Embed Size (px)
Citation preview

Monday, 24 November 2008
Small Tools for Big Problems: Microchips for Small Tools for Big Problems: Microchips for Global Health AIDS Diagnostics
Xuanhong Chengua o g C e gMaterials Science and Engineering
Bioengineering

Overview of Presentation
1 Global Health Challenges
2 HIV/AIDS Statistics and Biology
3 HIV/AIDS Diagnostics
4 Mi hi T h l f HIV/AIDS Di i 4 Microchip Technology for HIV/AIDS Diagnostics

Leading causes of death, Global
1 Ischemic heart disease 12.7
2 Cerebrovascular disease 9 9
Rank % of total
2 Cerebrovascular disease 9.9
3 Acute lower respiratory infections 7.1
4 HIV/AIDS 4.8
5 Chronic obstructive pulmonary disease 4.8
6 Perinatal conditions 4.2
7 Diarrheal diseases 4 07 Diarrheal diseases 4.0
8 Tuberculosis 3.0
11 Malaria 1.9
Source: WHO , The World Health Report 2000

Leading causes of death, Africa
1 HIV/AIDS 20.6
2 Acute lower respiratory infections 10.3
Rank % of total
2 Acute lower respiratory infections 10.3
3 Malaria 9.1
4 Diarrheal diseases 7.3
5 Perinatal conditions 5.9
6 Measles 4.9
7 Tuberculosis 3 47 Tuberculosis 3.4
8 Cerebrovascular disease 3.2
9 Ischemic heart disease 3.0
10 Maternal conditions 2.4
Source: WHO , The World Health Report 2000




Cell Bacteria(TB, Typhoid)
Virus(HIV, hepatitis, SARS, influenza)
.
HIV emerging from a cellHIV emerging from a cell
Cell
HIV

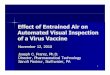
Global diversity of different HIV-1 strains
Source: Los Alamos Database http://hiv-web.lanl.gov/

39 million adults living with HIV/AIDS, 2006
Source: WHO

Growth of the AIDS Epidemic
40
45
People With HIV/AIDS, Cumulative Regional TotalsMillions
25
30
35
40
15
20
25
0
5
10
1986 1988 1990 1992 1994 1995 1998 2000 2002 20041986 1988 1990 1992 1994 1995 1998 2000 2002 2004
Sub-Saharan Africa Asia Latin AmericaEurope & N. America* Eastern Europe & Central Asia North Africa & Middle EastCaribbean
*Western and Central Europe & North America.Source: UNAIDS/WHO, 2004.

People With HIV/AIDS, by Region
Eastern Europe and Central Asia
Western and Central Europe
Latin America4%
Caribbean1%
4%
Oceania
North America3%
p2%
S th d S th
Oceania<1%
East Asia3%
Sub-Saharan Africa64%N h Af i d
South and South-East Asia
18%
64%North Africa and Middle East
1%
Source: UNAIDS, AIDS Epidemic Update 2004.

Changes in Life Expectancy, 1950 - 2000
65
55
60
Botswana
Uganda
45
50South Africa
Uga da
Zambia
40
45Zimbabwe
351950 1960 1970 1980 1990 2000
Source: United Nations Population Division, 1998

AIDS’ Toll on Population Structure, Botswana
Population Structure in 2020 (Projected)Thousands
Age80+
Males Females
80+75706560555550454035303025201510
150 100 50 0 50 100 150
With AIDS Without AIDS
50
With AIDS Without AIDS
Source: U.S. Census Bureau demographic estimates and projections, 2004.

P t f A i lt l L b F L t t HIV/AIDS 1985 2020
AIDS’ Effect on African Agriculture
26Namibia
Percent of Agricultural Labor Force Lost to HIV/AIDS, 1985-2020 (Projected)
23
23
Botswana
Zimbabwe
20
20
Mozambique
South Africa
17
14
Kenya
Malawi
14
13
Uganda
Tanzania
Source: Food and Agriculture Organization (FAO), “AIDS—A Threat to Rural Africa: Fact Sheet” (www.fao.org/focus/e/aids/aids6-e.htm).

HIV destroys immune defenses against TB
TuberculosisTuberculosis

HIVHIV
HIV Pathophysiology Life CycleHIV Pathophysiology - Life Cycle
HIVHIV
CD4
CD4 cell

HIVHIV
HIV Pathophysiology Life CycleHIV Pathophysiology - Life Cycle
CD4 Binding
Co-receptor
d g
CD4
p(CCR5 or CXCR4)

HIVHIV
HIV Pathophysiology Life CycleHIV Pathophysiology - Life Cycle
Fusion

HIVHIV
HIV Pathophysiology Life CycleHIV Pathophysiology - Life Cycle
Virion entryVirion entry

HIVHIV
HIV Pathophysiology Life CycleHIV Pathophysiology - Life Cycle

HIVHIV
HIV Pathophysiology Life CycleHIV Pathophysiology - Life Cycle
Reverse transcription
HIV DNA

HIVHIV
HIV Pathophysiology Life CycleHIV Pathophysiology - Life Cycle
Translocation to nucleus

HIVHIV
HIV Pathophysiology Life CycleHIV Pathophysiology - Life Cycle
Integrationg

HIVHIV
HIV Pathophysiology Life CycleHIV Pathophysiology - Life Cycle
Transcription / Translationof HIV mRNA / polyprotein/ p yp

HIVHIV
HIV Pathophysiology Life CycleHIV Pathophysiology - Life Cycle
Protease processingand viral assembly

HIV infection
HIV attacks CD4 cells, the generals of the immune system’s army
HIV inserts itself into our genes
HIV creates many different strainsHIV creates many different strains
CD4 cell

HIV infection
Viral loadViral load
CD4
time Years Weeks

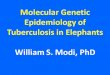
Relationship Between CD4 count and Viral Load
Slow: <5,000, Fast: 50,000+

WHO Stage 2 and 3:Symptomatic HIV infectionC 4 200 00
WHO Stage 1:Asymptomatic HIV infectionCD4 >500
1000CD4 200 - 500Mild infectionsWeight loss, fatigueTB Thrush
WHO Stage 4AIDSCD4 200
TB, Thrush
CD4Count
CD4 < 200TB, infectionsDeath ~18 months
200
642
Time(years)
642

WHO Stage 1 - Asymptomatic HIV Disease
• Minimal symptoms
• Daily battle between virus and immune system; 10,000,000 new virus copies each dayday
• CD4 count drops gradually• CD4 count drops gradually

WHO Stage 2 - Symptomatic HIV Disease
• Early signs of chronic HIV infection:– Weight loss (3-5 kg)– Skin rashes– Respiratory infections
Herpes zoster (“shingles”)– Herpes zoster (“shingles”)
– CD4 count =350-500
• Normal activity, able to work / attend school

Opportunistic Infections - Côte d’Ivoire, Thailand
Prevalence• Tuberculosis 29-37%• Cryptococcosis 19-38%• Wasting syndrome 8-28%• Wasting syndrome 8-28%• Pneumocystis pneumonia 5-20%• Bacterial pneumonia 4%• Esophageal candidiasis 3-6%• Toxoplasmosis 2-3%
Cryptosporidiosis 1 2%• Cryptosporidiosis 1-2%
Sources: Chariyalertsak, 2001; Tansuphasawadikul, 1999; Lorsina, 2004

Goals of HIV Treatment
• Improve quality of life
• Prevent opportunistic infections
• Prevent progression to AIDS
• Prevent death
d h l k l h d f h• Reduce the likelihood of transmission to others (“Secondary prevention”)

HIV Treatment - Antiretrovirals
Fusion/EntryInhibitors (1) Maturation
Inhibitors (~2008)
ProteaseInhibitors(8)
Inhibitors ( 2008)
(8)
ReverseTranscriptaseInhibitors(11) Integration
Inhibitors (~2008)

HIV Treatment - Antiretrovirals
25
30
20 No therapyMonotherapy
15Dual therapy
5
10
Triple therapy
0
5
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15

HIV Treatment - Timing of HIV Treatment
• Therapy is delayed until patients develop WHO Stage 3 or Stage 4 disease
Delaying therapy until Stage 3 or 4 if done carefully does not – Delaying therapy until Stage 3 or 4, if done carefully, does not decrease the likelihood of successful treatment
– Treatment is lifelong and expensive, do not want to start g p ,unnecessarily early
– Delayed therapy minimizes opportunity for side effects
– Delayed therapy minimizes opportunity for drug resistance

CD4 and Mortality - Zimbabwe
1.00
y
CD4 > 200
0.75
0.50Prob
abili
ty
CD4 50-2000.50
0.25
Surv
ival
P
0
0 1 2 3 4
S
CD4 < 50
0 1 2 3 4Time from enrolment to death (years)

Impact of Treatment
Before
AfterAfter

Impact of Treatment
After 9 months

Impact of Treatment
After 9 months

Impact of Treatment
“I was a walking skeleton before I began therapy. I was afraid to gog g py gout of my house and no one would buy things from my shop. Butnow I am fine again… My wife has returned to me and now mychildren are not ashamed to be seen with me. I can work again.”

Impact of Treatment

Impact of Treatment
Begin ART
CD4
Viral load(HIV RNA level)
time Years Weeks

Impact of Treatment - Society
Effective ARVs available
30
35
40Unintentionalinjury
Cancer
20
25
Deaths per 100,000 Population
Heart disease
Suicide
5
10
15
pHIV infection
Homicide
0
5
1982 1984 1986 1988 1990 1992 1994 1996 1998
Chronic liver
disease
Stroke
Diabetes
Source: Centers for Disease Control, 200
YearDiabetes

Current Status of Treatment - December 2004
Source: WHO

Current Status of Treatment - June 2005
Source: WHO

Number of Individuals Receiving ART
Source: WHO

Community-based Care
Care takes place pin the community. Reinforced in the
lclinic.

Basic Water SupplyClinical Indicators
900900101088
‘Viral load’‘Viral load’
CD4 cell countCD4 cell count
800800
700700
10107 7
101066
HIV RNAHIV RNAlevellevel
(cells/(cells/μμL blood)L blood)600600
500500101055
101044
(copies/(copies/mL plasma)mL plasma)
400400
300300
1010
101033
200200
100100
101022
101011
Years Years
WeeksWeeks 1 2 3 4 5 6 7 8 1 2 3 4 5 6 7 8
00101000

Basic Water SupplyState of the Art Technologies
BD FACSCalibur
CD4-countCD4 countstart treatment < 200 cells/ul
RT PCR
Viral load countViral load countmeasure resistance to treatment

Basic Water SupplyLab Diagnostics in Resource Poor Settings

What is Needed
• Low cost
• Easy to use
• Rapid and Robust
• Portable
S d f• Sensitive and specific

Basic Water SupplyMicrochip Technology for Medicine

Basic Water SupplyMicrochips for Bioseparation
–O –O–Si–(CH2)3–S––O
O O
N N–O
O
–O –O–Si–(CH2)3–S––O
O O
N N–O
O
–O –O–Si–(CH2)3–S––O
O O
N N–O
O
silane linker avidin anti-CD4


Basic Water SupplyMicroelectrodes for Biosensing
3x10-14
K+ Cl-
Na+K+K+
Cl-
Cl-lysis3x10-14
K+ Cl-
Na+K+K+
Cl-
Cl-lysis3 0mole ions
Low
NaK K+Cl-
High
3 0mole ions
Low
NaK K+Cl-
Highoconductance
gconductance
oconductance
gconductance
(ohm
-1)
0.0015
0.0020
due
to C
ell L
ysis
(
0.0005
0.0010
ucta
nce
Cha
nge
d
-0.0005
0.0000
MSE Lunch and Learn, Oct 16, 2008Captured Cells on Chip by Optical Microscopy
0 2000 4000 6000 8000 10000 12000
Con
du
-0.0015
-0.0010

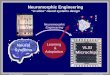
Basic Water SupplyClinical Validation of the Microchip
S iti itTest Positive
N = 49R2 = 0.86
N = 49R2 = 0.86
Sensitivity =
Specificity =
Total PositiveTest NegativeTotal Negativey = x
y = 1.1x
y = x
y = 1.1x
Total Negative
SpecificitySensitivityCD4 Counts(cells/μL)y
0.970.90< 350
1.00.86< 200
(ce s/μ )
0.940.97< 500

Basic Water SupplyCommercial Development