Embed Size (px)
Citation preview

New treatment options and international researchJens Hillengass MD
Section Multiple MyelomDepartment of Hematology and Oncology
University of Heidelbergand
Department E010 RadiologyGerman Cancer Research Center

Jens Hillengass MD University of Heidelberg, S.D.G
Indication for treatment

Jens Hillengass MD University of Heidelberg, S.D.G
Stages of monoclonal plasma cell diseaseMonoclonal Gammopathy
of undetermined Significance
(MGUS)
smoldering myeloma
MultipleMyeloma
Monoclonal Gammopathy of undetermined Significance
(MGUS)
EarlyMyeloma
clonal plasma cells in bone marrow
<10% >10% >10%
monoclonal protein <30g/l >30g/l >30g/l
End organ damage NO NO YES

Smoldering Multiple Myeloma
Current definition according to IMWG: ≥ 10% Plasma Cells in Bone Marrow NO End Organ Damage (CRAB) or myeloma-defining event (MDE)
Rajkumar 2014 Lancet oncolJens Hillengass MD University of Heidelberg, S.D.G

IMWG Criteria (2003)
Jens Hillengass MD University of Heidelberg, S.D.G
symptomatic MM M-protein in serume and/ or urine; clonal plasma cells or plasmacytoma and ROTI* including bone lesions
MGUS M-Protein < 30 g/l; clonal plasma cells < 10%; no „ROTI“*
ROTI *ROTI = myeloma Related Organ or Tissue ImpairmentCalcium level > 2.75 mmol/lRenal insufficiency (Kreatinin > 173 mmol/l oder 2.0 mg/dl)Anemia (hemoglobin < 10 g/dl)Bone lesions (lytic lesions or osteoporosis with fracture (X-ray, CT or MRI)
smoldering MM M-Protein ≥ 30 g/l and/ or clonal plasma cell ≥ 10%; no „ROTI“*
Others: symptomatic hyperviscosity; amyloidosis; recurrent bacterial infections (> 2 episodes in 12 months
IMWG 2003 Br. J. Haematol.

Smoldering Multiple Myeloma
Jens Hillengass MD University of Heidelberg, S.D.G

Treatment of smoldering Multiple Myeloma
Dispenzieri 2013 BloodJens Hillengass MD University of Heidelberg, S.D.G

Smoldering Multiple MyelomaT h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;25 www.nejm.org june 21, 20072586
protein level of 0.1 g or less per 24 hours was found in 84%; only four patients (1.5%) had a level of more than 1.0 g per 24 hours.
The bone marrow aspirate and biopsy speci-mens were examined in all 276 patients (Fig. 1). In the plasma-cell category, the most common proportion was 15 to 19%. Of the 276 patients, 10% had less than 10% plasma cells in the mar-row, and 10% had 50% or more plasma cells. Cy-clin D1 was expressed by the plasma cells in 18% of the bone marrow specimens.
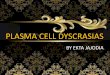
OutcomeDuring 2131 cumulative person-years of follow-up (range, 0 to 29; median, 6.1), 85% of the patients with smoldering multiple myeloma died (median follow-up of those still living, 11.6 years). During this period, active multiple myeloma developed in 158 patients (57%), who had a median survival af-ter the time of diagnosis of 3.4 years; amyloidosis developed in 5 (2%) (Table 1). The cumulative prob-ability of progression to active multiple myeloma or amyloidosis was 51% at 5 years, 66% at 10 years, and 73% at 15 years; the median time to progres-sion was 4.8 years (Fig. 2). The overall risk of pro-gression was 10% per year for the first 5 years, ap-proximately 3% per year for the next 5 years, and 1% per year for the last 10 years.
The number of patients with progression to ac-tive multiple myeloma was 522 times the number
of persons without smoldering multiple myeloma who would be expected to have active disease, and the risk of amyloidosis was increased by a factor of 50 (Table 1). Of 16 patients with Durie–Salmon stage II disease, 15 had progression to active mul-tiple myeloma; both patients with Durie–Salmon stage III had progression to active multiple my-eloma (median time to progression, 13.8 months and 15.1 months). Among patients with progres-sion of smoldering multiple myeloma, 97% had progression to active multiple myeloma. Rates of death owing to other diseases, including cardio-vascular and cerebrovascular disease and non–plasma-cell cancers, were 18% at 5 years, 26% at 10 years, 30% at 15 years, and 35% at 20 years. The overall rate of survival was 60% at 5 years, 34% at 10 years, and 20% at 15 years (median, 6.3). In the 128 patients who did not have progression to ac-tive disease after more than 10 years after diag-nosis, the disease was of the IgG subtype in 81%, the baseline median level of plasma cells in the bone marrow was 16%, the median spike in the serum monoclonal protein level was 2.8 g per deciliter, and uninvolved immunoglobulins were reduced in 78%.
Risk Factors for ProgressionWe evaluated baseline factors with respect to pro-gression of smoldering multiple myeloma to active disease or amyloidosis in 163 patients. These fac-tors included sex, hemoglobin level, a spike in the serum monoclonal protein level of 4 g per deciliter or more, the type of serum heavy chain, the serum albumin level, the presence and type of urinary light chain, a reduction in levels of uninvolved im-munoglobulins, the expression of cyclin D1, the proportion of plasma cells in the bone marrow, in-volvement of the interfatty marrow space, decreased proportion of normal hematopoietic elements (10% or more below the expected level for age), and as-signment to prognostic group 1, 2, or 3 (as defined in the Methods section). Significant baseline risk factors for progression of smoldering multiple myeloma to active disease or amyloidosis in the univariate analysis included the level of serum monoclonal protein (P<0.001), the presence of IgA monoclonal protein (P = 0.004), the presence of uri-nary light chain (P = 0.04), the extent of bone mar-row involvement (plasma cells, ≥20%; P<0.001), a reduction in levels of uninvolved immunoglob-ulins (P = 0.001), and the pattern of plasma-cell
100
80
60
40
20
00 5 10 15 20 25
Smoldering Multiple Myeloma
MGUS
AUTHOR:
FIGURE:
JOB:
4-CH/T
RETAKEICM
CASE
EMail LineH/TCombo
Revised
REG F
Enon
1st2nd3rd
Kyle
2 of 4
06-21-07
ARTIST: ts
35625 ISSUE:
22p3
51
6673
78
2116
104
Figure 2. Probability of Progression to Active Multiple Myeloma or Primary Amyloidosis in Patients with Smoldering Multiple Myeloma or Monoclonal Gammopathy of Undetermined Significance (MGUS).
I bars denote 95% confidence intervals.
The New England Journal of Medicine Downloaded from nejm.org on October 26, 2013. For personal use only. No other uses without permission.
Copyright © 2007 Massachusetts Medical Society. All rights reserved.
Kyle 2007 NEJMJens Hillengass MD University of Heidelberg, S.D.G

High Risk Smoldering Multiple Myeloma
Intended definition according to IMWG:=> progression of 80% within 2 years (IMW 2011 London) => 40% progression per year?!
Jens Hillengass MD University of Heidelberg, S.D.G Rajkumar 2014 Lancet oncol

New definition of multiple Myeloma
Kastritis 2014 Leukemia, Hillengass 2010 JCO
N = 65FL > 1high risk N = 9 (14%)
N = 149FL > 1high risk N = 23 (15%)
Jens Hillengass MD University of Heidelberg, S.D.G

Dispenzieri 2008 Blood, Larsen 2013 Leukemia
N = 273sFLC ratio abnormalhigh risk = n.d.
N = 586FLC ≧ 100high risk = 90 (15%)
New definition of multiple Myeloma
Jens Hillengass MD University of Heidelberg, S.D.G

Rajkumar 2011 NEJM, Waxman 2014 ASCO
N = 126BMPC ≧ 60%high risk N = 21 (17%)
N = 121BMPC ≧ 60high risk N = 6 (5%)
high risk
intermediate risk
low risk
New definition of multiple Myeloma
Jens Hillengass MD University of Heidelberg, S.D.G

New Definition of Multiple Myeloma
Rajkumar 2014 Lancet oncol
• Clonal bone marrow plasma cells ≥10% or biopsy proven plasmacytoma (not M-protein) and
ANY ONE OR MORE OF THE FOLLOWING MYELOMA DEFINING EVENTS (MDE)
• Evidence of end organ damage that can be attributed to the underlying plasma cell proliferative disorder, specifically
• Hypercalcemia: Serum calcium >0.25 mmol/L above upper limit of normal or > 2.75 mmol/L (> 1mg/dL above upper limit of normal)
• Renal insufficiency: Creatinine Clearance <40 ml/min or Serum creatinine > 173 µmol/L (>2mg/dL)
• Anemia: Normochromic, normocytic with a hemoglobin value of >2 g/dL below the lower limit of normal or a hemoglobin value <10 g/dL
• Bone lesions: Lytic lesions, or osteoporosis with compression fractures detected by X-ray, CT or PET-CT
• Any one or more of the following biomarkers of malignancy • Clonal bone marrow plasma cell percentage ≥ 60% (IHC, Flow, Immunofluorescence) • Involved/uninvolved serum free light chain ratio ≥100 and involved FLC ≥100 mg/L • >1 focal lesions on magnetic resonance imaging studies
SLIM-CRABJens Hillengass MD University of Heidelberg, S.D.G

Treatment of smoldering Multiple Myeloma
Jens Hillengass MD University of Heidelberg, S.D.G Mateos 2013 NEJM

History of myeloma treatment
Jens Hillengass MD University of Heidelberg, S.D.G
2015Panobinostat
2004Lenalidomide
2002Bortezomib
IxazomibElotuzumabDaratumumabSAR650984...
1970 1980 1990 2000 2010
1962Melphalan
1968Melphalan + Prednisone
1980sHigh dose melphalan + KMT
1984VAD
1990sSingleASCT
1984Supportivetherapy
2000sTandemASCT
1999Thalidomide
2014Carfilzomib
2014Pomalidomide

Jens Hillengass MD University of Heidelberg, S.D.G
How to treat in the future

Jens Hillengass MD University of Heidelberg, S.D.G
initialtreatment paths

Treatment paths
transplantation-eligible• up to 70 years (?)• normal organ function• stem cells collected• patient choice
not transplant-eligible• >70 years• comorbidities• no stem cells• patient choice
Jens Hillengass MD University of Heidelberg, S.D.G
Patients with Multiple Myeloma

Jens Hillengass MD University of Heidelberg, S.D.G
Treatment pathsTransplantation not possible Transplantation possible
age (65/ 70), performance status, comorbidities
Induction therapy Induction therapy(4-6 cycles)
maintenance therapy stem cell collection
stem cell transplantation
consolidation therapy
maintenance therapy

Jens Hillengass MD University of Heidelberg, S.D.G
What to do first?

Jens Hillengass MD University of Heidelberg, S.D.G
(Vincristin)
CyclophosphamidMelphalanBendamustin
Doxorubicin
Vinca-AlkaloidSpindelgift
Mikrotubulusdestabilisation
AntibioticumInterkalator: DNA-Strangbrüche
Topoisomerase-II-Inhibitor
AlkylansDNA-Strangbrüche
„Classical“ chemotherapy

Jens Hillengass MD University of Heidelberg, S.D.G
Benefit of novel agents
Kumar Blood 2008,Kumar Leukemia 2014

Jens Hillengass MD University of Heidelberg, S.D.G
Immunomodulatory drugsThalidomide/ Lenalidomide/ Pomalidomide

Jens Hillengass MD University of Heidelberg, S.D.G
Proteasome inhibitorsBortezomib/ Carfilzomib/ Ixazomib

Jens Hillengass MD University of Heidelberg, S.D.G
Improvement of induction therapyGMMG-MM5
3 x PAd (A1 + B1) 3 x VCD (A2 + B2)
CAD + stem cell collection
1-2 high dose melphalan + ASCT
2x Lenalidomide consolidation
Len for2 years
Len if no CR
Len for2 years
Len if no CR
A1 B1 A2 B2

Jens Hillengass MD University of Heidelberg, S.D.G
Improvement of induction therapyGMMG-MM5
Mai 2015 Leukemia
N = 504 newly diagnosed transplantat-eligible MM-patients
VCD PAd P-value⩾VGPR 37.0% 34.3% 0,001
PD 0.4% 4.8% 0,003
Leukopenia ⩾ 3° 35.2% 11.3% <0,001
Neuropathy 8.4% 14.9% 0,03
SAE total 24.0% 32.7% 0,04

Jens Hillengass MD University of Heidelberg, S.D.G
Induction therapy
Stewart Blood 2009; Jakubowiak Blood 2012
Stewart AK, et al. Blood. 2009;114:5436-5443. Jakubowiak AJ, et al. Blood. 2012;120:1801-1809.
100
90
80
70
60
50
40
30
20
10
0 TD VAD VTD RD CVD PAD CVRD RVD
CR/nCR R
espo
nse
(%)
Induction Regimen CRD
ORR VGPR

Jens Hillengass MD University of Heidelberg, S.D.G
Induction therapyKRD
Jakubowiak Blood 2012
All Pts (N = 66)
Phase II Pts (n = 35)
100 90 80 70 60 50 40 30 20 10 0
CR Near CR
VGPR PR
29
11
27
33
37
20
17
26

Jens Hillengass MD University of Heidelberg, S.D.G
Induction therapyKRD
Jakubowiak Blood 2012
Pat
ient
s (%
)
N = 53; Median 12 Cycles (Range 1-25)
Initial Response Best Response 100
75
50
25
0
M-P
rote
in L
evel
(% o
f Bas
elin
e)
100
75
50
25
0 0 12 11 10 9 8 7 6 5 4 3 2 1
Cycle
≥ nCR sCR M-protein
100
80
60
40
0
20
≥ PR ≥ nCR ≥ VGPR sCR
42
62
81
98

Jens Hillengass MD University of Heidelberg, S.D.G
Improvement of induction therapyGMMG-HD6
4 x VRD (A1 + A2) 4 x VRD + Elo (A2 + B2)
CAD + stem cell collection
1-2 high dose melphalan + ASCT
Len for2 years
Len+Elo for 2 years
Len for2 years
A1 A2 B1 B22xVRD 2xVRD
+Elo 2xVRD 2xVRD+Elo
Len+Elo for 2 years

Jens Hillengass MD University of Heidelberg, S.D.G
Do we still need transplantation?

Palumbo 2014 NEJM
Novel agent versus auto-SCT
Jens Hillengass MD University of Heidelberg, S.D.G

Conclusion
• auto-SCT leads to improved PFS and OS
• Lenalidomide maintenance improves PFS
Novel agent versus auto-SCT
Palumbo 2014 NEJMJens Hillengass MD University of Heidelberg, S.D.G

http://www.clinicaltrials.gov/ct2/show/NCT01208662?term=nct01208662&rank=1
Early versus late high dose chemotherapy
IFM/DFCI 2009 study Newly diagnosed MM patients (SCT candidates)
VRD x 3
VRD x 2
VRD x 5
Lenalidomide 12 mos
Melphalan 200mg/m2* +
ASCT
Induction
Consolidation
Maintenance
CY (3g/m2) MOBILIZATION Goal: 5 x106 cells/kg
VRD x 3
CY (3g/m2) MOBILIZATION Goal: 5 x106 cells/kg
Randomize, stratification ISS & FISH
Collection
Lenalidomide 12 mos SCT at relapse
MEL 200 mg/m2 if <65 yrs, ≥65 yrs 140mg/m2
Jens Hillengass MD University of Heidelberg, S.D.G

How can autologous transplant be improved?
• Induction with novel agents
• improvement of conditioning regimen
• consolidation and maintenance
Jens Hillengass MD University of Heidelberg, S.D.G

Harousseau 2007 ASH
0.00
0.25
0.50
0.75
1.00
0 6 12 18 24 30 36
Placebo Revlimid
IFM 2005-02 : PFS from randomization
Placebo
Revlimid
Consolidation and maintenance
Jens Hillengass MD University of Heidelberg, S.D.G

Neben 2011 Blood
Consolidation and maintenance
Jens Hillengass MD University of Heidelberg, S.D.G

Summary: Young patient (< 65/70 years)
• Autologous stem cell transplantation: standard of care
• Survival advantage is depending on achievement of a CR (VGPR)
• TBI (12Gy) or busulfan should not be used anymore
• Consider Double ASCT for patients, if no CR or nearCR after first SCT
PD Dr. Jens Hillengass Universitätsklinik Heidelberg, S.D.G

The elderly patient (≥ 65/70 years)
PD Dr. Jens Hillengass Universitätsklinik Heidelberg, S.D.G

Prospective study with 447 patients between 65 and 75 years=> Novel agent combination (MPT) better than MP and Mel100
Novel Agents versus ASCT
Facon 2007 LancetJens Hillengass MD University of Heidelberg, S.D.G

VISTA trial-update
San Miguel 2013 JCOJens Hillengass MD University of Heidelberg, S.D.G
VMP = Bortezomib (Velcade) + Melphalan + Prednison

FIRST trial
Benboubker 2014 NEJMJens Hillengass MD University of Heidelberg, S.D.G
Rd = Lenalidomid (Revlimid) + Dexamethason

Comparison FirstlineMM-‐015 VISTA VISTA FIRST IFM99-‐06
Palumbo 2012 NEJMPalumbo 2012 NEJMPalumbo 2012 NEJM San Miguel 2008 NEJM
San Miguel 2008 NEJM
San Miguel 2013 JCOSan Miguel 2013 JCO Benboubker 2014 NEJMBenboubker 2014 NEJMBenboubker 2014 NEJM Facon 2007 LancetFacon 2007 LancetFacon 2007 LancetSubstanzen MP MPR MPR-‐R MP VMP MP VMP Rd 18 Rd kont MPT MP MPT Mel100
Therapiedauer 9 9 kont 13 13 13 13 18 kont 18 18 18 5Follow-‐up 30 16,3 60 ,1 37 51,5
Medianes Alter 72 71 71 71 71 71 71 73 73 73Alter >/=65 >/=65 >/=65 >/=40 >/=65
Patienten 154 153 152 338 344 211 176 541 535 547 196 125 126PFS (median) 13 14 31 16,6 24 20,7 25,5 21,2 17,8 27,5 19,43-‐year OS (%) 66 62 70 68 68 66 70 625-‐year OS (%) 34,4 46OS (median) NR NR 45,2 NR NR 56,4 43,1 33,2 51,6 38,3
ORR 50 68 77 35 71 73 75 62 35 76 65Grad 4 Neutropenie 8 32 35 15 10 26 (3+4) 28 (3+4) 45 (3+4)Grad 4 febrile Neutropenie
0 1 2Grad 3 PNP 0 13Grad 4 PNP 0 1 1 (3+4) 1 (3+4) 9 (3+4) 0 6 (any) 0
Grad 3 Infektionen 7 13 9 4 Pneumoni
e
5 Pneumoni
e
9 (any) 13 (any) 49 (any)Grad 4 Infektionen 0 2 1 1
Pneumoni2
PneumoniJens Hillengass MD University of Heidelberg, S.D.G

Comparison FirstlineVISTA FIRST
San Miguel 2008 NEJM Benboubker 2014 NEJM
Substanzen VMP Rd kont
Therapiedauer 13 kont
PFS (median) 24 25,5
3-‐year OS (%) 68 70
OS (median) NR
ORR 71 75
Grad 4 Neutropenie 10 28 (3+4)
Grad 3 PNP 13
Grad 4 PNP 1 1 (3+4)
Grad 3 Infektionen 5 Pneumonie
Jens Hillengass MD University of Heidelberg, S.D.G

Outcome in terms of PFS and OS on ITT analysis (n=233)
Median follow-up: 30 m (9-43)
OS
Sequential : 73% at 3 yrs
Alternating: 71% at 3 yrs
PFS
Sequential: 32m
Alternating: 34 m
p=NS
45 40 35 30 25 20 15 10 5 0
1,0
0,8
0,6
0,4
0,2
0,0
45 40 35 30 25 20 15 10 5 0
1,0
0,8
0,6
0,4
0,2
0,0
p=NS
VISTA: 21m FIRST: 25m (cont Rd); 21m (Rd18)
VISTA: 68% at 3 yrs FIRST: 59% at 4yrs (cont Rd); 56% at 4yrs (Rd18)
Mateos et al. ASH 2014 (Abstract 178); oral presentation
Jens Hillengass MD University of Heidelberg, S.D.G

Comparison FirstlineVISTA FIRST Alternating
San Miguel 2008 NEJM Benboubker 2014 NEJM Mateos 2014 ASHMateos 2014 ASH
Substanzen VMP Rd kont Sequential Alternating
Therapiedauer 13 kont 18 18
PFS (median) 24 25,5 32 34
3-‐year OS (%) 68 70 73 71
OS (median) NR
ORR 71 75 77 80
Grad 4 Neutropenie 10 28 (3+4)
Grad 3 PNP 13
Grad 4 PNP 1 1 (3+4) 4 (3+4) 3 (3+4)
Grad 3 Infektionen 5 Pneumonie 6 (3+4) 6 (3+4)
Jens Hillengass MD University of Heidelberg, S.D.G

ASCT in elderly patients
Merz 2013 Ann OncolJens Hillengass MD University of Heidelberg, S.D.G

The elderly patient (≥ 65/70 Jahre)
Jens Hillengass MD University of Heidelberg, S.D.G
• Melphalan + prednisone + novel agent or lenalidomide + dexamethason for the majority of patients
- rarely MPT: improving PFS but not OS
- effectivity of VMP proven in VISTA trial1,2
- effectivity of Rd proven in FIRST trial3
• Bortezomib/ Thalidomid / Prednison (VTP) equivalent to VMP for elderly patients with myelosuppression4
- toxicity mainly cardio-tox (Thalidomid)1 San Miguel 2008 N Engl J Med
2 Mateos 2010 J Clin Oncol3 Benboubker 2014 NEJM
4 Mateos 2010 Lancet Oncol

What to do when the disease comes back?
PD Dr. Jens Hillengass Universitätsklinik Heidelberg, S.D.G

re-exposition
Jens Hillengass MD University of Heidelberg, S.D.G
NCCN
Re-exposition if relapse > 6 months after completion of initial therapy
IMWG
Re-exposition after „sustained“ remissionchange after „short“ remission
EMN
Re-exposition if relapse > 12 months after completion of initial therapyChange after „short“ remission
NCCN Clinical Practice Guidelines in Oncology Myeloma V. 2012,Palumbo 2009 Leukemia,
Ludwig 2012 The Oncologist,Rajkumar 2011 Blood

Jens Hillengass MD University of Heidelberg, S.D.Gadapted from Lonial 2011 CCR
Novel Agents at relapse

Jens Hillengass MD University of Heidelberg, S.D.Gadapted from Lonial 2011 CCR
Novel Agents at relapse

Sellner Cancer 2013
Retrospective analysis of 200 patients
=> Overall survival depending on remission after first auto-SCT
Auto-SCT at relapse
Jens Hillengass MD University of Heidelberg, S.D.G

ReLApsE-trial of the GMMG
Jens Hillengass MD University of Heidelberg, S.D.G

Summary
Jens Hillengass MD University of Heidelberg, S.D.G
-NCCN: Re-exposition after at least 6 months
-European opinion: after at least 12 months
-Re-exposition with Bortezomib: effective (but retrospective and no prospective trials)
-Re-exposition with IMiDs: effective (but mainly studies with Len after Thal)
NCCN Clinical Practice Guidelines in Oncology Myeloma V. 2012, Mothy 2012 Leukemia, Petrucci 2010 Haematologica, Hrusovsky
2010 Oncology

Jens Hillengass MD University of Heidelberg, S.D.G
future options

Targets for treatment
Jens Hillengass MD University of Heidelberg, S.D.G Ocio Leukemia 2014

Jens Hillengass MD University of Heidelberg, S.D.G
Proteasome inhibitorsBortezomib/ Carfilzomib/ Ixazomib
Kumar Lancet oncol 2014Stewart NEJM 2014
Ixazomib+Rd - Ixazomib maintenance Carfilzomib+Rd versus Rd

Jens Hillengass MD University of Heidelberg, S.D.G
AntibodiesElotuzumab/ Daratumumab/ SAR650984
Jagannath Myeloma.orgJagannath Myeloma.org

Jens Hillengass MD University of Heidelberg, S.D.G
AntibodiesElotuzumab/ Daratumumab
Lokhorst NEJM 2015Lonial NEJM 2015
Elotuzumab+RdDaratumumab dose escalation

Jens Hillengass MD University of Heidelberg, S.D.G
Histone deacetylase inhibitorsPanobinostat
San Miguel Lancet oncol 2015
Panobinostat + Vel/Dex

Jens Hillengass MD University of Heidelberg, S.D.G
Current research focus

Jens Hillengass MD University of Heidelberg, S.D.G
Assessment of minimal residual disease
ASO-PCR Flowcytometry Next-Generation Sequencing
Applicability 60-70% nearly 100% 90 %
Requirements for the sample
<1 Million cells Currently > 1 Million cells
< 1 Million cells
Processing of the sample
can be delayed within 48-72 hours can be delayed
Sensitivity ≧ 1 : 10-5 approx. 1 : 10-5 ≧ 1 : 10-6
adapted from Kumar

Jens Hillengass MD University of Heidelberg, S.D.G
Thank you very much for your attention