Embed Size (px)
Citation preview

3111F3
SNOHOMISH SCHOOL DISTRICT 201NEW STUDENT REGISTRATION FORM
SCHOOL: DATE:
Please complete additional registration information on back…
01/2017
IS THERE A JOINT‐CUSTODY OR PARENTING PLAN IN EFFECT? Yes No (If yes, plan must be on file with the school) Copy Attached
IS THERE A RESTRAINING ORDER IN EFFECT? Yes No (If yes, legal papers must be on file with the school) Copy Attached
Restraining order is against: Mother Father Other
SCHOOL PREVIOUSLY ATTENDED SCHOOL DISTRICT PREVIOUSLY ATTENDED PREVIOUS SCHOOL LOCATION (City and State)
HAS STUDENT EVER ATTENDED SNOHOMISH PUBLIC SCHOOLS? Yes No IF YES, NAME OF SCHOOL(S) ATTENDED DATE ATTENDED (Month/Year)
SECOND HOUSEHOLD (Non‐custodial parent/guardian not residing with student) Legal Last Name Legal First Name Middle Name
RELATIONSHIP TO STUDENT Father Mother Stepfather Stepmother Guardian
Grandfather Grandmother Uncle Aunt Agency Friend Self
PHONE #1 (include area code) Home Work Cell
Please check if unlisted
PHONE #2 (include area code) Home Work Cell
Please check if unlisted
PHONE #1 (include area code) Home Work Cell
Please check if unlisted
PHONE #2 (include area code) Home Work Cell
Please check if unlisted
FAMILY EMAIL ADDRESS RELATIONSHIP TO STUDENT: Father Mother Stepfather Stepmother
Guardian Grandfather Grandmother Uncle Aunt Agency
Friend SelfSECOND HOUSEHOLD MAILING ADDRESS (Street/PO Box, City, State, ZIP) ADDITIONAL MAILINGS REQUESTED
Yes No
PRIMARY HOUSEHOLD (primary parent/guardian where student resides) Legal Last Name (of primary contact) Legal First Name Middle Name
PRIMARY CONTACT # (include area code) Home Work Cell
Please check if unlisted
PRIMARY CONTACT PH #2 (area code) Home Work Cell
Please check if unlisted
Legal Last Name Legal First Name Middle Name PHONE #1 (include area code) Home Work Cell
Please check if unlisted
PHONE #2 (include area code) Home Work Cell
Please check if unlisted
FAMILY EMAIL ADDRESS ADDITIONAL EMAIL ADDRESS
RESIDENT ADDRESS
Street Apt # City State ZIP
MAILING ADDRESS (If different from above)
Street Apt # P O Box City State ZIP
Has any member of your family ever been enrolled in the Snohomish School District? Yes No
STUDENT NAME: Legal Last Name Legal First Name Legal Middle Name Also Known As:
BIRTHDATE (Month/Day/Year) GENDER F M
BIRTHPLACE: City County State Country Grade Level:
DISTRICT RESIDENT? Yes No
Resident District:
Military Family Status (circle) A – U.S. Armed Forces active duty G – National Guard member M – More than one member of Armed Forces/National Guard
N – No affiliation R‐ U.S. Armed Forces reserves Z – Do not wish to state
PRIMARY LANGUAGE SPOKEN AT HOME
English
Other
DO NOT WRITE IN SHADED AREA – FOR OFFICE USE ONLY
STUDENT SCHOOL NUMBER SCHOOL ENTRY DATE MEDICAL ALERT HOMEROOM NUMBER LOCKER NUMBER BUS ROUTE
AM PM
RELATIONSHIP TO STUDENT Father Mother Stepfather Stepmother Guardian
Grandfather Grandmother Uncle Aunt Agency Friend Self
RELATIONSHIP TO STUDENT Father Mother Stepfather Stepmother Guardian
Grandfather Grandmother Uncle Aunt Agency Friend Self
(Non‐custodial parent/guardian not residing with student) Legal Last Name Legal First Name Middle Name
RELATIONSHIP TO STUDENT Father Mother Stepfather Stepmother Guardian
Grandfather Grandmother Uncle Aunt Agency Friend Self

3111F1
STUDENT RELEASE AUTHORIZATION
When injury, illness or other non‐emergency situations occur involving your child, we want to be able to quickly reach families or otherresponsible adults. In the event we cannot reach a parent/guardian, please list persons you trust who are available during the day to provide care for your child.
Continue to next page for Ethnicity & Race Information
01/2017
EMERGENCY MEDICAL AUTHORIZATION: I understand that in the event of accident or illness, every effort will be made to contact parent/guardian immediately. If parent/guardian cannot be reached, I authorize school authorities to obtain emergency care for my child.
Legal Parent/Guardian Signature Date
PRIMARY EMERGENCY CONTACT (after parent/guardian contact) Legal Last Name Legal First Name
RELATIONSHIP TO CHILD PHONE #1 (include area code) Home Work Cell
PHONE #2 (include area code) Home Work Cell
PRIMARY CONTACT ADDRESS Street City State ZIP
SECONDARY EMERGENCY CONTACT (after parent/guardian contact) Legal Last Name Legal First Name
RELATIONSHIP TO CHILD PHONE #1 (include area code) Home Work Cell
PHONE #2 (include area code) Home Work Cell
SECONDARY CONTACT ADDRESS Street City State ZIP
STUDENT RELEASE AUTHORIZATION: In the event that the school is unable to contact the parent/guardian, I authorize that my child may be released to the person(s) listed above.
Legal Parent/Guardian Signature Date
SPECIAL INSTRUCTIONS REGARDING RELIGIOUS BELIEFS (Please provide information to school in writing)
PLEASE LIST OTHER SIBLINGS ATTENDING SNOHOMISH PUBLIC SCHOOLS
Last Name First Name School Grade
DOES STUDENT ATTEND CHILD CARE?
Before school After school Before and after school
CHILD CARE PROVIDER Name Address Phone Number
ADDITIONAL CHILD CARE ARRANGEMENTS (Please provide information to school in writing)
HAS YOUR CHILD EVER QUALIFIED FOR OR BEEN ENROLLED IN A SPECIAL EDUCATION
PROGRAM? Yes No
HAS YOUR CHILD EVER BEEN ON AN IEP? (Individualized Education Program) Yes No
HAS YOUR CHILD EVER QUALIFIED FOR OR HAD A 504 PLAN? Yes No
HAS YOUR CHILD EVER PARTICPATED IN: Title – Title 1 Services
LAP – Learning Assistance Program
Gifted – Accelerated Learning Program
ELL – English Language Learner
HAS YOUR CHILD EVER BEEN RETAINED?
Yes No
If yes, at what grade level(s)
HAS THE STUDENT EVER BEEN SUSPENDED FOR A WEAPONS VIOLATION? Yes No Date:

3111F1
SNOHOMISH SCHOOL DISTRICT NO. 201Ethnicity and Race Collection Form – State and Federally Required Information
QUESTION 1. Is your child of Hispanic or Latino origin? (Check all that apply)
QUESTION 2. What race(s) do you consider your child? (Check all that apply)
QUESTION 3. What local race do you consider your child? (Choose one only, please)
ASIAN BLACK, NON‐HISPANIC HISPANIC AMERICAN INDIAN/ALASKAN NATIVE
MULTIRACIAL PACIFIC ISLANDER WHITE, NON HISPANIC NOT PROVIDED
REQUIRED INFORMATION: If born in a country other than the United States, please answer these questions:
How many months have you been in US? How many years? Has your child had any formal education outside the US?
Where and how long?
Legal Parent/Guardian Signature of Verification: Date
02/2018
MEXICAN/ MEXICAN AMERICAN/ CHICANO CENTRAL AMERICAN
SOUTH AMERICAN
LATIN AMERICAN
OTHER HISPANIC/LATINO
NOT HISPANIC/LATINO
CUBAN
DOMINICAN
SPANIARD
ALASKA NATIVE
CHEHALIS COLVILLE
COWLITZ
HOH JAMESTOWN
KALISPEL LOWER
ELWHA LUMMI
MAKAH
MUCKLESHOOT
NISQUALLY
NOOKSACK
PORT GAMBLE KLALLAM
PUYALLUP
QUILEUTE
SAMISH
SAUK‐SUIATTLE
SHOALWATER
SKOKOMISH
SNOQUALMIE
SPOKANE SQUAXIN
ISLAND
STILLAGUAMISH
SUQUAMISH
SWINOMISH TULALIP
YAKIMA
OTHER WASHINGTON INDIAN
OTHER AMERICAN INDIAN
AFRICAN AMERICAN/BLACK
WHITE
NATIVE HAWAIIAN
FIJIAN
GUAMANIAN or CHAMORRO
MARIANA ISLANDER
MALANESIAN
MICRONESIAN
SAMOAN
TONGAN
OTHER PACIFIC ISLANDER
ASIAN INDIAN
CAMBODIAN
CHINESE FILIPINO
HMONG
INDONESIAN
JAPANESE
KOREAN
LAOTIAN
MALAYSIAN
PAKISTANI
SINGAPOREAN
TAIWANESE
THAI
VIETNAMESE
OTHER ASIAN

EMERGENCY INFORMATION
Snohomish School District No. 201, Snohomish, WA 98290
3431F1
Please print student’s last name
Bus #
In order to provide immediate and safe care for your child and carry out your wishes in case of injury or illness at school, we require the following information. Please fill out completely. Please Print.
Student Name
Last First Initial
Birth date Grad Year_
Home Address City Zip Home Phone
Mailing Address if different from home address: City Zip
Lives with: Parents Mother only Mother/Stepfather Guardian Father only Father/Stepmother Other_ Parent/Guardian Name 1. ____________________________ E‐mail Address _____________________ Employer _____________________Work Phone ____________Cell Phone___ _____________________
Parent/Guardian Name 2. ____E‐mail Address
Employer Work Phone Cell Phone
Primary language spoken at home: English Spanish Other
Day Care Provider (if applicable) Phone
Please complete the following if student has a non‐custodial parent who can make emergency decisions for the student and receive copies of records involving this student, including newsletters, grade reports, correspondence, etc.
Home Address City Zip Home Phone
Parent/Guardian Name 1. E‐mail Address _
Place of business Work Phone Cell Phone
Parent/Guardian Name 2. E‐mail Address
Place of business Work Phone Cell Phone
In addition to the parent/guardian, if you cannot be reached, the school may call and release your child to any of the following:
Name 1. Relationship Phone
Work Phone Cell Phone
2. Relationship Phone
Work Phone
Cell Phone
3. Relationship Phone
Work Phone
Cell Phone ___
Please list all children in Snohomish School District this year. (Please list students in this school first.)
Last Name First Name School Grade
Signature of Parent or Legal Guardian Date Please check here if any information on this form is new. ***THIS FORM MUST BE RETURNED AT REGISTRATION 1/2017

Health History 3431 F3
MEDICAL HISTORY (check all that apply) OR no health concerns at this time (please sign form).
State law requires written permission from parent and/or a health care provider before any medications, prescription or over-the-counter medication may be taken at school. Forms are available from the school health rooms or school office. * Law requires that life threatening conditions such as anaphylaxis, asthma, or diabetes have a care plan completed prior to the first day of school. Please contact the building nurse as soon as possible to insure the paper work is complete.
If parent/guardian or authorized emergency contact cannot be reached at the time of a medical emergency, and if immediate care is urgent in the judgment of school authorities. I authorize and direct the school authorities to send the student to the hospital or doctor most accessible. I understand that I will assume full responsibility for the payment of any services rendered. I understand that the information given above will be shared with appropriate school staff that needs to know in order to provide for the health and safety of my student.
I understand that SSD staff may obtain immunization info from Washington State Immunization Information System to update my student’s immunization status. If I do NOT want SSD staff to obtain info from Washington State Immunization Information System I will check here.
Date Signature Relationship Phone
1/2018
Is medication needed at home? ☐NO ☐YES Please List ____________________________________________________________________________________________________________________________________
Is medication needed at school? ☐NO ☐YES Please List ____________________________________________________________________________________________________________________________________
To be completed by parent/guardian
(Last, First): ____________________________________________DOB: ______________ M F Grade: ____________ ID #: _______________
Student Name This information is needed to plan an appropriate program for your student and to prepare for an emergency, should one arise. Your building nurse will contact you if there are any
additional questions.
Hospital preference ___________________________________________________
Health insurance ☐NO ☐YES Name of Company ___________________________
Dental insurance ☐NO ☐YES Name of Company ___________________________
Family doctor ______________________________ Phone ____________________ Date of last physical exam____________ Date of last vision exam _______
Specialist __________________________________ Phone ____________________ Date of last exam ________________________________________________
Dentist ____________________________________ Phone ____________________ Date of last dental exam ___________________________________________
Orthodontist _______________________________ Phone ____________________ Date of last exam ________________________________________________
Congenital Conditions
A_ Please List ___________________________________
Hematology (Blood)
BB *Hemophilia_________________________________
BC Sickle Cell Anemia_____________________________
BD Other Blood Condition_________________________
Cardiovascular/Heart Conditions
C_ Please List___________________________________
Endocrine, Allergy, Immune System, Metabolic, and Nutritional
ED Allergy-Food___________________________________
EE Allergy–Insect__________________________________
E- Other Allergy___________________________________
EG*Anaphylactic Condition (Epi-Pen)_________________
EJ Cystic Fibrosis__________________________________
EK/L*Diabetes Type 1 *Diabetes Type 2
ENEating Disorder________________________________
EU Thyroid Disorder_______________________________
E_ Other Endocrine, Immune, or Metabolic Disorder_____
Gastrointestinal, Dental, and Oral Conditions
GA/J/K Celiac Disease Crohn’s Irritable Bowel
GH/LGastroesophageal Reflux Lactose Intolerance
GI Other________________________________________
GMLiver Disease __________________________________
GD Dental Condition _______________________________
GNOral Condition _________________________________
Musculoskeletal and Connective Tissue
MC Juvenile Idiopathic Arthritis_______________________
MD Muscular Dystrophy_____________________________
MFOsgood-Schlatter_______________________________
MH Scoliosis______________________________________
M_ Other________________________________________
Nervous System
NA Autism Spectrum Disorder
ADHD-Inattentive ADHD-Hyperactive/Impulsive
NB ADHD-Combined Diagnosed by: __________________
NE Cerebral Palsy___________________________________
NF Developmental Delay_____________________________
NH/I/J Migraines Headaches Shunt
NL Intellectually Disabled____________________________
NN Paralysis_______________________________________
NP Seizure Disorder_________________________________
NQ Sensory Condition_______________________________
NS Spina Bifida_____________________________________
NT Spinal Cord Injury________________________________
NU Traumatic Brain Injury____________________________
Behavioral Health Conditions
PH Sleep Disorder__________________________________
PI Tourette Syndrome______________________________
P_ Other_________________________________________
Respiratory
RA Exercise-Induced Bronchospasm *Inhaler
RB/C/DAsthma Mild *Moderate *Severe *Inhaler
RE Reactive Airway Disease__________________________
RF Other_________________________________________
Skin and Subcutaneous Tissue
SB Contact Dermatitis (Eczema)_______________________ S_ Other_________________________________________
Neoplasms (Cancer/Tumors)
T_ Please List______________________________________
Renal and Genitourinary
UB/U- Chronic Urinary Tract Infection Urinary Reflux
UC Dysmenorrhea (painful periods)____________________
U_ Other_________________________________________
Eye and Ear
YB Hearing Impaired________________________________
YA/YC Chronic Ear Infections________ Ear Condition______
YD Visually Impaired________________________________
YE Eye Condition______________ Wears Glasses____

2018-2019 Student Transportation Input Form Will your student ride the school bus during the 2018-2019 school year? Yes ______ No ______ Student's name (first and last) _______________________________________________________________ Student's ID number (please provide if known) _________________________________________________ Student address (home address and city) ______________________________________________________ School student will attend during the 2018-2019 school year
Cathcart Elementary ______ Centennial Middle School ______ Central Primary Center ______ Valley View Middle School ______ Cascade View Elementary ______ Glacier Peak High School ______ Dutch Hill Elementary ______ Snohomish High School ______ Emerson Elementary ______ Aim High School _______ Little Cedars Elementary ______ Machias Elementary ______ Riverview Elementary ______ Seattle Hill Elementary ______ Totem Falls Elementary ______
Grade student will be in during the 2018-2019 school year
Kindergarten ______ 7th grade ______ 1st grade ______ 8th grade ______ 2nd grade ______ 9th grade ______ 3rd grade ______ 10th grade ______ 4th grade ______ 11th grade ______ 5th grade ______ 12th grade ______ 6th grade ______
A.M pick-up location Home ______ Student does not plan to ride the bus ______ Other ______ P.M. drop-off location Home ______ Student does not plan to ride the bus ______ Other ______ Will student be making a request for a permanent bus pass at the beginning of the year for alternative pick-up or drop-off location? If so, to where? _________________________________________________ Parent's name (printed) ___________________________________________________________________ Parent's signature ________________________________________________________________________ E-mail address ___________________________________________________________________________ Contact phone number ____________________________________________________________________ The form will need to be completed for every student in your household who will attend a Snohomish School District School in the 2018-2019 school year. Please return this completed form to your student’s school. Please contact the Transportation Dept. at (360) 563-3525 if you have any questions or
concerns.

School Attendanceform1601 Avenue D, Snohomish, WA 98290-1799
360-563-7300 Fax 360-563-7279
School attendance is required by state law.• State law requires children from age 8 to 17 to attend
school.
• Children that are 6- or 7-years-old, who are enrolled in school, must also attend school.
• Youth who are 16 or older may be excused from attending school if they meet certain requirements per state law (RCW 28A.225.010).
• If your child is going to be absent, please contact the school office.
School’s duties upon a student’s absences:• If your child has two unexcused absences in one
month, state law (RCW 28A.225.020) requires we schedule a conference with you and your child.
• In elementary school after five excused absences in any month, or ten or more excused absences in the school year, the school district is required to contact you to schedule a conference. A conference is not required if your child has provided a doctor’s note, or pre-arranged the absence in writing, and plans are in place so your child does not fall behind academically.
• If your child has seven unexcused absences in any month or ten unexcused absences within the school year, we are required to file a petition with the juvenile court, alleging a violation of RCW 28A.225.010, the mandatory attendance laws. You and your child may need to appear in juvenile court.
Did you know? • Attending school on-time, all day, every day will give
your child the best chance of graduating from high school.
• Starting in kindergarten, missing on average just two days a month, whether excused or unexcused, makes it more likely that your child will not meet academic standards in math and reading by third grade.
• By 6th grade, absenteeism is one of three signs that a student may drop out of high school.
• Absences can be a sign that a student is losing interest in school, struggling with school work, dealing with a bully or facing some other potentially serious difficulty.
• By 9th grade, regular attendance is a better predictor of high school graduation rates than 8th grade test scores.
What you can do:• Don’t let your child stay home unless they are truly
sick, such as fever, vomiting, diarrhea, or a contagious rash.
• Avoid appointments and travel when school is in session.
• Keep track of your child’s attendance. Missing more than nine days, excused or unexcused, could put your child at risk of falling behind.
• Set a regular bedtime and morning routine as well as finishing homework and packing backpacks the night before.
• Have a back-up plan in place with family members, neighbors, or other parents for getting your child to school in case something comes up.
If you are struggling to get your child to school for any reason, we are here to support you and work with you towards possible solutions. Please do not hesitate to contact the school office to schedule an appointment to discuss your child’s attendance.

I acknowledge that I have read (or I have had someone read this to me) and I understand this document.
Student Name: ____________________________________________________________________________________________ First Middle Last
Date of Birth: __________________ Age: ______ Grade: ______ Name of School: ___________________________________
Current address:___________________________________________________________________________________________ Street City Zip
Phone/Contact Number: ___________________________________________________________________________________
Do you have other children that attend a school in the Snohomish School District?
Name: _________________________Date of Birth: _________Age: _______ Grade:_______ School: ___________________
Name: _________________________Date of Birth: _________Age: _______ Grade:_______ School: ___________________
Name: _________________________Date of Birth: _________Age: _______ Grade:_______ School: ___________________
I declare under penalty of perjury under the laws of the State of Washington that the information provided here is true and accurate.
Print name of person completing form: ___________________________________________________________________
Signature: _____________________________________________________________Date: ___________________________
Relationship to student(s): Parent Guardian Self Other ––––––––––––––––––––––––––––––––––––––
Please read and complete this form and return to your child's school office by the end of September.

Student Housingquestionnaire
The answers to the following questions help determine educational services your child(ren) may be eligible to receive through the McKinney-Vento Homeless Assistance Act.
Are you ‘doubled up’ with another family due to a loss of housing or economic hardship? Yes No
Are you living in a motel/hotel due to lack of housing? Yes No
Are you living in a shelter? Yes No
Are you living in a car, park, campsite or location not usually used for sleeping accommodations? Yes No
As a student, are you living with someone other than your parent? Yes No
If you answered YES to any of the above questions, please complete the remainder of this form and return it to your child’s school.
If you answered NO to all of the above questions, you may stop here.
Student Name: ____________________________________________________________________________________________ First Middle Last
Date of Birth: __________________ Age: ______ Grade: ______ Name of School: ___________________________________
Current address:___________________________________________________________________________________________ Street City Zip
Phone/Contact Number: ___________________________________________________________________________________
Do you have other children that attend a school in the Snohomish School District?
Name: _________________________Date of Birth: _________Age: _______ Grade:_______ School: ___________________
Name: _________________________Date of Birth: _________Age: _______ Grade:_______ School: ___________________
Name: _________________________Date of Birth: _________Age: _______ Grade:_______ School: ___________________
I declare under penalty of perjury under the laws of the State of Washington that the information provided here is true and accurate.
Print name of person completing form: ___________________________________________________________________
Signature: ____________________________________________________________ Date: ___________________________
Relationship to student(s): Parent Guardian Self Other ––––––––––––––––––––––––––––––––––––––
1601 Avenue D, Snohomish, WA 98290-1799360-563-7300 Fax 360-563-7279
For School Staff Only: If “Yes” is checked for any question above, please give this form to the School Counselor or Administrator

01/2017
Photos/Recordings Opt‐Out Form
There are times during the year when photographs or audio‐visual recordings of studentsmay be taken for school or district use. When possible, we will alert parents in advance, but this is not always possible.
It is important that you know that student family members, community members, and attendees at school events may take and publish photos and other recordings of students without coordinating such with school district personnel, and it is possible that your student could appear in a third party's photos and other recordings. Snohomish School District is not responsible for the use of any of your student’s likeness (photo, voice, etc.) that appears in those photos and recordings.
You may choose to opt out of allowing your student to appear in photos or otherrecordings taken by or on behalf of the Snohomish School District by checking and signing below.
I do NOT want my student to appear in photos or audio‐visual recordings taken by or on behalf of the Snohomish School District. (By checking this box your student will NOT appear inANY photos and recordings taken for yearbook, classroom/school/district presentations,parent club/classroom/school/district newsletters, media, etc.)
Please note – Opt‐out restrictions must be renewed at the beginning of each school year.
Student _______________________________ _____________________________ Last Name First Name
Parent _______________________________ _____________________________ Last Name First Name
3600F3
F o r O f f i c e U s e O n l y 1. Enter opt‐out date in Skyward student record – custom forms/internet opt out. 2. From WS/ST/TB/CF – web student/student tabs/custom forms 3. Check photo opt‐out box and enter date of opt out. 4. Retain this signed form at the school for the duration of school year.
Parent Signature ___________________________________________________________________
Contact Phone __________________________ Date________________________________

If you have a disability and need this document in another format, please call 1‐800‐525‐0127 (TDD/TTY call 711). DOH 348-295 November 2017
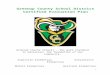
Parents - Are Your Kids Ready for School?
Required Immunizations for School Year 2018-2019
Hepatitis B
DTaP/Tdap (Diphtheria, Tetanus,
Pertussis) Vaccine doses required may
be fewer than listed
Polio Vaccine doses required
may be fewer than listed
MMR (Measles, Mumps,
Rubella)
Varicella (Chickenpox)
Kindergarten – 5th Grade
3 doses within the correct timeframes
5 doses within the correct timeframes
4 doses within the correct timeframes
2 doses within the correct timeframes
2 doses within the correct timeframes
OR Healthcare provider verified
child had disease
6th – 12th Grade 3 doses within the correct timeframes
5 doses DTaP
AND
1 dose Tdap, all within the correct timeframes
4 doses within the correct timeframes
2 doses within the correct timeframes
2 doses within the correct timeframes
OR Healthcare provider verified
child had disease (Exceptions are allowed for
certain students)
Students must get vaccine doses at correct timeframes to be in compliance with the requirements. Talk to your healthcare provider or school staff if you have questions about school immunization requirements.
Find information on other recommended vaccines not required for school: www.immunize.org/cdc/schedules/
Parent/Guardian Instructions: To see which vaccines are required for school, find your child’s grade and look only at that row going across to find the vaccines and number of doses required.

Certificate of Immunization Status (CIS) For Kindergarten-12th Grade / Child Care Entry
Please print. See back for instructions on how to fill out this form or get it printed from the Washington Immunization Information System.
Child’s Last Name: First Name: Middle Initial: Birthdate (MM/DD/YY): Sex: ____________________________________________________________________________________________________________________________________________________
I give permission to my child’s school to share immunization information with the Immunization Information System to help the school maintain my child’s school record. ______________________________________________________________ Parent/Guardian Signature Required Date
I certify that the information provided on this form is correct and verifiable.
______________________________________________________________ Parent/Guardian Signature Required Date
♦ Required for School and Child Care/Preschool Date MM/DD/YY
Date MM/DD/YY
Date MM/DD/YY
Date MM/DD/YY
Date MM/DD/YY
Date MM/DD/YY
Documentation of Disease Immunity Healthcare provider use only
If the child named in this CIS has a history of Varicella (Chickenpox) or can show immunity by blood test (titer) it MUST be verified by a healthcare provider I certify that the child named on this CIS has: a verified history of Varicella (Chickenpox). laboratory evidence of immunity (titer) to disease(s) marked below. Lab report(s) for titers MUST also be attached. Diphtheria Mumps Other: Hepatitis A Polio __________ Hepatitis B Rubella __________ Hib Tetanus Measles Varicella
Licensed healthcare provider signature Date (MD, DO, ND, PA, ARNP) Printed Name
● Required Only for Child Care/Preschool
Required Vaccines for School or Child Care Entry
♦ DTaP / DT (Diphtheria, Tetanus, Pertussis)
♦ Tdap (Tetanus, Diphtheria, Pertussis)
♦ Td (Tetanus, Diphtheria)
♦ Hepatitis B 2-dose schedule used between ages 11-15
● Hib (Haemophilus influenzae type b)
♦ IPV / OPV (Polio)
♦ MMR (Measles, Mumps, Rubella)
● PCV / PPSV (Pneumococcal)
♦ Varicella (Chickenpox) History of disease verified by IIS
Recommended Vaccines (Not Required for School or Child Care Entry)
Flu (Influenza)
Hepatitis A
HPV (Human Papillomavirus)
MCV / MPSV (Meningococcal)
MenB (Meningococcal)
Rotavirus
Office Use Only:
Reviewed by: Date:
Signed Cert. of Exemption on file? Yes No

To print with immunization information filled in: Ask if your healthcare provider’s office enters immunizations into the WA Immunization Information System (Washington’s statewide
database). If they do, ask them to print the CIS from the IIS and your child’s immunization information will fill in automatically. You can also print a CIS at home by signing up and logging into MyIR at https://wa.myir.net. If your provider doesn’t use the IIS, email or call the Department of Health to get a copy of your child’s CIS: [email protected] or 1-866-397-0337.
To fill out the form by hand: #1 Print your child’s name, birthdate, sex, and sign your name where indicated on page one. #2 Vaccine information: Write the date of each vaccine dose received in the date columns (as MM/DD/YY). If your child receives a combination vaccine (one shot that protects against
several diseases), use the Reference Guides below to record each vaccine correctly. For example, record Pediarix under Diphtheria, Tetanus, Pertussis as DTaP, Hepatitis B as Hep B, and Polio as IPV.
#3 History of Varicella Disease: If your child had chickenpox (varicella) disease and not the vaccine, a health care provider must verify chickenpox disease to meet school requirements.
If your healthcare provider can verify that your child had chickenpox, ask your provider to check the box in the Documentation of Disease Immunity section and sign the form. If school staff access the IIS and see verification that your child had chickenpox, they will check the box under Varicella in the vaccines section.
#4 Documentation of Disease Immunity: If your child can show positive immunity by blood test (titer) and has not had the vaccine, have your healthcare provider check the boxes for the appropriate disease in the Documentation of Disease Immunity box, and sign and date the form. You must provide lab reports with this CIS.
Reference guide for vaccine trade names in alphabetical order For updated list, visit https://fortress.wa.gov/doh/cpir/iweb/homepage/completelistofvaccinenames.pdf Trade Name Vaccine Trade Name Vaccine Trade Name Vaccine Trade Name Vaccine Trade Name Vaccine
ActHIB® Hib Fluarix® Flu Havrix® Hep A Menveo® Meningococcal Rotarix® Rotavirus (RV1)
Adacel® Tdap Flucelvax® Flu Hiberix® Hib Pediarix® DTaP + Hep B + IPV RotaTeq® Rotavirus (RV5)
Afluria® Flu FluLaval® Flu HibTITER® Hib PedvaxHIB® Hib Tenivac® Td
Bexsero® MenB FluMist® Flu Ipol® IPV Pentacel® DTaP + Hib + IPV Trumenba® MenB
Boostrix® Tdap Fluvirin® Flu Infanrix® DTaP Pneumovax® PPSV Twinrix® Hep A + Hep B
Cervarix® 2vHPV Fluzone® Flu Kinrix® DTaP + IPV Prevnar® PCV Vaqta® Hep A
Daptacel® DTaP Gardasil® 4vHPV Menactra® MCV or MCV4 ProQuad® MMR + Varicella Varivax® Varicella
Engerix-B® Hep B Gardasil® 9 9vHPV Menomune® MPSV4 Recombivax HB® Hep B
If you have a disability and need this document in another format, please call 1-800-525-0127 (TDD/TTY call 711). DOH 348-013 December 2016
Reference guide for vaccine abbreviations in alphabetical order For updated list, visit https://fortress.wa.gov/doh/cpir/iweb/homepage/completelistofvaccinenames.pdf Abbreviations Full Vaccine
Name Abbreviations Full Vaccine Name Abbreviations Full Vaccine
Name Abbreviations Full Vaccine Name Abbreviations Full Vaccine Name
DT Diphtheria, Tetanus Hep A Hepatitis A MCV / MCV4 Meningococcal Conjugate Vaccine OPV Oral Poliovirus
Vaccine Tdap Tetanus, Diphtheria, acellular Pertussis
DTaP Diphtheria, Tetanus, acellular Pertussis
Hep B Hepatitis B MenB Meningococcal B PCV / PCV7 / PCV13
Pneumococcal Conjugate Vaccine VAR / VZV Varicella
DTP Diphtheria, Tetanus, Pertussis Hib Haemophilus
influenzae type b MPSV / MPSV4 Meningococcal Polysaccharide Vaccine
PPSV / PPV23 Pneumococcal Polysaccharide Vaccine
Flu (IIV) Influenza HPV (2vHPV / 4vHPV / 9vHPV)
Human Papillomavirus MMR Measles, Mumps,
Rubella Rota (RV1 / RV5) Rotavirus
HBIG Hepatitis B Immune Globulin IPV Inactivated
Poliovirus Vaccine MMRV Measles, Mumps, Rubella with Varicella
Td Tetanus, Diphtheria
Instructions for completing the Certificate of Immunization Status (CIS): printing it from the Immunization Information System (IIS) or filling it in by hand.

Certificate of Exemption - Personal/Religious From School, Childcare, and Preschool Immunization Requirements Complete the box for the desired exemption type
If you have a disability and need this form in a different format please call 1-800-525-0127 (TDD/TTY Call 711) DOH-348-106 January 2018
Religious Membership Exemption Complete this section ONLY if you belong to a church or religion that objects to the use of medical treatment. Use the section above if you have a religious objection to vaccinations but the beliefs or teachings of your church or religion allow for your child to be treated by medical professionals such as doctors and nurses. Parent/Guardian Declaration I am the parent or legal guardian of the above named child. I affirm that I am a member of a church or religion whose teaching preclude health care practitioners from providing medical treatment to my child. I have received notice that if an outbreak of vaccine-preventable disease for which my child is exempted occurs, my child may be excluded from the school or child care center for the duration of the outbreak. The information on this form is complete and correct. Parent/Guardian Name (print) Parent/Guardian Signature Date Name of Church or Religion of which you are a member:
Personal/Philosophical or Religious Exemption Exemption Type: ☐Personal/Philosophical ☐Religious I am exempting my child from the requirement that my child be vaccinated against the following diseases to attend school or child care: Diphtheria Hepatitis B Hib Measles Mumps Pertussis (whooping cough) Pneumococcal Polio Rubella Tetanus Varicella (chickenpox)
Parent/Guardian Declaration One or more of the required vaccines are in conflict with my personal, philosophical or religious beliefs. I have discussed the benefits and risks of immunizations with the health care practitioner below. I have received notice that if an outbreak of vaccine-preventable disease for which my child is exempted occurs, my child may be excluded from the school or child care center for the duration of the outbreak. The information on this form is complete and correct. Parent/Guardian Name (print) Parent/Guardian Signature Date Health Care Practitioner Declaration I have discussed the benefits and risks of immunizations with the parent/legal guardian as a condition for exempting their child. I am a qualified MD, ND, DO, ARNP or PA licensed under Title 18 RCW, and the information provided on this form is complete and correct.
☐MD ☐ND ☐DO ☐ARNP ☐PA Licensed Health Care Practitioner Name (print) Licensed Health Care Practitioner Signature Date
Child’s Last Name: First Name: Middle Initial: Birthdate (mm/dd/yyyy): Gender:
NOTICE: A parent or guardian may exempt their child from some or all vaccinations listed below by submitting this completed form to the child’s school and/or child care. A person who has been exempted from a vaccination is considered at risk for the disease or diseases for which the vaccination offers protection. Exempted children/students may be excluded from school or child care settings and activities during an outbreak of the disease that they have not been fully vaccinated against. The diseases vaccines can protect against still exist, and can spread quickly in school and child care settings. Immunizations are one of the best ways to protect people from getting and spreading diseases that may result in serious illness, disability, or death.

Certificate of Exemption - Medical From School, Childcare, and Preschool Immunization Requirements Complete the box for the desired exemption type
If you have a disability and need this form in a different format please call 1-800-525-0127 (TDD/TTY Call 711) DOH-348-106 January 2018
NOTICE: A parent or guardian may exempt their child from some or all vaccinations listed below by submitting this completed form to the child’s school and/or child care. A person who has been exempted from a vaccination is considered at risk for the disease or diseases for which the vaccination offers protection. Exempted children/students may be excluded from school or child care settings and activities during an outbreak of the disease that they have not been fully vaccinated against. The diseases that vaccines can protect against still exist, and can spread quickly in school and child care settings. Immunizations are one of the best ways to protect people from getting and spreading diseases that may result in serious illness, disability, or death.
Child’s Last Name: First Name: Middle Initial: Birthdate (mm/dd/yyyy): Gender:
Medical Exemption Licensed Health Care Practitioner (MD, ND, DO, ARNP, PA) completes this section. A health care practitioner may grant a medical exemption to a vaccine antigen required by rule of the state board of health only if in his or her medical judgment, the vaccine antigen is not advisable for the child. When it is determined that this particular vaccine antigen is no longer contraindicated, the child will be required to have the vaccine (RCW 28A.210.090). Guidance for medical exemptions for vaccination can be obtained from the contraindications, indications, and precautions described in the vaccine manufacturer’s package insert and by the most recent recommendations of the Advisory Committee on Immunization Practices (ACIP) available in the Centers for Disease Control and Prevention publication, Guide to Vaccine Contraindications and Precautions. This guide can be found at the following website: https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/contraindications.html
Please indicate which vaccine antigen(s) the medical exemption is referring to:
Disease Permanent Temporary Expiration Date for Temporary Medical
Diphtheria
Hepatitis B
Hib
Measles Mumps
Pertussis
Pneumococcal
Polio Rubella
Tetanus
Varicella I declare that vaccination for the disease/s checked above is not advisable for this child. I have discussed the benefits and risks of immunizations with the parent/legal guardian as a condition for exempting their child. I am a qualified MD, ND, DO, ARNP or PA licensed under Title 18 RCW, and the information provided on this form is complete and correct.
☐MD ☐ND ☐DO ☐ARNP ☐PA Licensed Health Care Practitioner Name (print) Licensed Health Care Practitioner Signature Date
Parent/Guardian Declaration I have discussed the benefits and risks of immunizations with the health care practitioner granting this medical exemption. I have received notice that if an outbreak of vaccine-preventable disease for which my child is exempted occurs, my child may be excluded from the school or child care center for the duration of the outbreak. The information on this form is complete and correct.
Parent/Guardian Name (print) Parent/Guardian Signature Date

English/November 2016
Office of Superintendent of Public Instruction (OSPI)
Home Language Survey
The Home Language Survey is given to all students enrolling in Washington schools.
Student Name: Grade: Date:
Parent/Guardian Name Parent/Guardian Signature
Right to Translation and
Interpretation Services
Indicate your language preference so
we can provide an interpreter or
translated documents, free of
charge, when you need them.
All parents have the right to information about their child’s
education in a language they understand.
1. In what language(s) would your family prefer to communicate
with the school?
__________________________________
Eligibility for Language
Development Support
Information about the student’s
language helps us identify students
who qualify for support to develop
the language skills necessary for
success in school. Testing may be
necessary to determine if language
supports are needed.
2. What language did your child learn first?
__________________________________
3. What language does your child use the most at home?
__________________________________
4. What is the primary language used in the home, regardless of
the language spoken by your child?
__________________________________
5. Has your child received English language development support
in a previous school? Yes___ No___ Don’t Know___
Prior Education
Your responses about your child’s
birth country and previous
education:
Give us information about the
knowledge and skills your child is
bringing to school.
May enable the school district to
receive additional federal funding
to provide support to your child.
This form is not used to identify
students’ immigration status.
6. In what country was your child born? ___________________
7. Has your child ever received formal education outside of the
United States? (Kindergarten – 12th grade) ____Yes ____No
If yes: Number of months: ______________
Language of instruction: ______________
8. When did your child first attend a school in the United States? (Kindergarten – 12th grade)
_______________________
Month Day Year
Thank you for providing the information needed on the Home Language Survey. Contact your school
district if you have further questions about this form or about services available at your child’s school.
Note to district: This form is available in multiple languages on http://www.k12.wa.us/MigrantBilingual/HomeLanguage.aspx. A response that includes a language other than English to question #2 OR question #3 triggers English language proficiency placement testing. Responses to questions #1 or #4 of a language other than English could prompt further conversation with the family to ensure that #2 and #3 were clearly understood. ”Formal education” in #7 does not include refugee camps or other unaccredited educational programs for children.
Forms and Translated Material from the Bilingual Education Office of the Office of Superintendent of Public Instruction are licensed under a Creative
Commons Attribution 4.0 International License.

SNOHOMISH SCHOOL DISTRICT NO. 201
Snohomish, Washington 98290
CONSENT TO RELEASE EDUCATIONAL RECORDS
Student_________________________________________________________ Birth date__________________ Last First Middle
School_________________________________________________________________________________________________________________
For the purpose of gathering data relevant to educational programming, I authorize the release of information regarding the above‐named student between the Snohomish School District and:
Name/Agency___________________________________________________________ Phone_____________________
Address________________________________City/State_______________________ Zip________________________
Name/Agency___________________________________________________________ Phone_____________________
Address________________________________City/State________________________Zip________________________
I acknowledge notification of this transfer of records as required by the Family Educational Rights and Privacy Act of 1974 and understand that I
have a right to receive a copy at my own expense, if requested, and have an opportunity for a hearing to challenge the content of the records.
I understand that the information transferred will be treated in a confidential manner and will not be transmitted to a third party without
my consent, except as allowed by WAC 392‐171‐631.
Signature_________________________________________________________________________Date______________________Parent, guardian or adult student
Address________________________________________City/State__________________________Zip___________________
Phone__________________________________________
Responding agency please address information regarding this student to:
Snohomish School District No. 201
Attention__________________________________________________________________________________________
School/Department__________________________________________________________________________________
Phone____________________________________________________________________________________________
Email address_______________________________________________Fax Number______________________________
Address________________________________________ City/State___________________________ Zip_____________
3600F11/2017