Embed Size (px)
Citation preview

Address for correspondence:
M. JEANTET,7 bis, boulevard Louis-Blanc,30100 [email protected]
DOI: 10.1051/odfen/2012106 J Dentofacial Anom Orthod 2012;15:206� RODF / EDP Sciences
1
C L I N I C A L R U B R I C
Some clinical thoughts on how I havemanaged cranio-mandibular disordersover 20 years of practice
Muriel JEANTET
1 – INTRODUCTION
Managing cranio-mandibular disorderscan prove to be difficult as the therapeuticprotocols for them multiply and sometimesseem to contradict themselves, with splints,some types of surgical procedures, absten-tion from some types of mastication, pos-tural exercises, occlusal equilibration,kinesitherapy, and behavioral psychologyall having been proposed by ardent adher-ents as the ideal treatment. In this article weshall attempt to clarify these varying con-ceptions, basing our views on the physio-pathology of this unique articulation as wellas upon the objectives to be reached at theend of treatment.
Instead of speaking of the temporo-mandibular joint it seems to us preferableto refer to the dento-temporo-mandibularjoint and for the articulation itself we shalldistinguish between intra and extra-capsularmalfunctions. In more simple terms, is thearticular disc in place on the head of thecondyle and biomechanically operational orare its collateral attachments stretched orbroken and its biomechanics so altered that,
without treatment, irreversible tissue da-mage will result? Are mandibular kineticsmerely disturbed or are they totally limited?Is disc displacement recoverable on move-ment or isn’t it?‘
1 – 1 – From anatamo-physiologyto physiopathology
When the teeth come into contact, themotion of mandibular elevation stops andopens joint space where the disc is posi-tioned: vertical dimension of occlusion andvertical articulation are thus in harmony.During mandibular movements, the head ofthe condyle rotates inside the discal cavity,while the disco-condylar complex translatesalong the temporal eminence. In the act ofchewing, the disc, a malleable and hingedshock absorber, permits the articular sur-faces to meet. When the collateral liga-ments rupture, the disc is displaced, andbecause of the collagenous nature of theseattachments, this displacement becomespermanent.
Article available at http://www.jdao-journal.org or http://dx.doi.org/10.1051/odfen/2012106

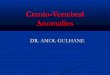
Orthodontists differentiate partialdisplacements that Farrar has namedantero-internal discal luxations or ante-rior discal luxations. They can be semi-permanent: discal luxation reduced bymandibular movement, or permanent:luxation unreduced. These are theprincipal malfunctions that alter TMJ(Figs. 1 and 2).
1 – 2 – This has as aconsequence
The backward movement, then ele-vation of the head of the condyle inthe glenoid fossa occur due to the
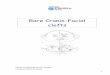
action of the elevator muscles. Themandible has a clockwise rotationbeginning with the most forward pointof occlusion, thus it overloads theposterior occlusion and leads to wear,migration and, most often, intrusion ofcertain teeth that patients describe asocclusal discomfort: ‘‘feels like myteeth are clenched’’. This loss ofvertical dimension of the posteriorocclusion is irreversible without treat-ment (Fig. 3).
When blood-rich innervated postdiscal tissue is crushed, it provokesan inflammation responsible for pain,edema and hemorrhaging. Fibrosiswill also begin to appear.
CL
IN
IC
AL
RU
BR
IC
Figures 1a and 1bSemi permanent anterior disc displacement.
Figures 2a to 2cPermanent anterior disc displacement.
MURIEL JEANTET
2 Jeantet M. Some clinical thoughts on how I have managed cranio-mandibular disorders over 20 years of practice

The septic influx sent to the centralnervous system by the receptors inthis area stimulates the depressor anddecompressor muscles: the head ofthe ptyergoid and especially the super-hyoid muscles and consequently thesub-hyoids that stabilize the hyoidbone. This helps us understand howa malfunctioning TMJ, via the hyoidbone, is going to have repercussionson the sternum, clavicle, scapula, thesuperficial and deep fascias as well asthe duremerians. In a process knownas the Littlejohn mechanics, the re-percussions extend as far as thefourth spinal vertebra. The movementof opposing muscles maintains bal-ance between the posterior para-ver-tebral chains. The discal blocking, if itcannot be bypassed by the mandibularcondyle, will require, if there is no
translation, an exaggerated rotation ofthe condyle. Due to wear of the discsurface, osteo-musculo-aponeuroticimbalances follow: cervical pain, cer-vico-brachia, etc.
To summarize, the loss of discsubstance therefore causes occlusalmodifications, local and remote neur-algia, kinetic disorders, joint noises,rearrangement of post-disc tissue anddisturbances of the osteo-musculo-aponeurotic system.
The goal after joint treatment shouldbe the elimination of painful episodesby recuperation of atraumatic dento-musculo-mandibular function. In suchcases, compensating for the loss ofdisc substance and the decreasedvertical dimension of posterior occlu-sion is indispensable; this requiresarticular therapy and bite stabilization.One without the other will not remedythis disorder.
Restoring discal substance can beperformed by repositioning the con-dyle orthopedically, recapturing thedisc, or thickening of the retro-discalarea or by using arthroscopic accesswith a pexia for discal surgery. As forocclusion, we systematically observechanges ranging from posterior openbite to closing of the inter-incisalangle, and even anterior open bite. Itis imperative to have occlusal balancein order to maintain the articular result.
2 – MATERIAL AND METHODS
Our study is based on a sampling of100 patients ranging in age from 8 to65 who are suffering from disc dis-placement. For certain patients, ther-apy started as far back as 20 yearsago.
We have excluded from our studypatients with blocked disc positionwho have isolated ‘‘over rotation’’with posterior disc displacement atthe end of opening their mouths ordisc bonding problems.
CL
IN
IC
AL
RU
BR
IC
Figure 3Model showing intrusion of posterior teeth.
SOME CLINICAL THOUGHTS ON HOW I HAVE MANAGED CRANIO-MANDIBULAR DISORDERS OVER 20 YEARS OF PRACTICE
J Dentofacial Anom Orthod 2012;15:206. 3

We have excluded the followingtherapies:– retro incisal appliances, maxillary
plates, Lucia’s jig, or an NTI shield.These treatments are entirely con-tra-indicated since they provokea postero-lateral open bite,which then aggravates articularcompression;
– behavioral, osteopathic or chiro-practic therapies, which used inisolation, are only a supplementaltherapy and do not treat the dento-temporo-mandibular area or in-volved tissue. These techniquesare, however, very useful for com-forting patients and help facilitatethe motion of the condyles. Nopatient in the study wore orthope-dic shoes or splints, prisms or anyother posture-aid device in ordernot to overload the central nervoussystem during TMJ treatment,which consisted of:
– selective grinding which accentu-ates the loss of discal and dentalsubstance;
– occlusal blocking which createssectorial inocclusion and causeslingual interpositions leading todental migrations, opening diaste-mas and lateral gliding during occlu-sion. The displacement of the headof the condyle is, in addition, totallyrandom since occlusal blocking iscreated in the mouth by adhesionbetween components. Teeth,which bear the weight of occlusalblocking, are in danger of beingintruded:
– For the same pathology dependingon the treatment, we analyzed theresults concerning certain neural-gias, the mandibular kinetics, jointnoises, remote symptoms andease of stabilization.
2 – 1 – Discal pexia
Arthroscopy can facilitate the inser-tion of a discal pexia, which helpseliminate possible intra-articular adhe-sions. It is a slightly invasive proce-dure requiring stabilization of occlusalcontact during and after surgery. Infact, disc repositioning implies low-ering and propulsing the mandible. Athermoformed activator made beforethe procedure, will be reinserted dur-ing the operation once the disc is inplace and will be worn full time duringthe healing phase, including duringmasticating, for approximately 6months.
Temporo-mandibular orthopedicprocedures are performed by usingrelaxation activators to capture thedisc and to increase bone density ofthe disc. Each activator is tested in thesame way, using a semi-adaptablearticulator programmed according tothe anatomical data of the patient. It ismade of auto-polymerisable transpar-ent resin, for ergonomic and estheticreasons, and used mostly for themandible. The activators are smooth,with no deep indentations, in order tostabilize the mandible without con-straining it, while simultaneously, al-lowing for mastication. Their thicknessshould not interfere with the openspace for inocclusion. Anterior gui-dance is still achieved. But orthodon-t is ts never leave an anter iorinfraocclusion that could generate alingual interposition. In the buccalarea, the motivators descend into theposterior sectors following the majorcontours of the teeth in order toensure their retention during mastica-tion. In the lingual zone, motivatorsdescend two to three millimetersbelow the tooth neck so as not to
CL
IN
IC
AL
RU
BR
IC
MURIEL JEANTET
4 Jeantet M. Some clinical thoughts on how I have managed cranio-mandibular disorders over 20 years of practice

irritate the edge of the tongue (Figs. 4and 5).
2 – 2 – The relaxation activator
It is still called the simple rotationactivator or central relational activatoreven though this term centric relationis inadequate without the articulardisc. The mandibular position is re-corded as unforced rotation with
moyco wax, used now in place ofaluwax. The patient sits at a 45� anglelegs uncrossed while the practitionermanipulates and rotates the mandibleand guides it vertically. Orthodontistsmust be careful not to press on thealveolar process during manipulationor push the mandible backwards. Theactivator works to eliminate prematureocclusal contact that could potentiallyoccur, by distributing the occlusalforces and by modeling appropriateguidance of functional operation. Thepoints of contact are punctiform anduniformly distributed; the tritural sur-face is smooth.
2 – 3 – The discal capitationactivator
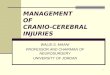
The mandibular condyle is reposi-tioned within the discal cavity. Thismandibular position is identified afteraxiographic analysis; three impres-sions are necessary in order to deter-mine more precisely the coordinatesof the point of disc displacementalong the line of closure (Fig. 7).
CL
IN
IC
AL
RU
BR
IC
Figure 4Limits of the splint.
Figure 5Mandibular splint in place.
Figure 6Registering pure rotation.
SOME CLINICAL THOUGHTS ON HOW I HAVE MANAGED CRANIO-MANDIBULAR DISORDERS OVER 20 YEARS OF PRACTICE
J Dentofacial Anom Orthod 2012;15:206. 5

Orthodontists guide mandibular pro-pulsion slightly beyond this point usingthe corresponding propulsion splint(Fig. 8). Practitioners never locateand record this position buccally; infact, vertical force is mandatory forthis type of displacement.
Only the articulator can make itsystematically integrate. The risk hereis excessive horizontal propulsion andthus permanently luxating the disc.This activator has some specific char-acteristics such as a raised caninezone used to secure an immediatedisocclusion. Some anti-recoil spacersare located at the back of the caninearea of the mandibular articulator. Inthese cases, we would rather fabri-cate a maxillary articulator with a retro-teeth wall to maintain the forwardpositioning.
2 – 4 – The activator for post-discal densification
The activator is made by interposingsplints along the posterior portion ofthe condylar slope situated on thearticular eminence of the temporalmuscle (Fig. 9). The condylar displace-ment is obtained in measurements of.5 to 1 mm a month until the space isequivalent to the disc thickness (ap-proximately 4 mm) or until total recup-eration of the amplitude of opening:with a passage under the articular discin case of permanent disc displace-ments. Before each activation, theorthodontist refits the simulator ofthe mandibular model: aluwax is ap-plied on the articulator and the articu-lar posit ion is recorded. Thisprocedure allows the practitioner tovalidate the preceding distension.
CL
IN
IC
AL
RU
BR
IC
Figure 7Axiogram of the coordinates of disc loss.
Figure 8Propulsion block.
MURIEL JEANTET
6 Jeantet M. Some clinical thoughts on how I have managed cranio-mandibular disorders over 20 years of practice

It sometime happens that patientsnullify posterior interference by propul-
sing. In this case, the orthodontistshould diminish or stop activation.
3 – THE RESULTS
TMJ treatment is over: the newmandibular position is achieved and isnow irreversible.
Visible occlusal modifications arestable and reproducible: identical inthe mouth and on the simulator fitting,performed during the last adjustmentof the activator (Figs. 10 and 11).
Procedures for prosthetic or ortho-dontic stabilization are used to com-
pensate any additional need ofmodifications: closing open bites andadjusting the contact points of theanterior segment of the dentition.
The protocol is always the same:the retention of the articular positionby extending the coronary prosthesisusing partial or total ceramic crownsmade with a simulator. The orthodon-tist only chooses this option when the
CL
IN
IC
AL
RU
BR
IC
Figure 9Distension block.
Figures 10a to 10cThe propulsion.
SOME CLINICAL THOUGHTS ON HOW I HAVE MANAGED CRANIO-MANDIBULAR DISORDERS OVER 20 YEARS OF PRACTICE
J Dentofacial Anom Orthod 2012;15:206. 7

patient is already wearing prosthesisor when prosthesis is necessary forclinical purposes. Most of the time, anorthodontic solution creates stabiliza-tion: the maxillary arch is treated andretained with an activator (Fig. 12).This is adjusted as dental displace-ments occur: sectorial recesses aremanaged by continually wearing theposterior splint.
The practitioner will have to removethe activator and to replace it withsplints on the first and second molarsor with a maxillary activator (Figs. 13and 14) in order to install the mandib-
ular apparatus. Anterior contact at thisstage is indispensable in order toavoid lingual interposition. To optimizeocclusion, the orthodontist modifiespoints of contact, adjusts extrusion ofthe posterior zone from mesial todistal and corrects inclinations androtations. Having obtained these re-sults, the practitioner removes thetemporo-mandibular splint either byegression or using a permanent pros-thesis for the tooth.
Out of the 100 patients representedin this study, 15 were not treatedbecause they presented no symptoms
CL
IN
IC
AL
RU
BR
IC
Figures 11a and 11bThe distension.
Figure 13Temporary bite blocks.
Figure 12Still wearing the splint.
Figure 14Substitution splint.
MURIEL JEANTET
8 Jeantet M. Some clinical thoughts on how I have managed cranio-mandibular disorders over 20 years of practice

of neuralgia; 20 were fitted with arotation activator intended for noctur-nal use; 25 successfully had eitherorthopedic or surgical recapture of thedisc; the rest were treated using post-disc densification.
Since 15 patients received no treat-ment, they obviously had undergoneno dental procedures that could affecttheir occlusion. For 10 of the patients,we observed a worsening of articularnoises, an onset of neuralgia andosteo-musculo-aponeurotic problemsthat were recurrent following osteo-pathic or chiropractic treatment. Twopatients indicated that they experi-enced occasional blocking when
opening the mouth. Five remainedstable.
Among the group fitted with a rota-tion activators intended for nocturnaluse, only 50% said that the treat-ment improved their condition anddecreased their pain. The other halfsaid that there was no improvement;so, the orthodontist suggested thatthey continually wear the rotationactivator full time. Subsequently,all local neuralgia completely disap-peared.
There are 5 adults and 20 adoles-cents represented in the recapturegroup. All of them suffered from classII skeletal malocclusion. Among the
CL
IN
IC
AL
RU
BR
IC
Pure
rotation splint
Post-discal lowering
densification splint
Pexie discal arthroscopic
retention splint
Wearing night continuous
including
mastication
continuous
including
mastication
Approximate
treatment time
lifetime 1 year 6 months
TMJ pain intermittent yes yes
Referred pain intermittent yes yes
Amplitude of
movement
unchanged total recuperation
of amplitude
total recuperation
of amplitude
Ressauts of
TMJ sounds
unchanged reappearance of
TMJ clicking
suppression of sounds
and ressauts
Tissuerecuperation no yes yes
Occlusal
consequences
none posterior open bite
slight change in anterior
guidance
posterior open bite
major change in
anterior guidance
Stabilization of
Treatment
none obligatory obligatory
Permanence of
results
highly variable good weak
TabIe IResults: displacements not reduced.
SOME CLINICAL THOUGHTS ON HOW I HAVE MANAGED CRANIO-MANDIBULAR DISORDERS OVER 20 YEARS OF PRACTICE
J Dentofacial Anom Orthod 2012;15:206. 9

adults, one female patient remainedstable (when she turned 20), foranother female, the recapture waspartial: a faint mandibular clickingsound persisted in the morning andthus invalidated the treatment. For theremaining 3 patients, their initial symp-toms reappeared 5 years after treat-ment, and required that they starttreatment all over again.
As for the adolescents, 10 werestable at the age of 10; 5 had a
reoccurrence of articular noises withno other symptoms; 5 others hada reoccurrence of noises andsymptoms.
Out of the 40 patients treated bypost-discal densification, 20 were stillstable at the age of 10. For the 10 to15 years old group, only 5 needed towear a rotation activator 24/7 for 3months and this resulted in balancedocclusion.
CL
IN
IC
AL
RU
BR
IC
Pure
rotation
splint
Post-discal
lowering
densification
splint
Retaining
Splint
pexie arthroscopic
discal
Wearing night continuous
including
mastication
continuous
including
mastication
continuous
including
mastication
Approximate
treatment time
lifetime 1 year 1 year 6 months
TMJ pain intermittent yes yes yes
Referred pain intermittent yes yes yes
Amplitude of
movement
unchanged unchanged unchanged unchanged
Ressauts of
of articular
unchanged suppression of
sounds and
ressauts
continuation of
sounds, lessening
ressauts
suppression of
sounds and
ressauts
Tissue
recuperation
no yes yes yes
Occlusal
consequences
none posterior open bite
major change in
anterior guidance
posterior open bite
slight change in
anterior guidance
posterior open bite
major change in
anterior guidance
Stabilization of
treatment
none obligatory obligatory obligatory
Permanence of
results
highly variable weak good Weak
Table IIResults of disc recapture.
MURIEL JEANTET
10 Jeantet M. Some clinical thoughts on how I have managed cranio-mandibular disorders over 20 years of practice

4 – DISCUSSION
The rotation articulator can be re-commended to patients without ne-cessarily compensating for discal loss.In fact, when the patient stops wear-ing it and the absence of condylardisplacement does not cause anymodification of tissue structure, thistemporary activator has relaxed themuscles, harmonized occlusal contactand improved guidance function. Itsuse prevents the worsening of exist-ing cranio-mandibular malfunctionswhen they are not excessively debil-itating. It is mostly recommended forasymptomatic patients who do notwish to begin ‘‘hardcore’’ articulartreatment. The time during whichpatients wear this type of activatorcan vary. However, it must be empha-sized that wearing it full time elim-inates painful symptoms in 90% ofthe cases.
The disc recapture activator is usedless and less: long-term results are notconvincing, the occlusal conse-quences of propulsion are often sim-ply unmanageable, the stabilization ofthe propulsed position is difficult tomaintain and the occlusal conse-quences of propulsion are quite oftensimply ungovernable, and stabilizingthe mandible’s anterior position isdifficult. For these reasons from about1980 to 1990 some practitionersattempted to guide the mandible to amore distal position by selective grind-ing but relapse from this position wasinevitable! Success requires obtaininga fixed and reproducible position forthe mandible. That is why practi-tioners today do not propose thisprocedure to young patients who still
have growth potential: a splint oper-ates like a mandibular activator. Butwe must not disregard however, thecollagenous nature of the collateralligaments attaching the disc to thehead of the mandibular condyle. Todaythis type of movement is contra-indicated in adults.
Use of the post disc densificationsplint is, accordingly, the therapy ofchoice for cranio-mandibular malfunc-tions because it allows lowered con-dyles to pass under articular discs incases of non-reducible disc displace-ment; stabilization of the new articularposition is smooth and reliable and thepermanence of results is good. Thedecompression suppresses the influxof harmful impulses soliciting the suband super hyoid muscles and the TMJno longer occupies itself with osteo-muscular-aponeurotic problems. Onthe other hand, practitioners shouldalways warn patients that this devicedoes not resolve the problem of jointnoises.
The arthroscopic disc pexie is todayused only rarely: practitioners cannotpredict what new mandibular positionwill be obtained and propulsion isimpossible to govern occlusally with-out orthognathic surgery.
On the other hand, for permanentdisc displacements of long standingwith good tissue restoration, arthro-scopic lavage presents interestingpossibilities because it can rid theTMJ of inflammatory factors andfibrous debris. Orthopedic treatmentthat is used as a follow up to thisprocedure operates smoothly.
CL
IN
IC
AL
RU
BR
IC
SOME CLINICAL THOUGHTS ON HOW I HAVE MANAGED CRANIO-MANDIBULAR DISORDERS OVER 20 YEARS OF PRACTICE
J Dentofacial Anom Orthod 2012;15:206. 11

5 – CONCLUSION
What can practitioners do and whatcan’t they do for TMJ problems?
Therapeutic results for TMD do notrestore ad integrum articular compo-nents to their original state. Recaptur-ing the disc is a myth but densificationof tissues distal to the disc is a clinicalreality.
Protocols for TMJ therapy are rela-tively profound: patients must wearsplints 24 hours a day even duringmastication, the average length oftreatment is about a year, and thepermanence of results is not absoluteeven though they have seemed quitesatisfactory. These remarks are basedon more than twenty years of practice.
Well then, whom should we treatand when?
For patients with no symptoms ofpain or function and who require nodental treatment, abstention wouldseem an obvious stance to adopt butpractitioners should always bear inmind that signs of TMD may bepresent in locations well removedfrom the TMJ. When patients havelimitations or pain in mouth opening,practitioners must direct their therapyto the source of these difficulties, theTMJ.
But confronted with serious irrever-sible changes to the occlusion as isthe case with orthodontics accompa-nied by the extraction of bicuspidteeth for adolescents, we are obligedto make sure that the TMJ continuesto function properly. Practitioners
should watch over the TMJ for manyreasons: the management of occlusalconstraints during orthodontic treat-ment, obtaining an occlusion in har-mony with articular determinants, theassurance of not aggravating initialarticular compression in case of cra-nio-mandibular malfunctions and thecertainty of physiological condylargrowth.
We are also frequently called uponto deal with temporo-mandibular pro-blems for patients that other specia-lists, chiropractors, osteopaths, andENT physicians refer to us hoping wecan provide TMJ equilibrium for them.
Practitioners should remember thatif they give in to the desire of a patientwith cranio-mandibular dysfunctionnot to have treatment for it beforereceiving extensive dental reconstruc-tion they are taking a big risk. If atemporo-mandibular disorder appearsovertly during or after the reconstruc-tion, courts will hold them culpable,not the patient who refused thetreatment. Courts will rule that pa-tients are not competent to makesuch therapeutic decisions.
As practitioners we must providepatients with enough information togive us well considered informedconsent and we are also obliged todiscern as much about them aspossible in order to make an informeddiagnosis of and treat, if necessary,any cranio-mandibular disorder.
CL
IN
IC
AL
RU
BR
IC
MURIEL JEANTET
12 Jeantet M. Some clinical thoughts on how I have managed cranio-mandibular disorders over 20 years of practice