Embed Size (px)
Citation preview

1
SleepParalysis:phenomenology,neurophysiologyandtreatment
ElizavetaSolomonova1,2
1UniversitédeMontréal,Individualizedprogram(CognitiveNeuroscience&Philosophy).2CenterforAdvancedResearchinSleepMedicine,DreamandNightmareLaboratory,Montreal,Canada
Toappearin:TheOxfordHandbookofSpontaneousThought:Mind-Wandering,Creativity,Dreaming,andClinicalConditions.Fox,K&Christoff,K.Eds.
AbstractSleepparalysisisanexperienceofbeingtemporarilyunabletomoveortalkduringthetransitional
periodsbetweensleepandwakefulness:atsleeponsetoruponawakening.Feelingofparalysismaybeaccompaniedbyavarietyofvividandintensesensoryexperiences,includingmentationinvisual,auditory,andtactilemodalities,aswellasadistinctfeelingofpresence.Thischapterdiscussesavarietyofsleepparalysisexperiencesfromtheperspectiveofenactivecognitionandculturalneurophenomenology.Currentknowledgeofneurophysiologyandassociatedconditionsispresented,andsometechniquesforcopingwithsleepparalysisareproposed.Asanexperiencecharacterizedbyahybridstateofdreamingandwaking,sleepparalysisoffersauniquewindowintophenomenologyofspontaneousthoughtinsleep.
Introduction
“Ihadafewterrifyingexperiencesafewyearsago.Iawokeinthemiddleofthenight.Iwassleepingonmyback,andcouldn'tmove,butIhadthesensationIcouldseearoundmyroom.Therewasa
terrifyingfigureloomingoverme.Almostpressingonme.ThebestwayIcoulddescribeitwasthatitwasmadeofshadows.Adeeprumblingorbuzzingsoundwaspresent.ItfeltlikeIwasinthepresence
ofevil...Whichsoundssostrangetosay!”(31yearoldman,USA)
Sleepparalysis(SP)isatransientandgenerallybenignphenomenonoccurringatsleeponsetoruponawakening.Classifiedasarapid-eye-movement(REM)sleep-relatedparasomnia,SPrepresentsapsychophysiologicalstatecharacterizedsimultaneouslybyqualitiesofbothsleepandwakefulness,whereintheexperiencercanopenhereyes(Hishikawa&Kaneko,1965),canbeawareofherphysicalenvironmentbutisunabletomoveandmaystartseeing,hearing,feelingorsensingsomething.
WhiledocumentedinstancesofSPseemtobeveryconsistentacrosscultures,SP’slivedqualities,phenomenology,andinterpretationasameaningfulexperiencevariesdependingontheculturalandreligiousbackground.RootingSPinaparticularbeliefsystemmayeitherhelptheexperiencerrecognizethatSPiscommonandtransient,oramplifynegativequalitiesofSPbygivingmoreconcreteshapetoanalreadyterrifyingexperienceofasupernaturalassault.
TheemotionalexperienceofSPisoftenoneoffear,terrorandpanic.Threateningpresences,thevulnerabilityofbeinginaparalyzedstate,uncontrollablevisions-alltheseelementscontributetointense,predominantlydysphoric,negativeaffect.SomequalitiesofspontaneousthoughtassociatedwithfeltpresenceduringSPcanbeseenasparanoid(Cheyne&Girard,2007),spatial,orinterpersonal/social(Nielsen,2007,Solomonova,2008).ThevastmajorityofSPexperiencesareassociatedwithintensefeelingsofrealism,andaremostoftencharacterizedbyfearanddistress,whichmaycarry-overintowakefulnessandcreateaviciouscycleofnegativeemotionalassociationwithsleep,includingaversiontogoingtobed,andeven,inextremecases,canresultinsymptomsreminiscentofpost-traumaticstressdisorder(McNallyandClancy,2005).Yet,someSPexperiencesaredescribedinpositiveterms,especiallyvestibulo-motorphenomenathatincludeout-of-bodyexperiences(OBE),orsensationsofflyingorfloating.WhiletheintuitiveandimmediatereactiontoSPistypicallynegative,aswillbediscussedinthesectiononpracticalconsiderations,therearenumerousreportsofneutral/positiveSP.Furthermore,thereisapossibilityofharnessingthepowerandpotentialofthedissociative/overlappingstateinordertotakeactivechargeof

2
one'sexperienceandtousetheopportunitypresentedbythesimultaneityofwakingandsleepingcognition-apotentialforenteringintoaluciddreamstateorforcontemplativeself-observation.
Neurophysiologically,SPiscurrentlyunderstoodasastatedissociationorastateoverlapbetweenREMsleepandwakefulness(AmericanAcademyofSleepMedicine,2014).DuringSPonecanopenhereyes,lookaroundtheroom,becomeawareofherenvironmentandsimultaneouslyexperienceREMsleep-relatedparalysis(muscleatonia)aswellasintenseandrealisticimagery1ofallsensorymodalities-anightmarespillingintotherealworld.Normally,duringREMsleep,skeletalmuscleatoniablocksmostmotoroutput,effectivelypreventingthesleeperfromactingoutherdreams(Peever,Luppi,&Montplaisir,2014).SPcanalsooccurinthecontextofnarcolepsy(Sharpless&Barber,2011;Terzaghi,etal,2012),butthemajorityofthosewhoexperienceSPreportitinitsisolatedform(oftenreferredtoasIsolatedSleepParalysis),withoutknownmedicalorneurologicalassociation.
Incurrentmedicalandneuroscientificliterature,SPisdiscussedintermsofitspresentationandnegativefactors:SP-associatedmentationisgenerallyseenasanon-desirableeffectofREMsleepintrusionintowaking.InthischapterIproposethatsituatingSPexperiencesasadreamphenomenonwithintheframeworkofembodiedmindandenactivecognitivescience,includingcontemplativeapproachestoconsciousness,isanalternativethataccountsforthephenomenologyofSPasalivedexperience,allowsforrichanddetailedculturalframingoftheexperience,andoffersavenuesforacross-culturalsocialneurophenomenologyofSP.
First,IwilldiscussthephenomenologyandneurophysiologyofSPexperiences.IwillpresentSPingeneral,withoutdistinguishingbetweenitsisolatedandnarcolepsy-relatedform,unlesssuchaseparationiswarranted.IwillstartbypresentingthecurrentstateofknowledgeofSPprevalence,aswellasthevarietiesofimageryaccompanyingSPandtheirculturalsignificance.IwillthendiscussSPintermsofaREMsleepparasomniaandoutlineitsprecipitatingandenablingfactors,aswellassleepanddreamcharacteristicsofthosewhoexperienceSP.Finally,IwillexamineSPinlightofvariousculturalandsharedpractices,includingpreventativemeasures,andpracticesaimedatinterruptingandtransformingSPexperiences.
TheexperientialexamplesofSPusedinthepresentchapterareallderivedfromanInternet-basedstudyofSP(Solomonovaetal,2008).Ourresearchgroupcollected193responsesfrompeoplewithrecurrentSPexperiences,usingamodifiedversionoftheWaterlooUnusualSleepExperiencesQuestionnaire(Cheyne,Newby-Clark,&Rueffer,1999).Ourparticipantswererecruitedonline,usingwordofmouth,andviaadvertisingonSP-relatedforums,informationandsupport.
Definitionsandprevalence
IdiopathicSP(SPnotassociatedwithnarcolepsy,andwithoutknowncause)isabenignandtransientparasomnia(Howell,2012),occurringduringtransitionsbetweenwakeandsleep:atsleeponsetoruponawakening.TheDiagnosticandStatisticalManualofMentalDisorders(DSM-5)classifiesisolatedSPaccompaniedbyfearfulmentationasaninstanceofanightmaredisorder(AmericanPsychiatricAssociation,2013).DuringanepisodeofSP,characteristicsofREMsleepintrudeuponseeminglyawakeconsciousness:thusthepersonexperiencingSP,whilehavinganimpressionofbeingawakeandawareofherenvironment,isunabletoinitiatevoluntarymovements(i.e.,experiencesREMsleepmuscleatonia/paralysis),andmayalsoexperienceintenseandrealisticsensationsinanysensorymodality-REMsleep-relatedmentation(AmericanAcademyofSleepMedicine,2014).SPshouldbedistinguishedfromnightterrors–earlynightawakeningswithfeelingsofpanic/terror,typicallyassociatedwithsomnambulism-spectrumarousalfromslowwave(Stages3and4)non-REM(NREM)sleep.Nightterrorsarecharacterizedbysuddenawakeninginanagitatedstate,anxiety,bodymotilityandgeneralamnesiawithregardstounderlyingcognitiveexperience(Szelenberger,Niemcewicz&Dabrowska,2009).
PrevalenceestimatesofSPrangewidely,andmaydependongeographicandculturalfactors.AsystematicreviewofSPprevalencehasrevealedthatstudiesreportSPlifetimeprevalencefromaslowas1.5%topossibly100%inthegeneralpopulation(Sharpless&Barber,2011).Theauthorsindicatedthat
1InthischapterIwillusetheterms‘imagery’and‘mentation’interchangeablytorefertovisual,auditory,somatosensoryandevensocialexperiencesduringSP.Theterm‘imagery’hereisthereforenotrestrictedtothevisualdomain.Iprefer‘imagery’and‘mentation’to‘hallucination’inordertoemphasizethedream-likeprocessofspontaneousimaginationthattakesplaceduringSP,andtode-emphasizetheassociationwithdelusionalthoughtandpathologies,associatedwiththeterm‘hallucination’.

3
aboutoneinfiveindividualsmayhaveexperiencedSPatleastonceintheirlifetime(of36,533personsintheirreview).PrevalenceestimationofSPisdifficultduetonumerousfactorssuchasethnicityandculturalbackground,includingvariablefamiliaritywiththephenomenonandinthewordingofquestions(Fukuda,1993).Forexample,inacross-culturalstudy,Fukudaandcolleagues(2000)reportedthatwhileitisunclearwhetherSPisequallyprevalentinCanadaandJapan,thelackoffamiliarityandofanormativeculturalframeworkforSPinCanadamaycontributetothefactthatmanyCanadian,butnotJapanese,respondentsqualifiedSPasakindofadream,andwouldnothave,therefore,readilyrecognizedSPinaprevalencestudy.Anadditionalreasonforunder-diagnosisofSPintheWestmaybethefactthatthosewhoexperienceSPmaybemisdiagnosedashavingpsychiatricdisturbances(Hufford,2005).ThedevelopmentaltrajectoryofSPistraditionallyassociatedwithanonsetduringadolescence,whichmayindicateaprocessassociatedwithsleeparchitecturematuration(Wing,Lee&Chen,1994).However,inonestudyofolderadults,abimodalonsetpatternwasreported,withasecondpatternofonsetofSPepisodesaftertheageof60yearsold(Wingetal,1999),suggestingapossibilitythatSPmayhaveavarietyofonsetconditions.
NeurologicallyandphenomenologicallySPissituatedontheREM-sleepbaseddream/nightmarecontinuum.Inthischapter,IwillapproachSPexperiencesasavariantofintensifiedordisturbeddreaming,andwillsituatethemwithinaframeworkofembodimentandenactivism.
The4EAcognitionandoneiricmentationRecentyearshaveseenthedevelopmentofaparadigmshiftfromastrictlyneurocentricviewofthe
mind,apositionthatcanbestatedas“embrained”(Morris,2010),toadiversefamilyofapproachesthatconsiderthemindembodied(Varela,Thompson&Rosch,1991;Gallagher,2005),enactive(Noe,2004;Thompson,2005;Stewart,Gapenne&DiPaolo,2010),extendedintoandembeddedinthephysicalandsocialworld(Clark&Chalmers,1998;Menary,2010),andaffective(Colombetti,2013;Pessoa,2013).Whiletheseapproachesareinmanyrespectsquitedifferent,theyhavesometimesbeenlabeledas4EA(embodied,embedded,extended,enactive,affective)cognition,withacommonthemeofofferingarobustalternativetocomputational,connectionist,andneuro-reductionistviewsofthemind(Wheeler,2005;Protevi,2012).Thesetheoriesattempttosituatecognition,brainactivity,andpsychophysiologywithinthelargercontextsoflivedsubjectiveexperience,byemphasizingtherolesofdevelopmentalsensorimotorattunementtotheworld,aswellasoftheactiveandmotivatedprocessesofperceptionandsense-making,theimportanceofthesocialandculturalmilieu,andtheroleofemotionandaffect.
Sleepanddreamingphenomenahavebeenonlyrarelyaddressedby4EAtheorists(withtheexceptionofThompson2014,2015a,b),andtheprevailingviewofthesleepingmindtodaysituatessleepmentationasbeingfirmlyconstrainedwithinthebrain(Rechtschaffen,1978;Hobson,Pace-Schott&Stickgold,2000;Revonsuo,2006).AsRevonsuostates:“Theconsciousexperienceswehaveduringdreamingareisolatedfrombehavioralandperceptualinteractionswiththeenvironment,whichrefutesanytheorythatstatesthatorganism-environmentinteractionorotherexternalrelationshipsareconstitutiveoftheexistenceofconsciousness”(Revonsuoetal,2015:3).Alternatively,situatingdreammentationwithinaframeworkof4EAapproachesimpliesthatthedreamingsubjectisnotentirelyisolatedordisconnectedfromenvironmentalandsomaticstimuli,andthatherexperientialselfretainsaffective,social,sensorimotorandsense-makingqualities.Dreamingthenisnotpassivelylivedasapurelymentalsimulation(Revonsuoetal,2015),butcanbeseenasaprocessofactiveimagination(Thompson,2014)rootedinthedreamer’sphysical,socialandaffectiveworld(Solomonova&Sha,2016).IproposethatSPexperiences,byvirtueoftheirspecialkindofoverlapbetweenandsimultaneouspresenceofbothwakinganddreamingcognition,areperfectcandidatesforneurophenomenologicalresearchonspontaneousthoughtinsleep,whichwouldhelpilluminateparticularqualitiesofdreamingcognitionthatmayotherwisebeinaccessibletoreflectiveconsciousnessuponawakeningfromadream.

4
Phenomenologyofsleepparalysisexperiences
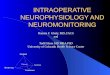
Figure1.Arepresentationofsleepparalysisexperience2.Thesleeperisawakenedsuddenlyandseesamenacing
shadowycreatureontopofhim.Heexperiencesthesensationofbeingpushedintothebed,whilethebeditselfisswirlinginasortofatornado.Thetwofacesofthedreamerrepresentthe“double”consciousnessduringsleepparalysis:heissimultaneouslyterrifiedofthesupernaturalattackerandalsoknowsthatifhedoesnotresisttheexperienceandallowshimselftodriftbackintosleephemayhavealuciddream(thislucidconsciousnessisrepresentedasasleepingfacewithacolorfulbrain,denotingvibrantpossibilitiesoflucidity.Artist:BenjamenSamaha,Montreal,Canada2016.Reproducedwithartist’spermission.
Inadditiontotransientexperienceofmuscleparalysis,themostdramaticqualityofSPisitssensory
content,characterizedbyvivid,intrusiveaudio-visualandsomatosensoryimagery.TheexperienceofSPcanbeextremelyrealistic,haveaquasi-perceptualandwake-likequality,andmaybeaccompaniedbytactileandkinestheticsensations.Reflectivethoughtprocesses,self-awarenessandmetacognitiveabilitiesseemtoberelativelypreservedduringSPexperiences,andpeoplewhohavehadmultipleSPexperiencesmaydevelopa“feel”forrecognizingSPimagery.
SP-associatedexperiencesaretypicallyreferredtoashallucinations(hypnagogic,whenoccurringatsleeponset,orhypnopompic,whenhappeninguponawakening),sincetheseoccurduringotherwiseseeminglyawakeconsciousness(Liddon,1967;AmericanAcademyofSleepMedicine,2014).ThisentailsthatapersonwhoexperiencesSPseessomethingthatisnotthere,somethingthatisdistortedorfalse.SuchaviewpresupposesthatduringSPoneiseffectivelyawakeandismisinterpretingherexperience.AnotherwayoflookingatSPistosituateitwithinthespectrumofdreammentationanddreamingimagination.Whiledreamingtoohasbeenseenasadelusional/hallucinatoryactivity,analternativeview,inlinewithembodiedmindtheoriesandenactiveapproach,hasalsobeenproposed:“Whenyouhallucinate,youseemtoperceive 2Excerptfromthedreamer’saccount:“Thetransitionbetweenwakeandsleepisacrucialmomenttoenterintotheworldofdreams.DuringthistransitiononcountlessoccasionsIwouldawakensuddenlynotbeingabletomove.Duringthisexperienceitseemsthattheveryessenceoffearpermeatesmyconsciousness.Eerinessgoesthroughmysoul,freezesmybloodandinterruptsallsubstantialnotionofmybeing.Nowordscandescribethatvisceralsensation,andinparallel,nowordscancomeoutofmymouth.Awareofthelackofmuscletonus,ItrytoescapethisinevitableMachiavellianblackbeast,thatmaterializesinmyheadbeforemyeyesandonmychest,slowingdownmybreathing.Moreover,mysensesaregrabbedbyanimpressionoffightingahurricanethatmaydragmeoutofmybody.Thiscyclone,thathasablackholeinlieuofaneye,forcesmetofightit,andthisfightseemscrucialtomysurvival(…)Inaddition,thereareauditoryexperiences,anamalgamofpetrifyingwordsandvibrationsthatfeellikesuddengustsofwindintheeardrums.Allthishappenswhenbybodyfeelslikeastatue,withoutapossibilityofscreaming.(…)Onoccasion,withdeterminationandlucidity,Icanhavepoweroverthisswirlofstillness.(…)Itakebacksomecontrolofmyimaginaryhands,andthenIholdthemouttoMorpheusforadazzlingandcolorfuldanceinadeepandenlightenednight”.(MaleSPsufferer,alsodiagnosedwithnarcolepsy.Montreal,Canada.AccounttranslatedfromFrench).

5
whatisnotthere.(…)Whenyouimagine,youevokesomethingabsentandmakeitmentallypresenttoyourattention”(Thompson,2014:179).InthischapterIadoptthislatterviewandwillrefertoSPexperiencesasvariantofspontaneousthought/mentationormentalimagery,ratherthanhallucinationsordelusions.
Kindsofsleepparalysisexperience
AfactoranalysisbyCheyneandcolleagues(1999)showedthatSPmentationtypicallyfallsintothreegeneralcategories.ThefirstcategoryisIntruder,anditischaracterizedbyafeltpresence,fear,aswellasauditoryandvisualimagery.ThepersonwhoexperiencesSPfeelsthatsomeoneisinthehouseorintheirroom.Thisexperienceissometimesaccompaniedbyseeingorhearingsomeoneorsomethingsentientmovearoundthehouse.ThesecondcategoryofSPexperiencesisknownasIncubus,inwhichthefeltpresenceisinterpretedasasupernaturalassaultandisoftenaccompaniedbyasensationofshallowbreathing,afeelingofbeingsmothered,pressureonthechest,orpain.Inthiscase,thesleeperoftenseesandfeelsthemaleficentbeingontopofher.Thethirdcategory,UnusualBodilyExperiences,appearstobeaseparate,lesswell-known,andaqualitativelydifferentkindofSPexperience:theseareoftendescribedaspositiveevents,suchassensationsoffloating,out-of-bodyexperiences(OBEs),andfeelingsofbliss.BothIntruderandIncubuscategoriestypicallyincludetheexperienceoffeltpresence–adistinctsensationthatsomeonesentientisintheimmediatevicinityofthesleeper(Cheyne,2005).
MostliteratureonSPfocusesalmostexclusivelyonthefirsttwokinds,IntruderandIncubus,possiblyduetotheirparticularlyintensifiedfeltpresenceimagery,whichcontributestodistressingSPexperiences(Solomonovaetal,2008;Cheyne,2013).However,neutralandpositiveinstancesofSPhavealsobeendescribed,andthethirdcategory,UnusualBodyExperiences,orvestibulo-motorexperiences,isoftencharacterizedbypleasantsensationsandaspiritofexploration,accompanyingsensationsofflying,out-of-bodyexperiences,orautoscopy(observationofone’sownbodyfromanunusual/novelpointofview)(Brugger,Regard&Landis,1997).
FeltPresence“JustbeforegoingtosleeporifawokensuddenlyIfeelasthoughapresence,usuallyadarkshadow
figureisstandingoverthebedstaringdownatme,orpacingbackandforth.”(22yearold,gendernotreported,USA).
AmongallSPexperiences,feltpresence,thedistinctsensationthatanothersentientbeing,humanornot,ispresentintheextracorporealspaceoftheexperiencer,isarguablythemostsalient,terrifying,andrich..FeltpresenceisconsistentlyreportedasthemostcommonSP-associatedexperience–about80%ofepisodes(Cheyneetal,1999),whichproducesmostfearandSP-relatedstateofdistress(Solomonovaetal,2008).OnesalientfeatureoffeltpresenceexperiencesduringSPisthefactthatitisadistinctsensation,andmayoccurintheabsenceofvisual,auditory,ortactileimagery.FeltpresenceexperiencesduringSPhavebeenclassifiedasaparanoiddelusion(Cheyne&Girard,2007),anexpressionofspatialsocialimagery(Nielsen,2007),andasavariantofbasicintersubjectiveexperienceoftheworld(Solomonova,Frantova,&Nielsen,2010).
Feltpresenceexperiencesareofteninterpretedwithintheculturalframeworkavailabletotheexperiencer(seethefollowingsectionontheculturalneurophenomenologyofSP),butsomebasiccharacteristicsseemtobecommonacrossculturesandages(Cheyne,2001):1)feltpresenceoftenmanifestsfromambiguousstimuli:itisoftendescribedas“shadowy”,anditsphysicalcharacteristicsareoftenunclear;2)theexperiencermayreportadistinctsensationofbeingwatched,andthatthepresencehassomeintentionstowardsthedreamer;theserangefromsomevagueinteresttofull-blownassault;3)feltpresenceisusuallyaccompaniedbyintenseemotions(oftenfearwhenthepresenceisinterpretedasthreatening),sometimestothepointofadistinctfeelingofdread,imminentdeath,orbeinginthepresenceofevil.Positiveemotions,however,arealsopossible,especiallywhentheexperienceisunderstoodasvisitationsbydeceasedrelativesorvisionsofthedivine.
Intruder
ConsiderthefollowingexamplesoffeltpresenceexperiencesoftheIntrudertype:A26-year-oldmanfromtheUnitedStatesreports:“Itfeltasifsomeonewaswatchingmebutsilentlystandingbehindme”.Inthisexamplethepresenceisfeltinadistinctandclearway,butnotseenorheard,yettheexperiencerknowswhereinspacethepresenceislocated.Similarly,a29-year-oldwomanfromUSAregularlyexperiencesthe

6
malevolentpresencewithouteverseeingit:“…feelingofevilthatiswatchingormonitoring;neverabletoactuallyseethis"evilentity".Evenintheabsenceofdirectvisual,auditoryortactileimageryshefeelsthatsheisobservedandthatthepresenceis“evil”.TheambiguousqualitiesofthephysicalattributesofSPvisitorscanbeillustratedbythefollowingtwoexamples.A39-year-oldmanfromUSAwrites:“The"presence"isatallblack/darkestgreyshadowofahumanformwithoutanyfeatures.Itstandsinthedoorwaytomybedroomwaitingtobe"noticed".Likewise,a30-year-oldwomanexperiencedvariouswaysinwhichthepresencewasmanifestingduringherSPattacks:“Onceitseemedashadowwasleavingtheroom.Oneothertimetheshadowseemedtohave"wild"hairorifitdoesn'thavehairatall,itlookedassomesortofblacksomething”.
IncubusTheIncubusexperiencehappenswhentheIntruderphysicallyoppressesthesleeper,sometimesina
ratherdramaticway.Inwordsofa52-year-oldmanfromtheUnitedStates:“Myworstexperiencewasbeingchokedbyamanwhoburstintomybedroom.TheexperiencewassorealandfrighteningthatIwasveryafraidofmySPformanymonthsafter.”TheIncubustakesmanyforms,includinghuman,supernaturalandmorerarely,animal:“Ioftenhallucinatecreatureslikelargecats-lionsortigers,…wrappingthemselvesfirmlyaroundmeandcrushingmybody”writesa20-year-oldwomanfromEngland.
SomeofthemostdramaticandpotentiallytraumaticSPIncubusexperiencesareinstancesthatarelivedassexualassaultoralienabduction.Considerthefollowingexample,reportedbya40-year-oldmanfromtheUnitedStates:“Whenitisa"DarkMan"episode,hemostlikelytouchesme.Eitherbylayingacrossmybody,inasexualwayorinthebeginning,hewouldgrabmeanddragme.IalwaysfeltthatifIletgo,hewouldpullmeoutofmybody”.Similarly,a29-year-oldwomanfromSpaindescribesherdistressingSPexperience:“…extremeterror,thefeelingthatairisdenseanddarker,thatshadowsboilandtakeshape…Ihearsomelowtonenoises,voices,tactilefeelingofgrabbing,ofnakedcoldskin,and,veryrarely,apresence.Verydarkwithroundeyes,spider-likefingers,thatlaughs,messesupthebed,andmakesmefeelterror,withsomesexualapproaches…”.InastudylinkingreportsofspacealienabductiontoSPepisodesMcNallyandClancypresentthiscase:“…femaleabductee…wascompletelyparalyzed,andfeltelectricalvibrationsthroughoutherbody.Shewassweating,strugglingtobreathe,andfeltherheartpoundinginterror.Whensheopenedhereyes,shesawaninsect-likealienbeingontopofherbed”(McNally&Clancy,2005:116).
PositivefeltpresenceexperiencesanddoublingWhilemosteasilyrecognizableandmostcommonlydocumentedcasesoffeltpresenceduringSP
havetodowithathreateningandominous“visitor”,someevidencesuggests,however,thatthepresenceisnotalwaysunderstoodashostile.Suchexperiencesincludeperceptionoffriendsandfamily;visitationfromdeceasedrelativesorbenevolentspirits;anderoticencounterswherethesenseofpresenceiscomforting.A20-year-oldSPsuffererfromtheUnitedStateswrites:“OnceortwiceIhavethoughtthatmyfriendorroommatewasstandingoverme.Iwasconfusedbutnotafraid.”Similarly,encounteringdeceasedfamilymembersinvisionsorindreamscanbeexperiencedasapositivespiritualevent,andpossiblyplayahealingroleinprocessesofbereavement(Garfield,1996;Belickietal,2003).
Finally,anotherrarekindofSP-relatedfeltpresenceepisodeinvolvesfirstanexperienceof“someonethere”,andthenadoublingofthedreamer’sownbody,aself-projectionintotheextracorporealspace.Someindividualsreportthatthefeltpresenceentitiesarebecominganexternalizedviewofthemselves:“SometimesIfeelthatthepresenceismyself,thatIcanwatchmyself”,reportsa21-year-oldmanfromJamaica;“IswitchtoanotherworldandImyselfbecomeapresence”,writesa19-year-oldmanfromRussia.
Bodyexperiencesinsleepparalysis
Most(ifnotall)SPepisodesaredefinedbyanalteredexperienceofthebody.Theseincludesimpleexperienceofmuscleparalysis;sensationsassociatedwithsupernaturalassault,includingtouch,pressureonthechest,orevenchoking;feelingsofunusualvibrationsorfallingintoavortex;andout-of-bodyexperiences,includingflying,falling,ormovingaroundone’shouse.
OneofthemostsalientfeaturesofSPistheREMsleep-relatedmuscleatonia.Theinabilitytomoveisastrikingandunusualexperienceformostindividuals,andthemismatchbetweensensingthebodyandthe

7
lossofvoluntarycontroloverthebody’smovementsmaycontributetoarangeofsomatosensoryexperiences.Asdiscussedabove,someofthemostintenseSPepisodesmayinvolveafeelingofbeingassaultedortouchedbyasupernaturalentity.Forinstance,a34-year-oldmanfromUSAdescribesthefollowingexperience:“Feltmyarmspinnedacrossmychestinastraitjackethold,felthandsonmychestpinningmeagainstawall”.Perceptionofnotbeingabletofullybreathe,oftenaccompaniedbyfeelingofpressureonthechest,maybeprevalentinasmuchas57%ofSPepisodes(Sharplessetal,2010).
AlthoughmostaccountsofandresearchonSPexperiencehavecenteredonparalysisaccompaniedbyterrifyingmentationandbyfeltpresence,notallSPexperiencesarecharacterizedbyimageryandmanyaresimplyexperiencesoftransientbodyparalysisduringthetransitionbetweensleepandwakefulness,withoutanyotheraccompanyingmentalactivity(AmericanAcademyofSleepMedicine,2001).Additionally,SPepisodesmaybepredominantlysomatosensoryinnature:Cheyne(1999)characterizestheseexperiencesasVestibulo-Motormentation.
Autoscopy,out-of-bodyexperiences,vibrations,floating,fallingandbodydoublingexperiences(Cheyne,2002)areallpossiblewithintheSPframeworkduetoitsrelianceondream-supportingREMsleepmechanisms.Duringadream,especiallyaluciddream(whereinoneisawareofthefactthatsheisdreaming),itispossibletohavesimultaneousexperienceofone’sdreambodyandrealbodyatthesametime.Thompson(2014)distinguishesbetweenthedreamingself(Ithedreamer)andthedreamego(Iasdreamt)astwocoincidingmodesofself-experience,whichmaysometimesbeexperiencedinparallel.Thedreamingselfisthesleepingself,itisthe“I”ofthewakinglife,nowengaginginthepracticeofsleepanddreaming.Thedreamego,ontheotherhand,istheexperientialself,immersedinthedreamscenario.TheIasdreamtisthetemporary“I”thattakesonthefirst-personperspectiveasasubject(andsometimesanobject)ofthedreamworld.Seenfromthispointofview,SPepisodesmayrepresentanintenseexperienceofthedreamingego,lackingadreambodyandtemporarily“stuck”withinherimmobilizedsleepingbodyofthedreamingself/Ithedreamerwhileexperiencingdream-likementation.Thisfeelingofbeingstuck,coupledwithawarenessoftheoverlapbetweenstatesofvigilance,maythentransformitselfintoasituationofperceptualdoublingofbodyimagery.
ContrarytomostSPepisodeswithafeltpresencecomponent,somebodilyexperiencesaredescribedinquitepositiveterms.Forinstance,a20-year-oldwomanfromEnglanddescribesthischaracteristicofhertypicalSPepisode:“Generally,theexperiencesstartwithalow,pleasantvibrationthatmovesthroughmybodyindefinedwaves,fromthefeetup.Ifeelthemmoststronglyinthethroatandinmyeardrums”.
Out-of-bodyexperiencesarealsorelativelycommoninSP–asmuchas39%ofSPexperiencershavehadoneatsomepoint(Cheyne,2002).A39-year-oldwomanfromtheUnitedStateswrites:“Ifloatedoutofmybedintothekitchen.But,asIfloatedovermybed,Isawlikethisbeastfigurecrouchedoveronthefrontofmybed.Ifloatedoveritdowntothekitchen.ThatiswhereIsawthisbeautifulkaleidoscope-likeleaves.Theyweresovibrant…Ithenfloatedbacktomyroomintomybody”.InthisexamplethereisacombinationofvariousSPcharacteristics:dream-likementationsuperimposedontotheenvironment,anocturnalvisitor,andanalteredsenseofthebody.
SPexperiencesarealsosometimesaccompaniedbyfalseawakenings—dreamswhereonehasavividandrealisticfeelingofwakingupintheirownbedandengaginginusualactivitiesonlytorealizethattheyarestillasleep(Buzzi,2011).Whilefalseawakeningsaretypicallycharacterizedasdreamexperiences,theirphenomenologyintermsofrealismandpossiblestateoverlapistoadegreesimilartoSP.InCheyne’sreport(2002),58%ofpeoplewhoexperienceSPalsoexperiencedfalseawakeningsatleastoccasionally.Additionally,falseawakeningsareoftenassociatedwithfeelingsofdread,anxiety,andoppression(Green&McCreery,1994;NielsenandZadra,2011),similarlytoSP.ThefollowingtwoexamplesfromourInternet-basedsampleillustratesuchcases:a24-yearoldmanfromtheUnitedStatesreports:“…sometimesIthinkIhavemoved...sometimesevengottenupandwalkedaroundonlytofindthatInevergotupatall.”Inasimilarvein,a21-yearoldmanfromJamaicadescribeshisexperience:“IwillwakeupintoanotherdreaminsidemybedroomandthinkIamawakeandrealizeIamstillsleepingminuteslaterandthesameprocedurerepeatsseveraltimes”.
Emotions
…Extremeanxietyandfear,mindisawake,butbodyisasleep.IfeelasthoughIamtrappedandcannotcommunicatewiththosearoundme.(23-year-oldwoman,USA)

8
ThemostprevalentemotionassociatedwithSPexperiencesisfear.Indeed,themostnaturalreaction
towakingupunabletomoveispanic,andthesensationofconstrictedbreathing(consistentwithREMsleepphysiology)mayincreasethestateofdistress.Sharplessandcolleagues(2010)introducedthetermfearfulisolatedsleepparalysistodenoteSPexperiencescharacterizedbyanintensestateofdistress.
Asmuchas90%ofreportedSPepisodesaredescribedasfearful(Cheyne,Rueffer,&Newby-Clark,1999).Similarly,inanIrishUniversitystudents'sample,fearwasfoundtobethemostprevalentemotion,with82%ofrespondentsstatingthattheyhaveexperiencedfearatsomepointduringaSPepisode(O’Hanlon,Murphy,&DiBlasi,2011).Moreover,nightmarefrequencywaspreviouslyreportedasapredictorofSPoccurrence(Liskovaetal,2016).ThisdatasuggeststhatSP,oratleasttheFearfulformofSP,canbeseenasanintensifiedformofanightmare:arecentstudybyRobertandZadra(2014)reportedthatabout65%ofnightmaresand45%ofbaddreamsarecharacterizedbyfear.
OneapproachtoclassifytheaffectiveandpersonalimpactofSPexperiencesistoassessnotonlyfrequencyorintensityofSPepisodes,butalsodistressassociatedwithSPexperiences(Solomonovaetal,2008;Cheyne&Pennycook,2013).TowhatextentistheindividualaffectedbySP?Towhatextentdonegativeemotionscarry-overfromanSPepisodeintowakinglife?DoSPexperiencespromoteanegativerelationshipwithsleep?Thesequestionshavebeensuccessfullyexaminedinpreviousresearchonnightmares(Belicki,1992;Blagrove,Farmer&Williams,2004),showingthattheindividualimpactofnegativeandintensedreamexperiencesdependsmoreonatrait-likereactivity,sometimesreferredtoasaffectdistress(Nielsen&Levine,2007).Thistraitisthoughttorepresentageneraldysfunctionofaffectregulationnetwork,andithasbeenshowntobeabettermeasureofhowmuchnightmaresinfluencewakinglifeemotionalwell-beingthanfrequencyorintensityofself-reportednightmareoccurrence.Furthermore,affectdistressmediatesreactivity,negativeinterpretationanddegreeofnegativereactiontonightmares(Belicki,1992;Levin&Fireman,2002).AccordingtoNielsenandLevine(2007;Levine&Nielsen,2009),dreaminghelpsregulateemotionalmemoryconsolidationandemotionalreactivityviafearextinction.Nightmares,therefore,representacaseofproblematic/dysfunctionalprocessesoffearextinction.Incombinationwithotherfactors,affectdistressislikelytoplayaroleinformation,experienceandinterpretationofSP.
PositiveemotionsassociatedwithSParemuchlessstudied,anditisnotpossibletoaccuratelyestimatetheirprevalence.Onepossiblereasonforthisislackofappropriatescreening(SPisoftendiagnosedasanunpleasantphenomenon)andlackofmedical/psychiatricconcern:patientsarenotverylikelytodescribesuchexperiencestotheirhealthpractitioner,sincetheyarenotbotheredbythem.Inaddition,thecurrentdiagnosticcriteriaforarecurrentisolatedSPaslistedinthelatesteditionoftheInternationalClassificationofSleepDisorders–3dedition(AmericanAcademyofSleepMedicine,2014),includethattheepisodesmustcause“clinicallysignificantdistressincludingbedtimeanxietyorfearofsleep”.Suchaprovisionwouldeffectivelyexcludeallpossiblepositiveandnon-distressingSPphenomenafrominvestigationand/ordiagnosis.Nonetheless,inaweb-basedSPstudyCheyne(2002)reportsthatinadditiontoanger(30%ofrespondents)andsadness(23%),bliss(17%)anderoticsensations(17%)arealsosometimespresentinSP.
Visualandauditoryexperiences
Feltpresenceisthemostprevalent,themostemotionallydisturbing,andthemostsalientSP-relatedexperience.Therefore,itisunsurprisingthatmostvisualandauditorymentationduringSPusuallyhassomethingtodowiththeseunwelcomevisitors.Theentities,however,whilefeltinaverydistinctiveandconcreteway,areoftendescribedvisuallyasrathergeneralandvagueshadowybeings.Visualexperiencesarereportedtooccurin54%–56%andauditoryexperiencesin55%-60%(Solomonovaetal,2008;Cheyne,2002)ofSPsufferers.
SPmaybeaccompaniedbyauditoryexperiences,rangingfromabstractandmechanicalsounds,suchaselectricsoundsandsoundsofbuzzing,tovividauditoryimagery,consistentwithSPexperienceofanIntruderoranIncubus.Soundsoffootstepsandofvoicesareoftenreported(Cheyne,Rueffer&Newby-Clark,1999;Cheyne,2002;Solomonovaetal,2008).

9
CulturalgroundingofSP
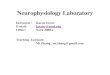
Figure2.HenryFuseli.TheNightmare.1781.DetroitInstituteofArt.PublicDomainimage:https://commons.wikimedia.org/w/index.php?curid=15453518
Whilesleepparalysisisalesser-knownsleepphenomenonintheWest,itisquiteprevalentandis
well-describedinmanyothercultures.DuetothelackofgeneralawarenessofSPintheWest,itisrarelydiscussedinthecontextoffamilymedicineorpsychology.Cross-culturalworkonSPrevealedthatitisrootedinavarietyofreligiousbeliefsandculturalschemas,includinginterpretationsoftheexperienceandtechniquestoengagewiththenocturnalvisitors.SomeofthecommonqualitiesofSPacrosscultures(Adler,2011)include:1)sensationofbeingawake;2)perceptionoftheenvironment;3)paralysis;4)feelingoffearanddread;5)feltpresence;6)chestpressure/breathingdifficulties;7)supineposition;6)variousunusualbodysensations.Theseapparentlyculturally-invariantqualitiesofSP-relatedoccurrencesoftheexperienceofasupernaturalattackhavebeenatthecenterofthephenomenologicalandcross-culturalcognitiveresearchonSP.
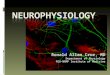
Figure2isareproductionofaneighteenth-centuryworkbyHenriFuselientitledTheNightmare.Itrepresentsasleepingwomaninasupinepositionbeingoppressedbyamaleficentcreaturesittingonherchestandwithanominouspresenceofthenight-mare.ItislikelythattheearlyuseoftheEnglishtermnightmarewastodescribeintenseSP(Orly&Haines,2014).Culture-specificpresentationsofSP-relatedfeltpresenceexperiencestypicallyinvolveamaleficentsupernaturalbeing,suchasawitchoranevilspirit.SomeexamplesfoundacrossculturesincludethekanashibaridemoninJapan(Fukudaetal,1987;Arikawa,Templer&Brown,1999);kokmaintheWestIndies(Ness,1983);“oldhag”inNewfoundland(Hufford,1989);pandafecheinItaly(Jalal,Romanelli&Hinton,2015);uqumangirniqamongtheInuitofBaffinIsland(Law&Kirmayer,2005);andmanyothers(foracomprehensivelistoftermsforSPexperiencesseeAdler,2011).Figure3illustratesapossibleSPrepresentation(Orly&Haines,2014):aJapanesedemonYamachichioppressesandinhalesthebreathofthesleeper.
ThefirstsystematicculturalexplorationofSPwasdonebyHufford(1989):hedescribedaphenomenonspecifictoNewfoundland–the“oldhag”witchattack.InhisbookHufforddiscussesthetensioninsituatingSPexperiencessomewherebetweenthe‘culturalsourcehypothesis’,whereinculturalinterpretationsandframinginfluencehowanexperienceunfolds,andthe‘experientialsourcehypothesis’,wheresomeinvariantlivedexperiences,suchasSP,mayinfluencethedevelopmentofaspiritual

10
interpretationandformationofculturalbeliefs(Hufford1989,2005).Similartothisnotion,McNamaraandBulkeley(2015)proposedanexperientialhypothesistodescribehowdreamsandotherdream-associatedexperiences,includingvisionsandtranscendentalexperiences,canbeseenasacornerstoneandasourceofreligiousbelief(McNamara&Bulkeley,2015).Accordingtothisview,anumberofcultural,religiousandparanormalbeliefsareshapedprimarilybydirectexperienceandthenframedwithinaparticulartradition,whichimbuesthemwithexistentialandmetaphysicalmeaning,anotionthatisreminiscentofWilliamJames’groundingofmysticalexperienceinthephenomenologyoflivedexperience(James,1985).
Theeffectofframingsuchintensesubjectiveexperienceswithinaculturaltraditioncanhaveatleasttwokindsofpotentiallyopposingeffects.Ontheonehand,manyculturesprovidenotonlysupernaturalexplanationsofSP,butalsoremediesandprotectiveritualsagainstit(someofwhicharedescribedinthelaterpartofthischapter),thusrootingtheSPinaframeworkwhichallowsforsharednarrativeandforpracticalinterventions.Ontheotherhand,intenseandfearfulSP,wheninterpretedassupernaturalassault,hasapotentialfortraumatizingthesleeper,thuscreatingaviciouscircleofanxiety,aversiontosleep,facilitationoffutureSPepisodes(Hintonetal,2005;Sharplessetal,2010),andincreasingthelevelofdistressvia“culturalfearpriming”(Ohayonetal,1999;Jalal,Romanelli,&Hinton,2015).Forinstance,theIncubusexperience,whenseenaspartoftheChristiantraditionstartingwiththelateAntiqueperiod,accordingtoGordon(2015),gainedadditionalstigmatizingpower,withaconnotationofanillicitsupernaturalsexualexperience.NotonlywereSPvictimslivingthroughawakingnightmareofanencounterwithademonicassailant,theywerealsoseenasresponsibleforhavingsummoneditduetotheirownsinfulpredisposition/thoughts/impurities.
ItisimportanttonotethatwhileSPcanincludearangeofexperiences,suchaspositiveexperiences,neutralemotions,vestibulo-motorphenomena,out-of-bodyexperiences,andothers,mostculturalinterpretationsofSPdealspecificallywithoverlappingaspectsofIntruderandIncubus.
Figure3.TakeharaShunsen.Yamachichi.Publicdomainimage:
https://commons.wikimedia.org/w/index.php?curid=2074508
Neuralbasis,associatedconditions,andprecipitatingfactors
Humansleepistypicallydividedintotwokinds:REMsleepandNREMsleep.HealthyadultsalternatebetweenNREMandREMincycleslastingabout90minutes,foratotalof5-6cyclesoveranightofsleep.

11
Whileitispossibletoexperiencedreaminginallstagesofsleep,REMsleepistypicallycharacterizedbythemostvivid,realistic,bizarre,andemotionallyintensesleepmentation(Nielsen,2000).Othervividdreamexperiences,suchasnightmares(Nielsen&Levin,2007)andluciddreams(LaBerge,Levitan&Dement,1986),arealsotypicallyassociatedwithREMsleep.
Withinthecontextofnarcolepsy,sleepparalysisisapartofthediagnostictetrad,alongsidedaytimesleepiness,cataplexy,andhypnagogichallucinations(Thorpy,2016).Thereisnotsufficientdatatoassesswhethertherearesignificantdifferencesinphenomenologybetweennarcolepsy-associatedSPandtheisolatedform.
SPepisodesarecharacterizedbysimultaneouspresenceofwakingthoughtandofREMsleeppsychophysiology(Mahowald&Schenck,1991,2005;Terzaghietal.,2012),andthesleepercanoftenopenhereyesandbecomerelativelyawareofherenvironment,whileREMsleep-relatedspontaneousmentation-vividdreaming-superimposesontootherwiseawakeconsciousness.Thisimagerymayoccuratsleeponset(hypnagogic)oruponawakening(hypnopompic).OthercharacteristicsofREMsleep,suchasairwayocclusionandrapidshallowrespiration(Gouldetal.,1988)maycontributetothefeelingofbeingsuffocatedortheperceptionofshortnessofbreathoftenreportedbySPsufferers.Additionally,inonestudyobstructivesleepapneawasfoundtobeapossibleprecipitatingfactorforISP(Hsiehetal,2010).
LittleresearchhasbeendoneonthesleepcharacteristicsofSPsufferers.SomepreliminarydatasuggeststhattheSPsleepprofilemaybesimilartothatoffrequentnightmaresufferers(Nielsenetal,2010),inthatSPparticipantsappear,paradoxically,toexhibitlessREMsleeppressure,havemore“skipped”REMsleepperiods,andshownoincreaseineyemovementdensity(asopposedtohealthycontrols)throughoutthenight(Solomonova,etal,2012).SPparticipantsalsoshowhigherdeltapowerduringsleepthannon-SPcontrols(Marquisetal,2015),whichsuggestsalterationofprocessesofwake-NREM-REMregulation.
Someofthevestibulo-motorcharacteristics,suchasautoscopy,out-of-bodyexperiences,andfeelingsofphysicaltransformation,maystemfromdisturbancesinrightparietalregions(Jalal&Ramachandran,2014):themismatchbetweenintendedmotormovementandinabilitytomovemaycontributetounusualphysicalsensations.
SPmaybeexperimentallyelicitedinlaboratorysettings,butonlyusinganarduousprotocolofrepeatedsleepinterruption.Forexample,SPepisodeswereexperimentallyinducedbylettingparticipantssleepuninterruptedforthefirstNREMperiod,thuseliminatingmostoftheslow-wavesleeppressure(atendencyofslow-waveNREMsleeptotakeprecedenceandoccupyalargeproportionofearlynightsleep),andthenrepeatedlyawakeningparticipantsafter5minutesofREMsleephaveelapsed,thusaugmentingREMsleeppressureandfacilitatingsleep-onsetREMperiods(SOREMPs).SOREMPsmaybeseenasafacilitatingfactorinaREM-wakestatedissociationthoughttocharacterizeSPexperiences.Itshouldbenoted,however,thatevenwithinsuchcontrolledsettingsanddemandingprotocols,ratesofSPwererelativelylow:6episodestotalin16participantswhoalreadyhadatendencytowardrecurrentisolatedSP(Takeuchietal.,1992),and8episodesfrom184sleepinterruptionsin13SPsufferers(Takeuchietal,2002).TheseresultssuggestthatincidenceofSPatsleeponsetmaysignifyanindividual’spropensitytoenterintoREMsleepdirectlyuponfallingasleep.ThisfurthersupportstheideathatSPmayresultfromalterationsinwake-REM-NREMregulationpatterns,resultinginstateoverlap.
AssociatedconditionsLittleisknownabouttheepidemiologyofSP,butgrowingevidencepointstoacombinationof
geneticandexperientialfactors.TheonlystudytodatetoexaminegeneticfactorsassociatedwithSPhasreportedmoderateheritabilityandthatthiseffectwasassociatedwithfactorsknowntocontributetodisruptedsleepcycles(Denisetal.,2015).Sleepfragmentationanddisruptioninwake-NREM-REMregulationareanimportantfactorfacilitatingSPoccurrence,butitisuncertainwhetheralltypesofSPcanbeexplainedbyapropensityforsleepfragmentation.SomeethnicgroupsseemtobemorelikelytoexperienceSPthanothers.TheHmongpopulationinWisconsin,forinstance,hadasignificantlyhigherincidenceofSPthananon-Hmongcohort(Youngetal,2013),withasmuchas31%ofinterviewedHmongparticipantreportingatleastweeklyoccurrenceofSPepisodes.IndividualsofAfricandescentalsoseemtohaveelevatedratesofSP(Belletal,1984;Friedman&Paradis,2002).
Linksbetweenaffectivedisorders,especiallydepressionandanxiety,andSPhavealsobeenreported.ArelationshiphavebeenfoundbetweenSPanddepressionmagnitudeandanxiety(Szklo-Coxe,Young,Finn,&Mignot,2007),socialphobiaandpanicdisorder(Paradis&Friedman,2005;Ottoetal,2006;Sharplessetal,2010)andsocialanxiety(Simard&Nielsen,2005),especiallywiththesensationofbeingobserved

12
(Solomonovaetal,2008).ChangesinREMsleepregulationareoftenfoundinmooddisorders,especiallyindepression(Arargun&Cartwright,2003;Nofzingeretal,1994)
Therelationshipbetweentrauma,especiallypost-traumaticstressdisorder(PTSD),andSPhasbeennotedbyanumberofresearchers.McNallyandClancyfoundthattherewasahigherproportionofSPreportsinparticipantswithahistoryofchildhoodsexualabuse(McNally&Clancy,2005a),andAbramsandcolleagues(2008)reportedthatsexualabusesurvivorsreportmoredistressingandmorefrequentSPincidence.Inaddition,higherratesofSPwerefoundinHmongpopulationinrelationtotraumaticVietnamWarexperiences(Youngetal,2013),aswellasinKhmer(Hintonetal,2005a)andCambodianrefugees(Hintonetal,2005b).Similarly,SharplessandGrom(2013)reportthatsomecasesofSPonsetinadolescentsbeginafterthelossofafamilymember.ConsideringthatSPmaybeconceptualizedasanightmarespectrumexperience,thisrelationshipmayrepresentthesamedysfunctionintheaffectregulationnetwork(LevinandNielsen,2007;Nielsen&Levin,2007)astheonethathasbeenproposedtobeinvolvedinnightmareproduction.PTSD-relatedsleepdisturbanceshavebeenextensivelydocumented(Spoormaker&Montgomery,2008;Germain,Buysse&Nofzinger,2008),includingREMsleepdysregulationandincreasednightmares(Melmanetal,2002;Germain,2013),whichinitselfmaycontributetoalteredREMsleeppressure,inturnfacilitatingoccurrenceofSPepisodes.
SinceSPisoftenassociatedwithintense,detailed,andtroublingvisions,alinkbetweenSPandpsychiatricdisordershasbeenhypothesized.Research,however,showsnoconsistentrelationshipbetweenpsychiatricconditionsandSP,withtheexceptionsofPTSD,panicdisorder,andsocialanxiety.InonestudyanumberoflinksbetweenSPandpsychiatricconditionswerefound(Ohayonetal.,1999);thesefindings,werechallenged,however,byaninternet-basedstudy(Solomonovaetal.,2008),withalargersamplesize,inwhichnostronglinksbetweenpsychopathologyandSPweredescribed.However,whileisolatedSPoftenpresentsitselfintheabsenceofpsychopathology,higherratesofhypnagogicandhypnopompicexperiences(dreamexperiencesoccurringduringthetransitionbetweensleepandwake:atsleeponsetoruponawakenings,respectively),someofwhichmaybeassociatedwithSP,areoftenfoundinpsychosis(PlanteandWinkelman,2008).
PrecipitatingfactorsIntheirrecentbook,SharplessandDoghramji(2015)listanumberofplausibleprecipitatingfactors
forSPoccurrenceinsusceptibleindividuals.Sleepfragmentationandinsufficientsleepareamongthemostobviousfactors.REMsleepdeprivationhasbeenshowntoincreaseREMsleeppressurecontributingtoREMreboundeffectandintensifieddreamsatsleeponset(Nielsenetal,2005).PoorsleepqualitywithfrequentawakeningsanddisruptionsmayalsofacilitateREM-wakeoverlap,creatingfruitfulconditionsfortheoccurrenceofSOREMPs(Takeuchietal,1991,2002;Spanosetal,1995).Shiftwork,jet-lag,useofsleepdisruptingmedication,stress,anxiety–allthesefactorsaffectsleepandmayfacilitateaSPepisode.AlcoholconsumptionwasalsoreportedtopromoteSP(Golzari&Ghabili,2013;Munezawaetal,2011),probablyduetoitseffectonalteringsleeparchitecture(Roehrs&Roth,2001).SleepinginasupinepositionalsoappearstoenhancetheriskofaSPepisode(Sharplessetal,2010).
NeurocognitiveconsiderationsAreturntofeltpresenceWhileundoubtedlyfeltpresencesareahallmarkofSP,especiallyoftheintenseandfrightening
episodes,presenceexperiencesarenotrestrictedtothisparasomniaandarereportedinavarietyofconditions,thuspossiblyrepresentingamoregeneralandbasicsocialimageryprocess(Nielsen2007,Solomonova,Frantova&Nielsen,2011).Arguably,themostsalientandcompellingfeltpresenceoccursinthecontextofmysticalandspiritualexperiences.Otto(1958)introducedtheideaofthenuminousasacornerstoneofreligiousmysticalexperiences.Someoftherecentworkcomesfromanthropology:theecstaticpresenceofGodismanifestedinthecommunityofEvangelicalChristiansintheUSA(Luhrmann,2012).Otherexamplesoffeltpresencehavebeendocumentedinsituationsthatarephysicallyandemotionallystrainingornovel.Someexamplesoftheseexperiencesincludehighaltitudeclimbing(Brugger,Regard,Landis,&Oelz,1999);feelingofthepresenceofababyinpostpartummothers(Nielsen&Paquette,2007);presenceofdeceasedrelativesinthecontextofbereavement(Simon-Buller,Christopherson&Jones,1989;Taylor,2005;Keen,Murray&Payne,2013);inextremeenvironments,suchassolitarysailing(seealsochapterbySuedfeld

13
inthisvolume),survivinginremoteandhostileenvironments(Suedfeld&Mocellin,1987),andothers.Whileinmostcasesfeltpresenceisexperiencedspontaneously,insomecasesitmaybeaproductofsustainedmentalpractices(asinprayerandsomeformsofmeditation).Onecontemporarynon-religiousphenomenonistulpamancy(Veissiere,2016)–along-termpracticeofconjuringupimaginarycompanions,that,overtime,maybeexperiencedasalmostasrealasotherpeople.
Additionally,beingabletohaveafeltsenseofothersmaybeseenasaprerequisiteforthedevelopmentofsubjectivity.Recentworkinphenomenologyandenactivismsuggeststhatdevelopmentofsenseofselfdependscruciallyonsensingothers,asearlyasinutero(Gallagher,2005;Ammaniti&Gallese,2014),thatthesenseofone’sownbodydependsonthesenseofothers(Maclaren,2008)andthattheself-otherdynamicisanecessaryconditionforthesenseofself(Zahavi,2014).Evidencefromdreamresearchtoosuggeststhatdreamprocessesarerelationalandintersubjective.Thefactthatdreamsaremostoftenaboutotherpeoplehasbeenconceptualizedassimulationsofsocialinteraction(Revonsuo,2016)andasrepresentationsofindividualattachmentstyles(McNamaraetal,2001).Additionally,dreams,similarlytowaking,canbeseenasadynamicinteractionbetweenthe“self”-relatedand“non-self”elementsofdreamcontent(everythingextraneoustothedreamer).Thesenon-selfelements(non-humancharacters,dreamenvironment,evendreamobjectscanbeseenasa“dreamother”duetotheirinherentrelationalproperty(Solomonovaetal2015)andtothefactthatdreamenvironmentinitsentiretyaffectivelymotivatesdreamertoengagewithit.
.TowardaculturalneurophenomenologyofSP
SPhasoftenbeencharacterizedasdissociative(Terzaghietal.,2012)state,sinceiteffectivelycombinescharacteristicsof'waking'consciousness(self-awareness,accesstoautobiographicalmemory,abilitytoopeneyesandperceivetheenvironment)withREM-sleepphenomena,specificallymuscleatonia/paralysisandmentation/dreams.ThisnotionofSPasdissociativehasbeenattheheartofthepreviousneurobiologicalworkonthelinkbetweendreamingandREMsleep.TherelativedeactivationofthedorsolateralprefrontalcortexcharacteristicofREMsleep(Hobson,Stickgold&Pace-Schott,1988;Maquet,2000)hasbeenlonghypothesizedtobeattherootofthelossofautobiographicmemoryandoftheinabilitytoappreciatethecontentsofthedreamas"bizarre"orimplausibleinrelationtoreality.ThishasledtothehypothesisthatinREMsleepdreamingoneiseffectivelydelusionalandinastateofatransientpsychosis(Hobson,2004).InSP,similarly,thereisoftenincompleteautobiographicalaccess.ThisassociationbetweenSPandREMsleephasalsodisplacedtheexperienceofSPfromthepsycho-spiritualdomainofmeaningfulencounterswithmenacing/unreal/supernaturalothers,intoamorereductionistaccountofuncontrollableandinescapableREM-initiatedhallucinations. Incontrast,anaccountofSPinthecontextofanoneiricphenomenologyandina4EAperspectivemayallowforamorenuancedreadingoftheseexperiences.Anemergingneurophenomenologicalframeworkofsleepchallengesstrictdistinctionsbetweenwake,NREM,andREMsleep.Indeed,whileSPisoneoftheexamplesofsimultaneouspresenceofREMsleepandwakeprocesses,itisnottheonlyphenomenonthatatteststothefluidityandinterpermeabilityofstatesofconsciousness.LuciddreamingisanotherexampleofREM-wakeco-occurrence(LaBerge,1986);REMsleepbehaviourdisorderischaracterizedbypreservedmotoroutputduringREMdreaming(Peever,Luppi&Montplaisir,2014);somnambulismepisodescombineNREMandwakephysiologyandphenomenology(Zadraetal,2004);andavarietyofdream-enactingbehaviours,suchaslaughing,simplemovement,cryingandlookingforababyinbed,areprevalentinnormalpopulations(Nielsen&Paquette,2007;Nielsen,Svob&Kuiken,2010).
AmorecontinuousviewofmentationinsleepincludesviewingSPasaformofoneiricexperience:asaprocessofintensifiedmind-wandering(Foxetal,2013),asaprocessofcreativity(Hartmann&Kunzendorf,2013),orasenactiveimagination(Thompson,2014),aprocessofsense-makinginarich,embodiedandintersubjectiveworld(Solomonova&Sha,2016).Inhisdiscussionofluciddreaming,Thompson(2014)proposesthatinadditiontoseeingthisstateasadissociativesuperimpositionoftwodistinctstatesofconsciousness,itmaybesimultaneouslyapproachedasanintegrativestate,thusallowingforanintegrationoftwodifferentyetrelatedwaysofself-experience.
WhileSPsufferersfeelawakeandintheirownbed,therealismoftheexperienceandthequalityoftotalimmersionarecompletelyoverpoweringtothedreamer,sothatsheisunabletoappreciatethedreamlikequalityortheunrealityoftheSPepisode.Thehighprevalenceoftactileandphysicalsensations

14
probablycontributestothiseffect.Thereare,however,numerousaccountsoflong-timeSPexperiencersthatarecharacterizedbyacertain'feel'fortheexperienceassomewherebetweenrealandunreal.SP-relatedexperiencesmayhaveaverycompellingandrealisticquality,buttheyareusuallyliveddifferentlyfromwakingexperiences,asakindofaliminalstate.
Considerthefollowingexample:whiletheparticipantisexperiencingintenseemotionandisquiteabsorbedintheunfoldingontheSP,heseemstohaveakindofadualawarenessregardingthenatureofhisSP:
“…Can’t.Move.Notamuscle.Notaneyelash.It'softenaccompaniedbyhallucinations.Sothisbizarreorterrifyingeventishappeningallaroundme,andIamcompletelyunabletorespondordefendmyself.SometimesIknowit'snotreal,somewhereinmymind,butitlooksreal,anditsoundsreal,andI'mterrifiedorrevolted(ormaybejustbemused),butIcannotwakemyselfuptostopit.”(30-year-oldman,USA)
Similarly,inanotherexampletheexperiencerisalsohesitanttoascribeanyparticularstatetoherexperience:
“…Imightbeansweringwrong,becauseIseethebeingsinmydream-stateimmediatelybeforewaking.Buttheirpresenceseemssoreal,Iwouldcomparetheexperiencetohavingthemaccompanyingmeintheroom”.(48-year-oldwoman,USA)
GroundingSPinitsculturalcontextallowsustoappreciatethevarietyoffactorscontributingto
qualitiesofthelivedexperience,anditmaynotbepossibletodissecttherelativecontributionofthemultitudeofneural,phenomenologicalandculturalnarrativefactors(Kirmayer,2009).Importantly,inthecurrentmedicalcontext,reducingSPtoadysfunctionofREMpsychophysiologymayalsohaveanimportanteffectonreducingthepotentialforadeeperexplorationofSPasaspiritualexperience(Hufford,2005).
TheculturalneurophenomenologyofSPisapowerfultoolforinvestigatingSPfromthe4EAcognitionperspective.Asneurophysiological,experientialaccountsofSPshow,thedreamerisinfactembodied–theoneiricscenarioisdependentonthedreamer’sstateofconsciousness(REMintrusion)andonthedreamer’sphysiologicalstate(atonia,shallowrapidbreathing).Sheisembeddedinaphysical(interpretsambiguousstimuliaroundher)andinaculturalworld(theseambiguousstimulitakeonafamiliarshape/areinfusedwithadeeperculturalandinterpersonalsignification).Thesleeperisalsoextendedintotheworld–thewholeenvironment,bothdreamtandreal,ispartofherongoingexperience;andherexperienceisenactive–thereisarelationalquality:sheisnotapassiveobserveroftheoneiricdramaunfoldingbeforehereyes,butrathersheisdeeplyengaged(Solomonova&Sha,2016).
InordertoelucidateneurophenomenologicalqualitiesofSPingreaterdetail,futureworkmayusemicrodynamicphenomenology/elicitationinterviews,aimedatuncoveringthefine-grainedtemporalandstructuralqualitiesoflivedexperience(Nielsen,thisvolume;Petitmengin,2006;Petitmengin&Lachaux,2013),inadditiontoneurophysiologicaldataanddeepawarenessofthecultural,religiousandspiritualcontextoftheexperiencer.
Sleepparalysispractices:prevention,disruption,treatmentandexploration
WhileSPremainsarelativelyunknownphenomenoninmuchofEuropeandAmerica,anumberofpracticalculture-specificpracticeshavebeendevelopedtoprotectthesleeperfromthenegativeinfluenceofpresumedsupernaturalforces.Whilesomeofthesemethodshavedeeprootsintheirrespectivemetaphysicalcontexts,andthereforeneedtobegroundedinexistingreligiousandmysticalpractices,anumberofpracticalandconceptuallyneutralrecommendationshaveemerged,andseembeneficialformostSPsufferers,regardlessofbackground.
NoestablishedtreatmentforSPcurrentlyexists;itsclinicalmanagementisinsteadoftenfocusedontreatingcomorbidproblems.AccordingtoareviewbySharpless&Doghramji(2015),psychoanalysis,cognitive-behaviouraltherapy(CBT),hypnosis,andeducationinsleephygienehavebeeninvestigatedinrelationtoSP,butnoempiricalconsensusonefficacyofsuchinterventionsiscurrentlyavailable.BasedontheavailableevidenceonSPandcognitive-behaviouralapproachestotreatmentofsleepdisorders,especiallyinsomnia,theauthorsproposeamanualforCBT-ISP.ThisisapromisingfirststeptowardfindingasystematicmethodofdealingwithSP.SparseevidenceforpharmacologicalinterventionsforSPalsoexists:inonestudyitwassuggestedthatREMsleep-suppressingantidepressantsmayprovidetemporaryrelief(PlanteandWinkelman,2008),andtreatmentofnarcolepsymayreduceSPfrequency(Mamelaketal.,2004).

15
Antidepressantsandanxiolyticswerealsousedinseverecases(Hsiehetal.,2010).TerrillonandMarques-Bonham(2001)proposedthatmanagementofSPmightbenefitfromadministrationofmelatonin,whichwouldhelpnormalizethecircadianrhythm.Thecostofsideeffectsassociatedwiththesetreatments,however,mayoutweighthebenefit,andShaplessandDoghramji(2015)argueforacautiousapproach,tailoredtoeachindividualsituation.
Whilemethodsfordealingwithsleepparalysishavenotbeensystematicallyexploredbyempiricalpsychologyorcognitivescience,thecontemporarycontextofInternet-facilitatedsupportgroupsandinformationsharingpracticesarechangingthesolitaryandculture-boundnatureofSPattacks.Furthermore,anumberofmethodshavebeenanecdotallyreportedanddocumentedonlineandinprint,thatseeSPexperiencesasanopportunityratherthananuisance,andpromoteexplorationofone’sownconsciousnessviaSP-supportedluciddreamingorevencontemplativeapproachestoSP(Hurd,2010).Onepopularsupportgroup-mailinglistisknownas“Awarenessduringsleepparalysis”(ASP),andaredditgrouponSPcountsover4000users,sharinginformationonthephenomenologyoftheirexperiencesandmethodsofovercomingthem.
CulturalandclinicalpracticesassociatedwithSPcanberoughlyseparatedintothreekinds:1)preventativepractices,focusedonavoidingSP-enablingcircumstances;2)disruptivepractices,designedtostopSPinthemiddleoftheexperience;and3)observational/explorativepractices,aimingatobservingSPandpossiblytransformingitintoapositiveevent,suchasaluciddreamoranout-of-bodyexperience.
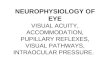
RaisingawarenessofSP-associatedphenomenaitselfmaybeoneofthemostimportantfactorsinreducingfearanddistressbefore,duringandafterSPoccurrence(Ottoetal.,2006;Sharplessetal,2010).Indeed,knowingthattheexperienceistransient(willnotlast),benign(doesnotcontainanyrealdanger),andcommon(issharedwithmanyindividualsacrosstheworld)arepowerfultoolsforpsychologicaldistancingandforfacilitatinganeventualobservational,asopposedtofullyimmersiveandfatalistic,attitudetowardSP.KnowingaboutSPphenomenologyandneurophysiologyandhavingaccesstoculturalgroundingwithavailablesymbolicgestureshelpsprevent,disruptandtransformanegativeexperienceintoatoolforself-exploration.Figure4summarizestheintricatelinksbetweenprecipitatingfactorsandeffectsofSPexperiencesinlightofdisruptive,andobservational/transformationalpractices.
Methodsforpreventingsleepparalysis
Whileundoubtedlyhelpful,simplyknowingthebasisofSPmaynotbeenoughtoalleviateterroranddistressassociatedwiththeexperiences,anddisruptiontechniquesareclearlywarranted.A25-year-oldmanfromtheUnitedStatesreports:“Thishappenssometimeseverynight,sometimesonlyonceeveryfewweeks.EventhoughI'know'whatishappening,andthatIaminnodanger,itisalwaysterrifying”.ThefirststudytosystematicallyassesspreventionstrategiesforSPbySharplessandGrom(2014)hassuggestedthatwhilenofoolproofmethodforpreventingSPisyetknown,somestrategies,suchasavoidingsleepingonone’sback(supineposition),maintainingoptimalsleephygiene(avoidingstimulants,noise,irregularsleeppatternsandanythingthatcontributestosleepfragmentation),andpre-sleeprelaxationpracticesmayhelpinpreventingSP.
Anumberofculture-specificpreventativeritualisticmeasurestopreventSPexist.Theseincludeplacingavarietyofdefensiveobjectsintheroomorinthebedbeforegoingtosleep,suchasavarietyofknives(Hufford,1982,Law&Kirmayer,2005);sprinklingsalt(acommonanti-witchremedy)(Roberts,1998);puttingabroombottom-up(Paradis&Friedman,2005)orapileofsandatthebedroomdoor(Jalal,Romanelli&Hinton,2015);andmanyothers.PuttingaBibleintheroom(Hufford,1982)andsayingaprotectiveprayerbeforebedtimearealsothoughtofaseffectivedeterrents.Otherritualisticactions,designedtodeter,divertandchaseawayunwelcomesupernaturalvisitorswerealsodocumentedinavarietyofcontexts(Sharpless&Doghramji,2015).
Techniquesfordisruptingsleepparalysis
Whilepreventativemeasures,whetherculturallyembeddedoraimedatincreasedawarenessandpromotionofsleephygiene,maybeeffectiveinreducingthefrequencyofSPepisodes,manymethodsfordealingwithanongoingSPexperiencealsoexist.ConsideringthatmostSPexperiencesarecharacterizedby

16
fearandotherunpleasantsensations,itisnotsurprisingthatinonestudythemajorityofparticipantsreportedhavingattemptedtodisrupttheongoingSPexperience.Movingtheextremitiesandself-monitoring(raisingawareness,promotingcalm)maybehelpfulduringtheSPepisode(Sharpless&Grom,2014).Notallattemptsorallstrategiesareequallysuccessful,butitseemsthatattemptingmicromovements,insteadoftryingtogetuportoscream,aremosteffective.Culture-boundritualsincludesayingaprayer(Hufford,1982),makingasignofacrosswithone’stongue(Davies,2010),andaskingsomeonetophysicallyshaketheoppressedsleeper(LawandKirmayer,2005).
Observational/transformationalpractices
OnemayarguethatISPandluciddreamingarepolaropposites.However,theysharethesameunderlyingpsychophysiologyandseemtoinvolvesimilarmechanisms:botharedependentuponREMsleepmechanisms;botharecharacterizedbysimultaneouspresenceofthedreamstateandbythefeelingofbeingawake,includingactivationofhigherordermetacognitivefunctionsindicativeofsomedegreeofwakingthoughtprocesses(LaBerge,Levitan&Dement,1986;Voss,Holzmann,Tuin,&Hobson,2009;Dresleretal,2012;Filevichetal,2015);andinbothcasesmuscleatoniaispresent.Thecrucialdifferencebetweenthetwostatesisthequalityandthefocusofawarenessandmetacognition:inluciddreamingoneisawareoftheillusorynatureofthedreamscenario,whereasinSPthedreamerisoftenabsorbedbythevision,notalwaysfullyrealizingthatitisdreamlike,and,incaseoffearfulSP,istooabsorbedinthepanickystateofperceivedimminentdanger.
ThelinkbetweenSPandluciddreaminghasnotbeensystematicallyinvestigatedinempiricalresearch,buttwostudiesreportapositivecorrelationbetweenfrequencyofluciddreamingandSP(Denis&Poerio,2016;Solomonova,Nielsen&Stenstrom,2009),suggestingthattheREM-wakeintertwinedstate,characterizingSP,maybeatrait-likephenomenonpredisposingindividualstoSPontheonehand,andfacilitatinglucidityinREMsleepdreamsontheother.
TransformingSPintoapositiveexperience,suchasanOBEoraluciddream,orutilizingSPexperiencesasameansofcontemplativeinsightintoone’sownmind,maybecomeapracticeinitself,sincenotonlytechniquesfordisruptingandpreventingSPexistinthecontemporarydigitalculture,butalsotechniquesforinducingSP,withthehopethattheexperiencewillfunctionasaportaltoadesirablealteredstateofconsciousness(Hurd,2010).ThefollowingtworeportsillustratethetransformativepotentialofSP:
“IhavewokenupfromdreamingandfoundIcan’tmoveoropenmyeyes.Igetthefeelingoflemonadebubblinginmybody,especiallymyhead.Itisveryfrightening.ButsinceIhavebeenhavingOBE3sInowrelaxandgowiththeflowofsleepparalysisandsometimesIactuallyachieveanOBE”(40-year-oldman,Australia)“AtfirstIwasveryfrighteneduntilIfoundtheASPemailgroupandfoundthatIwasnottheonlyonebeing“visited”bythisbeingduringsleepparalysis.…WhenitfirststartedhappeningitwasmoreofanassaultandIhadtofightterriblytoescape.Butafteryears,IlearnedtoignoreandnowI’vebeentryingtocommunicatewiththepresence”.(40-year-oldman,USA)
3OBE=out-of-bodyexperience

17
Figure4.Predisposing,precipitatingfactorsandexperienceandoutcomeofsleepparalysisepisodes.
Furtherconsiderationsandfuturedirections
Intermsofpossibleavenuesfortreatment,sinceSPcanbeconceptualizedasaformofnightmareoccurringinamixedstateofconsciousness,nightmaretreatmenttechniquescouldbeusefulinapproachingSP.Currently,themostusedandrecommendedtechniquefortreatingchronicnightmaresistheImageryRehearsalTherapy(Krakowetal,1995;Krakow&Zadra,2006),whichconsistsof“rehearsing”andtransformingdysphoriconeiricimageryinasafecontext.ThismethodhasbeeneffectiveintreatingPTSD-relatednightmares(Krakowetal,2001;Germainetal,2004;Cooketal,2010;Casement&Swanson,2012),whichseemsparticularlyappropriateforintenseandtrauma-relatedSPexperiences.Similarly,treatmentofnightmaresbyluciddreamingisapromisingavenue(Zadra&Pihl,1997;Spoormaker&VanDenBout,2006;LaBerge,2009).ConsideringthatneurophysiologicallybothstatesarecharacterizedbyanoverlapbetweenREMsleepandwakefulness,andthatanumberoffolkapproachestreatingSPasaportaltoluciddreamsalreadyexist,masteringluciddreamingcouldbeaneffectiveapproachtotransformationofanongoingSPepisode.Suchastrategymayalsobehighlyeffectiveinde-stigmatizinganddesensitisingtheexperiencer,andespeciallyinincreasinghermasteryandagencyoverherspontaneousoneiricexperiences.
Contemplativepractices,suchasmeditationorpranayama(yogicbreathing)mayalsobeusefulindealingwithrecurringSPepisodes.ThereiscurrentlynoempiricalevidenceforcontemplativetechniquesandSPmanagement,withtheexceptionofacasestudybyJalal(2016),butanecdotalevidencefrompractitionersaswellasgrowingempiricalliteraturelinkingcontemplativepracticeswithstressmanagement,emotionregulation,andincreasedself-awareness,providegroundsforfutureresearch.
Recentyearshaveseenanimportantincreaseinempiricalstudiesontheeffectsofmeditationandmeditation-basedmindfulnessinterventions.Therearedocumentedbenefitsofcontemplativepracticeinclinicalpopulationsincludingpositiveeffectsinmooddisorderssuchasanxietyanddepression(Hoffmanetal,2010;Goyaletal,2014),socialanxiety(Goldin&Gross,2010),andPTSD(Kearneyetal,2013).Atleastfourkindsofmeditationarecurrentlyinvestigatedinrelationtomentalhealth:focusedattention,openmonitoring(Lutzetal,2008),self-transcendence(Travis&Shear,2010)andlovingkindnessmeditation(Hoffman,Grossman&Hinton,2011).Differentkindsofmeditationpracticesmayrecruitdifferentneuralnetworks(Foxetal,2016),andparticularpsychologicalandneuroplasticchanges,associatedwithmeditationpractice,likelydependonthekindanddurationofmeditationexperience(Lutzetal,2015).ThesedifferentkindsofcontemplativepracticemaybehelpfulintargetingdifferentkindsofrecurrentSPexperiences,promotingde-automatization(Kang,Gruber&Gray,2013):deconstructingpatternsofbehaviour/reactivity.

18
MeditationmaybeeffectiveinSPmanagementasawayofcultivatinganon-judgementalor‘non-sticky’observationalattitudetoarisingimagery,sensationsandemotions,andinlettingtheexperienceunfold.Inaddition,oneimportantfeatureofmostmindfulness-relatedpracticesisthefocusontheexperienceofthebody(Kerretal,2013),andsomeevidencesuggeststhatmeditationpracticemayimproveawarenessofone’sownbodystates(Solomonovaetal,2016)andincreaseintrospectiveaccuracyforsomaticexperience(Foxetal,2012).Breathingpractices,suchaspranayama,maybeparticularlyeffectiveintransformingSPasitishappeningduetothefactthatmanySPepisodesarecharacterisedbyafeelingofdisordered/insufficientbreathing.Arecentstudy(Seppäläetal,2014)reportedthatbreathingexerciseswereeffectiveindecreasingPTSDsymptomsinwarveterans.ThisimpliesthatpracticingtechniquesthatimproveawarenessofbodysensationsmaylowerthereactivitytoSPepisodes,thusloweringthedistressingqualityoftheexperience,andincreasingthepotentialfordisruptingortransformingSP.
Acknowledgements:
TheauthorwassupportedbySocialSciencesandHumanitiesResearchCouncil(SSHRC)ofCanadaandbyaJ.-A.DeSèvesSacre-CoeurHospitalFoundationdoctoralscholarship.ThanksareduetoToreNielsen,PhilippeStenstromandMichelleCarrfornumerousconversationsonsleepparalysisanditsinterpretation,andtothemembersoftheDreamandNightmareLaboratoryattheCenterforAdvancedResearchinSleepMedicine.AdditionalthanksareduetoDonDonderiandElenaFrantova,aswellastoallparticipantswhohaveconsentedtosharetheirexperienceswithus.SpecialthankstoBenjamenSamaha(artist)andtotheanonymousSPsuffererforgenerouslyofferingthenarrativeandthedrawingofasleepparalysisepisode.

19
References:Abrams,M.P.,Mulligan,A.D.,Carleton,R.N.,&Asmundson,G.J.G.(2008).Prevalenceandcorrelatesofsleep
paralysisinadultsreportingchildhoodsexualabuse.JournalofAnxietyDisorders,22(8),1535–1541.doi:10.1016/j.janxdis.2008.03.007
Adler,S.R.(2011).Sleepparalysis:Night-mares,nocebos,andthemind-bodyconnection.RutgersUniversityPress.
AmericanAcademyofSleepMedicine.(2014).Internationalclassificationofsleepdisorders—thirdedition(ICSD-3).Darien,Illinois.
AmericanPsychiatricAssociation.(2013).Diagnosticandstatisticalmanualofmentaldisorders(DSM-5).AmericanPsychiatricPub.
Ammaniti,M.,&Gallese,V.(2014).Thebirthofintersubjectivity:Psychodynamics,neurobiology,andtheself.WWNorton&Company.
Antelmi,E.,Ferri,R.,Iranzo,A.,Arnulf,I.,Dauvilliers,Y.,Bhatia,K.P.,…Plazzi,G.(2016).Fromstatedissociationtostatusdissociatus.SleepMedicineReviews,28,1–13.doi:10.1016/j.smrv.2015.07.003
Agargun,M.Y.,&Cartwright,R.(2003).REMsleep,dreamvariablesandsuicidalityindepressedpatients.PsychiatryResearch,119(1),33-39.
Arikawa,H.,Templer,D.I.,&Brown,R.(1999).Thestructureandcorrelatesofkanashibari.TheJournalof….Retrievedfromhttp://www.tandfonline.com/doi/abs/10.1080/00223989909599749
Belicki,K.(1992).Nightmarefrequencyversusnightmaredistress:relationstopsychopathologyandcognitivestyle.Journalofabnormalpsychology,101(3),592.
Belicki,K.,Gulko,N.,Ruzycki,K.,&Aristotle,J.(2003).Sixteenyearsofdreamsfollowingspousalbereavement.OMEGA-JournalofDeathandDying,47(2),93-106.
Bell,C.C.,Shakoor,B.,Thompson,B.,Dew,D.,Hughley,E.,Mays,R.,&Shorter-Gooden,K.(1984).Prevalenceofisolatedsleepparalysisinblacksubjects.JournaloftheNationalMedicalAssociation,76(5),501.
Blagrove,M.,Farmer,L.,&Williams,E.(2004).Therelationshipofnightmarefrequencyandnightmaredistresstowell-being.Journalofsleepresearch,13(2),129-136.
Bloom,J.D.,&Gelardin,R.D.(1983).UqamairineqandUqumanigianiq:EskimoSleepParalysis.TheCulture-BoundSyndromes,117–122.doi:10.1007/978-94-009-5251-5_10
Brugger,P.,Regard,M.,&Landis,T.(1996).UnilaterallyFelt"Presences":TheNeuropsychiatryofOne'sInvisibleDoppelganger.CognitiveandBehavioralNeurology,9(2),114-122.
Brugger,P.,Regard,M.,&Landis,T.(1997).Illusoryreduplicationofone'sownbody:phenomenologyandclassificationofautoscopicphenomena.CognitiveNeuropsychiatry,2(1),19-38.
Brugger,P.,Regard,M.,Landis,T.,&Oelz,O.(1999).HallucinatoryExperiencesinExtreme-AltitudeClimbers.CognitiveandBehavioralNeurology,12(1),67.Retrievedfromhttp://journals.lww.com/cogbehavneurol/Fulltext/1999/01000/Hallucinatory_Experiences_in_Extreme_Altitude.8.aspx
Buzzi,G.(2011).Falseawakeningsinlightofthedreamprotoconsciousnesstheory:astudyinluciddreamers.InternationalJournalofDreamResearch,4(2),110-116.
Casement,M.D.,&Swanson,L.M.(2012).Ameta-analysisofimageryrehearsalforpost-traumanightmares:effectsonnightmarefrequency,sleepquality,andposttraumaticstress.Clinicalpsychologyreview,32(6),566-574.
Cheyne,J.A.(2001).Theominousnuminous.Sensedpresenceand'other'hallucinations.JournalofConsciousnessStudies,8(5-6),133-150.
CheyneJA(2002)WaterlooUnusualSleepExperiencesQuestionnaire—VIIIa:Technicalreport.http://watarts.uwaterloo.ca/*acheyne/spdoc/Techreport.pdf.Accessed15July2016
Cheyne,J.A.(2005).Sleepparalysisepisodefrequencyandnumber,types,andstructureofassociatedhallucinations.JournalofSleepResearch,14(3),319–324.doi:10.1111/j.1365-2869.2005.00477.x
Cheyne,J.A.,&Girard,T.A.(2007).Paranoiddelusionsandthreateninghallucinations:Aprospectivestudyofsleepparalysisexperiences,16(4),959–974.doi:10.1016/j.concog.2007.01.002
Cheyne,J.A.,Rueffer,S.D.,&Newby-Clark,I.R.(1999).HypnagogicandHypnopompicHallucinationsduringSleepParalysis:NeurologicalandCulturalConstructionoftheNight-Mare.ConsciousnessandCognition,8(3),319–337.doi:10.1006/ccog.1999.0404
Cheyne,J.A.,&Pennycook,G.(2013).SleepParalysisPostepisodeDistressModelingPotentialEffectsofEpisodeCharacteristics,GeneralPsychologicalDistress,Beliefs,andCognitiveStyle.Clinical

20
PsychologicalScience,2167702612466656.Clark,A.,&Chalmers,D.(1998).Theextendedmind.analysis,58(1),7-19.Colombetti,G.(2013).Thefeelingbody:Affectivesciencemeetstheenactivemind.MITPress.Davies,O.(2010).TheNightmareExperience,SleepParalysis,andWitchcraftAccusations.Folklore,114(2),
181–203.doi:10.1080/0015587032000104211Cook,J.M.,Harb,G.C.,Gehrman,P.R.,Cary,M.S.,Gamble,G.M.,Forbes,D.,&Ross,R.J.(2010).Imagery
rehearsalforposttraumaticnightmares:arandomizedcontrolledtrial.Journaloftraumaticstress,23(5),553-563.
Denis,D.,French,C.C.,Rowe,R.,Zavos,H.M.S.,Nolan,P.M.,Parsons,M.J.,&Gregory,A.M.(2015).Atwinandmoleculargeneticsstudyofsleepparalysisandassociatedfactors.JournalofSleepResearch,n/a.doi:10.1111/jsr.12282
Denis,D.,&Poerio,G.L.(2016).Terrorandbliss?Commonalitiesanddistinctionsbetweensleepparalysis,luciddreaming,andtheirassociationswithwakinglifeexperiences.JournalofSleepResearch.
Dresler,M.,Wehrle,R.,Spoormaker,V.I.,Koch,S.P.,Holsboer,F.,Steiger,A.,...&Czisch,M.(2012).Neuralcorrelatesofdreamlucidityobtainedfromcontrastinglucidversusnon-lucidREMsleep:acombinedEEG/fMRIcasestudy.Sleep,35(7),1017-1020.
Farhall,J.,Greenwood,K.M.,&Jackson,H.J.(2007).Copingwithhallucinatedvoicesinschizophrenia:areviewofself-initiatedstrategiesandtherapeuticinterventions.ClinicalPsychologyReview,27(4),476-493.
Filevich,Elisa,MartinDresler,TimothyR.Brick,andSimoneKühn."Metacognitivemechanismsunderlyingluciddreaming."TheJournalofNeuroscience35,no.3(2015):1082-1088.
Fox,K.C.,Zakarauskas,P.,Dixon,M.,Ellamil,M.,Thompson,E.,&Christoff,K.(2012).Meditationexperiencepredictsintrospectiveaccuracy.PloSone,7(9),e45370.
Fox,K.C.,Nijeboer,S.,Solomonova,E.,Domhoff,G.W.,&Christoff,K.(2013).Dreamingasmindwandering:evidencefromfunctionalneuroimagingandfirst-personcontentreports.Frontiersinhumanneuroscience,7,412.
Fox,K.C.,Dixon,M.L.,Nijeboer,S.,Girn,M.,Floman,J.L.,Lifshitz,M.,...&Christoff,K.(2016).Functionalneuroanatomyofmeditation:Areviewandmeta-analysisof78functionalneuroimaginginvestigations.Neuroscience&BiobehavioralReviews,65,208-228.
Friedman,S.,&Paradis,C.(2002).PanicdisorderinAfrican-Americans:symptomatologyandisolatedsleepparalysis.Culture,medicineandpsychiatry,26(2),179-198.
Fukuda,K.(1993).Oneexplanatorybasisforthediscrepancyofreportedprevalencesofsleepparalysisamonghealthyrespondents.PerceptualandMotorSkills.Retrievedfromhttp://www.amsciepub.com/doi/pdf/10.2466/pms.1993.77.3.803
Fukuda,K.,Miyasita,A.,Inugami,M.,&Ishihara,K.(1987).Highprevalenceofisolatedsleepparalysis:KanashibariphenomenoninJapan.SLEEP.(PAGES)
Fukuda,K.,Ogilvie,R.D.,&Takeuchi,T.(2000).RecognitionofsleepparalysisamongnormaladultsinCanadaandinJapan.Psychiatryandclinicalneurosciences,54(3),292-293.
Gallagher,S.(2005).Howthebodyshapesthemind(pp.173-178).Oxford:ClarendonPress.Gordon,S.(2015).MedicalCondition,DemonorUndeadCorpse?SleepParalysisandtheNightmarein
MedievalEurope.SocialHistoryofMedicine,28(3),NaN–NaN.doi:10.1093/shm/hkv005Garfield,P.(1996).Dreamsandbereavement.InTraumaandDreams,Barrett,D.editor.Pp.186-211Germain,A.,Krakow,B.,Faucher,B.,Zadra,A.,Nielsen,T.,Hollifield,M.,...&Koss,M.(2004).Increased
MasteryElementsAssociatedWithImageryRehearsalTreatmentforNightmaresinSexualAssaultSurvivorsWithPTSD.Dreaming,14(4),195.
Germain,A.,Buysse,D.J.,&Nofzinger,E.(2008).Sleep-specificmechanismsunderlyingposttraumaticstressdisorder:integrativereviewandneurobiologicalhypotheses.Sleepmedicinereviews,12(3),185-195.
Germain,A.(2013).SleepdisturbancesasthehallmarkofPTSD:wherearewenow?.AmericanJournalofPsychiatry,170(4),372-382.
Goldin,P.R.,&Gross,J.J.(2010).Effectsofmindfulness-basedstressreduction(MBSR)onemotionregulationinsocialanxietydisorder.Emotion,10(1),83.
Golzari,S.E.,&Ghabili,K.(2013).Alcohol-mediatedsleepparalysis:theearliestknowndescription.SleepMedicine,14(3),298.
Gould,G.A.,Gugger,M.,Molloy,J.,Tsara,V.M.S.C.,Shapiro,C.M.,&Douglas,N.J.(1988).BreathingpatternandeyemovementdensityduringREMsleepinhumans.AmRevRespirDis,138(4),874-877.

21
Green,C.E.,&McCreery,C.(1994).Luciddreaming:theparadoxofconsciousnessduringsleep.PsychologyPress.
Hartmann,E.,&Kunzendorf,R.(2013).ThymophorinDreams,Poetry,ArtandMemory:EmotionTranslatedintoImageryasaBasicElementofHumanCreativity.Imagination,CognitionandPersonality,33(1),165-191.
Hinton,D.E.,Pich,V.,Chhean,D.,&Pollack,M.H.(2005a).‘Theghostpushesyoudown’:sleepparalysis-typepanicattacksinaKhmerrefugeepopulation.TransculturalPsychiatry,42(1),46–77.
Hinton,D.E.,Pich,V.,Chhean,D.,Pollack,M.H.,&McNally,R.J.(2005b).SleepparalysisamongCambodianrefugees:associationwithPTSDdiagnosisandseverity.DepressionandAnxiety,22(2),47-51.
Hishikawa,Y.,&Kaneko,Z.(1965).Electroencephalographicstudyonnarcolepsy.ElectroencephalographyandClinicalNeurophysiology,18(3),249-259.
Hobson,J.A.,Stickgold,R.,&Pace-Schott,E.F.(1998).TheneuropsychologyofREMsleepdreaming.Neuroreport,9(3),R1-R14.
HobsonJ.A.,Pace-SchottE.F.&StickgoldR.(2000)Dreamingandthebrain:Towardacognitiveneuroscienceofconsciousstates.BehavioralandBrainScience23(6):793–842;discussion904–1121
Hobson,A.(2004).Amodelformadness?.Nature,430(6995),21-21.Hofmann,S.G.,Sawyer,A.T.,Witt,A.A.,&Oh,D.(2010).Theeffectofmindfulness-basedtherapyonanxiety
anddepression:Ameta-analyticreview.Journalofconsultingandclinicalpsychology,78(2),169.Hofmann,S.G.,Grossman,P.,&Hinton,D.E.(2011).Loving-kindnessandcompassionmeditation:Potential
forpsychologicalinterventions.Clinicalpsychologyreview,31(7),1126-1132.Howell,M.J.(2012).Parasomnias:anupdatedreview.Neurotherapeutics :TheJournaloftheAmericanSociety
forExperimentalNeuroTherapeutics,9(4),753–775.doi:10.1007/s13311-012-0143-8Hsieh,S.-W.,Lai,C.-L.,Liu,C.-K.,Lan,S.-H.,&Hsu,C.-Y.(2010).Isolatedsleepparalysislinkedtoimpaired
nocturnalsleepqualityandhealth-relatedqualityoflifeinChinese-Taiwanesepatientswithobstructivesleepapnea.QualityofLifeResearch :AnInternationalJournalofQualityofLifeAspectsofTreatment,CareandRehabilitation,19(9),1265–1272.doi:10.1007/s11136-010-9695-4
Hufford,D.(1989).Theterrorthatcomesinthenight:Anexperience-centeredstudyofsupernaturalassaulttraditions(Vol.7).UniversityofPennsylvaniaPress.
Hufford,D.J.(2005).Sleepparalysisasspiritualexperience.TransculturalPsychiatry,42(1),11–45.Hurd,R.(2010).SleepParalysis:AGuidetoHypnagogicVisionsandVisitorsoftheNight.HyenaPress.Goyal,M.,Singh,S.,Sibinga,E.M.,Gould,N.F.,Rowland-Seymour,A.,Sharma,R.,...&Ranasinghe,P.D.(2014).
Meditationprogramsforpsychologicalstressandwell-being:asystematicreviewandmeta-analysis.JAMAinternalmedicine,174(3),357-368.
Jalal,B.,&Ramachandran,V.S.(2014).Sleepparalysisand‘thebedroomintruder’:theroleoftherightsuperiorparietal,phantompainandbodyimageprojection.MedicalHypotheses,83(6),755–757.doi:10.1016/j.mehy.2014.10.002
Jalal,B.,Simons-Rudolph,J.,Jalal,B.,&Hinton,D.E.(2014).ExplanationsofsleepparalysisamongEgyptiancollegestudentsandthegeneralpopulationinEgyptandDenmark.TransculturalPsychiatry,51(2),158–175.doi:10.1177/1363461513503378
Jalal,B.,Romanelli,A.,&Hinton,D.E.(2015).CulturalExplanationsofSleepParalysisinItaly:ThePandafecheAttackandAssociatedSupernaturalBeliefs.Culture,Medicine,andPsychiatry,1–14.doi:10.1007/s11013-015-9442-y
Jalal,B.(2016).Howtomaketheghostsinmybedroomdisappear?Focused-attentionmeditationcombinedwithmusclerelaxation(MRtherapy)—adirecttreatmentinterventionforsleepparalysis.Frontiersinpsychology,7.
James,W.(1985).Thevarietiesofreligiousexperience(Vol.15).HarvardUniversityPress.Jiménez-Genchi,A.,Ávila-Rodríguez,V.M.,Sánchez-Rojas,F.,VargasTerrez,B.E.,&Nenclares-Portocarrero,
A.(2009).Sleepparalysisinadolescents:the‘adeadbodyclimbedontopofme’phenomenoninMexico.Psychiatryandclinicalneurosciences,63(4),546-549.
Kang,Y.,Gruber,J.,&Gray,J.R.(2013).Mindfulnessandde-automatization.Emotionreview,5(2),192-201.Kearney,D.J.,Malte,C.A.,McManus,C.,Martinez,M.E.,Felleman,B.,&Simpson,T.L.(2013).Loving-kindness
meditationforposttraumaticstressdisorder:Apilotstudy.JournalofTraumaticStress,26(4),426-434.Keen,C.,Murray,C.D.,&Payne,S.(2013).Aqualitativeexplorationofsensingthepresenceofthedeceased
followingbereavement.Mortality,18(4),339-357.Kerr,C.E.,Sacchet,M.D.,Lazar,S.W.,Moore,C.I.,&Jones,S.R.(2013).Mindfulnessstartswiththebody:

22
somatosensoryattentionandtop-downmodulationofcorticalalpharhythmsinmindfulnessmeditation.Frontiersinhumanneuroscience,7,12.
Kirmayer,L.J.(2009).Nightmares,neurophenomenologyandtheculturallogicoftrauma.Culture,medicineandpsychiatry,33(2),323-331.
Krakow,B.,Kellner,R.,Pathak,D.,&Lambert,L.(1995).Imageryrehearsaltreatmentforchronicnightmares.BehaviourResearchandTherapy,33(7),837-843.
Krakow,B.,&Zadra,A.(2006).Clinicalmanagementofchronicnightmares:imageryrehearsaltherapy.Behavioralsleepmedicine,4(1),45-70.
LaBerge,S.,Levitan,L.,&Dement,W.C.(1986).Luciddreaming:PhysiologicalcorrelatesofconsciousnessduringREMsleep.JournalofMindandBehavior.
LaBerge,S.(2009).Luciddreaming:Aconciseguidetoawakeninginyourdreamsandinyourlife.ReadHowYouWant.com.
Law,S.,&Kirmayer,L.J.(2005).Inuitinterpretationsofsleepparalysis.Transculturalpsychiatry,42(1),93-112.
Levin,R.,&Fireman,G.(2002).Nightmareprevalence,nightmaredistress,andself-reportedpsychologicaldisturbance.SLEEP-NEWYORK-,25(2),205-212.
Levin,R.,&Nielsen,T.A.(2007).Disturbeddreaming,posttraumaticstressdisorder,andaffectdistress:areviewandneurocognitivemodel.Psychologicalbulletin,133(3),482.
Liddon,S.C.(1967).Sleepparalysisandhypnagogichallucinations:Theirrelationshiptothenightmare.ArchivesofGeneralPsychiatry,17(1),88.
Liskova,M.,Janeckova,D.,KluzovaKracmarova,L.,Mlada,K.,&Buskova,J.(2016).Theoccurrenceandpredictivefactorsofsleepparalysisinuniversitystudents.NeuropsychiatrDisTreat,12,2957-2962.doi:10.2147/NDT.S115629
Luhrmann,T.M.(2012).WhenGodtalksback:UnderstandingtheAmericanevangelicalrelationshipwithGod.Vintage.
Lutz,A.,Slagter,H.A.,Dunne,J.D.,&Davidson,R.J.(2008).Attentionregulationandmonitoringinmeditation.Trendsincognitivesciences,12(4),163-169.
Lutz,A.,Jha,A.P.,Dunne,J.D.,&Saron,C.D.(2015).Investigatingthephenomenologicalmatrixofmindfulness-relatedpracticesfromaneurocognitiveperspective.AmericanPsychologist,70(7),632.
Mamelak,M.,Black,J.,Montplaisir,J.,&Ristanovic,R.(2004).Apilotstudyontheeffectsofsodiumoxybateonsleeparchitectureanddaytimealertnessinnarcolepsy.Sleep,27,1327-1336.
Mahowald,M.W.,&Schenck,C.H.(1991).Statusdissociatus:Aperspectiveonstatesofbeing.SLEEP.Retrievedfromhttp://psycnet.apa.org/psycinfo/1991-30903-001
Mahowald,M.W.,&Schenck,C.H.(2005).Insightsfromstudyinghumansleepdisorders.Nature,437(7063),1279-1285.
Maclaren,K.(2008).Embodiedperceptionsofothersasaconditionofselfhood?.JournalofConsciousnessStudies,15(8),63-93.
Maquet,P.(2000).Functionalneuroimagingofnormalhumansleepbypositronemissiontomography.Journalofsleepresearch,9(3),207-232.
McNally,R.(2011).Explaining‘Memories’ofSpaceAlienAbductionandPastLives:AnExperimentalPsychopathologyApproach.JournalofExperimentalPsychopathology.doi:10.5127/jep.017811
McNally,R.J.,&Clancy,S.A.(2005a).Sleepparalysisinadultsreportingrepressed,recovered,orcontinuousmemoriesofchildhoodsexualabuse.JournalofAnxietyDisorders,19(5),595–602.doi:10.1016/j.janxdis.2004.05.003
McNally,R.J.,&Clancy,S.A.(2005b).Sleepparalysis,sexualabuse,andspacealienabduction.TransculturalPsychiatry,42(1),113–122.
McNamara,P.,Andresen,J.,Clark,J.,Zborowski,M.,&Duffy,C.A.(2001).Impactofattachmentstylesondreamrecallanddreamcontent:atestoftheattachmenthypothesisofREMsleep.Journalofsleepresearch,10(2),117-127.
McNamara,P.,&Bulkeley,K.(2015).Dreamsasasourceofsupernaturalagentconcepts.FrontiersinPsychology,6,283.doi:10.3389/fpsyg.2015.00283
Mellman,T.A.,Bustamante,V.,Fins,A.I.,Pigeon,W.R.,&Nolan,B.(2002).REMsleepandtheearlydevelopmentofposttraumaticstressdisorder.AmericanJournalofPsychiatry,159(10),1696-1701.
Menary,R.(2010).Theextendedmind.Cambridge,MA:TheMITPress.MorrisD.(2010)Empiricalandphenomenologicalstudiesofembodiedcognition.In:GallagherS.&

23
SchmickingD.(eds.)Handbookofphenomenologyandcognitivescience.Springer,NewYork:235–252.Munezawa,T.,Kaneita,Y.,Osaki,Y.,Kanda,H.,Ohtsu,T.,Suzuki,H.,...Ohida,T.(2011).Nightmareandsleep
paralysisamongJapaneseadolescents:anationwiderepresentativesurvey.SleepMed,12(1),56-64.doi:10.1016/j.sleep.2010.04.015
Ness,R.C.(1983).TheOldHagPhenomenonasSleepParalysis:ABioculturalInterpretation.TheCulture-BoundSyndromes,123–145.doi:10.1007/978-94-009-5251-5_11
Nielsen,T.A.(2000).AreviewofmentationinREMandNREMsleep:“covert”REMsleepasapossiblereconciliationoftwoopposingmodels.BehavioralandBrainSciences,23(06),851-866.
Nielsen,T.,Stenstrom,P.,Takeuchi,T.,Saucier,S.,Lara-Carrasco,J.,Solomonova,E.,&Martel,E.(2005).PartialREM-sleepdeprivationincreasesthedream-likequalityofmentationfromREMsleepandsleeponset.Sleep28(9),1083.
Nielsen,T.(2007).Feltpresence:paranoiddelusionorhallucinatorysocialimagery?ConsciousnessandCognition,16(4),975.doi:10.1016/j.concog.2007.02.002
Nielsen,T.,&Levin,R.(2007).Nightmares:anewneurocognitivemodel.SleepMedicineReviews,11(4),295-310.
Nielsen,T.,&Paquette,T.(2007).Dream-associatedbehaviorsaffectingpregnantandpostpartumwomen.Sleep,30(9),1162.
Nielsen,T.,Svob,C.,&Kuiken,D.(2009).Dream-enactingbehaviorsinanormalpopulation.Sleep,32(12),1629-36.
Nielsen,T.A.,Paquette,T.,Solomonova,E.,Lara-Carrasco,J.,Popova,A.,&Levrier,K.(2010).REMsleepcharacteristicsofnightmaresufferersbeforeandafterREMsleepdeprivation.Sleepmedicine,11(2),172-179.
Noë,A.(2004).Actioninperception.Cambridge,MA:TheMITpress.Nofzinger,E.A.,Schwartz,R.M.,Reynolds,C.F.,Thase,M.E.,Jennings,J.R.,Frank,E.,...&Kupfer,D.J.(1994).
AffectintensityandphasicREMsleepindepressedmenbeforeandaftertreatmentwithcognitive-behavioraltherapy.JournalofConsultingandClinicalPsychology,62(1),83.
O’Hanlon,J.,Murphy,M.,&DiBlasi,Z.(2011).ExperiencesofsleepparalysisinasampleofIrishuniversitystudents.IrishJournalofMedicalScience,180(4),917–919.doi:10.1007/s11845-011-0732-2
Ohayon,M.M.,Zulley,J.,Guilleminault,C.,&Smirne,S.(1999).Prevalenceandpathologicassociationsofsleepparalysisinthegeneralpopulation.Neurology,52(6),1194–1200.doi:10.1212/WNL.52.6.1194
Olry,R.,&Haines,D.E.(2014).Kanashibari :aghost’sbusiness.JournaloftheHistoryoftheNeurosciences,23(2),192–197.doi:10.1080/0964704X.2013.862132
Otto,R.(1958).Theideaoftheholy(Vol.14).OxfordUniversityPress.Otto,M.W.,Simon,N.M.,Powers,M.,Hinton,D.,Zalta,A.K.,&Pollack,M.H.(2006).Ratesofisolatedsleep
paralysisinoutpatientswithanxietydisorders.JournalofAnxietyDisorders,20(5),687–693.doi:10.1016/j.janxdis.2005.07.002
Paradis,C.M.,&Friedman,S.(2005).SleepparalysisinAfricanAmericanswithpanicdisorder.Transculturalpsychiatry,42(1),123-134.
Peever,J.,Luppi,P.H.,&Montplaisir,J.(2014).BreakdowninREMsleepcircuitryunderliesREMsleepbehaviordisorder.Trendsinneurosciences,37(5),279-288.
Petitmengin,C.(2006).Describingone’ssubjectiveexperienceinthesecondperson:Aninterviewmethodforthescienceofconsciousness.PhenomenologyandtheCognitiveSciences,5(3-4),229-269.
Petitmengin,C.,&Lachaux,J.P.(2013).Microcognitivescience:bridgingexperientialandneuronalmicrodynamics.Frontiersinhumanneuroscience,7,617.
Pessoa,L.(2013).Thecognitive-emotionalbrain:Frominteractionstointegration.MITpress.Plante,D.T.,&Winkelman,J.W.(2008).Parasomnias:PsychiatricConsiderations.SleepMedicineClinics,3(2),
217–229.doi:10.1016/j.jsmc.2008.01.005PortocarreroA(2009):Sleepparalysisinadolescents:The"adeadbodyclimbedontopofme”phenomenon
inMexico.PsychiatryandClinicalNeurosciences63:546-549.Protevi,J.(2012).OneMore‘NextStep’:DeleuzeandBrain,BodyandAffectinContemporaryCognitive
Science.RevisitingNormativitywithDeleuze,25.RechtschaffenA.(1978)Thesingle-mindednessandisolationofdreams.Sleep1:97–109Revonsuo,A.(2006).Innerpresence:Consciousnessasabiologicalphenomenon.MitPress.Revonsuo,A.,Tuominen,J.,Valli,K.,Dresler,M.,Metzinger,T.&Windt,J.M."TheAvatarsintheMachine."Open
MIND.Frankfurta.M.,GER:MINDGroup(2015).

24
Roehrs,T.,&Roth,T.(2001).Sleep,sleepiness,sleepdisordersandalcoholuseandabuse.Sleepmedicinereviews,5(4),287-297.
Robert,G.,&Zadra,A.(2014).Thematicandcontentanalysisofidiopathicnightmaresandbaddreams.Sleep,37(2),409-417
Roberts,K.(1998).Contemporarycauchemar:Experience,belief,prevention.LouisianaFolkloreMiscellany,13,15-26.
Seppälä,E.M.,Nitschke,J.B.,Tudorascu,D.L.,Hayes,A.,Goldstein,M.R.,Nguyen,D.T.,...&Davidson,R.J.(2014).Breathing-basedmeditationdecreasesposttraumaticstressdisordersymptomsinUSMilitaryveterans:Arandomizedcontrolledlongitudinalstudy.Journaloftraumaticstress,27(4),397-405.
Sharpless,B.A.,McCarthy,K.S.,Chambless,D.L.,Milrod,B.L.,Khalsa,S.-R.,&Barber,J.P.(2010).,66(12),1292–1306.doi:10.1002/jclp.20724
Sharpless,B.A.,&Barber,J.P.(2011).Lifetimeprevalenceratesofsleepparalysis:asystematicreview.SleepMedicineReviews,15(5),311–315.doi:10.1016/j.smrv.2011.01.007
Sharpless,B.A.,&Grom,J.L.(2014).IsolatedSleepParalysis:Fear,Prevention,andDisruption.BehavioralSleepMedicine,1–6.doi:10.1080/15402002.2014.963583
Sharpless,B.,&Doghramji,K.(2015).Sleepparalysis:Historical,psychological,andmedicalperspectives.OxfordUniversityPress.
Simard,V.,&Nielsen,T.A.(2005).Sleepparalysis-associatedsensedpresenceasapossiblemanifestationofsocialanxiety.Dreaming,15(4),245.
Simon-Buller,S.,Christopherson,V.A.,&Jones,R.A.(1989).Correlatesofsensingthepresenceofadeceasedspouse.OMEGA-JournalofDeathandDying,19(1),21-30.
Solomonova,E.,Nielsen,T.,Stenstrom,P.,Simard,V.,Frantova,E.,&Donderi,D.(2008).Sensedpresenceasacorrelateofsleepparalysisdistress,socialanxietyandwakingstatesocialimagery.ConsciousnessandCognition,17(1),49–63.doi:10.1016/j.concog.2007.04.007
Solomonova,E.,Nielsen,T.,&Stenstrom,P.(2009).Luciddreamingisassociatedwithsleepparalysisbutnotnightmares.ThirdAnnualConferenceoftheCanadianSleepSociety.April26-28,Toronto,Canada
Solomonova,E.,Frantova,E.,&Nielsen,T.(2010).Feltpresence:theuncannyencounterswiththenuminousOther.AI&SOCIETY,26(2),171–178.doi:10.1007/s00146-010-0299-x
Solomonova,E.,Nielsen,T.,Takeuchi,T.Bezinger,E.&Carr,M.(2012).TherelationshipbetweenREMsleepeyemovementdensityanddreamcontent:differencesbetweenidiopathicsleepparalysissufferersandhealthycontrols.InternationalAssociationfortheStudyofDreamsannualmeeting.June24,2012.Berkeley,CA.
Solomonova,E.,Stenstrom,P.,Paquette,T.,&Nielsen,T.(2015).Differenttemporalpatternsofmemoryincorporationsintodreamsforlaboratoryandvirtualrealityexperiences:relationtodreamedlocusofcontrol.Internationaljournalofdreamresearch,8(1),10-26.
Solomonova,E.&Sha,X.W.(2016).Exploringthedepthofdreamexperience:Theenactiveframeworkandmethodsforneurophenomenologicalresearch.ConstructivistFoundations.SpecialIssue:ExploringtheDiversitywithinEnactivismandNeurophenomenology.TomFroese,AlexanderRieglerandSebastianVoros,editors.11(2),407-416.
Solomonova,E.,Dubé,S.,Blanchette-Carrière,C.,Samson,A.,Picard-Deland,C.&Nielsen,T.(2016).EffectofVipassanameditationonsleep-dependentproceduralmemoryconsolidationandposturalbalancefollowingadaytimenap:Makingimplicitmemoriesexplicit.MindandLifeSummerResearchInstitute,June2016,Garrison,NY,USA.
Spanos,N.P.,McNulty,S.A.,DuBreuil,S.C.,Pires,M.,&Burgess,M.F.(1995).Thefrequencyandcorrelatesofsleepparalysisinauniversitysample.JournalofResearchinPersonality,29(3),285-305.
Spoormaker,V.I.,&VanDenBout,J.(2006).Luciddreamingtreatmentfornightmares:apilotstudy.Psychotherapyandpsychosomatics,75(6),389-394.
Spoormaker,V.I.,&Montgomery,P.(2008).Disturbedsleepinpost-traumaticstressdisorder:secondarysymptomorcorefeature?.Sleepmedicinereviews,12(3),169-184.
Stewart,J.R.,Gapenne,O.,&DiPaolo,E.A.(2010).Enaction:Towardanewparadigmforcognitivescience.MITPress.
Suedfeld,P.,&Mocellin,J.S.(1987).The"SensedPresence"inUnusualEnvironmentsPeterSuedfeld.EnvironmentandBehavior,19(1),33-52.
Szelenberger,W.,Niemcewicz,S.,&Dabrowska,A.J.(2005).Sleepwalkingandnightterrors:psychopathologicalandpsychophysiologicalcorrelates.InternationalReviewofPsychiatry,17(4),263-

25
270.Szklo-Coxe,M.,Young,T.,Finn,L.,&Mignot,E.(2007).Depression:relationshipstosleepparalysisandother
sleepdisturbancesinacommunitysample.Journalofsleepresearch,16(3),297-312.Takeuchi,T.,Miyasita,A.,Sasaki,Y.,Inugami,M..(1992).Isolatedsleepparalysiselicitedbysleepinterruption.
SLEEP.(PAGES)Takeuchi,T.,Fukuda,K.,Sasaki,Y.,Inugami,M.,&Murphy,T.I.(2002).Factorsrelatedtotheoccurrenceof
isolatedsleepparalysiselicitedduringamulti-phasicsleep-wakeschedule.Sleep,25(1),89-96.Taylor,S.F.(2005).Betweentheideaandthereality:Astudyofthecounsellingexperiencesofbereaved
peoplewhosensethepresenceofthedeceased.CounsellingandPsychotherapyResearch,5(1),53-61.Terrillon,J.C.,&Marques-Bonham,S.(2001).Doesrecurrentisolatedsleepparalysisinvolvemorethan
cognitiveneurosciences.JournalofScientificExploration,15(1),97-123.Terzaghi,M.,Ratti,P.L.,Manni,F.,&Manni,R.(2012).Sleepparalysisinnarcolepsy:morethanjustamotor
dissociativephenomenon?NeurologicalSciences :OfficialJournaloftheItalianNeurologicalSocietyandoftheItalianSocietyofClinicalNeurophysiology,33(1),169–172.doi:10.1007/s10072-011-0644-y
Thompson,E.(2005).Sensorimotorsubjectivityandtheenactiveapproachtoexperience.Phenomenologyandthecognitivesciences,4(4),407-427.
Thompson,E.(2014).Waking,Dreaming,Being:SelfandConsciousnessinNeuroscience,Meditation,andPhilosophy.NewYork:ColumbiaUniversityPress.
ThompsonE.(2015a)Stepstowardaneurophenomenologyofconscioussleep.AReplytoJenniferM.Windt.In:MetzingerT.&WindtJ.M.(eds.)OpenMIND.MINDGroup,FrankfurtamMain:37(R).http://open-mind.net/papers/steps-toward-a-neurophenomenology-of-consciousness-in-sleep-a-reply-to-jennifer-m-windt
ThompsonE.(2015b)Dreamlesssleep,theembodiedmind,andconsciousness:TheRelevanceofaclassicalIndiandebatetocognitivescience.In:MetzingerT.&WindtJ.M.(eds.)OpenMIND.MINDGroup,FrankfurtamMain:37(T).http://open-mind.net/papers/dreamless-sleep-the-embodied-mind-and-consciousness-the-relevance-of-a-classical-indian-debate-to-cognitive-science
Thorpy,M.J.(2016).DiagnosticCriteriaandDelayinDiagnosisofNarcolepsy.InNarcolepsy(pp.45-49).SpringerInternationalPublishing.
Travis,F.,&Shear,J.(2010).Focusedattention,openmonitoringandautomaticself-transcending:categoriestoorganizemeditationsfromVedic,BuddhistandChinesetraditions.Consciousnessandcognition,19(4),1110-1118.
VarelaF.J.,ThompsonE.&RoschE.(1991)Theembodiedmind:Cognitivescienceandhumanexperience.MITPress,CambridgeMA.
Veissière,S.(2016).VarietiesofTulpaExperiences:TheHypnoticNatureofHumanSociality,Personhood,andInterphenomenality.InRazandLifshitz,eds.HypnosisandMeditationTowardsanIntegrativeScienceofConsciousPlanes.OxfordUniversityPress.
Wheeler,M.(2005).Reconstructingthecognitiveworld:Thenextstep.MITpress.Wing,Y.-K.,Chiu,H.,Leung,T.,&Ng,J.(1999).Sleepparalysisintheelderly.JournalofSleepResearch,8(2),
151–155.doi:10.1046/j.1365-2869.1999.00143.xWing,Y.-K.,Lee,S.T.,&Chen,C.-N.(1994).SleepparalysisinChinese:GhostoppressionphenomenoninHong
Kong.Sleep.Zadra,A.L.,&Pihl,R.O.(1997).Luciddreamingasatreatmentforrecurrentnightmares.Psychotherapyand
Psychosomatics,66(1),50-55.Zadra,A.,Pilon,M.,Joncas,S.,Rompré,S.,&Montplaisir,J.(2004).AnalysisofpostarousalEEGactivityduring
somnambulisticepisodes.Journalofsleepresearch,13(3),279-284.Zahavi,D.(2014).Selfandother:Exploringsubjectivity,empathy,andshame.OUPOxford.