Embed Size (px)
Citation preview

Paul P. Doghramji, MD, FAAFP
Family Practice Physician
Collegeville Family Practice & Pottstown Medical Specialists, Inc.
Medical Director of Health Services, Ursinus College – Collegeville, PA
Attending Family Practice Physician, Pottstown Memorial Medical Center – Pottstown, PA
Sleep Medicine for the Primary Care Provider

Learning Objectives
▪ Explain the sleep/wake cycle and circadian rhythms
▪ Review common sleep disorders in primary care
▪ Use appropriate diagnostic tools to assess patients’
sleep health
▪ Identify medications and/or treatment options used for
various sleep disorders

Agenda
▪ What is sleep?
▪ Sleep stages
▪ Sleep physiology
▪ Dreaming
▪ Sleepiness
▪ Sleep disorders
▪ Insomnia and comorbidities

Sleep Perspectives
▪ Behavioral
▪ Reversible
▪ Perceptual disengagement from, and unresponsiveness to, the environment
▪ Neurophysiological
▪ Two distinct states: REM sleep and NREM
▪ Actively produced, not a result of passive inactivity
▪ Highly regulated by homeostatic and circadian processes
▪ Produces changes in the entire organism, not just the CNS
▪ Teleological
▪ Necessary for survival; deprivation leads to functional impairments and eventual death
▪ Important for clearance of neurotoxic waste products (e.g., beta amyloid) that accumulate in
the brain during wakefulness
NREM = non-rapid eye movement
Carskadon MA, Dement WC (2005), Normal human sleep: an overview. In: Principles and Practice of Sleep Medicine, 4th ed., Kryger MH et al., eds. Philadelphia: Elsevier/Saunders, pp13-23. Science vol 342, 18 Oct 2013.

What Does Sleep Do?The 4R’s of Sleep:
▪ Rest
▪ Restore
▪ Repair
▪ Rejuvenate

3 PROPER-ties of Sleep
▪ Proper duration
▪ Proper timing
▪ Proper quality
▪ Improper duration and/or timing and/or quality can lead
to insufficient rest/restore/rejuvenate/repair -> poor
health and decreased longevity

Why is Sleep Important?
▪ Cognition and performance
▪ Mood regulation
▪ Mental health
▪ Physical health
▪ Safety


Sleep Stages
SLEEP REST

Two States of Sleep
Rapid eye movement (REM) sleep
▪ When dreaming occurs
▪ “Active brain in a paralyzed body”
Hours 1
N 1
& REM
N 2
N3
2 3 4 5 6 7 8
Non-REM sleep
▪ 3 stages
▪ Based primarily on EEG
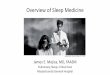
Typical Sleep Architectural Pattern of a Young Human Adult
Adapted from Hauri P. The Sleep Disorders. Kalamazoo, Mich: Upjohn;1982:8.
Stage I & REM sleep (red) are graphed on the same level because their EEG patterns are very similar

Sleep Architecture
▪ Sleep is entered through stage N1
▪ Orderly progression from stage N1 to N3 and, typically within 90
minutes of sleep onset, to the 1st REM period
▪ 90-minute cycle of REM-NREM repeats throughout sleep
▪ As the night progresses
▪ REM periods increase in duration and density of eye movements
▪ N3 sleep becomes less prominent in the 2nd half of the night

Sleep Stage Characteristics
NREM REM
Heart rate Steady Variable
Blood pressure Steady Labile
Respirations Regular Irregular
Skeletal muscle tone Normal Decreased
Thermoregulation Waking modes Decreased
Penile tumescence Infrequent Frequent
Mental activity Limited Dreaming
Brain O2 consumption Decreased Waking level
Lee-Chiong T, ed. Sleep: A Comprehensive Handbook. Hoboken, NJ: Wiley & Sons; 2006.

Sleep Across the Life Span
0
100
200
300
400
500
600
700
Tota
l Sle
ep T
ime
(min
)
Age (years)
Total Time in Bed
Awake in Bed
NREM N 1
REM
NREM N 2
NREM N 3
10 20 30 40 50 60 70 8050
Adapted from Williams RL, et al. Electroencephalography of Human Sleep: Clinical Applications. New York, NY: John Wiley & Sons; 1974.


Sleep Physiology

Brainstem Mechanisms Underlying Sleep and Arousal
Adapted from Saper CB, et al. Nature. 2005 Oct 27; 437(7063):1257-63.
Ascending
Arousal SystemSleep and
Arousal Centers

Orexin = Hypocretin
▪ Hypothalamic peptides (OX1 and OX2)
▪ Localized in the dorsolateral hypothalamus
▪ Wide projections throughout brain and spinal column
▪ Peptide neurotransmitters involved in
▪ Arousal
▪ Locomotion
▪ Metabolism (energy and appetite control)
▪ Increase blood pressure & heart rate
Peyron et al. J Neurosci. 1998;18:9996. Moore et al. Arch Ital Biol. 2001;139:195. Silber & Rye. Neurology. 2001;56:1616.

Flip Flop Switch Model of Arousal and Sleep
Modified from Saper CB, et al. Nature. 2005;437(7063):1257-1263.

Dreaming

When Do We Dream?
▪ Dreaming occurs in all stages of sleep
▪ 80% of persons who are awakened during REM sleep and
sleep onset (N1 & N2)
▪ 40% of persons who are awakened from a deep sleep

Foulkes D. Dreaming: a cognitive-psychological analysis. Hillsdale, N.J.: Erlbaum, 1985.
N1 & N2 N3 REM
Simpler, shorter
and have fewer
associations
than REM sleep
dreams
More diffuse
(e.g., about a
color or an
emotion)
Tend to be
bizarre and
detailed, with
storyline plot
associations
Highest recall during sleep stages with EEG patterns
most like those in the waking state
D
R
E
A
M
S
REM and Non-REM Dreams

Frightening Dreams
TYPE OF
DREAMINCIDENCE SYMPTOMS SLEEP STAGE
ASSOCIATED
FACTORSFrequent
nightmares in
children
20% to 30%,
declines with age
Frightening, detailed plots
Difficult return to sleep
REM sleep, usually
late in sleep (4 - 6
a.m.)
Usually no pathology
Frequent
nightmares in
adults
5% to 8%
Increased awakenings
Daytime memory
impairment and anxiety
REM sleep
“Thin-boundary” / creative
personality
May have associated
psychopathology
PTSD
8% - 68% of
veterans
>25% of trauma
victims
Stereotypic dreams of the
trauma
Intense rage, fear, grief
REM sleep and sleep
onset
Significant trauma
Daytime hyper-
arousability & anxiety
REM sleep
behavior
disorder
Most common in
late middle age and
in men
Acting out of dreams
Nocturnal injuries
REM sleep
REM EMG tone
Degenerative neurologic
illness in 50%
Night terrors
1% to 4% of
children
Declines with age
Rare in adults
Blood-curdling screams
Autonomic discharge
Limited recall
Deep sleep, early
(1- 3 a.m.)
Stages 3 & 4
arousals on PSG
No pathology in children
Psychiatric & neurologic
disorders in adults
PAGEL JF, Nightmares and Disorders of Dreaming. Am Fam Physician. 2000 Apr 1;61(7):2037-2042.
REM = rapid eye movement; EMG = electromyography

Sleepiness

Sleepiness: How Do Patients Describe It?
▪ “I’m tired all the time”
▪ “I have no energy”
▪ “I feel fatigued”
▪ “I feel depressed”
▪ “I don’t feel rested”
▪ “I don’t sleep well”
The International Classification of Sleep Disorders: Diagnostic and Coding Manual. 2nd ed. Westchester, IL: American Academy of Sleep Medicine; 2005.
Chervin RD. Chest 2000;118:372-379. Shen J, et al. Sleep Med Rev 2006;10:63-76.

Patients Also Mean Other Things“TIRED”
Sleepiness FatigueLack of
motivation
Tendency to fall
asleep or inability
to stay awake
Sensation of
weariness,
tiredness,
exhaustion,
loss of energy;
the desire to rest
“I don’t feel like
doing anything…”
Improved by sleep Improved by rest,
exertion makes it
worse

Sleepiness in America
37%
16%
0%
10%
20%
30%
40%
At least a few days per month At least a few days per week
% of US Adults Reporting that They Are So Sleepyit Interferes with Their Daily Activities
National Sleep Foundation. “Sleep in America” Poll. March 2002.

Assessment Options: Sleep Parameters
▪ Subjective: based on self-report
▪Epworth
▪ Insomnia Severity Scale
▪Diaries
▪Often do not reflect objective sleep measures
▪ Objective: Sleep lab or home sleep monitor
▪ Wearable technology (eg, Fitbit) increasingly capable of more
objective sleep assessment: eg, total sleep time, slow wave sleep,
REM sleep
▪Not reimbursable, not validated in clinical practice

Epworth Sleepiness Scale
Johns MW. Sleep. 1991;14:540-545.
Rate the chances of dozing in sedentary situations
Never Slight Moderate High
Sitting and reading 0 1 2 3
Watching television 0 1 2 3
Sitting, inactive in a public place (eg, a movie theater or a meeting)
0 1 2 3
As a passenger in a car for an hour without a break
0 1 2 3
Lying down to rest in the afternoon when circumstances permit
0 1 2 3
Sitting and talking to someone 0 1 2 3
Sitting quietly after lunch without alcohol
0 1 2 3
In a car, while stopped for a few minutes in the traffic
0 1 2 3
Score >=10 Prompts Further Evaluation

US women 20.8%,US men 29.7%2
South Africa1 24.5%
Japan1 12.4%
China1 6.2%
Austria1 17.5%
Belgium1 17.5%
Brazil1 14.3%
Germany1 7.2%
Portugal1 18.3%
Slovakia1 13.7%
Spain1 12.7%
Norway3 17.7%
N=35,327 survey respondents aged 39 ± 15.3 years.1
ESS, Epworth Sleepiness Scale
1. Soldatos CR, et al. Sleep Med. 2005;6:5-13; 2. Baldwin CM, et al. Sleep. 2004;27:305-311; 3. Pallesen S, et al. Sleep. 2007;30:619-624.
Worldwide Prevalence of ESS Scores >10

Categories of Sleepiness
▪ Insufficient sleep
▪ Factitious
▪ Insomnia
▪ Poor quality sleep
▪ Obstructive sleep apnea
▪ Restless Legs Syndrome
▪ Disturbed timing of sleep
▪ Circadian rhythm disorders
▪ Medications and substances
▪ Rx, OTC, herbals
▪ Illicit drugs, alcohol
▪ Brain “damage”
▪ MS, Parkinson’s, TBI, stroke,
Alzheimer's
▪ Narcolepsy

Sleep Disorders

Restless Legs Syndrome6
10%-15%
Comorbid Insomnias4
6%
Narcolepsy5
0.06%†
Obstructive Sleep Apnea1
3%-28%
Sleep-Wake Disorders: Prevalence in Adults
*Among night and rotating shift workers; †Prevalence of hypersomnias such as narcolepsy without cataplexy may be higher.
1. Young T, et al. Am J Respir Crit Care Med. 2002;165:1217-1239. 4. Ohayon MM. Sleep Med Rev. 2002;6:97-111.2. Drake CL, et al. Sleep. 2004;27:1453-1462. 5. Silber MH, et al. Sleep. 2002;25:197-202.3. Strine DP, et al. Sleep Med. 2005;6:23-27. 6. Merlino G et al. Neurol Sci. 2007;28:S37-S46. †Mignot E, et al. Brain. 2006;129:1609-1623. †Singh M, et al. Sleep. 2006;29:890-895.
Shift Work Disorder2
8%-32%* Insufficient Sleep
Syndrome3
26%

How to Diagnose the Cause of Sleepiness
▪ Get detailed sleep/wake history
▪ Determine whether sleepy, fatigue, or depression
▪ Quantify degree of sleepiness: ESS
▪ Start probing for the causes, looking for clues
▪ Insufficient Sleep Syndrome: doesn’t get enough sleep
▪ OSA: loud snoring, waking up choking, witnesses apneas, waking with sore throat,
headache, enuresis, nocturia
▪ RLS: uncomfortable feelings in legs prevent sleep, need to move them to relieve
symptoms
▪ PLMD: no clues except excessive sleepiness
▪ Narcolepsy: hypnogogic/hypnopompic hallucinations, sleep paralysis, cataplexy

Obstructive Sleep Apnea (OSA)
Symptoms
▪ Loud Snoring
▪ Gasping, choking
▪ Witnessed apneas
▪ Morning headaches, sore throat
▪ Enuresis/nocturia
Physical Findings
▪ Large neck
▪ Crowded pharynx
▪ Obesity
▪ Micrognathia, short chin
Treatment
▪ CPAP/BiPAP/Auto-AP
▪ Oral appliance
▪ Surgery
▪ Weight loss
▪ Positioning
▪ “Bongo” nasal valves
▪ “Inspire”

OSA is a Highly Prevalent Medical Condition1
▪ OSA prevalence varies based on patient demographics and definitions used for
respiratory events2
▪ US prevalence of moderate to severe OSA (AHI ≥15) is estimated at 10%4,b
▪ Prevalence in men (13.0%) is approximately twice that in women (5.6%)4
The Wisconsin Sleep Cohort estimates overall OSA (AHI ≥5) prevalence to be3,a
24%
in men
9%
in women
1. Franklin KA, Lindberg E. J Thor Dis. 2015;7(8):1311-1322. 2. American Academy of Sleep Medicine. International Classification of Sleep Disorders. 3rd
ed. Darien, IL: American Academy of Sleep Medicine; 2014. 3. Garvey JF et al. J Thorac Dis. 2015;7(5):920-929. 4. Peppard PE et al. Am J Epidemiol.
2013;177(9):1006-1014.
AHI=apnea-hypopnea indexaAges 30-60 years3
bAges 30-70 years4

Predisposing Conditions
▪ Age (40 to 70 years)
▪ Commercial motor vehicle driver
▪ Family history of obstructive sleep apnea
▪ Male sex
▪ Obesity (body mass index > 35 kg per m2)
▪ Postmenopausal woman not taking hormone therapy
▪ Preoperative for bariatric surgery
▪ Retrognathia
Semelka M, et.al. Am Fam Physician. 2016 Sep 1;94(5):355-360.

OSA is Associated with Negative Health Consequences
1. Somers VK et al. Circulation. 2008;118(10):1080-1111. 2. American Academy of Sleep Medicine. International Classification of Sleep Disorders. 3rd ed.
Darien, IL: American Academy of Sleep Medicine; 2014. 3. White DP. Am J Respir Crit Care Med. 2005;172(11):1363-1370. 4. Knauert M et al. World J
Otorhinolaryngol Head Neck Surg. 2015;1(1):17-27. 5. Dempsey JA et al. Physiol Rev. 2010; 90((1):47-112. 6. Lal C et al. Chest. 2012;141(6):1601-1610.
7. Semelka M, et.al. Am Fam Physician. 2016 Sep 1;94(5):355-360.
Systemic Inflammation
Airway opens & reoxygenation1,3
Reduced pharyngeal muscle tone2
Sleep onset1
Arousalfrom sleep1,3
Increasedpharyngeal
muscle tone1,3
Airway narrowingor collapse;reduction in airflow2
Increasedventilatory effort1,3
Hypoxemia &hypercapnia1,3
IntermittentHypoxemia
Stroke Hypertension
Diabetes
Depression OSA can lead to significant health
consequences, including4,5,6 7:
Neurocognitive impairment
SleepFragmentation
CAD
AtrialFibrillation
CHF

Prevalence of OSA in Co-morbidities
Schafer et al.
Cardiology 1999
83%
76%
37%
48%Diabetes
Obesity
All Hypertension
Atrial Fibrillation
Congestive HeartFailure
Drug-ResistantHypertension
49%
77%
Coronary Artery Disease
59%Pacemakers
Sjostrom et al.
Thorax 2002
Logan et al.
J Hypertens 2001
Oldenburg et al.
Eur J Heart Fail 2007
O'Keeffe & Patterson.
Obes Surg 2004
Einhorn et al.
Endocr Pract 2007
Gami et al.
Circulation 2004
Garrigue et al.
Circulation 2007
30%
74%

Benefits of CPAP Treatment
▪ In patients with obstructive sleep apnea, continuous positive airway pressure (CPAP)…
▪ Lowers blood pressure
▪ Reduces rates of arrhythmia and stroke
▪ Improves left ventricular ejection fraction in patients with heart failure
▪ Reduces fatal and nonfatal cardiovascular events
▪ A recent meta-analysis demonstrated similar rates of blood pressure lowering between continuous positive airway pressure and mandibular advancement devices
Semelka M, et.al. Diagnosis and Treatment of Obstructive Sleep Apnea in Adults. Am Fam Physician. 2016 Sep 1;94(5):355-360.

Screening for OSA: STOP-BANG Method
STOP Questionnaire*
▪ Snoring
▪ Tiredness (daytime)
▪ Observed you stop
breathing during sleep
▪ High blood Pressure
BANG†
▪ BMI > 35
▪ Age > 50 years
▪ Neck circumference
> 40 cm (~ 16 in)
▪ Gender: Male
* High risk = Yes to > 2 of 4 STOP items
† High risk = Yes to > 3 of 8 STOP-BANG items
Chung F, et al. Anesthesiology 2008;108:812-821.

OSA is Measured by:
▪ Apnea/Hypopnea Index (AHI), the average number of apnea/hypopneas per hour
▪ Apnea: cessation of airflow for at least 10 sec
▪ Hypopnea: partial obstruction that is either severe enough, and/or causes desaturation, and/or arousal
▪ AHI
▪ 5-15: mild OSA
▪ 16-30: moderate OSA
▪ >30 severe OSA

Airway Assessment: OSA Mallampati Scale
Nuckton TJ, et al. Sleep. 2006;29:903-908.
Odds of OSA increase >2-fold for every 1-point increase
Class I Class II Class III Class IV

Testing for OSA
▪ Overnight polysomnogram is gold standard
▪ Split night acceptable for those with AHI >20 in first few hours
▪ Home sleep study
▪ More accurate in identifying patients with a higher pretest probability of OSA and can rule out OSA in low-risk patients
▪ Not recommended in patients with comorbidities
▪ Less expensive
▪ More patient friendly
Semelka M, et.al. Am Fam Physician. 2016 Sep 1;94(5):355-360.

Excessive Daytime Sleepiness (EDS) is Common in Patients with OSA
▪ In a multicenter trial using the MSLT,a
among 136 patients with OSA (AHI
≥15) across 7 sleep clinics before
CPAP treatment1:
▪ 62.5% (n=85) of patients had ES (mean
sleep latency <7.5 min)
▪ Prevalence estimates of objective
EDS in OSA may vary with differences
in thresholds used across studies
>60%had objective EDSb prior to
CPAP treatment2
bMean MLST sleep latency <7.5 min.
Evaluated in 136 OSA patients (AHI ≥15) across 7 sleep clinics.
MSLT=Multiple Sleep Latency TestaThe MSLT is a laboratory-based, objective tool that uses mean sleep latency (eg, time from lights out to first epoch of sleep) and number of sleep-
onset REM periods to characterize the patient’s ability to fall asleep.1,2
1. Weaver TE et al. Sleep. 2007;30(6):711-719. 2. Littner MR, et al. Sleep. 2005;28(1):113-121.

Excessive Daytime Sleepiness May Persist Despite ≥6 Hours CPAP Use per Night1-3
▪ EDS is among the most frequently reported
complaints in patients with OSA4
▪ In a multicenter trial (n=128 patients with AHI
≥15) patients with OSA were treated with
CPAP for 3 months and assessed for
sleepiness before and after airway treatment
using2:
▪ Self-reported ESS and FOSQ
▪ Clinically-derived MSLT
FOSQ=Functional Outcomes of Sleep Questionnaire
1. Qaseem A et al. Ann Intern Med. 2013;159(7):471-483. 2. Weaver TE et al. Sleep. 2007;30(6):711-719. 3. Antic N et al. Sleep. 2011;34(1):111-119.
4. American Academy of Sleep Medicine. International Classification of Sleep Disorders. 3rd ed. Darien, IL: American Academy of Sleep Medicine; 2014.
aEvaluated in patients with pre- and post-treatment
assessments who had abnormal pretreatment values2
bSubjective EDS defined as ESS (>10)2
cObjective EDS according to MSLT sleep latency <7.5 min2
dFunctional impairment defined as FOSQ <17.92
For patients reporting ≥6 hours of CPAP use per night,
based on MSLT (n=23), more than half of participants
continued to experience EDS2
0
10
20
30
40
50
60
ESS MSLT FOSQ
Percent Patients Failing to Achieve a Normal Score With ≥6 h CPAP Use per
Night for 3 Months2,a
n=11/23 n=25/37n=28/36
% P
atie
nts
22b
52c
32d

Neurologic Regulation of Sleep/Wake Cycle
CNS=central nervous system
1. Schwartz JR, Roth T. Curr Neuropharmacol. 2008;6(4):367-378. 2. Slater G, Steier J. J Thorac Dis. 2012;4(6):608-616. 3. Saper CB et al. Nature.
2005;437(7063):1257-1263. 4. España RA, Scammell TE. Sleep. 2011;34(7):845-858.
ES may result from injury to neurons involved in
promoting wakefulness1,3,4
Increased Sleep Drive1,2
▪ Sleep disruption
▪ Insufficient sleep duration
▪ Comorbid sleep disorders
▪ Sedative hypnotics,
opiates
Inadequate Wake Drive1,2
▪ CNS disruption of
wake-promoting neurons
▪ Comorbid sleep-wake
disorders (eg, narcolepsy)

Emerging Research Suggests OSA May Cause Neuronal Injury and Brain Alterations Resulting in EDS
In Experimental Animal
Models of OSA
1. Zhu Y et al. Front Neurol. 2015;6:109. 2. Zhu Y et al. J Neurosci. 2007;27(37):10060-10071. 3. Joo EY et al. Sleep. 2010;33(2):235-241. 4. Lal C et al.
Chest. 2012;141(6):1601-1610. 5. Xiong Y et al. J Magn Reson Imaging. 2017;45(5):1371-1378. 6. Slater G, Steier J. J Thorac Dis. 2012;4(6):608-616.
Chronic intermittent hypoxia has been
associated with injury to certain wake-
promoting neurons (eg, noradrenergic,
dopaminergic)2
Chronic sleep fragmentation has been
associated with loss of certain wake-
promoting neurons (eg, noradrenergic,
orexigenic)1
In Patients With OSA
ES in patients adherent to CPAP was associated
with structural changes to white matter5:
▪ Potentially indicative of compromised neuronal connectivity
▪ Some structural changes correlated with clinical measures of EDS (ESS)
Diagnosis of EDS in OSA is based on a clinical assessment, which must be made by the treating physician after airway treatment is implemented and all other
causative disorders have been ruled out including other untreated sleep disorders, mental disorder, or the effects of medication.6
OSA was associated with reduced gray
matter volume in brain regions involved
in wakefulness and neurocognitive
performance compared with healthy
volunteers3,4

EDS in OSA May Lead to Involuntary Sleep Episodes
▪ Among 822 patients with newly diagnosed moderate to severe OSA,
43% (n=350) reported high levels of subjective EDS, including involuntary
sleep episodes1,b
aInvoluntary episodes of sleep can occur during walking, talking, and driving1; bIcelandic Sleep Apnea Cohort.
1. Ye L et al. Eur Respir J. 2014;44(6):1600-1607. 2. Weaver EM et al. Arch Otolaryngol Head Neck Surg. 2004;130(4):453-458.
Involuntary Sleep Episodesa Reported by Patients
With Moderate to Severe OSA1
n=350
Relaxing
(eg, watching TV)
99%
During the Day
65%
Driving
38%
Self-reported EDS does not
necessarily correlate with
polysomnographic measures
(eg, AHI), and can persist
despite improvement in the
AHI, the primary measure of
OSA severity2

Self-Report Measures Can Be Used in Clinical Practice
1. Miglis MG, Kushida CA. Sleep Med Clin. 2014;9(4):491-498. 2. Johns MW. Sleep. 1991;14(6):540-545. 3. Ahmed IM, Thorpy MJ. In: Sleepiness: Causes,
Consequences and Treatment. Cambridge, UK: Cambridge University Press; 2011:36-49. 4. Chapman JL et al. Sleep Med Clin. 2016;11(3):353-363. 5. Chasens
ER, Ratcliffe SJ et al. Sleep. 2009;32(7):915-919.
▪ The FOSQ (or shorter FOSQ-10)
assesses the effect of sleepiness on
daily functioning4,5
▪ Evaluates 5 domains4,5
1. General productivity
2. Activity level
3. Vigilance
4. Social outcomes
5. Intimate/sexual relationships
▪ The ESS is the most frequently used,
validated self-report assessment of a
patient’s sleepiness1
▪ On a 4-point scale, patients rate their
likelihood of falling asleep during
8 different situations (reading,
driving, etc)2
▪ The ESS can also be used to monitor
the progression of or improvement in
sleepiness over time3
Epworth Sleepiness Scale (ESS)Functional Outcomes of Sleep
Questionnaire (FOSQ)
▪ Subjective measures rely on patients to accurately report their own sleepiness, however, they are4
▪ Practical for monitoring progression or improvement in EDS
▪ Simple to administer

Objective Measures Can Be Used in a Laboratory Setting to Detect Excessive
Daytime Sleepiness and Other Sleep Disorders
1. Littner MR, et al. Sleep. 2005;28(1):113-121. 2. Weaver TE et al. Sleep. 2007; 30(6):711-719. 3. Chapman JL et al. Sleep Med Clin. 2016;11(3):353-363.
▪ Measures the ability to stay awake
using mean sleep latency
▪ Experimental measure useful for
detecting response to interventions
intended to maintain wakefulness
▪ Measures physiologic sleep tendencies
using latency to sleep
▪ Diagnostic test traditionally used to
assess narcolepsy and other sleep
disorders
Multiple Sleep Latency Test (MSLT)1 Maintenance of Wakefulness (MWT)1
▪ Objective measures may detect a greater percentage of patients with EDS than subjective patient
reporting2
▪ However, time and cost constraints make these tests impractical for routine use in monitoring EDS in OSA3

Management of EDS in OSA
Re-examine Treatment Objectives
▪ Adequate sleep duration and optimized airway therapy1
▪ First-line treatment of choice for OSA is typically CPAP
1. Santamaria J et al. Sleep Med Rev. 2007;11(3):195-207. 2. Provigil tablets [package insert]. North Wales, PA: Teva Pharmaceuticals USA, Inc; 2015.
3. Nuvigil tablets [package insert]. North Wales, PA: Teva Pharmaceuticals USA, Inc; 2017. 4. Iftikhar IH et al. Lung. 2014;192(1):175-184. 5. Aurora RN et
al. J Clin Sleep Med. 2015;11(3):357-383.
Rx
Reinforce Behavioral Interventions
▪ Weight management2,3
▪ Exercise2
▪ Cardiovascular fitness3
Consider Pharmacotherapies
▪ Wake-promoting agents (eg, modafinil, armodafinil, solriamfetol)4,5
▪ Indicated for EDS associated with narcolepsy and CPAP-adherent patients with OSA
▪ Modafinil and armodafinil also indicated for shift-work disorder

Restless Legs Syndrome

Movement disorder with sensory and motor components; Clinical diagnosis with 4 criteria
Rest or inactivity
precipitates or worsens
symptoms
Getting up or moving
improves the sensation
Evening or nighttime
appearance or worsening
of symptoms
Restless Legs Syndrome (RLS): Diagnostic Criteria
Allen RP, et al. Sleep Med. 2003;4:101-119.
Urge to move with
uncomfortable, unpleasant sensations
in legs
Supportive criteria: Family history, positive response to
dopaminergic therapy, and periodic limb movements in sleep

RLS: Most Common Presenting Complaints
▪ Insomnia: trouble getting to sleep, 88%
▪ Tiredness: drowsiness or daytime sleepiness, 90%

1. Gamaldo CE, Earley CJ. Chest. 2006;130(5):1596-1604. 2. Allen RP, et al. Arch Intern Med. 2005;165:1286-1292. 3. Allen RP, et al. Sleep Med.
2003;4:101-119. 4. Allen RP, Earley CJ. J Clin Neurophysiol. 2001;18:128-147. 5. Turjanski N, et al. Neurology. 1999;52:932-937.
Restless Legs Syndrome: Assessment and Diagnosis
▪ 7%-10% prevalence (US, northern Europe)1
▪ Female predominance 2:12
▪ Increases with age2
▪ Mostly occurs BEFORE going to sleep but can be all day
▪ Totally a clinical diagnosis, no sleep testing needed
▪ Differentiate primary RLS from RLS secondary (25%) to:4
▪ Pregnancy, CKD, iron deficiency, medications (ALL anti-depressants except bupropion)
▪ Primary more frequent in younger patients, with family history
▪ May be associated with dopaminergic dysfunction4,5

**consider iron absorption issues; *FDA-approved.
1. Allen RP, et al. Sleep Med. 2003;4:101-109. 2. Manconi M, et al. Sleep Med. 2004;5:305-308. 3. Hening WA. Am J Med. 2007;120(1 Suppl 1):S22-S27. 4. Panossian LA, Avidan AY. Med Clin North Am. 2009;93:407-425.
Restless Legs Syndrome: Diagnostic/Treatment Strategies
Nonpharmacologic
▪ Relaxing exercise before bedtime may reduce symptoms3
▪ Avoid medications and substances that may aggravate symptoms (SSRIs, antihistamines, caffeine, nicotine)3
Pharmacologic
▪ Iron replacement therapy if ferritin level <50 μg/L
▪ Management of symptoms3,4
▪ Meds
Laboratory Testing
▪ Low Ferritin (< 50) –highly associated with RLS**1
▪ CKD: check GFR
▪ HCG (if pregnancy is suspected) –Pregnancy raises risk of RLS by 2- to 3-fold2

Management of RLS
Kannan, R. et. A. Am Fam Physician. August 15, 2013; Volume 88, Number 4.

Periodic Limb Movement Disorder (PLMD) vs. RLS
▪ Substantial overlap
▪ Up to 85% of RLS patients have PLMD
▪ 30% of PLMD patients have RLS
▪ RLS diagnosis is made clinically after suspicion of patient with
EDS and nighttime symptoms
▪ PLMD diagnosis is made via PSG
▪ Treatments are the same

Characteristics
▪ Stereotyped leg movements
▪ Involve one or both limbs
▪ Triple flexion with leg flexion, ankle dorsiflexion, and great toe
extension
▪ Lasts approximately 2 seconds
▪ Periodicity ranges from 20-40 seconds with a variable duration
▪ Mainly in non-rapid eye movement (REM) sleep
▪ Occasionally, a bed partner may provide the history of limb
movements

Narcolepsy

Clinical Features
▪ Chronic, debilitating condition with a prevalence of around 0.02%
▪ Clinical features begin in the teens or twenties. Onset after 50 years of age is unusual
▪ Average time to diagnosis is 10 years
▪ The classic tetrad of narcolepsy:
▪ Excessive sleepiness
▪ Cataplexy (if present is called type 1 narcolepsy; if not, is called type 2)
▪ Hallucinations upon falling asleep (hypnagogic) and/or upon awakening (hypnopompic)
▪ Sleep paralysis (generalized, transient inability to move or speak during sleep-wake transitions)
Kannan, R et. al Am Fam Physician. 2013 Aug 15;88(4):231-238.

Cataplexy
▪ Sudden decrease or loss of voluntary muscle tone following
an emotional trigger – usually laughter, but sometimes anger
or surprise
▪ Manifests as jaw dropping, head nodding, arms dropping to
the side, knees sagging, or the patient collapsing to the floor
▪ May last from a few seconds to a few minutes, and the
patient's conscious awareness is preserved
▪ The presence of cataplexy is highly specific for narcolepsy
Kannan, R et. al Am Fam Physician. 2013 Aug 15;88(4):231-238.

Diagnosis
▪ Referral to a sleep clinic
▪ Two weeks of a sleep log or actigraphy to document sleep duration
▪ Polysomnography to evaluate for other sleep disorders and document
adequate sleep time
▪ Next day multiple sleep latency test
▪ Daytime nap test to objectively assess for sleepiness and for onset of rapid eye
movement (REM) sleep during naps
▪ The combination of a mean sleep latency of less than eight minutes plus at least
two naps with early onset REM sleep supports a diagnosis of narcolepsy
The International Classification of Sleep Disorders: Diagnostic and Coding Manual. 2nd ed. Westchester, Ill.: American Academy of Sleep Medicine; 2005.

Treatment
▪ REM-suppressing antidepressants
▪ Venlafaxine (Effexor)
▪ Selective serotonin reuptake inhibitors
▪ Sleepiness
▪ Adequate sleep hygiene and scheduled daytime naps
▪ Medications
▪ Wake promoting medications: modafinil (Provigil), armodafinil (Nuvigil), solriamfetol (Sunosi), pitolisant (Wakix)
▪ Stimulants such as methylphenidate or dextroamphetamine
▪ Gamma hydroxybutyric acid (sodium oxybate [Xyrem, or Xywave])
Kannan, R et. al Am Fam Physician. 2013 Aug 15;88(4):231-238.

Insomnia

Insomnia
As a disorder:
▪ Trouble getting to sleep and/or
▪ Trouble staying asleep and/or
▪ Waking up too early and/or
▪ Occurring more days of the week than not
▪ Ongoing for over 3 months

Why Should PCP’s be Proactive about Insomnia?
▪ Very prevalent in primary care
▪ But patients don’t tell you
▪ Serious consequences
▪ Day to day life
▪ Poor outcome on mental and
physical health
▪ Insomnia is a clue
▪ Most insomnia is co-morbid
▪ Easy to identify
Treatment
▪ Relieves an upsetting symptom
▪ Improves next day
consequences
▪ Improves outcome of
co-morbidity
▪ Psychiatric
▪ Medical
▪ Majority is done by PCP

Insomnia Risk Factors
▪ Age (older)
▪ Sex (especially post-1 and perimenopausal2 females)
▪ Divorce / separation / widowhood
▪ Psychiatric illness (mood and anxiety disorders)
▪ Medical conditions
▪ Cigarette smoking
▪ Alcohol and coffee consumption
▪ Certain prescription drugs
1. NIH Consens State Sci Statements. 2005;22:1-30.
2. Young T, et al. Sleep. 2003;26:667-672.

Insomnia Screening and Follow-up
▪ Sleep Schedule: Do you have trouble getting to sleep, staying asleep, or waking
up too early?
▪ Daytime consequences: Do you feel like you have slept well throughout the day?
▪ Sleep timing: When do you go to bed? …Wake up? …Middle of the night
awakening? …How long does it take you to fall back to sleep?
▪ Treatments: What remedies have you tried? Any previous Rx’s?
▪ Sleep hygiene/lifestyle issues: Alcohol? Smoking? Exercise? Medications that
cause insomnia?
▪ Duration, frequency, prior: How long has this been going on?...How often?...
Have you had it before?...
Sateia MJ, Doghramji K, Hauri PJ, Morin MM. Sleep. 2000;23:1-66.
Erman MK. In: Sleep Disorders: Diagnosis and Treatment. Totowa, NY: Humana Press; 1998:21-51.

How Frequent are Comorbidities?
Terzano MG, et al. Sleep Med. 2004;5:67-75. Katz DA, McHorney CA. (1998).
Clinical correlates of insomnia in patients with chronic illness. Arch Intern Med 158(10):1099-1107.
35
28
19 17 15 1411
0
10
20
30
40
50
30
47
37 39
50
3842
106
17
2522
1215
0
10
20
30
40
50
InsomniaSevere insomnia
Pre
vale
nce
%Medical Conditions in Primary
Care Patients with InsomniaInsomnia with Medical Conditions

How Does Inadequate Sleep Increase CVD?
▪ Total sleep time (TST) < 5 hours compared to TST > 5 hours
▪ Higher glucose & cortisol levels
▪ HPA-associated endocrine & metabolic imbalances
▪ Hypercholesterolemia even after controlling for other risk factors
▪ Night-time BP: Nighttime SBP higher and day-to-night SBP dipping was lower
(-8% vs -15%, P < 0.01) in insomniacs
▪ Atherosclerosis: Total sleep time (P = 0.005), and sleep quality (P = 0.05)
contributed to increased carotid intima-media thickness
▪ Inflammation: Serum CRP levels higher and increased at a steeper rate
Lanfranchi, PA, et al. (2009). Nighttime blood pressure in normotensive subjects with chronic insomnia: implications for cardiovascular risk. Sleep 32(6): 760-766.
Nakazaki, C, et al. (2012). Association of insomnia and short sleep duration with atherosclerosis risk in the elderly."Am J Hypertens 25(11): 1149-1155. Parthasarathy,
S, et al. (2015). Persistent insomnia is associated with mortality risk. Am J Med 128(3): 268-275 e262. Lin, CL, et al. (2016). The relationship between insomnia with short
sleep duration is associated with hypercholesterolemia: a cross-sectional study. J Adv Nurs 72(2): 339-347. Farina, B., et al. (2014). Heart rate and heart rate variability
modification in chronic insomnia patients. Behav Sleep Med 12(4): 290-306. de Zambotti, M., et al. (2011). Sleep onset and cardiovascular activity in primary insomnia.
J Sleep Res 20(2): 318-325.

Does Insomnia Contribute to Development of Hypertension?
Lewis, P. E., et al. (2014). Risk of type II diabetes and hypertension associated with chronic insomnia among active component, U.S. Armed Forces,
1998-2013. MSMR 21(10): 6-13.
Prospective Follow-up
▪ Active duty in US Military
▪ Excluded: Chronic
insomnia prior to
1/1/1998
▪ Without hypertension at
baseline
▪ Chronic insomnia led to
higher risk of
hypertension (aHR 2.00)
Rate of Developing
Hypertension(per 10,000 person-years)
46.2
95.6
0
20
40
60
80
100
Controls Insomnia

Does Insomnia Increase Risk of CVDs?
1.681.85
1.4 1.3
0
0.5
1
1.5
2
aOR of CV Event
0.961.35
4.53
0
1
2
3
4
5
1 2 3
aOR for CHF
1st CV Event
# Insomnia Symptoms
Hsu, CY, et al. (2015). The Association Between Insomnia and Increased Future Cardiovascular Events: A Nationwide Population-Based Study.
Psychosom Med 77(7): 743-751. Laugsand, LE, et al. (2014). Insomnia and the risk of incident heart failure: a population study. Eur Heart J 35(21):
1382-1393. Canivet, C, et al. (2014). Insomnia increases risk for cardiovascular events in women and in men with low SES: a longitudinal, register-
based study. J Psychosom Res 76(4): 292-299.

How Much Does Insomnia Contribute to CV Mortality?
Health Professionals Follow-Up Study
▪ US men free of cancer
▪ Insomnia symptoms in 2004, followed through 2010
▪ Adjusted for age, lifestyle factors, and common chronic conditions
Metaanalysis of 13 Prospective Studies
▪ 122,501 subjects followed for 3-20 yrs
▪ Insomnia increased risk by 45% of developing or dying from CVD ▪ (RR 1.45, 1.29-1.62; p < 0.00001)
Li, Y, et al. (2014). "Association between insomnia symptoms and mortality: a prospective
study of U.S. men." Circulation 129(7): 737-746. Sofi, F, et al. (2014). Insomnia and risk of
cardiovascular disease: a meta-analysis. Eur J Prev Cardiol 21(1): 57-64.
1.25
1.091.04
1
1.25
1.5
Total Mortality CVD MortalityDifficulty Initiating & Nonrestorative
Difficulty initiatingDifficulty maintainingEarly-morning awakenings
1.55 (1.19-2.04)
1.32 (1.02-1.72)
Health Professionals Follow-Up Study
Adjusted Hazards Ratio

How Does Insomnia Contribute to Diabetes Risk?
Insulin Resistance Associated with
Subjective Sleep Complaints In
Those without Diabetes
ORs
Adjusted
for
InsomniaDaytime
Sleepiness
Sex and age1.68
(1.09–2.58)
1.80
(1.22–2.66)
Fully*1.24
(0.74–2.09)
1.75
(1.10–2.77)
*Adjusting for sex, age, alcohol consumption,
smoking, exercise, occupational status, BMI,
and family history of diabetes
Pykkönen A-J, et al. (2012) Subjective Sleep Complaints Are
Associated With Insulin Resistance in Individuals Without Diabetes.
Diabetes Care 35:2271–8.
aORs for HbA1c >= 6.0%
6.79
3.96
2.33
0
2
4
6
8
Kachi, Y., et al. (2011). Association between insomnia symptoms and
hemoglobin A1c level in Japanese men. PLoS One 6(7): e21420.
Males 22-69 years old with no hx of diabetes
Difficulty maintaining
sleep
Lasting 2+wks
Early AM
awakening
Some-times
Some-times
Japanese company annual health check-up

Does Treating Insomnia Lower Blood Pressure?
Standard BP treatment + estazolam
vs.
Standard BP treatment + placebo
▪ Insomnia treatment efficacy
▪ Estazolam: 67.3% (P < 0.001)
▪ Placebo: 14.0%
▪ Goal BP(< 140/90 mmHg)
▪ Estazolam: 74.8% (P < 0.001)
▪ Placebo: 50.5%
Li, Y, et al. (2017). "The impact of the improvement of insomnia on blood
pressure in hypertensive patients." J Sleep Res 26(1): 105-114.
Blood Pressure Reduction
from Baseline
-2.6 -2.8-2.5
-3.4
0
-2.3-2
-2.5 -2.7
-0.7
-2.8
-5
-7.1
0
-2.5
-3.7
-5.4
-8
-6
-4
-2
07 14 21 28 7 14 21 28
Placebo Estazolam
Systolic Diastolic
N = 202N = 200
Days of Treatment

Does Insomnia Increase Risk of Psychiatric Disorders?
31.1
35.9
30
14.4
5
21
18
10
0
5
10
15
20
25
30
35
40
Pa
tie
nts
(%
)
Incidence (%) over 3.5 years
Insomnia (n=240)
No Insomnia (n=739)
Breslau N, Roth T, Rosenthal L, Andreski P. Sleep disturbance and psychiatric disorders: a longitudinal epidemiological study of young adults. Biol Psychiatry. 1996;39:411-418.

Does Treating Insomnia Improve Comorbidities?
0
20
40
60
80
100
4 Months 16 Months
Poor Good
0
20
40
60
80
100
4 Months 16 MonthsControl Tai Chi
By Sleep Quality
%
4 months
CBT .21 (.03-1.47) p<.10
TCC NS
16 months
CBT .06 (.005-.669) p<.01
TCC .10 (.008-1.29) p<.05
ORs of Remaining
at High Risk
2-hour group sessions
weekly for 4 mo with a
16-mo evaluationRisk score based on 8 biomarkers: HDL, LDL, triglycerides,
C-reactive protein, fibrinogen, HA1c, glucose, insulin• High risk = 4 or more abnormal
By Intervention
% Remaining at High Risk
Carroll, JE, et al. (2015). Improved sleep quality in older adults with insomnia reduces biomarkers of disease risk: pilot results from a randomized controlled comparative
efficacy trial. Psychoneuroendocrinology 55: 184-192.

How is Insomnia Best Conceptualized to Guide Treatment?
▪ Genetic: heritability 42% - 57% in chronic insomnia
▪ Final common pathway: Autonomic and CNS hyperarousal
▪ Greater whole-brain metabolism during both sleep and wake periods
▪ Increased secretion of corticotropin and cortisol throughout sleep-wake cycle
▪ Sleep-wake regulation imbalance
▪ Overactivity of arousal systems
▪ Hypoactivity of sleep-inducing systems
▪ Both
▪ Failure of wake-promoting structures to deactivate during the transition
from waking to sleep states
Riemann D., et al. (2015). The neurobiology, investigation, and treatment of chronic insomnia. Lancet Neurol 14(5): 547-558. Vgontzas, AN, et al. (2013).
Insomnia with objective short sleep duration: the most biologically severe phenotype of the disorder. Sleep Med Rev 17(4): 241-254. Vgontzas et al.
Nofzinger et al. Am J of Psychiatry. 2004;161:2126-2128.

1. Kupfer DJ, Reynolds CF III. N Engl J Med. 1997;336:341-346.
2. Consensus Conference. JAMA. 1984;251:2410-2414.
Stepwise Approach for Managing Insomnia
Discuss With
Patient How They Sleep
Diagnosis1, 2
Education,
Including
Good Sleep
Practices1, 2
Nonpharma-
cologic
and/or
Pharma-
cologic
Therapy1, 2
Referral to
Sleep
Specialist
(In Cases of
Treatment
Failure)1

Patient Education: Most Powerful Tool
▪ Inform WHY management is so important
▪ Consequences
▪ Emphasize keeping regimented sleep schedule
▪ Wake up same time every day
▪ Naps usually not a good idea
▪ Emphasize sleeping long enough
▪ Can’t catch up on weekends
▪ Emphasize lifestyle measures
▪ Alcohol, exercise, smoking, caffeine, diet (no large meals)

Treatments: Cognitive Behavioral Therapy (CBT) and/or Medications?
▪ Address the co-morbid condition as well as the insomnia
▪ Discuss with patient pros and cons of meds and CBT
▪ Medications:
▪ Which are best applicable?
▪ Habit forming?
▪ How long to use?
▪ Side effects?
▪ CBT: at your discretion—ability, time, interest
▪ Allow patient to voice his/her concerns, fears, and needs

How Does Cognitive Behavioral Therapy Compare To Pharmacotherapy?
Adapted from: Jacobs GD, et al. Arch Intern Med. 2004;164:1888-1896.
Schutte-Rodin S et al. J Clin Sleep Med. 2008;4(5):487-504. Morin CM, et al. Sleep 1999;22:1134-56.
CBT-I Components
▪ Sleep hygiene education
▪ Cognitive therapy
▪ Sleep restriction therapy
▪ Stimulus control therapy
▪ Relaxation training
Sleep Hygiene
▪ Regular wake time
▪ Limit time awake and in bed
▪ Limit napping during the day
▪ Avoid clock watching if awake
▪ Avoid caffeine (after 2 PM),
alcohol after dinner, or eating
dinner just before bedtime
▪ Avoid stressful activities in
the evening

Treating Insomnia: Choosing the Right Pharmacotherapy
▪ Trouble with sleep initiation only: rapid and short acting
▪ Ramelteon, triazolam, zaleplon, zolpidem
▪ Trouble staying asleep with sleep initiation problems: rapid and long acting (can use these for sleep initiation only if you so choose)
▪ Eszopiclone, temazepam, zolpidem ER, zolpidem, suvorexant, lemborexant
▪ Trouble staying asleep withOUT sleep initiation problems
▪ Doxepin (taken at sleep onset), sublingual zolpidem (taken if one awakens)
▪ Issues with controlled substances: both of these unscheduled
▪ Ramelteon, doxepin
▪ Generic medications
▪ Temazepam, triazolam, zaleplon, zolpidem, eszopiclone

When to Consider Referral to a Sleep Expert
▪ Suspected obstructive sleep apnea or narcolepsy1-3
▪ Violent behaviors or unusual parasomnias1-3
▪ Daytime tiredness (sleepiness) that you can’t figure out1
▪ Insomnia fails to respond to behavioral and/or pharmacologic
therapy after an appropriate interval1,3
▪ You don’t feel comfortable treating the condition
1. Doghramji P. J Clin Psychiatry. 2001;62(suppl 10):18-26.
2. Sateia MJ, Owens J, Dube C, Goldberg R. Sleep. 2000;23:243-308.
3. Kushida CA, Littner MR, Morgenthaler T, et al. Sleep. 2005;28:499-521.

Summary
▪ Sleep is a necessary function of life. The absence and/or
disruption of which has serious consequences with quality and
quantity of life
▪ Most patients don’t volunteer sleep symptoms, so the PCP
must extract this information from them
▪ Patients with EDS have to be assessed and diagnosed to be
managed adequately
▪ Most sleep problems that patients present with can be fully
addressed and managed by the PCP

Additional Resources
▪ For additional resources, visit:
▪ TheNSF.org
▪ TheNSF.org/continuing-medical-education/
▪ Sleephealthjournal.org