuli R, Kistler GS. Haarzell-leukkmie (hairy-
cell leukemia) mit osteolytischen Knochenveranderungen. Schiwi: Med Wsclrr 1977; 107:863-871. 30. Schafer AI, Rosenthal DS. Moloney WC. Hairy-cell
leukemia: diagnosis and management. A m J M e d Sci 1978; 275: 297-308.
31. Sebahoun G, Bouffette P, Flandrin G. Hairy cell leukemia. Lrrrk Res 1978; 2:187-195. 32. Stewart DJ, Benjamin RS. McCredie KB, Murphy S,
Keating M. The effectiveness of Rubidazone in hairy-cell leukemia (leukemic reticuloendotheliosis). Blood 1979; 54:298-303. 33. Turner A , Kjeldsberg CR. Hairy cell leukemia: a review.
Medicine 1978; 57: 477 - 499. 34. Wiedermann B, Chrohak L, Kodousek R, Indrak K ,
Kodouskova V. Contribution to the clinic and diagnosis of the so- called hairy cell leukemia (abstr) 17ih Congress of rlir hiterntitioncrl .Soc.irty of Henitriolo,qy, Paris, 1978. 35. Yam LT, Chaudhry AA, Janckila AJ. Impaired marrow
granulocyte reserve and leukocyte mobilization in leukemic reticulo- endotheliosis. Ann Intern Met1 1977: 85:444-446.
677-683.
1974: 57: I IS- 126.

No. 8 S P L E N E C T O M Y IN H A I R Y CELL L E U K E M I A . Jnnsc>n and Hc.r.rnrrn.s 2075
APPENDIX 1.
No. of No. of patients with Ref-
City Country patients splenectomies Investigator(s) erence
University of
University of Massa- chusetts
University of Minnesota
University of Utah
Stanford
Iowa
University
Evans Clinic A. Maxwell
University of Olomouc
Coventry Hospital
Hammersmith Hospital
Hopital St. Louis
Hopital Edouard- Herriot
Hopital St. Antoine
Hotel-Dieu
Institut d’ Hematol- ogie
Moabit Hos- pital
St. Georg Hospital
University of Tiibingen
University of Ferrara
Iowa City
Worcester
Minneapolis
Salt Lake City
Stanford
Vancouver
Olomouc Hradec Kralove
USA
USA
USA
USA
USA
Canada
Czechoslovakia
Coventry England
London England
Paris France
Lyon France
Paris France
Paris France
Montpellier France
Berlin W. Germany
Ham burg W. Germany
Tiibingen W. Germany
Ferrara Italy
18
36
17
14
15
17
65
2
15
130
13
12
18
4
3
15
9
4
14
33
9
7
15
5
43
2
15
34
13
0
8
4
1
10
8
4
C. P. Burns
I . Katayama H . E. Finkel
R. F . Branda
A. Turner C. R. Kjeldsberg
J. S. Burke
I . H. Plenderleith
B. Weidermann L. Chrobak R. Kodousek K. Indrak
N. K. Shinton
D. Catovsky
G. Flandrin
D. Espinousse P. A. Byron
G. Duhamel
C. M. Blanc Chr. Dao
P. Izarn J. M. Emberger M. Navarro
S. Mende
J. Dullmann K . Hausmann
H. W. von Heyden H. D. Waller
G. L. Castoldi
7
20
5
33
6
28
34
-
9
31
-
1 1
-
13
25
12
18
16

2076 CANCER April 15 1981 V O l . 47
Appendix 1. ( C o t i / i t i u d )
No. of No. of patients with Ref-
City Country patients splenectomies Investigator(s) erence
Meir General Kfar-Saba Israel Hospital
5 5 A. Gutman 17
University of Leiden Netherlands 23 1s J. Jansen 19 Leiden J . Hermans
J . te Velde
Radiumhos- Oslo pitalet
Norway S 2 R . Langholm 21
Universi- Zurich Switzerland 16 8 K. Rhyner 29 tatsspital J . Fehr
APPENDIX 2. Items included in the questionnaire
2-3 months
Before after At time of splenec- splenec- diagnosis tomy tomy
Agelsex Duration of
symptoms (months)
Date of diagnosis Splenomegaly
(cm ucm) Hepatomegal y
(cm ucm) Lymphadenopathy
( yeslno) Hemoglobin (gldl) Transfusions
(U/month) Leukocytes (/mm”) Neutrophils (%) Hairy cells (76) Platelets (lmm:’) Date of
splenectomy Weight of spleen Survival (months
after diagnosis) Cause of death Additional therapy
X
X
X
X
X
X
X
X
x X
X X
X X
X X
X X
X X
X
X
ucm = under costal margin