Embed Size (px)
Citation preview

© APON 2003
ONCOLOGIC EMERGENCIES
Karla Wilson RN MSN FNP CPON®

© APON 2003
ONCOLOGIC EMERGENCIES
• Recognize abnormal laboratory results
and associated nursing implications.
• Recognize the most common oncologic emergencies and important nursing interventions for each.
• Implement practices designed to improve the quality of life for patients and families affected by childhood cancer.

© APON 2003
ONCOLOGIC EMERGENCIES
• Occur at diagnosis or at any point in treatment process
• Life-threatening
• Arise as: – metabolic/hormonal problems
– result of obstruction/pressure
– consequence of cytopenias

© APON 2003
HYPERLEUKOCYTOSIS
• Definition – peripheral WBC >100,000/mm3
• Associated Malignancies – AML/ALL
– CML
• Clinical Presentation – SOB/tachypnea/cyanosis
– blurred vision/papilledema
– ataxia/agitation/confusion
– delirium/stupor
Photo courtesy of Dr. C-H. Pui

© APON 2003
HYPERLEUKOCYTOSIS
• Medical Management – IV hyperhydration (~3000 mls/M2/day)
– maintain urine output at 1-2 mls/kg/hr
– NaHCO3/allopurinol/rasburicase
– correct electrolytes
– leukapheresis/exchange transfusions
– blood product support
– anti-leukemia treatment

© APON 2003
HYPERLEUKOCYTOSIS
• Nursing Management/Interventions – assess cardiopulmonary/neurologic status
– monitor fluid/electrolyte balance
– recognize change in status/implement appropriate interventions

© APON 2003
HYPERLEUKOCYTOSIS
• Potential Complications – hemorrhage/intracranial bleed
– pulmonary leukostasis
– metabolic alterations
– renal failure
– sudden death

© APON 2003
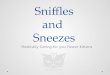
TUMOR LYSIS SYNDROME (TLS)
• Definition – rapid breakdown of malignant cells causing
inadequate renal function manifested by: • hyperuricemia (uric acid > 8 mgs/dl)
• hyperkalemia (K+ >6 mEq/ml)
• hyperphosphatemia (PO4 > 10 mgs/dl)
• hypocalcemia (Ca++ < 8 mgs/dl)

© APON 2003
Hyperuricemia
Uric acid crystals
CYTOTOXIC THERAPY/ SPONTANEOUS TUMOR CELL BREAKDOWN
Tumor Cell Lysis
Hyperkalemia
Ventricular arrhythmia
Death
Renal Failure
Dialysis
Hyperphosphatemia
Calcium/phosphate crystals

© APON 2003
TLS
• Associated Malignancies – B cell leukemia/Burkitt’s lymphoma
– T cell leukemia/lymphoma
– leukemia with WBC > 100,000/mm3
– neuroblastoma (rare)

© APON 2003
TLS
• Clinical Presentation – RAPID ONSET
– abdominal pain/cramping/fullness/vomiting/ascites
– back/flank pain/oliguria/anuria
– cardiac arrhythmias/tachycardia/pleural effusion
– numbness/tingling/tetany
– weakness/fatigue
– altered level of conscience
– seizures

© APON 2003
TLS
• Medical Management – IV hyperhydration (~3000 mls/M2/day)
– urine alkalization • NaHCO3/allopurinol/rasburicase
– correct electrolyte/metabolic abnormalities
– +/- dialysis

© APON 2003
TLS
• Nursing Management/Interventions – accurate I&O/monitor weights
– monitor urine pH/specific gravity
– assess for symptoms of hypocalcemia • Chvostek’s sign
• Trousseau’s
– patient/family support

© APON 2003
SEPTIC SHOCK
• Definition – systemic response to pathogenic micro-organisms
and endotoxins in the blood
– leads to perfusion, cellular hypoxia, and death
– usually associated with gram negative organisms arising from endogenous flora

© APON 2003
SEPTIC SHOCK
• Risk factors – ANC < 100/mm3
– prolonged neutropenia (> 7 days)
– immunosuppression
– asplenism
– infancy
– mechanical device
– poor skin integrity/mucositis

© APON 2003
SEPTIC SHOCK
SYMPTOM SEPSIS SEPTIC SHOCK
VITAL SIGNS
Temperature: < 360 C or > 380 C
HR: tachycardia
RR: tachypnea
BP: normal
Temperature: < 360 C or > 380 C
HR: tachycardia
RR: tachypnea
BP: hypotension unresponsive to fluid resuscitation
PHYSICAL CHANGES
Warm, flushed skin
Weak/malaise
Adequate urine output
Cool, clammy skin
Bilateral rales, hypoxia
Anasarca
Oliguria anuria
MENTAL STATUS
CHANGES Minor confusion/restlessness
Confusion, anxiety, agitation, delirium, LOC
SEPSIS VERSUS SEPTIC SHOCK

© APON 2003
COMPENSATED SEPTIC SHOCK HYPERDYNAMIC
Early stage of shock Patient usually pancytopenic Often initial presentation May not appear “sick”
CHILLS/FEVER
SLIGHT PO2
SLIGHT PERFUSION
BEGINNING URINE OUTPUT
EARLY SIGNS CONFUSION
10% BLOOD VOLUME
NORMAL RESPIRATORY RATE
NORMAL BP
NORMAL PULSE
TRUNK WARM, PINK

© APON 2003
COMPENSATED SEPTIC SHOCK HYPERDYNAMIC
Intermediate stage of shock Patient usually pancytopenic Appears “sick” May need intubation Still reversible
CHILLS/FEVER THIRST
PULMONARY CONGESTION
PERFUSION CLAMMY
URINE OUTPUT
OBVIOUS CONFUSION ANXIETY
15-20% BLOOD VOLUME
RESPIRATORY RATE HYPOXIA
NORMAL BP
NORMAL PULSE
SKIN COOL/MOTTLED

© APON 2003
DECOMPENSATED SEPTIC SHOCK CARDIOGENIC
Late stage of shock Patient usually pancytopenic Organisms often gram negative Metabolic/lactic acidosis May not be reversible
DELERIUM COMA
>25% BLOOD VOLUME/ CARDIAC OUTPUT
PROFOUND HYPOXIA
SEVERE BP
RAPID THREADY PULSE
TRUNK COOL/MOTTLED
RESPIRATORY FAILURE PULMONARY EDEMA
HEMORRHAGIC LESIONS IN GI TRACT/DIC
OLIGURIA RENAL FAILURE
COLD EXTREMETIES
PERIPHERAL EDEMA

© APON 2003
SEPTIC SHOCK
• Medical Management – symptom management
• pressor support medications
– fluid boluses/hyperhydration • isotonic crystalloid solution (NS) • 20 mls/kg IV
– blood product support – +/- dialysis/ventilator support – treat underlying cause – antibiotics/+/- antifungal agents – +/- CXR

© APON 2003
SEPTIC SHOCK
• Nursing Management/Interventions – obtain blood cultures
– administer IV antibiotics
– close monitoring of VS
– identify early trends
– good communication with team
– patient/family support

© APON 2003
DISSEMINATED INTRAVASCULAR COAGULATION (DIC)
• Definition – alteration in blood clotting mechanisms with amounts
of thrombin and plasmin in the circulation • platelets • prothrombin • fibrinogen
• Manifested by
– diffuse intravascular coagulation – tissue ischemia
• Risk Factors – malignancies – infection – trauma

© APON 2003
DIC
• Clinical Presentation – petechiae/ecchymosis/purpuric rash
– diffuse bleeding
– plt count <20,000/mm3
– PT/PTT 1 1/2-2 times normal
– fibrinogen < 75,000 mgs/dl
– D-dimer > 500 g/L

© APON 2003
DIC
• Medical Management – symptom management
– blood product
– clotting factor replacements
– +/- heparin
• Nursing Management/Interventions – accurate patient assessment
– communicating lab values/findings
– patient/family support

© APON 2003
TYPHLITIS
• Definition – inflammation of the cecum leading to necrotizing
colitis caused by bacterial invasion of the mucosa • most commonly occurs in neutropenic leukemic patients
• Risk Factors – severe/prolonged neutropenia
– acute leukemia induction
– infection/mucositis

© APON 2003
TYPHLITIS
• Clinical Presentation – profound neutropenia/fevers
– severe RLQ abdominal pain/distended abdomen
– high pitched “tinkling” bowel sounds
– N&V/diarrhea

© APON 2003
TYPHLITIS
• Medical Management – broad spectrum antibiotics
– supportive management/bowel rest
– radiology evaluation
– +/- surgery
• Nursing Management/Interventions – accurate patient assessment
– pain management/abdominal girths
– oral/skin/peri-anal care
– patient/family support

© APON 2003
SPINAL CORD COMPRESSION SCC
• Definition – neurological emergency
– occurs in ~ 5% of patients
– usually NOT life threatening
– goal is to preserve neurological function
• Risk Factors – primary CNS tumor of the spinal cord
– neuroblastoma
– lymphoma
– metastatic sarcoma

© APON 2003
SCC
• Clinical Presentation – pain which may be local, referred, or diffuse
– motor deficits • weakness/ataxia
• hypotonic/hyporeflexia
• paralysis/muscle atrophy
– sensory deficits • bowel/bladder dysfunction
• loss of pain/temperature sensation
• paresthesia

© APON 2003
SCC
• Medical Management – neuro exam/MRI
– steroids
– +/- surgical decompression/XRT
– treat underlying disease
• Nursing Management/Interventions – accurate patient assessment
– positioning/ROM/skin care
– safety related to altered mobility
– patient/family support

© APON 2003
SUPERIOR VENA CAVA SYNDROME SVCS
• Definition – compression of superior vena cava (SVC)
• Risk Factors – tumors arising in the anterior mediastinum
or involving mediastinal lymph nodes • NHL, Hodgkin’s disease, T cell ALL, thoracic
neuroblastoma, germ cell tumor
– obstruction of airway
– thrombosis
Tracheal deviation

© APON 2003
SVCS
• Clinical Presentation – cough/dyspnea/orthopnea
– wheezing/stridor
– anxiety/confusion
– edema/plethora
– cyanosis of face/neck/upper arm/chest

© APON 2003
SVCS
• Medical Management – symptom management
– treat underlying cause
– +/- steroids/XRT
• Nursing Management/Interventions – accurate respiratory assessment
– O2
– head of bed
– patient/family support

© APON 2003
SIADH • Definition
– continuous release of ADH without a relationship to plasma osmolality with Na++
leading to cerebral edema/seizures
• Associated with: – in urine output/ in weight without edema
– hyponatremia & H2O intoxification
• Risk Factors – vincristine/cyclophosphamide
– CNS tumors/ALL
– trauma/surgery

© APON 2003
SIADH
• Medical Management – restrict fluids
– treat symptoms/underlying cause
• Nursing Management/Interventions – know “high risk” population
– accurate assessment/I&O/weights
– understand significance of labs
– patient/family support

© APON 2003
ANAPHYLAXIS
• Definition – hypersensitivity reaction to foreign proteins – occurs within seconds/minutes of administration
or at any point during infusion
• Risk Factors – IV medications/infusions/chemotherapy/IVIG – ABX/antifungals – repeated blood product infusions – radiographic contrast media – latex hypersensitivity

© APON 2003
ANAPHYLAXIS
• Clinical Presentation – erythema/flushing/urticaria/pruritis
– anxiety/agitation
– wheezing/dyspnea
– laryngeal edema/stridor
– tachycardia
– N&V/diarrhea

© APON 2003
ANAPHYLAXIS
• Medical Management – administer “test” doses of high risk medications – pretreat with diphenhydramine/hydrocortisone – +/- steroids/cimetidine – epinephrine readily available
• Nursing Management – know risk potential of drug/patient – maintain airway/02
– stop infusion immediately – have emergency drugs/equipment accessible – STAY CALM!!!!!

© APON 2003
CONCLUSION
• Child diagnosed with cancer devastating experience
• Life-threatening event – added stress to a family in crisis
• Excellent nursing assessment – helps minimize severity of oncologic
emergencies

© APON 2003
CASE STUDY
• Jose, a 10 year old with AML, who has a double lumen VAD is on day 9 of induction chemotherapy
• He presents with c/o a sore throat and fever of 101.30 F
• What do you do first?
• VS show BP 80/46, HR 124, RR 28
• Labs: WBC 0.2, HGB 7.4, PLTS 54K
• What other labs might be obtained?
–Chem panel, possibly DIC screen
• What would you expect to be done next?
–Begin IVF’s @ 1.5-2 times maintenance
–Initiate ABX, always alternating lumens

© APON 2003
CASE STUDY
• After ABX begun BP 60/34, HR 130, RR 26 • Skin cool, cap refill > 5 seconds • What do you suspect?
–Septic shock/release of endotoxins
• What might be next step?
–Rapid infusion (s) NS at 20 ml/kg
• What other fluids might be given?
–+/- albumin
–pRBC 10-15 ml/kg when available
–Pheresis pack of platelets
• BP now 90/68, HR 110, RR 22
• Skin warm, pink, cap refill < 3 seconds
• What is most likely organism?
–Alpha strep in AML patients
–Gram negative bacteria

© APON 2003
BIBLIOGRAPHY
Abraham, E., et al. (2000). Consensus conference definitions for sepsis, septic shock, acute lung injury, and acute respiratory distress syndrome: time for a reevaluation. Crit Care Med.; 28: pp. 232-235.
Albin, A. R. (Ed). (1997). Supportive care of children with cancer. Current
therapies and guidelines from the children’s cancer group. (2nd ed). Baltimore: The John Hopkins University Press.
American Academy of Pediatrics (2000). Redbook 2000: Report of the
committee of infectious diseases (25th ed.). Elk Grove, IL: AAP. Bartlett, J. (2002). Pocket book of infectious disease therapy (11th ed.).
Baltimore: Lippincott, Williams, & Wilkins. Brant, J. M. (2002). Rasburicase: An innovative new treatment for
hyperuricemia associated with tumor lysis syndrome. Clinical Journal of Oncology Nursing, (6). pp. 12-16.

© APON 2003
BIBLIOGRAPHY
Carcillo, J. A., et al. (2002). Clinical practice parameters for the hemodynamic support of pediatric and neonatal septic shock. Crit Care Med.; 30(6).
Chernecky, C. C. & Berger, B. J. (Eds.) (1998). Advanced and critical
care oncology nursing: Managing primary complications. Philadelphia: WB Saunders.
Flounders, J. A. (2003) Oncology emergency modules: Spinal cord
compression. ONF January/February online exclusive. Volume 30 number 1. Retrieved February 2003 from ONS Online.
Hockenberry-Eaton M. J. (1998). Essentials of pediatric oncology
nursing: A core curriculum, Glenview IL: APON. Otto, S. E. (2001). Oncology Nursing (4th ed.). St. Louis: Mosby.

© APON 2003
BIBLIOGRAPHY Pizzo, P. & Poplack, D. (Eds.) (2002). Principles and practice of
pediatric oncology (4th ed.). Philadelphia: Lippincott Williams & Wilkins.
Secola, R, Cairo, M., Bessmertony, O., & Bergeron, S. (2002). Tumor
lysis guidelines. COG Nursing Clinical Practice Committee. Truini-Pittman, L., & Rosetto, C. (2002). Pediatric Considerations in
tumor lysis syndrome. Seminars in oncology nursing. (18): 3. pp. 17-22.
Weiner, M. A. & Cairo, M. (Eds.). (2002). Pediatric hematology oncology
secrets. Philadelphia: Hankey and Belfus Inc. Wilson, K. D. (2002). Oncologic emergencies. In Baggott, C. R., Et al.
(Eds.). Nursing care of children and adolescents with cancer (3rd ed.). Philadelphia: WB Saunders.