Embed Size (px)
Citation preview
Solihull CCG Survivorship and Cancer Pathway Programme
Jo Tolley.
Summary
•Primary Care Nurse Facilitator Role.•CQUIN & Contractual arrangements.•PN & Enhanced CCR’s.•Next Steps.
Background
• Primary Care Nurse Facilitator – Summer 2013• Collected Patient Stories.• “I feel like my comfort blanket has gone after treatment” • “You can’t remember everything said to you at diagnosis and treatment”
H&W• “there is a lack of communication between hospitals” TS• “The GP disregarded the information the consultant had recommended
stating no you don’t need that” TS• “I did not know about the warning signs of recurrence” TS, H&W• “hospital not interested in me now they’ve got rid of my cancer” H
Colorectal Pathway
• CQUIN– Health & Well Being Clinics + Breast
• 1 complete to date in colorectal.• 3 in breast.
– Treatment Summaries – Colorectal pilot.• Adapted from NCSI pack.
– 2 year CQUIN extending to 2 additional tumour sites next year.
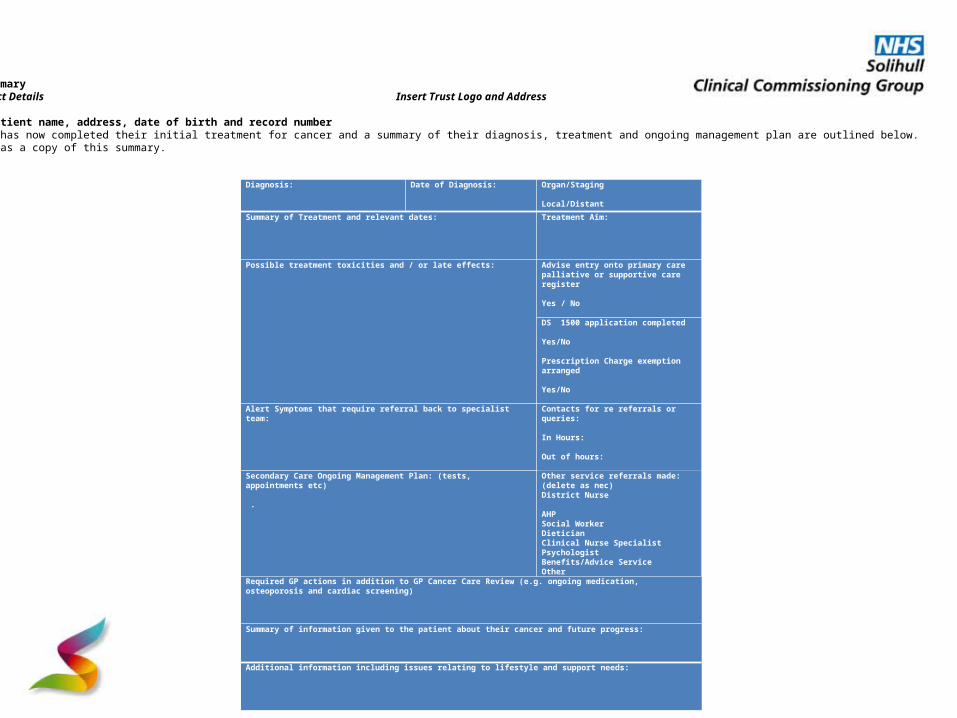
Diagnosis:
Date of Diagnosis:
Organ/Staging Local/Distant
Summary of Treatment and relevant dates:
Treatment Aim:
Possible treatment toxicities and / or late effects: Advise entry onto primary care palliative or supportive care register Yes / No DS 1500 application completed Yes/No Prescription Charge exemption arranged Yes/No
Alert Symptoms that require referral back to specialist team:
Contacts for re referrals or queries: In Hours: Out of hours: Other service referrals made: (delete as nec)District Nurse AHPSocial Worker DieticianClinical Nurse Specialist Psychologist Benefits/Advice ServiceOther
Secondary Care Ongoing Management Plan: (tests, appointments etc) .
Required GP actions in addition to GP Cancer Care Review (e.g. ongoing medication, osteoporosis and cardiac screening) Summary of information given to the patient about their cancer and future progress: Additional information including issues relating to lifestyle and support needs:
Treatment Summary Insert GP Contact Details Insert Trust Logo and AddressDear Dr XRe: Add in patient name, address, date of birth and record numberYour patient has now completed their initial treatment for cancer and a summary of their diagnosis, treatment and ongoing management plan are outlined below. The patient has a copy of this summary.

Cancer Care Reviews & Practice Nurse Course
Patient comments• “I think I had a review but I don’t remember”• “I feel aftercare was lacking, although the hospital was brilliant”• “I don’t feel like I can trouble anyone”• “Just left to it”• “I’ve just carried on”• “Practice nurse good point of contact and know patient well”• “We soldiered on”• “I’ve been in a black hole since treatment”• “No contact from GP surgery”• “Saw GP who said I needed antibiotics, didn’t ask about cancer – no
interaction, would have been nice”• “I didn’t know I could get a free wig on the NHS”• “I had lymphoedema, I wasn’t told about skin care or how I could massage
my arm”.• “Many ladies feel isolated at the end of treatment”
Macmillan PN Course
Course Aims1.Improve Knowledge, skills, attitude and confidence2.Identify transferrable skills3.Encourage “Cancer champions”4.Improve relationships5.Encourage opportunistic reviews6.Encourage a more proactive approach7.Encourage supported self management
Course Examples
• What is cancer?• Changing cancer story• The Recovery Package• Cancer care reviews• Living with cancer• Treatment pathways• Motivational
interviewing• Difficult conversations
• Role of Clinical Nurse Specialist
• Fatigue, Anxiety, Breathlessness
• Nutrition and cancer• Late effects• Transition to palliative
care including advanced care planning
Enhance CCR
• Nurse makes contact with patient• Patient completes the questionnaire.• Patient has 20 minute appointment• MAP of Medicine used to tailor care plan• Treatment summary will support CCR• Care plan completed on computer
template/carbonated copy
Patient comments
If CCR routinely carried out, how soon after diagnosis should it be offered?
•“Once treatment has started”•“The offer of a review needs to be soon”
•“About 6 months after diagnosis, you need to come to terms with things”
•“ASAP”
Patient comments cont.
Did you find CCR with the nurse a positive or negative experience overall? Why?
•“Positive but came a little late for me”•“Positive; it was good to talk to someone who
understands your position, and who is not a friend or relative”
•“Positive; the nurse showed genuine sympathy in my situation, giving relevant leaflets and a
support service if needed”
Patient comments cont.
One model of care would be to have a telephone call at the point of diagnosis by a doctor or nurse and offered a more detailed CCR at about 6 months, comments?•“A call from the surgery would be good as I felt a little that
my doctors just forgot me”.•“Phone call initially ok, but not the same as face to face. I also think 6 months is too long. I had a family and friends,
not everyone has”.•“Depends on the individual, the option could be offered”.•“Before 6 months ASAP after diagnosis. Support is of the
upmost (It can be a very stressful and anxious time)”.
Summary
1. QOF payments are significantly lower than for other chronic diseases, consider best practice
2. All patients are individuals with very different supportive needs
3. Practice nurses are ideally placed to support cancer patients
4. Enhanced CCR ensures a holistic approach to care and support
Enhanced CCR
• Use remaining Macmillan funding to pilot.• Enhanced Payment to support PN’s.• Enhanced Cancer Care reviews – as previously
described.
Next Steps
• Evaluating PN Course.• Pilot Enhanced CCR• Roll out H&W Clinics in Colorectal and Breast.• Use CQUIN 2015/16 to extend Survivorship
Agenda– Introducing H&W Clinics into 2 more tumour sites.– Roll out TS into 2 further tumour sites.
Questions?