Embed Size (px)
Citation preview
Dynamic Myocardial Perfusion in a Porcine Balloon-induced Ischemia Model
using Spectral Detector CT Rachid Fahmi 1, Ph.D.,
Brendan Eck1, Jacob Levi1, Anas Fares2, Mani Vembar3, Amar Dhanantwari3, Hiram Bezerra2, and David Wilson1,4
1 Biomedical Imaging Laboratory, Case Western Reserve University 2 Harrington Heart and Vascular Institute, University Hospitals, Case Medical Center 3 Philips Healthcare 4 Radiology, Case Western Reserve University
Investigate the performance of dual energy CT (DECT) with a prototype spectral detector CT (SDCT) scanner (Philips Healthcare) to perform dynamic myocardial CT perfusion (CTP) on a percutaneous porcine model with adjustable coronary occlusion guided by fractional flow reserve (FFR) measurements.
Objective
Adding robust cardiac CTP to coronary CTA will make CT a one stop shop imaging modality for cardiac imaging.
Clinical Relevance
Clinical use of CTP remains limited to date due in part to x-ray dose, BH artifacts, and partial scan artifacts.
Current Challenges

Context and motivation
How can we address some CTP challenges? • DECT has the potential of producing images free of beam hardening artifacts
by synthesizing mono-energetic (monoE) images. • Dynamic CTP requires faster scanners to avoid partial scan artifacts.
• Coronary CTA is the only non-invasive imaging method capable of detecting coronary stenoses.
• Significant discordance between angiographic stenosis (anatomy) and myocardial ischemia (function).
• Over 60% of invasive coronary angiographies (ICA) are negative, subjecting patients to unnecessary discomfort/risk, and driving up costs.
• No existing non-invasive test to assess both anatomic and functional ischemia in a single setting.
• Current guidelines recommend documenting ischemia with a non-invasive functional test (s.a., SPECT, MR).
• CT may be the perfect gatekeeper exam giving both anatomy (CTA) and function (CTP), a one-stop-shop for value-based reimbursement.
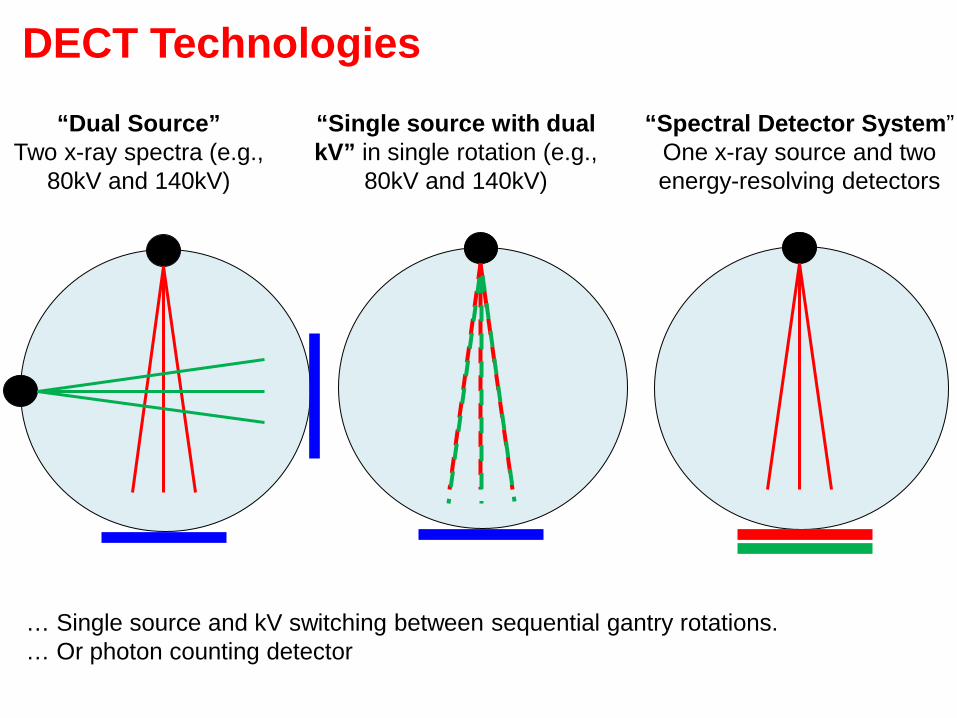
DECT Technologies “Dual Source”
Two x-ray spectra (e.g., 80kV and 140kV)
“Single source with dual kV” in single rotation (e.g.,
80kV and 140kV)
“Spectral Detector System” One x-ray source and two energy-resolving detectors
… Single source and kV switching between sequential gantry rotations. … Or photon counting detector
• Simultaneous detection of low and high x-ray photon energies: Low and high projection data are perfectly registered, spatially and temporally, with each other. Ideal for imaging moving objects such as a beating heart.
• Allows for projection space reconstruction and processes Accurate material decomposition and BH correction.
• Fast gantry rotation (0.27s) Allows full 360degree acquisitions No shading artifacts in dynamic acquisitions.
• Full field of view (FOV) acquisitions (50cm).
• No cross scatter .
Some advantages of the SDCT system
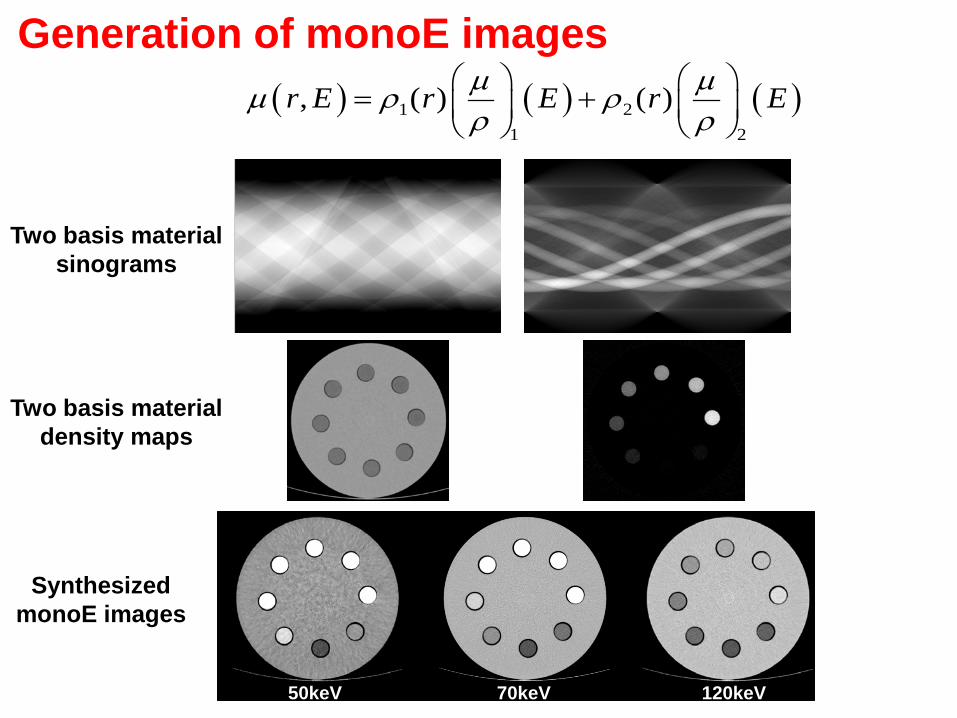
Generation of monoE images ( ) ( ) ( )1 2
1 2
, ( ) ( )r E r E r Eµ µµ ρ ρρ ρ
= +
Two basis material sinograms
Two basis material density maps
70keV 50keV 120keV
Synthesized monoE images
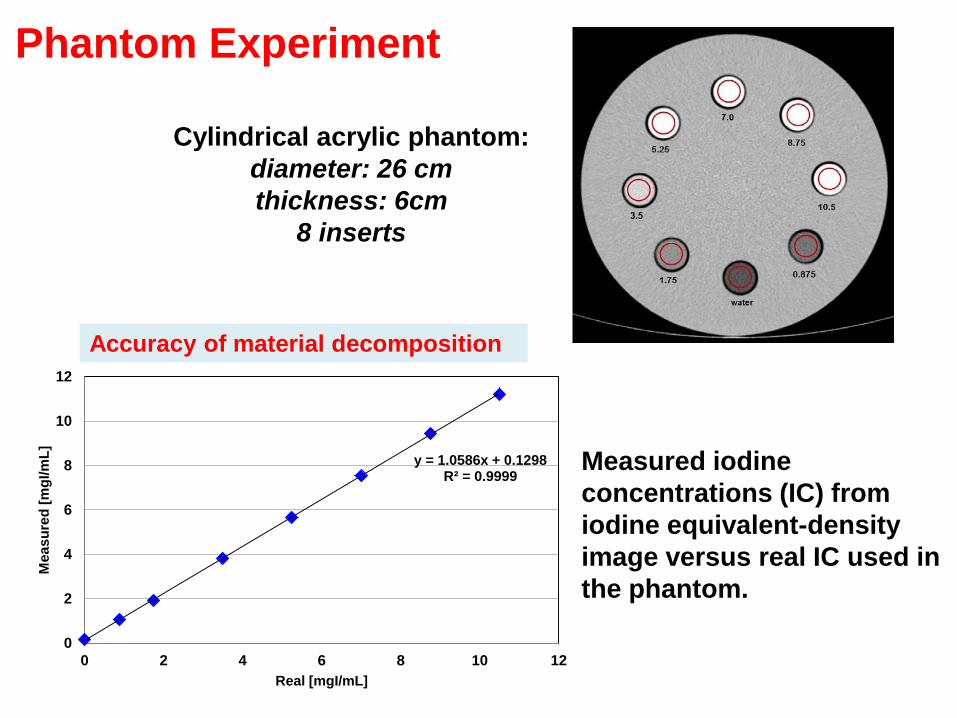
Cylindrical acrylic phantom: diameter: 26 cm thickness: 6cm
8 inserts
Measured iodine concentrations (IC) from iodine equivalent-density image versus real IC used in the phantom.
Phantom Experiment
y = 1.0586x + 0.1298 R² = 0.9999
0
2
4
6
8
10
12
0 2 4 6 8 10 12
Mea
sure
d [m
gI/m
L]
Real [mgI/mL]
Accuracy of material decomposition
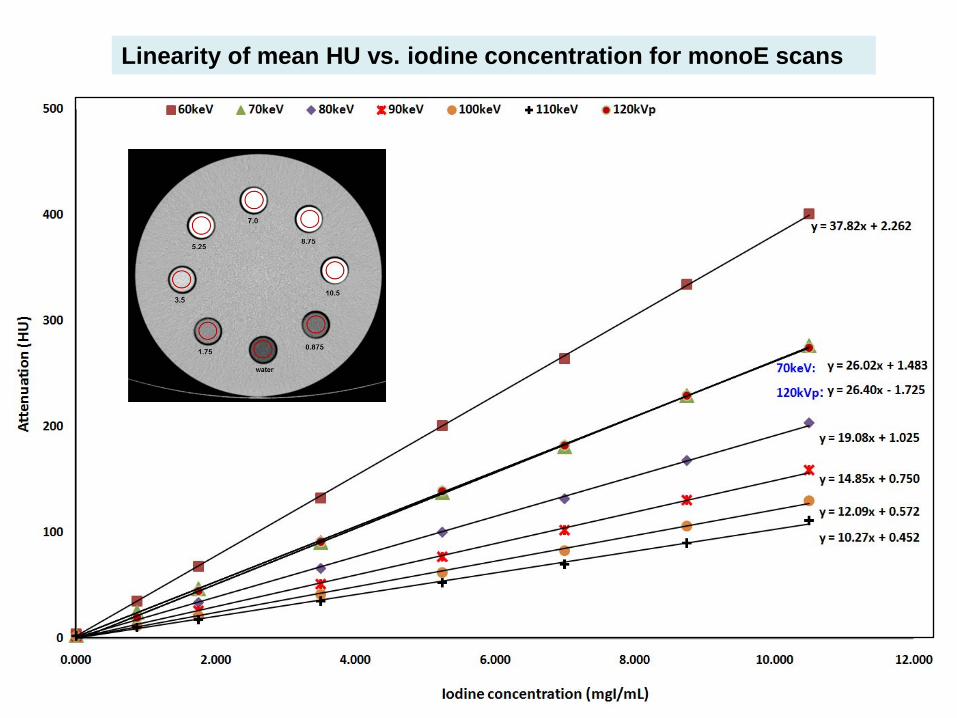
Linearity of mean HU vs. iodine concentration for monoE scans
-40
-20
0
20
40
60 70 80 90 100 110 120 120kVp
BHA
(HU
)
keV
conventional monoE
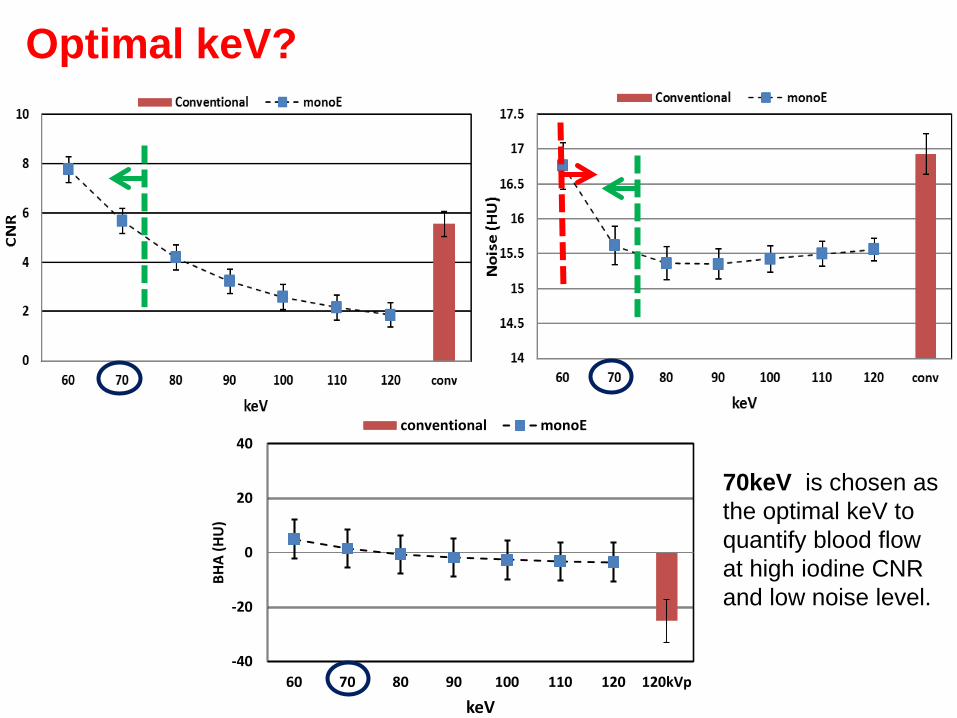
Optimal keV?
70keV is chosen as the optimal keV to quantify blood flow at high iodine CNR and low noise level.
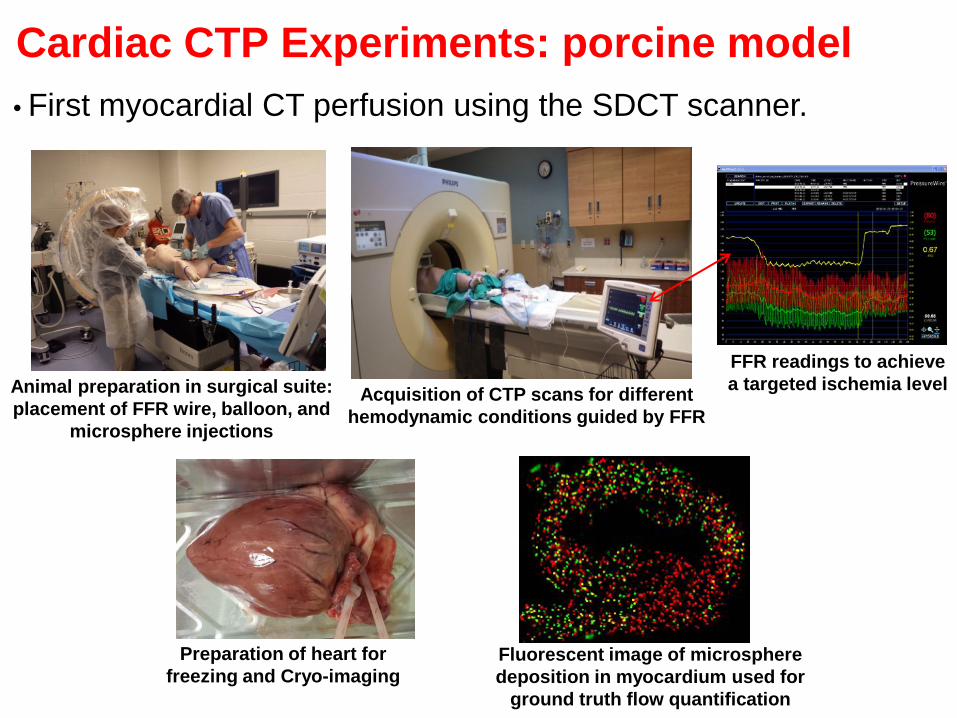
Cardiac CTP Experiments: porcine model
Animal preparation in surgical suite: placement of FFR wire, balloon, and
microsphere injections
Acquisition of CTP scans for different hemodynamic conditions guided by FFR
Fluorescent image of microsphere deposition in myocardium used for
ground truth flow quantification
FFR readings to achieve a targeted ischemia level
Preparation of heart for freezing and Cryo-imaging
• First myocardial CT perfusion using the SDCT scanner.
Imaging Protocol
11
• Prospective ECG-triggered scans at end systole (45% R-R). • Tube Voltage: 120kVp; Tube Current: 100mAs. • Full 360 degree scan coverage. • Omnipaque 350 followed by saline flush (20 mL @ 5 mL/sec). • Initiate scan 3-4sec post injection, and acquire every heart beat a total of
30-35 volumetric scans (< 25sec) with respirator off. • Scan under different hemodynamic conditions, with >15min between
consecutive scans.
• Conventional and monoE reconstructions of 2mm thick slices with no overlap. • Motion correction using a cubic B-spline deformable registration model. • Average CT map generation from registered scans. • Semi-automatic segmentation of LV myocardium using averaged CT volume. • Propagate segmentation results to entire 4D sequence. • Model-independent deconvolution method based on bSVD with Tikhonov
regularization to quantify myocardial blood flow (MBF).
Recons and Preprocessing
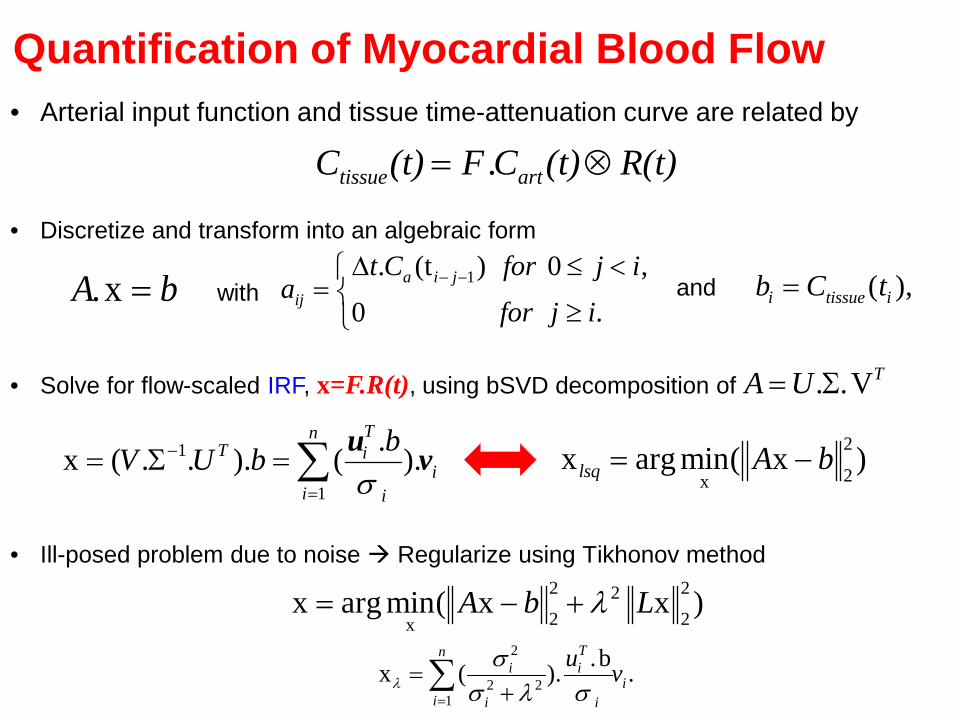
tissue artC (t) F .C (t) R(t)= ⊗• Arterial input function and tissue time-attenuation curve are related by
Quantification of Myocardial Blood Flow
• Ill-posed problem due to noise Regularize using Tikhonov method 2 222 2x
x arg min( x x )A b Lλ= − +2
2 21
.bx ( ). .Tn
i ii
i i i
u vλσ
σ λ σ=
=+∑
• Solve for flow-scaled IRF, x=F.R(t), using bSVD decomposition of
1
1
.x ( . . ). ( ).Tn
T ii
i i
bV U bσ
−
=
= Σ = ∑ u v 2
2xx arg min( x )lsq A b= −
. .VTA U= Σ
• Discretize and transform into an algebraic form
.xA b= 1. (t ) 0 ,0 .
a i jij
t C for j ia
for j i− −∆ ≤ <
= ≥
( ),i tissue ib C t=with and
log xA b−
optλ
Less filtering
More filtering
log L x
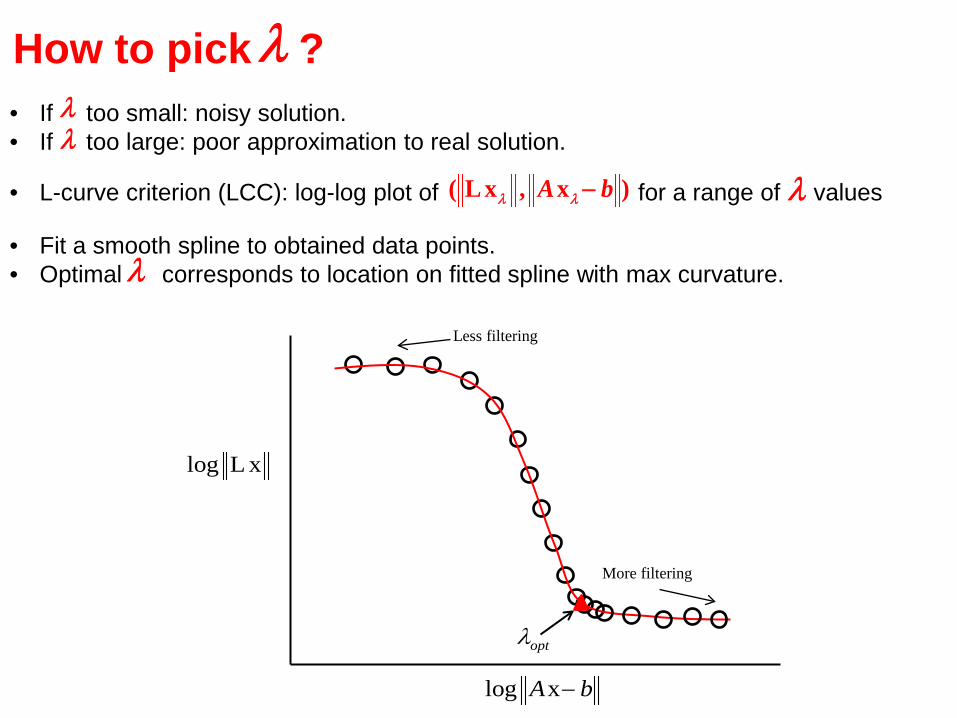
How to pick ? λ
• L-curve criterion (LCC): log-log plot of for a range of values ( L x , x )A bλ λ − λ
• Fit a smooth spline to obtained data points. • Optimal corresponds to location on fitted spline with max curvature. λ
• If too small: noisy solution. • If too large: poor approximation to real solution.
λλ
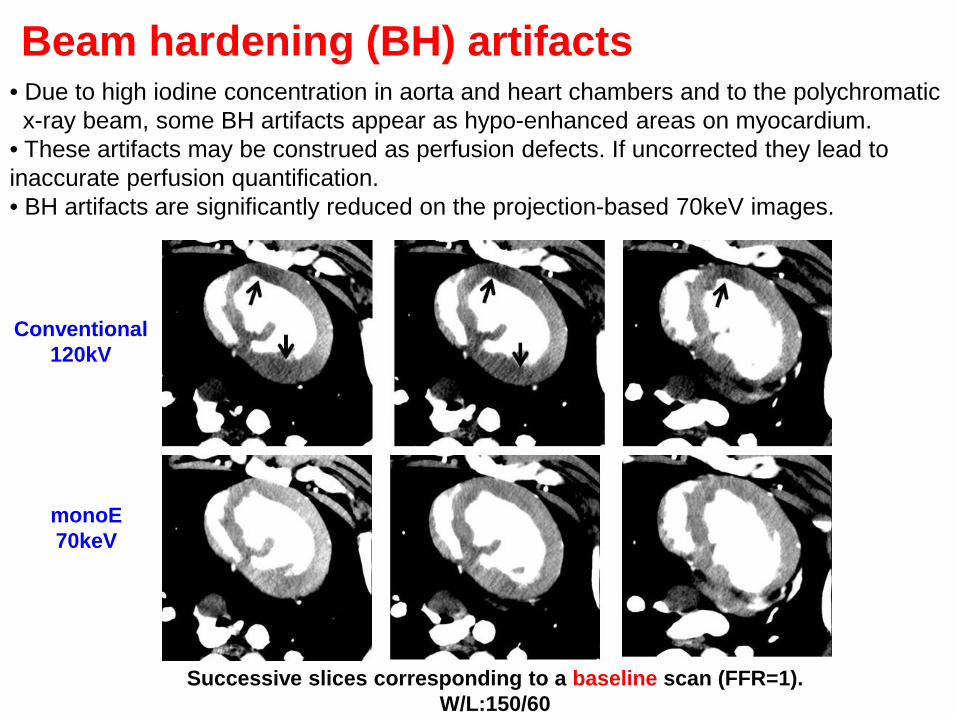
• Due to high iodine concentration in aorta and heart chambers and to the polychromatic x-ray beam, some BH artifacts appear as hypo-enhanced areas on myocardium. • These artifacts may be construed as perfusion defects. If uncorrected they lead to inaccurate perfusion quantification. • BH artifacts are significantly reduced on the projection-based 70keV images.
Beam hardening (BH) artifacts
Successive slices corresponding to a baseline scan (FFR=1). W/L:150/60
Conventional 120kV
monoE 70keV
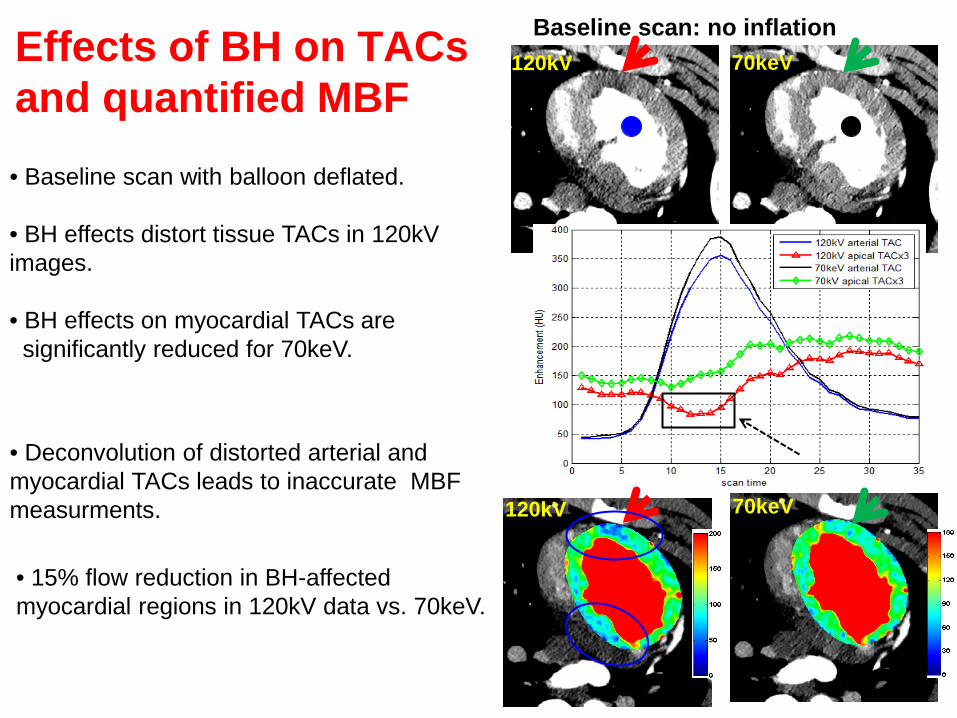
Baseline scan: no inflation
• Baseline scan with balloon deflated.
• Deconvolution of distorted arterial and myocardial TACs leads to inaccurate MBF measurments.
Effects of BH on TACs and quantified MBF
120kV 70keV
120kV 70keV
• 15% flow reduction in BH-affected myocardial regions in 120kV data vs. 70keV.
• BH effects distort tissue TACs in 120kV images. • BH effects on myocardial TACs are significantly reduced for 70keV.
0
20
40
60
80
100
120
Antero-septal Inferior Lateral Anterior
MB
F (m
l/min
/100
g)
Myocardial wall
120 kVp
0
20
40
60
80
100
120
Antero-septal Inferior Lateral Anterior
MB
F (m
l/min
/100
g)
Myocardial wall
70 keV
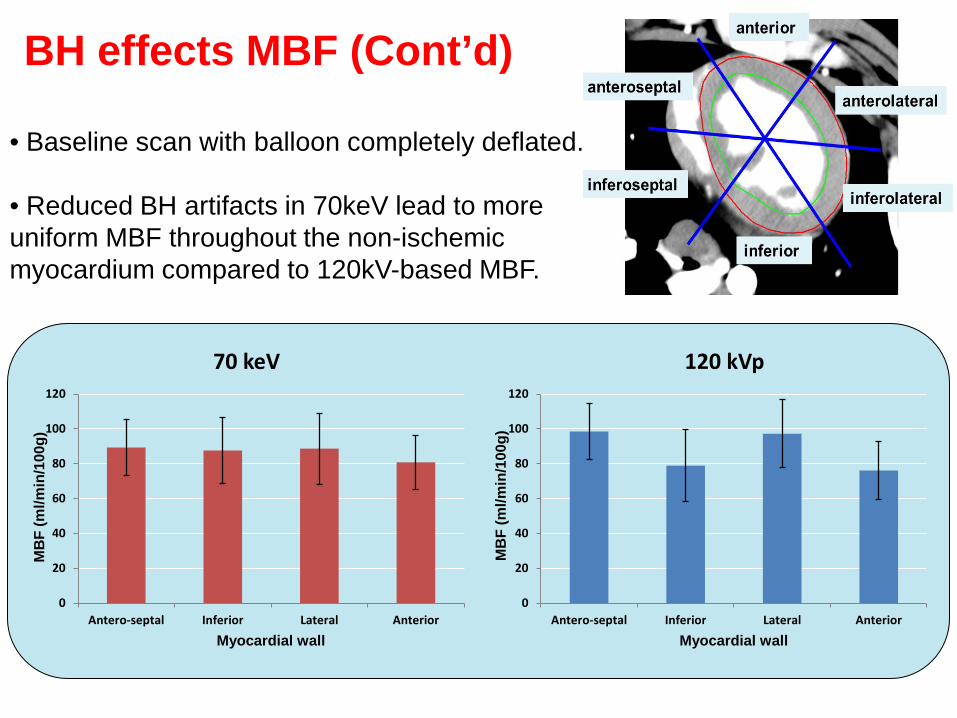
• Baseline scan with balloon completely deflated.
• Reduced BH artifacts in 70keV lead to more uniform MBF throughout the non-ischemic myocardium compared to 120kV-based MBF.
BH effects MBF (Cont’d)
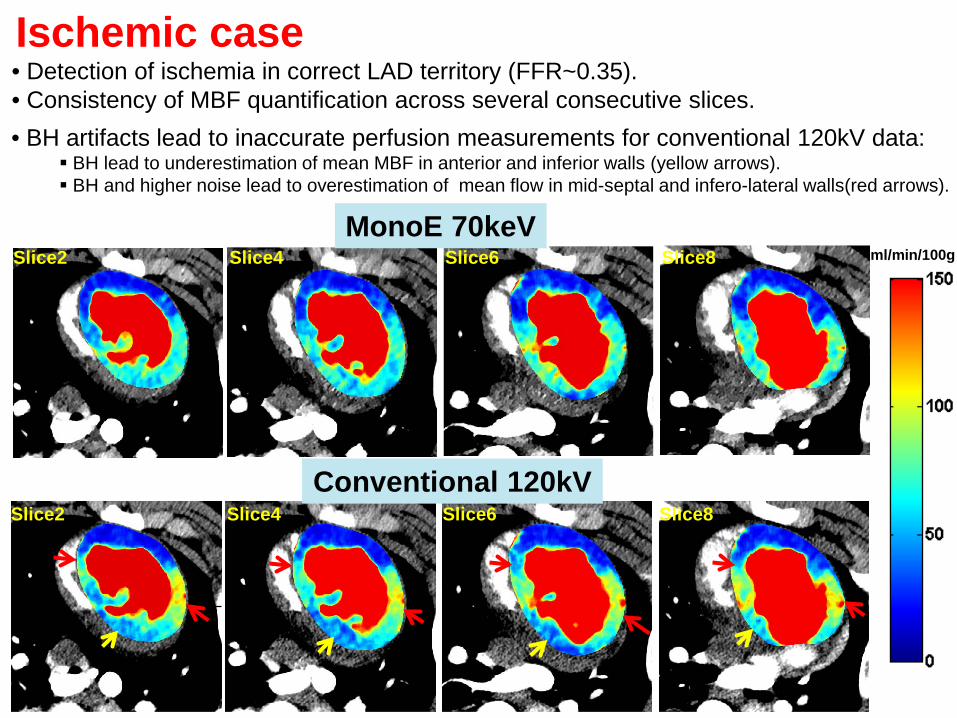
• Detection of ischemia in correct LAD territory (FFR~0.35). • Consistency of MBF quantification across several consecutive slices. • BH artifacts lead to inaccurate perfusion measurements for conventional 120kV data:
BH lead to underestimation of mean MBF in anterior and inferior walls (yellow arrows). BH and higher noise lead to overestimation of mean flow in mid-septal and infero-lateral walls(red arrows).
MonoE 70keV
Conventional 120kV
Slice2 Slice8 Slice6 Slice4 ml/min/100g
Ischemic case
Slice2 Slice8 Slice6 Slice4
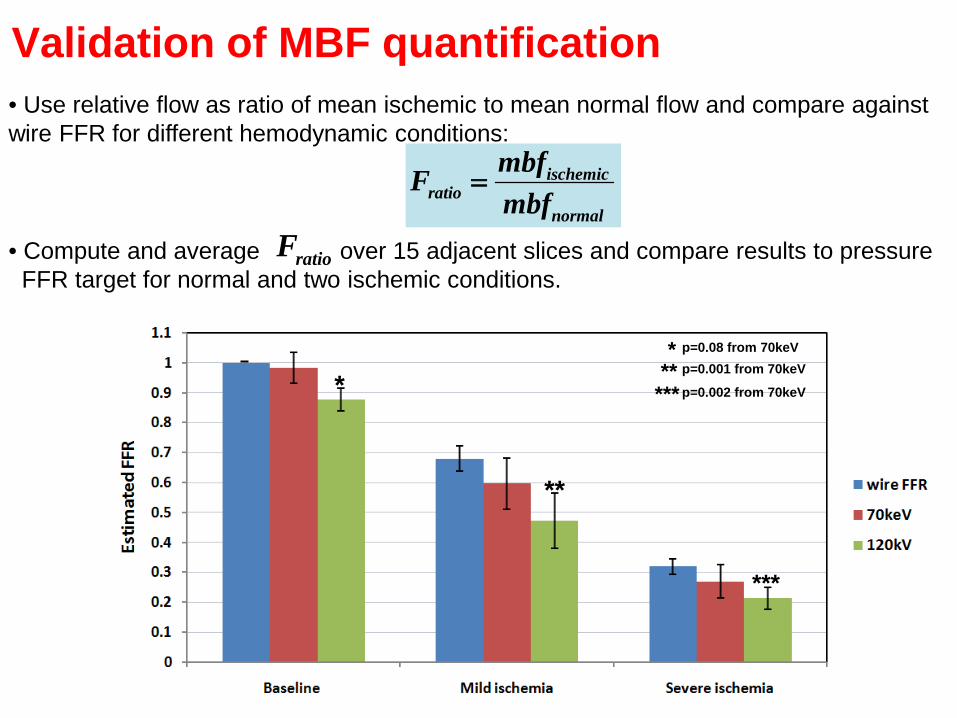
ischemicratio
normal
mbfFmbf
=
Validation of MBF quantification • Use relative flow as ratio of mean ischemic to mean normal flow and compare against wire FFR for different hemodynamic conditions:
*
**
***
p=0.001 from 70keV
p=0.002 from 70keV
p=0.08 from 70keV *
*** **
• Compute and average over 15 adjacent slices and compare results to pressure FFR target for normal and two ischemic conditions.
ratioF
Summary
• We reported the first dynamic CT perfusion findings using a novel
percutaneous porcine model and Philips’s SDCT scanner.
• Simultaneous acquisitions of LE & HE data permits synthesis of projection-based monoE images relatively free of BH artifacts.
• A phantom experiment designed to analyze sensitivity of iodine detection for monoE images vs. conventional single energy CT.
• 70keV chosen as the optimal energy for myocardial CTP assessment. • Designed a comprehensive processing tools for quantitative myocardial CTP.
• Compared to conventional SECT, 70keV-based flow less affected by BH and
corresponding relative flow correlates better with pressure FFR values.
• Ongoing work: • Additional animal studies. • CTP validation against microspheres-based measurements.
Acknowledgments
Biomedical Imaging Lab Hao Wu
Radiology Scott Esposito Philips Healthcare
Tsvi Katchalski, PhD (Haifa, Israel) Steve Utrup (Cleveland, OH)
Funding Ohio Third Frontier research grant from the state of Ohio to CWRU, Univ. Hospitals and Philips Healthcare, OH.
Surgery Steve Schomisch, PhD Cassandra Cipriano
Cardiovascular CORE Lab Xiaorong Zhou, MD Kashif Shaikh, MD
THANK YOU
QUESTIONS





























