-
1
Laser Technologies
for Dermatology
& Cosmetic Surgery
SmartXide DOT
Clinical User Manual
Version 2.2 - September 2008
-
2
-
I
Index
1 Disclaimer
...............................................................................
1
2
Introduction.............................................................................
2
2.1.1 Traditional Skin Resurfacing
................................................ 2
2.1.2 Non-Ablative Photorejuvenation
........................................... 3
2.1.3 Fractional Photothermolysis
................................................ 4
3 SmartXide DOT Technical
Features................................................ 6
4 Hi-Scan DOT - Technical Features
................................................... 7
4.1.1 Scanning Areas
................................................................
8
4.1.2 Scanning Modes
...............................................................
9
4.1.3 Smart Pulse
Emission........................................................10
5 Clinical Procedure
....................................................................11
5.1 Pre Treatment
Care..............................................................11
5.1.1 Patient Examination & Contraindications
................................11
5.1.2 PIH prevention
...............................................................12
5.1.3 Infection
prevention.........................................................12
5.2 Anaesthesia
Indications..........................................................13
5.2.1 Anaesthesia Techniques
....................................................13
5.2.2 Fractional Skin Resurfacing
................................................16
5.2.3 Traditional Skin Resurfacing
...............................................16
5.3 Treatment Procedure
............................................................17
5.3.1 FRACTIONAL MODE : Indications & Clinical
Protocol..................17
I
-
II
5.3.2 Traditional Skin Resurfacing: Clinical
Protocol..........................23
5.3.3 TRADITIONAL MODE: Indications & Clinical Protocol
...................25
5.4 Post Treatment care
.............................................................28
6 Clinical Cases
..........................................................................29
6.1 Fine wrinkles, Textures and Spots
.............................................29
6.2
Wrinkles...........................................................................32
6.3 Acne Scars
........................................................................34
6.4
Keloid..............................................................................35
6.5 Epidermal Linear
Nevus.........................................................36
6.6 Epidermal Pigmented
Lesion...................................................36
6.7 Lentigo Simplex
..................................................................37
6.8 Beckers
Nevus....................................................................37
6.9
Melasma...........................................................................38
II
-
1 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
1 Disclaimer While the information contained in these pages has
been compiled from sources believed to
be current and reliable, DEKA cannot be held responsible for any
errors, omissions, defects
in, or the accuracy, completeness, timeliness or usefulness of,
the information supplied to
users on this document.
The following materials are presented for educational purposes
only. Methods described may
not be the only or best method in every case. DEKA specifically
disclaims any and all liability
for injury or other damages of any kind for any and all claims
that may arise out of the use of
any drug, device or technique described in these pages, whether
such claims are asserted by
a physician or any other persons.
Information on this document may contain technical inaccuracies
or typographical errors.
DEKA takes no responsibility for the consequences of error or
for any loss or damage suffered
by users of any of the information published on any of these
pages. Such information does not
form any basis of contract with readers or users of these
pages.
Furthermore, DEKA will not be liable to users of any for any
damages, claims, demands or
causes of action, direct or indirect, special, incidental,
consequential or punitive, as a result
of the use of this document or any information obtained from
it.
Information may be changed or updated without notice. DEKA may
also make improvements
and/or changes in this document at any time without notice.
All information contained within this document is the property
of DEKA. Copyright 2008.
-
2 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
2 Introduction The natural ageing process together with exposure
to the sun and pollution
leads to a gradual deterioration of the skins structure and
function. This is
mainly evident at the level of the epidermis and the upper
papillary dermis,
with a tissue laxity and skin that appears more lined, often
accompanied by
telangiectasias, wrinkles, and dark spots.
2.1.1 Traditional Skin Resurfacing
Resurfacing with pulsed CO2 laser has always been considered the
first choice of
treatment for rhytids and photo-damaged facial skin1-6. However,
due to the
lengthy recovery times and frequent complications7-8, not all
patients agree to
undergo this type of operation9-10.
Traditional Skin Resurfacing. Skin Healing Process.
-
3 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
Besides the usual recovery time required for oedema, burning,
scabs and
erythema which may often last for months11-12, there is also a
high incidence of
complications connected with hyper-and hypo-pigmentation, HSV
infection,
outbreaks of acne, milia formation, and dermatitis13-18.
Cases of HSV infection and outbreaks of acne, after traditional
resurfacing with pulsed CO2 laser.
2.1.2 Non-Ablative Photorejuvenation
Over recent years, the market has therefore been orientated
towards less
invasive and less problematic systems and methods. This has led
to a wide-scale
production of a myriad of non-ablative devices for reducing
wrinkles and
improving photo-damaged skin with the consequent passing over
from skin
resurfacing to skin rejuvenation. However, a critical review of
the literature
inherent to these methods has revealed that in terms of
efficacy, none of the
results obtained with these non-ablative methods can be compared
with the
resurfacing results achieved with the CO2 laser19-23. Moreover,
these types of
treatment are usually quite expensive for the patient, the
devices themselves
are also costly for the medical practitioners, and the results
obtained are not
always satisfactory.
-
4 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
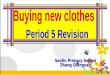
2.1.3 Fractional Photothermolysis
This situation has stimulated the search for new methods and
protocols that are
more efficient in combining quick recovery and minimal post-op
risks with
greater treatment efficacy. The advent of Fractional
Photothermolysis, initially
introduced with non-ablative methods, has given rise to the
development of a
new method that manages to effectively combine all the needs of
both medical
practitioners and patients, and namely, the Fractional Laser
Skin Resurfacing
with CO2 laser24-28
.
Fractional laser treatment allows to
obtain remarkable results with
minimal downtime.
The CO2 laser energy, applied in a
fractional way, creates very thin and
spaced columns of thermal damage
which penetrate deep into the
dermal skin layer and stimulate a
new collagen production. The tissue
between the columns of thermal
damage is spared, resulting in a faster healing process.
Various CO2 lasers with fractioned emission are currently
available on the market.
Despite the fact that all these systems are based on the same
principles, they present
significant differences with regard to output power, dwell-time,
distance between the
dots, varying scanner shapes and the laser beam profile. These
differences may
produce clinical results that differ greatly between one device
and another.
1. Manuskiatti W et al. Long-term effectiveness and side effects
of carbon dioxide laser resurfacing for photoaged facial skin. J Am
Acad Dermatol. 1999;40:401-11.
2. Fitzpatrick RE et al. Pulsed carbon dioxide laser resurfacing
of photo-aged facial skin. Arch Dermatol 1996;132:395402.3.Schwartz
RJ et al. Long term assesment of CO2 facial laser resurfacing:
Aesthetic results and complications. Plast Reconstr Surg. 1999;
103:592-601.
4. Lent WM, David LM. Laser resurfacing: a safe and predictable
method of skin resurfacing. J Cutan Laser Ther. 1999;1:87-94.
5. Fitzpatrick RE. Maximizing benefits and minimizing risk with
CO2 laser resurfacing. Dermatol Clin. 2002;20:7786.
6. Hruza GJ, Dover JS. Laser skin resurfacing. Arch Dermatol
1996;132:451455.
-
5 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
7. Bernstein L et al. The short and long term side effects of
carbon dioxide laser resurfacing. Dermatol Surg
1997;23:519525.8.Alster T, Hirsch R. Single-pass CO2 laser skin
resurfacing of light and dark skin: Extended experience with 52
patients.J Cosmet Laser Ther 2003;5:3942.
9. Trelles MA, et al. The origin and role of erythema after
carbon dioxide laser resurfacing: a clinical and histologic study.
Dermatol Surg. 1998;24:25-30.
10. Burkhardt BR, Maw R. Are more passes better? safety versus
efficacy with the pulsed CO2 laser. Plast Reconstr Surg.
1997;99:1531-1534.
11. Sullivan SA, Dailey RA. Complications of laser resurfacing
and their management. Ophthal Plast Reconstr
Surg.2000;16:41726.
12. Berwald C et al.. Complications of the resurfacing laser:
Retrospective study of 749 patients. Ann Chir Plast Esthet.
2004;49:3605.
13. Alster TS. Cutaneous resurfacing with CO2 and erbium: YAG
lasers: preoperative, intraoperative, and postoperative
considerations. Plast Reconstr Surg. Feb 1999;103(2):619-32.
14. Alster TS. Side effects and complications of laser surgery.
In Alster TS: Manual of Cutaneous Laser Techniques, ed 2.
Philadelphia, Lippinco. 2000;pp 175-187.
15. Alster TS, Lupton JR. Treatment of complications of laser
skin resurfacing. Arch Facial Plast Surg. Oct-Dec
2000;2(4):279-84.
16. Sriprachya-Anunt S et al. Infections complicating pulsed
carbon dioxide laser resurfacing for photoaged facial skin.
Dermatol Surg. 1997;23:527-36.
17. Nanni CA, Alster TS. Complications of carbon dioxide laser
resurfacing. An evaluation of 500 patients. Dermatol Surg
1998;24:315320.
18. Sadick NS. Update on non-ablative light therapy for
rejuvenation: A review. Lasers Surg Med. 2003;32:1208.
19. Nanni CA, Alster TS. Complications of carbon dioxide laser
resurfacing. An evaluation of 500 patients. Dermatol Surg
1998;24:315320.
20. Sadick NS. Update on non-ablative light therapy for
rejuvenation: A review. Lasers Surg Med. 2003;32:1208.
21. Williams EF III, Dahiya R. Review of nonablative laser
resurfacing modalities. Facial Plast Surg Clin North Am.
2004;12:30510.
22. Grema H et al. Facial rhytides subsurfacing or resurfacing?
A review. Lasers Surg Med. 2003;32:40512.
23. Bjerring P. Photorejuvenation an overview. Med LaserAppl.
2004;19:18695.
24. Le Pillouer-Prost A, Zerbinati N. Fractional laser skin
resurfacing with SmartXide DOT. Initial Results. J Cosmc and Laser
Ther, 2008;10(2):in press.
25. Matteo Tretti Clementoni et al. Non sequential fractional
ultrapulsed C02 resurfacing of photoaged skin. J Cosmc and Laser
Ther, 2007;9(4):21822.
26. Hantash BM et al. Ex vivo histological characterization of a
novel ablative fractional resurfacing device. Laser Surg Med.
2007;39:87-95.
27. Hantash BM et al. In vivo histological evaluation of a novel
ablative fractional device. Laser Surg Med. 2007;39:96-107.
-
6 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
3 SmartXide DOT Technical Features
Type of Laser CO2
Wavelength 10.6 m
Power to Tissue 30 W (max)
Repetition Rate from 5 to 100 Hz
Pulse Length from 0.2 to 80 ms
Delivery System Articulated Arm with 7 Mirrors
Aiming Beam Diode Laser, 3 mW@ 635-670 nm
Scanning Mode Traditional & DOT-Fractional
User Interface LCD Colour Touch Screen
Aiming Beam Diode laser 635 nm
Power Supply 230 Vac / 1.8 A (max) / 50-60 Hz
Dimensions 48 cm (W) x 55 cm (D) x 120 cm (H)
Weight 30 Kg
-
7 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
4 Hi-Scan DOT - Technical Features
Scanning Area Max: 15 x 15 mm Min: 1 x 4 mm
Spot Size
Stimulative Effect
Ablative Effect
350 m 120 m
Scanning Mode Traditional & DOT-Fractional
Pulse Emission
Dwell Time from 0.2 to 2 ms (DOT) from 0.2 to 20 ms (Std.)
DOT Pitch from 200 to 2000 m
-
8 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
4.1.1 Scanning Areas
-
9 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
4.1.2 Scanning Modes
Normal
Interlaced
-
10 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
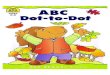
4.1.3 Smart Pulse Emission
The first part of the pulse has high peak power for few tens of
microseconds
that allows for rapid ablation of the epidermis and the first
layers of the derma,
while the second part of the pulse has low peak power allowing
for targeted
heating of the deeper areas of the skin.
Smart Pulse Emission
AAbbllaattiioonn
PPoowweerr
PPuullssee DDuurraattiioonn
-
11 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
5 Clinical Procedure
5.1 Pre Treatment Care
5.1.1 Patient Examination & Contraindications
First of all it is important to proceed with the visit and the
anamnesis of the
patient.
A persons history should be compiled by establishing the
following:
Sun and UV lamp exposure: avoid them before (at least 1 month),
during and after treatment. Apply SPF50 sunblock before and after
the treatment.
Make sure that the patient is not taking incompatible drugs as:
o Anticoagulants (as acetylsalicylic acid, heparin, etc),
o Retinoids these drugs can cause problems in the healing
process with possible scar results - (as isotretinoin, etc),
o Photo-sensitizers (as tetracycline [antibiotic], naproxen
[NSAD], auranofin [antirheumatic], estrogens and progestins
[oral
contraceptive], cloroquine [antimalarial], etc.)
Suspend the administration according to the specific drug so
that its effect is
expired before the treatment.
Recent exfoliation treatment (peels, scrubs, retin-A) and
surgical treatment (as lifting, etc.).
Past skin disorders. History of herpes virus infection. In order
to ensure a positive outcome with laser treatment, the patient
must
strictly follow a pre-operative protocol to help prevent the two
main possible
complications: Post-inflammatory Hyperpigmentation (PIH) and
infection.
-
12 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
5.1.2 PIH prevention
Especially with darker phototypes (III, IV, V and VI) and Asian
phototypes, it is
recommended to apply a topical cream every day for four weeks
before the
treatment for inhibiting melanin production.
It is possible to use cream containing hydroquinone or, as
alternative lighteners,
arbutin, azelaic acid, kojic acid or stabilized vitamin C.
This procedure is highly recommended with darker and Asian skin
types, while
for photo type I and II it is just a suggestion.
5.1.3 Infection prevention
The drugs used fall into two main categories:
antiviral drugs (aciclovir, valaciclovir, etc) It is suggested
to start the antiviral prophylaxis 6 days before the treatment
in subjects with a positive anamnesis of herpes virus infections
history.
The antiviral treatment can start 2 days before the treatment in
subjects
without previous experience of herpes infections.
It is recommended to continue the antiviral drugs at routine
doses for 5-15
days after the intervention.
antibiotic drugs (macrolides, cephalosporins, etc) The doctor
may consider prescribing antibiotic drugs as well, starting 6 or
1
days before the treatment (according to the patient anamnesis)
and
continuing for 7-8 days after the procedure.
Remark: It is not necessary to prescribe antibiotic drugs in all
cases. It is
often enough the application of a topical antibiotic cream or
ointment (like
gentamicin) after the procedure.
-
13 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
5.2 Anaesthesia Indications
Dermal treatments with laser may give rise to a painful
sensation described as
similar to an elastic band being pinged against the skin, or the
pain caused by
burns.
The anaesthetic protection for CO2 laser skin therapies becomes
necessary in specific cases,
such as:
Traditional CO2 laser skin resurfacing; The treatment of
extensive skin areas; The treatment of deep lesions;
Patients with a low pain threshold; Non-compliant patients;
Paediatric patients.
5.2.1 Anaesthesia Techniques
Irrespective of the anaesthetic method used, several
indispensable precautions are necessary:
A careful clinical assessment (if an anaesthetist is necessary
this will be their exclusive responsibility), with particular
attention to cardiovascular, pulmonary, and neurological
pathologies, hypertension, diabetes, allergic phenomena and/or
any idiosyncratic
reactions to the medicinal products to be administered;
Instrumental assessment (ECG, chest X-ray, etc.) wherever
indicated; Detailed indications regarding the administration,
modification or discontinuation of
therapies in progress (in the current condition and in relation
to the type of
intervention/treatment, the assessment will mainly concern the
anticoagulant therapy);
Pre-op fasting (6 hours for solids, 2 hours for liquids);
Informed consent; Outpatient safety devices;
-
14 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
Preventive insertion of peripheral venous cannula.
The following anaesthesia techniques may be used:
Transdermal anaesthesia;
Infiltrative anaesthesia; Peripheral blocks;
Locoregional blocks; Local anaesthesia techniques associated
with sedative analgesia; General anaesthesia.
Transdermal Anaesthesia (Topical Anaesthesia) A number of local
anaesthetics are available for topical use in various types of
preparation
that usually all provide efficacious analgesia albeit of brief
duration. Among the various
preparations, a product which is marketed worldwide, namely EMLA
(containing lidocaine
2.5% + prilocaine 2.5%), has to be applied 1 hour before the
treatment.
Infiltrative Anaesthesia
While the use of this type of anaesthetic does not necessarily
require the presence of the
anaesthetist, monitoring of the vital parameters is obligatory,
as well as the presence of all
the aids for coping with possible emergency situations. Any type
of local anaesthetic may be
used for the infiltration. The onset of the action is extremely
rapid with nearly all agents,
irrespective of whether used intradermically or subcutaneously.
Epinephrine considerably
prolongs the duration of the block via infiltration.
Both intradermal and subcutaneous infiltration may be painful,
above all due to the acid pH
that characterises all local anaesthetics. The problem can be
attenuated with suitable
administration techniques and the addition of NaHCO3 in a 10-15%
ratio.
The intradermal and subcutaneous infiltration techniques foresee
the use of fine needles (30
G) for the initial pomphus, after which larger gauge needles can
be used (25-23 G) for
achieving an optimal anaesthesia in the area to be treated, and
by always taking care to
inject the preselected solution very slowly.
-
15 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
Peripheral nerve blocks
Whereas with transdermal and infiltrative anaesthesia techniques
the presence of the
anaesthetist is not considered indispensable - except in the
case of elderly patients (when
sedative methods are required) or those with psycho-pathological
problems their presence
will be necessary for performing peripheral nerve blocks. In the
majority of cases it will be
the anaesthetist who personally performs the block, and they
must always be present for
correct intra and perioperative assistance.
The blocks used in the cervico-facial district consist of:
TRIGEMINAL Central blocks:
- ophthalmic bundle-branch
- maxillary bundle-branch
- mandibular bundle-branch
Peripheral blocks:
- supraorbital nerve
- infraorbital nerve
- mental nerve
The local anaesthetics used for peripheral nerve blocks are the
same as those used for the
infiltrative techniques.
Anaesthesia techniques associated with sedative analgesia
The aim is to reach a level of sedation in which the patient is
calm and relaxed while still
continuing to be responsive to the team carrying out the
procedure. Sedative analgesic
techniques are normally used in association with locoregional
methods. Ample multicentre
studies have demonstrated that while the sedative techniques are
very safe if performed by
expert anaesthetists, they could be hazardous in inexperienced
hands, especially if performed
without adequate monitoring systems.
The drugs used for these methods are:
CERVICAL PLEXUS
Superficial C.P.
Deep C.P.
-
16 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
SEDATIVES:
Benzodiazepine
Ketamine
Major sedatives
Hypnotics
General anaesthesia
The indications for general anaesthesia are restricted to
paediatric and non-compliant
patients. The presence of the anaesthetist is indispensable, and
the anaesthetic may be
performed in authorised structures including outpatients.
5.2.2 Fractional Skin Resurfacing
In case of fractional resurfacing with SmartXide DOT it is
usually enough to
apply a topical anaesthetic 1 hour before the treatment.
In case of quite superficial action, to use the SmartCryo skin
cooling system
during the treatment can be a possible alternative to the
topical anaesthetic.
5.2.3 Traditional Skin Resurfacing
Patient discomfort can vary widely in case of traditional laser
skin resurfacing.
Many patients find the topical application applied one or two
hours prior to the
treatment and combined with regional nerve blocks provides
appropriate
analgesia.
Other patients prefer to undergo intravenous sedation because
they find laser
resurfacing to be uncomfortable.
ANALGESICS:
Ketorolac
Tramadol
Opiates
Anaesthetics
-
17 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
5.3 Treatment Procedure
The face is divided into five aesthetic
units: right malar, perioral, left malar,
forehead and periorbital-nasal areas. In
case of laser skin resurfacing (both
fractional and traditional) full face
treatment is performed on each aesthetic
unit sequentially, with care being taken
to avoid overlapping.
5.3.1 FRACTIONAL MODE : Indications & Clinical Protocol
Topical anaesthetic has to be removed just before the
treatment.
Set the SmartXide DOT system in DOT mode according to patient
phototype, the
area to be treated and the application.
Usually we recommend performing a full-face and single passage
treatment to
obtain a better colour and texture uniformity.
SmartXide DOT offers the possibility to adapt the procedure
according to the
expectation of the patient: more or less aggressive treatment
corresponds to
longer or shorter down time after every session.
-
18 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
The quantity of fluence (density of energy measured in J/cm2)
delivered with
the scanner is correlated with the effect provoked on the skin.
The following
formula allows to calculate the fluence level delivered in DOT
mode:
As a simple result of the formula above, reducing the Power
and/or the Dwell
Time and/or increasing the Spacing, it is possible to reduce the
fluence and to
control the thermal effect on the skin.
5.3.1.1 Skin Resurfacing
Phototype Power (W) Dwell Time (s)
Spacing (m)
Nr. of Sessions
Nr. of Passages
I 30 2000 750 2 1
II 30 2000 1000 3 1
III 30 2000 1200 3 1
IV 25 2000 1200 3 1
V-VI 25 1500 1200 3 1
Fluence (J/cm2) =
Power (W) * Dwell Time (ms) * 105
[ Spacing (m) + 350 ]2
-
19 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
5.3.1.2 Chronoaging
Phototype Power (W) Dwell Time (s)
Spacing (m)
Nr. of Sessions
Nr. of Passages
I 30 1000 750 4 1
II 30 1000 1000 6 1
III 30 1000 1200 6 1
IV 25 1000 1200 6 1
V-VI 25 750 1200 6 1
Fair Asian Skin type
30 300 300 3 1
Dark Asian Skin Type
25 300 350 3 1
5.3.1.3 Acne Scars & Hypertrophic Scars
Phototype Power (W) Dwell Time (s)
Spacing (m)
Nr. of Sessions
Nr. of Passages
I 30 2000 1000 2-3 2
II 30 1500 1000 3 2
III 30 1000 1000 3-4 2
IV-VI 30 750 1000 3-4 2
Fair Asian Skin type
30 800 800 3 2
Dark Asian Skin Type
25 800 800 3 2
-
20 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
5.3.1.4 Keloid
Phototype Power (W) Dwell Time (s)
Spacing (m)
Nr. of Sessions
Nr. of Passages
I 30 2000 800 2-3 1
II 30 1500 800 3 1
III 30 1000 800 3-4 1
IV-VI 25 1000 800 3-4 1
Fair Asian Skin type
30 800 700 3 1
Dark Asian Skin Type
25 800 700 3 1
5.3.1.5 Superficial Pigmented lesions
Phototype Power (W) Dwell Time (s)
Spacing (m)
Nr. of Sessions
Nr. of Passages
I 30 500 500 1-2 1
II 30 400 500 1-2 1
III 30 300 500 1-2 1
IV 25 300 600 1-2 1
V 20 300 800 1-2 1
Fair Asian Skin type
25 300 650 1-2 1
Dark Asian Skin Type
20 250 650 1-2 1
-
21 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
5.3.1.6 Melasma
Phototype Power (W) Dwell Time (s)
Spacing (m)
Nr. of Sessions
Nr. of Passages
I 20 500 500 4 1
II 20 400 500 4 1
III 20 300 500 5 1
IV 15 400 500 5 1
Fair Asian Skin type
20 400 500 4 1
Dark Asian Skin Type
20 300 500 4 1
5.3.1.7 Special Care: Periocular Area
This area is very delicate. A common side effect is to have
swelling and oedema. It is recommended
to decrease the fluence 30% less.
Dwell Time
-
22 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
5.3.1.8 Special Care: Perinasal & Perimandibular Areas
In the perinasal area (where there are many sebaceous glands)
and in the submandibular area
(where there are few sebaceous glands) the risk
of post treatment scars is higher. It is
recommended to decrease the fluence 20% less.
Dwell Time
5.3.1.9 Special Care: Neck Area & Dcolletage
In the neck area and in the dcolletage the skin is thinner. It
is recommended to decrease the
fluence 30% less.
Power Dwell Time
-
23 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
5.3.2 Traditional Skin Resurfacing: Clinical Protocol
Each aesthetic unit has to be treated in its entirety avoiding
overlap.
Set the Hi-Scan unit in DOT OFF mode. Choose the appropriate
shape and size
of the scanning area. Set Power and Dwell Time according to the
area to be
treated. Please remember that with darker (III, IV, V and VI)
and Asian
phototypes, fractional skin resurfacing is strongly
recommended.
Moist saline-soaked gauzes are used to remove debris during the
procedure.
This should be done gently to minimize additional tissue trauma.
Debris removal
is necessary to avoid a heat-sink phenomenon, which results in
more thermal
irritation of tissues.
Most areas are treated with a second pass. Approximately 30% of
the time, a
third pass is employed, a fourth is used in less than 5% of
patients.
The endpoint of treatment is gauged to be ablation of wrinkles
or visual
estimation to have reached the basal layer.
Skilled surgeons could use more power and more dwell times than
recommended
in the protocol, avoiding multiple passes. In this case, please
remember that
skin removal is not proportional to the power increase whereas
thermal damage
is.
The neck
As in phenol-based exfoliation, the neck is not treated. The
pilosebaceous
density in the neck is such that deep vaporization can lead to
scarring.
However, the perimeter can be treated with a single pass at the
mandibular
margin to avoid a frank line of demarcation between
laser-resurfaced and non-
resurfaced skin.
-
24 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
Malar areas
For these areas the suggested setting is: Power= 17 W and Dwell
Time= 400 s. Normally a second laser pass is used to treat the
malar area, this should be done
transversely with respect to the previous one.
Perioral Area
In the perioral area, laser resurfacing is carried on to the
vermilion border.
Great care is taken to avoid allowing the laser beam to strike
teeth. Some
surgeons prefer to use a protective mouth-piece. Be careful
because it could
distort the perioral tissue. Initial parameters should be:
Power=13 W and Dwell
Time= 400 s. Forehead
When treating the forehead area, the hair is moistened and metal
shields or
moist towels are used to protect the eyes. Care is taken to
avoid lasering the
hairline or eyebrows. Initial parameters are: Power= 15 W and
Dwell time= 400
s. Periorbital area
Because the eyelid tissue is so delicate, reduced fluence is
used: Power=10 W
and Dwell Time= 400 s. The eye to be treated is anaesthetized
with two drops of tetracaine. A glass or metal eye shield is
inserted under the lid to protect the
globe. It is better to use a spherical protector to be sure that
the surface is
smooth and free of any irregularities. Resurfacing is carried no
closer than 3 to 4
mm from the ciliary margin to minimize oedema and possible
thermal irritation
to the meibomian glands in the eyelid area. Multiple passes may
be used to
treat deep wrinkles in the lateral canthal area. For the upper
eyelid, treatment
is carried down to the superior tarsal fold.
-
25 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
5.3.3 TRADITIONAL MODE: Indications & Clinical Protocol
Set the SmartXide DOT system according to the patient phototype,
the area to
be treated and the application.
TREATMENT EMISSION
MODE
LEVEL* FREQUENCY
(Hz)
REMARKS
Acne Scar PW 0.5-3 10-20 DOT treatment suggested. Topical
anaesthesia.
Actinic Cheilitis PW 0.5-5 10-20 Topical anaesthesia.
Actinic Keratosis (superficial)
PW 1.5 10 Topical anaesthesia. Spiral movements starting from
the edges to the centre.
Actinic Keratosis (tick)
PW 5 50
Angiokeratoma PW 1.5-5 10-20 Topical anaesthesia.
Balanitis Xerotic Obliterans
PW 2.5 20 Topical or infiltrative anaesthesia according to the
lesion size.
Basal Cell Carcinoma
PW 0.5-8 10-50 Indications: Nodular carcinoma with
-
26 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
TREATMENT EMISSION
MODE
LEVEL* FREQUENCY
(Hz)
REMARKS
Haemangioma PW 4-10 80 Not elective treatment. High risk of scar
results. It is better to use a vascular laser as Dye laser.
Hidrocystoma Apocrine
PW 0.5-2 10
Hypertrophic Scar PW 0.5-3 10-20 DOT treatment suggested.
Topical anaesthesia.
Keloid PW 0.5-3 10-20 DOT treatment suggested. Topical
anaesthesia.
PW 0.5-3 10-20 Topical anaesthesia. Keratosis (Seborrheic
Keratosis) PW 0.5-2 10
Lentigo Maligna PW 0.5-3 10-20 Perform the incisional
biopsy.Infiltrative anaesthesia.
Leukoplakia PW 0.5-5 10-50 Perform the incisional biopsy.
Lymphangioma PW 0.5-3 10-20 Only circumscribed lesion.
Molluscum Fibroma PW 0.5-3 10-20 Topical anaesthesia.
Neurofibroma PW 0.5-2.5 10-20 Infiltrative anaesthesia (in case
of big size).
Nevus Sebaceus PW 1.5-10 10-20 Infiltrative anaesthesia.
Pagets Disease PW 0.5-3 10-50 Infiltrative anaesthesia. Perform
the incisional biopsy.
Queyrats Disease** PW 2 20 Infiltrative anaesthesia. Perform the
incisional biopsy.
Rhinophyma 1 PW 2.5-10 50-100 Rough-shape phase. Infiltrative
anaesthesia.
Rhinophyma 2 PW 2.5-5 20 Finishing phase. Infiltrative
anaesthesia.
Sebaceous Adenoma*
PW 1.5-2.5 10-20 Topical anaesthesia.
Spider Nevus PW 3-8 80 Not elective treatment. High risk of scar
results. It is better to use a vascular laser as Nd:YAG.
Spinocellular Carcinoma
PW 2.5-8 20-50 Only selected cases. Perform the incisional
biopsy. Infiltrative anaesthesia.
-
27 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
TREATMENT EMISSION
MODE
LEVEL* FREQUENCY
(Hz)
REMARKS
Superficial Pigmented Lesions**
PW 1.5 10 DOT treatment suggested.
Syringoma PW 0.5-2.5 10-20 Infiltrative anaesthesia.
Trichoepitelioma PW 0.5-5 10-50 Infiltrative anaesthesia.
Tuberous Angioma PW 4-7 50-80 Better if used in combination with
Nd:YAG or Dye laser. Infiltrative anaesthesia.
Verruca 1 (Verruca Vulgaris)
PW 4-15 10-100 Topical anaesthesia.
Verruca 2
(Verruca Plana)
PW 0.5-2 10-20 Infiltrative anaesthesia.
Verruca Pedis** CW 8-10 Watt
Infiltrative anaesthesia.
Xanthelasma PW 0.5-3 10-20 Infiltrative anaesthesia.
Zoon Balanitis** PW 1-2 10-20 Topical or infiltrative
anaesthesia according to the lesion size.
*: In the LEVEL column the suggested ranges for the level
setting are shown.
Consider that usually, the procedure starts setting higher level
value (which
corresponds to a deeper skin ablation effect) for the
rough-shape phase. At
the end of the procedure the level value is reduced to perform
more precise
final touches.
**: Treatment not included in the Treatment Menu of SmartXide
DOT system.
-
28 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
5.4 Post Treatment care
Operations carried out with CO2 laser devices generate abrasion
or ablation of
the skin which makes daily care of the wound essential.
The aim is to achieve healing, preventing the formation of scabs
in the middle
and on the inner edges of the area treated, and thus
guaranteeing an adequate
cleanliness and softness (above all with regard to the skin
site).
In order to reduce the oedema and the inflammation that may
occur after the procedure, we recommend applying on the skin, just
after the treatment,
cool compression or wet gauzes cooled using the SmartCryo air
jet.
As post-treatment care, we suggest open-type medication with
accurate gentle skin cleansing, cold packs compression which must
always be carried
out with sterile gauze and physiological solution. We recommend
that the
patient re-applies every time emollient and/or antibiotic and
enzymatic
ointments, especially after cleaning and showers. This procedure
has to be
performed 3-4 times per day until the clinical healing is
observed (4-7 days).
After this time, apply a normal skin-care moisturizer and a
sunblock
protection (for 2-5 months according to the skin phototype and
the
environmental conditions).
It is suggested to wait for 1 day before having a shower (avoid
hot water on the treated area until healing is complete).
Avoid topical exfoliation for at least 4 weeks. The use of
active Vitamin C-based creams, useful for maintaining the
uniformity and compactness of the new tissue and reducing any
possible
deterioration, may be continued for unlimited time.
-
29 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
6 Clinical Cases
6.1 Fine wrinkles, Textures and Spots
Before and after 4 sessions. Courtesy of Dr Anne Le
Pillouer-Prost Marseille France.
Before and after 3 sessions. Courtesy of Dr Anne Le
Pillouer-Prost Marseille France.
-
30 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
Before and after 3 sessions. Courtesy of Dr Anne Le
Pillouer-Prost Marseille France.
Before and after 2 sessions. Courtesy of Dr Nicola Zerbinati
Pavia Italy.
-
31 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
Before and 21 days after 1 session. Courtesy of Dr C. William
Hanke Indianapolis, IN USA.
Before and 17 days after 1 session. Courtesy of Dr C. William
Hanke Indianapolis, IN USA.
-
32 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
6.2 Wrinkles
Before and after 2 sessions. Courtesy of Dr Anne Le
Pillouer-Prost Marseille France.
Before and after 2 sessions. Courtesy of Dr Anne Le
Pillouer-Prost Marseille France.
-
33 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
Before and after 1 session. Courtesy of Dr Patrick Treacy Dublin
- Ireland.
Before and 6 days after 1 session. Courtesy of Dr Hee-Jin Han
Seoul - Korea.
Before and 14 days after 1 session. Courtesy of Dr C. William
Hanke Indianapolis, IN - USA.
-
34 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
6.3 Acne Scars
Before and after 1 session. Courtesy of Dr Nicola Zerbinati
Pavia Italy.
Before and after 2 sessions. Courtesy of Dr Jahanara Ferdous
Khan - Dhaka Bangladesh.
-
35 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
Before and after 1 session. Courtesy of Dr Hee-Jin Han Seoul -
Korea.
6.4 Keloid
Before and after 2 sessions. Courtesy of Dr Nicola Zerbinati
Pavia Italy.
-
36 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
6.5 Epidermal Linear Nevus
Before and after 1 session. Courtesy of Dr Nicola Zerbinati
Pavia Italy.
6.6 Epidermal Pigmented Lesion
Before and after 1 session. Courtesy of Dr Nicola Zerbinati
Pavia Italy.
-
37 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
6.7 Lentigo Simplex
Before and after 2 sessions. Courtesy of Dr Jahanara Ferdous
Khan - Dhaka Bangladesh.
6.8 Beckers Nevus
Before and after 2 sessions. Courtesy of Dr Jahanara Ferdous
Khan - Dhaka Bangladesh.
-
38 SmartXide DOT Clinical User Manual- Version 2.2 - September
2008
6.9 Melasma
Before and after 2 sessions. Courtesy of Dr Jahanara Ferdous
Khan - Dhaka Bangladesh.
Before and after 5 sessions. Courtesy of Dr Nicola Zerbinati
Pavia Italy.
-
1
-
2
Deka M.E.L.A. srl, 2008
All rights reserved. All other brands and product names are
trademarks or registered
trademarks of their respective holders.
DEKA M.E.L.A. s.r.l.
Via Baldanzese, 17 50041 Calenzano (FI) Italy
Tel +39 055 8874942 - Fax +39 055 8832884
e-mail: [email protected]
web: www.dekalaser.com