Embed Size (px)
Citation preview
Archives of Cardiovascular Disease (2016) 109, 143—149
Available online at
ScienceDirectwww.sciencedirect.com
REVIEW
Specifics of cardiac magnetic resonanceimaging in childrenSpécificités de l’IRM cardiaque en pédiatrie
Laurent Bonnemainsa,b,c,d,∗, Francesca Raimondie,Freddy Odilleb,c,f
a Department of Cardiac Surgery, CHU de Strasbourg, 67000 Strasbourg, Franceb U947, Inserm, 54000 Nancy, Francec IADI, University of Lorraine, 54000 Nancy, Franced University of Strasbourg, 67000 Strasbourg, Francee Department of Paediatric Cardiology, CHU Necker—Enfants-Malades, 75000 Paris, Francef CIC-IT 1433, Inserm, 54000 Nancy, France
Received 14 September 2015; received in revised form 16 November 2015; accepted 18 Novem-ber 2015Available online 14 January 2016
KEYWORDSMRI;Paediatrics;Heart
Summary This review points out three specific features of cardiac magnetic resonanceimaging (MRI) in children: the small size of the heart modifies the usual balance betweensignal-to-noise ratio and spatial resolution; the higher and more variable heart rate limits tissuecharacterization and temporal resolution; and motion artefacts (notably respiratory motions)must be dealt with. In the second part of this review, we present the current and future prac-
tices of cardiac magnetic resonance (CMR) in children, based on the experience of all Frenchpaediatric cardiac MRI centres.© 2015 Elsevier Masson SAS. All rights reserved.Abbreviations: 2D, two-dimensional; 3D, three-dimensional; BB, black blood; CMR, cardiac magnetic resonance; CT, computed tomogra-phy; ECG, electrocardiogram; GRICS, generalized reconstruction by inversion of coupled systems; LGE, late gadolinium enhancement; MRI,magnetic resonance imaging; Nex, number of excitations; SNR, signal-to-noise ratio; SPECT, single photon emission computed tomography;SSFP, steady-state free precession; TR, repetition time; TSE, turbo spin echo.
∗ Corresponding author at: Inserm U947, IADI, Tour Drouet, rue du Morvan, 54500 Vandœuvre-lès-Nancy, France.E-mail address: [email protected] (L. Bonnemains).
http://dx.doi.org/10.1016/j.acvd.2015.11.0041875-2136/© 2015 Elsevier Masson SAS. All rights reserved.

144 L. Bonnemains et al.
MOTS CLÉSIRM ;Pédiatrie ;Cœur
Résumé Cette revue met l’accent sur trois particularités de l’imagerie par résonance mag-nétique (IRM) cardiaque pédiatrique : la petite taille du cœur imagé induit une modificationde la balance habituelle entre rapport signal/bruit et résolution spatiale ; le rythme cardiaqueplus rapide et plus variable limite la caractérisation tissulaire et la résolution temporelle ;et les mouvements (notamment mouvement respiratoires) doivent être pris en compte. Dansune deuxième partie, nous présentons la pratique clinique actuelle et future en IRM cardiaquepédiatrique, présentation basée sur l’expérience des centres francais.© 2015 Elsevier Masson SAS. Tous droits réservés.
I
CeafitatCtiEbuaoCwC
S
TEC•
•
•
Hs
Satatcntii
atterlarwf
rwtkdresaocor
H
Ttrpapc(orcptar[
ntroduction
ardiac magnetic resonance (CMR) has developed consid-rably in the past few years. Hardware and sequencesre improving very fast. Higher and more homogeneouselds and stronger gradients allow theoretically higher spa-ial resolution. Parallel imaging and compressed sensingllow theoretically higher temporal resolution. All condi-ions seemed aligned to witness the advent of paediatricMR as one of the most promising available investigationools in paediatric cardiology [1]. However, paediatric CMRs part of routine clinical practice in only a few centres inurope. Its own intrinsic limitations and the need for dou-le specific cardiological and radiological expertise make itsse difficult in clinical practice. Most cardio-paediatriciansre not familiar with the concepts of CMR. The first partf this review aims at clarifying the specific features ofMR in the paediatric population. In the second part,e present the current and future practices of paediatricMR.
pecifics of paediatric CMR
hree specific features of paediatric CMR will be discussed.ach one is the direct consequence of technical aspects ofMR that encounter limits in children:the magnetic resonance signal is produced by the heart,and paediatric hearts are small;the magnetic resonance imaging (MRI) process is relativelyslow, and paediatric hearts beat rapidly;the acquisitions require absence of motion and breath-holding that children cannot comply with.
eart size and the relationship between voxelize and signal-to-noise ratio
ince paediatric hearts are much smaller than adult hearts, compromise between two solutions must be chosen. First,he boundaries of the field of view may be reduced todjust to the child’s anatomy. If the number of voxels ofhe image is preserved, this will result in a smaller voxelontaining fewer protons and ultimately a lower MRI sig-
al. Second, the spatial resolution of the image (size ofhe k-space matrix) may be reduced. This will result in lessnformative images. The consequence of the compromises that the images have a lower signal-to-noise ratio (SNR)w(wo
nd/or a lower spatial resolution. SNR is actually propor-ional to the product of the voxel dimensions. To counterhis, the acquired data can be averaged over multiplexcitations, with SNR being proportional to the squareoot of the number of excitations (Nex) [1]. For instance,et us consider imaging with a single excitation (Nex = 1)nd a voxel size set to 1 × 1 × 8 mm3; if the voxel size iseduced to 0.7 × 0.7 × 8 mm3, the same SNR will be obtainedith Nex = 4, which implies increasing the scan time four-
old.Another element that is of utmost importance with
egard to SNR is the receiver coil. MRI scanners are equippedith a great variety of multiple-channel surface coil arrays
o fit all shapes of the average adult anatomy (head, torso,nee coils, etc.). However, they cannot be adapted to theimensions of each individual patient. Radio-frequency coileceivers can be thought of as simple coil loops. The diam-ter of these loops should be large enough to captureignals from protons deep inside the body, but as smalls possible to capture less noise coming from the restf the body. In general practice, only conventional adultoils are available, leading to a suboptimal SNR. Dedicatedr scalable coils would be an interesting field for futureesearch.
eart rate and cardiac synchronization
he normal heart rate in infants (90—180 bpm) is higherhan in adults (60—100 bpm). For cardiac MRI, higher heartates have two general consequences. Firstly, the heart resthase (diastasis in mid-diastole) shortens and disappearsfter 90 bpm [2]. Shorter diastasis implies that a smallerortion of the k-space can be acquired during each cardiacycle to avoid motion blurring. The use of end-systole40% of the cardiac cycle), instead of mid-diastole (75%f the cardiac cycle), has been advocated when heartate is > 70 bpm [3], but this has not been validated inhildren. The use of systole may not be compatible with allreparation pulses as they may require a certain amount ofime before the readout. Those pulses can be performed innticipation, during the previous cardiac cycle, but it couldequire a prospective guess of the next cardiac cycle length4]. Secondly, the cardiac cycle length becomes very short
ith regard to the corresponding cardiac time constantsT1 and T2). For T1-sensitive sequences, it is preferable toait between consecutive MRI excitations (ideally 3 × T1f the organ of interest, i.e. at least 2—3 s or several
145
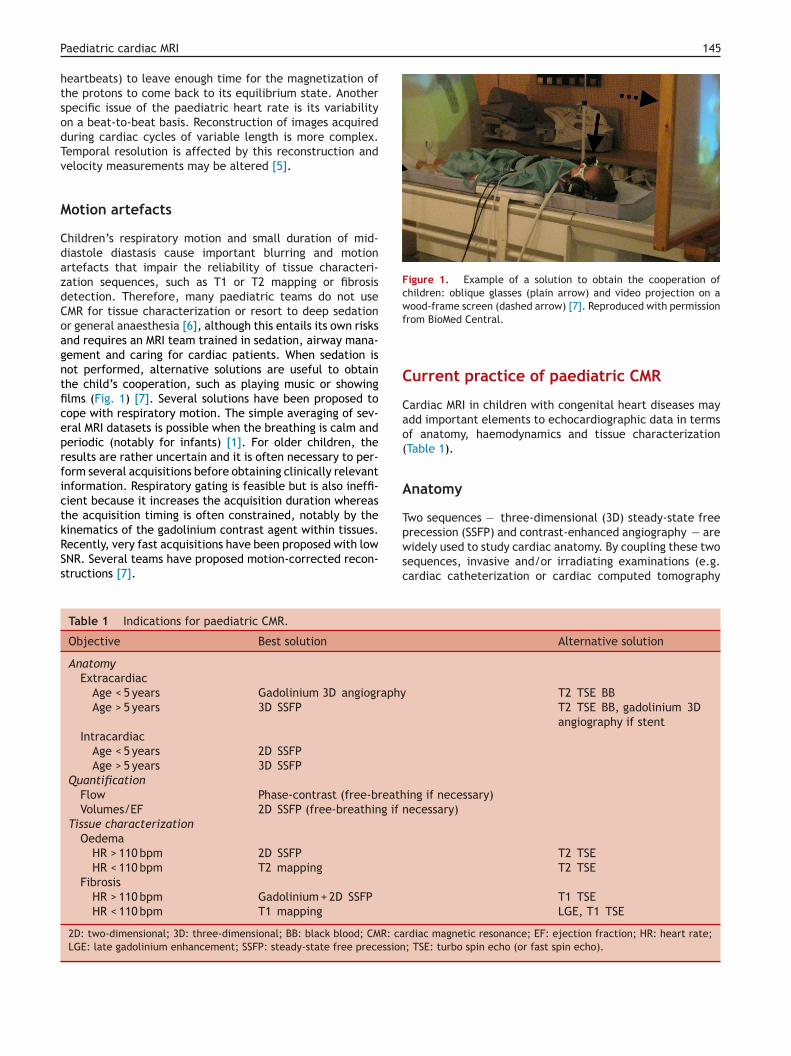
Figure 1. Example of a solution to obtain the cooperation ofchildren: oblique glasses (plain arrow) and video projection on awood-frame screen (dashed arrow) [7]. Reproduced with permissionf
C
Cao(
A
T
Paediatric cardiac MRI
heartbeats) to leave enough time for the magnetization ofthe protons to come back to its equilibrium state. Anotherspecific issue of the paediatric heart rate is its variabilityon a beat-to-beat basis. Reconstruction of images acquiredduring cardiac cycles of variable length is more complex.Temporal resolution is affected by this reconstruction andvelocity measurements may be altered [5].
Motion artefacts
Children’s respiratory motion and small duration of mid-diastole diastasis cause important blurring and motionartefacts that impair the reliability of tissue characteri-zation sequences, such as T1 or T2 mapping or fibrosisdetection. Therefore, many paediatric teams do not useCMR for tissue characterization or resort to deep sedationor general anaesthesia [6], although this entails its own risksand requires an MRI team trained in sedation, airway mana-gement and caring for cardiac patients. When sedation isnot performed, alternative solutions are useful to obtainthe child’s cooperation, such as playing music or showingfilms (Fig. 1) [7]. Several solutions have been proposed tocope with respiratory motion. The simple averaging of sev-eral MRI datasets is possible when the breathing is calm andperiodic (notably for infants) [1]. For older children, theresults are rather uncertain and it is often necessary to per-form several acquisitions before obtaining clinically relevantinformation. Respiratory gating is feasible but is also ineffi-cient because it increases the acquisition duration whereasthe acquisition timing is often constrained, notably by the
kinematics of the gadolinium contrast agent within tissues.Recently, very fast acquisitions have been proposed with lowSNR. Several teams have proposed motion-corrected recon-structions [7].pwsc
Table 1 Indications for paediatric CMR.
Objective Best solution
AnatomyExtracardiac
Age < 5 years Gadolinium 3D angiographyAge > 5 years 3D SSFP
IntracardiacAge < 5 years 2D SSFPAge > 5 years 3D SSFP
QuantificationFlow Phase-contrast (free-breathVolumes/EF 2D SSFP (free-breathing if n
Tissue characterizationOedema
HR > 110 bpm 2D SSFP
HR < 110 bpm T2 mapping
FibrosisHR > 110 bpm Gadolinium + 2D SSFP
HR < 110 bpm T1 mapping
2D: two-dimensional; 3D: three-dimensional; BB: black blood; CMR: caLGE: late gadolinium enhancement; SSFP: steady-state free precession
rom BioMed Central.
urrent practice of paediatric CMR
ardiac MRI in children with congenital heart diseases maydd important elements to echocardiographic data in termsf anatomy, haemodynamics and tissue characterizationTable 1).
natomy
wo sequences — three-dimensional (3D) steady-state freerecession (SSFP) and contrast-enhanced angiography — are
idely used to study cardiac anatomy. By coupling these twoequences, invasive and/or irradiating examinations (e.g.ardiac catheterization or cardiac computed tomography
Alternative solution
T2 TSE BBT2 TSE BB, gadolinium 3Dangiography if stent
ing if necessary)ecessary)
T2 TSET2 TSE
T1 TSELGE, T1 TSE
rdiac magnetic resonance; EF: ejection fraction; HR: heart rate;; TSE: turbo spin echo (or fast spin echo).

146 L. Bonnemains et al.
Figure 2. Examples of current usage of 3D SSFP sequences for anatomy in children. A. A 3D reconstruction of the aorta of a 6-year-oldboy several years after surgery for coarctation, based on a 3D SSFP acquisition without any gadolinium injection. B. A partial 3D printingof a complex double outlet right ventricle in a child of weight 5 kg. The tunnel from the left ventricle to the aorta has been outlined inwhite. C and D. 3D SSFP images of the coronary arteries in a 5-year-old child with transposition of the great arteries. The right coronary(C) is normal whereas the left coronary ostium (D) has been enlarged by a patch in a second surgery 1 month after the arterial switch. 3D:t free precession; RA: right atrium; RV: right ventricle; VSD: ventriculars
[s
33sdctmhircpvdapcasFFtcaatdcc
CCSbas(e
arteries, aorta (e.g. in Fig. 3A), pulmonary veins and inferiorvena cava. The time of acquisition is important accordingto different indications to visualize different anatomicalstructures. Stents and small vessels, as well as distal pul-monary arteries and aorto-pulmonary collaterals, are wellvisualized, as presented in Fig. 3B.
Haemodynamics
In the majority of cases, morphological studies need to becompleted by haemodynamic data.
Blood flowWith the velocity-encoded phase-contrast cine sequence,it is possible to measure the volume of blood flow passingthrough any vessel of interest by placing a slice perpendicu-lar to it. With specific software, it is possible to calculate thevolume and the direction of the blood stream to estimate theforward and backward volume and to calculate valve regur-gitation. It is important to repeat this measurement within
Figure 3. Examples of current usages of gadolinium-enhancedangiography for anatomy in children. A. A 3D reconstruction ofthe aorta of a 6-year-old child with coarctation, based on agadolinium-enhanced 3D angiography. B. An axial view (based ona 3D angiography) of the pulmonary trunk and proximal pulmonary
hree-dimensional; Ao: aorta; LV: left ventricle; SSFP: steady-stateeptal defect.
CT] angiography) can often be avoided for morphologicaltudies.
D SSFPD SSFP is an electrocardiogram (ECG)-triggered pulseequence with respiratory motion compensation byiaphragmatic navigators or navigation on the heart itself,alled self-navigation. It is acquired in free-breathing. Thisype of sequence may be used with or without contrastedium to produce high-resolution 3D data of the whole
eart and extracardiac structures. However, to obtain goodmage resolution, regular respiration and regular heartate are mandatory. Therefore, its use is difficult in younghildren and neonates. However, this sequence is veryowerful for defining congenital heart disease, to preciselyisualize the heart segmentation and to classify the car-iopathy properly. The acquired full volume is isotropic andllows reconstruction of the heart following any obliquelane, to better identify the correct surgical strategy inomplex congenital heart diseases. Part of the thoracicnatomy can be isolated and presented as a 3D object,uch as the post-surgery aorta coarctation presented inig. 2A. The heart can also easily be 3D-printed such as inig. 2B. It is also helpful to define the relationship betweenhe heart, the great vessels and thoracic structures. Forhildren, structures such as ostia of coronary arteriesnd their proximal segments (e.g. in Fig. 2C and D) ororto-pulmonary collaterals are well visualized. However,he spatial resolution is not sufficient to visualize theetails of mitral or tricuspid valve anatomy. Its other pitfalloncerns visualization of structures containing a stent thatauses important artefacts on its proximal structures.
ontrast-enhanced angiographyontrast-enhanced angiography is complementary to 3DSFP, especially in patients with high heart rate and irregularreathing. It needs intravenous gadolinium-based contrast
gents to reduce the T1 relaxation time of blood. The acqui-ition is made on 1—3 different times of the cardiac cycle1—2 if acquired in free-breathing) to visualize the differ-nt phases of contrast filling: superior vena cava, pulmonarybranches in a 12-year-old child with a prosthetic pulmonary trunkdilated by a stent (white arrow). A second, smaller, stent hasbeen positioned at the entrance of the left branch. 3D: three-dimensional.

Paediatric cardiac MRI 147
Figure 4. Examples of current usages of cardiac MRI for tissue characterization in children [7]. A. Mid-ventricular short-axis T1 mapping ofa 7-year-old boy with Duchenne myopathy. In the inferior and inferolateral segments, higher T1 values before injection and lower T1 valuesafter injection reveal the presence of diffuse fibrosis. B. Late gadolinium enhancement image of the same heart. The presence of fibrosisis shown by the red contouring. C. Post-gadolinium four-chamber SSFP view (T1/T2-weighed image) very clearly revealing the extension of
neti
T
TicdThsaasalcc•
•
fibrosis in the lateral wall of the same heart (red outline). MRI; mag
all of the principal veins and great vessels, and also witha phantom to correct errors and to test data consistency[8]. This sequence is reliable for large vessels, thereforepulmonary and aortic flow and regurgitation are fairly reli-able. However, it is less reliable for small vessels such aspulmonary veins or little collateral vessels, and rather dif-ficult to use for moving structures such as atrioventricularvalves [9,10]. This sequence can easily be used with free-breathing children or neonates with a simple averaging. Itmay be used to evaluate shunts (intracardiac or extracar-diac, except arteriovenous shunt) and regurgitation [11].
Ventricular function and volumesVentricular function and volumes are estimated by two-dimensional (2D) SSFP cine sequence. This sequence maybe acquired on any desired plane to study the global andregional functions in specific cardiopathies and in cardiomy-opathies of the right and/or left ventricle. Volumes arecalculated on short-axis views according to the interna-tional consensus policy [12]. This sequence is used to assessregional function of the right ventricle better than echocar-diography, so it is recommended in the study of pathologiesaffecting the right heart (cardiomyopathies or post-surgicalcongenital heart disease like Tetralogy of Fallot). It isacquired normally in breath-holding but it is possible toobtain good quality images in free-breathing small childrenwith a simple averaging (multiple Nex).
Myocardial perfusionMyocardial perfusion at rest and/or after pharmacologicalstress (dipyridamole or adenosine) may be evaluated bya first-pass perfusion imaging technique after gadolinium-based contrast medium injection. Stress perfusion CMR hasbeen extensively validated in adults affected by ischaemicheart disease. It is superior to single photon emission com-puted tomography (SPECT) and it has comparable diagnostic
accuracy to positron emission tomography and fractionalflow reserve [13]. Moreover, compared with SPECT, CMR pro-vides information about coronary artery anatomy, so it isa valid option to assess myocardial ischaemia. Its use isrestricted to children in our experience.c resonance imaging; SSFP: steady-state free precession.
issue characterization
he principal peculiarity of CMR in comparison to othermaging techniques is the possibility to perform tissueharacterization. Three cardiac components are usuallyetected: fat, oedema and fibrosis. Generally, fat has low1 and high T2, fibrosis has elevated T1, and oedema hasigh T1 and T2. To increase the contrast between fibro-is/oedema and normal myocardium, the use of a contrastgent (e.g. gadolinium) is recommended [14]. Tissue char-cterization is very difficult to achieve in neonates, and ithould be restricted, according to our experience, to infantsnd children with heart rates < 110 bpm (for quantification orate gadolinium enhancement [LGE]) and with breath-holdapacities (for T1 or T2 quantification). Two types of analysisan be performed:
quantification of T1 and T2 can be performed by T1 andT2 mapping sequences. These sequences are currentlyavailable on most MRI scanners. The images are usuallycoloured and each voxel colour directly codes for a T1or T2 value (e.g. in Fig. 4A). Each tissue (notably fat,oedema and fibrosis) can be recognized by analyzing thesame zone on T1 and T2 maps. T1 mapping sequence soonafter gadolinium injection is technically challenging andseveral artefacts often make the interpretation quite dif-ficult. In our experience, accurate quantification requiresbreath-holding capacities and heart rate < 110 bpm;T1- and T2-weighted images are specific sequencesdesigned to visually discriminate tissues according totheir T1 or T2. T1-weighted images have low repeti-tion time (TR) (10—20 ms) so that tissues with shortT1 appear brighter. T2-weighted images have long echotimes (TE and TR > 40—50 ms) so that tissues with longT2 appear brighter. LGE sequences are T1-weightedimages with a specific choice of the delay between theinversion pulse and the readout to ensure that normalmyocardium appears dark. In our experience, T1- or T2-weighted images can be acquired even in young children(breath-hold is not mandatory) but LGE requires heart
rate < 110 bpm. LGE is very informative when large zonesof the myocardium are infarcted, but its interpretationin children with diffuse fibrosis may be complex (e.g. inFig. 4B [7]). 2D SSFP constitutes a specific sequence with
1
vo(t
F
N
Bssppbsfcsab
A
RcoiaMobniroptsriw
F
UaF
fcMmahtEoleemsffeia
I
CidmMMcsam
ral
C
Ptrpmp
D
T
R
48
T2/T1-weighting that is very robust in children. In clin-ical practice, SSFP cine sequences just before and soonafter gadolinium injection is a good alternative to detectoedema/fibrosis, as illustrated in Fig. 4C [7]. Oedemaresulting in longer T2 results in spontaneously hyper-intense tissue before injection. This spontaneous signalmust be compared with the enhancement after contrastinjection, which is due to the gadolinium reduction in T1.In theory, it is possible to discriminate the oedema andfibrosis zones, but in practice, this distinction is complexand LGE at an early stage often decreases with time [15].
Tissue characterization has a high potential addedalue for the diagnosis and characterization of acquiredr congenital cardiomyopathies, inflammatory processesmyocarditis, graft rejection [16], etc.) and cardiacumours.
uture of paediatric CMR
ovel accelerated imaging techniques
eyond commercially available acceleration techniquesuch as partial [17] and parallel [18] acquisition of the k-pace, novel recent developments are expected to benefitaediatric CMR. In particular, the recent theory of com-ressed sensing, applied to MRI, states that an image cane reconstructed from a reduced subset of randomly cho-en k-space samples, which means the acquisition can beurther accelerated. The main condition to be able to applyompressed sensing is that the image should be compres-ible (e.g. the background of the image does not containny useful information). This technique has been applied toody (chest and abdomen) paediatric MRI [19].
dvanced motion correction
ecent motion correction techniques allow retrospectiveorrection of complex organ motion, including non-rigidr elastic deformations. Generalized reconstruction bynversion of coupled systems (GRICS) [20,21] is one suchlgorithm, able to produce clinically relevant images fromRI data corrupted by respiratory motion with the helpf respiratory motion sensors (two respiratory pneumaticelts positioned on the thorax and the abdomen) con-ected to a recording system. Acquisitions are performedn complete free-breathing and images are reconstructedetrospectively with a non-rigid motion correction basedn all data (no respiratory gating) and adapted to theatient’s specific motion. Preliminary results of the applica-ion of GRICS to CMR of children and young adults have beenhown in Duchenne muscular dystrophy patients [7]. Closelyelated approaches have been shown in paediatric abdom-nal applications that combine advanced motion correctionith compressed sensing [22].
oetal heart imaging
ltrasound is the recommended technique as the primarypproach for the assessment of foetal cardiac structures.actors that limit ultrasound, such as maternal obesity,
L. Bonnemains et al.
oetal position and oligohydramnios, do not necessarilyompromise the image quality of MRI. Therefore, cardiacRI has been investigated in various centres, but remainsainly restricted to research. Foetal cardiac MRI constitutes
complex challenge due to rapid foetal heart rate, smalleart size, foetal movements and because real ECG-gating ofhe foetal heart is not possible. Indeed, although the foetalCG is visible on the mother’s ECG [23], it is typically anrder of magnitude smaller in amplitude and might not bearge enough compared to the interferences caused by thelectromagnetic MRI environment (magneto-hydrodynamicffects caused by blood flows perpendicular to the staticagnetic field and gradient-switching artefacts during the
equences). Therefore, QRS detection is very difficult on theoetal ECG in MRI. Different solutions have been proposedor ECG triggering with varying results: no triggering [24],xternal ultrasound captor [25] and metric optimized gat-ng with retrospective reconstruction [26]. These solutionsre not yet available in clinical practice.
nterventional MRI
ardiac catheterization entirely guided by MRI was reportedn 2003 [27]. It requires specific non-magnetic equipmenturing the procedure. Several aspects of catheterization areuch more complex (plastic catheters are difficult to see inRI, metallic guide-wires are prohibited, etc.). However,RI allows a simple evaluation of flows and simplifies theomputation of pulmonary resistance. The higher cost ofuch dedicated environments constitutes a real drawbacknd it is not yet clear whether this technique will becomeore widespread.MRI may also be used to monitor temperature during
adio-frequency ablation, but this is rarely used in paedi-tric populations. MRI could also be a way to deliver energyocally by means of focalized radio-frequency.
onclusions
aediatric cardiac MRI is a challenging modality withremendous potential. It is non-invasive and may beepeated several times without harm to the patient. Itrovides anatomical, haemodynamic and pathological infor-ation and is rapidly acquiring a key role in the diagnosticrocess of congenital heart diseases.
isclosure of interest
he authors declare that they have no competing interest.
eferences
[1] Bernstein MA, King KF, Zhou XJ. Handbook of MRI pulsesequences. Elsevier; 2004.
[2] van der Hulst AE, Delgado V, Ten Harkel AD, et al. Tis-
sue Doppler imaging in the left ventricle and right ventriclein healthy children: normal age-related peak systolic veloc-ities, timings, and time differences. Eur J Echocardiogr2011;12:953—60.
[
[
[
[
[
[
[
[
[
[
[
[
Paediatric cardiac MRI
[3] Wu YW, Tadamura E, Yamamuro M, et al. Evaluation ofthree-dimensional navigator-gated whole heart MR coronaryangiography: the importance of systolic imaging in subjectswith high heart rates. Eur J Radiol 2007;61:91—6.
[4] Fernandez B, Oster J, Lohezic M, et al. Adaptive black bloodfast spin echo for end-systolic rest cardiac imaging. Magn ResonMed 2010;64:1760—71.
[5] Bonnemains L, Odille F, Meyer C, et al. Is high temporal res-olution achievable for paediatric cardiac acquisitions duringseveral heart beats? Illustration with cardiac phase-contrastcine-MRI. PLoS One 2015;10(1):e0143744.
[6] Fogel MA, Weinberg PM, Parave E, et al. Deep sedation for car-diac magnetic resonance imaging: a comparison with cardiacanesthesia. J Pediatr 2008;152:534—9 [9 e1].
[7] Bonnemains L, Odille F, Cherifi A, et al. Free-breathing withmotion correction and video projection during cardiac MRI:a paediatric design! J Cardiovasc Magn Reson 2014;16(Suppl.1):415 [abstract P319].
[8] Kecir K, Beaumont M, Chen B, et al. Quality control of cardiacMRI exams for Fallot patients: combination of standard mea-surements and physiological analysis to detect invalid exams.Arch Cardiovasc Dis 2016 [in press].
[9] Myerson SG. Heart valve disease: investigation by cardiovascu-lar magnetic resonance. J Cardiovasc Magn Reson 2012;14:7.
[10] Kramer CM, Barkhausen J, Flamm SD, et al. Standardizedcardiovascular magnetic resonance imaging (CMR) protocols,society for cardiovascular magnetic resonance: board oftrustees task force on standardized protocols. J CardiovascMagn Reson 2008;10:35.
[11] Devos DG, Kilner PJ. Calculations of cardiovascular shuntsand regurgitation using magnetic resonance ventricular vol-ume and aortic and pulmonary flow measurements. Eur Radiol2010;20:410—21.
[12] Hundley WG, Bluemke DA, Finn JP, et al.ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus doc-ument on cardiovascular magnetic resonance: a report ofthe American College of Cardiology Foundation Task Forceon Expert Consensus Documents. Circulation 2010;121:2462—508.
[13] Tobler D, Motwani M, Wald RM, et al. Evaluation of a com-prehensive cardiovascular magnetic resonance protocol inyoung adults late after the arterial switch operation for d-transposition of the great arteries. J Cardiovasc Magn Reson
2014;16:98.[14] Mewton N, Liu CY, Croisille P, Bluemke D, Lima JA. Assessmentof myocardial fibrosis with cardiovascular magnetic resonance.J Am Coll Cardiol 2011;57:891—903.
[
149
15] Raimondi F, Iserin F, Raisky O, et al. Myocardial inflammationon cardiovascular magnetic resonance predicts left ventricularfunction recovery in children with recent dilated cardiomyopa-thy. Eur Heart J Cardiovasc Imaging 2015;16:756—62.
16] Bonnemains L, Cherifi A, Girerd N, Odille F, Felblinger J. Designof the DRAGET Study: a multicentre controlled diagnostic studyto assess the detection of acute rejection in patients with hearttransplant by means of T2 quantification with MRI in compari-son to myocardial biopsies. BMJ Open 2015;5:e008963.
17] Noll DC, Nishimura DG, Macovski A. Homodyne detectionin magnetic resonance imaging. IEEE Trans Med Imaging1991;10:154—63.
18] Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P.SENSE: sensitivity encoding for fast MRI. Magn Reson Med1999;42:952—62.
19] Vasanawala SS, Alley MT, Hargreaves BA, et al. Improvedpediatric MR imaging with compressed sensing. Radiology2010;256:607—16.
20] Odille F, Vuissoz PA, Marie PY, Felblinger J. Generalized recon-struction by inversion of coupled systems (GRICS) applied tofree-breathing MRI. Magn Reson Med 2008;60:146—57.
21] Vuissoz PA, Odille F, Fernandez B, et al. Free-breathing imagingof the heart using 2D cine-GRICS (generalized reconstruction byinversion of coupled systems) with assessment of ventricularvolumes and function. J Magn Reson Imaging 2012;35:340—51.
22] Cheng JY, Alley MT, Cunningham CH, et al. Nonrigid motioncorrection in 3D using autofocusing with localized linear trans-lations. Magn Reson Med 2012;68:1785—97.
23] Taralunga DD, Ungureanu GM, Gussi I, Strungaru R, WolfW. Fetal ECG extraction from abdominal signals: a reviewon suppression of fundamental power line interferencecomponent and its harmonics. Comput Math Methods Med2014;2014:239060.
24] Gorincour G, Bourliere-Najean B, Bonello B, et al. Feasibil-ity of fetal cardiac magnetic resonance imaging: preliminaryexperience. Ultrasound Obstet Gynecol 2007;29:105—8.
25] Schoennagel BP, Remus CC, Yamamura J, et al. Fetal bloodflow velocimetry by phase-contrast MRI using a new trigger-ing method and comparison with Doppler ultrasound in a sheepmodel: a pilot study. MAGMA 2014;27:237—44.
26] Seed M, van Amerom JF, Yoo SJ, et al. Feasibility of quantifi-cation of the distribution of blood flow in the normal humanfetal circulation using CMR: a cross-sectional study. J Cardio-
vasc Magn Reson 2012;14:79.27] Razavi R, Hill DL, Keevil SF, et al. Cardiac catheterisationguided by MRI in children and adults with congenital heartdisease. Lancet 2003;362:1877—82.

![Strain imaging using cardiac magnetic resonance · 2017. 8. 26. · diac cycle [13]. Post-processing cardiovascular magnetic resonance technique to assess myocardial strain Feature](https://img.pdfslide.us/doc/110x75/601b196517a85f0b9166db11/strain-imaging-using-cardiac-magnetic-resonance-2017-8-26-diac-cycle-13.jpg)



























