Embed Size (px)
DESCRIPTION
Spiritual and religious beliefs as risk factors for the onset of major depression
Citation preview

Psychological Medicinehttp://journals.cambridge.org/PSM
Additional services for Psychological Medicine:
Email alerts: Click hereSubscriptions: Click hereCommercial reprints: Click hereTerms of use : Click here
Spiritual and religious beliefs as risk factors for the onset of major depression: an international cohort study
B. Leurent, I. Nazareth, J. BellónSaameño, M.I. Geerlings, H. Maaroos, S. Saldivia, I. Švab, F. TorresGonzález, M. Xavier and M. King
Psychological Medicine / FirstView Article / January 2013, pp 1 12DOI: 10.1017/S0033291712003066, Published online:
Link to this article: http://journals.cambridge.org/abstract_S0033291712003066
How to cite this article:B. Leurent, I. Nazareth, J. BellónSaameño, M.I. Geerlings, H. Maaroos, S. Saldivia, I. Švab, F. TorresGonzález, M. Xavier and M. King Spiritual and religious beliefs as risk factors for the onset of major depression: an international cohort study. Psychological Medicine, Available on CJO doi:10.1017/S0033291712003066
Request Permissions : Click here
Downloaded from http://journals.cambridge.org/PSM, IP address: 128.40.240.4 on 30 Jan 2013

Spiritual and religious beliefs as risk factors forthe onset of major depression: an internationalcohort study
B. Leurent1,2, I. Nazareth2, J. Bellon-Saameno3, M.-I. Geerlings4, H. Maaroos5, S. Saldivia6, I. Svab7,
F. Torres-Gonzalez8, M. Xavier9 and M. King1*
1 Mental Health Sciences Unit, Faculty of Brain Sciences, University College London Medical School, UK2 Research Department of Primary Care and Population Health, University College London Medical School, UK3 Department of Preventive Medicine, El Palo Health Centre, Malaga, Spain4 University Medical Centre, Utrecht, The Netherlands5 Faculty of Medicine, University of Tartu, Estonia6 Departamento de Psiquiatrıa y Salud Mental, Universidad de Concepcion, Chile7 Department of Family Medicine, University of Ljubljana, Slovenia8 CIBERSAM-Granada University, Granada, Spain9 Department of Mental Health, Faculdade Ciencias Medicas, CEDOC, Lisboa, Portugal
Background. Several studies have reported weak associations between religious or spiritual belief and psychological
health. However, most have been cross-sectional surveys in the USA, limiting inference about generalizability. An
international longitudinal study of incidence of major depression gave us the opportunity to investigate this
relationship further.
Method. Data were collected in a prospective cohort study of adult general practice attendees across seven countries.
Participants were followed at 6 and 12 months. Spiritual and religious beliefs were assessed using a standardized
questionnaire, and DSM-IV diagnosis of major depression was made using the Composite International Diagnostic
Interview (CIDI). Logistic regression was used to estimate incidence rates and odds ratios (ORs), after multiple
imputation of missing data.
Results. The analyses included 8318 attendees. Of participants reporting a spiritual understanding of life at
baseline, 10.5% had an episode of depression in the following year compared to 10.3% of religious participants
and 7.0% of the secular group (p<0.001). However, the findings varied significantly across countries, with
the difference being significant only in the UK, where spiritual participants were nearly three times more likely
to experience an episode of depression than the secular group [OR 2.73, 95% confidence interval (CI) 1.59–4.68].
The strength of belief also had an effect, with participants with strong belief having twice the risk of
participants with weak belief. There was no evidence of religion acting as a buffer to prevent depression after
a serious life event.
Conclusions. These results do not support the notion that religious and spiritual life views enhance psychological
well-being.
Received 13 July 2012 ; Revised 19 November 2012 ; Accepted 6 December 2012
Key words : General practice, longitudinal, major depression, religion, spirituality.
Background
Research findings, most originating from the USA,
have generally reported a positive, albeit weak, re-
lationship between higher levels of religious involve-
ment and better health once other influences, such as
age, sex and social support, have been taken into ac-
count (Koenig et al. 1998, 2001 ; McCullough & Larson,
1999 ; Johnstone et al. 2008). Nevertheless, many other
studies do not find such an association (Payne et al.
1991; Schaefer, 1997 ; Lewis et al. 2000; Gartner et al.
2012). There have been at least two meta-analyses of
relevant studies. The first examined the relationship
between religiosity and psychological adjustment
(Hackney & Sanders, 2003), while excluding studies
measuring a wider concept of spirituality or those
examining the relationship with mental disorders.
* Address for correspondence : Professor M. King, Mental Health
Sciences Unit, University College London, Charles Bell House, 67–73
Riding House Street, London W1W 7EJ, UK.
(Email : [email protected])
Psychological Medicine, Page 1 of 12. f Cambridge University Press 2013doi:10.1017/S0033291712003066
ORIGINAL ARTICLE

A small positive correlation between religiosity and
psychological status was found (r=0.10, p<0.0001)
when combining all effect sizes from 35 cross-sectional
studies. Seventy-eight negative relationships were
found in the data set of 264 effect sizes. Greater effects
were seen with institutional religiosity than personal
devotion, and with psychological distress rather
than of life satisfaction. The authors concluded that
greater ‘ internality ’ of religious belief was associated
with more positive psychological outcomes. A second
meta-analysis of 147 studies (of which 15 were long-
itudinal) examined associations between religiosity
and/or spirituality and depressive symptoms and/or
depressive disorder (Smith et al. 2003). Religious/
spiritual belief seemed to have a small negative
(x0.096) correlation with depressive symptoms but
the protective effect of belief was stronger on risk
of major depression after significant life events.
Unfortunately, the authors did not distinguish evi-
dence from longitudinal versus cross-sectional studies
in their analysis.
Numerous cross-sectional studies have been con-
ducted since 2003, including some outside the USA. In
one very large Canadian community health study,
greater participation in worship was associated with
lower odds of psychiatric disorders but people who
placed greater importance on spiritual values had
higher odds of most psychiatric disorders (Baetz et al.
2006). A further cross-sectional study of more than
6000 people in Korea also reported that strong spiri-
tual values were associated with increased rates of
current depressive disorder (Park et al. 2012).
Most of the studies in the meta-analyses described
above (Hackney & Sanders, 2003 ; Smith et al. 2003)
were cross-sectional in nature and thus we need more
prospective research in a variety of cultures and so-
cieties. Recent prospective studies have been small
scale but generally positive in their findings. Kasen
et al. (2012) andMiller et al. (2012) reported data on 114
adults who were the grown-up children of a cohort of
people at high risk of depression, and matched con-
trols, enrolled in a multi-generational 10-year longi-
tudinal study. Participants for whom religion or
spirituality was highly important seemed to be pro-
tected from major depression, especially relapse in
those with a history of depression (Miller et al. 2012).
Religion was also more protective in participants
exposed to negative life events (Kasen et al. 2012).
However, there were few participants, the sample
was very specific (catholic or protestant Caucasians,
who were offspring of depressed parents for the ex-
posed cohort) and findings were of borderline signifi-
cance.
In earlier cross-sectional work in a large sample of
people from a range of ethnic groups in England and
Wales, we reported that holding a spiritual life view
without religious affiliation was associated with a
higher prevalence of anxiety and depression (King
et al. 2006a). However, the direction of this association
was unclear. Lack of religion may lead to common
mental disorders in vulnerable people who seek
meaning in their lives. Conversely, people developing
a common mental disorder who are not affiliated
to any religious group may become involved in a
search for meaning for relief from symptoms. The
New Age movements and other non-traditional faiths
in Western Europe may reflect a search for meaning in
societies such as the UK, where religious practice has
declined steeply in recent decades. We previously
undertook a prospective study to develop a risk pre-
diction algorithm for the onset of major depression in
general practice attendees in seven countries : six
European and one Latin American (King et al. 2008).
These data provided an opportunity to examine the
impact of spiritual and religious beliefs on the devel-
opment of depression. Our aims were to : (1) examine
the impact of a religious or spiritual life view on
onset of major depression over 12 months ; (2) assess
whether this impact varied for first or recurrent
episodes of depression ; (3) examine how the impact
varied by religious denomination, change in life
view and change in strength of belief over the
12 months ; and (4) determine whether the form of life
view mediated the impact of significant life events on
onset of major depression. Our principal hypothesis
was that people expressing a spiritual life view in the
absence of religious affiliation or practice are more
likely to develop DSM-IV major depression than those
who have a religious life view or are secular in out-
look.
Method
Study setting and design
The study, described in detail elsewhere (King et al.
2006b, 2008), was approved by research ethics com-
mittees in each country. It was a prospective cohort
study conducted in (1) 25 general practices in the
Medical Research Council (MRC) General Practice
Research Framework (GPRF) in the UK; (2) nine large
primary care centres in Andalucıa, Spain ; (3) 74 gen-
eral practices nationwide in Slovenia ; (4) 23 general
practices nationwide in Estonia ; (5) seven large gen-
eral practice centres near Utrecht, The Netherlands ;
(6) two large primary care centres in the Lisbon area of
Portugal ; and (7) 78 general practices in Concepcion
and Talcahuano in the Eighth Region of Chile. General
practices covered urban and rural populations with
considerable socio-economic variation.
2 B. Leurent et al.

Study participants
Consecutive attendees aged 18–75 years were re-
cruited in Europe between April 2003 and September
2004 and in Chile between October 2003 and February
2005. Exclusion criteria were inability to understand
the country’s main language, psychosis, dementia and
incapacitating physical illness. Recruitment varied
slightly because of local service differences. In the UK
and The Netherlands, researchers spoke to patients
while they waited in the practices. In the remaining
European countries, general practitioners (GPs) in-
troduced the study before contact with researchers. In
Chile, attendees were stratified on age and gender on
the basis of local figures and participants were selected
randomly within each stratum. Participants gave in-
formed consent and undertook a research evaluation
within 2 weeks. Only attenders without a DSM-IV di-
agnosis of major depressive disorder at baseline were
part of this analysis.
Assessments at baseline
Each instrument or question not available in the rel-
evant languages was translated from English and
back-translated by professional translators (King et al.
2006b).
Demography
We collected standard information on participants’
sex, age, education, marital status, employment and
ethnicity.
Religious and spiritual beliefs
The self-report version of the Royal Free Interview
for Spiritual and Religious Beliefs (King et al. 2001)
examines religious affiliation and practice, and spiri-
tual beliefs whether or not in the context of religion. In
this study only the first three items of the question-
naire were used. Before the questions are posed the
respondent reads an introductory statement : ‘ In using
the word religion, we mean the actual practice of a
faith, e.g. going to a temple, mosque, church or syna-
gogue. Some people do not follow a religion but do
have spiritual beliefs or experiences. For example, they
believe that there is some power or force other than
themselves, which might influence their life. Some
people think of this as God or gods, others do not.
Some people make sense of their lives without any
religious or spiritual belief ’. On the basis of this state-
ment, respondents were asked to indicate whether
their understanding of life was primarily religious,
spiritual, or neither religious nor spiritual (this latter
category will be referred to as ‘secular ’). If religious or
spiritual they were then asked to indicate whether
they regarded themselves as having a specific religion.
People with a spiritual life view may identify them-
selves with a religion, even if they do not practice it.
Finally, religious and spiritual participants were asked
to indicate on scale from 1 to 6 how strongly they held
their life view.
Diagnosis of depression
A DSM-IV diagnosis of major depression in the pre-
ceding 6 months was made using the Depression
Section of the Composite International Diagnostic
Interview (CIDI ; Robins et al. 1988; WHO, 1997).
Screen for lifetime history of depression
Lifetime depression was considered possible if the re-
spondent answered affirmatively to both of the first
two questions of the CIDI Depression Section (WHO,
1997).
Life events
The List of Threatening Experiences questionnaire
(Brugha et al. 1985) enquired about major life events in
the preceding 6 months.
Social support
Adequacy of support from family and friends was
measured using brief standardized questions (Blaxter,
1990).
Follow-up assessments at 6 and 12 months
All participants were re-evaluated for DSM-IV major
depression after 6 and 12 months. At 6 months they
also completed the Royal Free Interview for Spiritual
and Religious Beliefs and the questions on life events.
Statistical analysis
To manage missing data we undertook multiple im-
putation by chained equation, using the ice procedure
in Stata (Royston, 2005). We generated two imputed
databases each containing 30 imputed versions using
all relevant variables predicting depression or miss-
ingness ; one database was used for the analysis of the
understanding of life and the other for the analysis of
religious denomination and strength of belief in re-
ligious or spiritual participants. Regression results
were combined using Rubin’s rule (mim command
in Stata). We explored the pattern of missing data
and performed sensitivity analyses on complete cases.
t tests and x2 tests were used to compare groups at
baseline. Incidence rates of major depression were
Spiritual and religious beliefs and psychological well-being 3

obtained on imputed data by univariable logistic re-
gression and presented graphically. Odds ratios (ORs)
unadjusted and adjusted for age, sex, education, em-
ployment, social support, past history of depression
and country were computed using logistic regression.
Interactions between the predictor and each covariate
were tested and the model was stratified if an inter-
action was found. In view of multiple testing, we
considered an interaction significant at the level of
p<0.01. All other p values reported are two-sided, and
considered significant at the level of p<0.05. Incidence
rates and ORs are reported along with their 95% con-
fidence intervals (CIs). Standard errors are based on
robust sandwich estimates to account for the cluster-
ing effect of each general practice (Huber, 1967).
For the analyses on imputed data, the exact number
of participants in each category of the exposure
variables cannot be reported as it varied slightly
with each imputation. In the presence of missing
data, CIs are a more reliable guide to the precision
around estimates than estimated frequencies. Statis-
tical analyses were performed using Stata Release 11
(Stata Corp, 2009).
Results
Response rates and prevalence of DSM-IV major
depression at recruitment
Response to recruitment was high in Portugal (76%),
Estonia (80%), Slovenia (80%) and Chile (97%) but
lower in the UK (44%) and The Netherlands (45%).
Ethical constraints did not allow collection of data on
non-responders at baseline. Across all countries the
response to follow-up at 6 months was at 89.5%. A
total of 10045 people took part : 219 were excluded on
grounds of age, 143 had a missing CIDI diagnosis
and five a missing practice identification at baseline.
Of the remaining 9678, 8318 without DSM-IV major
depression (86%) at baseline were analysed. The me-
dian age was 49 years, two-thirds were women,
and 75% of participants held a religious or spiritual
understanding of life. Women were more likely
than men to have a religious or spiritual understand-
ing of life, and a past history of depression was least
common in people with a spiritual understanding
(Table 1). The characteristics of participants by coun-
try are reported in Supplementary Table S1 (available
online). Eleven per cent of participants did not com-
plete the 6-month follow-up and 16% did not com-
plete the 12-month follow-up. Non-completers tended
to be younger and less educated and had experienced
more serious life events in the 6 months before base-
line.
Understanding of life and onset of DSM-IV major
depression over 12 months
Of participants reporting a religious understanding of
life, 10.3% experienced an episode of major depression
over the subsequent 12 months, compared to 10.5% of
participants with a spiritual life view and 7.0% of the
secular group (p<0.001). This finding was examined
more closely in a logistic regression with secular
participants as the reference group. The results are
reported unadjusted and adjusted for age, sex, edu-
cation, employment, social support, past history of
depression and country. Participants with a spiritual
understanding of life had a greater risk of major de-
pression at 6 or 12 months than participants with
neither a spiritual nor a religious life view (Table 2).
Participants holding a religious understanding of life
were also more at risk than secular participants, but
this finding lost statistical significance after adjust-
ment. When stratified by country, however, our find-
ing that a spiritual life view predisposed people to
major depression was significant only in the UK,
where spiritual participants were nearly three times
more likely to experience an episode of depression
than the secular group (OR 2.73, 95% CI 1.59–4.68)
(Table 2). In a post-hoc analysis, using international
surveys (European Values Study, 2012 ; World Values
Survey, 2012) we ranked the countries on the pro-
portion of people considering themselves religious
(from least to most : the UK, Estonia, The Netherlands,
Spain, Chile, Slovenia, Portugal). The variation in re-
sults between countries was not explained by the im-
portance of religion in each country (results available
from the authors on request).
Understanding of life and onset of first episode or
recurrence of major depression over 12 months
To investigate the effect of religion on first episode
versus recurrence of depression, we stratified the
analysis by lifetime history of depression. The effect of
a religious versus a secular understanding of life
was similar in predicting new onset (OR 1.60, 95% CI
1.05–2.42) and recurrence (OR 1.44, 95% CI 1.07–1.93).
A spiritual view of life did not predict onset of de-
pression in participants with no history of depression
(OR 1.04, 95% CI 0.63–1.73) but was related to new
occurrence for participants with a past history of de-
pression (OR 1.61, 95% CI 1.19–2.17). However, this
interaction was not significant (p=0.15).
Religious denomination and onset of major
depression
In the 6094 participants with a spiritual or religious
understanding of life, the incidence of major
4 B. Leurent et al.

Table 1. Demographic characteristics and understanding of life
Understanding of life
Totala
(n=8318) p valuebReligious
(n=4348, 52%)
Spiritual
(n=1746, 21%)
Neither
(n=2087, 25%)
Country, n (%)
UK 462 (10.6) 300 (17.2) 354 (17.0) 1131 (13.6) <0.001
Spain 714 (16.4) 136 (7.8) 153 (7.3) 1006 (12.1)
Slovenia 322 (7.4) 328 (18.8) 387 (18.5) 1048 (12.6)
Estonia 189 (4.3) 227 (13.0) 506 (24.2) 923 (11.1)
The Netherlands 358 (8.2) 143 (8.2) 469 (22.5) 1077 (12.9)
Portugal 833 (19.2) 75 (4.3) 97 (4.6) 1005 (12.1)
Chile 1470 (33.8) 537 (30.8) 121 (5.8) 2128 (25.6)
Gender, n (%)
Female 3045 (70.0) 1235 (70.7) 1235 (59.2) 5599 (67.3) <0.001
Male 1303 (30.0) 511 (29.3) 852 (40.8) 2719 (32.7)
Age (years), n (%)
18–29 498 (11.5) 332 (19.0) 406 (19.5) 1244 (15.0) <0.001
30–39 585 (13.5) 356 (20.4) 429 (20.6) 1380 (16.6)
40–49 764 (17.6) 356 (20.4) 398 (19.1) 1540 (18.5)
50–59 946 (21.8) 333 (19.1) 435 (20.8) 1745 (21.0)
60–69 1022 (23.5) 266 (15.2) 293 (14.0) 1619 (19.5)
70–76 533 (12.3) 103 (5.9) 126 (6.0) 790 (9.5)
Married/living with partner, n (%)
No 1333 (30.7) 615 (35.3) 634 (30.5) 2614 (31.5) 0.001
Yes 3005 (69.3) 1129 (64.7) 1445 (69.5) 5681 (68.5)
Missing 10 2 8 23
Education, n (%)
Above school 656 (15.1) 533 (30.5) 749 (36.0) 1965 (23.7) <0.001
Secondary 1324 (30.5) 627 (35.9) 820 (39.4) 2844 (34.3)
Primary/no education 2011 (46.3) 388 (22.2) 343 (16.5) 2769 (33.4)
Trade/other 349 (8.0) 197 (11.3) 167 (8.0) 718 (8.7)
Missing 8 1 8 22
Employment, n (%)
Employed/student 1663 (38.4) 975 (56.1) 1313 (63.5) 4003 (48.4) <0.001
Retired 1017 (23.5) 276 (15.9) 336 (16.2) 1662 (20.1)
Unemployed/other 1654 (38.2) 487 (28.0) 420 (20.3) 2610 (31.5)
Missing 14 8 18 43
European ethnicity, n (%)
No 1535 (35.4) 563 (32.3) 162 (7.8) 2265 (27.3) <0.001
Yes 2806 (64.6) 1180 (67.7) 1921 (92.2) 6039 (72.7)
Missing 7 3 4 14
Past history of depression, n (%)
No 2021 (46.5) 728 (41.8) 1039 (49.9) 3863 (46.5) <0.001
Yes 2322 (53.5) 1015 (58.2) 1046 (50.2) 4445 (53.5)
Missing 5 3 2 10
Family and friends support
Mean (S.D.) 12.7 (2.4) 12.3 (2.7) 12 (2.7) 12.4 (2.5) <0.001
Missing 34 10 19 77
Religious denomination, n (%)
Catholic 2680 (62.2) 563 (33.0) 3243 (53.9) <0.001
Protestant 1248 (29.0) 317 (18.6) 1565 (26.0)
Other religion 243 (5.6) 118 (6.9) N.A. 361 (6.0)
No specific religion 137 (3.2) 708 (41.5) 845 (14.1)
Missing 40 40 80
Strength of belief
Mean (S.D.) 4.3 (1.5) 3.7 (1.6) N.A. 4.1(1.6) <0.001
Missing 90 30 120
S.D., Standard deviation ; N.A., not applicable.a Including 137 missing understanding of life.b p value for difference between understanding of life, from t tests or x2 tests, as appropriate.
Spiritual and religious beliefs and psychological well-being 5

depression over the subsequent 12 months was similar
across the different religious denominations (Catholic
9.8%, Protestant 10.9%, other religion 11.5%, no spe-
cific religion 10.8%, p=0.65). In a post-hoc analysis
in the 1746 participants who reported a spiritual
understanding of life, a similar incidence of major de-
pression over the subsequent 12 months was found
between those who were able to nominate a religious
affiliation and those who were not (10.7% v. 11.1%,
p=0.41).
Strength of belief at baseline and onset of major
depression
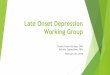
Higher strength of belief in the 6094 participants
who reported a spiritual or religious life view was as-
sociated with a greater likelihood of DSM-IV major
depression over the subsequent 12 months after ad-
justment for age, sex, education, employment, social
support, past history of depression, and country
(unadjusted OR per unit increase on the scale of
strength of belief 1.14, 95% CI 1.07–1.21 ; adjusted OR
1.08, 95% CI 1.00–1.15) (Fig. 1). There was no interac-
tion between country and strength of belief (p=0.16).
Those with a strongly held belief were twice as likely
to experience major depression in the subsequent
12 months as those with a weakly held belief.
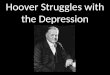
Change in strength of belief and subsequent onset
of major depression
The incidence rate of depression between 6 and
12 months was 5.5%. We examined whether change
over the first 6-month follow-up in the strength of
spiritual or religious belief (strength score at 6 months
minus score at baseline) was associated with onset
of major depression between 6 and 12 months, after
adjustment for strength of belief at baseline and other
Table 2. Odds ratios (ORs) for onset of major depression over 12 months by understanding
of life, compared to neither religious nor spiritual
Unadjusted OR (95% CI) Adjusted ORa (95% CI)
Overall
Religious 1.52 (1.19–1.93)** 1.14 (0.87–1.50)
Spiritual 1.56 (1.21–2.02)** 1.32 (1.02–1.70)*
UK
Religious 1.35 (0.68–2.68) 1.86 (0.88–3.92)
Spiritual 2.73 (1.59–4.68)*** 2.68 (1.52–4.71)**
Spain
Religious 1.41 (0.78–2.54) 1.34 (0.73–2.46)
Spiritual 1.53 (0.73–3.20) 1.50 (0.73–3.07)
Slovenia
Religious 0.62 (0.26–1.46) 0.69 (0.27–1.73)
Spiritual 1.06 (0.52–2.16) 1.10 (0.52–2.34)
Estonia
Religious 1.16 (0.63–2.13) 1.06 (0.51–2.22)
Spiritual 1.08 (0.59–1.98) 1.14 (0.62–2.12)
The Netherlands
Religious 0.63 (0.31–1.28) 0.69 (0.35–1.37)
Spiritual 1.15 (0.62–2.13) 1.07 (0.57–2.02)
Portugal
Religious 2.40 (0.55–10.43) 1.78 (0.39–8.08)
Spiritual 1.96 (0.38–10.05) 1.52 (0.27–8.48)
Chile
Religious 1.12 (0.58–2.17) 1.08 (0.54–2.14)
Spiritual 1.03 (0.53–2.00) 1.04 (0.56–1.96)
CI, Confidence interval.
Values based on imputed data.a Adjusted for age, sex, education, employment, social support, past history of
depression, and country.
* p <0.05, ** p<0.01, *** p<0.001.
6 B. Leurent et al.

covariates. Those whose belief decreased seemed
to be at greater risk of depression whereas those
whose belief increased had slightly less risk (Fig. 2).
However, CIs were wide, especially for the larger
degrees of change.
Change in the nature of life view and subsequent
onset of major depression
Although an understanding of life (religious, spiritual
or secular) is relatively stable in most people
(King et al. 1999), 27.1% of participants in this
study changed their life view between baseline and
the 6-month interview. Thus, we examined whether
change in the nature of the life view between
baseline and 6 months had any association with onset
major depression between 6 and 12 months. Point
estimates were in the direction of higher risk of de-
pression for change in a religious direction and
lower risk for change in a secular direction, but the
CIs were wide and no significant difference was found
(Table 3).
7.4
6.2
10.19.2
11.712.5
0
2
4
6
8
10
12
14
16In
cide
nce
of d
epre
ssio
n ov
er 1
2 m
onth
s (%
)
Weakly 2 3 4 5 Strongly
How strongly do you hold your religious or spiritual view of life?
Incidence 95% CI
n*= 520 443 1075 1255 947 1734
Fig. 1. Incidence of major depression versus strength of spiritual or religious belief. Based on imputed data. * Frequencies based
on observed data, not numbers included in analysis. CI, Confidence interval.
2.21
0.94
1.471.25
1.00 0.93 0.920.77 0.79
0.25
0.5
1
2
4
OR
and
95%
CI fo
r de
pres
sion
at 1
2 m
onth
s
–5/–4 –3 –2 –1 0 (Ref.) +1 +2 +3 +4/+5
Difference in strength of belief between baseline and 6 months
n*= 51 140 328 844 2193 806 405 171 113
Fig. 2. Adjusted odds ratio (OR) for onset of major depression between 6 and 12 months after a change in strength of belief
between baseline and 6 months. OR adjusted for strength of belief at baseline, age, sex, education, employment, social support,
past history of depression, and country. Values based on imputed data. * Frequencies based on observed data, not numbers
included in analysis. CI, Confidence interval.
Spiritual and religious beliefs and psychological well-being 7

Impact of belief on the relationship between serious
life events and onset of major depression
Finally, we examined whether a religious or spiritual
understanding of life modified the risk of major de-
pression following a serious life event. As expected,
the incidence of major depression between baseline
and 12 months was higher for patients who experi-
enced serious life events (Fig. 3). Understanding of
life was not a significant modifying factor of the
effect of life events on depression (unadjusted p=0.57,
adjusted p=0.48).
Sensitivity of the analysis to imputation of missing
data
When imputed data were compared to the observed
data we found a similar distribution between under-
standing of life categories, but the incidence of major
depression at 6 or 12 months was higher in the im-
puted data (8.7% v. 9.5%), reflecting the higher likeli-
hood of dropping out for patients at risk of depression
at baseline. No major discrepancy was found between
imputed data and complete-case analyses. For ex-
ample, the OR of developing major depression by 6 or
Table 3. Odds ratios (ORs) for onset of major depression between 6 and 12 months, after a
change in understanding of life between baseline and 6 months
Understanding of life
FrequencyaUnadjusted OR
(95% CI)
Adjusted ORb
(95% CI)At baseline At 6 months
Religious Religious 3004 1.00 (Reference) 1.00 (Reference)
Spiritual 658 0.98 (0.62–1.53) 0.97 (0.61–1.55)
Neither 175 0.64 (0.26–1.56) 0.87 (0.35–2.16)
Spiritual Religious 436 1.40 (0.84–2.32) 1.51 (0.87–2.61)
Spiritual 887 1.00 (Reference) 1.00 (Reference)
Neither 253 1.05 (0.54–2.03) 1.09 (0.56–2.14)
Neither Religious 196 1.53 (0.70–3.36) 1.31 (0.53–3.19)
Spiritual 265 1.46 (0.72–2.96) 1.35 (0.66–2.78)
Neither 1413 1.00 (Ref) 1.00 (Ref)
CI, Confidence interval.
Values based on imputed data.a Frequencies based on observed data, not numbers included in analysis.b Adjusted for age, sex, education, employment, social support, past history of
depression, and country.
5
10
15
20
Inci
denc
e of
dep
ress
ion
over
12
mon
ths
(%)
0 1 >1
Life events between baseline and 6 months
Religious Spiritual
Neither
n* = 3474 2235 1749
Fig. 3. Modifying effect of life understanding on major depression after serious life events. Values based on imputed data.
* Frequencies based on observed data, not numbers included in analysis.
8 B. Leurent et al.

12 months was 1.64 (95% CI 1.26–2.15) for people with
a religious understanding and 1.74 (95% CI 1.34–2.26)
for people with a spiritual understanding of life,
compared to 1.52 and 1.56 respectively on imputed
data (Table 2).
Discussion
Main findings
We found that people who held a religious or spiritual
understanding of life had a higher incidence of de-
pression than those with a secular life view. However,
this finding varied by country ; in particular, people in
the UK who had a spiritual understanding of life were
the most vulnerable to the onset of major depression.
Regardless of country, the stronger the spiritual or re-
ligious belief at baseline, the higher the risk of onset of
depression. Although our main finding of an associ-
ation between religious life understanding and onset
of depression varied by country, we found no
evidence that spirituality may protect people, and
only weak evidence that a religious life view was
possibly protective in two countries (Slovenia and The
Netherlands). Finally, there was no moderating effect
of religious and spiritual understanding of life on the
impact of life events on onset of major depression.
Strengths and limitations
The main strengths of our study are its prospective
cohort design, the involvement of several countries,
the large sample size and the use of standardized as-
sessments of religious/spiritual belief, other risk vari-
ables and major depression. However, combining
people from different cultures creates heterogeneity
and runs the risk of missing real differences within
countries. Despite a large sample size, we lacked
power for some of the analyses, particularly the as-
sessment of statistical interactions. However, to our
knowledge there are very few data sets available con-
taining variables on spiritual and religious beliefs that
are large enough to undertake interaction analyses.
Thus we consider it is important to show the results to
avoid a reporting bias that favours statistically sig-
nificant results (Dwan et al. 2008). Another strength
of this study is the use of multiple imputation to take
account of participants who dropped out. Assuming
predictors of missingness have been examined at
baseline, this should give unbiased findings, as op-
posed to restricting the analysis to participants who
completed both follow-ups only, which may represent
a sample at lesser risk of depression than the original
one. However, participations rates were low in some
countries, and we cannot assume that findings in
general practice attendees can be generalized to the
whole population. Our study sample is likely to have
a more complex medical history ; for example, 53%
reported a lifetime history of depression although
other evidence would suggest this figure is usually in
the range 30–40% (Kruijshaar et al. 2005). However,
our population may be more representative of life
views than those who might participate in a study of
religion. The original aim of this study was to develop
a risk prediction algorithm for depression (PredictD;
King et al. 2008), and thus our analysis is limited to the
religiosity data available. Religion did not appear as a
variable in the final prediction algorithm PredictD,
which included only the most parsimonious combi-
nation of risk factors of depression, but this does
not imply the absence of a relationship between re-
ligiosity and depression. Although our questions were
limited to people’s overall view of religion and spiri-
tuality, rather than the detail of any specific belief,
they applied to all people and not just those with a
Christian background, which is often the case in North
American research. Another limitation is the difficulty
distinguishing religion and spirituality and the trouble
respondents may have in placing themselves in one of
the two categories. This may account for a proportion
of the 27% of participants who changed their life view
between baseline and 6 months. However, the ques-
tions have high repeatability (King et al. 2001) and
clear definitions were given in a short note preceding
the question, ensuring a universal understanding of
the term across the different countries and cultures.
Furthermore, they avoided the common pitfall in re-
ligion studies of conflating questions on religion and
spiritual belief with those on psychological well-being
(Koenig, 2008). Finally, the relationship between
religion, spirituality and mental symptoms should
not necessarily be interpreted as causal in nature.
Although the longitudinal design removes the possi-
bility of reverse causation, unmeasured confounders
in the complex relationship between religiosity and
depression are likely to remain, even after adjustment
for main risk factors of depression.
Relationship to other findings
Our work adds to a growing body of evidence that
spiritual beliefs in the absence of a clear religious
affiliation or practice increase vulnerability to de-
pression (Baetz et al. 2006; Braam et al. 2007; Park et al.
2012) ; it also contrasts with many studies where re-
ligious and spiritual beliefs and practice have been
found to be associated with better mental health.
An explanation for this disparity could be the complex
relationship between the concepts of religiosity
and well-being, and that findings in any specific
Spiritual and religious beliefs and psychological well-being 9

population may not generalize to another. Research in
this field has been dominated by North American
studies, whereas in the more secular cultures of
Europe, religious people may feel less supported in
their faith. Alternatively, it may relate to the ways in
which such beliefs are measured in research. In their
meta-analysis, Hackney & Sanders (2003) criticized
many studies for measuring religion and spirituality
with insufficient depth and suggested that a multi-
faceted concept such as religious belief and practice
may have complex associations with mental health.
In their meta-analysis of 147 studies on religious
belief and depression, Smith et al. (2003) found that
extrinsic religious orientation and so-called negative
religious coping were associated with higher levels of
depressive symptoms. However, they also reported
that the negative correlation between religiousness
and depressive symptoms was at its greatest in the
presence of life stress and suggested that religion may
have a buffering effect on the impact of life events. We
did not find evidence of such buffering. They specu-
lated that social desirability of response (exaggerating
religiousness and downrating depressive symptoms),
or the possibility that religious people might be better
at expressing emotion and thus coping with stress,
might explain some of the correlation in their studies
that were mainly cross-sectional in nature.
Recent longitudinal research suggests that attaching
a high importance to religion was associated with
lower risk of recurrence of depression in the subsequent
10 years (Miller et al. 2012) and had a protective effect
after negative life events (Kasen et al. 2012). We have
not been able to replicate either of these findings in
this cohort. Our study was, however, consistent with
their finding of no clear relationship between religious
denomination and depression.
The disparity in the findings suggests that, if there
is an association between religion/spirituality and
psychological well-being, it is likely to be weak. If re-
ligious belief has a powerful positive effect on mental
health, we would expect to detect it in most studies.
Implications
Why a religious or spiritual life view might place
people at risk of depression remains unclear. One ex-
planation is that people predisposed to depression at
baseline may seek meaning in spiritual or religious
sources. The possibility that people predisposed to
depression increase their search for existential mean-
ing in religion and spirituality is supported by our
finding that change in belief over time towards greater
religiosity did seem to be related to greater risk of de-
pression.
In conclusion, we found that holding a religious or
spiritual life view, in contrast to a secular outlook,
predisposed people to the onset of major depression
and that such beliefs and practice did not act as a
buffer to adverse life events. Our findings highlight
the complexity of the relationship between religion,
spirituality and mental health and offer a challenge to
an increasing tendency to regard religion and spiritu-
ality as being good for mental well-being (Schumann
& Meador, 2003).
Supplementary material
For supplementary material accompanying this paper
visit http://dx.doi.org/10.1017/S0033291713003066.
Acknowledgements
The study in Europe was funded by a European
Commission Vth Framework grant (PREDICT-QL4-
CT2002-00683). Funding in Chile was provided by
project FONDEF DO2I-1140. We are grateful for part
support in Europe from: the Estonian Scientific
Foundation (grant 5696) ; the Slovenian Ministry for
Research (grant 4369-1027) ; the Spanish Ministry of
Health (FIS references : PI041980, PI041771, PI042450)
and the Spanish Network of Primary Care Research,
redIAPP (ISCIII-RETIC RD06/0018) and SAMSERAP
group; and the UK NHS Research and Development
office for service support costs in the UK. The funders
had no direct role in the design or conduct of the
study, interpretation of the data or review of the
manuscript.
M. King had full access to the data and takes re-
sponsibility for their integrity and the accuracy of
the data analysis. We thank all patients and general
practice staff who took part ; the European Office at
University College London for their administrative
assistance at the coordinating centre ; K. McCarthy,
the project’s scientific officer in the European
Commission, Brussels, for his helpful support and
guidance ; the UKMRCGPRF; L. Letley from the MRC
GPRF; the GPs of the Utrecht General Practitioners’
Network ; and the Camden and Islington Mental
Health and Social Care Trust. We also acknowledge
the Maristan network, through which the collabor-
ation in Spain, Portugal, the UK and Chile first devel-
oped.
Declaration of Interest
None.
10 B. Leurent et al.

References
Baetz M, Bowen R, Jones G, Koru-Sengul T (2006). How
spiritual values and worship attendance relate to
psychiatric disorders in the Canadian population. Canadian
Journal of Psychiatry 51, 654–661.
Blaxter M (1990). Health and Lifestyles. Routledge : London.
Braam AW, Deeg DJ, Poppelaars JL, Beekman AT,
van Tilburg W (2007). Prayer and depressive symptoms
in a period of secularization : patterns among older adults
in the Netherlands. American Journal of Geriatric Psychiatry
15, 273–281.
Brugha T, Bebbington P, Tennant C, Hurry J (1985). The
List of Threatening Experiences : a subset of 12 life event
categories with considerable long-term contextual threat.
Psychological Medicine 15, 189–194.
Dwan K, Altman DG, Arnaiz JA, Bloom J, Chan AW,
Cronin E, Decullier E, Easterbrook PJ, Von Elm E,
Gamble C, Ghersi D, Ioannidis JP, Simes J,
Williamson PR (2008). Systematic review of the empirical
evidence of study publication bias and outcome reporting
bias. PLoS One 3, e3081.
European Values Study (2012). Research theme : religion
(www.europeanvaluesstudy.eu/evs/research/themes/
religion/). Accessed 6 July 2012.
Gartner J, Larson DB, Allen DG (2012). Religious
commitment and mental health : a review of the empirical
literature. Journal of Psychology and Theology 19, 6–25.
Hackney CH, Sanders GS (2003). Religiosity and mental
health : a meta-analysis of recent studies. Journal for the
Scientific Study of Religion 42, 43–55.
Huber PJ (1967). The behavior of maximum likelihood
estimates under non-standard conditions. Proceedings of the
Fifth Berkeley Symposium on Mathematical Statistics and
Probability 1, 221–233.
Johnstone B, Franklin KL, Yoon DP, Burris J, Shigaki C
(2008). Relationships among religiousness, spirituality, and
health for individuals with stroke. Journal of Clinical
Psychology in Medical Settings 15, 308–313.
Kasen S, Wickramaratne P, Gameroff MJ, Weissman MM
(2012). Religiosity and resilience in persons at high
risk for major depression. Psychological Medicine 42,
509–519.
King M, Speck P, Thomas A (1999). The effect of spiritual
beliefs on outcome from illness. Social Science and Medicine
48, 1291–1299.
King M, Speck P, Thomas A (2001). The Royal Free
Interview for Spiritual and Religious Beliefs : development
and validation of a self-report version. Psychological
Medicine 31, 1015–1023.
King M, Walker C, Levy G, Bottomley C, Royston P,
Weich S, Bellon-Saameno J, Moreno B, Svab I, Rotar D,
Rifel J, Maaroos H, Aluoja A, Kalda R, Neeleman J,
Geerlings MI, Xavier M, Carraca I, Goncalves-Pereira M,
Vicente B, Saldivia S, Melipillan R, Torres-Gonzalez F,
Nazareth I (2008). Development and validation of
an international risk prediction algorithm for
episodes of major depression in general practice
attendees : the PredictD study. Archives of General
Psychiatry 65, 1368–1376.
King M, Weich S, Nazroo J, Blizard R (2006a).
Religion, mental health and ethnicity. EMPIRIC – a
national survey of England. Journal of Mental Health 15,
153–162.
King M, Weich S, Torres-Gonzalez F, Svab I, Maaroos HI,
Neeleman J, Xavier M, Morris R, Walker C,
Bellon-Saameno JA, Moreno-Kustner B, Rotar D, Rifel J,
Aluoja A, Kalda R, Geerlings MI, Carraca I,
de Almeida MC, Vicente B, Saldivia S, Rioseco P,
Nazareth I (2006b). Prediction of depression in European
general practice attendees : the PREDICT study. BMC
Public Health 6, 6.
Koenig HG (2008). Concerns about measuring ‘ spirituality ’
in research. Journal of Nervous and Mental Disease 196,
349–355.
Koenig HG, George LK, Peterson BL (1998). Religiosity and
remission of depression in medically ill older patients.
American Journal of Psychiatry 155, 536–542.
Koenig HK, McCullough ME, Larson DB (2001).
Handbook of Religion and Health. Oxford University Press :
Oxford.
Kruijshaar ME, Barendregt J, Vos T, de Graaf R, Spijker J,
Andrews G (2005). Lifetime prevalence estimates of major
depression : an indirect estimation method and a
quantification of recall bias. European Journal of
Epidemiology 20, 103–111.
Lewis CA, Maltby J, Burkinshaw S (2000). Religion and
happiness : still no association. Journal of Beliefs and Values
21, 233–236.
McCullough ME, Larson DB (1999). Religion and
depression : a review of the literature. Twin Research 2,
126–136.
Miller L, Wickramaratne P, Gameroff MJ, Sage M,
Tenke CE, Weissman MM (2012). Religiosity and
major depression in adults at high risk : a ten-
year prospective study. American Journal of Psychiatry
169, 89–94.
Park JI, Hong JP, Park S, Cho MJ (2012). The relationship
between religion and mental disorders in a Korean
population. Psychiatry Investigation 9, 29–35.
Payne IR, Bergin AE, Bielema KA, Jenkins PH (1991).
Review of religion and mental health : prevention and the
enhancement of psychosocial functioning. Prevention in
Human Services 9, 11–49.
Robins LN, Wing J, Wittchen HU, Helzer JE,
Babor TF, Burke J, Farmer A, Jablenski A, Pickens R,
Regier DA, Sartorius N, Towle LH (1988). The
Composite International Diagnostic Interview.
An epidemiologic instrument suitable for use in
conjunction with different diagnostic systems and
in different cultures. Archives of General Psychiatry 45,
1069–1077.
Royston P (2005). Multiple imputation of missing values :
update of ice. Stata Journal 5, 527–536.
Schaefer WE (1997). Religiosity, spirituality, and personal
distress among college students. Journal of College Student
Development 38, 633–644.
Schumann JJ, Meador KG (2003). Heal Thyself : Spirituality,
Medicine, and the Distortion of Christianity. Oxford
University Press : New York.
Spiritual and religious beliefs and psychological well-being 11

Smith TB, McCullough ME, Poll J (2003). Religiousness and
depression : evidence for a main effect and the moderating
influence of stressful life events. Psychological Bulletin 129,
614–636.
StataCorp (2009). Stata Statistical Software : Release 11. Stata
Corporation : College Station, TX.
WHO (1997). Composite International Diagnostic
Interview (CIDI). Version 2.1. World Health Organization :
Geneva.
World Values Survey (2012). Online Data Analysis, WVS
2005–2008 (www.wvsevsdb.com/wvs/
WVSAnalizeStudy.jsp). Accessed 6 July 2012.
12 B. Leurent et al.















![Biochimica et Biophysica Acta - University of Hong Kong of corticosterone.pdf · past history of depression,female gender, and early onset of AD [5,6].A historyofdepressionitselfhasalsobeenassociatedwithincreasedrisks](https://img.pdfslide.us/doc/110x75/5c684f1e09d3f2f5638b552f/biochimica-et-biophysica-acta-university-of-hong-of-corticosteronepdf-past.jpg)