Embed Size (px)
Citation preview

Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida
Angela Dispenzieri, M.D.
Professor of Medicine and Laboratory Medicine
October 22, 2015
Smoldering multiple myeloma: who and when to treat
Mayo Clinic College of Medicine
Mayo Clinic Comprehensive Cancer Center

Disclosures
Company Disclosure
Celgene Research dollars
Millenium Research dollars
Pfizer Research dollars
Jannsen Research dollars

SMM: who and when to treatOUTLINE
1. New definitions of MM and SMM
2. Whom to treat?

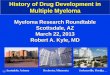
Progression of SMM & MGUS
0
20
40
60
80
100
0 1 2 3 4 5
Years since diagnosis
Pro
bab
ilit
y o
f p
rog
res
sio
n (
%)
Smoldering multiple myeloma
MGUS
1016
21
7873
66
51
4
Kyle NEJM 2007;356:2582-90
5 10 15 20 25
10%/year
3%/year
1%/year

Time from SMM diagnosis (years)
Pro
bab
ilit
y o
f p
rog
ressio
n
(%)
DispenzieriKyle RajkumarLarsen HillengassPersona-Perez
RajkumarNeben
BMPC ≥10
M-protein≥30 g/L
BMPC ≥10
M-protein≥30 g/L
iFLC/uFLC≥8
i/u FLC ≥100 Del 17p, t(4;14)
Trisomies
Any otheriFISH abnl
Normal iFISH
Aberrant PC% >95%
Suppressionof Igs
>1 focal lesion on whole body MRI
Del 17p, t(4;14), +1q21 or hyperdipoid
M-protein≥20 g/L
BMPC ≥60%
SMM Risk of Progression: Different prognostic factors
Dispenzieri 2013. Blood 122:4172-80

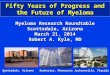
Risk of progression in SMM using multiparameter flow cytometry of BMPCs
SMM
N=58
SMM with
MGUS-like
profile
N=41
SMM with
MM-like
profile
N=15
15 mo.
Not reached
108 mo. .
Paiva B, Leukemia 2013;27:2056-61.

Diagnosis of myeloma: Revised Definition of MM
1. Term “symptomatic MM” “MM”
• MM does not require the presence of symptoms
• Attributable end-organ damage or presence of other myeloma defining events (MDEs) is sufficient
Rajkumar SV, Lancet Oncology 2014; 15:e538-48

Features in SMM posed risk for progression,
so now “Myeloma Defining Events”
Biomarker
2-year risk
of
progression
Comments
BM PCs > 60% 90% Reproducible in 3 independent studies
Involved/uninvolved FLC
ratio > 10080% Reproducible in 2 independent studies
Whole-body MRI 70% Reproducible in 2 independent studies
Rajkumar SV, Lancet Oncology 2014; 15:e538-48

• No MDE AND
• <10% BMPC AND
• <3gm/dL M protein
• No MDE AND
• ≥10-60% BMPC OR
• ≥3 gm/dL S. M protein OR
• ≥500 mg/24h Ur. M protein
• PCPD, AND
• 1 or more MDE
• CRAB
• ≥60% BMPC
• ≥100 FLC ratio
• >1 MRI focal lesion
CRAB= Hypercalcemia, renal failure, anemia, or lytic bone lesions attributable to a clonal plasma cell disorder
MDE= Myeloma Defining Events
MGUS SMM MM
Rajkumar SV, et al. Lancet Oncol. 2014;15:e538-e548.
Revised IMWG Criteria

Revised Definition of MMClarification of MDE’s
a. CT and PET-CT can be used for detecting
osteolytic bone lesions
b. Osteoporosis and compression fractures
alone are NOT considered as MDEs
c. CrCl <40ml/min can be used as cut-off for
renal failure in addition to serum creatinine
d. Infections and hyperviscosity are NOT
enough to qualify as MDEs
e. Anemia and hypercalcemia unchanged
Rajkumar SV, Lancet Oncology 2014; 15:e538-48

PET-CT has major diagnostic value in the evaluation of smoldering myeloma
Unpublished data Dysktra ASH 2014
198 Patients
82 PET positive 116 PET negative
33 obs as SMM 49 dx’d and
treated as MM(12 upstaged
by PET alone)
17 dx’d and
treated as MM
89 obs as SMM
Prog by
2 years:19
(56%)
27
(28%)
Med.
TTP:16 mo 55 mo
14/19
(74%)
12/44
(27%)
If PET w/in 90 days
of SMM dx

SMM: who and when to treatOUTLINE
1. New definitions of MM and SMM
2. Whom to treat?

PRIMUM NON NOCEREFirst do no harm

SMM: Pilot and Phase 2 Studies
Ref Regimen N PFS OS
1 Delayed MP 54 2-yr PFS 75% 5-yr 80%
2 Pamidronate 12 2-yr TTP 25% NA
3 Thal. + Pam. 76 4-yr EFS 60% 4 yr OS 91%
4, 5 Thalidomide 29 35 m 49 m
6 Thalidomide 28 NA NA
7IL-1 receptor antagonist
+/- dex47 37 m NA
8 Curcumin 17 NA NA
9 Car-Len-Dex 12 NA NA
1. Peest D, Eur J Cancer 1995;2:146-51. 2. Martin A, BJH 2002;118:239-42.
3. Barlogie B, Blood 2008;112:3122-5. 4. Rajkumar SV, Leukemia 2001;15:1274-6.
5. Detweiler-Short K, AJH 2010;85:737-40. 6. Weber D, JCO 2003;21:16-9.
7. Lust JA, Mayo Clin Proc 2009;84:114-22. 8. Golombick T, AJH 2012;87:455-60.
9. Landgren O, Blood 2014 124(21): abstract

SMM: Randomized Controlled Trials
Ref Therapy N PFS OS
1Mel-Pred: early
v delayed50 12 m ND
2,3Mel-Pred: early
v delayed145 ~12 m 64 v 71 m
4,5 Pam v Obs. 1775-yr 53%;
SRE 74% v 39%*46 v 48 m
6 Zol. v Obs. 16367 v 59 m, p=NS; SRE 55% v 78%**
ND
7Thal + Zol. v
Zol.68 29 v 14 m* 6-yr >70%
8Len+dex len
v Obs.119 2-yr: 92 v 50%* 3 yr: 93 v 76%**
ND * P < 0.01 **P <0.05
1. Hjorth M, EJH 1993;50:95-102. 2. Riccardi A, BJC 1994;70:1203-10.
3. Riccardi A, BJC 2000;82:1254-60. 4. Musto P, Leuk & lymph 2003;44:1545-8.
5. D'Arena G, Leuk & lymph 2011;52:771-5. 6. Musto P, Cancer 2008;113:1588-95.
7. Witzig TE, Leukemia 2013;27:220-5. 8. Mateos MV, NEJM 2013;369:438-47.

Lenalidomide 10 mg/day, D1-21 (28 day cycle) for 2 yrs
Therapeutic abstention
• Primary endpoint: time to progression to symptomatic MM
• Secondary endpoints: response rates, duration of response, progression-free survival, overall survival, and safety and tolerability
Lenalidomide 25 mg/day, D1-21 Dexamethasone20 mg D1-D4 and D12-D15
Therapeutic abstention
Randomization of high-risk* smoldering MM patients:
Induction:9 28-day cycles
Maintenance:until progression
*PCs BM ≥ 10% plus M-protein ≥ 30 g/L or PCs BM ≥ 10% or M-protein ≥ 30 g/L but BM aPC/nPC > 95% plus immunoparesis.aPC, abnormal plasma cell; MM, multiple myeloma; nPC, normal plasma cell; PC plasma cell.
Mateos MV, et al. N Engl J Med. 2013;369:438-447.
High-risk SMM: len/dex vs observation

1. BMPC ≥ 10% and M-protein ≥ 30 g/L
or
2. BMPC ≥ 10% or M-protein ≥ 30 g/L and
• BM aPC/nPC > 95% and
• Immunoparesis
High-risk SMM: len/dex vs observation
Eligibility
Mateos MV, et al. N Engl J Med. 2013;369:438-447

Lenalidomide plus dexamethasone for high-risk smoldering MM.
Baseline Characteristics
Mateos NEJM 2013;369:438-47.

Lenalidomide-dex for high-risk SMM. Freedom from progression
Mateos NEJM 2013;369:438-47.
Len-dex for high-risk smoldering MM. PFS

Len-dex for high-risk SMM. Overall survival
Mateos NEJM 2013;369:438-47.

Lenalidomide-dex for high-risk SMM. Response to therapy
Mateos NEJM 2013;369:438-47.

Len-dex for high-risk SMMAdverse Events
Mateos NEJM 2013;369:438-47.

Len-dex for high-risk SMM. Lessons learned
1. Treating patients with higher risk SMM can prevent morbidity & mortality
2. Waiting for end-organ damage alone to start therapy may increase morbidity & mortality

How does the GEM SMM trial high-risk population compare to high-
risk, new criteria?
GEM SMM
trial
‘high-risk’
IMWG ultra
high-risk
that is
now MM
?

Time from SMM diagnosis (years)
SMM Risk of Progression:
Different prognostic factors
Dispenzieri 2013. Blood 122:4172-80
High risk according to
PETHEMA/GEM SMM trial
Ultra-high risk
which is now MM
Pro
gre
ss
ion
, %
Rajkumar
BMPC ≥60%
1 3 51 3 51 3 51 3 5 1 3 5

A Theoretical Model
Landgren et al, Clin Cancer Research 2011

A Theoretical Model
Chemotherapy Disruption of
homeostasis
with death of
‘benign’ clone
& growth of ‘malignant’ clone
‘Benign’ clone
‘Malignant’ clone

How do new definitions affect management / prognosis of
SMM?

Progression of SMM & MGUS
0
20
40
60
80
100
0 1 2 3 4 5
Years since diagnosis
Pro
bab
ilit
y o
f p
rog
res
sio
n (
%)
Smoldering multiple myeloma
MGUS
1016
21
7873
66
51
Modified from Kyle NEJM 2007;356:2582-90
5 10 15 20 25
SMM w/o high risk?

Hypothetical Progression of SMM
0
20
40
60
80
100
0 1 2 3 4 5
Years since diagnosis
Pro
bab
ilit
y o
f p
rog
res
sio
n (
%)
MGUS
1016
21
Modified from Kyle NEJM 2007;356:2582-90
5 10 15 20 25
SMM w/o high risk?

On-going trials for SMM
Sponsor Design Drug N, SMM End-points
ECOG Open
label RCT
Len v Obs 370 high-
risk
TTP
Novartis Phase II BHQ880
(DKK1) Ab
58 high-risk Response
rate
BMS Phase II Elotuzumab 40 high-risk NK & efficacy
Jannsen Phase II
RCT
Siltuximab 100 high-
risk
1-yr PFS
Landgren Phase II Car-Len-
Dex
30 high-risk Response
rate
BioInvent Phase II BI-505 12 M-protein
change

SMM: who and when to treat?Conclusions
1. Treat only those SMM who are now reclassified as MM based on MDE
2. Only treat SMM patients on clinical trials*
* If osteopenia or osteoporosis, consider a bisphosphonate













![Research Article Prognostic Significance of Serum Free Light … · 2019. 7. 31. · the progression of MGUS [ ], solitary plasmacytoma [ ], and smoldering myeloma [ ]intomultiplemyeloma](https://img.pdfslide.us/doc/110x75/60b139df8dfefb1baa01f551/research-article-prognostic-significance-of-serum-free-light-2019-7-31-the.jpg)