Embed Size (px)
Citation preview
South West Regional Wound Care Toolkit
SWRWC Toolkit B.2.1 Lower Leg Assessment: Purpose and Instructions_July-10_2011
1
B. 2. INTERDISCIPLINARY LOWER LEG ASSESSMENT
2.1 Purpose and Instructions for the Lower leg Assessment Tool
Purpose
This tool is to assist the nurse in assessment of the lower leg and in particular, to identify and document
any abnormality of the lower leg and contains recommendations for actions based on abnormal
findings.
Instructions
Please include the individual’s demographics at the top right hand corner of the tool, either with an
identifier sticker/addressograph or by printing the information in by hand.
Sections a-l: This is to be used by a qualified health care professional (see Competency Levels in
Introduction to Toolkit) to do a thorough assessment of the lower leg when an ulcer is present and/or
when peripheral or arterial issues are noted.
Sections m- p: A Wound Care Specialist is required to complete. While a Wound Care Specialist nurse
may not diagnose, they can assess characteristics to allow them to request further investigations in
order for the physician to form a definitive diagnosis.
Please note: Patient permission was received to use all photos contained in this document for
educational purposes.
a. Ulcer or pre-ulcerous conditions
Please add the history of previous ulcer(s) and date of onset of the new ulcer(s)/pre-ulcerous
condition(s). If there are numerous sites, please list. Use the tick boxes to identify characteristics of the
ulcer and surrounding skin.
b. Pain (specific to legs)
Check off the box that identifies the type of pain the patient is experiencing. If pain is uncontrolled use
the tick box to indicate that you are requesting or referring to pain specialist to address control.
Pain occurs in as much as 76% of venous ulcers. Deep ulcers, particularly those around the malleolus, or
small ulcers surrounded by atrophie blanche are the most painful.
.

South West Regional Wound Care Toolkit
SWRWC Toolkit B.2.1 Lower Leg Assessment: Purpose and Instructions_July-10_2011
2
c. Foot Deformities, Nails and Footwear
Use the check boxes to check off all those that apply when examining the foot
Foot Deformities
Description Examples
Hammer toes - in a hammertoe
deformity, the first joint (MTP) is
cocked upward, and the middle joint
(PIP) bends downward.
Illustration used with permission of artist Nancy Bauer
and the Registered Nurses’ Association of Ontario
(2005). Assessment & Management of Foot Ulcers for
People with Diabetes. Toronto, Canada: Registered
Nurses’ Association of Ontario.
Hallux valgus (bunion deformity) –
occurs when the great toe begins to
deviate, developing a firm bump on the
inside edge of the foot. It is not painful
at first, but when the toes deviate even
more, redness, swelling and pain at or
near the joint occur. The pain is caused
by pressure of the footwear on the
bunion or from the pressure inside the
joint. Hallux valgus describes the
change in position of the toe, and
bunion describes the bump on the foot.
http://www.epodiatry.com/bunion.htm Illustration used with permission of artist Nancy Bauer
and the Registered Nurses’ Association of Ontario
(2005). Assessment & Management of Foot Ulcers for
People with Diabetes. Toronto, Canada: Registered
Nurses’ Association of Ontario.
Fixed ankle joint- Fibrous or bony
ankylosis at the ankle can occur
because of immobility (joint assumes
the least painful position and becomes
fixed). In venous insufficiency, fibrotic
tissue deposits due to
lipodermatosclerosis also decrease
ankle mobility—lose ability to dorsiflex.
This decreases the chance of healing by
70%.
No illustration available
Hallus Valgus or Large
Bunion (Severe) –big toe
may move under
second toe
Halgus Valgus or Small
Bunion(Mild/Moderate)
– joint at the base of big
toeis pushed to the side
South West Regional Wound Care Toolkit
SWRWC Toolkit B.2.1 Lower Leg Assessment: Purpose and Instructions_July-10_2011
3
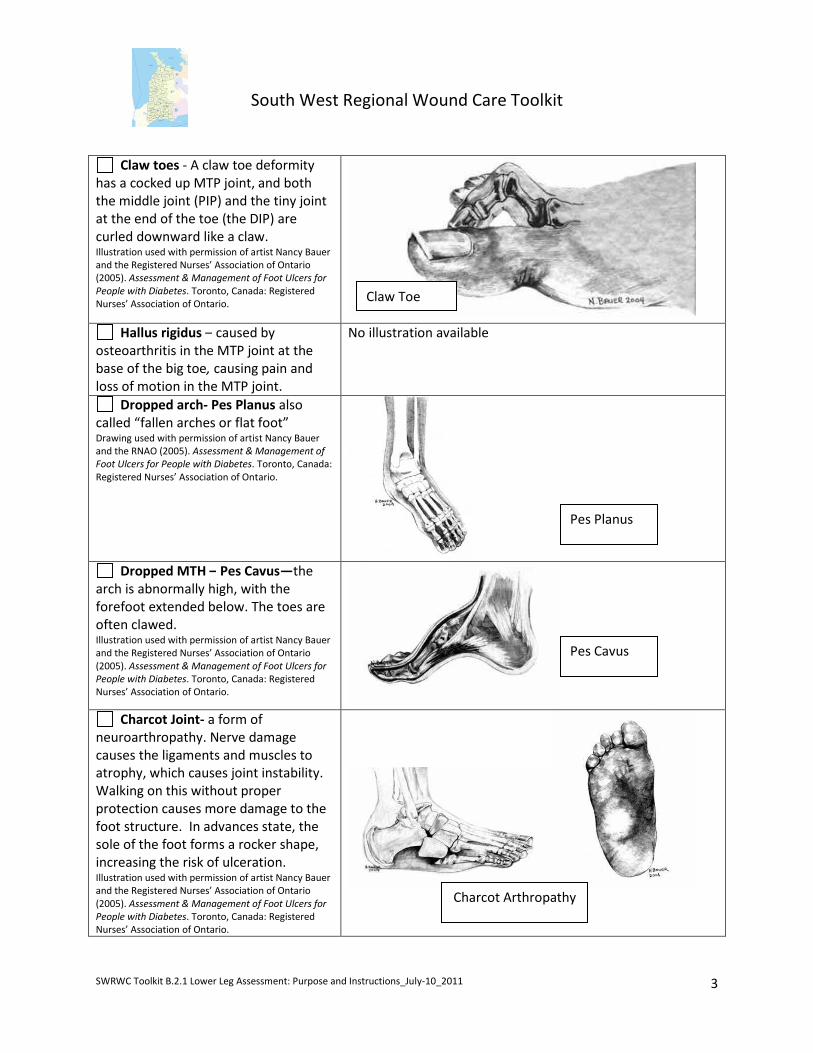
Claw toes - A claw toe deformity
has a cocked up MTP joint, and both
the middle joint (PIP) and the tiny joint
at the end of the toe (the DIP) are
curled downward like a claw. Illustration used with permission of artist Nancy Bauer
and the Registered Nurses’ Association of Ontario
(2005). Assessment & Management of Foot Ulcers for
People with Diabetes. Toronto, Canada: Registered
Nurses’ Association of Ontario.
Hallus rigidus – caused by
osteoarthritis in the MTP joint at the
base of the big toe, causing pain and
loss of motion in the MTP joint.
No illustration available
Dropped arch- Pes Planus also
called “fallen arches or flat foot” Drawing used with permission of artist Nancy Bauer
and the RNAO (2005). Assessment & Management of
Foot Ulcers for People with Diabetes. Toronto, Canada:
Registered Nurses’ Association of Ontario.
Dropped MTH – Pes Cavus—the
arch is abnormally high, with the
forefoot extended below. The toes are
often clawed. Illustration used with permission of artist Nancy Bauer
and the Registered Nurses’ Association of Ontario
(2005). Assessment & Management of Foot Ulcers for
People with Diabetes. Toronto, Canada: Registered
Nurses’ Association of Ontario.
Charcot Joint- a form of
neuroarthropathy. Nerve damage
causes the ligaments and muscles to
atrophy, which causes joint instability.
Walking on this without proper
protection causes more damage to the
foot structure. In advances state, the
sole of the foot forms a rocker shape,
increasing the risk of ulceration. Illustration used with permission of artist Nancy Bauer
and the Registered Nurses’ Association of Ontario
(2005). Assessment & Management of Foot Ulcers for
People with Diabetes. Toronto, Canada: Registered
Nurses’ Association of Ontario.
Charcot Arthropathy
Claw Toe
Pes Planus
Pes Cavus
South West Regional Wound Care Toolkit
SWRWC Toolkit B.2.1 Lower Leg Assessment: Purpose and Instructions_July-10_2011
4
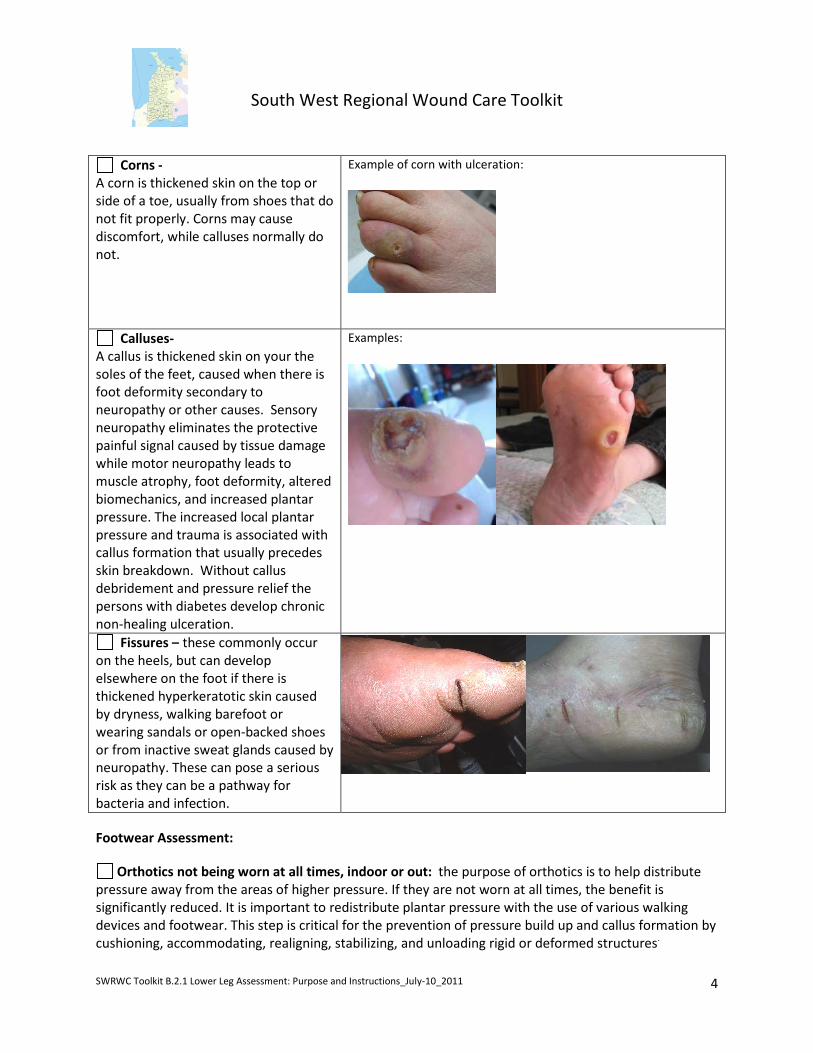
Corns -
A corn is thickened skin on the top or
side of a toe, usually from shoes that do
not fit properly. Corns may cause
discomfort, while calluses normally do
not.
Example of corn with ulceration:
Calluses-
A callus is thickened skin on your the
soles of the feet, caused when there is
foot deformity secondary to
neuropathy or other causes. Sensory
neuropathy eliminates the protective
painful signal caused by tissue damage
while motor neuropathy leads to
muscle atrophy, foot deformity, altered
biomechanics, and increased plantar
pressure. The increased local plantar
pressure and trauma is associated with
callus formation that usually precedes
skin breakdown. Without callus
debridement and pressure relief the
persons with diabetes develop chronic
non-healing ulceration.
Examples:
Fissures – these commonly occur
on the heels, but can develop
elsewhere on the foot if there is
thickened hyperkeratotic skin caused
by dryness, walking barefoot or
wearing sandals or open-backed shoes
or from inactive sweat glands caused by
neuropathy. These can pose a serious
risk as they can be a pathway for
bacteria and infection.
Footwear Assessment:
Orthotics not being worn at all times, indoor or out: the purpose of orthotics is to help distribute
pressure away from the areas of higher pressure. If they are not worn at all times, the benefit is
significantly reduced. It is important to redistribute plantar pressure with the use of various walking
devices and footwear. This step is critical for the prevention of pressure build up and callus formation by
cushioning, accommodating, realigning, stabilizing, and unloading rigid or deformed structures.
South West Regional Wound Care Toolkit
SWRWC Toolkit B.2.1 Lower Leg Assessment: Purpose and Instructions_July-10_2011
5
Inappropriate footwear- e.g. high-heeled or narrow-toed shoes may cause pressure areas. If the
toes are squeezed or pinched together, the bony prominences of the toes can cause pressure ulcers.
Presence of pressure areas: document any areas of redness
d. Test for Neuropathy
To test for neuropathies use a monofilament (available at
http://www.cawc.net/images/uploads/Order_Form.pdf). The filament is
pressed against part of the foot. When the filament bends, its tip is exerting a
pressure of 10 grams (therefore this monofilament is often referred to as the
10 gram monofilament). If the patient cannot feel the monofilament at certain
specified sites on the foot, he/she has lost enough sensation to be at risk of
developing a neuropathic ulcer. Please refer to the diagram in the tool for the
10 pressure points to test. Score is out of ten.
Please check off any other sensory and motor findings.
Please refer to a foot specialist if there is a loss of protective sensation and refer to an OT if underlying
pressure and/or surface concerns.
e. DIABETIC FOOT RISK CLASSIFICATION SYSTEM: The International Working Group Original and
Modified Criteria 2010
Use the International Working Group on the Diabetic Foot Risk Classification System: Modified Criteria
2010
Indicate the level of risk that you have identified based on your findings.
f. The University of Texas Staging System for Diabetic Foot Ulcers (only for clients with Diabetic Foot
Ulcer)
Describe the Stage and Grade of the ulcer based on the descriptors in the chart.
g. Edema (if present)
Check off all areas affected.
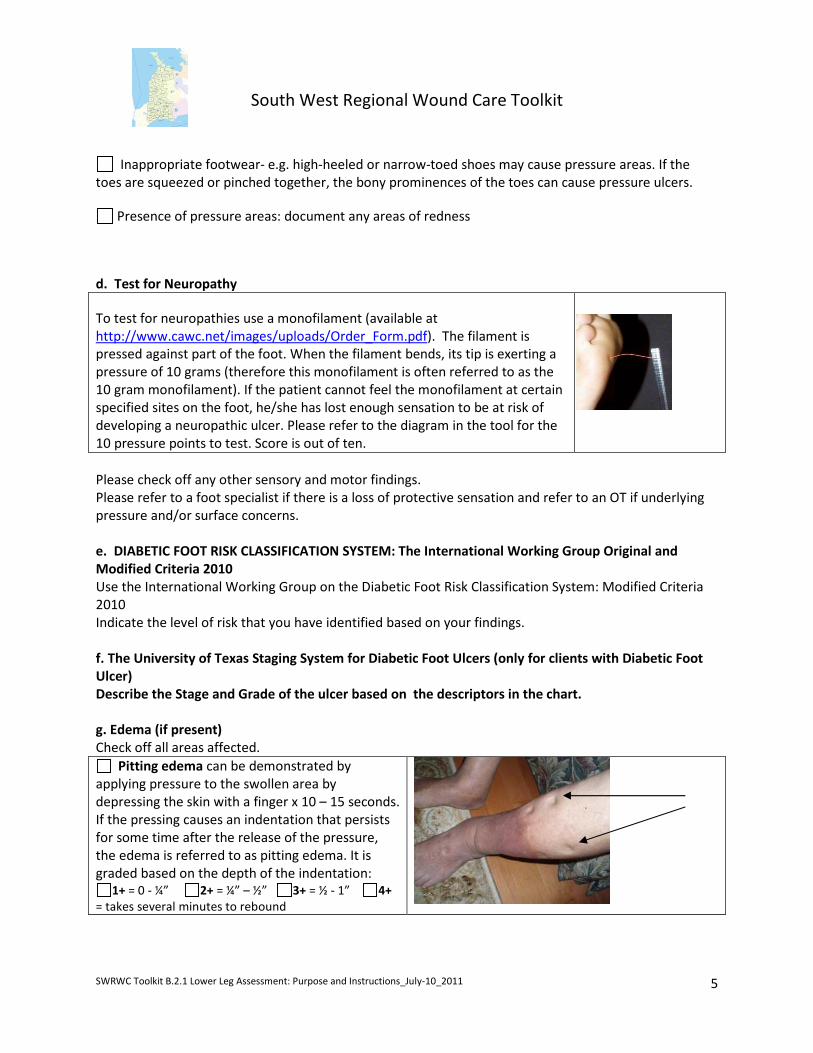
Pitting edema can be demonstrated by
applying pressure to the swollen area by
depressing the skin with a finger x 10 – 15 seconds.
If the pressing causes an indentation that persists
for some time after the release of the pressure,
the edema is referred to as pitting edema. It is
graded based on the depth of the indentation:
1+ = 0 - ¼” 2+ = ¼” – ½” 3+ = ½ - 1” 4+
= takes several minutes to rebound
South West Regional Wound Care Toolkit
SWRWC Toolkit B.2.1 Lower Leg Assessment: Purpose and Instructions_July-10_2011
6
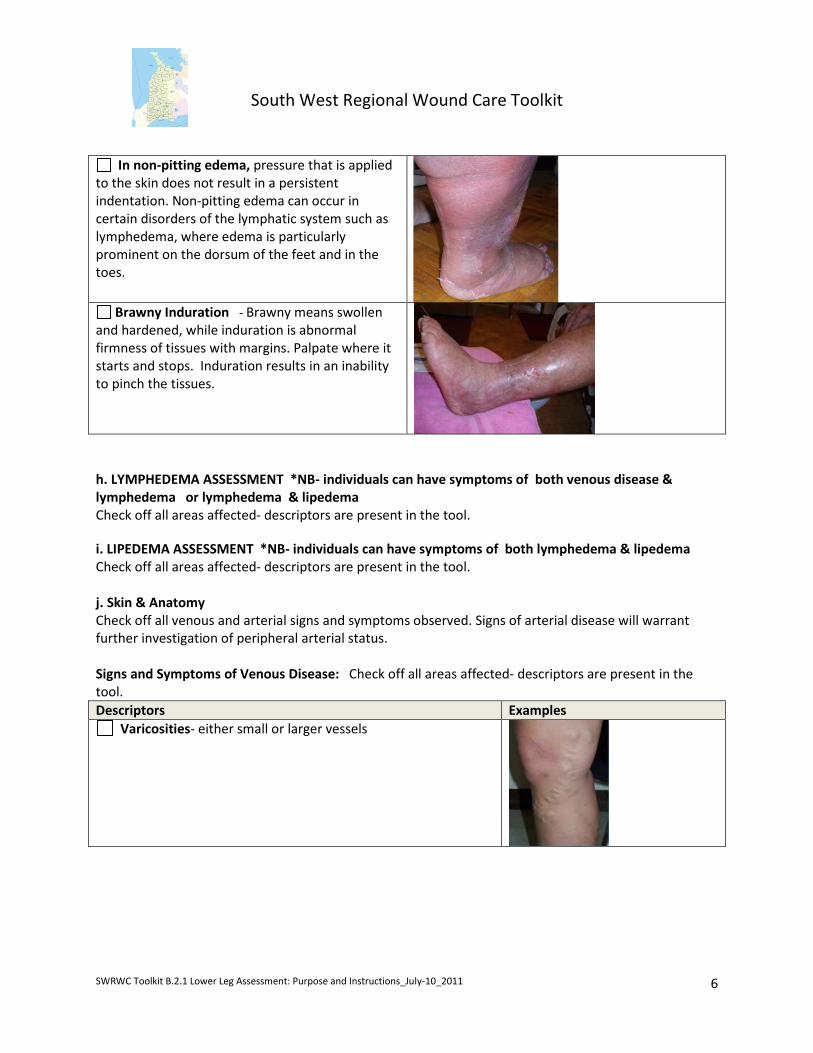
In non-pitting edema, pressure that is applied
to the skin does not result in a persistent
indentation. Non-pitting edema can occur in
certain disorders of the lymphatic system such as
lymphedema, where edema is particularly
prominent on the dorsum of the feet and in the
toes.
Brawny Induration - Brawny means swollen
and hardened, while induration is abnormal
firmness of tissues with margins. Palpate where it
starts and stops. Induration results in an inability
to pinch the tissues.
h. LYMPHEDEMA ASSESSMENT *NB- individuals can have symptoms of both venous disease &
lymphedema or lymphedema & lipedema
Check off all areas affected- descriptors are present in the tool.
i. LIPEDEMA ASSESSMENT *NB- individuals can have symptoms of both lymphedema & lipedema
Check off all areas affected- descriptors are present in the tool.
j. Skin & Anatomy
Check off all venous and arterial signs and symptoms observed. Signs of arterial disease will warrant
further investigation of peripheral arterial status.
Signs and Symptoms of Venous Disease: Check off all areas affected- descriptors are present in the
tool.
Descriptors Examples
Varicosities- either small or larger vessels

South West Regional Wound Care Toolkit
SWRWC Toolkit B.2.1 Lower Leg Assessment: Purpose and Instructions_July-10_2011
7
Hemosiderin staining- Brown or brownish red pigmentation
and purpura caused by extravasation of red blood cells into the
dermis
Chronic Lipodermatosclerosis- lower 1/3 of leg becomes
sclerotic and woody. Leg becomes champagne bottle or bowling-
pin shaped – ulcers are more difficult to heal.
Acute lipodermatosclerosis- This presents as a painful and
tender condition of the leg. It is frequently misdiagnosed as
cellulitis or morphea. It represents a panniculitis associated with
venous insufficiency. Ulcers can occur within the lesion, which
becomes intensely fibrotic over time.
Photograph used with permission of Dr. V. Falanga. Stasis or venous dermatitis - erythema, scaling, pruritis, and
sometimes weeping- may develop cellulitis through breaks in the
skin.
Atrophie blanche - Located on the ankle or foot, ivory white
lesions, atrophic plaques. Ulcerations tend to be exquisitely
painful. The white lesions represent scarring from previous
injuries.
Woody fibrosis - deposits of fibrin in the deep dermis and fat
results in a woody induration of the gaiter area of the leg

South West Regional Wound Care Toolkit
SWRWC Toolkit B.2.1 Lower Leg Assessment: Purpose and Instructions_July-10_2011
8
Ankle (submalleolar) flare - Incompetence in perforating vein
valve which results in venous hypertension and causes dilation of
the venules
Ulcer base moist with granulation &/or yellow slough/ fibrin
Ulcer located in gaiter region (lower 1/3 of calf) - Ulceration
usually on the medial lower leg superior to malleolus but can be
on lateral aspect as well. Ulcerations may encircle the entire ankle;
ulcers occurring above mid-calf or on the foot likely have other
origins.
Ulcer located superior to the medial malleolus
Scarring from previous ulcer(s)- evidence of previous
ulcerations noted
Signs and Symptoms of Arterial Disease:
Descriptors Examples
Hairless –little or no hair on the lower legs or feet
No illustration available
Thin- skin appears thin and fragile and pale in colour
No illustration available
Shiny skin on legs and feet
No illustration available
South West Regional Wound Care Toolkit
SWRWC Toolkit B.2.1 Lower Leg Assessment: Purpose and Instructions_July-10_2011
9
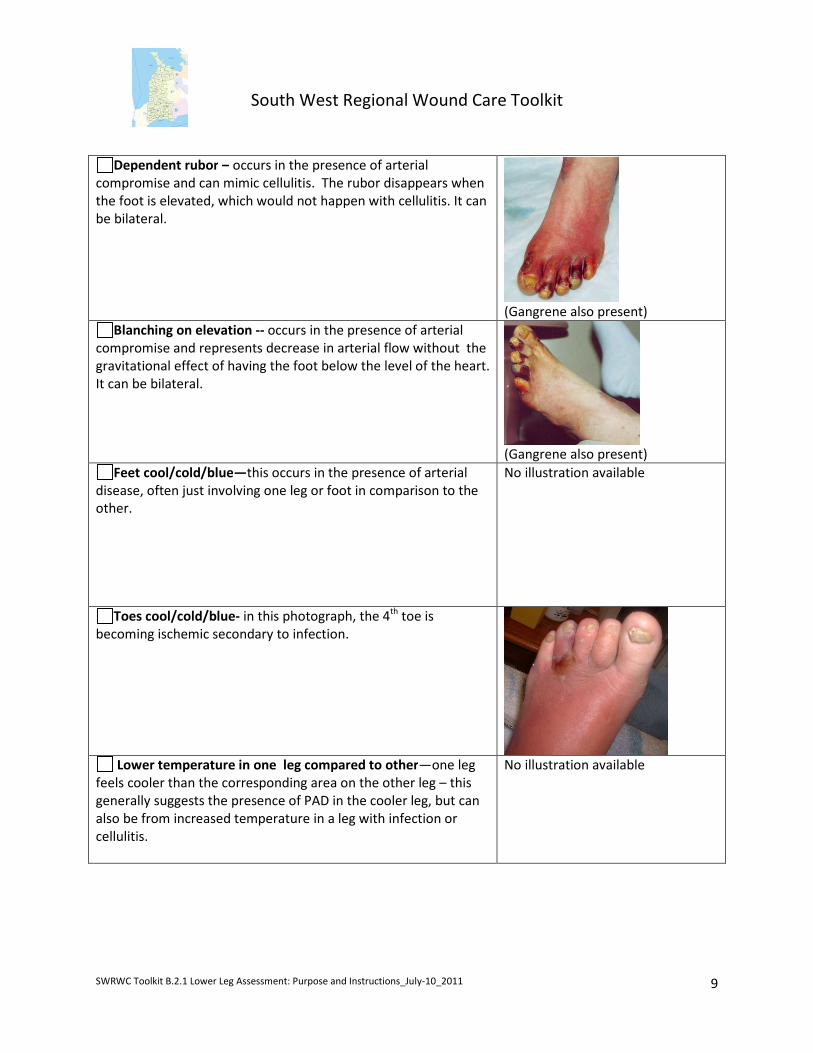
Dependent rubor – occurs in the presence of arterial
compromise and can mimic cellulitis. The rubor disappears when
the foot is elevated, which would not happen with cellulitis. It can
be bilateral.
(Gangrene also present)
Blanching on elevation -- occurs in the presence of arterial
compromise and represents decrease in arterial flow without the
gravitational effect of having the foot below the level of the heart.
It can be bilateral.
(Gangrene also present)
Feet cool/cold/blue—this occurs in the presence of arterial
disease, often just involving one leg or foot in comparison to the
other.
No illustration available
Toes cool/cold/blue- in this photograph, the 4th
toe is
becoming ischemic secondary to infection.
Lower temperature in one leg compared to other—one leg
feels cooler than the corresponding area on the other leg – this
generally suggests the presence of PAD in the cooler leg, but can
also be from increased temperature in a leg with infection or
cellulitis.
No illustration available
South West Regional Wound Care Toolkit
SWRWC Toolkit B.2.1 Lower Leg Assessment: Purpose and Instructions_July-10_2011
10
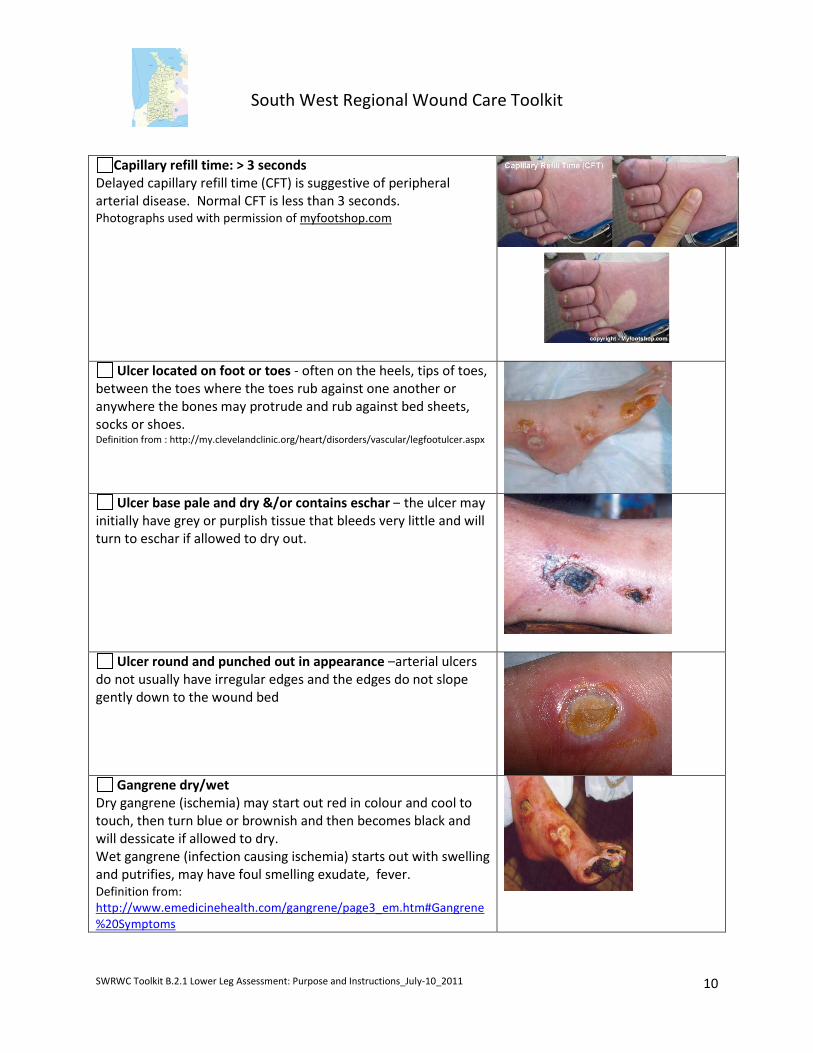
Capillary refill time: > 3 seconds
Delayed capillary refill time (CFT) is suggestive of peripheral
arterial disease. Normal CFT is less than 3 seconds.
Photographs used with permission of myfootshop.com
Ulcer located on foot or toes - often on the heels, tips of toes,
between the toes where the toes rub against one another or
anywhere the bones may protrude and rub against bed sheets,
socks or shoes. Definition from : http://my.clevelandclinic.org/heart/disorders/vascular/legfootulcer.aspx
Ulcer base pale and dry &/or contains eschar – the ulcer may
initially have grey or purplish tissue that bleeds very little and will
turn to eschar if allowed to dry out.
Ulcer round and punched out in appearance –arterial ulcers
do not usually have irregular edges and the edges do not slope
gently down to the wound bed
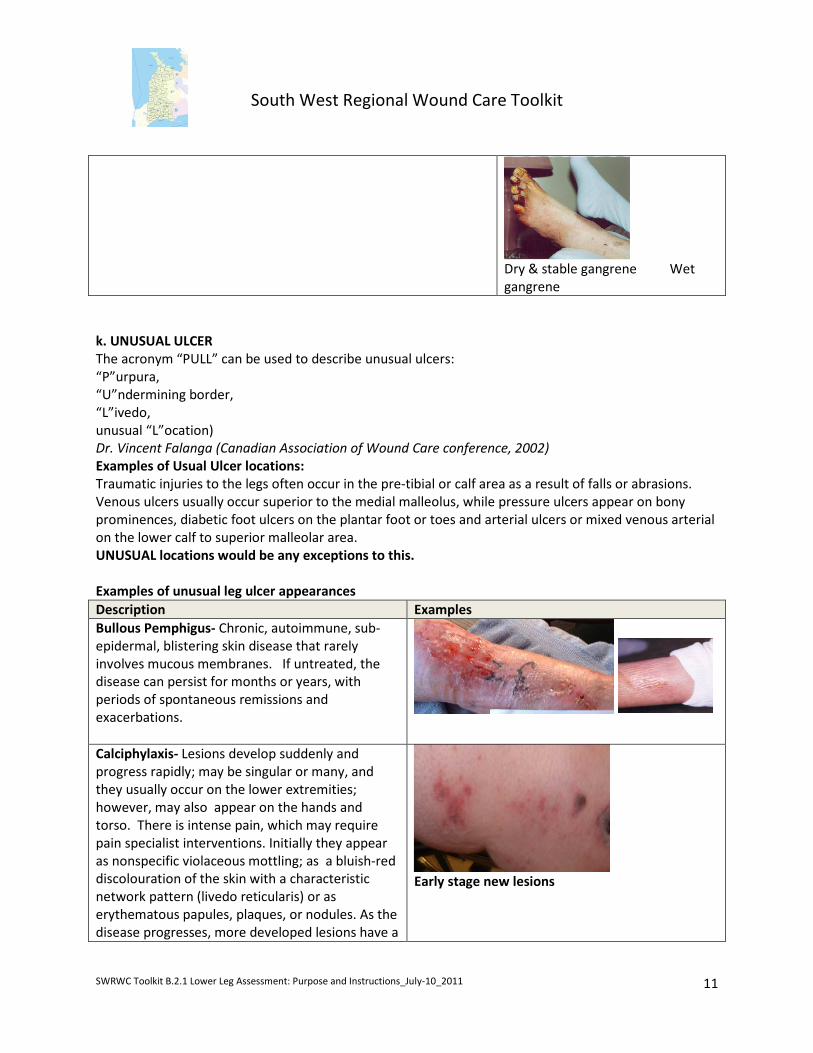
Gangrene dry/wet
Dry gangrene (ischemia) may start out red in colour and cool to
touch, then turn blue or brownish and then becomes black and
will dessicate if allowed to dry.
Wet gangrene (infection causing ischemia) starts out with swelling
and putrifies, may have foul smelling exudate, fever.
Definition from:
http://www.emedicinehealth.com/gangrene/page3_em.htm#Gangrene
%20Symptoms
South West Regional Wound Care Toolkit
SWRWC Toolkit B.2.1 Lower Leg Assessment: Purpose and Instructions_July-10_2011
11
Dry & stable gangrene Wet
gangrene
k. UNUSUAL ULCER
The acronym “PULL” can be used to describe unusual ulcers:
“P”urpura,
“U”ndermining border,
“L”ivedo,
unusual “L”ocation)
Dr. Vincent Falanga (Canadian Association of Wound Care conference, 2002)
Examples of Usual Ulcer locations:
Traumatic injuries to the legs often occur in the pre-tibial or calf area as a result of falls or abrasions.
Venous ulcers usually occur superior to the medial malleolus, while pressure ulcers appear on bony
prominences, diabetic foot ulcers on the plantar foot or toes and arterial ulcers or mixed venous arterial
on the lower calf to superior malleolar area.
UNUSUAL locations would be any exceptions to this.
Examples of unusual leg ulcer appearances
Description Examples
Bullous Pemphigus- Chronic, autoimmune, sub-
epidermal, blistering skin disease that rarely
involves mucous membranes. If untreated, the
disease can persist for months or years, with
periods of spontaneous remissions and
exacerbations.
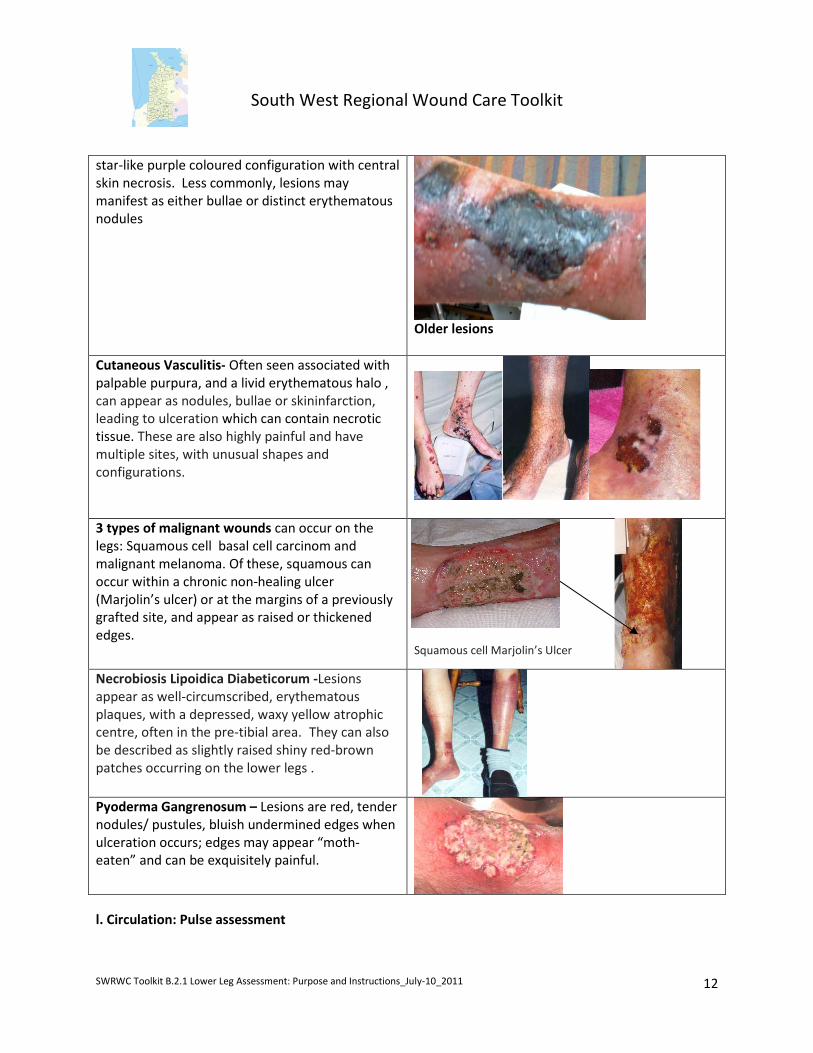
Calciphylaxis- Lesions develop suddenly and
progress rapidly; may be singular or many, and
they usually occur on the lower extremities;
however, may also appear on the hands and
torso. There is intense pain, which may require
pain specialist interventions. Initially they appear
as nonspecific violaceous mottling; as a bluish-red
discolouration of the skin with a characteristic
network pattern (livedo reticularis) or as
erythematous papules, plaques, or nodules. As the
disease progresses, more developed lesions have a
Early stage new lesions
South West Regional Wound Care Toolkit
SWRWC Toolkit B.2.1 Lower Leg Assessment: Purpose and Instructions_July-10_2011
12
star-like purple coloured configuration with central
skin necrosis. Less commonly, lesions may
manifest as either bullae or distinct erythematous
nodules
Older lesions
Cutaneous Vasculitis- Often seen associated with
palpable purpura, and a livid erythematous halo ,
can appear as nodules, bullae or skininfarction,
leading to ulceration which can contain necrotic
tissue. These are also highly painful and have
multiple sites, with unusual shapes and
configurations.
3 types of malignant wounds can occur on the
legs: Squamous cell basal cell carcinom and
malignant melanoma. Of these, squamous can
occur within a chronic non-healing ulcer
(Marjolin’s ulcer) or at the margins of a previously
grafted site, and appear as raised or thickened
edges.
Squamous cell Marjolin’s Ulcer
Necrobiosis Lipoidica Diabeticorum -Lesions
appear as well-circumscribed, erythematous
plaques, with a depressed, waxy yellow atrophic
centre, often in the pre-tibial area. They can also
be described as slightly raised shiny red-brown
patches occurring on the lower legs .
Pyoderma Gangrenosum – Lesions are red, tender
nodules/ pustules, bluish undermined edges when
ulceration occurs; edges may appear “moth-
eaten” and can be exquisitely painful.
l. Circulation: Pulse assessment
South West Regional Wound Care Toolkit
SWRWC Toolkit B.2.1 Lower Leg Assessment: Purpose and Instructions_July-10_2011
13
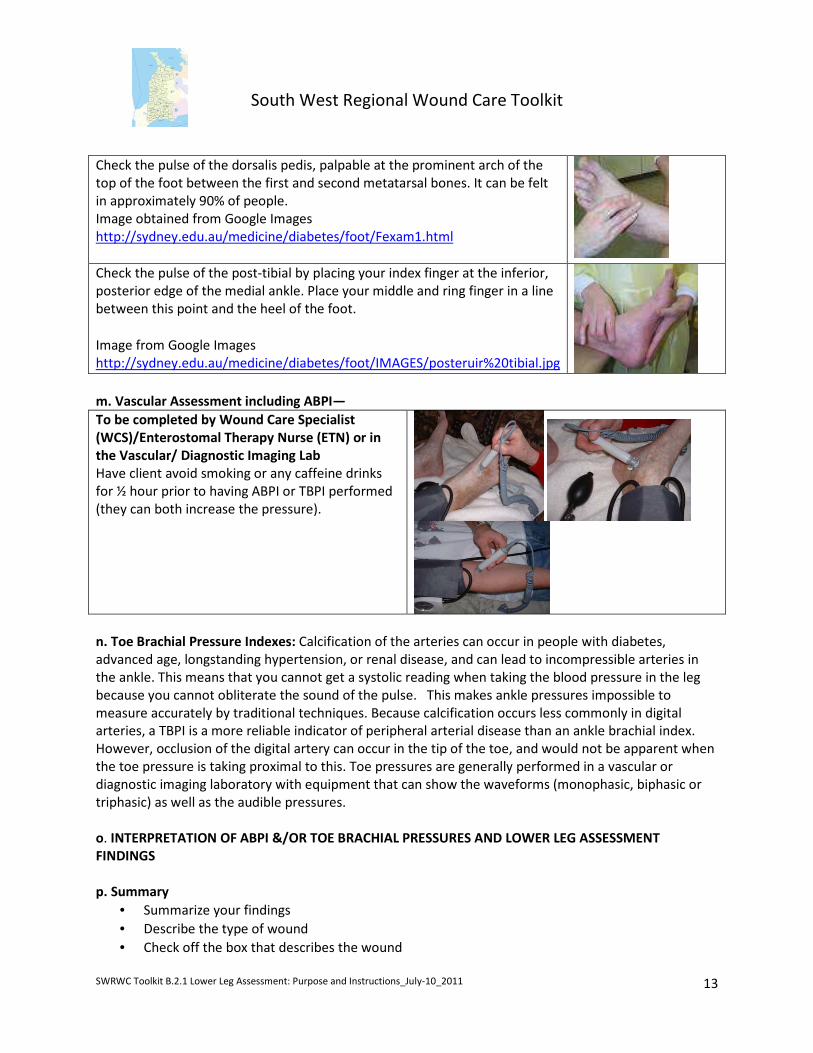
Check the pulse of the dorsalis pedis, palpable at the prominent arch of the
top of the foot between the first and second metatarsal bones. It can be felt
in approximately 90% of people.
Image obtained from Google Images
http://sydney.edu.au/medicine/diabetes/foot/Fexam1.html
Check the pulse of the post-tibial by placing your index finger at the inferior,
posterior edge of the medial ankle. Place your middle and ring finger in a line
between this point and the heel of the foot.
Image from Google Images
http://sydney.edu.au/medicine/diabetes/foot/IMAGES/posteruir%20tibial.jpg
m. Vascular Assessment including ABPI—
To be completed by Wound Care Specialist
(WCS)/Enterostomal Therapy Nurse (ETN) or in
the Vascular/ Diagnostic Imaging Lab
Have client avoid smoking or any caffeine drinks
for ½ hour prior to having ABPI or TBPI performed
(they can both increase the pressure).
n. Toe Brachial Pressure Indexes: Calcification of the arteries can occur in people with diabetes,
advanced age, longstanding hypertension, or renal disease, and can lead to incompressible arteries in
the ankle. This means that you cannot get a systolic reading when taking the blood pressure in the leg
because you cannot obliterate the sound of the pulse. This makes ankle pressures impossible to
measure accurately by traditional techniques. Because calcification occurs less commonly in digital
arteries, a TBPI is a more reliable indicator of peripheral arterial disease than an ankle brachial index.
However, occlusion of the digital artery can occur in the tip of the toe, and would not be apparent when
the toe pressure is taking proximal to this. Toe pressures are generally performed in a vascular or
diagnostic imaging laboratory with equipment that can show the waveforms (monophasic, biphasic or
triphasic) as well as the audible pressures.
o. INTERPRETATION OF ABPI &/OR TOE BRACHIAL PRESSURES AND LOWER LEG ASSESSMENT
FINDINGS
p. Summary
• Summarize your findings
• Describe the type of wound
• Check off the box that describes the wound

South West Regional Wound Care Toolkit
SWRWC Toolkit B.2.1 Lower Leg Assessment: Purpose and Instructions_July-10_2011
14
• Summarize the Interdisciplinary interventions that are recommended (based on Section B.2, B.3)
Literature References :
Armstrong, D.G., Lavery, L.A., & Harkless, L.B. (1998). Diabetic Foot Ulcers: Prevention,
Diagnosis and Classification American Academy of Family Physicians. March 15, 1998.
Available at: http://www.aafp.org/afp/980315ap/armstron.html Accessed Aug. 23, 2010.
Botros, M., Goettl, K., Parsons, L., Menzildzic, S., Morin, C., Smith, T., Hoar, A., Nesbeth, H.,
McGrath, & Best, S. (Update: 2010) Practice Recommendations for the Prevention, Diagnosis
and Treatment of Diabetic Foot Ulcers: Update 2010. Wound Care Canada 8(4): 6-40.
Coutts et al. (2007). RNAO Assessment and Management of Venous Leg Ulcers Guideline
supplement.
Dissemond, J., Körber,A. & Grabbe, S. Differential diagnosis of leg ulcers Journal der Deutschen
Dermatologischen Gesellschaft 2006 4:627–634.
Gorst, R. Bagg, G., Albert, M., Shier,B. The Interdisciplinary Lower Leg Assessment Form: The
Evolution of a Clinical Assessment Tool Wound Care Canada 2006 4(3): 30-50. Available at:
http://www.cawc.net/images/uploads/wcc/4-3-gorst.pdf
Hess, C.T. (2010). Venous ulcer checklist. Advances in Skin and Wound Care. 23(8):384.
International Society of Lymphology (ISL) Lymphoedema Staging: (From International
Consensus Document Best Practices for the Management of Lymphoedema available at:
http://www.lympho.org/mod_turbolead/upload/file/Lympho/Best_practice_20_July.pdf
Moloney, M.C., & Grace, P. Understanding the underlying causes of chronic leg ulceration. JWC
13(6): 215-218.
Patel, K., Grey, J.E., & Harding, K.G. (2006). Abc Of Wound Healing: Uncommon Causes Of
Ulceration BMJ: British Medical Journal, Vol. 332, No. 7541 (Mar. 11, 2006), 594-596.
Peters, E.J.G., & Lavery, L.A. (1998). Effectiveness of the Diabetic Foot Risk Classification System
of the International Working Group on the Diabetic Foot. Diabetes Care 21 (5): 1442-1447.
Vowden, P., & Vowden, K., (2001). Doppler assessment and ABPI: Interpretation in the
management of the leg ulceration. Worldwide wounds. Available at: http://www.worldwidewounds.com/2001/march/Vowden/Doppler-assessment-and-ABPI.html
South West Regional Wound Care Toolkit
SWRWC Toolkit B.2.1 Lower Leg Assessment: Purpose and Instructions_July-10_2011
15
Suzuki, K. (2007). How to diagnose Peripheral Arterial Disease. Podiatry Today 20(4) Available
at: http://www.podiatrytoday.com/article/6952, accessed June 13, 2010





























