Embed Size (px)
Citation preview

SLEEP , COMFORT
REST
• When people are at rest, they usually feel mentally relaxed, free from anxiety, and physically calm
• Rest does not imply inactivity
SLEEP• Sleep is a recurrent, altered state of
consciousness that occurs for sustained periods
• Sleep is a cyclical physiological process – Circadian rhythm– Biological clocks

Sleep Regulation• Sleep involves a sequence of physiological
states maintained by the CNS
• RAS ( reticular activating system) = wakefulness & BSR (bulbar synchronizing region) = sleep

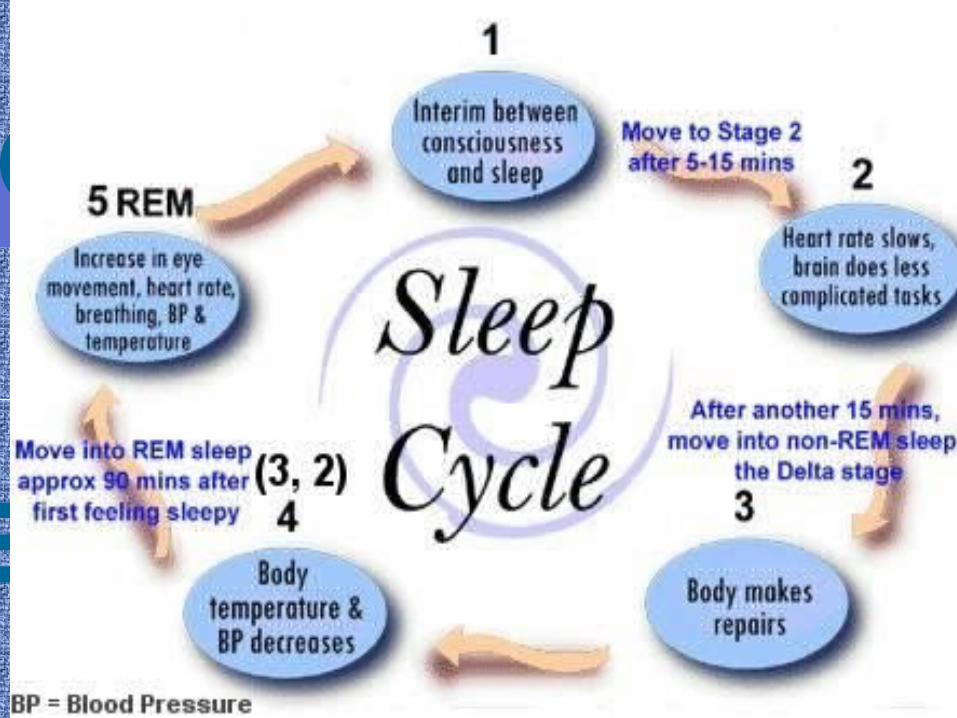
STAGES OF SLEEP
• NREM sleep = nonrapid eye movement - involves 4 stages
• REM sleep = rapid eye movement



Stage 1: NREM
• Lightest level of sleep
• Lasts a few minutes
• Easily aroused by sensory stimuli
• Waken, person feels as though daydreaming has occurred
Stage 2: NREM
• Period of sound sleep
• Relaxation progresses
• Arousal is still relatively easy
• Stage lasts 10-20 minutes
• Body functions, vital signs & metabolism, slow

Stage 3: NREM
• Involves initial stages of deep sleep
• Sleeper is difficult to arouse and rarely moves
• Muscles are completely relaxed
• Lasts 15-30 minutes
Stage 4: NREM
• Very difficult to arouse sleeper
• Deepest stage of sleep
• If sleep loss has occurred, sleeper will spend considerable portion of night in this stage
• Vital signs are significantly lower than during waking hours
• Lasts approximately 15-30 minutes
• Sleepwalking and enuresis may occur

REM SLEEP• Vivid, full-color dreaming
may occur in REM.
• Usually begins about 90 minutes after sleep has begun
• Typified by autonomic response of rapidly moving eyes, fluctuating heart and resp rates, increased BP
• Loss of skeletal muscle tone occurs
• Gastric secretions increase
• Very difficult to arouse• Duration of REM sleep
increased with each cycle and averages 20 minutes
Functions/Purpose of Sleep
• Restoration– Psychological– Physiological
• Biological
• Cognitive
• Conservation of energy
FACTORS THAT AFFECT SLEEP
• Physical illness
• Drugs and substances
• Lifestyle
• Emotional stress
• Environment
• Exercise and fatigue
• Food and caloric intake

SLEEP DISORDERS• INSOMNIA
• SLEEP APNEA
• NARCOLEPSY
• SLEEP DEPRIVATION
• PARASOMNIAS

INSOMNIA
• Chronic difficulty falling asleep
• Frequent awakenings from sleep
• Short sleep or nonrestorative sleep
SLEEP APNEA
• Disorder in which the individual cannot breath and sleep at the same time
• Lack of airflow through the nose and mouth for periods from 10 seconds to 1-2 minutes, there can be 10 or 15 to more than 100 respiratory events per hour of sleep
• Three types: central, obstructive, and mixed

CENTRAL SLEEP APNEA• Caused by cessation of diaphragmatic and
intercostal respiratory effort as a result of dysfunction of the brain’s respiratory control center
• Impulse to breath fails, temporarily
• Least common form

OBSTRUCTIVE APNEA
• Most common form
• Characterized by cessation of airflow despite the effort to breath
• Occurs when muscles or structures of the oral cavity or throat relax during sleep
• Usually have loud snoring


NARCOLEPSY
• A CNS dysfunction of mechanisms that regulate the sleep and wake states
• Falls asleep uncontrollably at inappropriate times
• Treated with stimulants
SLEEP DEPRIVATION
• S/S: blurred vision, fine motor clumsiness, decreased reflexes, slowed response time, decreased reasoning and judgment, cardiac arrhythmias
• Psychological S/S: confusion, disorientation, increased sensitivity to pain, irritable, withdrawn, agitation, decreased motivation

PARASOMNIAS• Sleep problems that are more common in children, one
common exception is bruxism (tooth grinding)
• SIDS
• Somnambulism(sleepwalking)
• Nightmares
• Nocturnal enuresis (bedwetting)
ASSESSMENT
• Normal sleep pattern, restful? sufficient?
• Self- reported
• Sleep log
• Bedtime routines
• Bedtime environment
• Client expectations
Pain
• Physical sensation
• Involves physical, emotional and cognitive components
• Stimulus
Physiology of Pain
• Transduction
• Transmission
• Perception
• Modulation

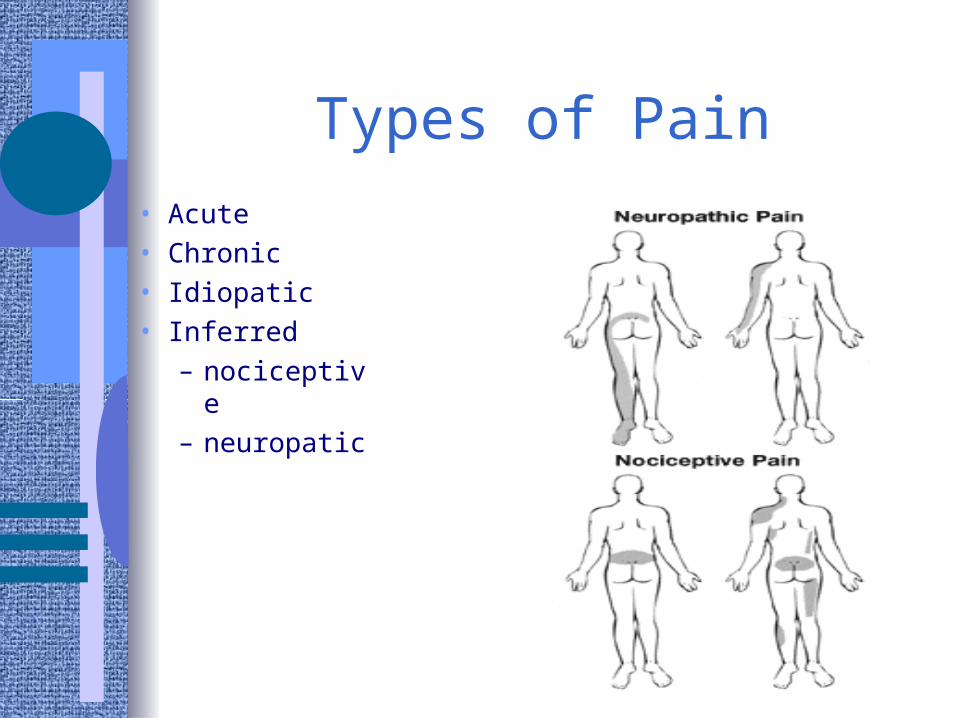
Types of Pain
• Acute• Chronic• Idiopatic• Inferred
– nociceptive– neuropatic
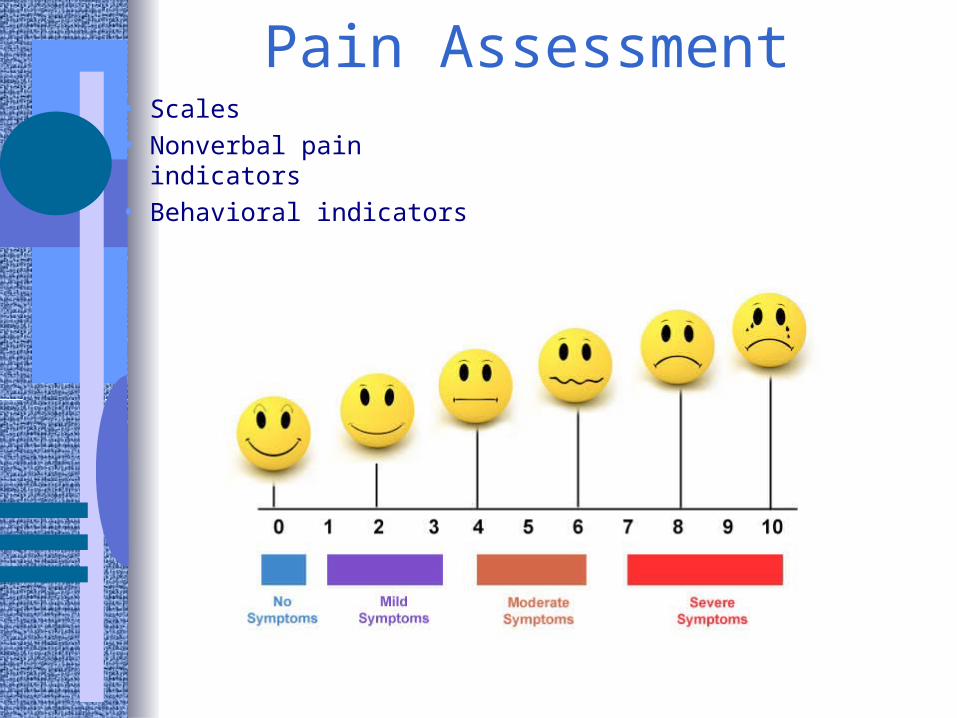
Pain Assessment• Scales
• Nonverbal pain indicators
• Behavioral indicators

Pain Management
• Pharmacological interventions
• Non-pharmacological interventions
• Barriers
• Cultural considerations
• Reassessment

Environmental factors affecting common and sleep
• Comfortable room temperature
• Proper ventilation
• Minimal noise
• Comfortable bed
• Proper lighting

Promoting Bedtime Routines
• Help client to relax in preparation for sleep
• Avoid mental stimulation before bedtime
• Relaxation exercises
• Guided imagery
• Good sleep hygiene

Sleep Hygiene
• Avoid sleeping long hours during weekend or holiday
• Bedroom should not be used for intensive studying, snacking, TV watching, or other nonsleep activity
• Avoid worrisome thinking when going to bed
• Avoid heavy meals for 3 hours before bedtime

Promoting comfort
• Encourage client to wear loose-fitting nightwear
• Instruct family on ways to position client and support dependent body parts to aid in muscle relaxation
• Have client void before going to bed
• Back massage
• Keep bed linens dry

Activity
• If client is at home, encourage physical activity during daytime
• Avoid rigorous exercise at least several hours before bedtime
Control of noise in hospital
• Close doors to client’s room
• Keep doors to work areas closed
• Reduce volume of nearby telephones and paging equipment
• Avoid abrupt loud noises
• Keep necessary conversations at low levels