Embed Size (px)
Citation preview

Tobias S. Köhler, MD, MPH, FACSSouthern Illinois University – Springfield, IL
May 16, 2015

AMS, Coloplast, Abbvie – Consulting / Research
I will mention on-label and off-label use of medications by both generic and brand name during this talk
The use of off-labeled medications is not approved by the FDA and use of these medications will be up to the discretion of the treating practitioner based on clinical presentation and experience

What is a normal hormonal profile for ejaculation
Evaluation & Treatment Protocol
Practice Patterns and Outcomes of SMSNA
Medication Review

Testosterone o Androgen Receptors ubiquitous including in pelvic floor muscleso High T = premature & Low T = delayed in someo However T levels very widely in men with DE (one cohort of 2400 men
had a DE prevalence of 26%) Thyroid Hormone
o Similar to testosterone, high Thyroid levels = PE, low Thyroid levels = DE Prolactin
o May be a surrogate marker of serotonergic activityo High levels suppress testosterone and ejaculatory functiono Suppressed during climax, spikes after orgasm (likely at least in part
responsible for refractory period) Oxytocin
o Oxytocin surges during male ejaculation, orgasm and detumescencereturning to baseline by 10 minutes after surge
o Increases ejaculation, paternal nurturing, sexual desire, and long-term romantic bonds and attachments


Sex therapists report better success rates overall addressing underlying causal factors.
DE with concurrent ED should be treated with PDE5Is Vibratory Stimulation shown to be helpful (72% success with
three 1 minute rest/application cycles) Most helpful “drug effect” is switching away from SSRIs to
Bupropion (66%) All published studies use small samples, have no controls, are
nonrandomized and lack validated outcome measures. Disparities in outcomes likely reflect clinically different
treatment populations There is no FDA approved drug for treatment

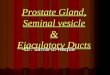
Normalization ofhypogonadism PDE5i for ED Sexual counseling PVS Medication adjustments
Always 4 5 4 1 8Mostly 24 35 30 16 58Seldom 58 45 50 46 26Never 7 9 9 26 2
0
10
20
30
40
50
60
70
Num
ber R
espo
nden
ts
How Successful Are These Treatments in the SMSNA?
30% 43% 37% 19% 70%

Alcohol Clomipramine Lorazepam PhentolamineAlprazolam Desmethylimipramine Mebanizine Phenylzine sulphate
Aminocaproic acid
Fluoxetine* Mesoridazine Prazosin
Amitriptyline Fluvoxamine Methadone Protriptyline
Amoxapine Guanadrel Methyldopa Reserpine
Baclofen Guanethidine Naproxen Sertraline*
Bethanidine Haloperidol Nortriptyline Thiazide diuretics
Butaperazine Hexamthonium Pargyline Thioridazine
Chlordiazepoxide Imiprimine Paroxetine* Trazadone
Chlorimipramine Iproniazid Perphenazine Trifluoperazine
Chlorpromazine Isocarboxazid Phenothiazine * All selective serotonin reuptake Inhibitors (SSRI’s = 7x risk of DE!)Chlorprothixine Labethanol Phenoxybenzamine

DrugGeneric / (Trade)
Delayed Ejaculation Dosage(Not FDA Approved) Indication
(FDA Approved)Side Effects
(At Therapeutic FDA Indication Dose)As needed Daily
Cyproheptadine^(Periactin)
4-12 mg (3-4 hours prior to sex)
--- • Allergic rhinitis• Urticarial• Anorexia nervosa
Nausea, dizziness, urinary retention, photosensitivity, rash, abdominal pain, fatigue, agranulocytosis, thrombocytopenia, heat stroke
Bethanechol^(Urecholine)
20mg po (1-2 hours prior to sex)
--- • Urinary Retention• Neurogenic bladder• GERD• TCA adjunct treatment• Phenothiazine adjunct Tx
Abdominal pain, nausea, diarrhea, headache, urinary urgency, malaise, flushing, miosis, broncospasm, hypotention, tachycardia, seizures
Amantadine^(Symmetrel)
100-400 mg (for 2 days prior to sex)
75-100 mg BID or TID
• Influenza A Tx and Prophylaxis
• Extrapyramidal sx• Parkinsonism
Nausea, dizziness, depression, anorexia, halluncinations, compulsivity, hypotension, abnormal dreams, headache, constipation/diarrhea, arrhythmias, psychosis, coma, impaired vision, pulmonary edema, neutropenia, seizure, heat stroke
Bupropion^(Wellbutrin, Zyban, Budeprion, Forfivo)
--- 75 mg BID or TID • Major Depressive disorder• Seasonal affective
disorder• Smoking cessation• Attention Deficit-
Hyperactivity Disorder (ADHD)
Palpitations, urinary frequency, blurred vision, chest pain, agitation, psychosis, hallucinations, seizures, hepatotoxicity, HTN, arrhythmias**Suicidality, Neuropsychiatric symptoms
Buspirone^(BuSpar)
--- 5-15 mg BID • Anxiety Dizziness, nausea, headache, fatigue, blurred vision, numbness, weakness, abdominal pain, insomnia, serotonin syndrome, tardive dyskinesia, dsytonia, hositity, depression
Loratadine^(Claritin, Alavert)
--- 10 mg daily • Allergic rhinitis• Chronic idiopathic urticaria
Drowsiness, fatigue, headache, dry mucous membranes, pharyngitis, bronchospasm, hepatotoxicity, syncope, seizures, thrombocytopenia
Bold terms represent more common reactions Un-bolded terms represent serious reactions** Black Box Warning# None of these drugs are FDA approved for Delayed Ejaculation
DE TREATMENT MEDS WITH SSRI USE

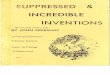
Cabergoline Buproprion Oxytocin Cyproheptadine Buspirone Yohimbine Methylphenid
ate Amantadine Midodrine
First Line 14 11 6 5 1 1 1 0 0Frequently 10 6 5 0 2 1 1 2 1Occassionally 15 13 6 4 11 2 4 2 1Rarely 5 15 12 13 10 6 6 10 10Never 41 39 52 57 58 69 67 65 65
0
10
20
30
40
50
60
70
80
Num
ber o
f Res
pond
ents
What Medications Do Members of the SMSNA Use?

First Line Meds used by SMSNA

DrugGeneric / (Trade)
Delayed Ejaculation Dosage(Not FDA Approved)
Indication(FDA Approved)
Side Effects(At Therapeutic FDA Indication Dose)
As needed DailyOxytocin†
(Pitocin)24 IU intranasal during sex or SL prior to sex
--- • Labor induction• Abortion adjunct• Postpartum hemorrhage
Nausea, vomiting, hypertension, afibrinogenemia, SAIDH**Not for elective labor induction
Pseudoephedrine*(Sudafed)
60-120 mg (120-150 min prior to sex)
--- • Nasal congestion Insomnia, anxiety, nausea, insomnia, tremor, urinary retention, headache, palpitations, arrhythmias, hypertension
Ephedrine* 15-60 mg (1 hour prior to sex)
--- • Acute bronchospasm• Hypotension
Nausea, headache, dizziness, insomnia, hypertension, tremor, urinary retention, anxiety, palpitations, arrhythmias, stroke, seizures, MI, nephrotoxicity, hepatotoxicity
Midodrine*(Orvaten, ProAmatine)
5-40mg daily (30-120 min. prior to sex)
--- • Orthostatic Hypotension Dysuria, paresthesia, rigors, pruittus, piloerection, rash,bradycardia, erythema multiforme, visual field defect** Supine Elevated Blood Pressure
Apomorphine(Apokyn)
0.5-1.5mg Intranasal (20min before sex)
--- • Parkinson Ds Yawning, dyskinesia, rhinorrhea, hallucinations, anxiety, UTI, chest pain, diaphoresis, hypotension, syncope, MI, Priapism, abuse potential, hallucinations
Yohimbine(Yocon)
--- 5.4 mg TID • Impotence Urinary retention, hyperglycemia, tachycardia, irritability, tremor, nausea, dizziness, headache, flushing, diaphoresis, hypertension, respiratory depression
Cabergoline†
(Dostinex)--- 0.25-2 mg twice a
week• Hyperprolactinemia Nausea, dizziness, fatigue, abdominal pain, somnolence,
anxiety, vertigo hot flashes, flatulence, breast pain, compulsivity, orthostatic hypotension, pleural effusion, retroperitoneal fibrosis, depression, psychosis, pulmonary and pericardial fibrosis
Roboxetine(not available in USA)
--- 4-8 mg • Major depressive disorder• Panic Disorder• Attention deficit-
hyperactivity disorder (ADHD)
Insomnia, nausea, excessive sweating, constipation, urinary tract infection, dysuria, urinary retention, ejaculatory pain,tachycardia, blood pressure changes
Imipramine*(Tofranil)
--- 25-75mg daily • Depression• Chronic pain
Drowsiness, dizziness, blurred vision, palpitations, increase appetite, weakness, confusion, anxiety, impotence, galactorrhea, gynecomastia, photosensitivity, change in libido, hypotension, syncope, QT Prolongation, AV block, MI, stroke, seizures, ataxia, leukopenia, hallucinations, depression, hepatitis, angioedema, heat stroke, psychosis, withdrawal symptoms**Suicidality
Bold terms represent more common reactions and un-bolded terms represent serious reactions† May help when abnormalities of Prolactin or other hormonal issues considered* Known to help with retrograde ejaculation** Black Box Warning
DE TREATMENT MEDS (NO SSRI USE)

If patient is on SSRIo If possible switch to Bupropion 75 mg PO BID or TID
• Watch for palpitations, chest pain, blurred vision, SUICIDALITY**o If switching not possible, try cyproheptadine 4-12 mg 3-4 hrs before sex
• Watch for nausea, dizziness, urinary retention, photosensitivity, rash, abdominal pain, fatigue
o Next line try loratidine 10 mg po qday, watch for drowsiness, fatigue, headache, dry mucous membranes, pharyngitis
If patient is not on SSRI measure prolactino If prolactin high/high normal try cabergoline 0.25-2 mg po 2/week
• Watch for nausea, dizziness, fatigue, abdominal pain, somnolence, anxietyo If prolactin low/low normal try oxytocin 24 IU/SL intranasal prior to sex
Back up agents (can be used in combination)o Yohimbine 5.4 mg po TID (cheap and easy)
• Watch for urinary retention, hyperglycemia, tachycardia, irritability, tremor, nausea, dizziness, headache, flushing, diaphoresis, hypertension


Lue, T.F., et al., Sexual medicine : sexual dysfunctions in men and women. Chapter 13: Disorders of Orgasm and Ejaculation in Men, ed. C.G. McMahon, et al. 2004, Plymouth: Health publications. 409-68.
McMahon, C.G., et al., Standard operating procedures in the disorders of orgasm and ejaculation. J Sex Med, 2013. 10(1): p. 204-29. Richardson, D., A. Nalabanda, and D. Goldmeier, Retarded ejaculation - a review. Int J STD AIDS, 2006. 17(3): p. 143-50. Porst, H., J. Buvat, and Standards Committee of the International Society for Sexual Medicine, Standard practice in sexual medicine. Chapter 16 - Ejaculatory Disorders, ed. C.G. McMahon, et al.
2006, Malden, Mass. ; Oxford: Blackwell Pub. 188-209. Mulhall, J.P. and W. Hsiao, Men's sexual health and fertility : a clinician's guide. Chapter 9 - Delayed Ejaculation and Orgasm, ed. C.J. Nelson, D. Brock, and R.C. Dean. 2014: Springer. pages cm. Rowland, D., et al., Disorders of orgasm and ejaculation in men. J Sex Med, 2010. 7(4 Pt 2): p. 1668-86. Jannini, E.A., C. Simonelli, and A. Lenzi, Disorders of ejaculation. J Endocrinol Invest, 2002. 25(11): p. 1006-19. Corona, G., et al., Different testosterone levels are associated with ejaculatory dysfunction. J Sex Med, 2008. 5(8): p. 1991-8. Corona, G., et al., The hormonal control of ejaculation. Nat Rev Urol, 2012. 9(9): p. 508-19. Paduch, D., et al., Effects of testosterone solution 2% for the treatment of ejauclatory dysfunction in androgen-deficient men. 20th Annual Fall Scientific Meeting of SMSNA, November 20-23, 2014
Program Book, 2014(Abtract 003): p. 53. Paduch, D., et al., Prevalence of ejaculatory dysfunction as a function of testosterone. 20th Annual Fall Scientific Meeting of SMSNA, November 20-23, 2014 Program Book, 2014(Abstract 004): p. 52. Paduch, D., et al., Preceived sexual dissatisfaction with ejaculatory dysfunctions. 20th Annual Fall Scientific Meeting of SMSNA, November 20-23, 2014 Program Book, 2014(Abstract 005): p. 53. Carani, C., et al., Multicenter study on the prevalence of sexual symptoms in male hypo- and hyperthyroid patients. J Clin Endocrinol Metab, 2005. 90(12): p. 6472-9. Corona, G., et al., Sexual dysfunction in subjects with Klinefelter's syndrome. Int J Androl, 2010. 33(4): p. 574-80. Fitzgerald, P. and T.G. Dinan, Prolactin and dopamine: what is the connection? A review article. J Psychopharmacol, 2008. 22(2 Suppl): p. 12-9. Kruger, T.H., U. Hartmann, and M. Schedlowski, Prolactinergic and dopaminergic mechanisms underlying sexual arousal and orgasm in humans. World J Urol, 2005. 23(2): p. 130-8. Corona, G., et al., Selective serotonin reuptake inhibitor-induced sexual dysfunction. J Sex Med, 2009. 6(5): p. 1259-69. Kiev, A. and A. Feiger, A double-blind comparison of fluvoxamine and paroxetine in the treatment of depressed outpatients. J Clin Psychiatry, 1997. 58(4): p. 146-52. Butcher, M., et al., Delayed ejcaultion remains a recalcitrant condition: Results of a SMSNA survey. 20th Annual Fall Scientific Meeting of SMSNA, November 20-23, 2014 Program Book,
2014(Abstract 041): p. 70. Aukst-Margetic, B. and B. Margetic, An open-label series using loratadine for the treatment of sexual dysfunction associated with selective serotonin reuptake inhibitors. Prog Neuropsychopharmacol
Biol Psychiatry, 2005. 29(5): p. 754-6. Shin, D. and A. Spitz, The Evaluation and Treatment of Delayed Ejaculation. Sexual Medicine Reviews, 2014. 2((3-4)): p. 121-133. Menendez Abraham, E., et al., Modifications of the sexual activity in male rats following administration of antiserotoninergic drugs. Behav Brain Res, 1988. 30(3): p. 251-8. Ashton, A.K., R. Hamer, and R.C. Rosen, Serotonin reuptake inhibitor-induced sexual dysfunction and its treatment: a large-scale retrospective study of 596 psychiatric outpatients. J Sex Marital Ther,
1997. 23(3): p. 165-75. DeBattista, C., et al., A placebo-controlled, randomized, double-blind study of adjunctive bupropion sustained release in the treatment of SSRI-induced sexual dysfunction. J Clin Psychiatry, 2005.
66(7): p. 844-8. Veening, J.G., et al., The role of oxytocin in male and female reproductive behavior. Eur J Pharmacol, 2014. Ashton, A.K. and R.C. Rosen, Bupropion as an antidote for serotonin reuptake inhibitor-induced sexual dysfunction. J Clin Psychiatry, 1998. 59(3): p. 112-5. Melnyk, J. and M. Marcone, Aphrodisiacs from plant and animal sources—A review of current scientific literature. Food Research International, 2011. 44: p. 840-850. Sadowski et al. How is Delayed Ejaculation Treated in North America, Andrology, In Press Butcher et al, Delayed Ejaculation, a condition whose time has come, AUA Updates 2015, In Press