Embed Size (px)
Citation preview
1405
Spectrum of Lateral Medullary SyndromeCorrelation Between Clinical Findings and Magnetic
Resonance Imaging in 33 Subjects
Jong S. Kim, MD; Jay H. Lee, MD; Dae C. Suh, MD; Myoung C. Lee, MD
Background and Purpose Computed tomography is insuffi-cient in evaluation of medullary lesions. Although lateralmedullary infarction is a relatively common type of cere-brovascular disease, detailed correlation between clinical find-ings and magnetic resonance imaging (MRI) has not yet beenreported.
Methods We studied 33 consecutive patients with lateralmedullary infarction who showed appropriate MRI lesionsand correlated their clinical findings with the MRI results.
Results Gait ataxia (88%), vertigo/dizziness (91%), nausea/vomiting (73%), dysphagia (61%), hoarseness (55%), Hornersign (73%), and facial (85%) and hemibody (94%) sensorychanges were frequent clinical findings. MRI results showedthat the lesions located in the rostral part of the medulla wereusually diagonal band-shaped and were associated with more
Computed tomography (CT) usually fails to identifymedullary vascular lesions. With the advent ofmagnetic resonance imaging (MRI), brain stem
ischemic strokes can be more definitively evaluated.1-2
Ross et al3 found MRI-identified lesions in their 4 patientswith lateral medullary syndrome (LMS), and Bogouss-lavsky et al4 described 6 patients who had small verte-brobasilar territory infarcts with good clinical-MRI corre-lation. Recently Sacco et al5 analyzed 33 patients withLMS and described the MRI findings as abnormal in 20 of22 patients in whom MRI was performed. However, theyfailed to correlate the diverse clinical manifestations withMRI findings, and a detailed clinical-MRI correlationstudy remains to be reported. In the present study wedescribe 33 patients with LMS in whom MRI showedappropriate lesions and attempt to correlate their clinicalfindings with the results of MRI.
Subjects and MethodsAt Asan Medical Center (Seoul, South Korea), MRI scan
was performed in 37 patients with clinically suspected LMSfrom June 1990 to December 1993. In this anatomicoclinicalcorrelation study, 4 patients were excluded: 2 with equivocallesions, 1 with additional pontine lesions, and 1 with bilateralmedullary lesions. The remaining 33 patients showed unilat-eral lesions mainly involving the dorsolateral portion of themedulla oblongata. Some patients with lesions extending be-
Received January 4, 1994; final revision received March 10,1994; accepted March 25, 1994.
From the Departments of Neurology (J.S.K, J.H.L., M.C.L.)and Radiology (D.C.S.), University of Ulsan, Asan Medical Cen-ter, Seoul, South Korea.
Correspondence to Jong S. Kim, MD, Department of Neurol-ogy, Asan Medical Center, Song-Pa PO Box 145, Seoul 134-600,South Korea.
O 1994 American Heart Association, Inc.
severe dysphagia, hoarseness, and the presence of facialparesis, whereas the caudal lesions, situated usually in thelateral surface of the medulla, appeared to correlate with moremarked vertigo, nystagmus, and gait ataxia. Nausea/vomitingand Horner sign were common regardless of the lesion loca-tion, and lesions extending ventromedially correlated withfacial sensory change on the contralateral side of the lesion.
Conclusions Analysis of MRI findings in rostrocaudal anddorsoventral aspects allows us, although not unequivocally, tomake anatomicoclinical correlations in the evaluation of pa-tients with lateral medullary stroke syndrome. (Stroke. 1994;25:1405-1410.)
Key Words • cerebral infarction • lateral medullarysyndrome • magnetic resonance imaging • strokeassessment
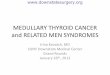
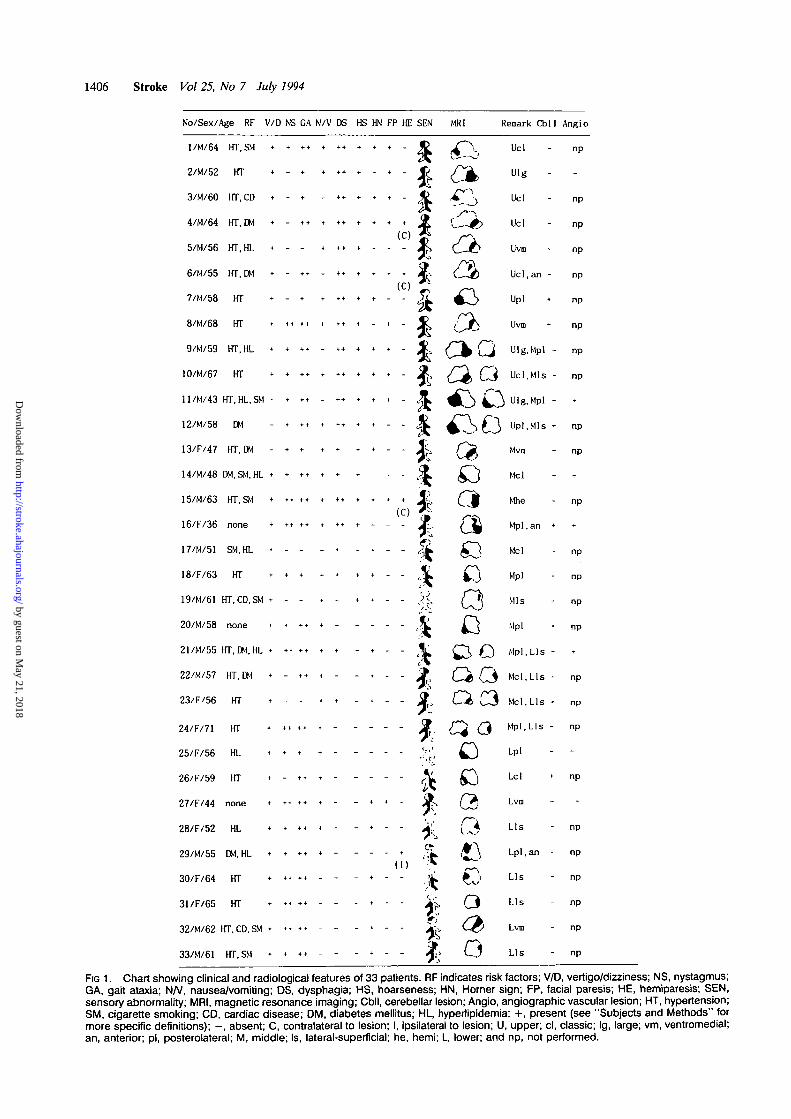
yond the dorsolateral portion were included. The 33 patientscomprised 22 men and 11 women (age range, 36 to 71 years[mean, 59 years]). Risk factors for stroke included hyperten-sion in 24, hyperlipidemia in 9, diabetes mellitus in 8, cigarettesmoking in 8, and cardiac disease in 3. No significant riskfactors were identified in 3 patients. All patients except 2 wereexamined within 5 days after the onset of stroke. Their mainclinical symptoms and signs were evaluated as follows: vertigo/dizziness: — (absent), -I- (present); nystagmus: — (absent), +(present on extreme gaze), ++ (present on forward gaze); gaitataxia: - (absent), + (present but able to walk), + + (unableto walk); nausea/vomiting: - (absent), + (present); dysphagia:- (absent), + (mildly present), ++ (needs nasogastric tubefor feeding); hoarseness: - (absent), + (present); Hornersign: — (absent), + (present); facial palsy: — (absent), +(present); hemiparesis: - (absent), + (present); and sensorydysfunction (depicted in Fig 1).
MRI studies were performed using a 1.5-T superconductingmagnet (GE). Axial T2 (repetition time [TR], 2500 millisec-onds; echo time [TE], 80 milliseconds) scan was performed inhorizontal plane at 5- or 6-mm intervals from the medulla tothe midbrain. T,-weighted (TR, 600 milliseconds; TE, 20milliseconds) axial and sagittal images were also obtained.Coronal sections were done in two cases. Evaluation of thelesions generally depended on T2-weighted axial cuts of themedulla, which are imaged at three different levels*: the uppermedulla, characterized by posterolateral bulging of the resti-form body (Fig 2, top left panel); the middle medulla, charac-terized by nodular lateral surface due to the olivary nucleus(Fig 2, top right panel); and the lower medulla, characterizedby a relatively round figure with closed fourth ventricle (Fig 2,bottom left panel). The patients' MRI findings were evaluatedin rostrocaudal and dorsoventral aspects.
Results
Neurological Symptoms and Signs
The patients' neurological symptoms and signs aresummarized in Fig 1. Vertigo/dizziness (30 [91%]), gait
by guest on May 21, 2018
http://stroke.ahajournals.org/D
ownloaded from
1406 Stroke Vol 25, No 7 July 1994
No/Sex/Age RF V/D NS GA N/V DS HS HN FP HE SEN MR1 Remark Cbll Angio
l/M/64 HT.SM + + ++ + + + + «• + - J£ i^1'- Ucl " "P
2/M/52 HT + - + + + + • - + - © / j ^ i U 1 8
3/M/60 HT.CD + - + - + + + + + - < ? ^T\ Ucl " n P
4/M/64 HT.DM + - ++ + ++ t + • • Jj (---<•> Ucl - np<C) 5 /^k5/M/56 HT, HL + - - + *•+ + + + - * , C - £ > Uvm - np
6/M/55 HT.DM * - ** - ** * * * * X - (.„£> Ucl, an - np
7/M/58 HT + - + + •+ + + - - 5? ^ 3 Upl + np
8/M/68 HT + +• ++ + ++ + - + - jC {\JD Uvm * "P
9/M/59 HT.HL • + ++ - ++ + * • - 2L £ ^ Q Ulg.Mpl - np
10/M/67 HT + + t+ + +* + + + . * ^ / ^ Q Ucl.Mis - np
l l / M / 4 3 H T . H L . S M - • • • - + * + t + -
1 2 / M / 5 8 D M - * + + * * * * * " "
13/F/47 HT.DM - + + * * * + - - X > { ^ Mvm - np
14/M/48 DM.SM.HL + * ++ * * * - - - ,3L £ ) Mel - -
15/M/63 HT.SM + ++ ++ + *+ + + + * jE, ( f l Mhe - np(C) g ^
1 6 / F / 3 6 n o n e + + • + + + + + + - - . j ? _ . / ^ M p l . a n * *
17/M/51 SM.HL * - - - * - • - - ,|k ,O Mel - np
18/F/63 H T + + + + + + * - - jL £ ) Mpl - np
19/M/61 HT.CD.SM * - - * - + • - - }<, Q^l Mis - np
20/M/58 none • • + • + - . . . . f|t £_J Mpl . np
21/M/55 HT, DM.HL + + • + + + + - • - - ^ C^ (Q Mpl.Lls -
22/M/57 HT.DM + - ** * - - • - - ^ O (3 Mcl.Lls- np
23/F/56 HT t ... t .... 9 Ci C3 Mcl.Lls - np
24/F/71 HT + ++ • + • - - - - - J J ^ (^ Mpl.Lls - np
25/F/56 HL • • • + - - - - - V ^ J Lpl
26/F/59 HT + - * • + - . - - - ^ ^ \ Lcl + np
27/F/44 none + ++ ++ + - - * * - & Q, Lvm
28/F/52 HL + + + * * - - + - - £ . { ̂ Lls - np
2 9 / M / 5 5 DM.HL • • • • + - - - - • "k. , * \ Lpl . an - np
( I ) > ^3 0 / F / 6 4 HT • * » « - - - + - - i . £J L l s - n p
3 1 / F / 6 5 HT * +< ** - - - * - - i } > . O L l s - n p
3 2 / M / 6 2 HT. CD. SM • • • • • - - - * - - jL €£> Lvm - np
3 3 / M / 6 1 H T . S M • + • + - - - + - - J^> L j L l s - n p
FIG 1. Chart showing clinical and radiological features of 33 patients. RF indicates risk factors; V/D, vertigo/dizziness; NS, nystagmus;GA, gait ataxia; UN, nausea/vomiting; DS, dysphagia; HS, hoarseness; HN, Homer sign; FP, facial paresis; HE, hemiparesis; SEN,sensory abnormality; MRI, magnetic resonance imaging; Cbll, cerebeliar lesion; Angio, angiographic vascular lesion; HT, hypertension;SM, cigarette smoking; CD, cardiac disease; DM, diabetes mellitus; HL, hyperlipidemia; +, present (see "Subjects and Methods" formore specific definitions); - , absent; C, contralateral to lesion; I, ipsilateral to lesion; U, upper; cl, classic; Ig, large; vm, ventromedial;an, anterior; pi, posterolateral; M, middle; Is, lateral-superficial; he, hemi; L, lower; and np, not performed.
by guest on May 21, 2018
http://stroke.ahajournals.org/D
ownloaded from

Kim et al Lateral Medullary Syndrome and MRI 1407
ataxia (29 [88%]), nausea/vomiting (24 [73%]), nystag-mus (22 [67%]), Horner sign (24 [73%]), dysphagia (20[61%]), hoarseness (18 [55%]), and facial (28 [85%])and hemibody (31 [94%]) sensory changes were fre-quent clinical manifestations. Mild facial paresis of thecentral type on the side ipsilateral to the lesion was seenin 12 patients (36%), and 4 had mild hemiparesis, 1 onthe side ipsilateral to the lesion. Although facial sensorychange ipsilateral to the lesion was usual, 9 patientsshowed facial sensory dysfunction on the side contra-lateral to the lesion, and 1 had bilateral facial sensoryabnormalities. In 4 patients facial sensory change wasrestricted to the ophthalmic division of trigeminal (VI)area, and in 2 there was no facial sensory change. In 2patients there was no definite sensory dysfunction ineither the face or the body.
Imaging and Vascular StudiesEight patients had lesions in the upper medulla, 8 in
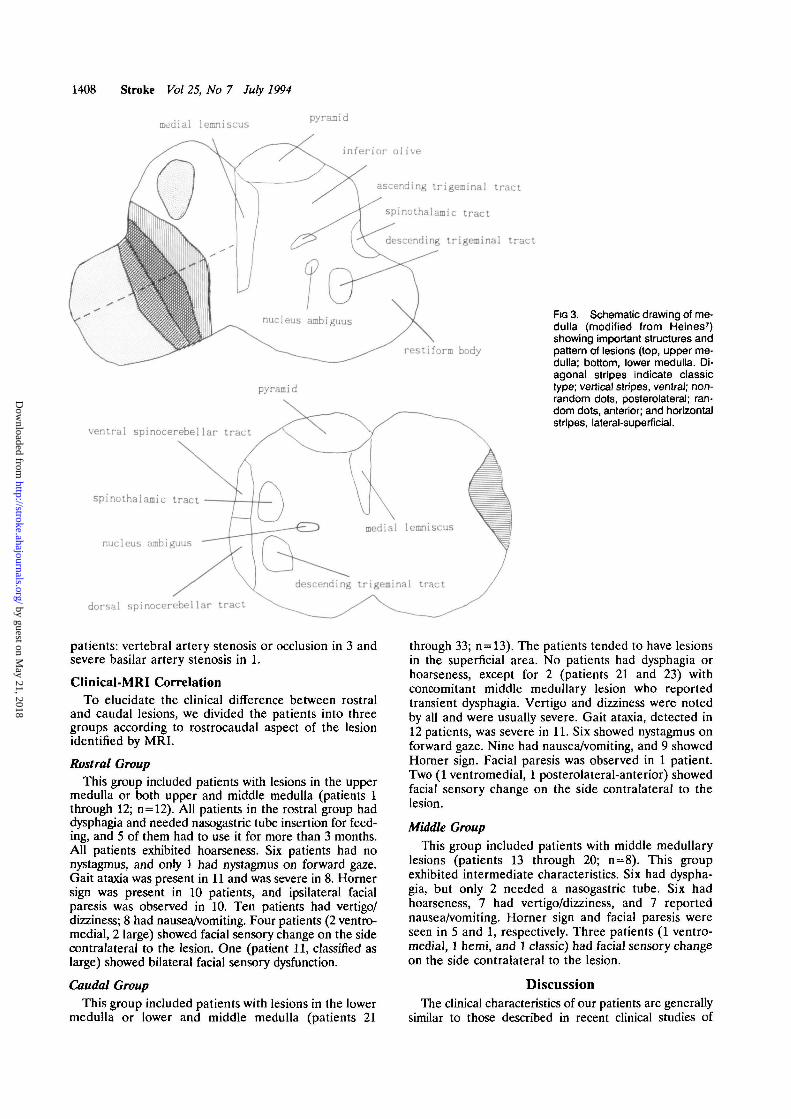
the middle medulla, and 9 in the lower medulla. Fourhad lesions in the upper and middle medulla, and 4 inthe middle and lower medulla. The lesions in the upperand the middle medulla were usually diagonal band-shaped and situated in the posterolateral portion of themedulla. Diagonal band-shaped lesions sparing themost posterolateral portion were most common andtherefore classified as the classic type (Fig 3, top panel).Diagonal band-shaped lesions situated more ventrome-dially were classified as the ventromedial type (Fig 3,top panel), which was defined when the center of thelesion was located inside the medial half of a line drawnas in Fig 3, top panel. Lesions encompassing the mostposterolateral surface of the medulla were designated
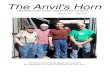
Fra 2. Magnetic resonance Imaging showing characteristics ofmedulla: upper medulla (top left), middle medulla (top right), andlower medulla (bottom left).
as posterolateral. However, a few lesions were largeenough to encompass the ventromedial and posterolat-eral part of the medulla and were designated as large. Insome patients (usually those with lower medullary le-sions), the lesions were located in the lateral surface ofthe medulla and were classified as the lateral-superficialtype (Fig 3, bottom panel). In a few patients, additionalor extended lesions were seen in the anterior half of themedulla; these were classified as anterior and hemitypes, respectively. This classification was made by oneof the authors, who was blind to the patients' clinicalfindings.
Twelve patients showed lesions in the upper medulla(4 of them had concomitant middle medullary lesions).Generally, the lesions in the upper medulla were thickand diagonal band-shaped. They were classified asclassic in 4, classic and anterior in 1, ventromedial in 2,large in 3, and posterolateral in 2. Sixteen had lesions inthe middle medulla (4 had lesions in the upper medullaand 4 had lesions in the lower medulla concomitantly).Lesions were classified as classic in 4, ventromedial in 1,posterolateral in 6, posterolateral and anterior in 1,hemi in 1, and lateral-superficial in 3. Thirteen hadlesions in the lower medulla. The lesions were mostoften located superficially: lateral-superficial in 8, pos-terolateral in 1, posterolateral and anterior in 1, classicin 1, and ventromedial in 2.
In addition to the medullary lesions, 7 patientsshowed infarcts in the cerebellum. Fourteen had CTscan before MRI examination, which universally failedto localize medullary lesions but detected concomitantcerebellar infarcts in 3 patients. Seven patients hadangiography, which showed vascular abnormalities in 4
by guest on May 21, 2018
http://stroke.ahajournals.org/D
ownloaded from
1408 Stroke Vol 25, No 7 July 1994
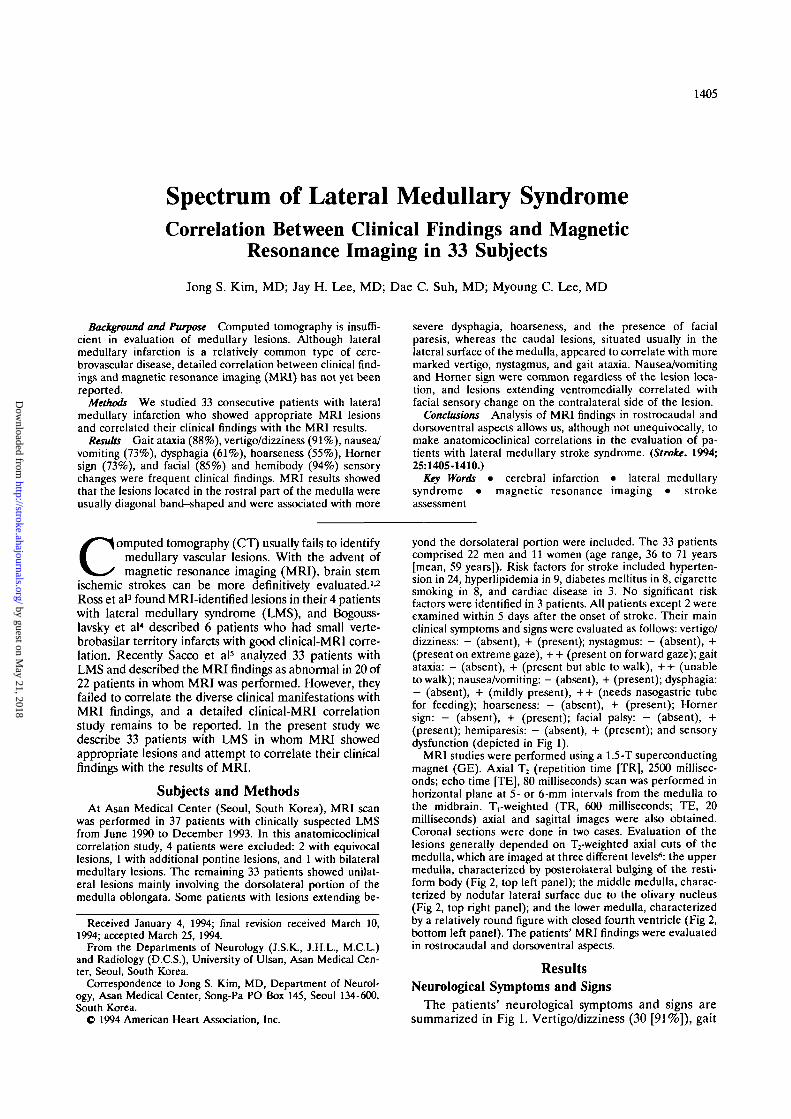
medial lemniscuspyramid
inferior olive
ascending trigeminal tract
spinothalamic tract
descending trigeminal tract
restiform body
pyramid
ventral spinocerebellar tract
spinothalamic tract
nucleus ambiguus
dorsal spinocerebellar tract
descending trigeminal tract
Fra 3. Schematic drawing of me-dulla (modified from Heines7)showing important structures andpattern of lesions (top, upper me-dulla; bottom, lower medulla. Di-agonal stripes Indicate classictype; vertical stripes, ventral; non-random dots, posterolateral; ran-dom dots, anterior; and horizontalstripes, lateral-superficial.
patients: vertebral artery stenosis or occlusion in 3 andsevere basilar artery stenosis in 1.
Clinical-MRI CorrelationTo elucidate the clinical difference between rostral
and caudal lesions, we divided the patients into threegroups according to rostrocaudal aspect of the lesionidentified by MRI.
Rostral GroupThis group included patients with lesions in the upper
medulla or both upper and middle medulla (patients 1through 12; n=12). All patients in the rostral group haddysphagia and needed nasogastric tube insertion for feed-ing, and 5 of them had to use it for more than 3 months.All patients exhibited hoarseness. Six patients had nonystagmus, and only 1 had nystagmus on forward gaze.Gait ataxia was present in 11 and was severe in 8. Homersign was present in 10 patients, and ipsilateral facialparesis was observed in 10. Ten patients had vertigo/dizziness; 8 had nauseaA'omiting. Four patients (2 ventro-medial, 2 large) showed facial sensory change on the sidecontralateral to the lesion. One (patient 11, classified aslarge) showed bilateral facial sensory dysfunction.
Caudal GroupThis group included patients with lesions in the lower
medulla or lower and middle medulla (patients 21
through 33; n = 13). The patients tended to have lesionsin the superficial area. No patients had dysphagia orhoarseness, except for 2 (patients 21 and 23) withconcomitant middle medullary lesion who reportedtransient dysphagia. Vertigo and dizziness were notedby aU and were usually severe. Gait ataxia, detected in12 patients, was severe in 11. Six showed nystagmus onforward gaze. Nine had nauseaA'omiting, and 9 showedHorner sign. Facial paresis was observed in 1 patient.Two (1 ventromedial, 1 posterolateral-anterior) showedfacial sensory change on the side contralateral to thelesion.
Middle GroupThis group included patients with middle medullary
lesions (patients 13 through 20; n=8). This groupexhibited intermediate characteristics. Six had dyspha-gia, but only 2 needed a nasogastric tube. Six hadhoarseness, 7 had vertigo/dizziness, and 7 reportednauseaA'omiting. Homer sign and facial paresis wereseen in 5 and 1, respectively. Three patients (1 ventro-medial, 1 hemi, and 1 classic) had facial sensory changeon the side contralateral to the lesion.
DiscussionThe clinical characteristics of our patients are generally
similar to those described in recent clinical studies of
by guest on May 21, 2018
http://stroke.ahajournals.org/D
ownloaded from

Kim et al Lateral Medullary Syndrome and MRI 1409
LMS.5'8 In our study we attempted to correlate the clinicalmanifestations with MRI results. Although it is difficult toclassify the various lesions satisfactorily, we attempted todivide the cases with reference to the rostrocaudal aspectsto elucidate possible clinical difference.
The most distinguishing rostrocaudal symptomatic dif-ference was dysphagia, which was distinctly more severe inthe rostral group than in the caudal group. Patients withmiddle medullary lesions showed an intermediate degreeof severity. The different degrees of severity of dysphagiamay be explained in several ways. Dysphagia in medullarystroke is caused by involvement of the nucleus ambiguus,a vertical columnar structure extending to the level ofpyramidal decussation.7 This structure, seen in the middleportion of the medulla (Fig 3), may have been morefrequently involved in the rostral group because lesions inthis group were generally thick and tended to involve theventral portion of the medulla. The lesions of the caudalgroup usually involved the superficial area and may havespared the more medially located nucleus ambiguus. How-ever, patients with deep lesions in the caudal group(patients 27 and 32) also showed no dysphagia. Possiblyonly a caudal part of the nucleus ambiguus, a portion notdirectly related with visceral efferent fibers,9 may havebeen involved in this group. Whatever the actual explana-tion, caudal group patients have a more benign prognosisin terms of aspiration. As expected, hoarseness, anothersymptom related to nucleus ambiguus involvement, wasalso more marked in the rostral group than in the caudalgroup.
Nystagmus, gait ataxia, and vertigo/dizziness wereapparently more severe in patients in the caudal group,although the latter symptoms were not objectivelygraded in this study. Nystagmus in LMS is attributed toinvolvement of the vestibular nuclei or their connectionsto the cerebellum,911 which begin at the caudal part ofthe medial and inferior vestibular nuclei.9 A focal lesionin this area was reported to cause severe vestibulo-ocular symptoms.12 The vestibulocerebellar pathwayruns through the juxtarestiform body, a part of theinferior cerebellar peduncle, in the posterolateral me-dulla.9 These areas tended to be spared in the patientswith upper medullary lesions, among whom 6 of 8 didnot show nystagmus. Gait ataxia, a very common sign inour series, is attributed to involvement of either therestiform body or the spinocerebellar pathway.10'11 Inthe lower medulla, both of these structures are locatedin the lateral surface,7-9 which may have been frequentlyinvolved in patients in the caudal group (Fig 3, bottompanel). The involvement of the cerebellum, detected in7 patients, does not appear to augment the severity ofgait ataxia.
The neural substrate for nausea and vomiting, com-mon symptoms of LMS, is not clearly defined. WhereasPeterman and Siekert13 suggested that nausea andvomiting are attributed to lesions of the vestibularnuclei, Currier et al10 stated that these symptoms arerelated to involvement of the medullary vomiting cen-ter, which may be identical to the nucleus ambiguus. Inour series symptoms of nausea/vomiting were not spe-cifically associated with the presence of dysphagia ornystagmus. The neural substrate for these symptomsmay be related to both of the above structures. Hornersyndrome, a sign related to the descending sympathetic
pathways in the lateral reticular formation,10 is alsocommon in our series regardless of lesion location.
Although dissociated sensory abnormality seen inclassic LMS is usual in our series, 9 patients showedfacial sensory change on the side contralateral to thelesion. All had lesions involving the ventromedial oranterior part of the medulla (ventromedial in 4, large in2, hemi in 1, classic in 1, and posterolateral-anterior in1), which would involve the ascending trigeminal sen-sory tract located in the medial-ventral portion of themedulla679 (Fig 3, top panel). One patient (patient 11)had bilateral facial sensory change, probably because ofa wide lesion involving both the descending and ascend-ing trigeminal sensory tract.11 Two (patients 19 and 25)did not reveal any sensory abnormalities, probablybecause of sparing of the spinothalamic and trigeminalpathways. Three (patients 28, 30, and 31) showedhemihypesthesia without facial sensory change. Facialsensation was spared in 7 of 39 patients in the study ofCurrier et al,10 who suggested that the descendingtrigeminal sensory tract may be spared in ventrallysituated lesions. Our patients, however, had lateral-superficial lesions in the lower medulla, suggesting thatthe descending trigeminal tract located posteromedially(Fig 3, bottom panel) may have been spared. Four ofour patients had facial sensory change restricted to theVI area: 2 in the side ipsilateral and 2 in the sidecontralateral to the lesions. Because the VI area islocated most ventrally in the descending trigeminaltract, Currier et al10 thought that this sensory patternmay be associated with a ventrally located lesion. How-ever, the patients with ventromedial-type lesions did notreveal this type of sensory change in our series, and themechanism of restricted facial sensory deficit in patients7 and 17 remains unclear. Restricted sensory change ofthe VI area on the side contralateral to the lesion(patients 29 and 32) may be due to selective involvementof the lateral part of the ascending trigeminal tract,where the sensory fibers from the upper part of the faceare located.10
Facial paresis ipsilateral to the lesion was observed in12 patients (36%) in our series. Fisher and Tapia14
reported an autopsy-proven case of LMS associatedwith a severe peripheral type of facial paralysis, whichwas caused by extension of the lesion to the lower pons,involving intra-axial facial nerve fascicles. In our seriesno patients showed obvious lesions in the pons, and allhad a mild, usually transient facial paresis of the centraltype. Currier et al10 and Sacco et al5 noted weakness ofthe facial muscles in 51% and 42% of their patients,respectively, and suggested that aberrant, looping cor-ticobulbar fibers15 may have been involved in thesepatients. Most of our patients with facial paresis hadlesions in the rostral medulla, suggesting that the aber-rant fibers, if they exist, may not descend to the level ofthe lower medulla, although 1 patient (patient 27) witha caudal lesion of the ventromedial type also showedfacial paresis. Finally, 4 of our patients showed mildhemiparesis. All except 1 had lesions extending anteri-orly, suggesting that the corticospinal tract was involved.Of the 4,1 (patient 29) showed hemiparesis on the sideipsilateral to the lesion. In this patient a coronal cut ofthe MRI showed that the lesion extended into the uppercervical cord (Fig 4), which probably involved thepyramidal tract after decussation.
by guest on May 21, 2018
http://stroke.ahajournals.org/D
ownloaded from

1410 Stroke Vol 25, No 7 July 1994
FIG 4. Patient 29. TV-weighted coronal imaging showing lesioninvolving the upper cervical area lower than pyramidal decussatton.
In conclusion, our study illustrates that the clinicaland topographic spectra of LMS are diverse, and MRIanalysis in rostrocaudal and dorsoventral aspects allowsus, although not unequivocally, to make clinical-MRIcorrelations. Generally, the rostral lesions are diagonalband-shaped and correlate with severe dysphagia,hoarseness, and the presence of facial paresis, whereascaudal lesions, usually involving lateral superficial areas,appear to correlate with more marked nystagmus, ver-tigo, and gait ataxia. Nausea/vomiting and Horner signare common regardless of the lesion location. Lesionsextending ventromedially correlate with contralateralfacial sensory change, whereas anteriorly located le-sions are associated with hemiparesis.
References1. Lee BCP, Kneeland JB, Deck MDF, Cahill PT. Posterior fossa
lesion: magnetic resonance imaging. Radiology. 1984;153:137-143.2. Kistler JP, Buonanno FS, DeWitt LD, Davis KR, Bray TJ, Fisher
CM. Vertebra-basilar posterior cerebral territory stroke: delin-eation by proton nuclear magnetic resonance imaging. Stroke.1984;15:417-426.
3. Ross MA, Biller J, Adams HP, Dunn V. Magnetic resonanceimaging in Wallenberg's lateral medullary syndrome. Stroke. 1986;17:542-545.
4. Bogousslavsky J, Fox AJ, Barnett HJM, Hachinski VC, Vinitski S,Carey LS. Clinico-topographic correlation of small vertebrobasilarinfarct using magnetic resonance imaging. Stroke. 1986;17:929-938.
5. Sacco RL, Freddo L, Bello JA, Odel JG, Onesti ST, Mohr JP.Wallenberg's lateral medullary syndrome: clinical-magnetic res-onance imaging correlations. Arch NeuroL 1993;50:609-614.
6. Bradley WG Jr. MR of the brain stem: a practical approach.Radiology. 1991;179:319-332.
7. Heines DE. Neuwanatomy: An Atlas of Structures, Sections andSystems. 2nd ed. Berlin, Germany: Urban & Schwarzenberg;1987:78-91.
8. Norrving B, Cronqvist S. Lateral medullary infarction: prognosis inan unselected series. Neurology. 1991;41:244-248.
9. Carpenter MB, Sutin J. Human Neuroanatomy. 8th ed. Baltimore,Md: Williams & Wilkins Co; 1983:315-357.
10. Currier RD, Giles CL, DeJong RN. Some comments on Wal-lenberg's lateral medullary syndrome. Neurology. 1961;l:778-792.
11. Caplan LR, Pessin MS, Mohr JP. Vertebrobasilar occlusivedisease. In: Barnett HJM, Mohr JP, Stein BM, Yatsu FM, eds.Stroke: PathophysUAogy, Diagnosis, and Management. 2nd ed. NewYork, NY: Churchill Livingstone, Inc; 1992:443-515.
12. Grant G. Infarction localization in a case of Wallenberg's syn-drome: a neuroanatomical investigation with comments onstructures responsible for nystagmus. JHirnforsch. 1966;8:419-422.
13. Peterman AF, Siekert RG. The lateral medullary (Wallenberg)syndrome: clinical features and prognosis. Med Gin North Am.1960;ll:778-790.
14. Fisher CM, Tapia J. Lateral medullary infarction extending to thelower pons. / Neurol Neurosurg Psychiatry. 1987;50:620-624.
15. Kuypers HGJM. Cortico-bulbar connections to the pons and lowerbrainstem in man: an anatomical study. Bram. 1958;81:364-388. by guest on M
ay 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from

J S Kim, J H Lee, D C Suh and M C Leemagnetic resonance imaging in 33 subjects.
Spectrum of lateral medullary syndrome. Correlation between clinical findings and
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1994 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.25.7.1405
1994;25:1405-1410Stroke.
http://stroke.ahajournals.org/content/25/7/1405World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 21, 2018
http://stroke.ahajournals.org/D
ownloaded from