Embed Size (px)
Citation preview
Cardiac Magnetic Resonance Imagingand Computed Tomography in NewbornsWith Congenital Heart DiseaseDipankar Gupta, MD,*
Arun Chandran, MD*
Author Disclosure
Drs Gupta and
Chandran have
disclosed no financial
relationships relevant
to this article. This
commentary does not
contain a discussion of
an unapproved/
investigative use of
a commercial product/
device.
Educational Gaps
1. Neonatologists may be unfamiliar with history and evolution of cardiac imaging.
2. Neonatologists may be unfamiliar with imaging principles behind the use of computed
tomography angiography (CTA) and cardiac magnetic resonance imaging (CMRI).
3. Neonatologists may be unfamiliar with indications and utility of CTA and CMRI in
congenital heart disease.
AbstractCongenital heart disease continues to be a leading cause of neonatal morbidity; however, ad-vancements in diagnostic technology and surgical techniques have markedly improved patientsurvival. In particular, in-depth noninvasive imaging with computed tomography angiography(CTA) and cardiac magnetic resonance imaging (CMRI) has had a tremendous effect on theamount of information available to the surgeonor interventionalist before any procedure.CTAandCMRI have their own advantages and disadvantages, and this review provides an overviewof these technologies, highlighting clinical indications. This article also provides images andvideotapes to better highlight our understanding of various complex congenital heart lesions.
Objectives After completing this article, readers should be able to:
1. Understand the basic imaging principles behind computed tomography angiography
(CTA) and cardiac magnetic resonance imaging (CMRI).
2. Understand basic indications for CTA and CMRI in the diagnosis of congenital heart
disease (CHD).
3. Understand the advantages and disadvantages of CTA vs CMRI.
4. Become familiar with key CTAs and CMRIs of common CHD lesions.
IntroductionThe incidence of congenital heart disease (CHD) in the United States is approximately 1%. (1)(2) CHD is the leading cause of neonatal mortality attributable to birth defects, accounting for27.5% of affected neonates, with chromosomal anomalies being the second highest at 22.4%. (3)Echocardiography continues to be the primary initial modality used to define these congenitalheart lesions, but there are limitations to its use, especially as it applies to extracardiac arterial orvenous and thoracic delineation. Often, further diagnostic workup is required before any form ofintervention. With recent advancements in technology in computed tomography angiography(CTA) and cardiac magnetic resonance imaging (CMRI), pediatric cardiologists have been ableto furnish these answers, thus obviating the need for more traditional invasive procedures, suchas diagnostic cardiac catheterization. In our institution, we primarily use CTA for extracardiacgreat vessel imaging, including aortic arch, pulmonary artery, and venous anomalies, as well asdefining adjoining thoracic structures, including the airway. In addition, CMRI can be used forthese purposes with the added benefit of intracardiac anatomical and functional imaging.
Cardiac CTAComputed tomography (CT) was introduced in the 1970s by Sir Godfrey Hounsfield, andsince then, there has been tremendous development in CT technology. (4)(5) CT uses
*Congenital Heart Center, Department of Pediatrics, University of Florida, Gainesville, FL.
Article cardiology
e362 NeoReviews Vol.16 No.6 June 2015
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from
x-rays or ionizing radiation, which is emitted from thesource and detected by special detectors opposite tothe source. After data acquisition, special algorithmsare used to create the final image. (4) Initially, single-slicescanners were used. Today, CT contains 320-slice scan-ners called multidetector-row CT (MDCT). The tempo-ral and spatial resolution of CT with the advent ofMDCT scanners has paved the way for improved imagingof complex CHD, thus bypassing the restrictions other-wise posed by faster neonatal heart rates and smaller neo-natal structures. (6)(7)
Indications for Neonatal Cardiac CTAThe indications for neonatal cardiac CTA include the fol-lowing: (1) aortic arch anomalies (coarctation of theaorta, interrupted aortic arch, and vascular ring or sling),(2) pulmonary artery anomalies (pulmonary artery steno-sis and aortopulmonary collaterals), (3) anomalies of pul-monary venous return (anomalous pulmonary venousreturn and pulmonary vein stenosis), (4) coronary arteryanomalies (anomalous coronary artery origins or course),(5) extracardiac thoracic anatomy (extracardiac masses,airway compression, and lung disease), and (6) postoper-ative assessment after CHD surgery.
Sample CTA ProtocolAt our institution, we use a 320-slice Aquilion ONEscanner (Toshiba Medical Systems Corp, Tustin, CA).Neonatal images are typically obtained without any se-dation or breath-holding and usually without adminis-tration of b-blockers even with heart rates greaterthan 80 beats per minute. Low-osmolar iodine contrastmedium (Visipaque) is injected intravenously at a doseof 2 mL/kg via a 24-gauge or larger peripheral catheteror a peripherally inserted central catheter not exceedingthe rate of 0.5 mL/s manually. The scan is initiated afterthe injection of contrast without using bolus tracking.The scan volume typically extends superiorly from thethoracic inlet to just below the diaphragm inferiorly.With suspected heterotaxy, interruption of the inferiorvena cava, and infracardiac anomalous pulmonary ve-nous return, the scan volume is extended to the infrare-nal region. All scans are performed in a cranial-caudaldirection with CT parameters adapted to the patient’sweight. Postprocessing of the MDCT scans is per-formed on a dedicated Vital Images workstation usingVitrea 2 software, version 4.0 (Vital Images Inc, Minne-tonka, MN). (8)
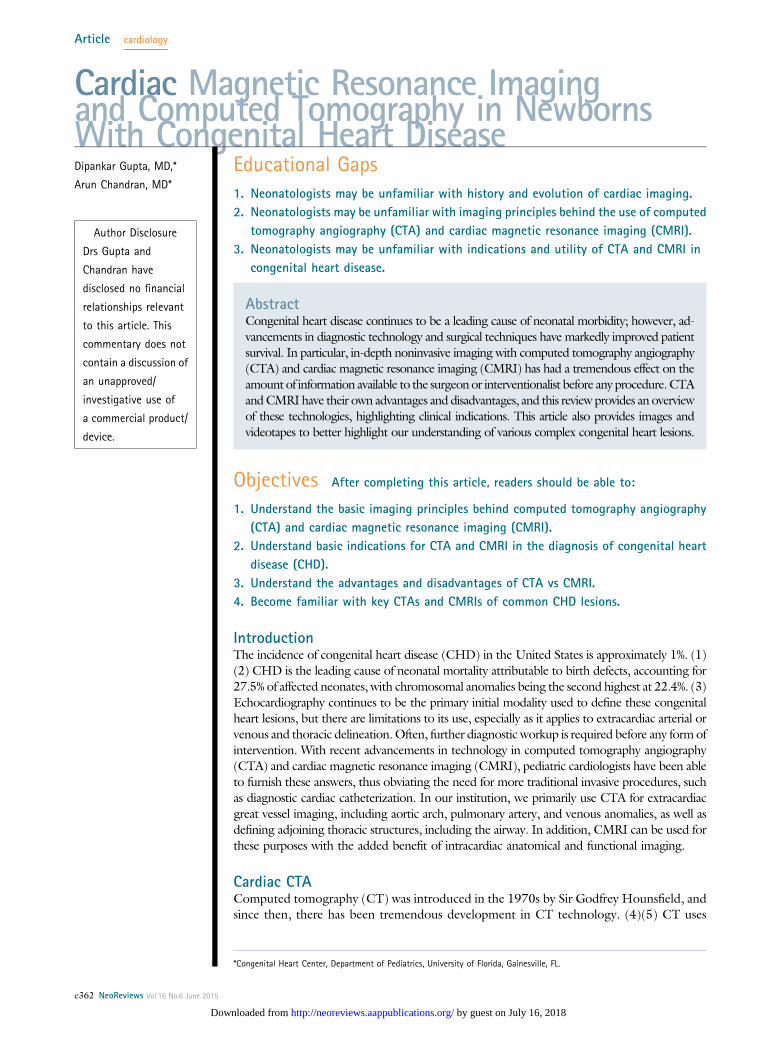
Figure 1. Saggital section of arch showing a discrete (redarrow) juxtaductal coarctation of the aorta in a newborn.
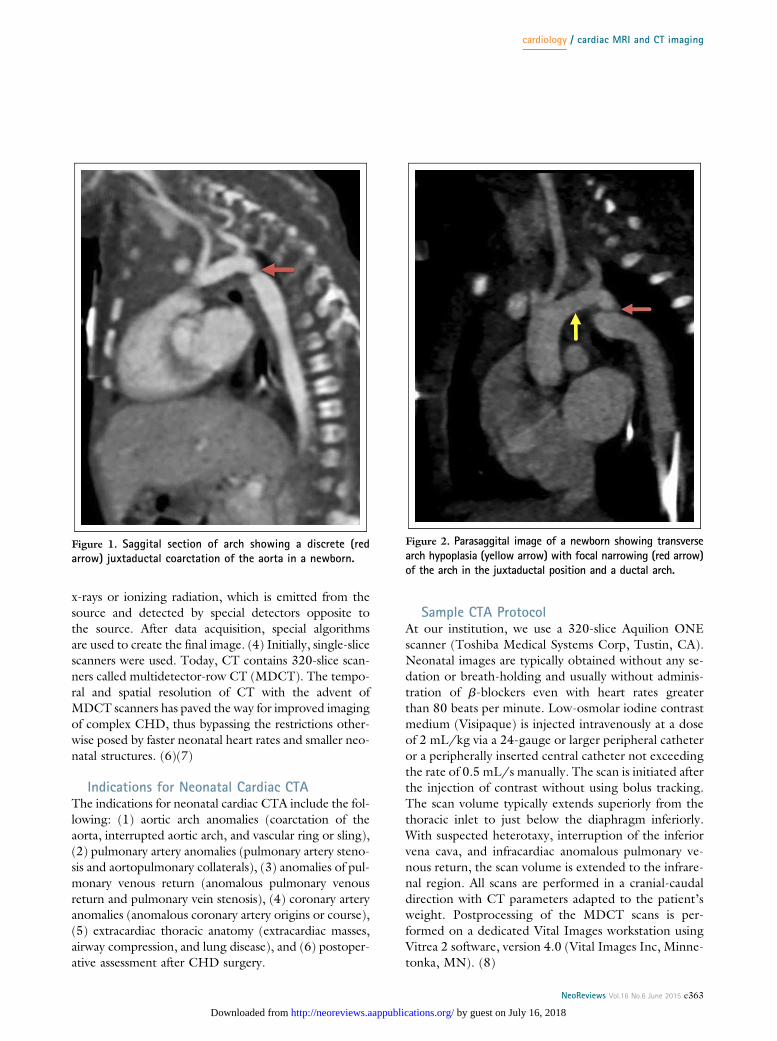
Figure 2. Parasaggital image of a newborn showing transversearch hypoplasia (yellow arrow) with focal narrowing (red arrow)of the arch in the juxtaductal position and a ductal arch.
cardiology / cardiac MRI and CT imaging
NeoReviews Vol.16 No.6 June 2015 e363
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from
Cardiac Morphologic Findings in Complex CHDAORTIC ARCH ANOMALIES. Coarctation of the aorta
(CoA) is associated with clinical symptoms in the new-born period after the patent ductus arteriosus (PDA)
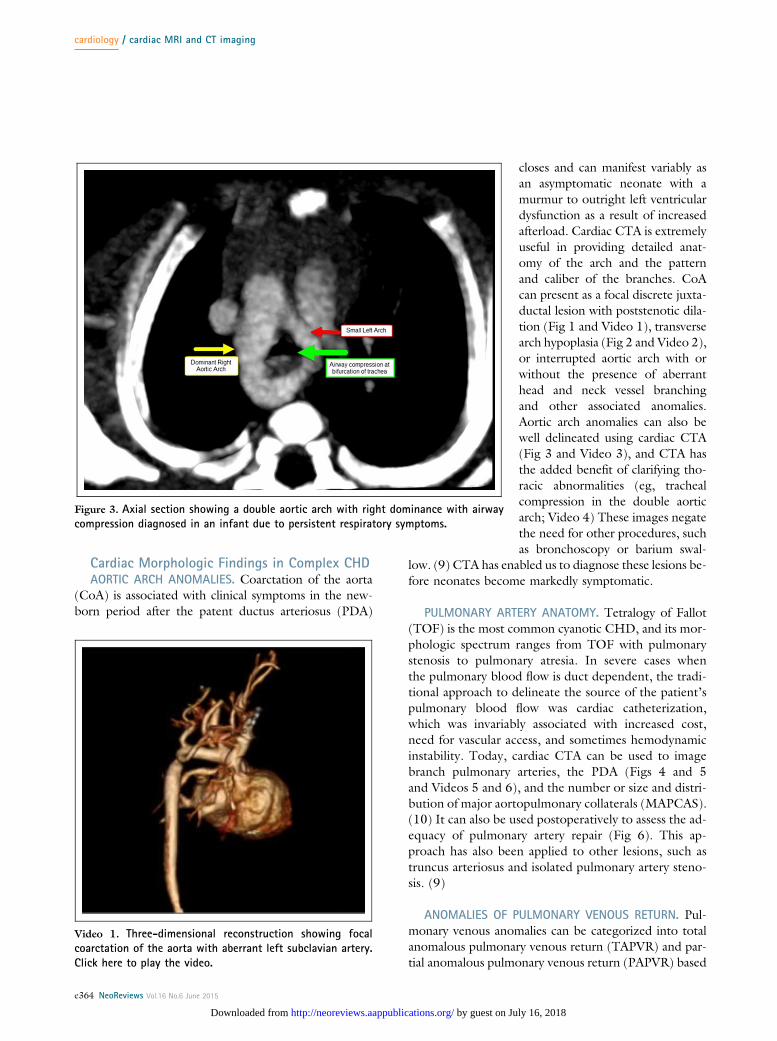
closes and can manifest variably asan asymptomatic neonate with amurmur to outright left ventriculardysfunction as a result of increasedafterload. Cardiac CTA is extremelyuseful in providing detailed anat-omy of the arch and the patternand caliber of the branches. CoAcan present as a focal discrete juxta-ductal lesion with poststenotic dila-tion (Fig 1 and Video 1), transversearch hypoplasia (Fig 2 and Video 2),or interrupted aortic arch with orwithout the presence of aberranthead and neck vessel branchingand other associated anomalies.Aortic arch anomalies can also bewell delineated using cardiac CTA(Fig 3 and Video 3), and CTA hasthe added benefit of clarifying tho-racic abnormalities (eg, trachealcompression in the double aorticarch; Video 4) These images negatethe need for other procedures, suchas bronchoscopy or barium swal-
low. (9) CTA has enabled us to diagnose these lesions be-fore neonates become markedly symptomatic.
PULMONARY ARTERY ANATOMY. Tetralogy of Fallot(TOF) is the most common cyanotic CHD, and its mor-phologic spectrum ranges from TOF with pulmonarystenosis to pulmonary atresia. In severe cases whenthe pulmonary blood flow is duct dependent, the tradi-tional approach to delineate the source of the patient’spulmonary blood flow was cardiac catheterization,which was invariably associated with increased cost,need for vascular access, and sometimes hemodynamicinstability. Today, cardiac CTA can be used to imagebranch pulmonary arteries, the PDA (Figs 4 and 5and Videos 5 and 6), and the number or size and distri-bution of major aortopulmonary collaterals (MAPCAS).(10) It can also be used postoperatively to assess the ad-equacy of pulmonary artery repair (Fig 6). This ap-proach has also been applied to other lesions, such astruncus arteriosus and isolated pulmonary artery steno-sis. (9)
ANOMALIES OF PULMONARY VENOUS RETURN. Pul-monary venous anomalies can be categorized into totalanomalous pulmonary venous return (TAPVR) and par-tial anomalous pulmonary venous return (PAPVR) based
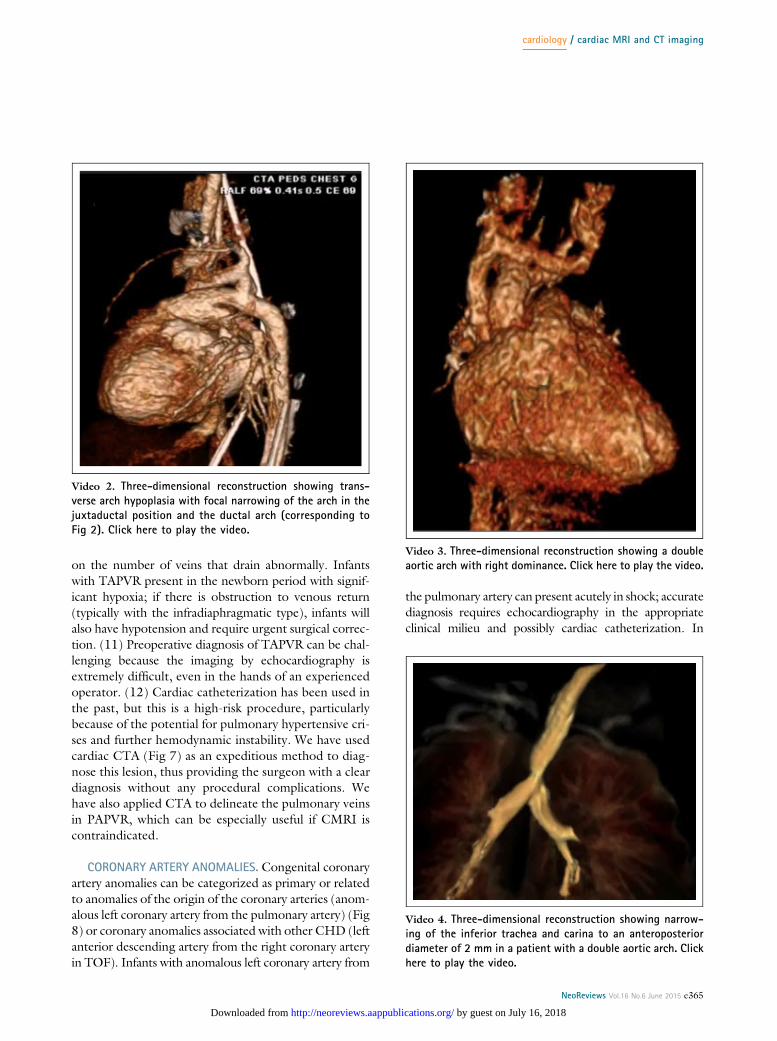
Video 1. Three-dimensional reconstruction showing focalcoarctation of the aorta with aberrant left subclavian artery.Click here to play the video.
Figure 3. Axial section showing a double aortic arch with right dominance with airwaycompression diagnosed in an infant due to persistent respiratory symptoms.
cardiology / cardiac MRI and CT imaging
e364 NeoReviews Vol.16 No.6 June 2015
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from
on the number of veins that drain abnormally. Infantswith TAPVR present in the newborn period with signif-icant hypoxia; if there is obstruction to venous return(typically with the infradiaphragmatic type), infants willalso have hypotension and require urgent surgical correc-tion. (11) Preoperative diagnosis of TAPVR can be chal-lenging because the imaging by echocardiography isextremely difficult, even in the hands of an experiencedoperator. (12) Cardiac catheterization has been used inthe past, but this is a high-risk procedure, particularlybecause of the potential for pulmonary hypertensive cri-ses and further hemodynamic instability. We have usedcardiac CTA (Fig 7) as an expeditious method to diag-nose this lesion, thus providing the surgeon with a cleardiagnosis without any procedural complications. Wehave also applied CTA to delineate the pulmonary veinsin PAPVR, which can be especially useful if CMRI iscontraindicated.
CORONARY ARTERY ANOMALIES. Congenital coronaryartery anomalies can be categorized as primary or relatedto anomalies of the origin of the coronary arteries (anom-alous left coronary artery from the pulmonary artery) (Fig8) or coronary anomalies associated with other CHD (leftanterior descending artery from the right coronary arteryin TOF). Infants with anomalous left coronary artery from
the pulmonary artery can present acutely in shock; accuratediagnosis requires echocardiography in the appropriateclinical milieu and possibly cardiac catheterization. In
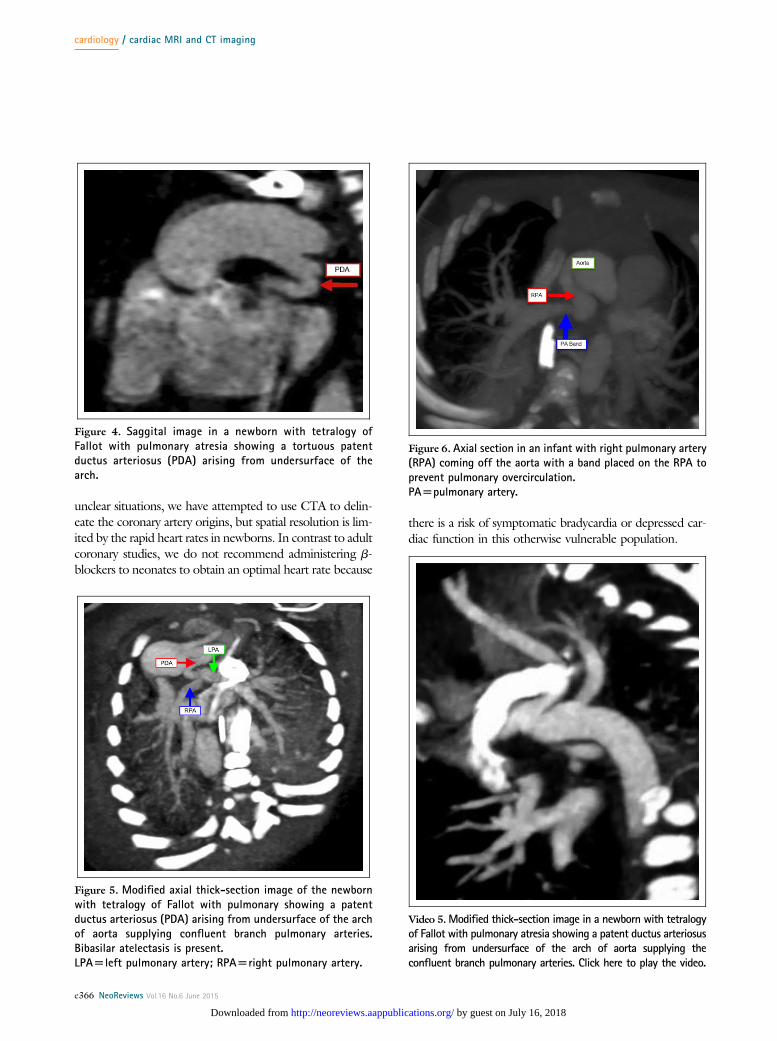
Video 2. Three-dimensional reconstruction showing trans-verse arch hypoplasia with focal narrowing of the arch in thejuxtaductal position and the ductal arch (corresponding toFig 2). Click here to play the video.
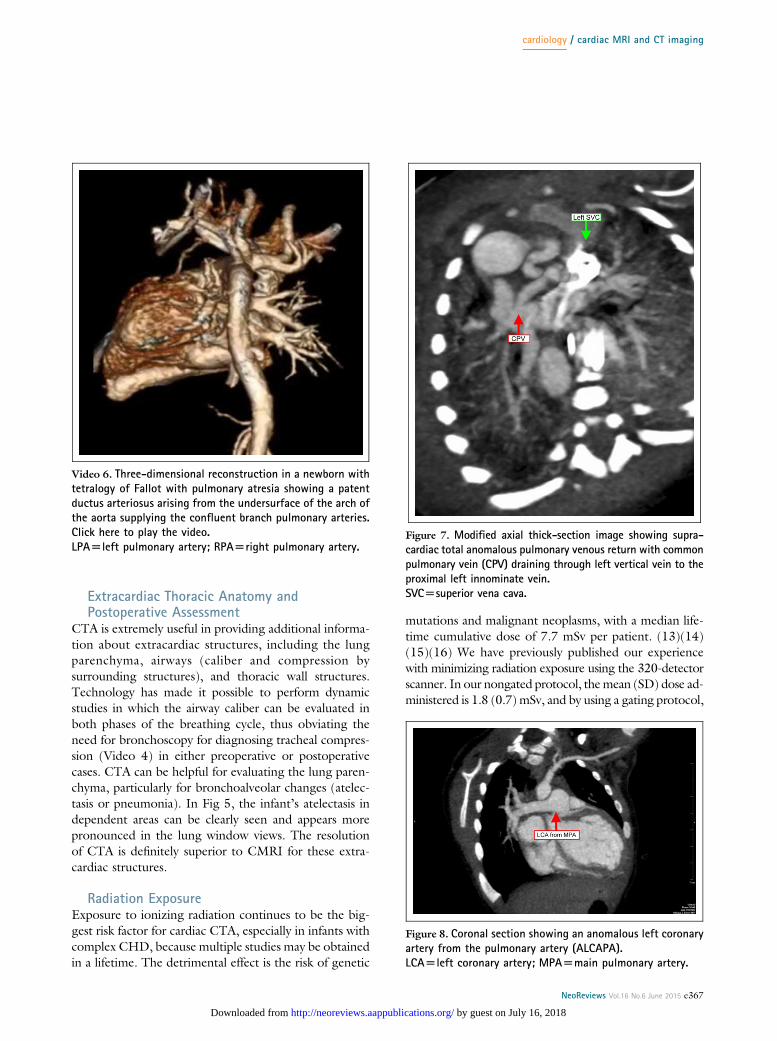
Video 3. Three-dimensional reconstruction showing a doubleaortic arch with right dominance. Click here to play the video.
Video 4. Three-dimensional reconstruction showing narrow-ing of the inferior trachea and carina to an anteroposteriordiameter of 2 mm in a patient with a double aortic arch. Clickhere to play the video.
cardiology / cardiac MRI and CT imaging
NeoReviews Vol.16 No.6 June 2015 e365
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from
unclear situations, we have attempted to use CTA to delin-eate the coronary artery origins, but spatial resolution is lim-ited by the rapid heart rates in newborns. In contrast to adultcoronary studies, we do not recommend administering b-blockers to neonates to obtain an optimal heart rate because
there is a risk of symptomatic bradycardia or depressed car-diac function in this otherwise vulnerable population.
Figure 4. Saggital image in a newborn with tetralogy ofFallot with pulmonary atresia showing a tortuous patentductus arteriosus (PDA) arising from undersurface of thearch.
Figure 5. Modified axial thick-section image of the newbornwith tetralogy of Fallot with pulmonary showing a patentductus arteriosus (PDA) arising from undersurface of the archof aorta supplying confluent branch pulmonary arteries.Bibasilar atelectasis is present.LPA[left pulmonary artery; RPA[right pulmonary artery.
Figure 6. Axial section in an infant with right pulmonary artery(RPA) coming off the aorta with a band placed on the RPA toprevent pulmonary overcirculation.PA[pulmonary artery.
Video 5.Modified thick-section image in a newborn with tetralogyof Fallot with pulmonary atresia showing a patent ductus arteriosusarising from undersurface of the arch of aorta supplying theconfluent branch pulmonary arteries. Click here to play the video.
cardiology / cardiac MRI and CT imaging
e366 NeoReviews Vol.16 No.6 June 2015
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from
Extracardiac Thoracic Anatomy andPostoperative Assessment
CTA is extremely useful in providing additional informa-tion about extracardiac structures, including the lungparenchyma, airways (caliber and compression bysurrounding structures), and thoracic wall structures.Technology has made it possible to perform dynamicstudies in which the airway caliber can be evaluated inboth phases of the breathing cycle, thus obviating theneed for bronchoscopy for diagnosing tracheal compres-sion (Video 4) in either preoperative or postoperativecases. CTA can be helpful for evaluating the lung paren-chyma, particularly for bronchoalveolar changes (atelec-tasis or pneumonia). In Fig 5, the infant’s atelectasis independent areas can be clearly seen and appears morepronounced in the lung window views. The resolutionof CTA is definitely superior to CMRI for these extra-cardiac structures.
Radiation ExposureExposure to ionizing radiation continues to be the big-gest risk factor for cardiac CTA, especially in infants withcomplex CHD, because multiple studies may be obtainedin a lifetime. The detrimental effect is the risk of genetic
mutations and malignant neoplasms, with a median life-time cumulative dose of 7.7 mSv per patient. (13)(14)(15)(16) We have previously published our experiencewith minimizing radiation exposure using the 320-detectorscanner. In our nongated protocol, themean (SD) dose ad-ministered is 1.8 (0.7) mSv, and by using a gating protocol,
Video 6. Three-dimensional reconstruction in a newborn withtetralogy of Fallot with pulmonary atresia showing a patentductus arteriosus arising from the undersurface of the arch ofthe aorta supplying the confluent branch pulmonary arteries.Click here to play the video.LPA[left pulmonary artery; RPA[right pulmonary artery.
Figure 7. Modified axial thick-section image showing supra-cardiac total anomalous pulmonary venous return with commonpulmonary vein (CPV) draining through left vertical vein to theproximal left innominate vein.SVC[superior vena cava.
Figure 8. Coronal section showing an anomalous left coronaryartery from the pulmonary artery (ALCAPA).LCA[left coronary artery; MPA[main pulmonary artery.
cardiology / cardiac MRI and CT imaging
NeoReviews Vol.16 No.6 June 2015 e367
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from
the dose was further reduced to 0.8 (0.39) mSv. (8) Toput this into perspective, the approximate effective radia-tion dose of chest radiography for an average-sized adultis 0.1 mSv, and a similar scan for pediatric patients exposesthem to a much higher radiation dose. In the UnitedStates, the mean exposure to radiation is 3 mSv per year.The best way to decrease this risk is by applying the prin-ciple of ALARA (as low as reasonably achievable) and re-ducing the dose of ionizing radiation using varioustechniques, such as decreasing the scan time and/or mod-ifying the kilovoltage, current, and scan pitch. (4)(7)
CMRIHistorical Perspective
Initial use of CMRI dates back to the 1970s when it wasused to measure in vitro myocardial metabolism in
perfused rat hearts. In the past 3 decades, its use hasevolved to assist with cardiac anatomy, ventricular func-tion, extracardiac vasculature, and viability and metabo-lism of the myocardium. Because CMRI can providesuch an extensive amount of information, it has been de-scribed as a one-stop-shop for cardiac imaging. (17)
MRI PhysicsFelix Bloch and Edwin Purcell independently describedthe phenomenon of nuclear magnetic resonance in
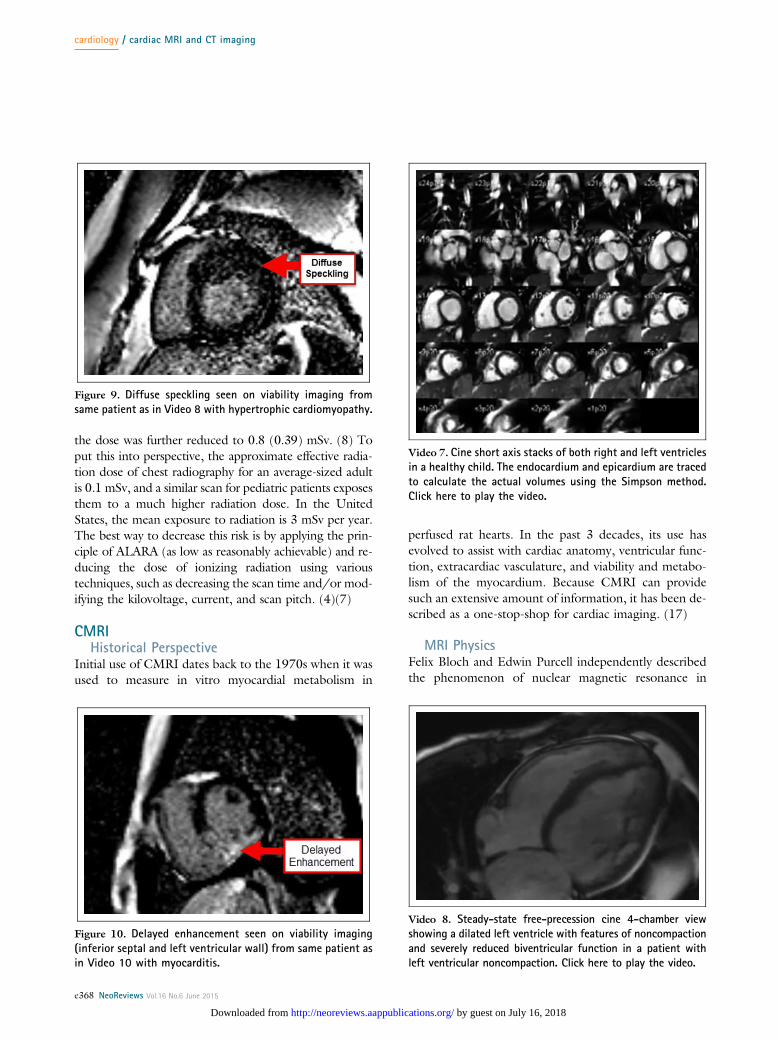
Figure 9. Diffuse speckling seen on viability imaging fromsame patient as in Video 8 with hypertrophic cardiomyopathy.
Figure 10. Delayed enhancement seen on viability imaging(inferior septal and left ventricular wall) from same patient asin Video 10 with myocarditis.
Video 7. Cine short axis stacks of both right and left ventriclesin a healthy child. The endocardium and epicardium are tracedto calculate the actual volumes using the Simpson method.Click here to play the video.
Video 8. Steady-state free-precession cine 4-chamber viewshowing a dilated left ventricle with features of noncompactionand severely reduced biventricular function in a patient withleft ventricular noncompaction. Click here to play the video.
cardiology / cardiac MRI and CT imaging
e368 NeoReviews Vol.16 No.6 June 2015
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from
1946 and were awarded the Nobel Prize in Physics in1952. Since then, many other principles have been de-scribed that have enabled technology to improve the res-olution and information obtained by CMRI. Hydrogennuclei (protons) are present in large numbers in the bodyand have an intrinsic alignment, which is essentially ran-dom without any net magnetization. On application ofa high-strength magnetic field, the spins of these protonsalign with the direction of the magnetic field. For the pur-poses of CMRI, the magnetic field strength typically usedis 1.5 T, although other centers have started using 3-Tscanners. Radiofrequency energy applied during thealignment excites the spins and changes their alignmentrelative to the direction of energy application. In the
process of returning to their baseline state (relaxation),the released magnetic energy is then converted to a reso-nant signal in a receiver signal placed perpendicular to thetransverse plane (based on the principle of the electro-magnetic effect). During the last step, the computer con-verts these electrical signals to an image by the complexprocess of Fourier transformation. (4)(17)(18)
Indications of Neonatal CMRIIndications of neonatal CMRI include the following: (1)cardiac chamber volume, mass, and functional analysis;(2) cardiac morphologic findings in complex congenitalheart disease (including aortic arch anomalies [coarcta-tion of the aorta, interrupted aortic arch, and vascular
Video 9. Cine short axis of the ventricles showing severelyhypertrophied ventricular septum in a newborn with hyper-trophic cardiomyopathy. Click here to play the video.
Video 10. Cine short axis of the ventricles in a child withmyocarditis showing ventricular function and abnormal wallmotion especially of the inferoseptal wall. Click here to playthe video.
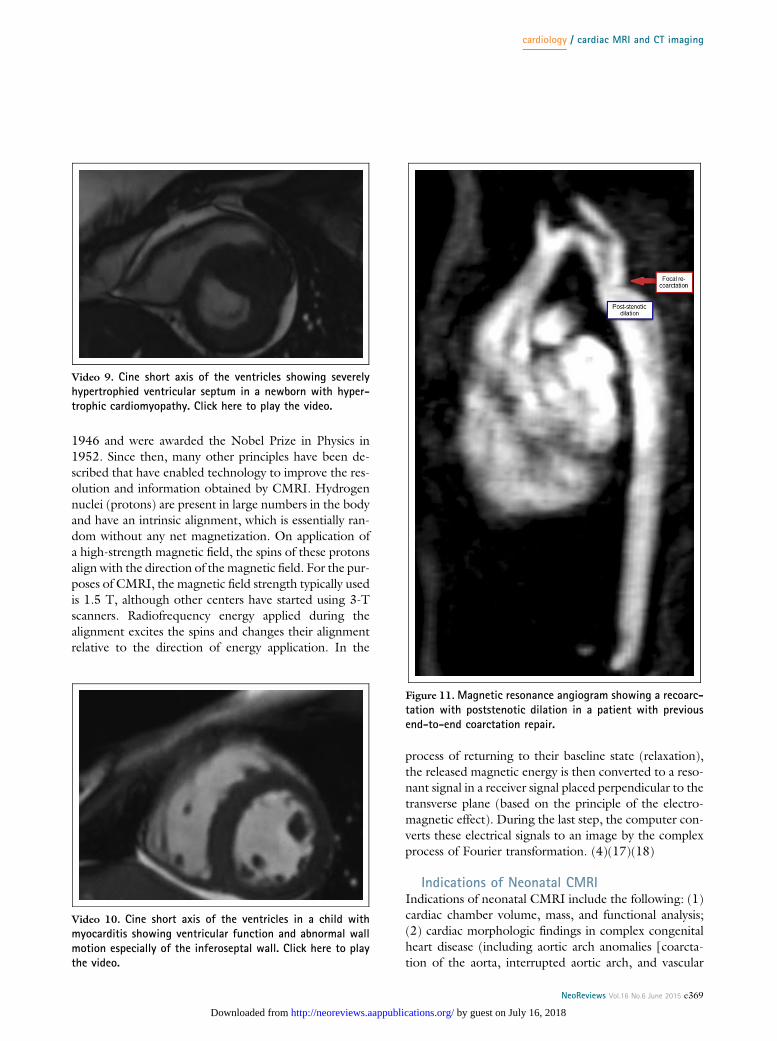
Figure 11.Magnetic resonance angiogram showing a recoarc-tation with poststenotic dilation in a patient with previousend-to-end coarctation repair.
cardiology / cardiac MRI and CT imaging
NeoReviews Vol.16 No.6 June 2015 e369
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from

ring or sling], pulmonary artery anomalies [pulmonaryartery stenosis and aortopulmonary collaterals], anoma-lies of pulmonary venous return [total or partial anoma-lous pulmonary venous return and pulmonary veinstenosis], and complex CHD); (3) tissue characterizationand viability imaging (including evaluation of cardiacmasses and tumors, evaluation of cardiomyopathiesand myocarditis, and evaluation of ischemic tissue or fi-brosis using delayed enhancement sequences); (4)hemodynamic data (including quantification of pulmo-nary to systemic blood flow ratio when assessing shuntlesions, right and left ventricular ejection fraction, andassessment of valvular regurgitation and stenosis); (5)extracardiac thoracic anatomy (including complex vas-cular anatomy, extracardiac masses, airway compression,and lung disease); and (6) postoperative assessment afterCHD surgery. (19)
Myocardial Ventricular Volume, Mass, andFunction
CMRI remains the gold standard for quantification ofventricular volumetrics and function, predominantly be-cause of its ability to measure acquired images withoutthe need for any geometric assumptions. (18) This is es-pecially useful in newborns with complex CHD, such ashypoplastic right or left heart syndrome or an unbalancedatrioventricular septal defect with borderline chambersizes. The actual chamber volume thresholds determineadequacy for a single-ventricle vs a biventricular or 1½-ventricle repair. (20)(21)(22)
The general approach involves acquiring multiplecine sections in the short-axis plane of the ventriclesand tracing both the epicardial and endocardial marginsin systole and diastole. The volumes and ejection frac-tions are then calculated using the Simpson method.This method allows for accurate and reproducible calcu-lations of the ejection fraction, and the cine loops pro-vide an extremely useful visual impression of overallcardiac function and wall motion (Video 7). The appli-cations of CMRI are multifold, and it remains the stan-dard for diagnosing cardiomyopathies (Videos 8–10 andFigs 9 and 10), especially in older children because theneonatal presentations of such diseases are rare. (23)(24)(25)
Video 12. Cine magnetic resonance image of the same patientin Fig 11 showing a discrete focal coarctation with poststenoticdilation. Click here to play the video.
Video 11. Three-dimensional reconstruction of the samepatient in Fig 11. Click here to play the video.
cardiology / cardiac MRI and CT imaging
e370 NeoReviews Vol.16 No.6 June 2015
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from

Cardiac Morphologic Findings in Complex CHDIn complex CHD, even though the cardiac anatomy isusually easily delineated using echocardiography, thereare multiple situations wherein CMRI is required for fur-ther enhancement of the diagnosis. In our center, whereCTA is used to delineate extracardiac anomalies, we tendto use CMRI in the neonatal period for evaluating a com-bination of both complex intracardiac and extracardiaclesions. CMRI is extremely helpful in these situations,and it also provides the additional benefit of obtaininginformation about abdominal and thoracic visceraand other associated anomalies, as well as functionalinformation.
AORTIC ARCH ANOMALIES. In the newborn period,echocardiography is usually a very good tool for assessingfor aortic arch anomalies. Major anomalies in neonatesconsist of a CoA, vascular rings or slings, or a double aor-tic arch. Suspicion based on initial evaluation needs con-firmation with advanced imaging. In this case, CMRI canbe beneficial with the major limitations of longer scantime and need for sedation to diminish breathing or mo-tion artifact, adding potential risks. At our center, we pre-fer to use CTA for the assessment of a neonate witha diagnosis of neonatal arch anomalies. CMRI, however,remains a mainstay of assessing aortic arch defects in older
children (Fig 11). Videos 11 and 12 show a child witha significant recoarctation with collateral formation aftera previous end-to-end CoA repair.
RIGHT VENTRICULAR OUTFLOW TRACT AND PULMONARY
ARTERY ANOMALIES. In cases with duct-dependentpulmonary blood flow (especially TOF and pulmonaryatresia), it is essential to assess the source of pulmonaryblood flow. The presence and size of MAPCAS (Fig 12)and the size and confluence of the pulmonary arterieshave an effect on the surgical repair and prognosis.(26)(27)(28) In our center, we have selectively usedCMRI with magnetic resonance angiography to delineatethe right ventricular outflow tract, branch pulmonary ar-teries (Fig 13), and MAPCAS, while dynamically assess-ing biventricular function and relative branch pulmonaryartery flow using differential flow quantification.
ANOMALIES OF PULMONARY VENOUS RETURN. As de-scribed previously, infants with infradiaphragmatic TAPVRusually require emergency surgery. In this scenario, longerscan times or additional procedures that involve sedationand intubation can be detrimental. In our center, CTAis often used to establish this diagnosis. Patients with
Figure 13. Magnetic resonance angiogram showing a rightpulmonary artery (RPA) arising from the patent ductus arterio-sus (PDA) and discontinuous from the left pulmonary artery ina patient with tetralogy of Fallot and pulmonary atresia.
Figure 12. Cardiac magnetic resonance image showing anaortopulmonary collateral in a newborn with tetralogy ofFallot and pulmonary atresia arising from the descendingaorta and supplying the left lung.
cardiology / cardiac MRI and CT imaging
NeoReviews Vol.16 No.6 June 2015 e371
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from
PAPVRmay be asymptomatic and may not have their con-ditions diagnosed until adolescence or adulthood after pre-senting with unexplained right heart enlargement. CMRI is
extremely useful for such cases and accurately reveals theanomalous drainage of one or more pulmonary veins intoanother systemic venous structure while providing addi-tional information about right heart dimensions and shuntfraction (Videos 13 and 14).
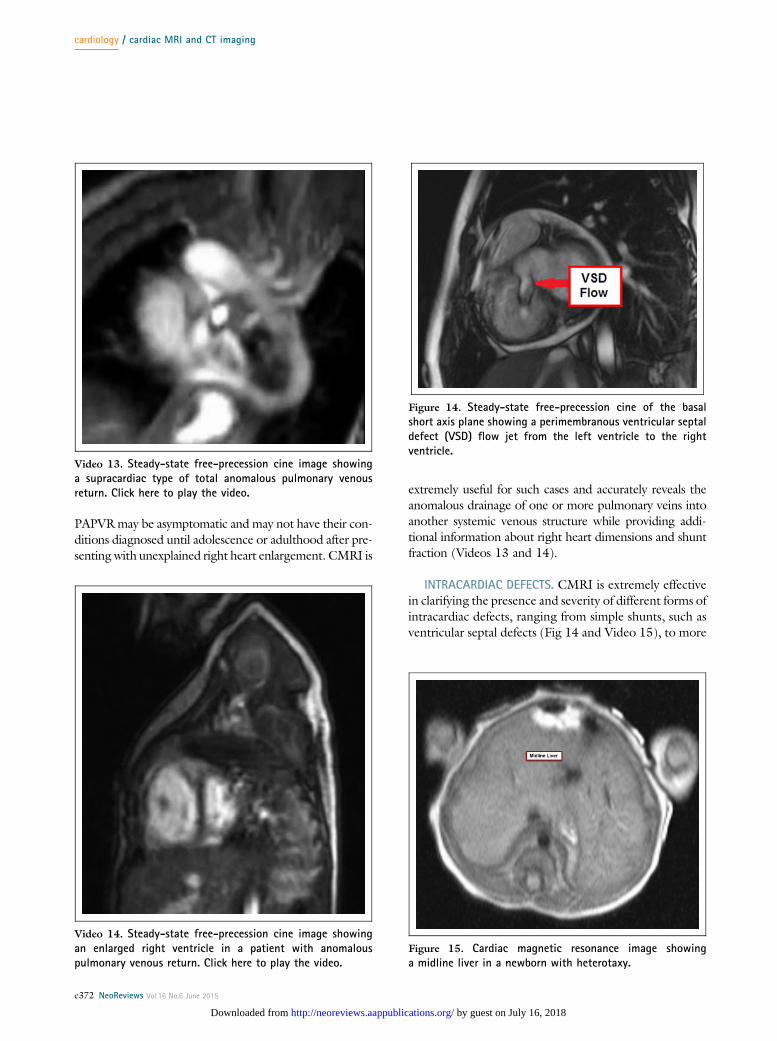
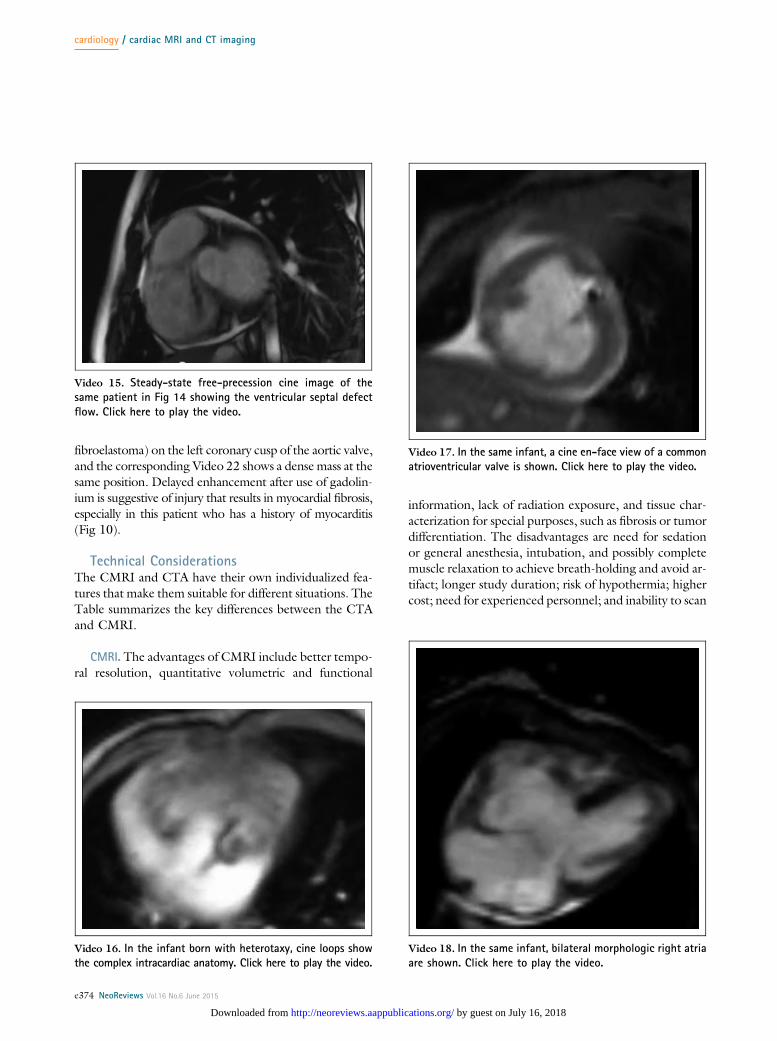
INTRACARDIAC DEFECTS. CMRI is extremely effectivein clarifying the presence and severity of different forms ofintracardiac defects, ranging from simple shunts, such asventricular septal defects (Fig 14 and Video 15), to more
Video 13. Steady-state free-precession cine image showinga supracardiac type of total anomalous pulmonary venousreturn. Click here to play the video.
Video 14. Steady-state free-precession cine image showingan enlarged right ventricle in a patient with anomalouspulmonary venous return. Click here to play the video.
Figure 14. Steady-state free-precession cine of the basalshort axis plane showing a perimembranous ventricular septaldefect (VSD) flow jet from the left ventricle to the rightventricle.
Figure 15. Cardiac magnetic resonance image showinga midline liver in a newborn with heterotaxy.
cardiology / cardiac MRI and CT imaging
e372 NeoReviews Vol.16 No.6 June 2015
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from
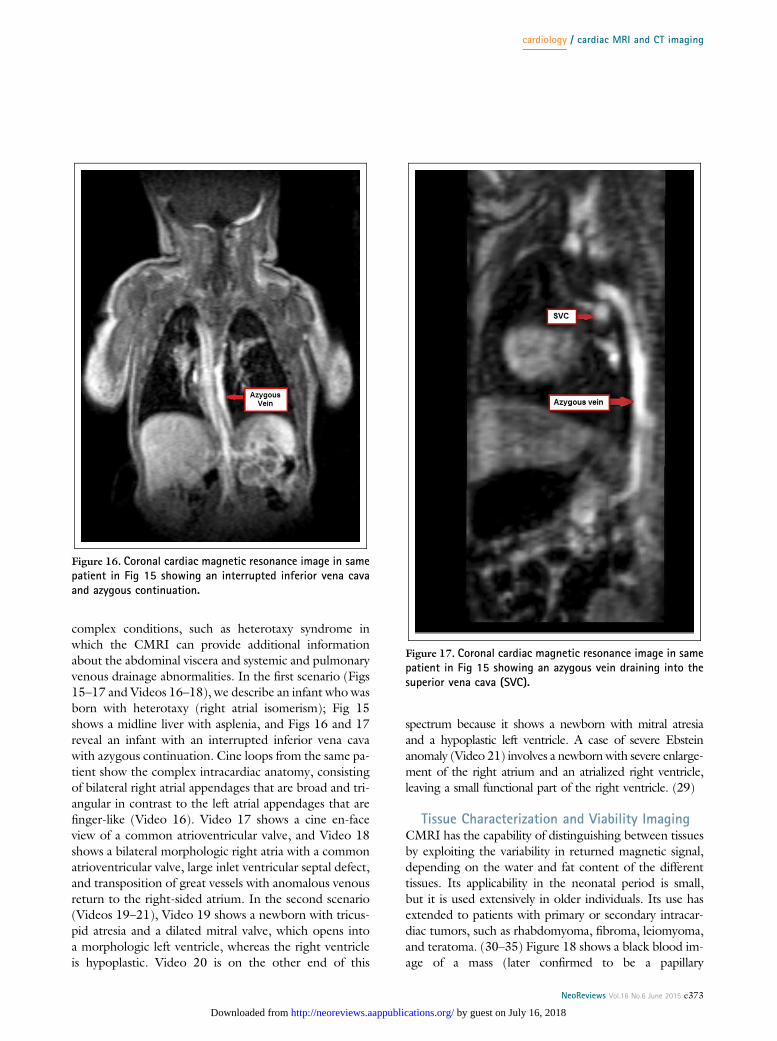
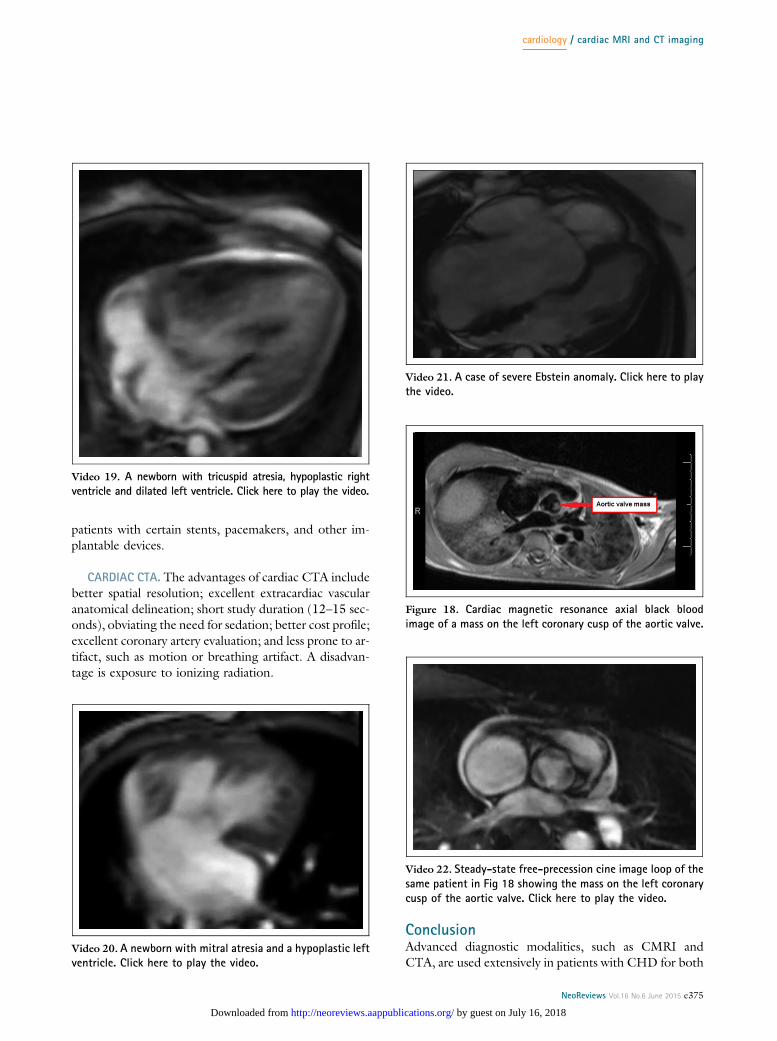
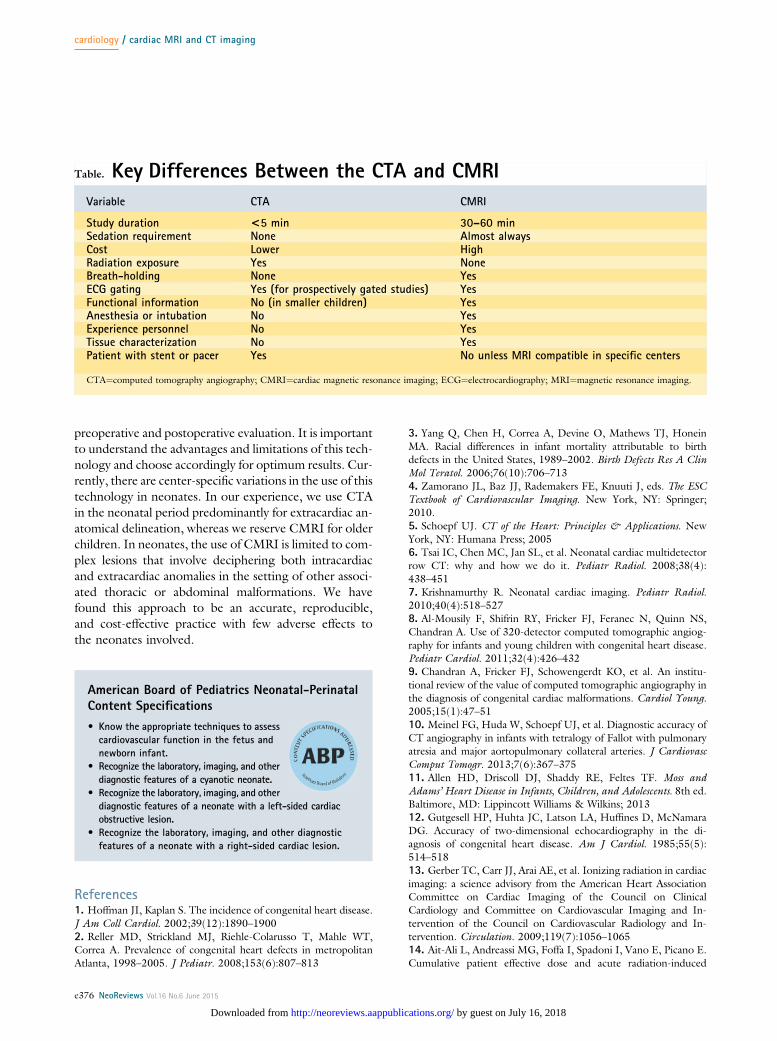
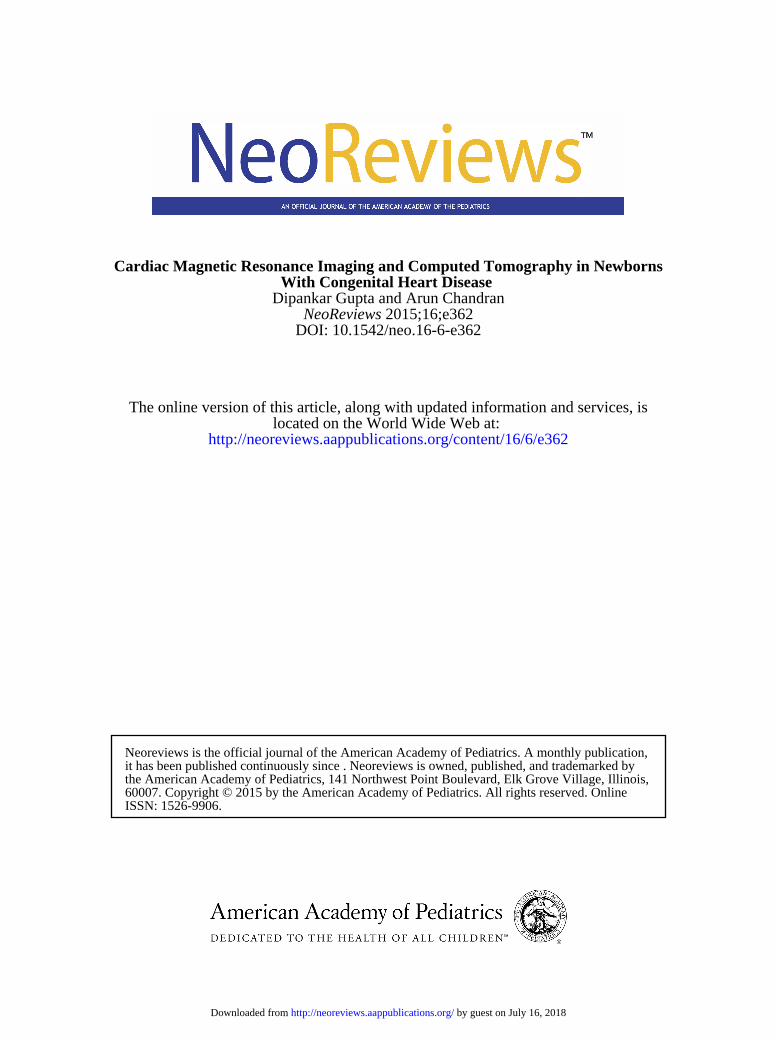
complex conditions, such as heterotaxy syndrome inwhich the CMRI can provide additional informationabout the abdominal viscera and systemic and pulmonaryvenous drainage abnormalities. In the first scenario (Figs15–17 and Videos 16–18), we describe an infant who wasborn with heterotaxy (right atrial isomerism); Fig 15shows a midline liver with asplenia, and Figs 16 and 17reveal an infant with an interrupted inferior vena cavawith azygous continuation. Cine loops from the same pa-tient show the complex intracardiac anatomy, consistingof bilateral right atrial appendages that are broad and tri-angular in contrast to the left atrial appendages that arefinger-like (Video 16). Video 17 shows a cine en-faceview of a common atrioventricular valve, and Video 18shows a bilateral morphologic right atria with a commonatrioventricular valve, large inlet ventricular septal defect,and transposition of great vessels with anomalous venousreturn to the right-sided atrium. In the second scenario(Videos 19–21), Video 19 shows a newborn with tricus-pid atresia and a dilated mitral valve, which opens intoa morphologic left ventricle, whereas the right ventricleis hypoplastic. Video 20 is on the other end of this
spectrum because it shows a newborn with mitral atresiaand a hypoplastic left ventricle. A case of severe Ebsteinanomaly (Video 21) involves a newborn with severe enlarge-ment of the right atrium and an atrialized right ventricle,leaving a small functional part of the right ventricle. (29)
Tissue Characterization and Viability ImagingCMRI has the capability of distinguishing between tissuesby exploiting the variability in returned magnetic signal,depending on the water and fat content of the differenttissues. Its applicability in the neonatal period is small,but it is used extensively in older individuals. Its use hasextended to patients with primary or secondary intracar-diac tumors, such as rhabdomyoma, fibroma, leiomyoma,and teratoma. (30–35) Figure 18 shows a black blood im-age of a mass (later confirmed to be a papillary
Figure 16. Coronal cardiac magnetic resonance image in samepatient in Fig 15 showing an interrupted inferior vena cavaand azygous continuation.
Figure 17. Coronal cardiac magnetic resonance image in samepatient in Fig 15 showing an azygous vein draining into thesuperior vena cava (SVC).
cardiology / cardiac MRI and CT imaging
NeoReviews Vol.16 No.6 June 2015 e373
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from
fibroelastoma) on the left coronary cusp of the aortic valve,and the corresponding Video 22 shows a dense mass at thesame position. Delayed enhancement after use of gadolin-ium is suggestive of injury that results in myocardial fibrosis,especially in this patient who has a history of myocarditis(Fig 10).
Technical ConsiderationsThe CMRI and CTA have their own individualized fea-tures that make them suitable for different situations. TheTable summarizes the key differences between the CTAand CMRI.
CMRI. The advantages of CMRI include better tempo-ral resolution, quantitative volumetric and functional
information, lack of radiation exposure, and tissue char-acterization for special purposes, such as fibrosis or tumordifferentiation. The disadvantages are need for sedationor general anesthesia, intubation, and possibly completemuscle relaxation to achieve breath-holding and avoid ar-tifact; longer study duration; risk of hypothermia; highercost; need for experienced personnel; and inability to scan
Video 15. Steady-state free-precession cine image of thesame patient in Fig 14 showing the ventricular septal defectflow. Click here to play the video.
Video 16. In the infant born with heterotaxy, cine loops showthe complex intracardiac anatomy. Click here to play the video.
Video 17. In the same infant, a cine en-face view of a commonatrioventricular valve is shown. Click here to play the video.
Video 18. In the same infant, bilateral morphologic right atriaare shown. Click here to play the video.
cardiology / cardiac MRI and CT imaging
e374 NeoReviews Vol.16 No.6 June 2015
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from
patients with certain stents, pacemakers, and other im-plantable devices.
CARDIAC CTA. The advantages of cardiac CTA includebetter spatial resolution; excellent extracardiac vascularanatomical delineation; short study duration (12–15 sec-onds), obviating the need for sedation; better cost profile;excellent coronary artery evaluation; and less prone to ar-tifact, such as motion or breathing artifact. A disadvan-tage is exposure to ionizing radiation.
ConclusionAdvanced diagnostic modalities, such as CMRI andCTA, are used extensively in patients with CHD for both
Video 19. A newborn with tricuspid atresia, hypoplastic rightventricle and dilated left ventricle. Click here to play the video.
Video 20. A newborn with mitral atresia and a hypoplastic leftventricle. Click here to play the video.
Video 21. A case of severe Ebstein anomaly. Click here to playthe video.
Figure 18. Cardiac magnetic resonance axial black bloodimage of a mass on the left coronary cusp of the aortic valve.
Video 22. Steady-state free-precession cine image loop of thesame patient in Fig 18 showing the mass on the left coronarycusp of the aortic valve. Click here to play the video.
cardiology / cardiac MRI and CT imaging
NeoReviews Vol.16 No.6 June 2015 e375
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from
preoperative and postoperative evaluation. It is importantto understand the advantages and limitations of this tech-nology and choose accordingly for optimum results. Cur-rently, there are center-specific variations in the use of thistechnology in neonates. In our experience, we use CTAin the neonatal period predominantly for extracardiac an-atomical delineation, whereas we reserve CMRI for olderchildren. In neonates, the use of CMRI is limited to com-plex lesions that involve deciphering both intracardiacand extracardiac anomalies in the setting of other associ-ated thoracic or abdominal malformations. We havefound this approach to be an accurate, reproducible,and cost-effective practice with few adverse effects tothe neonates involved.
References1. Hoffman JI, Kaplan S. The incidence of congenital heart disease.J Am Coll Cardiol. 2002;39(12):1890–19002. Reller MD, Strickland MJ, Riehle-Colarusso T, Mahle WT,Correa A. Prevalence of congenital heart defects in metropolitanAtlanta, 1998–2005. J Pediatr. 2008;153(6):807–813
3. Yang Q, Chen H, Correa A, Devine O, Mathews TJ, HoneinMA. Racial differences in infant mortality attributable to birthdefects in the United States, 1989–2002. Birth Defects Res A ClinMol Teratol. 2006;76(10):706–7134. Zamorano JL, Baz JJ, Rademakers FE, Knuuti J, eds. The ESCTextbook of Cardiovascular Imaging. New York, NY: Springer;2010.5. Schoepf UJ. CT of the Heart: Principles & Applications. NewYork, NY: Humana Press; 20056. Tsai IC, Chen MC, Jan SL, et al. Neonatal cardiac multidetectorrow CT: why and how we do it. Pediatr Radiol. 2008;38(4):438–4517. Krishnamurthy R. Neonatal cardiac imaging. Pediatr Radiol.2010;40(4):518–5278. Al-Mousily F, Shifrin RY, Fricker FJ, Feranec N, Quinn NS,Chandran A. Use of 320-detector computed tomographic angiog-raphy for infants and young children with congenital heart disease.Pediatr Cardiol. 2011;32(4):426–4329. Chandran A, Fricker FJ, Schowengerdt KO, et al. An institu-tional review of the value of computed tomographic angiography inthe diagnosis of congenital cardiac malformations. Cardiol Young.2005;15(1):47–5110. Meinel FG, Huda W, Schoepf UJ, et al. Diagnostic accuracy ofCT angiography in infants with tetralogy of Fallot with pulmonaryatresia and major aortopulmonary collateral arteries. J CardiovascComput Tomogr. 2013;7(6):367–37511. Allen HD, Driscoll DJ, Shaddy RE, Feltes TF. Moss andAdams’ Heart Disease in Infants, Children, and Adolescents. 8th ed.Baltimore, MD: Lippincott Williams & Wilkins; 201312. Gutgesell HP, Huhta JC, Latson LA, Huffines D, McNamaraDG. Accuracy of two-dimensional echocardiography in the di-agnosis of congenital heart disease. Am J Cardiol. 1985;55(5):514–51813. Gerber TC, Carr JJ, Arai AE, et al. Ionizing radiation in cardiacimaging: a science advisory from the American Heart AssociationCommittee on Cardiac Imaging of the Council on ClinicalCardiology and Committee on Cardiovascular Imaging and In-tervention of the Council on Cardiovascular Radiology and In-tervention. Circulation. 2009;119(7):1056–106514. Ait-Ali L, Andreassi MG, Foffa I, Spadoni I, Vano E, Picano E.Cumulative patient effective dose and acute radiation-induced
Table. Key Differences Between the CTA and CMRI
Variable CTA CMRI
Study duration <5 min 30–60 minSedation requirement None Almost alwaysCost Lower HighRadiation exposure Yes NoneBreath-holding None YesECG gating Yes (for prospectively gated studies) YesFunctional information No (in smaller children) YesAnesthesia or intubation No YesExperience personnel No YesTissue characterization No YesPatient with stent or pacer Yes No unless MRI compatible in specific centers
CTA¼computed tomography angiography; CMRI¼cardiac magnetic resonance imaging; ECG¼electrocardiography; MRI¼magnetic resonance imaging.
American Board of Pediatrics Neonatal-PerinatalContent Specifications
• Know the appropriate techniques to assesscardiovascular function in the fetus andnewborn infant.
• Recognize the laboratory, imaging, and otherdiagnostic features of a cyanotic neonate.
• Recognize the laboratory, imaging, and otherdiagnostic features of a neonate with a left-sided cardiacobstructive lesion.
• Recognize the laboratory, imaging, and other diagnosticfeatures of a neonate with a right-sided cardiac lesion.
cardiology / cardiac MRI and CT imaging
e376 NeoReviews Vol.16 No.6 June 2015
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from

chromosomal DNA damage in children with congenital heartdisease. Heart. 2010;96(4):269–27415. Andreassi MG. Radiation risk from pediatric cardiac catheter-ization: friendly fire on children with congenital heart disease.Circulation. 2009;120(19):1847–184916. Andreassi MG, Foffa I, Manfredi S, Botto N, Cioppa A, PicanoE. Genetic polymorphisms in XRCC1, OGG1, APE1 and XRCC3DNA repair genes, ionizing radiation exposure and chromosomalDNA damage in interventional cardiologists. Mutat Res. 2009;666(1–2):57–6317. Pohost GM. The history of cardiovascular magnetic resonance.JACC Cardiovasc Imaging. 2008;1(5):672–67818. Fogel MA. Principles and Practice of Cardiac MagneticResonance in Congenital Heart Disease: Form, Function and Flow.Hoboken, NJ: Wiley-Blackwell Publishing; 201019. Weiss F, Habermann CR, Lilje C, et al. MRI in postoperativeassessment of univentricular heart disease: correlation with echo-cardiography and angiography [in German]. Rofo. 2002;174(12):1537–154320. Grosse-Wortmann L, Yun TJ, Al-Radi O, et al. Borderlinehypoplasia of the left ventricle in neonates: insights for decision-making from functional assessment with magnetic resonanceimaging. J Thorac Cardiovasc Surg. 2008;136(6):1429–143621. Fenchel M, Greil GF, Martirosian P, et al. Three-dimensionalmorphological magnetic resonance imaging in infants and children withcongenital heart disease. Pediatr Radiol. 2006;36(12):1265–127222. Van Arsdell GS, Williams WG, Freedom RM. A practical approachto 1½ ventricle repairs. Ann Thorac Surg. 1998;66(2):678–68023. Alpendurada F, O’Hanlon R, Prasad SK. Cardiovascularmagnetic resonance of cardiomyopathies. Curr Cardiol Rep.2009;11(1):61–6924. Moon JC, McKenna WJ. The emerging role of cardiovascularmagnetic resonance in refining the diagnosis of hypertrophiccardiomyopathy. Nat Clin Pract Cardiovasc Med. 2009;6(3):166–16725. Mavrogeni S, Sfendouraki E, Theodorakis G, Kolovou G. Diag-nosis, severity grading and prognosis of left ventricular non-compaction
using cardiovascular magnetic resonance. Int J Cardiol. 2013;167(2):598–59926. Kellenberger CJ, Yoo SJ, Büchel ER. Cardiovascular MRimaging in neonates and infants with congenital heart disease.Radiographics. 2007;27(1):5–1827. Holmqvist C, Hochbergs P, Björkhem G, Brockstedt S, LaurinS. Pre-operative evaluation with MR in tetralogy of Fallot andpulmonary atresia with ventricular septal defect. Acta Radiol. 2001;42(1):63–6928. Geva T, Greil GF, Marshall AC, Landzberg M, Powell AJ.Gadolinium-enhanced 3-dimensional magnetic resonance angiog-raphy of pulmonary blood supply in patients with complexpulmonary stenosis or atresia: comparison with x-ray angiography.Circulation. 2002;106(4):473–47829. Kastler B, Livolsi A, Zhu H, Roy E, Zollner G, Dietemann JL.Potential role of MR imaging in the diagnostic management ofEbstein anomaly in a newborn. J Comput Assist Tomogr. 1990;14(5):825–82730. Melo IS, Belo F, Gouveia R, Anjos R. Primary cardiacleiomyoma of the ventricular septum: a rare form of pediatricintracardiac tumor. Pediatr Cardiol. 2012;33(4):649–65131. Beroukhim RS, Prakash A, Buechel ER, et al. Characterizationof cardiac tumors in children by cardiovascular magnetic resonanceimaging: a multicenter experience. J Am Coll Cardiol. 2011;58(10):1044–105432. Christophe C, Bartholome J, Blum D, et al. Neonatal tuberoussclerosis. US, CT, and MR diagnosis of brain and cardiac lesions.Pediatr Radiol. 1989;19(6–7):446–44833. Kiaffas MG, Powell AJ, Geva T. Magnetic resonance imagingevaluation of cardiac tumor characteristics in infants and children.Am J Cardiol. 2002;89(10):1229–123334. Lund JT, Ehman RL, Julsrud PR, Sinak LJ, Tajik AJ. Cardiacmasses: assessment by MR imaging. AJR Am J Roentgenol. 1989;152(3):469–47335. Patel A, Rigsby C, Young L. Cardiac teratoma of theinterventricular septumwith congenital aortic stenosis in a newborn.Pediatr Cardiol. 2008;29(6):1126–1128
Answer Key for June 2015 NeoReviews:Genetic Basis of Congenital Heart Disease: 1. B; 2. E; 3. D; 4. C; 5. D.
Inotrope and Vasopressor Support in Neonates: 1. D; 2. B; 3. C; 4. A; 5. D.
Parent Resources from the AAP at HealthyChildren.org• http://www.healthychildren.org/English/health-issues/conditions/heart/Pages/Common-Heart-Defects.aspx (Englishonly)
cardiology / cardiac MRI and CT imaging
NeoReviews Vol.16 No.6 June 2015 e377
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from

DOI: 10.1542/neo.16-6-e3622015;16;e362NeoReviews
Dipankar Gupta and Arun ChandranWith Congenital Heart Disease
Cardiac Magnetic Resonance Imaging and Computed Tomography in Newborns
ServicesUpdated Information &
http://neoreviews.aappublications.org/content/16/6/e362including high resolution figures, can be found at:
Referenceshttp://neoreviews.aappublications.org/content/16/6/e362#BIBLThis article cites 31 articles, 4 of which you can access for free at:
Subspecialty Collections
_drug_labeling_updatehttp://classic.neoreviews.aappublications.org/cgi/collection/pediatricPediatric Drug Labeling Updatefollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
htmlhttp://classic.neoreviews.aappublications.org/site/misc/Permissions.xin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.neoreviews.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from
DOI: 10.1542/neo.16-6-e3622015;16;e362NeoReviews
Dipankar Gupta and Arun ChandranWith Congenital Heart Disease
Cardiac Magnetic Resonance Imaging and Computed Tomography in Newborns
http://neoreviews.aappublications.org/content/16/6/e362located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1526-9906. 60007. Copyright © 2015 by the American Academy of Pediatrics. All rights reserved. Online the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,it has been published continuously since . Neoreviews is owned, published, and trademarked by Neoreviews is the official journal of the American Academy of Pediatrics. A monthly publication,
by guest on July 16, 2018http://neoreviews.aappublications.org/Downloaded from