Embed Size (px)
Citation preview

Assessment,interventionandoutcome
EditedbyAnitaMcAllister

Skriftserie i logopedi 2013:1
Advances in speech and language pathology 2013:1
Editor Anita McAllister

1
Copyright The publishers will keep this document online on the Internet—or its possible replacement—from the date of publication barring exceptional circumstances.
The online availability of the document implies a permanent permission for anyone to read, to download, to print out single copies for your own use and to use it unchanged for any non‐commercial research and educational purpose. Subsequent transfers of copyright cannot revoke this permission. All other uses of the document are conditional on the consent of the copyright owner. The publisher has taken technical and administrative measures to assure authenticity, security and accessibility.
According to intellectual property law, the author has the right to be mentioned when his/her work is accessed as described above and to be protected against infringement.
For additional information about Linköping University Electronic Press and its procedures for publication and for assurance of document integrity, please refer to http://www.ep.liu.se/.
Skriftserie i logopedi, 2013:1 Linköping University Electronic Press Linköping, Sweden, 2013 ISBN: 978‐91‐7519‐418‐9 © The Authors, 2013

2
Table of Contents Introduction
Anita McAllister & Edythe Strand ............................................................................ 1
1. A Danish Checklist for Children with Childhood Apraxia of Speech ‐
from Idea to first Edition
Louise Skov ............................................................................................................... 5
2. A case study of a six year old boy with normal language abilities and
childhood apraxia of speech
Zafira Karakezlidis .................................................................................................. 17
3. Evaluation of intensive Dynamic Temporal and Tactile Cueing therapy
for a 17‐year‐old male with verbal dyspraxia, intellectual disability and ADHD.
A case study
Catarina Ragnar ...................................................................................................... 31
4. Childhood Apraxia of Speech and concomitant functional problems:
A case study
Susanne Rex ........................................................................................................... 45
5. Speech‐facilitating oral motor treatment of a suspected childhood apraxia
of speech and oral apraxia in a 3 – year‐old girl. A case study
Birgitta Fog‐Poulsen ............................................................................................... 63
6. Oral and Verbal Motor Function in a child with childhood Apraxia of Speech
Helena Björelius ..................................................................................................... 71
7. Verbal Dyspraxi och Alternativ och Kompletterande Kommunikation (AKK) –
en forskningsstudie
Marlene Andersson ................................................................................................ 79
8. Diagnostisering av barn med misstänkt verbal dyspraxi. Bedömning med
VMPAC
Laura Olsson ........................................................................................................... 89
9. Behandling av två barn med verbal dyspraxi enligt Dynamic Temporal and
Tactile Cueing (DTTC). En multipel fallstudie
Åsa Engström .......................................................................................................... 99
10. Sensorisk stimulans med eldtandborste och DTTC. En kombinerad behandling
i två steg tillämpat på en 3‐årig flicka med förmodad verbal dyspraxi
Vanessa Westerlind .............................................................................................. 111

1
Introduction Two advanced courses on oral and verbal apraxia in children have been held at Linköping University in the spring of 2009 and 2011. Several international researchers participated as lecturers and contributed to the success of the courses and the high course evaluations. As an examination assignment several students chose to do case studies investigating the treatment outcome of different methods for children or teenagers with oral and verbal apraxia. Many were inspired by the method Dynamic Temporal and Tactile Cueing, DTTC that was thoroughly described by Professor Edythe Strand during the course. The case studies are presented as chapters in the present publication. Most chapters are written in English but some also in Swedish depending on the requirements of the specific course. At present there is a significant lack of treatment efficacy research in the area of childhood verbal apraxia, and many publications have indicated the need for this type of clinical research. Since these reports represent an important contribution to the limited number of outcome studies in children with diagnosed or suspected CAS we decided to make them available to a larger audience.
Childhood Apraxia of Speech – An eluding diagnosis in developmental speech disorders The terminology to describe the disorders has varied historically and is still not agreed upon worldwide. Childhood Apraxia of Speech, CAS, has been proposed by the American Speech‐Language‐Hearing Association and is now the most common term. However, the National Institute of Health, NIH, still uses the term Developmental apraxia of speech (DAS) on their web‐page (www.nidcd.nih.gov/health/voice/pages/apraxia.aspx). CAS, or DAS, is defined as a neurological childhood speech sound disorder where the precision and consistency of movements underlying speech are impaired in the absence of neuromuscular deficits (www.asha.org/docs). In 2007 the ASHA Ad Hoc Committee on Childhood Apraxia of Speech reviewed the available research and published two reports (ASHA2007a and b). Consensus on three features consistent with a deficit in the planning and programming of speech movements was reached, these features are: 1) inconsistent errors on consonants and vowels in repeated productions of syllables or words, 2) lengthened and disrupted coarticulatory transitions between sounds and syllables and 3) inappropriate prosody (ASHA, 2007a). Regardless of terminology the disorders is present from birth and appears to affect more boys than girls. CAS is not just a developmental delay of speech where the child follows the “typical” path of speech development but does so more slowly. Children with CAS commonly have disrupted and limited speech production that may be difficult to understand even for the immediate family. Generally their understanding of language is much better than their speech production may lead the listener to believe. The severity of the disorder varies. Many children with CAS also have other co‐occurring problems such as dysarthria; language problems, problems with reading, writing or spelling, coordination or gross and fine motor problems, and/or chewing and swallowing difficulties. CAS sometimes occurs in the context of specific syndromes such as velocardiofacial syndrome or Galactosemia. Many times there is no specific etiology and CAS is considered idiopathic. CAS may also occur with severe cognitive impairment, autism or neuropsychiatric disorders. In these children the diagnostic procedure may be particularly challenging.

2
The papers in this report provide important observations regarding children with CAS. Four studies address assessment issues in children with CAS, a few of whom might have normal language abilities and others different types of concomitant problems. One study examines the effects of augmentative and alternative communication – AAC in a child with severe speech difficulties. Five papers provide observations of treatment effects based on intensive programs and motor learning principles using different combinations of dynamic, temporal and tactile cueing, DTTC, or sensory stimulation with vibration. Results are quite promising and noteworthy for most participants and rather remarkable for one patient in his late teens with CAS, an intellectual disability and ADHD (see chapter 2).
The treatment research in CAS is still in its infancy. Case studies provide an important first step in developing important research questions for examining treatment efficacy in experimentally controlled single subject design research, and ultimately in larger randomized control trials. In this collaborative effort these studies on the characteristics of CAS and treatment outcome based on well described case studies provide an important contribution to the field.
Anita McAllister & Edythe Strand Stockholm and Rochester, October 2013

3
References American Speech‐Language‐Hearing Association (2007a). Childhood apraxia of speech
[Position Statement]. Available from www.asha.org/policy. In 2013‐07‐05
American Speech‐Language‐Hearing Association (2007b). Childhood Apraxia of Speech: [Technical Report] Ad Hoc Committee on Apraxia of Speech in Children, Rockville Pike, MD:ASHA. In 2011‐01‐15
Apraxia of Speech. http://www.nidcd.nih.gov/health/voice/pages/apraxia.aspx. In 2013‐07‐05

4

5
1. A Danish Checklist for Children with Childhood Apraxia of Speech ‐ from Idea to first Edition
Louise Skov, Department of Language and Communication, University of Southern Denmark, Denmark
Abstract The aim of this paper is to describe the first step in creating a Danish checklist for children with Childhood Apraxia of Speech to be used in the everyday life of the Danish Speech and Language Pathologists in cases where they are in doubt of whether it is severe phonological problems or suspected CAS. The first edition was evaluated by a questionnaire with six questions about the checklist sent by e‐mail to twenty Speech and Language Pathologists. The results of the questionnaire showed unanimous positive impressions of the checklist and an agreed‐upon need for a Danish checklist for children with Childhood Apraxia of Speech in clinical practice. Next step is to access the validity and reliability of the checklist in future studies.
Introduction The first steps in the creation of a Danish checklist for children with Childhood Apraxia of Speech (CAS) are described in this paper, from the first idea to the evaluation of the first edition. The creation of the checklist is based on inspiration from the study of Joy Stackhouse (1992) and her four perspectives on the symptoms identified in children diagnosed with CAS. Symptoms from other studies are also brought in as supplement to the author’s view of CAS as a motor‐speech disorder (Caruso & Strand, 1999; Love, 2000, Kent, 2000; McAllister, 2007; ASHA, 2007; Morgan & Vogel, 2008) and studies of tests, to get an idea of what is important to be aware of in the creation of a checklist useful in the SLP clinic (McCauley & Strand, 2008).
The idea behind making a Danish checklist is the general lack of detailed knowledge of the differential symptoms between more severe phonological problems in children and symptoms of CAS. It can sometimes be a challenge to differentiate between these two diagnoses. There are several reasons for this statement. First of all: Danish speech and language pathologists (SLP) do not know that much in detail about the diagnosis CAS often suspecting the child of having severe phonological problems without thinking of the possibility that it could be CAS (Skov, 2007). One of the doctors in Denmark who are responsible for diagnosing children with CAS, Svend Prytz, once said: ”if you don´t know what to look for – you will not find it” (quote from a one day visit at his clinic, January 2007). Second: In correlation with statement one, the

6
SLP’s has less experience with children showing symptoms of CAS. This in combination with the low rate of children with CAS makes it even tougher to get clinical experience with the symptoms of CAS and later on experience with the specific intervention used for children with CAS (Portwood, 1996; Shriberg et al., 1997; Caruso & Strand, 1999). Third: The symptoms of CAS vary over time in relation to the child’s developmental stage and degree of severeness (Davis, Jakielski & Marquardt, 1998; Davis & Velleman, 2000; Williams & Stephens, 2004; Morgan & Vogel, 2008). This change of symptoms makes differentiating between CAS, dysphonology, and dysarthria a complicated task. In Denmark many children are first diagnosed when they are five to six years old after long periods of intervention at the SLP by methods directed to children with dysphonology. Some may also have attended examinations at the hospitals pediatrics department without any conclusions of the childs problem (Stackhouse, 1992, www.dyspraksi.dk). Therefore, a checklist seems to be a missing tool in the Danish Speech and Language Pathologist’s toolbox.
The differentiation to dysarthria is less common in the clinic because children with suspected dysarthria most commonly are sent to further examination at the neurologist early in life, often before they start in kindergarten and school. Nevertheless of cause the SLP has to be aware of symptoms of dysarthria, because dysarthria still is a diagnosis often mentioned in the discussion on the differential diagnosis for children with CAS (Milroy and Morgan‐Barry; 1992, Caruso and Strand; 1999; Williams & Stephen, 2004).
This first edition is supported by the Danish parental foundation ”Dyspraksiforeningen”. They have an interest in spreading the word of the existence of CAS among children with severe speech problems. The first sketch of the Danish checklist for children suspected of having CAS were created of three SLP’s deeply interested in the diagnosis (www.lydbyggeren.dk, Lahti & Skov, 2009). After the first sketches – the responsibility was giving to one of the three SLP members of the group, Louise Skov as a project for a course at Linköping University, ”Oral and Verbal Apraxia in Children: Assessment, Diagnostics, Therapy”.
The aim of this paper is to describe the first step in creating a Danish checklist for children with Childhood Apraxia of Speech to be used in the everyday life of the Danish Speech and Language Pathologist´s in cases where they are in doubt of whether it’s severe phonological problems or suspected CAS.
Joy Stackhouse’s four perspectives and other studies
The study is a review on CAS where Stackhouse deals with four perspectives: The phonetic perspective, The clinical perspective, The linguistic perspective and The cognitive perspective. As a result of the review she is able to come up with a list of symptoms in relation to CAS under each perspective (Stackhouse, 1992; table 1). Because almost all symptoms are described and documented in the literature reviewed one should expect that the symptoms would be rather valid and therefore useful as a main inspiration for the creation of the Danish checklist.
Another study important for the creation of the Danish checklist is the Master thesis of Louise Skov (2008). The study investigates the difficulties twelve Danish children diagnosed with CAS had with the Danish language. In the study eight hypotheses were posed based on results from studies of CAS. One of the interesting results in relation to the aim of this paper was a tendency shown that CAS is not language specific. This means that the symptoms that were studied among the twelve Danish children are also described as difficult for children suspected of having CAS in the results from the international research in the field (Holmberg &

7
Bergström, 1996; Shriberg, 1997; Davis, Jakielski & Marquardt, 1998; McCabe, Rosenthal & McLeod, 1998; Caruso & Strand, 1999; Love, 2000; Davis, Jakielski & Marquardt, 2005; Jacks, 2006). This makes it reasonable to get inspiration from research studies outside Denmark and in that way update the Danish SLP´s with the newest results in relation to CAS.
Method First step in the creation of the checklist was the selection of symptoms that should be included and excluded from Stackhouse’s table 1 (1992). This selection was made in consideration of some practical issues in the daily work as a clinical Danish SLP. The following criteria were set up for the checklist:
Less time‐consuming as possible, but including all necessary questions to be able to check all kinds of symptoms seen in children with CAS. Not too long and not too short.
The design had to be very structured and simple.
The possible answers had to be straight forward – a bit ”black and white” to make it more simple, hoping that the SLP would find it an easy tool to use.
With these three criteria in mind the selection and redefinition of the symptoms mentioned in Stackhouse’s table 1 (1992) started. The redefinition was necessary because we wanted the design of the checklist to be a ”Yes”, ”No”, ”Don’t know” list. In this way all the symptoms had to be included in a sentence defined as a question.
After a lot of consideration it was decided that the checklist should only include questions considering the symptoms in relation to CAS and that the questions of more in depth anamnesis character had to be answered before the SLP uses the checklist. Additionally I skipped the four perspectives as headlines and instead used Stackhouse’s table 1(1992) as main inspiration combined with other studies both published recently and with a view more in the direction of CAS as a motor‐speech disorder as mentioned in the introduction.
The checklist ended up consisting of 44 questions under 10 headings: “General questions about the child’s speech and language” (five questions), “Questions about the child’s babbling” (four questions), “Questions about the child’s use of phonemes and articulation” (twelve questions), “Questions about the child’s prosody” (four questions), “Question about the child’s resonance” (one questions), “Questions about genetics” (two questions), “Questions about the child’s neurology” (two questions), “Question to pregnancy, birth and early development” (one question), “Questions about the child’s oral motor skills” (six questions) and “Questions about the child’s cognitive skills” (seven questions).
The purposes for using the checklist in the clinic were pinpointed in the introduction to the checklist. The purposes were as follows: 1) If the child had delayed speech and language problems, 2) If former speech and language therapy had a minimum effect even though the child had attended many hours of teaching over a longer period of time, and 3) If the child had severe problems with pronunciation.
To find out more about the need of a Danish checklist it was decided to make an evaluation of the checklist consisting of a questionnaire with six questions in relation to the checklist. The checklist including the six questions was sent out via e‐mail to twenty SLP´s with clinical experience ranged from one to more than twenty years. Nine SLP´s answered the questions. The six questions were formulated with the main interest to find out what the SLP thought of

8
it as a new tool in their toolbox but there were also questions about the design. The six questions were as follows:
1) What is your general impression of the checklist?
2) What do you think of the design of the checklist?
3) What do you think of the content of the checklist?
4) What do you think of the length of the checklist?
5) What is the possibility that you will find it relevant to use the checklist if you in your clinical work meet a child with symptoms that may seems like suspected Childhood Apraxia of Speech?
6) Do you think there is a need for a Danish checklist for children with Childhood Apraxia of Speech?
There were four possible answers to the first five questions, “Very good”, “Good”, “Less good” and “Not good”. Question number six could only be answered with “Yes” or “No”. Every answer from the nine SLP´s was registered in a Microsoft Excel table. After registration the distribution in percent was calculated. The overall distributions of every question were shown in table 1 and the distributions in percent were illustrated by figures 1 to 6.
Results In this section the results of the questionnaire are shown. First the more overall results and later question by question.
The nine SLP´s who answered the questionnaire ranged the overall impression of the checklist very positive, which means that they in almost all cases answered “Very good” or “Good” to the question asked. The only question with answers other than “Very good” and “Good” was question five. In table 1 is shown all answers to the six questions in each category and also in percent.

9
Table 1: The distribution of all the answers from the nine Danish SLP´s who participated in the questionnaire. The results are shown both in numbers of answers to each of the four possible answers*: “very good”, “Good”, “Less good” and “Not good” and also in percent. *Question six had only two possible answers: “Yes” and “No”. N = 9.
Question Very good Good Less good Not good
1. "What is your generel impression 5 4 0 0
of the checklist?" Percent Percent Percent Percent
56% 44% 0% 0%
2. What do you think of the design of the checklist? Very good Good Less good Not good
1 8 0 0
Percent Percent Percent Percent
11% 89% 0% 0%
3. "What do you think of the content of the checklist?" Very good Good Less good Not good
5 4 0 0
Percent Percent Percent Percent
56% 44% 0% 0%
4. "What do you think of the length of the checklist?" Very good Good Less good Not good
1 8 0 0
Percent Percent Percent Percent
11% 89% 0% 0%
5. "What is the possibility that you will find it relevant to
Very good Good Less good Not good
use the checklist if you in your clinical work meet a child
3 4 1 1
with symptoms that may seems like suspected Percent Percent Percent Percent
Childhood Apraxia of Speech?" 33% 45% 11% 11%
6. "Do you think there is a need for a Danish checklist Yes No
for children with Childhood Apraxia of Speech?" 9 0
Percent Percent
100% 0%
Next follows a description of the results from every question in more detail.
Question one
The answers to question one “What is your general impression of the checklist?” were distributed with five out of nine answering ”Very good” the same as 56 % and four out of the nine answering ”Good” counting for 44 % of the answers received. The distribution of the answers to question one is shown in figure 1.

10
Figure 1: The distribution in percent of the nine answers to question one: “What is your general impression of the checklist?”
Question two
The answers to question two “What do you think of the design of the checklist?” were distributed with one out of nine answering ”Very good” the same as 11 % and eight out of the nine answering ”Good” counting for 89 % of the answers received. The distribution of the answers to question two is shown in figure 2.
Figure 2: The distribution in percent of the nine answers to question two: “What do you think of the design of the checklist?”
Question three
The answers to question three “What do you think of the content of the checklist?” were distributed with five out of nine answering ”Very good” the same as 56 % and four out of the nine answering ”Good” counting for 44 % of the answers received. The distribution of the answers to question three is shown in figure 3.
Distribution in percent of the answers to question two
Very Good; 11%
Less Good; 0%
Not Good; 0%
Good; 89%
Distribution in percent of the answers to question one
Very good; 56%
Good; 44%
Not good; 0%
Less good; 0%

11
Figure 3: The distribution in percent of the nine answers to question three: “What do you think of the content of the checklist?”
Question four
The answers to question four “What do you think of the length of the checklist?” were distributed with one out of nine answering ”Very good” the same as 11 % and eight out of the nine answering ”Good” counting for 89 % of the answers received. The distribution of the answers to question four is shown in figure 4.
Figure 4: The distribution in percent of the nine answers to question four: “What do you think of the length of the checklist?”
Distribution in percent of the answers to question three
Very good; 56%
Good; 44%
Not good; 0%
Less good; 0%
Distribution in percent of the answers to question four
Very good; 11%
Good; 89%
Not good; 0%
Less good; 0%

12
Question five
The answers to question five “What is the possibility that you will find it relevant to use the checklist if you in your clinical work meet a child with symptoms that may seems like suspected Childhood Apraxia of Speech?” were distributed with three out of nine answering ”Very good” the same as 33 % and four out of the nine answering ”Good” counting for 45 % of the answers received, one out of nine answering “Less good”, 11 % and one out of nine answering “Not good”, 11 %, to the question. The distribution of the answers to question five is shown in figure 5.
Figure 5: The distribution in percent of the nine answers to question five: “What is the possibility that you will find it relevant to use the checklist if you in your clinical work meet a child with symptoms that may seems like suspected Childhood Apraxia of Speech?”
Question six
The answers to question six “Do you think there is a need for a Danish checklist for children with
Childhood Apraxia of Speech?” only had two possible answers, ”Yes” or ”No”. The distribution of the
answers to this question was very convincing. All of the nine SLP´s answered ”Yes” to the question,
which resulted in a distribution nine to cero in relation to ”Yes” versus ”No”. The distribution of the
answers to question six is shown in figure 6.
Distribution in percent of the answers to question five
Very good; 33%
Good; 45%
Not good; 11%
Less good; 11%

13
Figure 6: The distribution in percent of the nine answers to question six: “Do you think there is a need for a Danish checklist for children with Childhood Apraxia of Speech?”
Discussion The results of the questionnaire were very positive which means that the creation of the first edition of a checklist seems to have been a success. But it is very important not to forget the fact that we are only dealing with a first edition and not yet a complete checklist ready to use out in the clinic! Before it’s ready to be published, it needs to be further investigated whether the checklist is both valid and reliable. This should be tested with a much larger group of participants under very controlled conditions and criteria.
One of the important parts for further developing of the checklist is a careful review of the scoring of all the questions in correlation to the three possible answers: “Yes”, “No” and “don’t know”. As seen under the results the only question where the spreading of the four possible answers was wider than “Very good” to “Good” was question five ‐ the question about the possibility that the SLP´s will use the checklist in their clinic. One good reason why the answers are more varied than for all the other answers could be explained by the fact that the checklist are not yet tested for its reliability and validity regarding the scoring system. This is needed for the future version of the checklist to make it a meaningful tool in the assessment of suspected CAS (McCauley & Strand, 2008).
Conclusion In general the results from the questionnaire about the first edition of a Danish checklist for children with CAS were positive regarding the content, design and need as a future tool in the SLP´s daily work at the clinic. The fact that all participants found it relevant as a future tool can only be taken as a promising sign and a motivating factor in the further steps in the development of the Danish checklist for children with CAS.
Distribution in percent of the two possible answers to question six
Yes; 100%
No; 0%

14
References American Speech‐Language‐Hearing Association. Childhood apraxia of speech. Position paper
(short‐term in the paper: ASHA, 2007). http://asha.org/docs/html/PS2007‐00277.html (25th of June 2013).
Caruso, A.J., & Strand, E.A. (1999). Clinical management of Motor Speech Disorders in Children. New York: Thieme.
Davis, B.L., Jakielski, K.J., & Marquardt, T.P. (1998). Developmental apraxia of speech: determiners of differential diagnosis. Clinical Linguistics & Phonetics, 12, 25–45.
Davis, B.L., Jacks, A., & Marquardt, T.P. (2005). Vowel patterns in developmental apraxia of speech: three longitudinal case studies. Clinical Linguistics & Phonetics, 19(4), 249 ‐ 274.
Davis, B.L. & Velleman, S.L. (2000). Differential diagnosis and treatment of developmental apraxia of speech in infants and toddlers. The transdisciplinary journal; 10, No. 3, 177–192.
Holmberg, E. & Bergström, A. (1996). ORIS Munmotoriskt funktionsstatus. Löddeköpinge, Sverige: Pedagogisk Design.
Jacks, A., Marquardt, T.P., & Davis, B.L. (2006). Consonant and syllable structure patterns in childhood apraxia of speech: Developmental change in three children. Journal of Communication Disorders, 39, 424–441.
Kent, RD. (2000) Research on speech motor control and its disorders: a review and prospective. J Commun Disord.; 33, 391–428.
Lahti, U. & Skov, L. (2009) Lydalfabetet – et anderledes alfabet. Logos, 55, 5–8.
Love, R.J. (2000). Childhood motor speech disability. Needham Heights, U.K.: Allyn & Bacon. Pearson Education Company.
McAllister, A. (2007). Oralmotoriska störningar hos barn och ungdomar. In L. Hartelius, U. Nettelbladt, & B. Hammarberg (red), Logopedi. Lund, Sverige: Studentlitteratur.
McCabe, P., Rosenthal, J.B., & McLeod, S. (1998). Features of developmental dyspraxia in the general speech‐impaired population? Clinical Linguistics & Phonetics, 12, 105–126.
McCauley, RJ. & Strand, E. (2008). A Review of Standardized Tests of Nonverbal Oral and Speech Motor Performance in Children. American Journal of Speech‐Language Pathology, 17, 81‐91.
Milloy, N. & Morgan‐Barry R. (1992): Developmental neurological disorders. In Grunwell, P. (ed.): Developmental Speech Disorders; Clinical Issues and Practical Implications. London: Whurr Publishers Ltd.
Morgan, AT. & Vogel, AP. (2008). Intervention for childhood apraxia of speech. Cochrane Database Syst Rev. 16(3):CD006278. Review.
Portwood, M. (1996). Developmental dyspraxia. Identification and intervention. A manual for Parents and professionals. London, UK: David Fulton Publishers.
Shriberg, L.D., Aram, D.M., & Kwiatowski, J. (1997). Developmental Apraxia of Speech: I–III. Journal of Speech, Language, and Hearing Research, 40, 273–337.
Skov, L. (2007). Et spørgsmål om kendskab til PRAXIS, Dansk Audiologopædi, 43, 11–16.
Skov, L. (2008) Danske Børn med verbal dyspraksi – hvor har de deres vanskeligheder? Master thesis in Audiologopædi, University of Southern Denmark, Odense.

15
Stackhouse, J. (1992). Developmental verbal dyspraxia I: A review and critique. European Journal of Disorders of Communication, 27, 19–34.
Williams, P. & Stephens, H. (Eds) (2004). Therapy folder. Nuffield Centre Dyspraxia Programme, London, UK: The Miracle factory.
http://www.dyspraksi.dk/ (25th of June 2013).
www.lydbyggeren.dk (25th of June 2013).

16

17
2. A case study of a six year old boy with normal language abilities and childhood apraxia of speech
Zafira Karakezlidis, Department of speech and language pathology, Danderyd University Hospital, Stockholm, Sweden
Abstract This is a case study of a six year old boy (called T) that exhibits some of the clinical markers for Childhood Apraxia of Speech (CAS): a limited vowel repertoire, metathetic substitution errors, vowel distortions and articulatory struggle (groping). A analysis of the development of the speech sound repertoire show that syllable and word shapes are getting more complex but with great difficulty over a long period of time; approximately two years. There is no neurological or developmental disorder, no non‐speech oral motor problems or phonological speech problems which confirm that the origin of T’s speech problem is praxis; a deficit in the motor planning ability.
Introduction Childhood apraxia of speech (CAS) is, according to the definition stated by the American Speech‐Language‐Hearing Association (ASHA 2007), “...a neurological childhood (paediatric) speech sound disorder in which the precision and consistency of movements underlying speech are impaired in the absence of neuromuscular deficits (e.g., abnormal reflexes, abnormal tone). CAS may occur as a result of known neurological impairment, in association with complex neurobehavioral disorders of known or unknown origin, or as an idiopathic neurogenic speech sound disorder. The core impairment in planning and/or programming spatiotemporal parameters of movement sequences results in errors in speech sound production and prosody.” That is to say that children with CAS present speech problems that originate in problems with praxis, praxis being “[..] ‘the generation of volitional movement patterns for the performance of a particular action, especially the ability to select, plan, organize, and initiate the motor pattern ‘(Shriberg et al. 2003)”. These difficulties are different from phonological speech problems and therefore need a different approach in therapy. The aim of this case study is to present such a case. A six year old boy with pervasive speech problems that do not match his overall age appropriate language abilities and that cannot be explained by any coexisting syndrome or other developmental delay ‐ a boy with problems of praxis. This six year old boy represents a group of children that is rare and stand out from the vast majority of children with speech problems that a speech and language pathologist

18
normally encounters in the clinic. As T has age appropriate language skills in every area except phonology and articulation this study will present the development and variation of the speech sound repertoire and motor speech skills over time. All examples of words and phonem substitutions are in T’s mother tongue Swedish and written with Swedish letters. The symbol ‐> that occur in the text and tables is indicating how a word is pronounced by T.
Case History T was referred to the clinic at an age of 2 years and 11 months by the BVC Barnavårdscentralen (child health care clinic). The referral reported that he had problems with pronunciation and that he was almost completely unintelligible to everyone else but his mother. The history tells us that he babbled a lot as a baby and that his first words appeared early and two word sentences at 2:05 years of age. Language comprehension and vocabulary were adequate for his age. There was a history of speech delay in the family with three cuisines having problems with speech and literacy and the father still having mild pronunciation problems at the age of seven. No delay of motor development or oral motor problems, however there was a history of snoring.
Direct treatment at the clinic was started after a three month period of homework with the Oral stimulation program with an electric toothbrush (Lundeborg&McAllister, 2006) to improve the sensory ability and the precision of the lingual movements. Treatment at the clinic was planed at a rate of once a week (45 minute session) with additional exercises at the preschool for 10 minutes twice a day and exercises at home on a daily bases. At the start of treatment the focus was to target and establish articulatory placement and gestures for a range of sounds.
T had no problem understanding the underlying phonological principles but there were evident problems finding the place of articulation and when found it was difficult to sustain and equally difficult to shift. Much time was spent on practicing at a single sound and syllable level only. After four months the fricatives /s/ and /f/ started appearing in spontaneous speech. At this point, after about two years the fricatives /s//f/ have been established in speech but still the articulatory movement for these phonemes is exaggerated. Alveolar/palatal fricatives are starting to appear (sje/tje). Velar plosives appear in new positions but there is still a confusion of velar‐dental place of articulation and often there are metathetic substitutions.
There has been a need for visual cues for every new sound that has been introduced. Being a fast talker T himself realised the need to slow down the rate of speech during the exercises in order to find the right movement. T has always paid much attention to the clinician’s mouth and face and has been very accurate in describing his observations of the form of the mouth.
Method The study consists of two different types of data. First there is a retrospect from earlier conducted testing of language abilities and earlier follow‐up testing of the speech sound repertoire. Secondly there are recent assessments of the speech sound repertoire, phonological awareness, sentential stress, basic oral motor skills and motor speech ability in connected speech and elicited utterances from April 2009. The recent assessments are not follow‐ups but complementary to earlier testing to give a full survey of T’s language and

19
speech abilities. The motor speech examination was recorded on an audio recorder, part of the motor speech examination and some sessions with free speech and conversation were videotaped. All other assessments are available from transcripts only.
Instruments for assessment
Language comprehension, vocabulary and grammar
The Reynell Developmental Language Scales III (Aug 2006) was used to assess the language comprehension (age of patient 2:11 years). The vocabulary and grammar has not been formally assessed but the speech and conversation of T has never revealed any difficulties in need of further examination.
Phonological awareness
The assessment of phonological awareness was performed 2009. Three parts of the Swedish test ‘Bedömning av Språklig Medvetenhet hos förskolebarn och skolbarn’ by Nauclér & Magnusson (1993) was used: Rimigenkänning (identification of words that rhyme), Fonemidentifiering (identification of phonemes in words), Stavelsegmentering (syllable segmentation).
Speech sound repertoire
For the assessment of the speech sound repertoire the Swedish test ‘Fonemtestet’ by Hellqvist (1991) was used in august 2006 (age of patient 2:11), September 2007 (age of patient 4:00) and September 2008 (age of patient 5:00), May 2009 (age of patient 5:07)
Motor speech ability
For the assessment of the motor speech ability parts of the worksheet for Motor Speech Examination by Edith Strand (Strand, E. 2009) was used. Part A. Observations during connected speech and part B. Elicited utterances; monosyllabic words with the same and different first‐last phoneme, multisyllabic words, sentences of various length.
Lexical and sentential stress
Lexical stress was assessed with the repetition of three sets of words. Three words with acute accent (stegen, tomten, armen) and three words with grave accent (stegen, tomten, armen). Sentential stress was assessed in repetition of two short sentences with the stress shifting between words. Utterances used: kom hit, kom hit, kom hit nu, kom hit nu. There has also been an analysis of the sentences in connected speech.
Oral motor skills
For the assessment of oral motor skills parts of the test Nellie ‐ Neurolingvistisk undersökningsmodell för barn med språkstörning (Sahlén&Holmberg, 1986) was used in 2006 and later in 2009.

20
Results
Language comprehension, vocabulary and grammar
Assessment of other areas of language such as language comprehension (Reynell 2006) shows age appropriate results. No grammatical errors were noted and therefore there has been no need for a formal assessment. The vocabulary had always met the age expectations.
Phonological awareness
Rimigenkänning (Rhyme identification): 18 compared to the average score for the age at 21,2. Fonemidentifiering (Phoneme identification): 20 compared to the average score for the age at 18,8.
Stavelsesegmentering (Syllable segmentation): 5 compared to the average score for the age at 6,6. April 2009, patient 5:07 years). The overall phonological awareness is at an age appropriate level which tells us that the origin of the pronunciation problems is not phonological.
Speech sound repertoire
Fonemtestet, Aug 2006: The initial phonological assessment showed almost total absence of fricatives except /j/ and /v/ in medial/final position, fricatives were omitted at the beginning of words and replaced by velar plosives in other positions. Bilabial plosives were in place, no voicing problem. Dental plosives were replaced by velar plosives. Bilabial and velar nasals were in place; however the dental nasal was sometimes replaced by a velar nasal. All vowels were present but sometimes distorted (ex. Duscha‐>åcka, fot‐>åt). There were no consonant clusters and no deletions of unstressed syllables (see Appendix 1‐5).
Fonemtestet, Sep 2007: At the second speech sound repertoire assessment dental plosives and dental nasals appeared in final position but still no voiceless fricatives. Assimilations of place of articulation and manner of articulation occured (banan‐>maman). Some confusion with distinction. There were no syllable deletions. In general no significant difference from the last assessment a year earlier (see Appendix 1‐5).
Fonemtestet, Sep 2008: The third assessment showed that fricatives that had been addressed in therapy (/s//f/) were established but not in combination with consonants. The alveolar fricative (tje) was now present and replaced the palatal fricative (sje) (see Appendix 1‐5).
Fonemtestet, May 2009: All fricatives exist in almost every position. There is still some difficulty with the voiceless palatal fricative (tje) and the voiceless palato‐alveolar fricative (sje) in medial/final position that is substituted with /s/. /l/ is established in initial position, substituted with /j/ in other positions. /r/‐ > /j/ in all positions. Velar plosives are substituted with dental plosives most of the times but backing also occurs in free speech. No cluster reduction but substitutions occur. Most clusters with s+consonant as well as cluster tv‐ are in place. No supradentals. Some vowel errors (see Appendix 1‐5).
There have occasionally been some consistent processes of substitution, these processes have however shifted over time (see Tabel 1). Fronting of the velar plosives have followed on a period of backing of the dental plosives and there is still some confusion with velar‐dental articulation. Non‐developmental processes such as initial consonant deletion, backing, vowel

21
errors and substitutions of fricatives for stops have also been part of T’s speech development. In longer words T sometimes makes use of a rounded half‐closed back vowel (w) and the precision of articulation differs from time to time for the same word. Vowels in isolation are correct, in words however they are distorted and sometimes prolonged. In addition there is some glottal phonation and a hypo nasal resonance that have become more prominent over the last six months

22

23
Motor speech ability The motor speech examination reveals that motor planning is a major problem regardless of context. In short words with the same first and last phoneme there is inconsistency in articulation, the same word will be differently produced after immediate repetition and after a pause. However, the immediate repetition does not always guarantee a successful articulation (ex sås‐>såk, båt‐>båk immediate repetition, sås‐>sås, båt‐>båt after a pause). Problems finding the correct articulatory position for a speech sound in context with other sounds is obvious, even though the phoneme in isolation is correct. This is true even for phonemes that have been in focus of therapy for a while. Most consonants are difficult to produce even in mono syllable words with a CVC structure. Both consonants in a word cannot be successfully produced; if the initial phoneme is achieved the final will be omitted or substituted or vice versa. There are also signs of groping to find the right position for speech sounds and sounds that have been established in spontaneous speech still have an over emphasized movement of articulation. The need for visual cues is obvious for multi syllable words and for new sounds introduced in therapy. In multi syllable words the vowel errors, omissions and metathetic substitutions increase. However some phonemes that are substituted in a CVC‐word (mål‐>måj) may appear correctly in a CVCV (måla‐>måla) and CVCVCV (målare‐>målaje) structure.
The syllable shapes have for a long time been the same since the first assessment at 3:00 years of age. T has exhibited different syllable shapes (CV, VC, CVC, VCV) and have gradually added more syllables to a word. Still it is difficult to handle syllables with more than one consonant before vowel but this is slowly improving, there is also a change in word shapes in mulisyllable words. One example is the word ‘telefonbok’ which consists of four syllables CV‐CV‐CVC‐CVC that changed to V‐V‐V‐CV (/eeåbo/), another example is the word ‘dammsugare’ with the four syllables CVC‐CV‐CV‐CV that changed to CVC‐V‐V‐V (/pamuae/). The latest assessment shows increased rates of CCV and VCC syllables (see Appendix 6).
Lexical and sentential stress
Lexical and sentential stress is kept intact over shorter segments and in sentence repetitions. The imitation of the therapist’s intonation is exact during exercise with immediate repetition. In free speech the overall prosodic contour is effected and often deviant.
Oral motor skills
The first assessment (2006) of oral motor skills with ‘Nellie’ (Sahlén&Holmberg, 1986) showed normal range of movement for the lips but difficulties to elevate the tongue tip. A second assessment was performed in 2009 with the same assessment material that shows no indication of oral motor problems. Neither does the medical history reveal any oral motor problems. Since the ability to perform voluntary non‐speech movements is intact and there are no signs of weakness the oral motor skills are not causing the speech problems.
Informal observations of gross and fine motor skills and temperament
Teverovsky et al. (2009) states in their research paper that “ Children with motor speech disorders, including CAS, may show generalized motor incoordination, problems with manual

24
dexterity and/or oral motor dysfunction.” This is true for the boy of this case study as well. T himself has often mentioned that his balance and coordination is not as good as it is for other children in his age and this has often been observed at sessions in an activity such as getting on and off a chair repeatedly. According to the parents this is confirmed by a pedagogue at T’s preschool and he has been assigned some special exercises for this purpose. The fine motor skills are also affected; T has difficulties handling scissors. He has no clear preference of hand and often grips the scissors upside‐down and his cutting is not smooth and the edges of the paper uneven. T has also noted that his hands are shaking after a physically demanding activity (leaning on a toy car while driving and steering it) and that he has to wait a few minutes before taking on a more fine motor activity such as using scissors or hold a pen. Teverovsky et al. (2009) also mention in the same paper that a survey amongst parent whose children exhibit speech and language problems to some degree have “ineffective behaviour management strategies”. Some sensitivity and low “threshold” for emotional stress has been observed in some situations, however these manifestations are difficult to classify.
A more general observation is the fatigue after a therapy session with focus on articulatory exercises which indicates just how demanding the articulation is.
Discussion Looking at the development of the speech sound repertoire the unusual shift of one phonological process to another, from backing of dental plosives to fronting, is a red flag marking that the speech problems in this patient do not fall into the category of phonological difficulties. The persistence of metathetic substitution errors that have been noted in this case is another clinical marker for CAS. Although metathetic substitution errors is a sign of increasing awareness of the consonant clusters and a strategy to address the difficulty of producing the consonants (Håkansson G, 1998) for children with phonological problems, it is for children with CAS yet another indication of motor planning problems. Another characteristic of the speech, and sign of motor planning difficulties, is the groping behaviour and the altered syllable shapes. The prolonged vowels, perceived as exaggerated stress, could be a way to compensate for co articulation problems.
Another indication of praxis problems is the slow pace of progress. Even though the phonemic repertoire has expanded and is more complete (see Appendix 1‐5) it is a very slow process that is only half way and the difficulty of establishing the new articulatory movements is evident. The amount and frequency that is needed for these children is not easily met in the setting of the average speech and language clinic so the importance of having the parents and preschool involved in therapy is crucial and unquestionable. A valuable lesson from this case about the responsibilities of the SLP is the importance of explaining the severity and pervasiveness of CAS but also the need to give a clear picture of the plan for treatment of CAS to parents and other care‐givers. Here the use of “carry over phrases” and “core vocabulary” is useful.
The boy in this study has adapted some communicative manners that could be considered strategies to improve his chances of being understood. Some of them are repeating utterances or parts of an utterance and giving clarifications during conversation even when this has not been asked for. The often non‐stop speech of T could be seen in the context of being unintelligible to others. In the light of not being understood by most people, people may often walk away before he has completed what he wants to say. This behaviour has, most likely,

25
evolved as a response to that. It would be interesting and beneficial for the children with CAS and other severe speech disorders to further examine the impact of the speech impairment on the children’s social interaction with peers and adults. Shriberg & Kwiatkowski (1994) address the issue of “psychosocial behaviour” of children with developmental phonological disorders and conclude that “..descriptive data indicate that a significant number of children with developmental phonological disorders experience psychosocial difficulties. As with most of the other descriptors, it is not known whether sampling biases inflate the magnitudes of these findings or whether they would differ significantly from data in a non‐speech‐delayed group. For intervention questions, however, such information clearly confirms the need to account for psychosocial variables in the overall plan of treatment.“
Conclusions According to the definition of CAS some of the diagnostic markers are among others articulatory struggle (groping), metathetic substitution errors and vowel errors which all have been observed in the speech of this six year old boy in both habitual performance as well in controlled contexts. Pervasive articulatory problems exist in the absence of any neurological condition, however, there are some general gross and fine motor difficulties. The sound repertoire and the syllable and word shapes have gradually expanded but only after a considerable time and treatment. Great effort and struggle is still needed in order to achieve the articulatory movements and all the phonemic features, such as the distinction voiced‐voicless and aspiration are not mastered. However, in other areas of language, such as comprehension, vocabulary, grammatics and phonological awareness, T’s performance is at an age appropriate level.

26
References American Speech‐Language‐Hearing Association. (2007). Childhood Apraxia of Speech
[Position Statement]. Available http://www.asha.org/policyDownloaded 2009‐03‐04.
Edwars, S. et al. (1997). The Reynell Developmental Language Scales III, RDLS Third Edition Manual. London: Thomas Nelson Publishing Company Ltd
Hellqvist, B. (Ed.). (1991). Fonemtest (Test of Phonology). Skivarp: Pedagogisk Design.
Lundeborg, I. & McAllister, A. (2006). Treatment with a combination of intra‐oral sensory stimulation and electropalatography in a child with severe developmental dyspraxia. Logopedics Phoniatrics Vocology, 1–9, Preview article.
Nauclér, K., & Magnusson, E. (1993). Bedömning av Språklig Medvetenhet hos förskolebarn och skolbarn (Assessment of language awearness in preschool children and children at school). Löddeköpinge: Pedagogisk Design.
Sahlén, B., & Holmberg, E. (1986). Nelli ‐ Neurolingvistisk undersökningsmodell för språkstörda barn (Neurolinguistic modell of assessment for language impaired children). Malmö: Utbildningsproduktion AB (UPAB).
Shriberg, L., Campell, T. F., Karlsson, H. B., Brown, R.L, McSweeney, J. L & Nadler, C. J. (2003). A diagnostic marker for childhood apraxia of speech: the lexical stress ratio. Clinical Linguistics & Phonetics, 17(7), 549–574.
Shriberg, L & Kwiatkowski, J. (1994). Developmental Phonological Disorders I: A Clinical Profile. Journal of Speech and Hearing Research, Volume 37, 1100–1126.
Strand, E. (2009). Oral and Verbal Apraxia in Children: Assessment, Diagnostics; Therapy / Assessment and Differential Diagnosis. Handout, 24–26 (Seminar at Linkoping University, Speech Language Pathology March 12, 2009)
Teverovsky, E. Glick, Bickel, J. Ogonowski & Feldman, H.M. (2009). Functional characteristics of children diagnosed with Childhood Apraxia of Speech. Disability and Rehabilitation, 31(2):94–102

27
Appendices

28

29

30

31
3. Evaluation of intensive Dynamic Temporal and Tactile Cueing therapy for a 17‐year‐old male with verbal dyspraxia, intellectual disability and ADHD. A case study
Catarina Ragnar, Habilitation services, Region Kronoberg, Sweden
Abstract This paper describes the procedure for and evaluates the result of an intensive speech therapy period using Dynamic Temporal and Tactile Cueing (for Speech Motor Learning). The subject is a 17‐year‐old male with intellectual disability and ADHD, whose dyspraxic motor speech problems have been identified since childhood and who is clearly communicatively disabled by his speech impairment. Speech sound inventory and oral motor assessment was carried out prior to the therapy period. A baseline for the production of the chosen practice words was established. DTTC treatment was given during three weeks. The pre‐ and post‐therapy word productions were compared, using percentage measures regarding correctly produced units. These indicated improvement for the majority of the practiced stimuli, as well as some generalisation of performance to non‐practiced stimuli. The overall oral motor control was unchanged after the therapy but a minor improvement was noticed for lingual control. The cueing techniques applied and the subject’s response to them are described.
Introduction A consensus definition of verbal dyspraxia has only recently been reached and described by the American Speech‐Language‐Hearing Association in Childhood Apraxia of Speech: Position Statement (2007). The definition includes three segmental and suprasegmental distinctive criteria concerning difficulties in the planning and programming of speech movements: 1.Inconsistent errors for both consonants and vowels in repeated syllable and word production, 2. Prolonged and distorted transitions between speech sounds and syllables (coarticulation “mistakes”), 3. Prosodic deviations, especially concerning word and sentence stress.
Descriptions of comorbidity in cases of ‘verbal dyspraxia’ are frequently reported. Björelius Hort (2009) found that three out of four in a group of children with ‘verbal dyspraxia’

32
performed below expected level on gross and fine motor tasks. In a parental survey by Teverovsky, Bickel & Feldman (2009), balance problems and manual motor difficulties were reported for about 50 % of the children with ‘verbal dyspraxia’. Problems concerning focusing, writing and temperament were other common coexisting symptoms.
As to ‘verbal dyspraxia’ in combination with intellectual disability (mental retardation, MR), Kumin (2006) finds that Childhood Apraxia of Speech, CAS, in the past has not been identified or treated in children with Down Syndrome, DS. The study investigates whether and to what extent this is done today and the results indicate that considerably more children than those having been diagnosed with CAS had clinical symptoms of CAS. Battini et al (2007) report on a boy with mental retardation and CAS resulting from a genetical deviation.
There is some documentation concerning ‘verbal dyspraxia’ treatment in individuals with intellectual disability, although not very extensive. According to Van Bystervelt, Gillon & Foster‐Cohen (2010), a combined intervention including speech training, phonological awareness activities and letter knowledge activities, is efficient for speech improvement in DS children but ‘verbal dyspraxia’ is not mentioned as being part of the children’s speech problem. In a study by Hejdedal & Westerlind (2010), an electric toothbrush stimulation programme resulted in improved orofacial motor function and oral sensory function in a group of DS children. Karin Bengtsson & Irene Johansson (2002) present a model for speech therapy in children with DS. The use of a palatal plate is central in the model, as well as creating awareness and knowledge of speech in both the child and its environment. One of the children in a study by Strand, Stoeckel & Baas (2006) has a mild mental impairment complementary to the ‘verbal dyspraxia’. The authors show that “frequent treatment, incorporating the principles of motor learning, may facilitate the treatment of severe developmental speech disorders accompanied by motor impairment”, reporting a positive therapy outcome for children with severe CAS, using the Dynamic Temporal and Tactile Cueing for Speech Motor Learning (DTTC). Baas, Strand, Elmer & Barbaresi (2008) describe DTTC treatment for a child exhibiting moderate mental retardation and severe CAS. It is evident from their results that functional verbal communication can improve even in older children with severe apraxia of speech.
Several reports on ‘verbal dyspraxia’ treatment in children without intellectual disability have been found, among others Lundeborg & Mc Allister (2006) studying the effect of electropalatography therapy in a dyspraxic child.
DTTC is an integral stimulation (“watch‐listen‐imitate”) approach for children with motor speech planning disorders, based on a treatment program designed for adults with acquired apraxia of speech. The method was described in Strand & Skinder (1999). DTTC emphasizes shaping the movement gestures for speech production and the continued practice of those in the context of speech. Imitation is facilitated by the therapist using tactile and temporal cueing techniques together with auditory and visual ones, e.g. guiding the articulators to the correct place and position, simultaneous production, reduced speech rate and delayed imitation. Tactile guiding and use of movement have been helpful in earlier speech therapy with the subject of this study, who is 17:8 years old. His diagnoses are moderate mental impairment, ADHD, oral and verbal apraxia (dyspraxia) and expressive language disorder.

33
Method
Case history
J was six weeks premature, born by acute Caesarean section. (CT of the brain: widened ventricles; chromosome analysis: nothing remarkable.) He was referred to the ‘habilitation’ centre at 19 months of age, due to psycho‐motor developmental delay. J’s general muscle tone is hypotone. Gross and fine motor functions, especially coordination skills are affected. ‘Hand‐on‐hand‐practising’ has led to some manual praxis progress but a lot of everyday manual activities are still unmanageable for J. Riding has helped improve his balance and posture. Signs of possible visual problems were noticed early and a visuo‐functional assessment at the age of 12 revealed crowding problems. Hearing was considered normal after testing at four years of age. From the age of three, symptoms of concentration problems became more and more noticeable in J’s behaviour, such as difficulty being still and increased distractibility. His interactive‐communicative skills have always been good. He uses body language and mimics to enhance messages, even though his ‘general’ facial expression is not very pronounced.
J’s babbling was normal. At 2:4 years he had comprehensible approximations of “mamma”, “pappa”, “nä”, “hej” and was using ‘yes/no’ adequately. Sentence building started before the age of four but spontaneous utterances are still ‘minimalistic’, although more grammatically developed. J’s pragmatic ability is fundamentally good. He likes having conversations but has become more and more embarrassed in encounters with new people, due to his expressive language problems. He very apparently has to struggle to ‘get the words from his brain to his mouth’. A lot of the time planning and programming the motor gesture of the word seems to be the “only” problem in J’s word production – that is he seems to know which word he wants to utter. On some occasions though, difficulties on a lexical level, too, seem apparent. J’s general language reception and interpretation ability is good. (PPVT‐III score at 11:8 years: appr. level 9:7 years, although proper Swedish norms were not available; TROG results relatively high). Signing was introduced early and for some years was his main means of language expression. J shows a strong awareness of the fact that he is not able to say what he wants to say in lots of situations and now has decided he wants a graphic communication aid. J has a reasonably good ability to discriminate between speech sounds but difficulty identifying phonemes in mono‐syllabic words. His letter knowledge is good and he can combine phonemes with graphemes and vice versa.
The speech development has been very slow and specific articulation problems have been obvious since pre‐school age. No real generalisation of new speech sounds and places of articulation has ever taken place. Also imitation of words has always been hard for J, even words which are phonologically simple. Reproducing the phonological structure of nonsense words has been quite impossible for him. At 8:6 years, J was using CV, VC, CVCV and VCV structures and even if more complex ones are becoming more common, the majority of his word production still consists of simple word forms. Earlier notifications of J’s speech include reduced vowel system and generally unsharp vowel production; difficulties producing /l/ in words, despite lots of therapy focusing on this, the tongue movement either being too short (/j/ sound) or too long; a strong tendency of moving articulation backwards; explosives sometimes inaccurately voiced/devoiced. At 17:5 years, a couple of months before therapy start, J’s speech was characterised both by ‘developmental’ and by ‘non‐developmental’

34
phonological processes. The former is represented by e.g. final consonant deletion, assimilation, cluster reduction and unstressed syllable omission (syntagmatic processes), fronting and devoicing (paradigmatic processes). These processes are not consistent across contexts in J’s production. Examples of the latter in J’s speech are backing, idiosyncratic cluster
reduction (/sku:la/ becomes /su:la/) and vowel errors (/bu:k/ becomes /bɔt/. Word final consonant addition is quite frequent and vowel distortion is common, often resulting in schwa.. There is a large variety in the production of a word, as well as in the realisation of a particular phoneme. Groping is often seen in J’s articulation efforts. Struggling in the speech production is obvious and sometimes J gives up. Although his word production difficulties increase in longer structures, he often has problems producing the sound structure of short words, too. His best word production skills are heard in ice hockey related words, which he uses a lot in conversation and for which his managing motivation is particularly high.
No big problems handling food orally have been reported during J’s growing‐up. Problems controlling the saliva is still seen in therapy trying to master tongue movement. In earlier oral motor assessment J exhibited problems with spatial orientation of lip and tongue movements, difficulty holding the tongue still, difficulty sustaining a movement pattern, accompanying facial movements and inability to perform complex movements. Also, touching the tongue surface with a toothbrush, caused involuntary tongue movements. A more recent observation is that J is not using his low pitch voice for speech. His natural vocal cord tone is only heard when he is laughing or coughing.
J has had direct speech and language therapy during a few periods, sometimes with a speech pathology student; about 60 sessions altogether. The rest of the speech pathologist contact for J has concerned the palatal plate, AAC, compensatory aids and language assessment. Thus, a lot of the treatment has been indirect, carried out by school staff. Palatal plate therapy was introduced when J was 10 years old. The plate is of a flexible type and it variably has been set up to guide the tongue in finding a certain position and to stimulating and practising a particular tongue movement. J’s parents’ and teachers’ opinion is that it has helped him to become more intelligible. An electric toothbrush oral stimulation programme has been carried out in periods. When J has had direct therapy on a more regular basis, a positive effect on his speech has always been noticeable. He has responded well to drill type exercises and there have been clear signs of motor learning. Using target words which J find highly motivating to be able to produce, has worked particularly well. J has never been able to imitate a new speech sound after just watching a model. Tactile/proprioceptive articulation guiding has been necessary, given manually or with a toothbrush. When labiodentals were introduced, his lips were repeatedly manipulated into the proper position and for some time, J used his own hands to do this. Sometimes the mobilisation of arm/hand movement has helped him imitate speech units which would otherwise be hard for him to produce. The Praxis method (the Nuffield Centre) has been useful reminding J of how those speech sounds are produced, which he cannot quite manage but it has also been used to stimulate the development of basic reading and writing skills. J is using computer software for picture and synthetic speech supported reading and writing exercises and for listening to newspaper articles (text‐to‐speech function).
Material and procedure
Pre‐therapy assessment: Speech sound system description (phonological system and phonetic repertoire) and inventory of syllable structure and word shapes, was made using the

35
Fonemtest (Hellqvist, B, 1995) and speech samples from conversation. Speech motor functions were assessed using parts of Verbal Motor Production Assessment for Children VMPAC (Hayden & Square, 1999). Motor speech examination was carried out along the lines suggested by Edythe Strand (lecture 2011) but less dynamically. J was asked to repeat progressively longer and phonetically more complex speech units. This procedure provided specific information for the choice of stimuli to be worked on in therapy. The assessment sessions were video recorded.
Ten stimuli were chosen for practice, monosyllabics, bisyllabics and multisyllable speech units (one phrase). The words included speech sounds not present in J’s production, neither as a
phoneme nor phonetically (/y/ and /ʃ/), sounds produced correctly or incorrectly, depending on the phonetic context and consonant clusters also not yet used. The criterion of usefulness was a common denominator in the choice of words, regardless of the phonetic complexity. Some words were chosen even though the complete structures of the words were beyond reach at this point. Hence the wide range of phonetic complexity among the items.
Baseline data were collected on three occasions over a period of 16 days. Production of the target words was elicited by imitation. Audio recording of the production was made.
Speech therapy period: Treatment was given during three weeks, 14 sessions altogether, one 30 minute session per day. Probe testing was carried out on four occasions, by elicitation of the target words plus ten words with a phonetic and phonotactic structure similar to the majority of the stimulus words. The probe items were presented randomly and no word was presented twice in a row. The probes were audio recorded. The ambition was to apply the principles of DTTC as much as possible in therapy. Except for a plastic glove, no equipment or materials were used. The total number of items worked on was 14, as four words were exchanged for new ones during the course of the therapy. The old word was passed on from direct therapy to home or ‘maintenance training’, i.e. the parents were asked to elicit the word as often as possible in everyday activities. The criterion for passing on a word was a few (3‐5 as it turned out) consecutive correct productions of the word without a model. The targeted words were practiced (approximately) 10 to 20 times during each session. Some words were focused for more practice than the rest in a session. The total number of trials to produce the whole unit or parts of it varied greatly when the therapy period was finished ‐ from 50 to 200 times (very approximately!). Two of the therapy sessions were recorded on video.
Post‐therapy assessment: Two days after the last session, a new speech sound system inventory and oral motor assessment were carried out, using the same tests as in the pre‐testing. Six weeks later, after a period of no speech therapy, an audio‐recording was made of the production of all the practiced words together with the 10 probe words.
The video and audio recordings were analysed for two purposes: 1. To measure therapy outcome. 2. For observations concerning the therapy situation – methods applied, response to cueing, the behaviour of both J and the speech pathologist.
Analysis The production of each individual stimuli was analysed for percentage phonemes correct (PPC) before, during and after therapy. The same procedure was applied to the controls, on two occasions during therapy and after it was finished. As each stimuli was elicited a number of times at every measuring point, a mean value of the PPC for each stimuli was calculated.

36
Percentage correct production measures were also calculated for the total production of the practiced items and the controls respectively and the figures from the three recording points were compared. The measures used were percentage word correct (PWC), percentage phonemes correct (PPC), percentage consonants correct (PCC) and “percentage initial phonemes correct” (“PIPC”). The “PIPC” was regarded as relevant in the performance comparison, as success in getting the initial sound right often proves helpful for the listener in the “decoding”. The Fonemtest word production before and after therapy was analysed in a similar way. As only parts of the VMPAC test was administered and no area (e.g. Focal Oromotor Control, Sequencing) was tested fully, there were no total scores to make a profile and to be compared with average skills. Thus, a qualitative comparison between J’s oral motor performance at the two assessment points, was made.
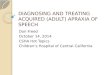
Results Figure 1 shows the mean value of the percentage phonemes correct for the 10 practiced words at the three measuring points. For the majority of the words, the PPC is higher at the end of the therapy period than before but the difference varies a lot. For four items (ny, bil, Levin, Istanbul), the second and third PPC figures indicate that some of the improvement during therapy has been lost during the rest period. For three items (lampa, penna, min bror Niklas), a further development of the production during the rest period is reflected by the third PPC figure being higher than the second. For two of the words (bil, skola), the pre‐ and post‐therapy PPC figures are the same but the performance patterns in‐between those differ. The production of the four stimulus words introduced during the ongoing therapy, also exhibit clear signs of various degrees of improvement, when the first and the last recording of the word are compared.
In Figure 2, the improvement in terms of PPC that took place during therapy also for the majority of the control words, is obvious although the pattern is somewhat different. For one word (apelsin) the pre‐therapy production is the best one and for one word (mål) the production is unchanged.

37
Figure 1. Percentage phonemes correct before, during and after intensive therapy for the production of the practiced stimuli
Figure 2. Percentage phonemes correct for the production of the control stimuli during and after intensive speech therapy.
Table 1 shows the four different percentage correct measures for the total production of the practiced stimuli on each of the three measuring occasions. The two multisyllable words have been excluded. The figures reveal a general increase in correct production from pre‐ to post‐ therapy testing but whereas the increase continues during the rest period for PWC, PPC and
0%
20%
40%
60%
80%
100%
ny bil lampa penna Levin bra skola Istanbul Sjögårdsvägen min bror Niklas
baseline value
after 13 therapy sessions
6 weeks after the end of intensive therapy
0%
20%
40%
60%
80%
100%
mål tupp banan pass docka gympa fem duscha stol apelsin
after 3 therapy sessions
after 13 therapy sessions
6 weeks after the end of intensive therapy

38
PCC, the peak performance in terms of initial phonemes is at the end of intensive therapy. The largest increase happened for percentage words correct – from 5% before therapy to 32,5% after the rest period and for percentage consonants correct – from 50,4% pre‐ therapy to 91,2% post‐therapy.
Some other noticeable differences between pre‐ and post‐therapy productions are not captured by the presented measures. Prosodic features were improved, e.g. intonation and word stress were better and vowel length more adequate. Also, some habituation has taken place in the production of the still non‐existing phonemes, even though the result is incorrect
(/s/ or /ç/ for /ʃ/; /y/ produced less like /ʉ/and closer to /y/). Table 1. PWC (percentage words correct), PPC (percentage phonemes correct), PCC (percentage consonants correct) and PIPC (percentage initial phonemes correct) for the total production of the practiced stimuli at the three measuring points.
Measurement
Before
therapy
%
At the last
session
%
Six weeks
after
therapy
%
PWC 5,0 27,5 32,5
PPC 63,0 73,5 76,5
PCC 50,4 60,8 71,2
PIPC 77,5 95,0 90,0
The percentage correct analysis of the word production in the Fonemtest also exhibits an increase for correct phonemes, consonants and initial sound, although a smaller one. The improvement in performance from before to after therapy was about 10 %, except for word production, for which the percentage correct was unchanged. However, a clear difference in the overall word production is evident, on a word structure level. The correct number of syllables is often produced and more commonly than before the vowels are correct, even if the consonants cannot quite be managed. Table 2 illustrates some of these changes in word production.

39
Table 2. Word production before and after therapy for eight Fonemtest‐items.
Test word Best production before therapy Best production after therapy
snögubbe sˈœg ̊ʰ sˈœːʷˌgɵwəb
gaffel gɔf ˈgasɛm
paraply pə ˌʀaˈpɛiːj
svamp fã çamp
flygplan fʉːpʰ ˈfœːgˌpɑ̃ː
bandspelare ba ˈb ̥anˌseːla
glasögon g ̊sk g ̊ɑːsˌœːjɔ
dammsugare sat ˈtãnˌsœːja
The VMPAC scoring figures for the oral motor tasks assessed before and after the treatment period, are to some extent different but when it comes to complex speech movements and sequencing in particular, the result is unchanged. A small improvement is noticeable for lingual control and double oromotor non‐speech movements, as well as for repeated vowel and /m/ repetition. Tactile guiding was needed for some of the tongue tasks in the pre‐therapy assessment but not when tried post‐therapy. These findings suggest that speech production therapy of the described type for J has some effect on his oromotor speech control function. This is noticable in J’s speech production both as a better tongue movement in /l/, making his /l/ no longer resemble a /j/. Change of articulation place being more common in his word production, is another sign of improved lingual control. No change is seen when it comes to mandibular and labial‐facial control. A qualitative description of J’s oral‐motor performance, both before and after the therapy period, includes multiple notifications of extensive motor control problems in the speech production, all the way from a respiratory‐phonatory level: Problems with vocal onset, with sustained phonation on /a/, as well as increasing the voice intensity. Opening the mouth is unsmooth, jaw instability is common (the bottom lip is used to stabilise the jaw), as is asymmetry of jaw and tongue activity and accompanying head movements. Blowing is labio‐dental and kissing is done with lip spreading. The tongue cannot be pointed or held still, moves towards one side when stretched out. Groping is seen when the tongue is going up to touch the top lip and movement from one side to the other is fast and uncontrolled, with minimal jaw opening.
The therapy situation
J exhibited a strong motivation for practicing all through the therapy period. He was boosted by hearing himself saying a word almost like the target word. All types of cueing described as part of the DTTC concept were used but tactile guiding was applied most extensively and sometimes ‘almost forcefully’. J verbally confirmed that this tactile monitoring was “good”. Visually cueing him to the initial articulatory position often worked well as a “middle‐step”,

40
also to remind him of coarticulation. In simultaneous production J had difficulty controlling his speech tempo and at the same time focus on the therapist. Successively he managed this a bit better, like he did slowing down the rate of speech. He also learnt to wait a little before imitating in the delay “mode” but had to be reminded each time. J was helped by a prosodically exaggerated model and rhythm was used throughout the therapy as a guiding component, together with illustration of movement. The usefulness of the very marked oral model was particularly evident in the practice of the word /ny:/ (new), where prolonging the vowel seemed to help J approach the target vowel quality. Feedback was given immediately, informing J about the result and quality of his production effort. Because of J’s massive problems with the speech gestures itself, prosodic variation in production was practiced very limitedly; some voice intensity and syllable stress variation. Towards the end of the period, J started to “react” to the intonation of the presented stimuli and imitate this a little. J’s efforts in trying to control the tongue movements noticeably increased his saliva production, making his articulation “wet”. A lot of the time during practicing, J’s eyes were almost shut and the instruction “look at me” had to be repeated often.
The tactile guiding was given both intra‐ and extraorally, often simultaneously, e.g. when /y/
and /ʃ/ were practiced. Correct production was not achieved during the therapy period for either of these sounds but J’s awareness of the target sounds and his articulation pattern in the stimulus words changed in the correct direction. To help J achieve the /y/, the cheeks and lips were positioned and shaped in order to counteract their hypertension in the spontaneous
production manner. In working with the /ʃ/, the tongue was pressed down and the cheeks/lips positioned at the same time. This way the sound was eventually managed in isolation and by
the end of the period /ʃœː/(lake) was produced. When J was beginning to get the production of his family name (Levin) almost right (/levivin/), his jaw was held down after the labiodental was produced, to stop the movement for the reproduction of the syllable. Cheek and lip manipulation was also applied in order to give J the sensation of the proper, lip rounded and coarticulated, initial position of the word “fågel” (bird), which J without tactile cueing produced with spread lips and spontaneously began with an /s/.
A lot of effort was spent on the forward movement of the tongue, e.g. the production of medial and final /n/ and /l/ and on increasing the time and force of the lingual‐dental/palatal contact. After some sessions the instruction “the tongue should stay there for a while” helped J in doing this. Working on “bil” (car), focusing on getting the final consonant right sometimes resulted in /l/ being produced initially instead ‐ /lbi:/. Later on /l/ would be pronounced after J’s own production ‐ /bi:j‐l/ or the bilabial would reappear at the end of the word ‐ /bi:lb/. It was easier for J to find the correct movement gesture after practicing the longer form of the word; “bilen” (the car). At the last session, J was able to say “bil” for the first time without a model, now with a somewhat longer than normal tongue‐palate contact. The direction of the (tongue/lip) movements was demonstrated with “whole body action” and with the hands representing the tongue and palate. J made progress with “skola” (school), even if the amount of practice was not enough to change his spontaneous production. The transition from /s/ to the velar was first practiced in isolation and managed quite well without phonation half way through the period. In the next session, the first part “sko” (shoe) was produced both whispering and loud a couple of times. Two sessions later all the movements of the whole word were produced in one sequence without phonation. The /‐kl‐/ in “Niklas” is still not produced but J’s way of saying the word changed during therapy. The first development from the original /nika/ or /nikas/ was /niknas/. After separately practicing the last syllable, focusing

41
the forward movement for the /l/ and by providing lots of visual and tactile cueing, J produces his brother’s name correctly for the first time.
The stimulus “Istanbul” is also pretty unchanged in spontaneous production but during the therapy period it went through different stages of altered pronunciation. The problem for J mainly seems to be finding the “three syllables‐program” for the word and he always wants
to go directly from the first to the third syllable, /ɪsbʊ̈l/. In the tenth session, J produces the sequence /istan/ without difficulty, after practicing it separately but trying to add the last syllable results either in the new form /isban/ or the old one. In the next session, J says
/ɪsbʊ̈ltan/ once and after simultaneous elicitation, the correct word structure is heard a couple of times. In the last session, the three syllable form comes easier and J whisperingly says the whole word, with a short pause between the syllables.
Discussion Therapy for people with verbal dyspraxia should be individual, intense and carried out on the basis of motor learning principles (Strand & Skinder, 1999), a design which was applied in the therapy period described. The intensity in terms of session regularity was far more than any therapy J has had in the past. Also the intensity of practice during the sessions differed a lot from earlier, when focus has usually been split between articulation and other aspects of language building. Another difference was the considerably larger number of elicitations for a practiced speech gesture. The combination of mass and distributed practice, is likely to have been of importance, both for the improvement of cued motor performance during training and for the signs of generalisation of movement performance to a non‐training situation (motor learning), which were noticed. E. Strand (lecture 2011) stresses the importance of such a combination. Some of the features of the DTTC concept have intermittently and intuitively been used in earlier therapy with J, without a proper “tool”. Both the amount and the manner of the cueing during the DTTC period, have no doubt played a crucial part for the outcome. However, the number of trials per session was considerably less than the amounts reported by Strand, Stoeckel & Baas (2006). Differences in stimulus length may explain some of the discrepancy, as practicing the multisyllabic items, which were initially divided into more manageable parts, took much longer than practicing the short ones.
J’s preference for tactile guiding and avoidance of visual information, especially during the introduction of new verbal motor exercises, could lead to the assumption of a difference in mirror neuron function. The activation of mirror neurons in the speech motor areas of the brain while observing speech movements in another individual, has been demonstrated by among others Watkins, Strafella & Paus (2003). Hammarbäck & Jansson (2006) find the hypothesis of mirror neuron activation as a basis for imitation, to be strengthened by the results in various studies and discuss the importance of visual facial information in speech motor learning. Focused attention is mentioned as an important precursor to motor learning and visual focus on the therapist’s face and eye contact are stressed in the “guidelines” for DTTC (Strand & Skinder, 1999). Even though J was not visually focusing the therapist’s face all the time, his overall attention during the sessions was good. Him closing his eyes part of the time during instruction and practice, may well be caused by his problems changing focus and integrating sensory information. Still, it would be interesting to see whether increased demand for visual attention during the sessions in future therapy, would further increase therapy results.

42
Motivation is another important pre‐requisite for motor learning (Strand, Stoeckel & Baas, 2006), a condition which was also fulfilled during the therapy period. J was highly motivated, as were his parents who were also strongly supportive and encouraging during the treatment.
As it turned out, the treatment during the intensive therapy described in this report, consisted of a mix of techniques, from older as well as contemporary approaches suggested for speech motor impairments: DTTC, phonetic placement, articulatory positioning, movement gestures and auditory/prosodic cueing. Tactile and proprioceptive feedback, however, played a particularly central part.
Whether J’s problems of oral motor control extend also to the vocal cord function, remains to be assessed. J does not like his dark voice (being seen as grown‐up worries him) but given his general speech motor control problems, a dysfunctional factor in his present voice behaviour is also likely.
The experience from the therapy period with J shows that the DTTC concept can be applied in the treatment of verbal dyspraxia combined with intellectual disability and/or ADHD, although not in a totally orthodox manner. However, some of the adjustments which were needed concerning cueing techniques, i.e more tactile than visual cueing, do not necessarily have to be linked to general cognitive level but could be indicative of cognitive style and/or “sensory profile or settings”. J’s attention‐hyperactivity disorder answers for his difficulty to pause before imitating (impulsivity) and his need for repeated instruction (short memory span). J’s own motivation for therapy and his understanding regarding his speech problem and its implications, as well as his understanding of the fact that it helps to practice, are in fact as good as would be expected for anybody with normal cognitive development. He was motivated by the possibility of being able to speak better and, later on, by his progress and no other reward system was needed. Generally DTTC therapy for individuals with intellectual disability would require more adjustments and consideration, both in the planning of sessions and in terms of motivation and reward factors.
The rate of change in J’s word production during the three week intensive period positively differ from earlier speech therapy outcome for J; e.g. velar production was worked on for two years. Apart from improvement concerning practiced items, the results also show ́ some carry‐over‐effect for non‐practiced language units. The parents think that J’s ‘speech sound awareness’ has increased and report that he tries more than before to say ‘difficult words’. Others have remarked that J speaks more and his mentor at school noticed an increased verbal capacity after the summer holiday. J’s own experience is that the therapy is helping him to speak better. The wide complexity range of the practice items made goal fulfilment prospect, i.e the chances of reaching correct production, for the words differ widely.
The fact that J proved very receptive to the feedback given by the manual /tactile cueing, could lead to the assumption that he should benefit from the sensory information provided in electropalatography(EPG) treatment, which according to Lundeborg & McAllister (2006), “provides direct and precise feedback to the subject about the articulatory changes that are necessary”. However, feedback during EPG‐training comes from visual patterns exposed on the computer monitor, requiring good enough visual interpretation ability, a demand which might make the method unsuitable for him, given his visual perception problems. Everyday‐at home‐practicing with EPG would otherwise be a way of meeting his treatment needs after growing out of the child and youth ‘habilitation’ services.

43
Conclusion Considering the degree of his speech dysfunction and its implications in terms of communicative disability, the amount of direct therapy addressing J’s speech problem has been vastly insufficient. The experience from the DTTC therapy period, suggests that J would have benefited from having considerably more direct speech pathology by a speech pathologist during his childhood and teens than has been the case. The generally very limited access to speech pathologist services for direct treatment in the Swedish ‘habilitation’ centres, is a problem when it comes to meeting the therapeutic needs of children and adolescents with ‘verbal dyspraxia’ in addition to other disabling dysfunction.

44
References American Speech‐Language‐Hearing Association. Childhood Apraxia of Speech [Position
statement]. Available from http://www.asha.org/docs/html/PS2007‐00277.html 2011‐01‐18.
Baas, B S, Strand, E A, Elmer, L M, Barbaresi, W J (2008). Treatment of severe childhood apraxia of speech in a 12‐year‐old male with CHARGE association. Journal of Medical Speech‐Language Pathology, Dec. 2008.
Battini, R, Chilosi, A, Mei, D, Casarano, M, Alessandri, M G, Leuzzi, V et al. (2007). Mental retardation and verbal dyspraxia in a new patient with de novo creatine transporter (SLC6A8) mutation. American Journal of Medical Genetics Part A 143A, 1771–1774.
Björelius Hort. (2009). Are Oral and Verbal Motor Functions Related to Manual and Overall Motor Performance in Children with Developmental Apraxia of Speech? Master thesis in logopedics, Karolinska Institut, Stockholm.
Hammarbäck, K, Jansson, E. (2006). Hur fungerar observerad motorinlärning och vilka implikationer har det för språkinlärning? Student paper. Department of philosophy and linguistics, Umeå University.
Hayden, D A, Square, P. (1999). VMPAC, Verbal Motor Production Assessment for Children. San Antonio, TX: The Psychological Corporation.
Hejdedal, M, Westerlind, V. (2010). The Effect of an Intra‐ and Extraoral Intensive Sensory Treatment with an Electric Toothbrush – A study on nine children with Down syndrome. Master thesis in logopedics, Linköping University.
Hellquist, B. Praxis: Träningsmaterial för dyspraktiska barn (In Swedish). [Therapy material for dyspraxic children]. Malmö. Pedagogisk Design. 1996
Hellquist, B. Fonemtest. [Phonology test]. Malmö. Pedagogisk design. 1995.
Kumin, L (2006). Speech intelligibility and childhood verbal apraxia in children with Down syndrome.
Down Syndrome Research and Practice. 2006; 10(1), 10–22.
Lundeborg, I, McAllister, A. (2007). Treatment with a combination of intra‐oral sensory stimulation and electropalatography in a child with severe developmental dyspraxia. Logopedics Phoniatrics
Vocology, 32(2), 71–79.
Strand, E A, Skinder, A. (1999). Treatment of developmental apraxia of speech: Integral stimulation methods. In Caruso, A J and Strand, E A (Eds.), Clinical management of motor speech disorders in children. New York: Thieme.
Strand, E, Stoeckel, R, Baas, B (2006). Treatment of severe childhood apraxia of speech: A treatment efficacy study. Journal of Medical Speech‐Language Pathology, Dec. 2006.
Teverovsky, E G, Bickel, J O & Feldman, H M. (2009). Functional characteristics of children diagnosed
with Childhood Apraxia of Speech. Disability and Rehabilitation, 31(2), 94–102
Van Bysterveldt, A K, Gillon, G, Foster‐Cohen, S. (2010). Integrated speech and phonological awareness intervention for pre‐school children with Down syndrome. International Journal of Language &
Communication Disorders, 45(3), 320–335.
Watkins, K E, Strafella, A P, Paus, T. (2002). Seeing and hearing speech excites the motor system
involved in speech production. Neuropsychologia, 41, 989–994.

45
4. Childhood Apraxia of Speech and concomitant functional problems: A case study
Susanne Rex, MSc, Skåne University Hospital Lund, ENT department
Abstract This paper describes a child with severe Childhood Apraxia of Speech and connected problems from the viewpoint of the International Classification of Functioning, Disability and Health (ICF) and Sensory Integration (SI). The analysis was performed by using the Short Sensory profile questionnaire (SSP), selected items from the Sensory Integration and Praxis Test (SIPT) and chosen questions/statements from the ICF. The results show that clustering the difficulties that one find could be a useful tool for Speech Language Pathologists to obtain a perspective of the speech problem and to help determine the relative contribution of fundamental deficits which is valuable when planning comprehensive intervention.
Introduction Childhood apraxia of speech (CAS) or verbal dyspraxia is a severe childhood speech sound disorder characterized by deficits in sequencing the movements required for speech production and carrying out purposeful voluntary movements for speech (Strand & Skinder, 1999). Childhood apraxia of speech is a neurological childhood speech sound disorder, in which the precision and consistency of movements underlying speech are impaired in the absence of neuromuscular deficits (World Health Organisation, 2004). Clinical markers are groping and/or trial and error behaviour, vowel distortions, limited consonant and vowel repertoire, use of simple syllable shapes, frequent omissions of sounds, altered suprasegmentals (e.g. prosody) and inconsistent error patterns (Strand, 2009).
When working with children with verbal dyspraxia one often experience concomitant functional problems. Communication disorders are highly likely to impact children’s functioning beyond the domains of speech and language (Teverovsky, 2007). The position statement concerning CAS (American Speech‐Language‐Hearing Association, 2007) defines apraxia of speech and also includes a line about its complexity: “CAS may occur as a result of known neurological impairment; in association with complex neurobehavioral disorders of known or unknown origin, or as an idiopathic speech sound disorder.” Children with language deficiencies frequently have problems associated with disorders in sensory processing (Cermak & Mitchell, 2006). Sensory processing disorders include motor planning deficits, poor attention, mild learning problems and difficulties in emotional and behavioural regulation.

46
It is important to understand how the whole child is functioning in order to systematically plan comprehensive evaluations and rehabilitation therapies and to be able to work efficiently with parents and other professionals engaged in the child with CAS. What kind of functional problems may co‐occur with verbal dyspraxia and how can we categorize and describe them? Different viewpoints will lead us to describe the CAS child’s connected problems in diverse terms and this paper will elucidate two of them by studying seven year old Liam.
The first viewpoint is The International Classification of Functioning, Disability and Health (World Health Organisation, 2004) which is a classification system for describing function independent of the underlying health conditions. The system, which is designed by an international team of researchers, has been promoted specifically as a useful tool for describing the functional problems associated with communications disorders (Teverovsky et al., 2008). The ICF provides an organized list of codes to describe the integrity of Body functions, the ability to carry out Activities of daily living, the individual’s social Participation and environmental factors. With a set of codes that apply to an individual one can get a functional assessment of that person, complementary to medical diagnoses. The information from ICF together with information from ICD‐10 (International Classification of Diseases) will give a detailed and meaningful description of a person’s health (Hartelius, 2008).
Sensory integration (SI) is the second perspective and it describes how we organize sensory inputs from the environment and from our own bodies and process these inputs for use (Cermak and Mitchell, 2006). Today Sensory Integration is widely used as a framework for understanding behaviour and for guiding assessment and intervention with children showing sensory processing disorders including motor planning deficits and poor attention (Cermak and Mitchell, 2006). When looking at the child’s difficulties from a SI perspective you may divide the deficits in two categories; sensory modulation and sensory discrimination and praxis. Sensory modulation is the ability to regulate different sensory inputs to produce an appropriate graded response. It can show as sensory overresponsivity (tactile defensiveness, gravitational insecurity or auditory defensiveness), sensory underresponsivity, sensory seeking or a combination of these. Sensory discrimination is the ability to accurately interpret the temporal and spatial characteristics of stimuli, for example to find an object among others in a pocket. Praxis, the process of ideation, planning and executing a planned response, is divided into somatodyspraxia, visuodyspraxia and bilateral integration and sequencing disorder. Somatodyspraxia refers to poor processing of tactile, vestibular and proprioceptive sensation and includes learning new motor skills. Visuodyspraxia refers to poor processing of visuomotor and constructional abilities. Children with difficulties in bilateral integration and sequencing have a hard time learning jumping rope, skipping and anticipating the effects of actions of their bodies needed in ball games. There are two assessments that are commonly used to examine sensory integration. The Sensory Profile is a questionnaire designed for caregivers of 3‐10 year olds and has 125 items. The short version, Short Sensory Profile (SSP) (Tomchek & Dunn, 2007) has 38 items. The Sensory Integration and Praxis Test (SIPT), (Ayres, 1989) is administered through performance‐based tasks and clinical observations and have normative scores for children ages 4;0‐8;11.

47
Method
Participant ‐ Case history
Liam (not his real name), 7;09 years old, was referred for a speech and language assessment at 2;10 because of using an unintelligible speech with primarily single words. Back for a control at the age of 4;05 years he was still showing a very simplified sound system. At 6:02 he got his diagnosis of Childhood Apraxia of Speech and by then had regular speech therapy according to the Swedish version of the Nuffield Praxis Program (Hellqvist, 1996). School was involved in the speech therapy as well as the mother. Co‐existing problems with fine and gross motor abilities was addressed by the teachers in preschool and in 2007 Liam saw a team at Lund University Hospital including child psychologist, paediatrician and physiotherapist and Motor impairment was diagnosed. Starting school meant new challenges and after a while difficulties with reading and writing was shown. Today he has a resource teacher in school and visits his SLP regularly together with his resource teacher for motor speech therapy.
Material
Data from the speech and language assessments the past year and from the physiotherapist and paediatrician at the Children’s department at Lund University Hospital have been considered for the SIPT test items. A questionnaire with the Short Sensory Profile and some questions/statements from the ICF was distributed to the mother of Liam and to his resource teacher in April 2009 (see appendix). School, caregivers and SLP/medical staff did not score the same about Liam’s performance on some tasks and those have then been indicated as difficult if any of them has scored/assessed it as hard and marked with an asterisk if the mother does not notice a problem in the home environment. The parts ‘perceptual functions’ (with exception of balance) and ‘sleep’ from ICF was scored only by the mother.
Analysis
The data was arranged in two tables from the viewpoint of function or sensory integration, analysed from the perspective of fundamental deficits, clustered and compared.
Results The data of Liam’s functional and sensory difficulties is presented in the two tables below from the Sensory Integration perspective and the viewpoint of ICF‐classification of function.

48
Table 1. Sensory Integration – based on The Sensory Integration and Praxis Test (SIPT) and Short Sensory Profile (SSP)
SIPT Age appr Difficult
Visual perception Figure‐background x
Visual‐motor Design copying x
Motor accuracy x
Constructional praxis x
Praxis Postural praxis x
Bilateral motor coordination x
Sequencing praxis x
Oral praxis x
Praxis on verbal command x
Somatosensory Manual form perception x
Oral form perception: stereognosis x
SSP No Yes
Tactile sensitivity Expresses distress during grooming x
Prefers long‐sleeved clothing when it is warm x
Avoids going barefoot (grass and sand) x
Reacts emotionally or aggressively to touch x
Withdraws from splashing water x
Difficulty standing in line or close to other x
Rubs a spot that has been touched x
Taste/smell sensitivity Avoids certain tastes or food smell x*
Will only eat certain tastes x*
Limits self to particular food textures/temp x
Picky eater x*
Movement sensitivity Distressed when feet leave the ground x*
Fears falling of heights x
Dislikes activities where head is upside down x
Underresponsive Enjoys strange noises x
Seeks all kinds of movement x
Overly excitable during o movement activity x
Touches people and objects x
Doesn’t notice when face/hands are messy x
Jumps from activity which interferes with play x
Leaves clothing twisted on body x
Auditory filtering Is distracted if a lot of noise around x

49
SIPT Age appr Difficult
Appears to not hear what you say x
Can’t work with background noise x*
Has trouble completing tasks when radio on x
Doesn’t respond when name is called x x
Has difficulty paying attention x x
Low energy/weak Seems to have weak muscles x*
Tires easily (when standing/body positions) x*
Has a weak grasp x*
Can’t lift heavy objects x
Props to support self x
Poor endurance/tires easily x*
Visual/auditory sensitivity
Responds negatively to unexpected loud noises x
Holds hands over ears to protect from sound x
Bothered by bright lights (after others adapted) x
Watches everyone moving around the room x
Covers eyes or squints to protect eyes from light x*
* no problems noted at home, but in school and clinic

50
Table 2. ICF – body functions, activities and participation
Functional domain
Body Functions Age equivalent Difficult
Memory Short‐term memory x*
Long‐term memory x*
Retrieval of memory x
Orientation Orientation to time x
Orientation to place x
Orientation to person x
Temperament and personality Conscientiousness x
Extraversion x
Agreeableness x
Psychic stability x
Open to experience x
Optimism x
Confidence x*
Trustworthiness x
Energy and drive functions Energy level x*
Motivation x*
Appetite x*
Craving x
Impulse control x
Sleep Amount of sleep x
Onset of sleep x
Quality of sleep x
Attention functions Sustaining attention x
Shifting attention x
Sharing attention x*
Psychomotor functions Psychomotor control x*
Quality of psychomotor functions x*
Emotional functions Appropriateness of emotion x*
Regulation of emotion x*
Range of emotion x
Perceptual functions Hearing functions x
Vestibular functions x*
Visual perception x
Olfactory perception x

51
Functional domain
Body Functions Age equivalent Difficult
Gustatory perception x
Visuospatial perception x
Sequencing complex movements Dressing x*
Speech movements x
Hand movements x
Mental function of language Reception of language; spoken x
; written x
Expressive language; spoken x
; written x
Articulation Production of speech sounds x
Voice and speech functions Production and quality of voice x*
Fluency and rhythm of speech Fluency of speech x
Speed of speech x*
Rhythm, tempo, stress patterns x*
Modulation of pitch patterns x*
Ingestion functions Chewing and biting x*
Manipulating food in the mouth x
Salivation x
Activities and Participation
Learning to read/reading skills x
Learning to write/writing skills x
Learning to calculate x x
Receiving spoken messages x
Receiving non‐verbal messages x
Conversation x
Discussion x
Changing basic body position x
Lifting and carrying objects x
Moving objects with legs and feet x*
Fine hand use x*
Hand and arm use, throw/catch x
Walking, diff surfaces/climb/run x*
Dressing x*
Avoiding dangerous situations x
Relating with strangers x

52
Functional domain
Body Functions Age equivalent Difficult
Formal relationships (teachers …) x
Informal relationships (peers) x
Family relationships x
* no problems noted at home, but in school and clinic
The information gathered from SSP and SIPT provides valuable insights into Liam’s sensory processing abilities. Within the first category which is sensory Modulation it stands clear that sensory seeking and sensory underresponsivity is age appropriate. Sensory overresponsivity shows normal tactile responses, but smell/taste sensitivity is affected. Gravitational insecurity is seen and some problems are also seen in auditory filtering. The second category of discrimination and praxis show no problems with discrimination, but somatopraxis, visuodyspraxia and bilateral integration and sequencing disorder is present. Low energy and weakness is also scored or assessed as present.
The information from the ICF perspective show impairments in Body functions in twelve functional areas out of fifteen. Those are memory, orientation, energy, psychomotor, emotional, vestibular, sequencing complex movements, mental functions of language, ingestion, voice and rhythm of speech. No or small problems are reported concerning personality and temperament, sleep, attention and perceptual functions (to hear, see, smell, taste – except vestibular functions). Identified disabilities in Activity and Participation are learning to read, learning to write and learning to calculate, moving objects with legs and feet, fine hand use, hand and arm use, walking and dressing. There are no prominent problems with receiving spoken messages, receiving non‐verbal messages, conversation, discussion, changing basic body position, lifting and carrying objects, avoiding dangerous situations, relating with strangers, formal relationships, informal relationships (peers) and family relationships.
The Sensory Integration approach targets multiple levels of functioning according to the International Classification of Functioning terminology (Cermak & Mitchell, 2006). If we compare Liam’s difficulties in Modulation with those in Body functions we see that they correspond in several areas; gravitational insecurity with vestibular dysfunction, overresponsivity to food and tastes with problems within ingestion, sequencing praxis with sequencing complex movements, body tone/energy with energy, and auditory sensitivity with perceptual functions. Comparing Praxis with Activities and Participation we also see corresponding disabilities; visuodyspraxia with psychomotor quality e.g. eye‐hand use, somatodyspraxia (learning new motor skills) with fine hand use and learning to write, bilateral motor coordination with motor abilities and coordination with body.
For a better overview the areas of disabilities are put in a more structured list:
1. Body tone (body tone/energy – energy) 2. Balance (gravitational insecurity – vestibular dysfunction) 3. Sequencing movements (sequencing praxis – sequencing complex movements) 4. Bilateral motor coordination (bilateral motor coordination – motor abilities and coordination
with body 5. Eye‐hand use (visuodyspraxia – psychomotor quality) 6. Eating (overresponsivity to food and tastes – ingestion) 7. Perception (auditory sensitivity – perceptual functions)

53
Using this overview it is clear that when clustering Liam’s difficulties we get a predominant profile with a motor base or a motor component e. g. sequencing movements (speech, writing) and eye‐hand use (puzzles, copying, and construction). A second cluster that one can make from Liam’s data is cognitive & learning. See figure 1 and table 1 + 2 for references. Clusters with no or small problems are social relations and personality.
Figure 1. Main clusters of difficulties
Discussion The aim of this case study is to describe a child with severe verbal dyspraxia and connected problems. Using ICF classification and/or an SI approach make it easy to put words on what we observe about the child in the clinical setting, to cluster the difficulties and to get an overview. We obtain a perspective to the speech problem and it also may help us to understand why some intervention programs are not working very well for our client. If we for example are using Sign as a complement to motor speech therapy it may be very difficult for the child with a severe motor speech disorder to learn the Signs, because learning them include good skills concerning bilateral motor coordination, motor sequencing, processing tactile, vestibular and proprioceptive sensation and memory.
The most important aspect of normal speech motor control concerns the moment‐to‐moment contribution of sensory (afferent) information to the multiple interactive pathways involved in movement planning, programming and execution (Caruso & Stand, 1999). This reflects the important role of sensory input to speech motor output. The two major types of sensory input are tactile; the ability to perceive touch, pressure or temperature information and locate the place that the stimuli is felt, and proprioceptive information; the ability to know what position each structure is in relation to other structures and in what direction a structure is moving. Describing the child’s sensory deficits, with a Sensory Integration framework or another model, will make it possible to determine the relative contribution of tactile and proprioceptive deficits not only when it comes to speech and oral motor abilities, but also within the whole child. This will give the Speech and language pathologist invaluable knowledge and information to incorporate when planning a comprehensive intervention
Motor based
Throw and catch
Jumping and climbing
Construction and copying
Fine hand motor ability
Chewing
Speech
Rhytm of speech
Cognitive and learning
Learning to read
Learning to write
Memory
Orientation

54
program. The assessment data in this described case of Liam indicate that focus in speech therapy should be the sequencing of speech movements (cuing the position of tongue, lips and jaw during the movement) i.e. proprioceptive, and a somewhat smaller amount of exercises should concern tactile information such as working with vibration and increased oral sensibility and awareness. The outcome of this case study illustrate that our Speech and language assessment and information gathered from SI or ICF perspectives are valuable to plan intervention regarding the child with severe Childhood Apraxia of Speech and concomitant problems.
Conclusion This case study show that using models like ICF or SI give us invaluable insights to the CAS child’s concomitant functional problems. Using a classification model helps the Speech language pathologist to describe and categorize the difficulties in a way that make intervention planning and cooperation with family, school personnel and professionals easier.
Acknowledgement I would like to thank the mother of the child described in this paper and also the resource teacher in his school; both inviting me to their home while answering the questionnaire.

55
References American Speech‐Language‐Hearing Association. (2007). Childhood apraxia of speech.
Position paper.
Ayres JA. (1989) Sensory Integration and Praxis Tests. Los Angeles: Western Psychological Services
Cermak SA & Mitchell TW. (2006).Sensory Integration. In McCauley RJ & Fey ME (Eds), Treatment of language disorders in children
Caruso, A.J.,& Stand E.A. (Eds) (1999). Motor speech disorders in children: Definitions, Background, and a Theoretical Framework. In Caruso, AJ and Strand, EA (Eds.), Clinical management of motor speech disorders in children. New York: Thieme.
Hartelius, L. (2008). Klassifikation av funktionstillstånd, funktionshinder och hälsa: ICF‐perspektivet inom logopedi. In Hartelius L, Nettelbladt U & Hammarberg B (eds.), Logopediboken. Lund, Studentlitteratur.
Hellqvist, B. (1996). Praxis, Träningsmaterial för dyspraktiska barn (adapted Swedish version of the training material from the Nuffield Centre in London). Malmö: Pedagogisk design.
Strand, EA, and Skinder, A. (1999). Treatment of developmental apraxia of speech: integral stimulation methods. In Caruso, AJ and Strand, EA (Eds.), Clinical management of motor speech disorders in children. New York: Thieme.
Strand, EA. (2009). Oral and Verbal Apraxia in Children: Assessment, Diagnostics; Therapy / Assessment and Differential Diagnosis. Handout, (Seminar at Linköping University, Speech Language Pathology March 12, 2009)
Teverovsky EG, Ogonowski Bickel J & Feldman HM. (2008). Functional characteristics of children diagnosed with Childhood Apraxia of Speech. Disability and Rehabilitation, pp 1–9.
Tomchek, SD & Dunn W. (2007). Sensory Processing in children with and without autism: a comparative study using the Short Sensory Profile. The American Journal of Occupational Therapy. March/April 2007, Volume 61, number 2, 190‐200.
World Health Organiziation, (2004). ICF Browser The International Classification of Functioning, Disability and Health. From the internet:
http://www.who.int/classifications/icfbrowser/?undefined&version=7 2009‐04‐01

56
Appendix 1. Short Sensory Profile (McIntosh, Miller & Shyu, 1999 in Tomchek
& Dunn, 2007)
Taktil sensitivitet
1. Uttrycker obehag när man pysslar om/sköter Ja Nej
2. Föredrar långärmat även när det är varmt/kort när det är kallt Ja Nej
3. Undviker att gå barfota, speciellt i sand eller gräs Ja Nej
4. Reagerar emotionellt eller aggressivt på beröring Ja Nej
5. Drar sig undan från vattenplaskande Ja Nej
6. Har svårt att stå i kö eller nära andra människor Ja Nej
7. Gnider eller river på ställen på kroppen där andra har berört Ja Nej
Smak/luktsensitivitet
8. Undviker vissa smaker eller matlukter som barn brukar gilla Ja Nej
9. Vill bara äta vissa smaker Ja Nej
10. Begränsar sig till viss matkonsistens/temperatur Ja Nej
11. Petig med maten, särskilt vad gäller konsistens Ja Nej
Rörelsesensitivitet
12. Tycker det är obehagligt när fötterna lämnar marken Ja Nej
13. Är rädd för att falla och rädd för höjder Ja Nej
14. Tycker inte om aktiviteter där huvudet är upp o ner Ja Nej
Söker sinnesförnimmelser/låg mottaglighet
15. Tycker om konstiga ljud/gör ljud för ljudet skull Ja Nej
16. Gör alla sorters rörelser o detta stör dagliga rutiner Ja Nej
17. Blir överdrivet upprymd vid aktiviteter med rörelser Ja Nej
18. Rör ofta på människor och saker Ja Nej
19. Verkar inte märka när händer och ansikte är smutsiga Ja Nej
20. Växlar mellan aktiviteter så att det stör leken Ja Nej
21. Låter kläder vara vridna på kroppen Ja Nej

57
Hörselfiltrering
22. Blir distraherad eller har svårt att fungera om det är mycket ljud omkring Ja Nej
23. Verkar som om han inte hör vad man säger ibland Ja Nej
24. Kan inte arbeta med bakgrundsljud Ja Nej
25. Har svårt att avsluta vad man håller på med när radion är på Ja Nej
26. Svarar inte när namnet ropas upp, men hör bra Ja Nej
27. Har svårt med uppmärksamheten Ja Nej
Energinivå
28. Verkar ha svaga muskler Ja Nej
29. Blir lätt trött, speciellt stående eller då kroppen hålls i speciell position Ja Nej
30. Har svagt handgrepp Ja Nej
31. Kan inte lyfta tunga saker Ja Nej
32. Stödjer sig själv med händer o armar Ja Nej
33. Dålig uthållighet/blir lätt uttröttad Ja Nej
Visuell/auditiv sensitivitet
34. Reagerar negativt på oväntade höga ljud Ja Nej
35. Håller för öronen för att skydda sig mot ljud Ja Nej
36. Känslig för skarpt ljus även efter att andra vant sig Ja Nej
37. Tittar på alla andra när de rör sig runt i rummet Ja Nej
38. Håller för ögonen eller kisar för att skydda ögonen mot ljus Ja Nej

58
Appendix 2. Enkät utifrån Internationella klassifikationen av
funktionstillstånd, funktionshinder och hälsa; ICF
Minne (memory)
1. Har bra korttidsminne (repetera, minnas en instruktion och utföra den Ja Nej ganska omgående) (short‐term memory)
2. Har bra långtidsminne (komma ihåg vad som hänt tidigare, Ja Nej minnas något inlärt tex en adress, en faktakunskap) (long‐term memory)
3. Har snabb och god ordmobilisering (kan hitta de rätta orden som behövs Ja Nej för att berätta och beskriva så omgivningen hänger med (retrieval of memory)
Orientering (orientation functions)
4. Kan tala om vad det är för dag/tid på dygnet/veckodag/årstid Ja Nej 5. Vet var man befinner sig till plats/ort/land Ja Nej 6. Kan tala om vad man heter i för‐ och efternamn, vad familj och Ja Nej
vänner heter
Temperament och personlighet (temperament and personality)
Är…
7. samvetsgrann (conscientiousness) Ja Nej 8. utåtriktad (extraversion) Ja Nej 9. följsam (agreeableness) Ja Nej 10. psykiskt stabil (psychic stability) Ja Nej 11. öppen för nya utmaningar (open to experience) Ja Nej 12. optimistisk (optimism) Ja Nej 13. självförtroende (confidence) Ja Nej 14. förtroendeingivande (trustworthiness) Ja Nej
Energi och drivande (energy and drive functions)
Har mycket stor/hög…
15. energi nivå (energy level) Ja Nej 16. motivation (motivation) Ja Nej 17. aptit (appetite) Ja Nej 18. begär t.ex. vill ha läsk var dag, ska alltid gnaga på pennor (craving) Ja Nej 19. impulskontroll, t.ex. svårt att vänta när mat sätts fram, vill ta Ja Nej
på allt som ser intressant ut i omgivningen, svårt att lita på att han/hon
inte springer ut på gatan i trafiken (impulse control)
Sömn (sleep)
20. mängden sömn (amount of sleep) Normal Liten Stor 21. hur går nattningen till/hur somnar barnet (onset of sleep) Lätt Svår

59
22. sömnens kvalitet (quality of sleep) God Dålig
Uppmärksamhet (attention functions)
23. kan upprätthålla uppmärksamheten (sustaining attention) Ja Nej 24. kan skifta uppmärksamhet (shifting attention) Ja Nej 25. kan dela uppmärksamhet mellan två aktiviteter (sharing attention) Ja Nej
Psykomotoriska funktioner (psychomotor functions)
Har svårt med…
26. psykomotorisk kontroll, t.ex. reglera hastigheten hos beteendet Ja Nej eller svarstiden som involverar både motoriska och psykologiska komponenter,
kan vara överdrivet beteende som att trumma med tårna eller vifta med händerna
(psychomotor control)
27. kvaliteten på psykomotorisk funktion, dvs. att producera ickeverbalt Ja Nej beteende i rätt sekvens och utförande t.ex. öga‐handkoordination (rita,
forma bokstäver, rita mönster) och gång (quality of psychomotor functions)
Emotionella funktioner (emotional functions)
28. korrekt visad känsla i förhållande till situationen (appr. of emotion) Ja Nej
29. reglera känslor, kunna styra över sina känslor och anpassa hur Ja Nej
man visar dem i olika sammanhang (regulation of emotion)
30. variation och vidd av känslor, t.ex. kunna visa kärlek, hat, oro, sorg, Ja Nej
glädje, rädsla och ilska (range of emotion)
Perceptuella funktioner (perceptual functions)
31. hörsel, dvs. uppfattar tonhöjd, styrka, diskriminerar ljud (auditory perception); Hur är…
ljuduppfattning (hör t.ex. svaga ljud) God Dålig
ljuddiskrimination (hör skillnad på liknande ljud) God Dålig
lokalisation av ljud (varifrån kommer ljudet) God Dålig
lateralisering av ljud (skilja på ljud från vä och hö) God Dålig
taldiskrimination (kan skilja ut tal ur t.ex. bullrig miljö) God Dålig
32. balans (vestibular functions) av position, balans, rörelseuppfattning God Dålig annat kopplat till hörsel o balans,
tinnitus, yrsel, fallkänsla, illamående, tryckkänsla, irritation i öra. Om Ja, stryk under
33. syn, dvs. diskriminera form, storlek och färg (visual perception); Hur är…
kvaliteten på synen (quality of vision) God Dålig
ljuskänslighet God Dålig

60
färgseende God Dålig
kontrastkänslighet God Dålig
34. lukt, dvs. uppfatta olika lukter (olfactory perception) God Dålig
35. känsel, dvs. uppfatta skillnad mellan olika texture som t.ex. strävt God Dålig
och glatt stimuli genom att ta på dem (taktile perception)
36. visuospatialt, dvs. med synen se den relativa platsen hos objekt i God Dålig
omgivningen eller i relation till sig själv (visuospatial perception)
Sekvensera komplexa rörelser (mental function of sequencing complex movements)
37. påklädning går lätt o smidigt Ja Nej 38. talrörelser går lätt o smidigt Ja Nej 39. handmotorik smidig (t.ex. hantera penna, knappar, smålego) Ja Nej
Språkförmåga (mental function of language)
40. impressiva förmågor, (reception of language) talat språk, dvs. förstår bra vad som sägs Ja Nej
skrivet språk, dvs. kan läsa bra för åldern Ja Nej
41. expressiva förmågor talat språk, kan uttala och artikulera bra Ja Nej
skrivet språk, kan skriva bra för åldern Ja Nej
Röst och talfunktioner (voice and speech functions)
42. röstproduktion (production of voice) rösten produceras på ett normalt Ja Nej sätt med god samverkan mellan muskler i buk, lungor och struphuvud.
43. Röstkvalitet (quality of voice) låter rösten; hes, sträv, läckande, Ja Nej spänd, dov, nasal (stryk under om Ja)
röstläge Högt Lågt
röststyrka Stark Svag
Talflyt och prosodi (fluency and rhythm of speech functions)
Finns svårigheter med…
44. talflyt (fluency of speech) t.ex. stamning, skenande tal Ja Nej 45. hastighet (speed of speech) Ja Nej 46. betoning och tempo (rhythm of speech, functions of the modulated, Ja Nej
tempo and stress patterns in speech)
47. melodi och intonation (modulation of pitch patterns in speech) Ja Nej t.ex. monotont tal

61
Ätande (digestive functions)
Finns svårigheter med att…
48. tugga och bita (chewing and biting) Ja Nej 49. manipulera maten i munnen (manipulating food in the mouth) Ja Nej 50. Salivering (salivation), dregling Ja Nej
Rörelseförmåga (movement)
Finns svårigheter med att…
51. Ändra kroppsposition såsom lägga sig ner, sätta sig på knä, Ja Nej sätta sig, stå upp stilla på stället, böja sig framåt, skifta kroppens
tyngdpunkt. Om Ja, stryk under
52. Lyfta och bära saker i händerna, bära med armarna, sätta ner saker Ja Nej 53. Flytta på saker med ben och fötter t.ex. sparka Ja Nej 54. Finmotorik
a. Plocka upp små saker Ja Nej b. Greppa små saker Ja Nej c. Manipulera små saker Ja Nej d. Släppa små saker Ja Nej
55. Hand och arm‐motorik a. Dra saker Ja Nej b. Putta Ja Nej c. Sträcka sig efter Ja Nej d. Vrida och snurra händerna Ja Nej e. Kasta saker (boll) till annan Ja Nej f. Fånga Ja Nej
56. Gång och rörelse a. Gå korta sträckor Ja Nej b. Gå långa sträckor Ja Nej c. Gå på olika underlag Ja Nej d. Ta sig runt hinder Ja Nej e. Krypa och åla sig fram Ja Nej f. Klättra Ja Nej g. Springa Ja Nej h. Hoppa Ja Nej i. Simma Ja Nej
Källor:
1. ICF Browser = den internationella klassifikationen av funktionstillstånd, funktionshinder och hälsa http://www.who.int/classifications/icfbrowser/?undefined&version=7 den 2009‐04‐01
2. Short Sensory Profile McIntosh, Miller & Shyu, 1999 in Scott D. Tomchek, Winnie Dunn i The American journal of occupational therapy, March/April 2007, volume 61, number 2.

62

63
5. Speech‐facilitating oral motor treatment of a suspected childhood apraxia of speech and oral apraxia in a 3 – year‐old girl. A case study
Birgitta Fog‐Poulsen, Physiotherapist at the Institut for Kommunikation og Handicap, Region Midt, Denmark
Abstract This paper describes the use of oral motor treatment of a suspected childhood apraxia of speech and oral apraxia in a 3 – year‐old girl. The oral motor treatment is a supplementary activity to the language and phonological therapy, carried out in co‐operation with the speech therapist. The aim is to improve eating and the ability to plan non‐speech movements with the purpose of imitating and producing speech sounds. The treatment is based on principles from theories of motor control and motor learning and Dynamic Temporal and Tactile Cueing (DTTC). It also takes the child’s cognitive, linguistic, social, emotional and motor development into account.
A multiple baseline is used. Treatment duration was 3 month. The non‐speech oral motor execution and praxis (motor planning and programming) were assessed by NOT‐S before and after treatment. The subject’s ability to voluntary plan non‐speech movement and voluntary imitate speech sounds were improved by the treatment. The results and the controversies associated with the use of oral motor treatment for children with speech problems are discussed.
Introduction
What is Childhood apraxia of speech (CAS) and Oral apraxia?
Children with speech problems form a heterogeneous group. For many children the difficulties are related to the cognitive and linguistic processes in the speech production. Some children seem to have difficulties, with the articulation, caused by problems at one or more of the levels of speech motor processing. In the speech motor processes the language formulation is transcribed by motor planning and motor programming, before the execution of movement, resulting in the acoustic output – the intelligible speech. These children have, despite no structural or functional abnormalities in the speech apparatus, inconsistent difficulties

64
initiating speech movements and problems with achieving and maintaining articulatory configurations. “Language and speech motor processes interact and are inextricably linked that they cannot be separated” (Caruso & Strand, 1999).
The American Speech‐Language‐Hearing Association (ASHA) provides definition of CAS in a position statement:
“Childhood apraxia of speech (CAS) is a neurological childhood (pediatric) speech sound disorder in which the precision and consistency of movements underlying speech are impaired in the absence of neuromuscular deficits (e.g., abnormal reflexes, abnormal tone). CAS may occur as a result of known neurological impairment, in association with complex neurobehavioral disorders of known or unknown origin, or as an idiopathic neurogenic speech sound disorder. The core impairment in planning and/or programming spatiotemporal parameters of movement sequences results in errors in speech sound production and prosody.”
The position also discusses the problem to differentiate CAS from other types of childhood speech sound disorders as phonological‐level deficits or neuromuscular disorders (dysartria) (ASHA, 2007).
Children with CAS have speech problems that depend on difficulties with praxis, meaning the “volitional movement patterns for the performance of a particular action, especially the ability to select, plan, organize, and initiate the motor pattern” (Shriberg et al., 2003).
Strand talks about the necessity of finding out if the primary contribution to the speech disorders is linguistic processing deficit or if one or more levels of motor processing are impaired. Often both motor and linguistic processing will be impaired and the treatment has to reflect on the relative contribution and the level of impairment. (Strand, Linköping, 2009).
In the literature you also read about difficulties to initiate and program oral non‐speech movements, described as Oral dyspraksi (Hartelius et al., 2008). A definition of Oral dyspraksi / apraxia provides the disorder as: A neurological deviation affecting volitional control of oral non‐speech movements without other observable symptoms such as pareses (Morley, Court, Miller 1954; Darley 1967), (McAllister, Linköping, 2009).
Dyspraxia/apraxia and Developmental Coordination Disorders (DCD)
In literature dealing with motor control and learning the terminology of motor disorders, such as dyspraxia / apraxia and Developmental Coordination Disorders (DCD) can be confusing. A study of the differential diagnosis of dyspraxia and DCD, conclude that in practice dyspraxia and DCD should be regarded as synonyms. They describe the motor problem as a developmental condition in the absence of any known neurological condition or intellectual impairment. It is an inability to plan, organise and coordinate voluntary movements. That results in fine and gross motor problems and/or speech difficulties (Gibbs et al., 2006). Several studies describe the co‐existence between specific language impairment and poor motor skill. The explanation is discussed in terms of shared cognitive processes or neuromaturational delay (Hill, 2001).
Strand differentiates between two main types of motor processing: the execution and the ability to plan movement (praxis). The assessment of Oral apraxia looks for problem with praxis for oral non‐speech movements, and should be differentiate from Dysarthria, which

65
shows execution problems, coursed by deviant neorumuscular conditions (Caruso & Strand, 1999).
Sugden and Hendersen (2007) have illustrated praxis as a solution to a movement problem. Their intervention system, named Ecological Intervention, is built upon the Cognitive‐Motor Approach and the success (or failure) of an intervention programme is a function of the dynamic interaction between the child, the environment and the task.
Sugden and Hendersen (2007) have also suggested a model for the three major components in motor planning and execution: ‐ sensory input, ‐ perceptual and cognitive processes, ‐ motor output processes. Intrinsic and extrinsic feedback is used to guide and improve performance. Conditions for automation and generalization are discussed (Sugden & Henderson, 2007).
Sensory stimulation and speech‐ motor control.
Different physiotherapy methods use sensory stimulation with a view to contributing motor control (Bader‐Johansson, 2003). The kinaesthetic and tactile information have a role in motor control in humans (Laszlo & Bairstow, 1985)
In Irene Johansson’s model for speech production she describes, the speech function as a result of processes between cortex, cerebellum, sub‐cortical structures and the periphery sensory‐ and motor systems. She talks about the importance of the control process and the role of feedback from the sensory system, especially the auditory, visually, tactile and proprioceptive / kinaesthetic systems The feedback is a important part of the learning process (Johansson, 1995,1996,1997).
Castillo Morales has developed a concept to facilitate movements by stimulating the sensory system. He talks about the relation between well coordinated oro‐facial function and clearly articulated speech (Morales et al.,1998). In a single case study building on these principles a positive result was reported with the use of a combination of intra‐oral sensory stimulation and electropalatography (EPG) in the treatment of a case with severe CAS (Lundborg & McAllister, 2007).
Children with CAS can also have other developmental problems.
Children with CAS are often seen having other problems together with speech problems, such as Cognitive and learning problems, including focusing and maintaining attention, Social Communication Difficulties, Behavioural Dysregulation, and other Oral Motor Problems (Teverovsky et al., 2009).
At The Speech & Hearing Institute in Århus, Denmark we work with groups of children with severe speech difficulties. We work as a team; speech therapist, physiotherapist, psychologist, neuropediatrician and have the possibility to give an intensive help with a program set up for 6 months or more. Our common interests are to help the children to learn and develop an intelligible speech. Some of the children also have oral motor problems and DCD in relation to the fine and gross motor functions.
The oral sensory stimulation and the learning of oral motor control is a part of the treatment, if there are difficulties with oral motor praxis and / or execution.
Can oral motor treatment, built on principles from knowledge of motor performance, motor learning and DTTC improve the oral‐motor function in eating, in voluntary planning of oral

66
non‐ speech movement and in voluntary pronouncing speech sounds in a three year old girl, who did not use spoken language at all?
Method
Case History
M. was 3:2 year when this study started. She had no verbal language and she was only using very few sounds, like /umm/ and /ah/. She communicated with handsigns and gestures. She communicated with her parents and reacted adequately to their questions, but was very passive in other situations outside the home.
M. had been seen by a speech therapist in March 2008. She had described M. as a girl with an adequate understanding of spoken language and having the desire to communicate. She had been a healthy child and had only had one episode of otitis media. There had been problems with breastfeeding and also with the transition to solid food. She had had no drooling problem.
The parents told that she had very limited babbling in early childhood and there has being and still are feeding problems. The fine‐ and gross motor development had been normal, but M. had always been a cautious child with poor initiative.
M. had been seen by a neuropediatrician in August 2008 and had been diagnosed with severe expressive dysphasia. The anamneses and the assessment of the oral structural, oral function and the motor speech production had made him suspect that the motor processing impairment was contributing to the speech disorders and he proposed the problem should be looked upon and treated as CAS. M had not dysarthria.
Despite her overall normal development she did not progress regarding speech production and she was referred to the team specialised in children with CAS at The Speech & Hearing Institute in November 2008. The first impression was a girl with poor mimic control, general difficulties to initiate and carry out purposeful voluntary movements, both for speech and gross motor function. When she managed to make a voluntary movement, for example rounding the lips to a blow position or jump with both feet, she could not maintain the position or movement pattern, not repeat it and continue a sequence of the movement. She had to see the activities several times and guiding by doing the activity simultaneously seemed to be a useful strategy when working with performance of voluntary gross motor skills. The parents told us that she spontaneously could execute the practised motor skills at home.
Procedure
M attended a little group with 4 children, 2 speech therapists, a psychologist and a physiotherapist. M got weekly treatment by speech‐ therapist and physiotherapist for three hours, during three months, with the participation of a parent or a pedagogue from the kindergarten. M started in the group in November 2008. In the period from March 2009 to June 2009 there was a special focus on the oral‐motor planning process. The target oral movement, articulation of speech sound and word should be practised at home and in the kindergarten.
In order to test the oral motor function and to establish a base‐line we used NOT‐S (Bakke et al., 2007).

67
Three consecutive assessments were made during a 2‐mounth period.
1. Assessment: December 2008. NOT‐S interview scores 3 and NOT‐S examination scores 5
2. Assessment: January 2009. NOT‐S interview scores 3 and NOT‐S examination scores 5
3. Assessment: February 2009. NOT‐S interview scores 3 and NOT‐S examination scores 5
There was no spontaneous improvement of M.´s ability to control voluntary oral‐motor praxis.
There were problems in the domains of: sensory function, habits, chewing and swallowing, facial expression, oral motor function, and speech.
A study, with the aim of collecting norm data for NOT‐S for children with typical development aged 3:0‐6:0 years, showed that children aged 3:0‐3:11 years can be expected a mean score of 1,41 ±0,94. M had got a total score of 8 points. A score of 3 points at this age indicates oro‐ facial‐ motor praxis problems (Gustavsson et al., 2007).
Treatment
The oral‐motor treatment had three components:
1. Sensory stimulation with an electric toothbrush and manual methods from the concept
of C. Morales.
2. Consciousness about the lips movements and volitional control of oral non‐speech
movements we started with the 4 basic skills: open the mouth, close the mouth, show
the teeth – smiling and round the lips. It was necessary to use guiding with tactile,
proprioceptive and visual stimulus. Also facilitating the movement with resistance.
3. Connect the position of the mouth with a volitional pronounced speech sound. M.
started with learning that the “open mouth” could say the vocal /a/ and closed lips ‐
/m/ and later rounded lips ‐ /u/ and smiling lips ‐ /i/.
The treatment session was about 20 minutes every time and the training movements, sounds and words were coordinated with the speech therapists training program. M. trained the same program daily at home and in kindergarten. We did the movements and pronounced the sounds simultaneous with M. in the first two months. She got feedback every time she tried to plan and execute an oral movement or sound. As M. was very interested in animals, we used toy animals that could make sounds, like /mu/, /mia/, /mæ/, /hi/, /øf/, /vov/. The animals repeated their sounds 3 times, and that stimulated M. to repeat her planning and execution. We played with the animals and encouraged M. to produce the different sounds many time during the sessions with both the speech therapist and the physiotherapist.
The children also had had lunch together, and we guided M to go on chewing and swallowing as she often stopped and just was sitting passive.

68
Results M. was retested with NOT‐S in June 2009 after the three months training period.
NOT‐S interview scored 1 and NOT‐S examination scored 2. The total score had improved from 8 to 3. NOT‐S in August 2009 scored 3 and showed that M had maintained the functions, as she had the same functions as in June 2009. She still took a long time to eat a main meal, but did not put too much food in her mouth. She could imitate, plan and execute the oral motor movements, except “lick her lips”, as she was not able to lift the tip of the tongue upwards. Before the treatment she had not tried to count out loud to ten, now she counted quietly to ten using the right vowels and some consonants.
The speech therapist told that M. was able to say single words together with her, but still vey quite and only words with one syllable. We could not make her say the words loud and sometimes she still only formed the word with her mouth, other times we heard M. saying the word correct.
Her parents told us that M. often played with the pictures of the trained lip positions, and voluntary showed them that she can say the corresponding sound quit loud and clear. As a new skill, she has started to voluntary move the tip of the tongue. They see more facial expressions when she is playing. She said the target words, given by the speech therapist, when playing with her parents.
The planning and execution of oral non‐speech movements, speech sounds and the few words she said were still marked by visible groping behaviour.
Discussion The aim with the case study was to see if a oral motor treatment, built upon theories of Motor Performance, Motor learning and DTTC could improve the oral motor function in eating, in voluntary planning non‐ speech oral movement and in voluntary pronouncing speech sounds in a three year old girl, who did not use spoken language at all?
If M. has CAS, the level of the problems in the motor planning processes probably is considerably. NOT‐S showed difficulties in imitating oral non‐speech movements and she had had and still has feeding problems. M. does not have dysarthria, so the difficulties are related to praxis.
It is difficult to find the exact diagnose in a little child without verbal language. To stimulate the speech you have to work with both the communication and the language and the motor praxis.
It seemed that M., through sensory simulation and guiding to movements, found a way to planning, programming and executing oral non‐ speech movement. She even learned to say the corresponding vowel and consonant; /a/, /u/, /i/, /m/ and /h/. Later the animal sounds; /mu/, /mæ/, /mia/…
Working with the motor processing, stimulating the three major components in motor planning and execution: ‐ sensory input, ‐ perceptual and cognitive processes, ‐ motor output processes, and with a clear aim for the child and the environments has been successful. Intrinsic and extrinsic feedback has been used to guide and improve performance. NOT‐S showed impairment in imitating non‐speech oral movements. Her ability to imitate and say

69
sounds and short words has been improved by using DTTC. The help to initiate the movement or speech movement has been successful.
It has been interesting to compare methods of Cognitive Motor Training with DTTC.
There are a lot of different programs for Nonspeech Oral Motor Exercises (NOME). In an article, written by Watson et al., 2008, they discuss the evidence for NOME’s effect in relation to speech production and the confusion between “speech facilitating oral motor techniques and non‐speech oral motor techniques”. The way we have treated M. has been mainly using “speech facilitating oral motor techniques”, however the intervention have also included non‐speech items such as sensory stimulation and simple lips movements to enhance the patients awareness of the oral structures and improve volitional control.
Through the close cooperation between the physiotherapist and the speechtherapist, M. has been conscious about, why she has to learn the oral non‐speech movements and they have been linked to the speech production. Our experiences are that Children with Speech Sound Disorders (SSD) or expressive dysphasia do not have oral praxis difficulties showed in NOT‐S.
M’s development is very slow and we have discussed her problems with the neuropediatrician and the psychologist in the purpose to find out if there are other developmental problems, that can explain the poor speech production, the tendency to stop in the middle of an activity and the big difference in her performance at home and at The Speech & Hearing Institute. In the near future M. will have a MR‐scanning, an EEG and a cognitive test.
Beside the stimulation to improve the speech‐motor process through training by playing, we will continue to work on hand‐signs to communicate her wishes and develop the impressive language.

70
References American Speech‐Language and Hearing Association (ASHA). (2007). Childhood Apraxia of Speech,
Position Statement. Available from www.asha.org/policy. Downloaded 2009‐05‐01.
Bader‐Johansson, C. (2003). Grundmotorik. Studentlitteratur. Lund.
Bakke M., Bergendal B., McAllister A. Sjögren L., Åsten P. (2007). Nordisk Orofacial Test – Screening NOT‐S. Avialable from www.mun‐h‐center.se. Downloaded 2009‐05‐01.
Caruso A.J. and Strand, E.A. (1999). Clinical Management of Motor Speech Disorders in Children. Thieme, New York, Stuttgart.
Gibbs J., Appleton J., Appleton R. (2006). Dyspraxia or developmental coordination disorders? Unravelling the enigma. Available from www.archild.com. Down‐loaded 2009‐05‐01.
Gustavsson, C., Skoglund, C., Thelin, H., (2007). Normering av Nordiskt Orofacialt Test‐Screening (NOT‐S) för barn I åldrarna 3 till 6 år. ( Norm data for the Nordic Orofacial Test‐Screening (NOT‐S) for children aged 3 to 6 years) Department of clinical and experimental medicin, division of speech and language pathology, Linköping University, Sweden. Avialable from www.mun‐h‐center.se. Downloaded 2009‐05‐01.
Hartelius, L., Nettelbladt, U., Hammarberg, B. (2008). LOGOPEDI. Studentlitteratur. Lund
Hill E. L., Non‐specific nature of specific language impairment: a review of the literature with regard to concomitant motor impairments. (2001), International Journal of Language & Communication Disorders, 36(2), 149–171, 2001.
Johansson, I. Tal‐,mun och bettfunktion hos barn med Downs syndrom. Arbetsrapport nr. 1/1995, 2/1996, 3/1997. Rrefereret i Oralmotorisk funktion og funktiosvanskeligheder hos børn med Downs syndrom. Lene Lykkebo (2001). Dansk Audiologopædi, dec.2001.
Lundborg, I., McAllister, A. (2007). Treatment with a combination of intra‐oral sensory stimulation and electropalatography in a child with severe developmental dyspraxia. Logopedics Phoniatrics Vocology, 32(2), 71–9.
McAllister A. (2009). History and Controversies of Childhood apraxia. Handouts, Seminar at Linköping University, Speech Language Pathology March 12, 2009.
Morales, R. C., Brondo J., Haberstock B. (1998). Orofacial regulationsterapi. Studentlitteratur. Lund
Shriberg L., Campel T. F., Karlsson H.B., Brown R.L., McSweeney J.L., Nadler C. J.. (2003). A diagnostic marker for childhood apraxia of speech: the lexical stress ratio, Clinical Linguistics & Phonetics, 17(7), 549–574, (2003).
Strand E. A. (2009), Oral and Verbal Apraxia in Children: Assessment, Diagnostics; Therapy/Assessment and Differential Diagnosis. Handouts, Seminar at Linköping University, Speech Language Pathology March 12.
Sugden D. A., Henderson S. E. (2007). Ecological Intervention for Children with Movement Difficulties. Harcourt Assessment.
Teverovsky, E.G., Ogonowski Bickel, J., Feldman, H.M. (2009). Functional characteristics of children diagnosed with Childhood Apraxia of Speech. Diability and Rehabilitation, 31(2), 94–102.
Watson, M. M., Lof G. L. (2008). Epilog: What We Know about Nonspeech Oral Motor Exercises. Seminars in speech and language, 29(4), 2008. Thieme medical Publishers, New York.

71
6. Oral and Verbal Motor Function in a child with childhood Apraxia of Speech
Helena Björelius, MSc, Department of speech and language pathology, Danderyd University hospital, Stockholm
Abstract The aim of this study was to describe a child with childhood apraxia of speech in terms of oral and verbal motor function. The results of this study show that the child with CAS had lower results compared with standardized means of typically developed children (VMPAC) in terms of focal oromotor control, sequencing maintenance control and connected speech and language control. The interpretation of VMPAC shows that the most prominent problems seemed to be associated with sequencing maintenance control. The articulatory movements involved in sequencing maintenance control items are possibly part of the characteristic features for CAS confirmed by earlier research. These findings make VMPAC interesting to use among other speech and language assessments and especially considering CAS.
Introduction Childhood apraxia of speech (CAS) is a speech disorder characterized by deficits in speech motor planning for sequenced speech output in the absence of overt neuromuscular impairment (Hall, Jordan & Robin, 1993; Davis, 2003).
The diagnosis CAS is much disputed. The general ambiguity of the diagnostic criteria for CAS is evident from a report by Forrest (2003), who identified 50 different characteristics that were included in the diagnoses of CAS made by 75 speech‐language pathologists.
The search for an instrument with which clinicians can differentiate between children with CAS and children with other speech delays (SD) is a very important matter that has been thoroughly addressed by Shriberg, Aram and Kwiatkowski (1997 a, b and c).
The American Speech and Hearing Association (2007) recently reached consensus on three features that have diagnostic validity: (1) inconsistent error production on both consonants and vowels across repeated production of syllables and words, (2) lengthened and impaired co‐articulation transitions between sounds and syllables, and (3) inappropriate prosody.
The controversy about diagnosing CAS makes the choice of intervention even more of a challenge for the SLP (Speech‐Language Pathologist) clinician. In a review in the Cochrane Collaboration (2008), Morgan and Vogel found that there is a critical lack of well‐controlled

72
treatment studies addressing treatment efficacy for CAS, making it impossible to draw conclusions about which intervention is most effective for treating CAS in children or adolescents.
Etiology
Researchers have not yet established the underlying cause of CAS (Davis, Jacks & Marquardt 2005). As with many other diagnoses, CAS probably includes an inheritable factor. One theory that is gaining ground stems from discoveries of mutations in the FOXP2 gene located in chromosome 7q31. A possible genetic disruption in the FOXP2 gene has been found in the three‐generation KE family; all the members of this family who are affected by a pronounced verbal dyspraxia have a mutation of the FOXP2 gene (Vargha‐Kadem, Watkins, Price & Ashburner, 1998; Vernes, Nicod, Elahi & Coventry, 2006; Lennon, Cooper, Peiffer & Gundersson, 2007).
The motor deficit theory proposes a motor programming deficit in the light of the inconsistency in repeated utterances and the slow speaking rate found in children with CAS (Strand & McNiel, 1996; Maasen, Nijland & van der Meulen, 2001; Nijland, & Maasen, 2003).
Test for oral and verbal motor function VMPAC
In Sweden, no standardized test is available for assessing presumed CAS. In a review, McCauley and Strand (2008) recently demonstrated that only a few tests are diagnostically dependable for motor speech disorders. Verbal motor production assessment for children (VMPAC) (Hayden & Square 1999) was the only test that met McCauley and Strand’s operational definition on adequate norms. It also had test‐retest and interexaminer reliability as well as content and construct validity. VMPAC is designed to aid in the systematic assessment of the neuromotor integrity of the motor speech system in children aged 3 through 12 years who have speech production disorders. It is not a test of articulation or language but a step‐by‐step assessment of the speech production system at rest and when engaged in vegetative and volitional non‐speech and speech tasks. Speech and language pathologists can use the VMPAC in determining whether or not a motor disruption such as dysarthria or CAS is a dimension of a child’s speech production disorder (Hayden, 1994; Hayden & Square, 1999). The author of this study has therefore chosen VMPAC as a test for assessing oral and verbal motor function for the child with CAS.
Aim
The aim of this study is to compare oral and verbal motor functions from a child with CAS with standardized mean (VMPAC) from typically developed children within the three subtests of VMPAC; focal oromotor control; sequencing maintenance control and connected speech and language.
The aim is also to give a qualitative description of errors made by a child with CAS in terms of oral and verbal motor functions interpreted from Verbal motor production assessment for children (VMPAC).

73
Material and Method The child included in this study also participated in a thesis study by Helena Björelius Hort (2009).
Case history
Child (C) age 6 was given the diagnose CAS (R48.2) in May 2008. Before the diagnose CAS C had been diagnosed with a phonological disorder (F80.0A). C has been treated with speech therapy for patients with phonological disorders during 18 sessions between age 3:6 to 5:0 by two different speech and language pathologist at Karolinska University Hospital, Huddinge. C did not make the progress that was expected when treating children with phonological disorders and therefore new investigations were made which lead the diagnose CAS. From then C has been treated with multisensory techniques. In all other aspects C has a typical development.
Procedure
C was seated on one side of a table and a camera was positioned at an appropriate angle on the opposite side. The examiner SLP student Helena Björelius Hort (HBH) was seated beside the table to assess the child. The assessments took approximately 20 minutes. The assessment was video recorded (Digital video, Canon, F5100) so as to be able to certify the test results. After watching the video recordings, the results from the VMPAC were processed by HBH.
Material
The Verbal Motor Production Assessment for Children, VMPAC (Hayden & Square 1999), was used to assess non‐speech and speech oromotor control. The speech tasks consist of linguistically meaningful and non‐meaningful vocal production. The VMPAC uses a form that lists all the items for each subtest. It provides information about how to conduct the assessment and what criteria each item needs. The scores for the child are entered directly on the form. The VMPAC contains five subtests, organised into three main areas and two supplementary areas. All subtests have standardized norms, in percent with the standard deviation, for 3, 4, 5, 6 and 7‐12 years of age. In the VMPAC form there are profiles included for each age group with standardized mean, percentile 95 and 5. The clinician transfer’s the percentage results from each subtest into the profile.
The main areas are: Global Motor Control, Focal Oromotor Control and Sequencing Maintenance Control. The supplementary areas are Connected Speech and Language Control and Speech Characteristics.
The subtests that were implemented in this study were:
Focal Oromotor Control area consists of 46 items and assesses the child’s volitional oromotor control for three individual subsystems: mandibular, labial‐facial, and lingual control, both in isolation and in combination with each other. The items comprise non‐speech oromotor movements (17 items) and speech oromotor movements (29 items). If the child makes an articulatory error in the production of a vowel and consonant, they are scored minus 1 point when the test manual maximum has 2 points.

74
Sequencing Maintenance Control area consists of 23 items, constructed to assess the child’s ability to produce non‐speech and speech movements in the correct sequential order (Sequence Maintenance). The items comprise both non‐speech and speech movements. They have combinations of Double and Triple Oromotor‐Phoneme Movement sequences in Word Sequences and Sentences. The tasks are the same as in the Focal Oromotor Control area and the clinician examines the child to determine whether or not the correct order or sequence of movements is produced. Sequencing Maintenance Control scores the child’s ability to produce non‐speech and speech movements in the correct sequential order, with maximum 2 points and minimum 0 points
Connected Speech and Language Control area assesses the child’s motor control as it varies with the complexity of language formulation. The area contains 5 items. The child formulates a story that corresponds to four sequenced pictures. The precision and coordination of jaw, lip and tongue movements and their interaction, such as co‐articulation, are closely observed during the task. Connected Speech and Language Control in spontaneous speech scores the child’s abilities in Motor Control, with maximum 7 points and minimum 0 points, and the presence or absence of correct spoken language (Syntax), with maximum 6 points and minimum 0 points.
Results Figure 1 below presents an example of a Standardization Sample profile from the VMPAC (age 6). In figure 1 the results for the child with CAS show a lower level in percent than seen in standardized mean for all three subtests. In focal oromotor control and connected speech and language the child’s percentage level is in percentile 5.
In sequencing maintenance control the level difference is considerably lower than standardized mean.
Figure 1. Shows standardization sample profile age 6 from VMPAC’s form with percentile 5, 95, standardized mean and result from child with CAS; in focal oromotor control (FOMC) (85%); sequencing maintenance control (SEQMC) (50%) and connected speech and language control (CS&LC) (87%).

75
Qualitative description of errors made by the child with CAS
Focal oromotor control
The child made only two errors on single and multiple non‐speech oromotor tasks. One error was jaw assistance when licking around the lips and the other was difficulties to touch the upper lip only with the tip of the tongue.
No errors were made when producing a single (/a/, /p/). In double oromotor‐phoneme movement with target phoneme (/a‐u/) the child produced /aeu/ by vowel distortion towards schwa phoneme and also lengthening of vowels.
In triple oromotor‐phoneme movement the child made many errors. In the target phonemes /u‐i‐a/ the child produced /euea/ by vowel distortion towards schwa, lengthening vowels, and adding a schwa phoneme. In the target phoneme pa‐ta‐ka/ the child was not able to find the dental articulatory position and produced /pa‐ka‐ka/ which in phonological terminology would be described as assimilation. In the word and sentences task the target words for one item were /bi‐de‐kö/ and the child interchanged to /bi‐di‐kä/. This showed vowel distortion or assimilation.
Sequencing maintenance control
The child made many errors and signs of groping when producing double and triple oromotor movements in a sequence with target utterance as /u‐i‐a,‐u‐i‐a‐u‐i‐a‐u‐i‐a/ or /pa‐ta‐ka‐pa‐ta‐ka‐pa‐ta‐ka‐pa‐ta‐ka/. The vowel production interchanged to /euea/ through the whole sequence and consonant production interchanged to /pakaka/ through the whole sequence see explanation under the previous section; focal oromotor control. In words and sentences difficulties with sequencing maintenance control was seen mainly leaving target words out for example in /bit, bok, båt, bak/ the child produced /bik, bok, bak/. The child did not have the capacity to change between velar and dental phonemes, all articulation had backed muscle bias pattern (backing).
Connected speech and language
The child made many errors in spontaneous speech and was very difficult to understand. The criteria’s that was chosen for the result was (referred from VMPAC form); full use of jaw, lip and tongue but with backed muscle bias pattern (backing). The child replaced all dental articulation with velar fonems, /t/ to /k/.
Discussion The results of this study show that the child with CAS had lower results compared with standardized mean of typically developed children in terms of focal oromotor control, sequencing maintenance control and connected speech and language control (Fig. 1). The qualitative results show that C did not have any problems with non‐speech oromotor movements which mostly are part of subtests focal oromotor control and a few are included in sequencing maintenance control. C had limited repertoire of vowels (vowel distortion) mainly towards schwa phoneme and showed signs of groping when producing a double or triple phoneme movement sequence as well as in word sequence and sentences. Similar articulatory problems occurred when C was asked to produce a sequence of multi‐syllabic utterances for example /pa‐ta‐ka/ were C also had constant backing patterns. The most

76
prominent problems seemed to be associated with sequencing maintenance control and spontaneous speech produced in connected speech and language control. The articulatory movements involved in sequencing maintenance control are possibly the part of VMPAC items that are able to capture the characteristic features of CAS confirmed by earlier research (Forrest, 2003; Morgan & Vogel, 2008).
One question is if the items in focal oromotor control subtest with non‐speech oromotor tasks support findings for CAS? McCauley & Strand (2008) consider the value of non‐speech oral motor exercises (NSOMEs) for children with CAS and discuss whether there are non‐speech oral motor tasks that in general are difficult to perform for children with CAS. The child participating in this study had almost no errors in non‐speech oromotor movement tasks and probably not any praxis dysfunctions orally.
It is not possible to be totally sure after just assessing C with VMPAC that the articulatory problems found could be or be a part of phonological processes. Also the scale used in VMPAC only has 2 or 3 levels (0, 1 and 2) which made the results less detailed. Even if VMPAC assessment includes some non‐speech oromotor tasks and has other weaknesses mentioned above most items included in this study possibly have the ability to grasp the special characteristics of CAS. These findings make VMPAC interesting to use among other speech and language assessments and especially considering CAS.
Conclusion The results of this study show that the child with CAS had lower results compared with standardized mean of typically developed children in terms of focal oromotor control, sequencing maintenance control and connected speech and language control. The qualitative analyses show that the most prominent problems seemed to be associated with sequencing maintenance control and spontaneous speech produced in connected speech and language control.

77
References American Speech‐Language and Hearing Assiciation (ASHA) (2007). Childhood Apraxia of
Speech [Technical Report]. Available from www.asha.org/policy (accessed May 2008), 1–74.
Björelius Hort, H. (2009). Oral and Verbal function and Manual and Overall Performance in Children with Developmental Apraxia of Speech. Magisteruppsats, logopedprogammet, Institutionen för klinisk vetenskap, intervention och teknik, Karolinska Institutet Stockholm.
Davis, B L, Jacks A, Marquardt, T P. (2005). Vowel patterns in developmental apraxia of speech: three longitudinal studies. Clinical Linguistics & Phonetics; 2005, 19(4), 249–274.
Forrest, K. (2003). Diagnostic criteria of development apraxia of speech used by clinical speech‐ language pathologists. American Journal of Speech‐Language Pathology, 12(3), 376–380.
Hall, P K, Jordan L S, Robin D A. (1993). Developmental apraxia of speech: Theory and clinical practice. Austin: TX: Pro‐ed.
Hayden, D A. (1994). Different Diagnoses of Motor Speech Dysfunction in Children. Clin Commun Disord. June, 4(2), 119–41.
Hayden, A., & Square, P. (1999). VMPAC, Verbal Motor Production Assessment for Children. San Antonio, TX: The Psychological Corporation.
Lennon P A, Cooper M L, Peiffer D A, Gundersson K L; Patel A, Peters S, Cheung S W, BacinoC (2007). A. Deletion of 7q31.1 supports involvement of FOXP2 in language impairment: Clinical report and review.
Maasen B, Nijland L & van der Meulen S J. (2001). Accustic studies to determine syllable planning and motor programming deficits in DAS. In B. Maasen, W. Hultstijn, R D HFM Peters & PHHM, van Lieshouut (Eds), Speech motor control in normal and disordered speech (pp. 347–350). Nijmegen, The Netherlands:Uitgeverij Vantilt.
McCauley, R & Strand, E. A (2008). Review of Standardized Tests of Nonverbal Oral and Speech Motor performance in Children. American journal of Speech‐Language Pathology, Vol. 17, 81–91.
Morgan, T, Vogel, A P, (2008). Intervention for childhood apraxia of speech (Review). The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Nijland, L, Maasen B. (2003). Evidence of Motr Programming Deficiets in Children Diagnoses With DAS. JSLHR. Vol. 46. 437–450.
Shriberg, L D, Aram D M, Kwiatkowski J. (1997). Developmental Apraxia of Speech: II. Toward a Diagnostic Marker. JSLHR, Vol. 40, 286–312.
Strand E A & McNiel M R. (1996). Effects of length and linguistic complexity on temporal acoustic measures in apraxia of speech. Journal of Speech and Hearing Research, 39, 1018–1033.
Vargha‐Kadem F, Watkins KE, Price CJ, Ashburner J, Alcock KJ, Conelly A, Frackowiak RS, Friston KJ, Pembrey ME, Mishkin M, Gadian DG, Passingham RE. (1998). Neural Basis of an inherited speech and language disorder. Proceeding of National Academy of Science USA, 95(21), 12695–700.

78
Vernes S C, Nicod J, Elahi F M, Coventry J A, Kenny N, Coupe A M, Bird LE, Davies K E, Fisher S E. (2006). Functional genetic analysis of mutations implicated in a human speech and language disorder. Hum Mol Genet. Nov. 1, 15(21), 3154–67.

79
7. Verbal Dyspraxi och Alternativ och Kompletterande Kommunikation (AKK) – en forskningsstudie
Marlene Andersson, Drottning Silvias Barn‐ och Ungdomssjukhus, Göteborg
Sammanfattning Föreliggande litteraturöversikt har genomförts med syfte att få en bild kring behov och användande av Alternativ och Kompletterande Kommunikation (AKK) för barn med diagnosen verbal dyspraxi. Målet har varit att få fram kunskap via litteratur, forskning samt även yrkesverksamma logopeders erfarenhet för att få en bild av hur barnens tal‐ , språk‐ och kommunikation kan underlättas och utvecklas med hjälp av kommunikativa hjälpmedel vid en grav talstörning. Litteratur och forskning visar samstämmigt på att både lågteknologiska och högteknologiska hjälpmedel är till stor nytta för barnen och dess omgivning. Detta gäller i kommunikativa samtalssituationer likväl som vid deras språkutveckling och talutveckling. Parallellt med en intensiv träning av talet bör barnet erbjudas alternativa sätt att kommunicera och utveckla sitt språk.
Bakgrund Verbal dyspraxi innebär svårigheter att viljemässigt initiera talrörelser, svårigheter att uppnå, känna av och upprätthålla artikulatoriska positioner samt svårigheter med sekvensering av ljud (Hartelius & Lyons, 2008). Ofta förekommer finmotoriska svårigheter i samband med verbal dyspraxi (Cumley & Swanson, 1999). Ett intensivt arbete med att förbättra den naturliga talproduktionen är av största vikt och det finns flera olika behandlingsmetoder (Beukelman & Mirenda, 1998). Artikulationsterapi är speciellt viktigt i de tidiga utvecklingsåren när talets utveckling är svårt att prognostisera (Weitz, Dexter, & Moore, 1997).
Då behandlingsinsatserna är stora och utvecklingen går långsamt (Hartelius & Lyons, 2008) är det ofta stora svårigheter för barnet att kommunicera med sin omgivning. Barn med grav verbal dyspraxi, vars tal inte är förståeligt i den dagliga kommunikationen, kan komma att bli kandidater för ett kompletterande kommunikationssätt (Beukelman & Mirenda, 1998). Behovet av ett alternativt och kompletterande kommunikationssätt är således stort.
Att införa ett alternativt kommunikationssätt kan många gånger vara svårt av flera anledningar. Av erfarenhet är kunskapen bland föräldrar och omgivning varierande och det kan ta tid att förstå hur stora barnets svårigheter är. Talet betraktas ofta som det sätt man vill kommunicera på, även för personer med nedsatt talförmåga (Weitz et al., 1997).

80
De barn som har ett svårförståeligt tal bör få både behandlingsinsatser för talet samtidigt som de erbjuds alternativa och kompletterande kommunikationstekniker.
För barn med verbal dyspraxi kan man ibland härleda deras sena språkliga utveckling till deras oförmåga att använda språket via sitt tal som små. Deras språkförsening är ett högt pris att betala under tiden som man väntar på att talet ska förbättras naturligt eller via terapi. Det är således av stor vikt att man erbjuder barn med verbal dyspraxi olika AKK från tidig ålder så de kan leka/utforska språket (Beukelman & Mirenda, 1998).
Vikten av en fungerande alternativ kommunikation för barn och ungdomar med motoriska talsvårigheter lyfts fram i litteraturen som mer än bara en möjlighet att kompensera för sina svårigheter, det är även en möjlighet att samtala med sin familj och sina vänner och delta i olika sociala sammanhang på ett mer fullständigt sätt (Caruso & Strand, 1999). Samma författare (1999) för fram vikten av en grundlig genomgång av barnets kommunikativa miljö och dess möjligheter samtidigt som det är av största vikt att titta på barnets olika förmågor såsom kognition, finmotoriska svårigheter och inte minst grad av talsvårigheter. Många barn med verbal dyspraxi har svårigheter med exakta motoriska rörelser i armar och händer, vilket direkt påverkar förståeligheten vid deras teckenanvändande (Cumley & Swanson, 1999). Enligt Caruso och Strand (1999) bör man arbeta tillsammans med en AKK specialist då insatserna för barnen med svår talsvårighet är extremt komplicerade. (En AKK specialist i Sverige kan väl närmast vara en konsult på Hjälmedelscentral eller logoped inom habilitering som arbetar mycket med alternativ kommunikation). Beslutet att implementera AKK kräver således en omfattande tal‐ och språkbedömning, perioder med terapi, och frekventa utvärderingar av den integrerade AKK metoden till den övergripande kommunikationsplanen (Weitz et al., 1997).
Den utmaning som möter kliniker som arbetar med barn med verbal dypraxi är deras komplexa kommunikation, sociala, emotionella och akademiska behov. Ett AKK interventionsprogram kan tillhandahålla en möjlighet att underlätta utveckling av den kommunikativa kompetensen. Ett multimodalt AKK system ger personen ett varierat kommunikativt val såsom tal, gester, tecken, lågteknologiska symbolkartor och högteknologiska talapparater (Cumley & Swanson, 1999). Många barn med grav språkstörning behöver ett alternativt och kompletterande kommunikationssätt (Binger, Berens, Kent‐Walsh, & Taylor, 2008) och det finns idag många olika alternativ att välja på som är antingen lågteknologiska eller högteknologiska (Caruso & Strand, 1999).
Barn med verbal dyspraxi kan behöva AKK strategier som ett komplement eller för att stärka språkutvecklingen. AKK är inte menat att vara ett system som ska ersätta, utan ska användas tillsammans med den förmåga man har att tala och skriva. Barnen behöver öva för att förbättra både sitt tal samt även den alternativa kommunikationen till dess talet blir det primära kommunikationssättet (Weitz et al., 1997). För att barnet ska utveckla sitt språk på bästa sätt är det av största vikt att kontinuerligt utvärdera dess förmågor och användandet av AKK (Caruso & Strand, 1999).
En längre beskrivning i Augmentative and Alternative Communication (Beukelman & Mirenda, 1998) tar upp tre förmågor som barnet med verbal dyspraxi kan behöva i olika kommunikativa situationer. Dels behövs olika sätt att ge information kring ämnet man vill prata om. Ofta använder barnen sitt tal, men kan behöva någon form av AKK som underlättar när man vill byta ämne och för att underlätta för samtalspartner att förstå snabbare och inte behöva gissa inom vilket ämne barnet nu vill prata. Strategier att förtydliga och reparera är en viktig förmåga och innebär exempelvis repetition, omformulering, lägga till eller ändra

81
kommunikationssätt, tecken samt kroppsspråk. Författarna beskriver även att barnet behöver lära sig att ta beslut när och i vilka situationer som de olika kommunikationssätten såsom tecken och talapparater ska användas.
Det är flera faktorer som är utmärkande gällande AKK som gör det till ett naturligt inslag i terapi för barn med verbal dyspraxi. Vanligt att barnen har en diskrepans mellan impressivt och expressivt språk. AKK tillåter barnen att kontinuerligt utveckla språkliga förmågor samtidigt som den ger dom ett alternativt expressivt språk. De expressiva syntaktiska förmågorna kan utvecklas genom AKK vilket innebär att när talet förbättrats kan dessa förmågor överföras till talad kommunikation (Weitz et al., 1997).
Vid införandet av AKK är det av stor vikt att försäkra oss om att våra insatser leder till en bättre fungerande och meningsfull kommunikationsförmåga. Barn med språk‐ och talstörning är ofta mer olika än lika (Weitz et al., 1997) vilket bör beaktas då man inför diverse tecken, symboler, talapparater. AKK kan användas som en metod till att öka talet samtidigt som det används som en kompletterande kommunikationsmetod, att AKK kan vara en kortsiktig strategi till dess talet når en acceptabel nivå av förståelighet eller så kan det vara en långsiktig strategi att bygga upp och bibehålla en effektiv kommunikation. Enligt Weitz et al (1997) kan AKK även vara ett komplement i olika situationer. AKK hämmar inte utveckling av talet utan är en form av stöd och hjälp till användandet av talet i de tidiga utvecklingsåren. När man presenterar ett AKK förslag till föräldrar med ett barn med verbal dyspraxi är det viktigt att komma ihåg den starka önskan som föräldrar ofta har att deras barn ska prata (Beukelman & Mirenda, 1998; Weitz et al., 1997). När professionella först förslår användande av AKK metoder, kan föräldrar ofta känna att man ger upp att barnet ska tala eller att deras barn aldrig kommer att tala. Att samtala med föräldrarna är ofta ett första steg i att introducera AKK. AKK är en terapiform för barn med verbal dyspraxi och i artikeln av Weitz et al (1997) föreslås ett utbildningsprogram både gällande dyspraxi samt AKK till föräldrar/omgivning.
För icketalande personer eller personer med begränsat tal som ska förvärva lingvistiska kunskaper, kan ett AKK system vara till hjälp att strukturera de kommunikativa meddelandena (Velleman, 2003 ; Weitz et al., 1997). För personer med grav talstörning kan ett AKK system användas som en väg till mer komplexa kommunikativa samspel (Weitz et al., 1997). I en studie som man refererar till i Augumentative and Alternativ Communication (Beukelman & Mirenda, 1998) gjord av Cumley 1997 ser man att barn med de största talsvårigheterna använde sina talapparater i större utsträckning än de barn med lättare svårigheter som främst använde tecken som ett stöd till sitt tal.
Ett alternativt kommunikationssätt bör åtminstone innehålla tecken samt visuella symboler. Lågtekonologiska kommunikationsböcker är ofta användbara liksom talapparater. Fördelen med de sistnämnda alternativen är att dessa är lättare att förstå för utomstående än vad det är att förstå tecken (Beukelman & Mirenda, 1998)
Metod Litteratursökning via Universitetsbibliotek. Sökning av artiklar gjordes i april 2011 via PubMed, SpeechBite, Informa healthcare, Google Scholar samt via den rekommenderade litteraturen från aktuell kurs; Oral and verbal apraxia in children. Tillhandahålla frågeformulär till yrkesverksamma logopeder som därefter kommer sammanställas.

82
Ett kortare frågeformulär, se bilaga 1, överlämnades till 15 yrkesverksamma logopeder i Göteborgsregionen som samtliga arbetar inom barnlogopedi. Svaren lämnades anonymt via postfack eller mailades.
Resultat Vid sökning på SpeechBite användes sökorden ’apraxi’ samt ’augmentative’ för barn. Resultatet av den sökningen gav två artiklar: “The Effects of Aided AAC Interventions on AAC Use, Speech, and Symbolic Gestures” från 2008 samt artikeln “The use of digital voice output device to facilitate language development in a child with developmental apraxia of speech: a case study” från 2001.
På PubMed gjordes sökningar i MeSH där kriterierna har varit verbal dyspraxi samt Alternativ och Kompletterande Kommunikation (AKK). Här användes MeSH termerna Apraxias and SignLanguage vilket gav ett resultat på 9 artiklar som dock inte var relevanta. Sökning gjordes även med MeSh termerna Communication Aids for Disabled and Apraxias vilket gav 5 icke relevanta artiklar. Inga artiklar framkom vid avancerad sökning på PubMed.
Artiklar söktes även via Google Scholar med sökorden Verbal apraxia of speech and AAC. Resultat gav 594 träffar, dock var långtifrån alla relevanta. Via Google Scholar fann jag flera artiklar som varit till hjälp i min efterforskning kring AKK hos barn med verbal dyspraxi. Några av artiklarna publiceras via InformaHealthCare medan andra hämtades via VgRegionens sidor.
Även i The Cochrane Library söktes artiklar i ämnet med sökorden Communication Aids for Disabled. Inget resultat då båda sökorden användes. Vid enbart sökning med apraxias blev det tre träffar varav en aktuell ”Intervention for childhoods apraxia of speech”. Vid enbart sökning med Communication Aids for Disabled blev det nio träffar, dock ej relevanta för denna uppsats.
Resultat, studie 1
I en studie från USA (Cumley & Swanson, 1999) med titeln “Augmentative and alternative communication options for children with developmental apraxia of speech: three case studies” har man fokuserat på tre fall där barnen har fått diagnosen Developmental Apraxia of speech eller misstänks ha diagnosen. De tre barnen har ett svårförståeligt tal och deras funktionella kommunikation har inte visat på några större framsteg under behandling som fokuserat på artikulatoriska färdigheter samt tecken. För att förbättra barnens kommunikativa färdigheter infördes behandling med AKK. Effekterna av dessa behandlingar för varje enskilt barns språk, kommunikation och sociala och akademiska utveckling presenteras i artikeln. Primärt mål med interventionsprogrammet i studien var att tillhandahålla framgångsrika kommunikativa strategier i hemmet, på skolan och i samhället. Dessutom, de kommunikativa strategierna tillhandahölls till familjemedlemmar, kamrater och skolpersonal så att de kunde ge den kommunikativa support som behövdes för att upprätthålla barnets kommunikativa samspel. Resultatet av dessa tre fall visar på att insatser med kombinerad AKK är ett tillvägagångssätt som kan vara genomförbart för barn med verbal dypraxi. En metod med kombinerade AKK insatser ger barnen bättre möjligheter till kommunikativa framgångar och en flexibilitet vad gäller initiering, delta i och reparera kommunikativa sammanbrott. Som visat sig vid dessa tre studier är det viktigt att insatserna som planeras balanserar mellan talbehandling och AKK insatser. Det rapporterades av föräldrar/omgivning att negativt beteende utvecklades eller ökade när barnen inte hade ett effektivt sätt att uttrycka sig på.

83
Resultat, studie 2
Fallstudien ”The use of a digital voice output device to facilitate language development in a child with developmental apraxia of speech: a case studie” från Sydafrika (Bornman, Alant, & Meiring, 2001) studerar språk och kommunikation hos ett barn med diagnosen verbal dyspraxi. I introduktionen till artikeln tar författarna upp flera saker som även framkommit i litteraturen. De skriver att en ökad vilja att delta i aktiviteter, en ökad koncentrationsförmåga, en minskad hyperaktivitet, en ökad självkänsla, en ökad självständighet samt bättre prestation i klassrummet till följd av införandet av talapparat är väl dokumenterat. De nämner även att ett AKK system inte reducerar en persons motivering att kommunicera verbalt. AKK brukar tillhandahålla större motivation till att börja använda talet i kommunikativt syfte och underlätta talutvecklingen. Syftet med införande av AKK är således att uppmuntra talet och inte hämma det. Det är väsentligt att barn med verbal dyspraxi startar tidigt med att använda AKK, så att de får möjlighet att använda språket och börja ’leka’ med det. De tre barn som är med i denna studien är i låg‐ mellan‐ samt högstadieåldern. Resultatet indikerar att användandet av en talapparat underlättar kommunikationen och språkutvecklingen hos barn med verbal dyspraxi. Specifik evidens finns gällande ökning av den kognitiva komplexiteten på frågorna som barnet fick samt ökning av antalet frågor som ställdes direkt till barnet. Gällande barnets respons noterades att korrekta svar ökade samt även antalet kommunikationsförfaranden och kommunikativa försök. Longitudinell data indikerar att barnet bibehåller dessa positiva effekter. Studien visar att en talapparat kan användas för att underlätta en mer komplex kognitiv språkanvändning för barn med verbal dyspraxi. Ett annat positiv utfall från denna studie relaterar till ökningen av försök till kommunikativa initiativ från barnen. I studien diskuteras vidare hur AKK strategier och speciellt då talapparater, kan underlätta tal‐ och språkutveckling hos barn med verbal dyspraxi. AKK strategierna kan användas som komplement för personer med lite tal för att underlätta socialt deltagande. I samma studie för författarna fram vikten av utbildningsprogram för modern och resultat visar att efter att modern utbildats tenderade hon att ställa frågor med en högre komplexitet.
Resultat, studie 3
I ett fallexempel i studien ”Developmental apraxi and augmentative or alternative communication – a case example” från USA (1989) framför författaren att det fortfarande fanns väldigt lite forskning kring användandet av AKK för barn med verbal dyspraxi. Syftet med detta fallexempel var att dels beskriva de kommunikativa egenskaperna hos en 8‐årig flicka med diagnosen verbal dyspraxi och dels diskutera frågor rörande verbal dyspraxi och AKK. Resultatet i studien visade att flickan gav mer språklig information än tidigare och svarade mindre på frågor. De kommunikativa hjälpmedel som användes var tecken och gester. Flickan använde inte sin kommunikationsbok varken före eller efter bedömning, vilket författarna tror beror på att hennes mamma var duktig på tecken och de därmed klarade sig med tecken och gester. Den mest markanta förändringen utgjordes av att modern minskade sina ickeförtydligande frågor vilket i sin tur ledde till ett bättre samspel mellan mor och dotter. Flickans mamma rapporterade också att hela familjen fortsatte att ändra sitt kommunikativa samspel. Hon noterade även att denna förändring varit väldigt givande och att flickan nu kunde berätta vad hon verkligen ville prata om. Flickan pratade nu också mer spontant med olika personer och i olika situationer.

84
Resultat från frågeformulär
Av 15 tillfrågade logopeder inkom svar från 10 stycken. Svaren sammanställdes och vid analysen framkom att det både finns tydliga likheter samt skillnader vad gäller införandet av AKK.
Figur 1. På frågan ”Sätter du diagnosen verbal dyspraxi eller fonologisk språk störning?” är det främst diagnosen fonologisk språkstörning som sätts (se figur 1), men ofta i kombination med annan diagnos såsom oralmotorisk språkförsening. I journaltext ges beskrivning av barnets svårigheter och man väljer ibland att använda termen dyspraxi.
0
1
2
3
4
5
6
7
8
9
10
Fonologisk språkstörningF80.A
Oralmotoriskspråkförsening F80.0B
Expressiv språkstörningF80.1
Journaltext Dyspraxi
10 LOGOPEDERS DIAGNOSSÄTTNING

85
Fråga 2. På frågan ”Vilka alternativa kommunikationshjälpmedel förskriver du för yngre barn?” svarar samtliga logopeder (se figur 2) att de förser/förskriver teckenmaterial till barnet/familjen. Någon förser med bildmaterial/bildkartor.
10
2
1
Teckenmaterial Bildmaterial Talapparat
Yngre barn

86
Figur 3. På frågan ” Vilka alternativa kommunikationshjälpmedel förskriver du för äldre
barn?” syns en klar förändring där det endast är ett fåtal logopeder som förskriver
hjälpmedel (se figur 3) såsom exempelvis läs‐ och skrivstödjande programvaror och
talapparat. För sex av logopederna har det inte varit aktuellt med förskrivning för de
äldre barnen.
På frågan ”Vilket AKK fungerar bäst utifrån din erfarenhet?” ges samstämmiga svar att det från tvåårsåldern fungerar klart bäst med tecken. När det gäller skolbarn blir svaret läs‐ och skrivstöd samt skriftspråket.
På frågan ”Förutom barnets svårigheter, vilka andra faktorer påverkar ditt val av AKK?” gällande faktorer som påverkar valet av AKK förs föräldraengagemang, förskoleengagemang samt barnets motivation fram.
Andra funderingar/erfarenheter som fördes fram var att talsyntes är viktig för koppling mellan ljud‐bokstav. Talapparater kan fungera som stimulerande leksak men är svårt att få som en naturlig del i kommunikationen. Bildstöd är möjligtvis underskattat som AKK och att det är positivt med samarbete med specialpedagog som kan ge nära stöd till den alternativa kommunikationen i vardagen.
1
2
3
1
6
Teckenmaterial Talapparater Läs‐ ochskrivstöd
Skriftspråk Ej aktuellt
Äldre barn

87
Diskussion Både i litteratur och i forskning framkommer att barn med verbal dyspraxi är hjälpta av olika former av AKK. Det framkommer att AKK både kan användas som en hjälp i kommunikativa situationer samt ge stöd vid talträning. Då det är vanligt med en diskrepans gällande barnets expressiva och impressiva förmåga kan olika AKK således ge stöd vid kommunikativt samspel men även stärka barnets språkutveckling. De språkliga kunskaperna kan sedan överföras till talad kommunikation när talet förbättrats.
Då det ofta krävs stora behandlingsinsatser för barn med verbal dyspraxi är det viktigt med ett gott samarbete mellan samtliga vuxna i omgivningen. Utbildning till föräldrarna förs fram i en av studierna och att som logoped ta tid till samtal kring AKK är viktigt då föräldrars önskan ofta är att barnet ska tala. Föräldrars behov av kunskap kring diagnosen är ofta stor och de bör få utbildning kring barnets svårigheter och hur olika AKK kan fungerar. Detta för att på bästa sätt hjälpa barnet i sin tal‐ och språkutveckling.
På fråga kring AKK för barn med verbal dyspraxi som ställdes till yrkesverksamma logopeder framkommer det att tecken är vanligast förekommande och av erfarenhet det som fungerar bäst för de yngre barnen. För de äldre barnen med verbal dyspraxi är talsyntes viktig och de blir även hjälpta av skriftspråket. Min bedömning är att vi inte arbetar med högteknologiska samtalsapprater i den utsträckning som litteratur och forskning förespråkar. I det dagliga arbetet är det tecken och bilder som fungerar väl, men mer avancerade talapparater blir inte lika lätt naturliga inslag i kommunikationen. Detta kan troligtvis bero på många olika saker. Insatserna är tidskrävande och som logoped arbetar man sällan nära barnet i dess vardag. Barn med enbart språkstörning är inte aktuella för insatser inom barn‐ och ungdomshabiliteringen vilket troligtvis hade underlättat arbetet med att utveckla barnets alternativa kommunikation. Kunskaperna ute i förskolor är varierad och begränsad vilket även det påverkar barnets möjlighet att använda ett alternativt kommunikationshjälpmedel.
Slutsats Litteratur och studier visar på samstämmiga resultat vad gäller insatser som barn med verbal dyspraxi är i behov av. Den behandling som ska ges bör vara intensiv med inriktning på både talträning samt AKK. Utbildning till föräldrar kring diagnosen och AKK bör ges.
Av de tio logopeder som besvarade frågeformuläret kring AKK för denna patientgrupp rekommenderar samtliga tecken som AKK från tidig ålder. Detta skiljer sig från de äldre barnen där endast några logopeder förskriver programvaror alternativt talapparat. Av detta dras en försiktig slutsats att tecken redan etablerats och därmed inte behöver förskrivas.
Att föra fram det stora behovet av insatser som barnen och deras familj är i behov av bör ske kontinuerligt på flera plan inom vården.
Utifrån det magra resultatet gällande studier i ämnet är behov av fler studier således stort.

88
Referenser Beukelman, D. R., & Mirenda, P. (1998). Augmentative and alternative communication :
Management of severe communication disorders in children and adults (2nd ed.). Baltimore: Brookes.
Binger, C., Berens, J., Kent‐Walsh, J., & Taylor, S. (2008). The effects of aided AAC interventions on AAC use, speech and symbolic gestures. Seminars in Speech and Language, 29(2) 101–111.
Blischak, D., Lombardino, L., & Dyson, A. (2003). Use of speech‐generating devices: In support of natural speech. Augmentative and Alternative Communication, 19(1), 29–35.
Bornman, J., Alant, E., & Meiring, E. (2001). The use of a digital voice output device to facilitate language development in a child with developmental apraxia of speech: A case study. Disability & Rehabilitation, 23(14), 623–634.
Caruso, A. J., & Strand, E. A. (1999). Clinical management of motor speech disorders in children. New York: Thieme.
Culp, D. M. (1989). Developmental apraxia and augmentative or alternative communication–a case example. Augmentative and Alternative Communication, 5(1), 27–34.
Cumley, G., & Swanson, S. (1999). Augmentative and alternative communication options for children with developmental apraxia of speech: Three case studies. Augmentative and Alternative Communication, 15(2), 110–125.
Hartelius, L., & Lyons, L. (2008). Logopedi (1 uppl ed.). Lund: Studentlitteratur.
Morgan, A. T., & Vogel, A. P. (2009). Intervention for childhood apraxia of speech. Cochrane Database of Systematic Reviews 2008,
Velleman, S. L. (2003). Childhood apraxia of speech resource guide. Clifton Park, N.Y.: Delmar Learning.
Weitz, C., Dexter, M., & Moore, J. (1997). AAC and children with developmental disabilities. Handbook of Augmentative and Alternative Communication, 395–431.

89
8. Diagnostisering av barn med misstänkt verbal dyspraxi. Bedömning med VMPAC
Laura Olsson, Logopedmottagningen, Karlskrona, Blekinge läns Landsting, Sverige
Sammanfattning Syftet med denna studie har varit att prova att använda ett bedömningsmaterial designat för att testa barns talmotoriska förmåga, VMPAC (Hayden & Square 1999) samt att jämföra detta med de tecken på verbal dyspraxi som barnen i undersökningen uppvisade. Testet genomfördes med tre barn där verbal dyspraxi misstänkts för att ta reda på om de hade störningar i talmotoriken av dyspraktiskt slag. Resultatet jämfördes med resultat på tidigare bedömningar och observationer av deras tal, språk och oralmotorik samt vad föräldrarna berättat om barnet. Två av barnen fick ett resultat under percentil 5 på flera av uppgifterna på VMPAC, och de bedömdes ha dyspraktiska svårigheter troligen tillsammans med en fonologisk språkstörning. Ett av barnen fick ett resultat på testet som inte riktigt nådde upp till genomsnittet, men det låg inte heller under percentil 5. Dyspraktiska svårigheter uteslöts dock ändå inte i hans fall, utan bedömdes vara i mindre grad jämfört med de två andra barnen. Det visade sig att det barn som hade lägst resultat på VMPAC också hade flest tecken på verbal dyspraxi samt att det barn som hade högst resultat på VMPAC hade färre tecken på verbal dyspraxi. Utifrån detta resultat konstaterades att VMPAC är ett bedömningsmaterial väl värt att använda vid misstänkt verbal dyspraxi.
Bakgrund
Differentialdiagnostisering
När ett barn har svårt att göra sig förstådd och remitteras till en logopedmottagning är det i syfte att ställa diagnos och att planera åtgärder såsom behandling. Under arbetet med detta väcks frågan varför barnet har svårt att göra sig förstådd. Hur ska behandlingen planeras? Varför låter barnets tal inte som förväntat för åldern? Om barnet har problem med talljuden ställs frågan ofta på sin spets: är det främst språkliga svårigheter eller motoriska svårigheter som barnet har? Är det en språkstörning eller verbal dyspraxi? Svaret på frågan är viktig för att planera behandling. Ett mer nyanserat synsätt är att man får vänta sig att barnet har både språkliga och motoriska svårigheter (Caruso & Strand 1999). Det finns också teorier som

90
bedömer det som rimligt att ett barns motoriska förmåga påverkar den språkliga förmågan, och tvärtom (Nettelbladt 2007, refererat till Locke 1993).
Verbal dyspraxi
Det finns flera teorier med olika perspektiv på vad verbal dyspraxi är (Velleman 2003).
Man har inom American Speech‐Language‐Hearing Association (ASHA) enats om att verbal dypraxi hos barn kan vara förvärvad, förekomma tillsammans med andra neurologiska störningar eller förekomma utan känd orsak. Det definieras vidare som en neurologisk talstörning men utan neuromuskulära avvikelser. Verbal dypraxi innebär svårigheter med planeringen och/eller med programmeringen av sekvenserade talrörelser och orsakar störningar i produktionen av talljud och prosodi. De har vidare konstaterat att det inte finns någon klar definition av vilka ljudfel barn med verbal dyspraxi kan uppvisa, som man kan använda för att skilja mellan verbal dyspraxi och andra tal‐ och språkstörningar som påverkar talljuden. Däremot har man sett att det finns tre kännetecken som återkommer inom forskningen kring verbal dyspraxi: inkonsekvent produktion av fonem vid upprepad produktion av stavelser eller ord, förlängd eller avbruten koartikulation mellan fonem och stavelser samt avvikande prosodi särskilt vad gäller betoning. ASHA framhåller dock att dessa symptom varken är nödvändiga eller tillräckliga för att ställa diagnosen verbal dyspraxi (ASHA 2007). I en studie av Forrest (2003) undersökte man vilka symptom olika logopeder ansåg att barn med verbal dyspraxi uppvisade. Logopederna angav 50 olika symptom varav inkonsekvent talproduktion, trevande talrörelser, generella oralmotoriska svårigheter, svårigheter att imitera ljud, ökade talsvårigheter vid ökad komplexitet på yttrandet och brister vid sekvensering av talljud var de vanligaste svaren. Ibland förekommer det också att barn med verbal dyspraxi även uppvisar andra störningar, så kallade ”soft signs” såsom svårigheter med koordination av fin‐ och grovmotorik (Yorkston, Beukelman, Strand & Bell 1999). Verbal dyspraxi kan visa sig på olika sätt beroende på barnets ålder och graden av störning (McCauly & Strand 2008). Teverovsky et al. (2009) lät 201 föräldrar till barn med verbal dyspraxi ange vid vilken ålder barnet diagnostiserades med verbal dyspraxi. De fann att den genomsnittliga åldern för diagnostisering var vid två och ett halvt år. Föräldrarna angav att tal‐ och språkproblemen då visade sig genom minimal talmängd, svårigheter att imitera ord, svårförståelighet, brister i grammatik, att behöva kämpa med talet samt brister i intonation. I Yorkston et al. (1999) nämns flera olika typiska svårigheter vid verbal dyspraxi såsom utelämning, substituering och tillägg av fonem, att fler ljud blir fel när yttrandet blir längre, inkonsekventa ljudfel, trevande talrörelser, långsamt tal och förändrad prosodi. Vidare nämns svårigheter med distinktionen nasal‐iceknasal, tonande‐tonlös och avvikande vokalklang samt att barnet kan ha andra språkliga svårigheter och oral dyspraxi. Oral dyspraxi motsvarar verbal dyspraxi fast drabbar enbart orala rörelser som inte involverar tal (McAllister 2008). Verbal dyspraxi är också förknippat med små eller inga framsteg trots behandling hos logoped (Shriberg, Aram & Kwiatkowski 1997a), men det är då troligt att behandlingen inte har anpassats efter barnets svårigheter (Velleman 2003).
Ibland förknippas verbal dyspraxi med att en viss typ av sensorik är nedsatt i talorganen, nämligen proprioceptionen, som förmedlar till hjärnan var talorganen befinner sig eller vilken form de har (Yorkston et al. 1999). När man talar utför bland annat käken, läpparna, tungan och mjuka gommen rörelser och de måste vara på rätt plats, röra sig i rätt riktning, ha rätt styrka och de ska röra sig i rätt tid (Strand 1999). Utöver detta tillkommer koartikulationen,

91
det vill säga att talrörelserna påverkas av varandra, så att de i viss mån utförs samtidigt (Lindholm 2008). För att detta ska fungera är sensoriken mycket viktig (Strand 1999).
Yoss och Darley (1974), som var bland de första att beskriva dyspraktiska svårigheter hos barn, jämförde två grupper av barn med tal‐ och språksvårigheter varav en grupp med och en grupp utan verbal dyspraxi. För barnen med dyspraktiska svårigheter beskrevs nedsatt hastighet vid diadochokinesi, såsom ”pataka”, samt att stavelserna producerades i fel ordning vid repetition. De beskrev bland annat också att barnen med dyspraktiska svårigheter hade svårare med flerstaviga ord där utelämning och tillägg av stavelser kunde förekomma. Däremot menade de att de prosodiska svårigheter som kunde förekomma var ett resultat av att barnen försökte tala långsammare för att göra sig bättre förstådda. Det förekom också i högre grad hos de barn som var lite äldre eller hos de som genomgått talträning. De noterade också att barnen hade andra motoriska svårigheter, så som att knäppa knappar eller att lära sig cykla samt att barnen med dyspraktiska svårigheter, liksom barn med andra typer av tal‐ och språkvårigheter, uppvisade sämre resultat på test av auditiv perception jämfört med barn utan tal‐ och språksvårigheter.
Språkstörning
Språkstörning beskrivs enligt Nettelbladt och Salameh (2007) översiktligt som att barnet inte tillägnar sig språket så som förväntas i en viss ålder. Vid fonologisk språkstörning har barnet svårigheter inom fonologin och det yttrar sig genom olika fonologiska processer som gör barnet mer eller mindre svårt att förstå. Det finns olika förklaringsmodeller till varför språkutvecklingen inte sker som förväntat. Nettelbladt (2007) beskriver modeller som presenterats i olika studier: problem med arbetsminne, perception och språklig bearbetning. Samtliga av modellerna beskriver alltså att störningen primärt återfinns i barnets förmåga att särskilja och bearbeta ljuden i språket. Nettelbladt (2007) nämner dock också att barnet kan ha motoriska svårigheter, vilket kan påverka barnets organisering av fonologiska mönster. Vidare beskriver hon olika fonologiska processer som förekommer vid fonologisk språkstörning såsom dentalisering, velarisering, h‐sering, strykning av obetonad stavelse, utlämning av fonem, förenkling av konsonantförbindelser, av‐ och påtoning, förändring av vokaler och prosodi.
Bedömningsmaterial för fonologi, oralmotorik och talmotorik
Ett vanligt bedömningsmaterial som används i Sverige är Fonemstatus, stora versionen (Hellquist 2004). Med hjälp av det kan man bedöma barnets fonologiska system. För att undersöka oralmotorik finns det några olika svenska bedömningsmaterial, ett ofta använt är Stockholms Oralmotoriska bedömningsprotokoll, STORM (Henningsson, McAllister, Hartstein & Raud Westberg 2008). I Sverige finns ännu inget tillförlitligt test som provar barns talmotorik enligt Björelius Hort (2009). I Björelius Horts (2009) studie användes en svensk översättning av det amerikanska Verbal Motor Production Assessment for Children, förkortat VMPAC (Hayden & Square 1999). Testet har även använts av Gruhonjić och Stengård (2010) där de i en studie av 23 barns resultat på VMPAC, konstaterade att dessa svenska barn presterade ungefär som de amerikanska barnen som deltagit vid standardisering av VMPAC. VMPAC provar oralmotorik och talmotorik både vid enskilda rörelser och sekvenserade rörelser såsom produktion av /p/, /pa/, /pata/ och /pataka/. Talrörelserna testas dels isolerat men även i serier om fyra repetitioner efter varandra. Man tar också reda på om barnet klarar rörelserna enbart på eftersägning, behöver guidas visuellt eller guidas taktilt. Man provar även deras

92
spontantal och det finns även delar som är konstruerade för att undersöka barnets övriga motorik. Testet är noggrant utvärderat av McCauly och Strand (2008). De undersökte vilka test som finns att tillgå för att undersöka barns talmotorik, och fann att VMPAC var det som bäst nådde upp till deras krav på reliabilitet, validitet och normering, även om det inte var komplett. Då inget test ansågs vara helt tillförlitligt uppmanades logopeder att använda dylika test med försiktighet.
Syfte Syftet med denna studie är att prova att använda VMPAC på några barn där verbal dyspraxi misstänks samt att jämföra de tecken på verbal dyspraxi som barnen uppvisar med resultat av bedömning med testet. Vidare syftar detta till att ta reda på om barnen har verbal dyspraxi eller inte. Syftet är också att ta reda på om VMPAC är lämpligt att använda i fortsättningen.
Frågeställningar
Hur klarar barnen VMPAC?
Vilka tecken på verbal dyspraxi uppvisar de?
Finns det något samband mellan resultatet på VMPAC och de tecken på verbal dyspraxi de
har?
Bedöms barnen ha verbal dyspraxi efter bedömning med VMPAC?
Kan VMPAC rekommenderas för fortsatt användning?
Metod
Deltagare
Tre pojkar valdes ut för att delta i studien. De deltog efter att föräldrarna fått information och tackat ja till att delta. De valdes ut för att verbal dyspraxi misstänktes vara en komponent i deras svårförståeliga tal. De hade alla stora svårigheter med fonologin men inga påfallande svårigheter med övriga språkliga förmågor eller språkförståelse. Pragmatiken var god och de brukade medverka väl. Försökspersonerna kallas hädanefter för Barn A, Barn B, och Barn C. Barn A var 6;3 år vid genomförandet av VMPAC, Barn B var 4;8 år och Barn C var 6 år.
Material
Resultat från tidigare undersökningar inhämtades från barnens journaler. Där fanns resultat från undersökningar med Fonemstatus, stora versionen, STORM, övrig information om barnet och bedömning av spontantal. De senaste bedömningarna med Fonemstatus, stora versionen genomfördes under sommaren 2011. STORM genomfördes under våren för barn A, under sommaren för barn B och för barn C var bedömningen daterad 101222. Uppgifter om spontantal hämtades från barnens journaler från och med våren 2011, detsamma gäller information föräldrarna lämnat om barnet, såsom motoriska svårigheter. Bedömningen med VMPAC utfördes utan tillgång till manualen och enbart protokollet användes. Samma översättning som i Björelius Horts studie (2009) användes. Då VMPAC:s bilder inte fanns tillgängliga producerades respektive valdes sådana ut av uppsatsförfattaren. En digital

93
videokamera användes vid bedömningen med VMPAC för att barnets prestation skulle kunna analyseras i efterhand.
Genomförande
Föräldrarna till testpersonerna tillfrågades att delta i studien. De fick information muntligt och skriftligt och skrev under på att de lät sina barn delta i studien.
De delar som testades var Focal Oromotor Control, men av denna kategori endast de delar som gällde Speech Movements. Även delarna Sequencing, Connected Speech and Language Control samt Speech Characteristics genomfördes. På Focal Oromotor Control finns tre olika sätt för att göra så att barnet säger rätt: auditivt, visuellt och taktilt. Det var främst det auditiva som användes för att förenkla testförfarandet. Visuell guidning genomfördes dock i några fall då det bedömdes lämpligt. Taktil guidning gjordes ej. På grund av att alla testuppgifter därmed inte genomfördes förändrades poängräkningen och varje barn fick ett resultat inom ett visst intervall. Inom delen Focal Oromotor Control och Sequencing räknades ett lägsta och högsta värde ut genom att barnet antogs klara antingen alla eller inga av uppgifterna 14‐37, vilket var de delar av Focal Oromotor Control som inte genomfördes. De gällde enbart oralmotorik och inte talmotorik. Samtidigt antogs barnet få mellan 0 och 2 poäng, det vill säga minmal och maximal poäng, på visuell guidning respektive taktil guidning. Detta gällde i de fall där barnet inte hade klarat rörelsen utifrån endast auditiv guidning.
Bedömningen med VMPAC gjordes under sommaren 2011 av uppsatsförfattaren på den logopedmottagning där uppsatsförfattaren arbetar. Hela testningen filmades med digital videokamera. En förälder till varje barn närvarade i rummet och kontrollerade så att videokameran fick med barnet i bild hela tiden. I ett fall närvarade även ett syskon. För ett barn genomfördes STORM vid samma tillfälle som VMPAC, och då togs en paus när ungefär hälften av den sammanlagda testningen var genomförd. För ett av barnen missades en uppgift och denna kompletterades vid ett senare tillfälle, utan videoinspelning. Testningen tog ungefär 30 minuter att genomföra.
Resultat Det är möjligt att resultatet av undersökningarna skulle blivit ett annat om manualen till VMPAC funnits tillgängligt under genomförandet av studien. Tack vare att testprotokollet är utförligt förefaller ändå sannolikheten att resultatet är förhållandevis rättvisande. Grad av medverkan och uthållighet hos barnen varierade, något som kan ha påverkat resultatet. Det var tydligt att förmågan att medverka och följa instruktionerna varierade mycket mellan barnen. Vad gäller detta kan bristande medverkan även tolkas som ett uttryck i att uppgiften var alltför svår.
Barn A fick ett poängintervall mellan 29 % och 88 % på Focal Oromotor Control, vilket ligger under percentil 5. På Sequencing fick han ett intervall mellan 41 % och 63 % vilket också liger under percentil 5. Barn B fick ett poängintervall mellan 16 % och 85 % vilket sträcker sig mellan under percentil 5 och nästan upp till genomsnittet för åldern på delen Focal Oromotor Control. På Sequencing fick han ett intervall mellan 54 % och 85 % vilket ligger mellan strax över percentil 5 och upp till genomsnittet. Barn C fick ett poängintervall mellan 28 % och 81 % vilket ligger under percentil 5 på delen Focal Oromotor Control. På Sequencing fick han ett poängintervall mellan 50 % och 80 % vilket ligger mellan strax över percentil 5 och en bit under

94
genomsnittet. Alla tre barnen fick ett resultat under 5:e percentilen på både Connected Speech and Language Control och Speech Characteristics.
Nedan redovisas resultaten på VMPAC för barn A och C (6 år) i Tabell 1 och för barn B (4 år) i Tabell 2. Genomsnittsresultat och percentil 5 för respektive åldersgrupp, hämtat från protokollet från VMPAC, det vill säga det resultat som erhållits från testning av amerikanska barn (Hayden & Square 1996).
Tabell 1. Resultat på VMPAC för barn A och barn C, 6 år
Barn A Barn C Genomsnitt,
Hayden &
Square 1996?)
5:e percentilen
Focal Oromotor Control 29‐88% 28‐81% 96 % 90 %
Sequencing 41‐63% 50‐80% 90 % 65 %
Connected Speech and
Language Control 75% 80% 96% 86%
Speech Characteristics 71% 57% 98% 85%
Tabell 2. Resultat på VMPAC för barn B, 4 år
Barn B Genomsnitt 5:e percentilen
Focal Oromotor Control 16‐85% 90 % 75 %
Sequencing 54‐76% 75 % 47 %
Connected Speech and
Language Control 53% 91% 73%
Speech Characteristics 84% 98% 85%
Tecken på verbal dyspraxi
I Tabell 3 redovisas de tecken på verbal dyspraxi som presenterats i bakgrunden samt huruvida barnen uppvisade dem. Angivelsen ”delvis” innebär att barnen har svårigheten, men i liten grad. Uppgifter om svårigheter inhämtade från barnens journaler. Tecken på dyspraxi är en sammanställning från flera tidigare studier.

95
Tabell 3.
Tecken på verbal dyspraxi Barn A Barn B Barn C
Inkonsekvent produktion av
fonem
Ja Ja Delvis
Förlängd eller avbruten
koartikulation
Nej Nej Ja
Avvikande prosodi Nej Nej Nej
Övriga motoriska svårigheter Ja Nej Nej
Utelämning, tillägg eller byte
av fonem
Ja Ja Ja
Ökad svårighet vid ökad längd Delvis Ja Ja
Trevande talrörelser Ja Nej Delvis
Långsamt tal Nej Nej Ja
Svårt med nasal/ickenasal Ja Nej Nej
Svårt med tonlös/tonande Delvis Enstaka Nej
Avvikande vokalklang Ja Nej Nej
Andra språkliga svårigheter Ej formellt
undersökt
Ej formellt
undersökt
Ej formellt
undersökt
Oral dyspraxi Ja Delvis Nej
Mycket långsamma framsteg
trots behandling
Nej Delvis Ja
Svårigheter med
diadochokinesi
Ja Ja Ja
Utelämning eller tillägg av
stavelser
Nej Nej Delvis
Nedsatt auditiv perception Ej formellt
undersökt
Ej formellt
undersökt
Ej formellt
undersökt
Barn A hade 10/17 tecken på verbal dyspraxi, varav två tecken förekom delvis. Barn B hade 7/17 tecken på verbal dyspraxi, varav 4 tecken förekom delvis eller enstaka gånger. Barn C hade 9/17 tecken på verbal dyspraxi, varav 3 tecken förekom delvis.
Jämförelse av tecken på verbal dyspraxi och resultat på VMPAC samt diagnostisering
Resultaten på VMPAC och barnens tecken på verbal dyspraxi stämmer någorlunda överens på så sätt att det barn som hade sämst resultat på VMPAC i relation till åldern uppvisade också fler tecken på verbal dyspraxi. Det barn som hade bäst resultat på VMPAC i relation till åldern hade också färre tecken på verbal dyspraxi.
Resultaten talar för att Barn A och Barn C har verbal dyspraxi troligen tillsammans med fonologisk språkstörning. Sett mot bakgrunden av tidigare undersökningar och observationer är det sannolikt att Barn A:s tal‐ och språksvårigheter till större del beror på verbal dyspraxi jämfört med Barn C. Barn B visar också tecken på motoriska svårigheter av dyspraktiskt slag, men de fonologiska svårigheterna överväger.

96
Diskussion Den stora variationen i rapporterade tecken på verbal dyspraxi försvårar arbetet med diagnostisering. Även det faktum att tecken på fonologisk språkstörning ofta kan överlappa med verbal dyspraxi innebär en komplicerande faktor. Eftersom det är så viktigt att differentialdiagnostisera upplevs det som nödvändigt att det finns tillförlitliga metoder för detta. Det uttalande ASHA gjort där de framhåller att inkonsekvent produktion av fonem vid upprepad produktion av stavelser eller ord, förlängd eller avbruten koartikulation mellan fonem och stavelser samt avvikande prosodi särskilt vad gäller betoning, kan vara en hjälp. Eftersom det finns så många olika mer eller mindre vedertagna tecken på verbal dyspraxi är det en stor hjälp att använda test för talmotorik, såsom VMPAC. VMPAC finns dock ej i svensk upplaga ännu, men kommer förhoppningsvis att finnas i framtiden. Diagnostiseringen påverkar hur behandlingen planeras och utförs och förhoppningsvis kan tecknet ”uteblivna framsteg trots behandling” uteslutas i framtiden.
Även om VMPAC är konstruerat för att testa talmotoriken finns det säkert flera olika andra faktorer som avgör hur väl ett barn klarar testet. Dels måste barnen koncentrera sig och känna sig motiverade att genomföra testet. De måste också komma ihåg vad det var de skulle säga. Man skulle kunna prova fonologiskt minne genom att be barnet upprepa orelaterade ord och meningar och därmed ta reda på om det fonologiska minnet verkar fungera som förväntat. Men det är inte den typen av fonologiskt minne som behövs vid genomförandet av VMPAC, utan även förmågan att minnas orelaterade fonem och stavelser snarare än ord. Skulle man prova det så kan man å andra sidan inte avgöra om barnet inte minns eller bearbetar ljuden, eller om barnet inte klarar att producera dem korrekt. Fonologisk språkstörning å andra sidan bygger på just detta, att barnen har svårt att bearbeta taljuden, så man skulle även kunna tolka testet som ett test på fonologiskt minne. Hur man än gör förefaller det vara svårt att avgöra om det är produktionen eller det fonologiska minnet som avgör barnets resultat på VMPAC. Vad som också framstår som viktigt är att göra en samlad bedömning av barnets tal, språk och anamnes. Ett annat sätt att differentialdiagnostisera kunde vara att prova behandling för fonologisk språkstörning respektive verbal dyspraxi och sedan utvärdera vilket som hjälpte barnet mest, men självklart är det önskvärt att rätt behandling väljs från början.

97
Referenser American Speech‐Language‐Hearing Association (2007). Childhood Apraxia of Speech [Position
Statement] Tillgänglig på www.asha.org/policy
Björelius Hort, H. (2009). Are Oral and Verbal Motor Functions Related to Manual and Overall Motor Performance in Children with Developmental Apraxia of Speech? Examensarbete i logopedi, Karolinska Institutet, Institutionen för klinisk vetenskap, intervention och teknik.
Caruso, A. J. & Strand, E. A. (1999). Motor Speech Disorders in Children: Definitions, Background, and a theoretical framework. In Caruso, A. J. & Strand, E. A. (Eds), Clinical Management of Motor Speech Disorders in Children (pp. 1‐27). New York: Thieme.
Forrest, K. (2003). Diagnostic Criteria of Developmental Apraxia of Speech Used by Clinical Speech‐Language Pathologists. American Journal of Speech‐Language Pathology, 12, 376–380.
Hayden, A. & Square, P. (1999). VMPAC, Verbal Motor Production Assessment for Children. Record form. San Antonio, TX: The Psychological Corporation
Hellquist, B. (2004). Fonemtest, stora versionen. Skivarp: Pedagogisk design
Henningsson, G., McAllister, A., Hartstein, M. & Raud Westberg, L. (2008). STORM, Stockholms oralmotoriska bedömningsprotokoll. Version 1. Danderyds sjukhus, Karolinska Universitetssjukhuset
Lindholm, B. (2008). Röst‐ och talfunktion. I Hartelius, L., Nettelbladt, U. & Hammarberg, B. (Red.) Logopedi (pp 21–35). Lund: Studentlitteratur
McAllister, A. (2008). Oralmotoriska störningar hos barn och ungdomar. I Hartelius, L., Nettelbladt, U. & Hammarberg, B. (Red.) Logopedi (ss 377‐386). Lund: Studentlitteratur
McCauley, R. & Strand, E. A. (2008) Review of Standardized Test of Nonverbal Oral and Speech Motor Performance in Children. American Journal of Speech‐Language Pathology, 17, 81–91.
Nettelbladt, U. (2007). Fonologiska problem hos barn med språkstörning. I Nettelbladt, U. & Salameh, E‐K. (Red.), Språkutveckling och språkstörning hos barn, del 1 (pp 95–134). Lund: Studentlitteratur
Nettelbladt, U., & Salameh, E‐K. (2007). Språkstörning hos barn. I Nettelbladt, U. & Salameh, E‐K. (Red.), Språkutveckling och språkstörning hos barn, del 1 (pp 13–33). Lund: Studentlitteratur.
Shriberg, L. D., Aram, D. M., Kwiatkowski, J. (1997a). Developmental Apraxia of Speech: I Descriptive and Theoretical Perspectives. Journal of Speech and Hearing Research, 40(2), 268–312.
Teverovsky, E. G., Ogonowski Bickel, J., & Feldman, H. M. (2009). Functional characteristics of children with Childhood Apraxia of Speech. Disability and Rehabilitation, 31(2), 94–102.
Velleman, S. L. (2003). Childhood Apraxia of Speech. A Resource Guide. Clifton Park, New York: Delmar Learning.
Yorkston, K. M., Beukelman, D. R., Strand, E. A., & Bell, K. R. (1999) Management of Motor Speech Disorders in Children and Adults. Austin, Texas: Pro Ed.
Yoss, K. A. & Darley, F. L. (1974). Developmental Apraxia of Speech in Children with Defective Articulation. Journal of Speech and Hearing Research, 17, 399–416

98

99
9. Behandling av två barn med verbal dyspraxi enligt Dynamic Temporal and Tactile Cueing (DTTC). En multipel fallstudie
Åsa Engström, Logopedbyrån Dynamica AB, Stockholm, Sverige
Sammanfattning Syftet med den här studien är att använda och utvärdera effekten av en behandlingsmetod för barn med verbal dyspraxi, Dynamic Temporal and Tactile Cueing, DTTC.
Två barn, 2:7 och 3:4 år gamla, diagnosticerades med Verbal dyspraxi och fick behandling enligt DTTC vid 6‐7 tillfällen under en 14‐dagarsperiod. Framsteg under behandlingen mättes i procent korrekta ord, konsonanter, vokaler och fonem i 20 kontrollord utvalda utifrån fonem och strukturer som barnen ännu inte etablerat i sitt tal. Resultatet efter behandling jämfördes med en baslinjebedömning gjord vid flera tillfällen under en tvåveckorsperiod före påbörjad behandling. Resultatet visade stora framsteg för båda barnen. Tydligast framsteg var i uttalet av hela ord där en ökning från 25% till 50% respektive från 14% till 42% korrekta ord uppmättes. Det talar således för att DTTC är en effektiv behandlingsmetod för barn med verbal dyspraxi.
En stor bidragande faktor till framgång bedöms vara barnets egen motivation att träna sitt tal och det är viktigt att i valet av träningsstimuli utgå från ord som är viktiga för barnet själv. Troligt är att ännu bättre resultat skulle uppnås om man inväntat högre motivation hos framför allt ett av barnen. Behandlingsperioden var också relativt kort och tydligare slutsatser skulle kunnat dras med en längre period att utvärdera.
Bakgrund Hur man definierar verbal dyspraxi är omtvistat. ASHA (American Speech Language and Hearing Association) kom 2007 överens om en definition där man konstaterar att verbal dyspraxi är en motorisk talstörning där svårigheter med planering och programmering av talrörelserna orsakar ett otydligt tal (ASHA 2007). Enligt Morgan och Vogel (2009) finns det tre alltid förekommande drag: inkonsekventa fel både när det gäller vokaler och konsonanter ‐ samma ord eller stavelse uttalas olika vid olika tillfällen, förlängda eller försämrade övergångar mellan ljud och stavelser och avvikande prosodi. Strand ger exempel på andra drag

100
som svårigheter att initiera talrörelser, sökande (groping) för att hitta rätt artikulatorisk position, tvekanden, oförmåga att imitera talljud trots avsaknad av strukurella och funktionella avvikelser i talapparaten, minskad proprioception av artikulatorerna, svårigheter med timing och artikulatoriska fel som ersättningar och utelämnande av ljud. (Caruso & Strand, 1999). Flera studier räknar upp samma symptom på verbal dyspraxi (Davis, Jacks, & Marquardt, 2005; Forrest, 2003; Jacks, Marquardt, & Davis, 2006; Peter & Stoel‐Gammon, 2008; Terband, Maassen, Guenther, & Brumberg, 2009). Andra visar också på att svårigheterna ligger på stavelsenivå, och att det är vanligare med utelämnande av initial eller final konsonant, hel stavelse eller klusterreducering hos barn med dyspraxi jämfört med barn med andra språkliga diagnoser (Lewis, Freebairn, Hansen, Iyengar, & Taylor, 2004; Shriberg, Aram, & Kwiatkowski, 1997). Barn med verbal dyspraxi gör långsamma framsteg i terapi och svårigheterna består under lång tid, så pass markant att detta till viss del har använts som ett kriterium för att sätta diagnosen dyspraxi. (Jacks et al., 2006)
Ytterligare en faktor som komplicerar diagnosticeringen av dyspraxi är att förmågan varierar kraftigt från gång till gång, det är därför viktigt att samla många exempel på uttal av varje ord, i olika kontext, isolerat och satsnivå, för att säkerställa att det artikulatoriska mönstret blivit befäst. (Jacks et al., 2006)
I en studie där man jämfört barn med misstänkt dyspraxi med barn med andra språkliga svårigheter (multiple phonological disorders) och barn med normal språkutveckling, noterar man att barnen med dyspraxi jollrade betydligt mindre och med mindre fonetisk variation. Deras första ord kom också signifikant senare. Barnen med dyspraxi presterade bättre på ett impressivt språkförståelsetest jämfört med hur de presterade expressivt medan barnen med andra språkliga svårigheter presterade under medelvärdet på båda typen av uppgifter jämfört med normalspråkiga. Uppgifter med ickeverbala oralmotoriska moment klarade alla grupper lika bra ända tills man kom till sekvensering av rörelser, där de dyspraktiska barnen presterade signifikant sämre. Barnen med dyspraxi hade större variation i sina uttalsfel, och fler fel på stavelsenivå. Författarna diskuterar vikten av att bedöma sekvensiella motoriska rörelser snarare än isolerade. De konstaterar också att barnen med dyspraxi har stor variation i uttal från bedömning till bedömning och talar liksom Jacks om att talet måste bedömas i olika kontexter för att säkerställa validiteten.(Aziz, Shohdi, Osman, & Habib, 2010)
Verbal dyspraxi förekommer sällan utan fonologiska svårigheter. En teori är att då dyspraxin uppkommer under den tid då barnet ska utveckla sitt språk, påverkar den även den lingvistiska delen av talet jämfört med en dyspraxi som uppkommer pga en skada i vuxen ålder (Crary 1993, citerad av Caruso & Strand, 1999).
Dynamic Tactile and Temporal Cueing DTTC
Metoden som kommer att användas i denna studie, DTTC, är en metod utvecklad av Edythe Strand delvis baserad på ”Eight step continuum”, en metod utvecklad för vuxna med tillägnad dyspraxi som baseras på integrerad stimulering (Caruso & Strand, 1999). Med integrerad stimulering menas att patienten ska imitera yttranden där logopeden först uttalar modellen. Patienten ska ha uppmärksamheten riktad både på hur det låter och hur det ser ut när man artikulerar. En förutsättning för att kunna använda DTTC är alltså att patienten vill och kan imitera och kan hålla en selektiv uppmärksamhet och ögonkontakt. DTTC betonar talrörelsen och hur den skapas och används i olika talkontexter, snarare än enskilda fonem. Yttranden övas långsamt och simultant till en början för att underlätta att rörelsen utförs korrekt. Barnet lyssnar och tittar och logopeden hjälper barnet hitta rätt position för artikulatorerna med

101
taktil stimulans och gester efter behov. Allteftersom barnet klarar övningen bättre minskas ledtrådarna från logopeden och barnet blir mer och mer oberoende av stödet. Ledtrådarna ökas och minskas dynamiskt utifrån hur barnet klarade föregående yttrande.
Innan behandlingen påbörjas gör man en bedömning av var patientens svårigheter ligger genom anamnes, neuromuskulärt status, motorisk förmåga/praxisförmåga. Detta för att utesluta dysartriska svårigheter och se på vilken nivå man ska inleda behandlingen. Klarar barnet CV/VC‐ord men inte CVC‐ord, eller blir det svårt först vid ännu längre ord? Vilka ljudtransitioner är svåra? Fokus är på övergångarna mellan ljud, koartikulation och själva talrörelsen. Utifrån bedömning av praxisförmåga och fonemstatus skapar man en hierarkiskt ordnad lista med ord eller stavelser att använda i behandlingen. Svårighetsgraden kan öka på olika sätt, samma stavelsestruktur, men nya fonem (från ”baba” till ”baby”) eller utökad stavelsestruktur (”ma” till ”mamma”, ”tå” till ”stå” eller ”gå” till ”gå upp”).
För att uppnå effektiv behandling börjar man med ganska få stimuli, ju svårare dyspraxi desto färre antal stimuli. Dessa repeteras i block många gånger (15‐30 gånger). Blocken varieras också efter hur grav dyspraxin är så att t ex vissa block repeteras fler gånger än andra. Så snart patienten klarar att upprepa talrörelsen flera gånger utan hjälpstimuli bör kontexten börja varieras för att öka förutsättningarna för den motoriska inlärningen. Först genom att minska antalet repetitioner inom varje block så att man så småningom bara säger varje ord en gång. Därefter med olika prosodi, olika kroppsställningar (sittande, stående, gående, med armarna i luften osv) och i kombination med andra ord. Strand rekommenderar att man förändrar någonting, t ex kroppspositionen efter var 10:e repetition (Caruso & Strand, 1999). När barnet klarar av att självständigt använda ett yttrande i olika kontexter flyttar man det till ”generaliseringsfasen” då ordet istället tränas hemma. Bedömningen av när en talrörelse är generaliserad görs genom att mäta ”probe‐ord” i slutet av behandlingsbesöken. Probe‐orden är inte de samma som yttrandena som tränas, men innehåller samma typ av talrörelse. Strand föreslår att man använder ett kumulativt kriterium, dvs man lägger ihop totala antalet lyckade uttal delat med totala antalet försök sammantaget från alla behandlingstillfällen. 80% av försöken ska ha lyckats för att talrörelsen ska betraktas som generaliserad (Caruso & Strand, 1999).
DTTC innehåller grundläggande principer för motorisk inlärning. Det finns ännu lite forskning gjord kring dessa principer när det gäller barn och tal (Strand EA, Stoeckel R, & Baas B, 2006). Studier på vuxna som utför motoriska uppgifter har visat att det är lättare att generalisera och komma ihåg en inlärd rörelse om den lärs in i en varierad kontext snarare än genom många likadana upprepningar (Giuffrida, Shea, & Fairbrother, 2002; Hall & Magill, 1995).
Ett par studier finns publicerade där man använt DTTC. Försökspersonen i den första studien använde tal som kommunikationssätt. Hon använde vokaler och enstaka bilabiala och dentala konsonanter, och förståeligheten före behandling bedömdes till ca 10%. Hon gjorde mätbara framsteg tack vare den intensiva behandlingen som pågick 2 gånger om dagen under sex veckor (Strand & Debertine, 2000). I den andra studien använde försökspersonerna initialt ickeverbal kommunikation, och 3 av 4 gjorde framsteg efter behandling med samma intensitet. Den fjärde deltagaren var svår att motivera under behandlingen och visar på vikten av egen motivation hos patienten för lyckat behandlingsresultat (Strand EA et al., 2006).

102
Patientbakgrund
Deltagarna i denna studie är två pojkar 3:4 (M) resp 2:7 (T) år gamla. M blev remitterad till logopedmottagningen i samband med 3‐årsbesöket på BVC och första kontakten var 3 månader innan denna studie påbörjades. Det finns en ärftlighet i familjen, mamma och storasyster var båda sena i sin talutveckling. Anamnesuppgifterna visar inte på några påverkande faktorer när det gäller hörsel, syn eller allmän utveckling. M har dock hypertrofa tonsiller och mamma upplevde att han var lite spänd kring munnen, det var svårt att borsta tänderna. Viss dregling förekom. M hade jollrat ganska lite och även om första orden kom vid 1 års ålder upplevde mamma ganska tidigt att hans språkutveckling var kraftigt försenad.
Vid detta första besök hade M ett mycket begränsat tal, framför allt ettordssatser noterades, men även enstaka 2‐3‐ordssatser. Han var dock mycket kommunikativ och använde spontant gester och tecken för att kommunicera. Mamma berättade att M nu sällan ville försöka säga saker eller repetera något han sagt, han var lite uppgiven och låtsades att han blivit förstådd när man samtidigt kunde se på hela kroppsspråket att han var besviken över att inte kunna förmedla sig.
Försök att bedöma fonologin gjordes med Hellqvists fonemtest, men det fick avbrytas då M inte ens ville försöka säga orden på bilderna utan antingen tecknade ordet eller skakade på huvudet och sa ett uppgivet ”nej”. I spontantalet noterades mycket assimilationer och avsaknad av flera fonem som velarer och vissa frikativor.
Språkligt bedömdes han som åldersadekvat vad gäller begrepp, satsförståelse och ordförståelse. Behandling påbörjades ca 1 gång i veckan med fokus på AKK (tecken som stöd) och artikulationsträning.
Vid senare besök gjordes en bedömning av oralmotoriken och svårigheter att runda läpparna noterades. M har också svårt att runda läpparna kring blåsleksak så att det sluter tätt. I slutet på februari fick M ett eltandborstprogram (Allmänna programmet från OMC, Danderyd) att utföra tre gånger dagligen. Eltandborststimuleringen kom igång regelbundet i början av mars då det också blev ett uppehåll i kontakten med logopedmottagningen. Remiss för bedömning och ev tonsillotomi skickades till ÖNH‐specialist.
Vid första bedömningen inför denna studie hade M gjort stora framsteg i sitt tal. Så pass att behovet av AKK nästan inte fanns kvar. Föräldrarna bedömer att stimuleringen med eltandborste var den största enskilda orsaken till dessa framsteg. M hade också fått en annan inställning till tal, var inte längre så uppgiven och ett fonemtest var nu möjligt att genomföra.
Deltagare 2 (T) kom till logopedmottagningen vid 2:2 åå, oktober 2010. Remissen skrev då han börjat få ilskeutbrott i sin förskolegrupp pga sina kommunikationssvårigheter.
T har också en ärftlig belastning, storasyster har haft kontakt med logoped som mycket liten pga sen talstart, dock ganska kortvarig. Dyslexi finns i familjen. Syn, hörsel och allmän utveckling har varit ua. T jollrade mycket lite som barn och första orden kom vid 18 månaders ålder. Vid detta första besök hade han ett fåtal ord (ca 10), och använde ett /a/ för de flesta andra ord, även vid eftersägning när han försökte härma ord. Han var mycket medveten om sina svårigheter och reagerade kraftigt på frågor som ”Vad är det?” eller ”Vad vill du ha?”. Vände sig då bort eller gick därifrån och påbörjade något annat. Behandling inleddes med inbokade besök ca varannan vecka med primärt syfte att hitta ett alternativt kommunikationssätt för T för att om möjligt minska frustration och konflikter på förskolan. Många besök blev inställda pga sjukdom, men efter ca 3 månader minskade T:s talgenans

103
betydligt, han fick lättare att härma och en mer artikulationsinriktad behandling påbörjades med syfte att börja använda mer bilabiala och dentala konsonanter. Denna behandling har pågått i ca 3 månader med besök bokade ca varannan vecka, dock flera inställda pga sjukdom.
Metod 2 deltagare med verbal dyspraxi bedöms med VMPAC och Hellqvists fonemtest (Hellqvist 2004). VMPAC (Verbal Motor Production Assessment for Children) finns ännu ej helt översatt till svenska, men har till viss del översatts av Björelius Hort (2009). De delar av testet som finns används för att bedöma oralmotorisk förmåga/praxisförmåga. Utifrån resultatet på dessa test utformas därefter en lista på 7‐8 ord som ska tränas under en behandlingsperiod. Behandlingsperioden omfattar 8 besök hos logoped under en period på 14 dagar. Inför behandlingsperioden görs en baslinjemätning med tre bedömningar under en 14‐dagarsperiod, där barnens uttal av målorden, ord med liknande fonemkombinationer samt ytterligare testningsord, totalt ca 20 ord, bedöms. Barnen får då benämna bilder, och endast i undantagsfall få en auditiv modell att följa. Bedömningstillfällena spelas in och auditiva bedömningar görs.
Under behandlingsperioden görs probetestningar då kontrollorden spelas in på nytt. Även vid probetestningarna får barnen benämna bilder, varje bild endast en gång. En sista inspelning av samma ord görs en tid efter avslutad behandling. De auditiva bedömningarna jämförs och sammanställs. Förutom en kvalitativ analys av uttalsförändringen görs också en jämförelse av resultatet i procent korrekt uttalade ord (PWC), fonem (PPC), konsonanter (PCC) och vokaler (PVC) före och efter behandling (Shriberg & Kwiatkowski, 1982).
Resultat
Deltagare 1
Deltagare 1 (M) spelades in och bedömdes inför behandlingsperioden vid tre tillfällen. En inspelning gjordes mitt i behandlingsperioden och ytterligare en ca en månad efter att behandlingen avslutats. Orden som spelades in valdes utifrån en bedömning med fonemtestet och delar av VMPAC som ännu inte finns helt tillgängligt på svenska.
VMPAC‐bedömningen inför behandlingen visade att M klarade repetition av enstaka vokaler utom /o/ som ibland istället uttalades /a/. Det hände också att /u/ avslutades med en schwa‐vokal. Repetition av nonsensstavelser som bestod av flera vokaler /oi/, /au/, /uia/ var svårare och M klarade ett fåtal repetetioner ua. CV‐stavelser gick bättre, bortsett från dentalisering av velara klusiler. Lite dålig läpprundning noterades också på de rundade vokalerna.
M medverkade inte till en full testning av ickeverbala motoriska uppgifter, men klarade läpprundning/läppspridning samt olika grad av käköppning ua. Han bedömdes dock ej ha en generell oral dyspraxi. Fonemtestet visade vokaldistortioner, dentalisering av velarer samt h‐sering av /l/ och frikativor initialt.
Bedömningarna resulterade en lista med CV‐ eller CVC‐ ord som innehöll vokalerna /œ/, // eller /e/ samt /l/ eller frikativor initialt. Bland kontrollorden fanns CVCV‐ord med samma CV eller CVC‐kombinationer för att se om någon generalisering till mer komplicerade stavelsestrukturer skulle ske. Träningsord samt kontrollord redovisas i tabell 1 där

104
träningsorden är markerade i fetstil. Transkriptionen är M:s uttal under baselinjebedöm‐ningen.
Tabell 1. Kontroll‐ och träningsord, M. Baslinjebedömning. Träningsordningen är markerade i fetstil
sol [hu:] se [he] så [ho] sover [hov] fot [hu] tå [do] såg [ho]
tåg [tot] le [je]/[le] lamm [lam] löv [jav] lök [jœt] nalle [nal] tumme [tʊm]
katt [dat] lampa [japa] penna [bn:a] kanin [ni:n] leker [let] teve [tev] bänk [bnt]
Under baslinjebedömningen började /l/ komma, vokaldistortionerna var inte heller så stora under baslinjemätningen som vid de första bedömningarna.
Totalt kom behandlingen att bestå av 7 besök på ca 25 minuter under 2 veckor. M gjorde tydliga framsteg så under de sista tillfällena tog vi in ord med pretonisk stavelse samt –l‐kluster.
Det var periodvis svårt att få M att medverka under behandlingen. Uppskattningsvis repeterades varje ord ca 15 gånger i genomsnitt under varje besök. För att öka motivationen blandade vi tidigt in för M viktiga ord, som namnet på hans leksaksdinosaurie (Nils), ordet ”pirat” samt flera av hans förskolekompisars namn (flerstaviga, i flera fall med pretonisk stavelse).Den avslutande bedömningen visade fortsatt h‐sering av /s/ och /f/, även om M under i övningssituationen klarade att fonera frikativorna ua. M dentaliserade fortfarande och växlade ibland tonlös/tonande konsontant, men i övrigt klarade han orden ua, se tabell 2. Orden valda helt utifrån egen motivation klarade han också av att säga ua.
Tabell 2. Kontroll‐ och träningsord, M. En månad efter avslutad behandling. Träningsorden är markerade i fetstil. Ord markerade med + uttalades ua, uttalet av övriga ord har transkriberats.
sol [hul] se + så [ho] sover [hovj] fot [hut] tå + såg [hot]
tåg [tot] le + lamm + löv + lök [lœt] nalle + tumme +
katt [dat] lampa + penna [bn:a] kanin [dani:n] leker [let] teve + bänk [bnt]
En jämförelse mellan procent korrekta ord, fonem, konsonanter och vokaler bland kontrollorden före och efter behandling visar på en klar ökning i samtliga fall. Resultaten redovisas i Figur 1.

105
Figur 1. Förändring i uttal mätt i procent korrekta ord (PWC), fonem (PPC), konsonanter (PCC) och
vokaler (PVC)
Deltagare 2
Samma förberedelser inför behandling planerades för deltagare 2 (T) som för M, men pga sjukdom var någon baslinje inte möjlig att göra. T har dock ett mycket begränsat tal och det är inte troligt att någon större förändring skedde under de två veckorna. En första inspelning gjordes dock vid första behandlingsbesöket, en mitt under behandlingen och en avslutande två veckor efter sista behandlingen.
Bedömning med VMPAC gjordes ca en månad före behandlingsperioden, dock inget fonemtest då T endast kan uttala ett fåtal ord. Det var svårt att få T att medverka vid bedömningen. Han repeterade enstaka fonem ua, men vid CV‐ eller VC‐stavelser fick han ibland problem med det ena fonemet. I VCV‐ord ersatte T konsonanten med en glottisstöt. CVCV med samma upprepade stavelse gick ofta bra, men med växlande stavelse höll han vokalen konstant och/eller ersatte den mediala konsonanten med en glottisstöt. T klarade de ickeverbala uppgifterna som han medverkade till ua, dvs rundning/spridning av läpparna samt olika grad av käköppning. Bedömningen var, trots dålig medverkan, att T inte har en generell oral dyspraxi.
Liksom för M sammanställdes en lista med träningsord och kontrollord, se tabell 3, träningsord är markerade med fetstil, transkriptionen är från första bedömningstillfället. Orden valdes för att träna CVC‐ och VCV‐konstruktioner samt att träna vokalerna /ʉ/ och /u/ som T ersatte med
//.
0
10
20
30
40
50
60
70
80
90
100
PWC PPC PCC PVC
Baslinje
Efterbehandling

106
Tabell 3. Kontroll och träningsord, T. Första bedömningen. Träningsorden är markerade i fetstil
min [min] pinne [miʔi] Tor [ta] ton [tn] tå [to]
då [do] tåg [do] nå [no] mat [ma] mata [maʔa]
bana [baʔa] gul [gʉ] kul [gʉ] bil [bi] bi [bi]
pil [bi] apa [aʔa] paket [ade] banan [anba] sol [dʉ]
Pga sjukdom och uteblivna besök inledningsvis i behandlingsomgången, bestod behandlingen av endast 6 besök under 10 dagar för T. Varje besök var ca 30 minuter långt och det var ibland svårt att få T att medverka. Ibland behövde han längre tid på sig att komma igång och då räckte den inbokade tiden inte riktigt till. Antalet repetitioner per ord uppskattas till i genomsnitt mellan 5 och 10 gånger vid varje besök. När han medverkade var det dock tydligt att han blev bättre och bättre på att uttala målorden. Han var till en början mycket beroende av både auditivt och visuellt stöd och sökte spontant med ögonen mot logopedens mun för att se hur orden uttalades. Hjälpstimulansen kunde gradvis minskas mer och mer och mot slutet av behandlingsperioden var han inte lika beroende av det auditiva stödet längre. Vi plockade in några extra ord som T själv valde. Det blev de övriga grundfärgerna, blå, röd och grön. I tabell 4 redovisas resultatet av den avslutande inspelningen. Där ser man att i de flesta av träningsorden finns final konsonant nu med i CVC‐ord och medial konsonant i VCV‐ord. Någon direkt generalisering av detta till övriga ord har dock ej skett. Vokaldistortionerna i samtliga ord är borta. I övningssituationen hittade T vid sista besöket även /s/ i sol, men utan hjälpstimulans blir det fortfarande klusilerat.
Tabell 4. Kontroll och träningsord, T. Två veckor efter avslutad behandling. Träningsorden är markerade i fetstil. Ord markerade med + uttalades ua, uttalet av övriga ord har transkriberats
min + pinne (ej med) Tor [tu] ton + tå +
då + tåg [to] nå + mat + mata [maʔa]
bana [baʔa] gul + kul [gʉ] bil + bi +
pil [pi] apa + paket [aje] banan [aba] sol [tu]
En jämförelse mellan procent korrekta ord, fonem, konsonanter och vokaler bland kontrollorden före och efter behandling visar på en ökning även för T, även om den inte är lika markant som för M. Tydligaste ökningen ser man på antalet korrekta ord som har fördubblats. Resultaten redovisas i Figur 2.

107
Figur 2. Förändring i uttal mätt i procent korrekta ord (PWC), fonem (PPC), konsonanter (PCC) och vokaler (PVC)
Diskussion M hade en dryg månad före behandlingsomgången påbörjat en mycket positiv utveckling av sitt tal. En trolig bidragande orsak till utvecklingen var den sensorimotoriska stimulansen med eltandborste som föräldrarna utförde 3 gånger dagligen. Att stimulans med eltandborste kan ha positiv påverkan på talutvecklingen hos barn med grav verbal dyspraxi har visats tidigare (Lundeborg & McAllister 2007). Eltandborststimulansen fortsatte även under DTTC‐behandlingen och det är svårt att urskilja hur respektive behandling påverkade utvecklingen. Tydligt under behandlingen var dock att ord som var mycket motiverande för M att lära sig, gick snabbt både att klara av att repetera och att fort införliva i spontantalet. I vissa fall behövde han bara höra och se det rätta uttalet ett fåtal gånger för att sedan kunna göra det helt själv. Detta stämmer väl överens med de slutsatser som Strand drar i en behandlingsstudie (Strand et al., 2006) där en av försökspersonerna är svår att motivera till att medverka. Resultaten visar sedan att det är bara den personen som inte gör några framsteg under behandlingen.
Viss generalisering till andra ord kunde ses. Flera av M:s egna valda ord innehöll pretonisk stavelse och vid slutinspelningen uttalade han den pretoniska stavelsen i kontrollordet. M:s tal uppfattades ofta som ”grötigt” han hade mycket saliv i munnen och en trolig orsak till detta var hans hypertrofa tonsiller. Bedömningen hos ÖNH‐läkare resulterade i ett beslut att utföra tonsillotomi och operationen utfördes några dagar efter sista inspelningen.
För T var behandlingssituationen inte optimal eftersom det ofta var så att han medverkade en stund i början av varje besök, men sedan behövde pyssla med lite annat för att efter ett tag komma igång på allvar, vilket tiden inte riktigt räckte till. Det blev inte heller lika många besök. Trots detta kan en del framsteg ses i talet.
Även för T bedömdes motivationsfaktorn som mycket stor. Han var inte 3 år fyllda och hade större behov av avbrott i form av lek. Det var svårt att få till en större mängd repetitioner före
0
10
20
30
40
50
60
70
80
90
100
PWC PPC PCC PVC
Baslinje
Efterbehandling

108
belöning och belöningarna förlorade ganska fort sin attraktion. Det var också svårt att motivera T att använda träningsorden i lite mer varierande kontext, t ex i kombination med ett annat ord. Vikten av varierande kontext för generalisering och befästande av artikulatoriskt mönster påpekas i flera studier (Aziz et al., 2010; Jacks et al., 2006). Troligt är att längre tid avsatt för varje besök, längre behandlingsperiod än 10 dagar och än mer motiverande ord som lättare vävs in i korta fraser skulle ge större och tydligare framsteg.
Någon inspelning och formell bedömning av kontrollorden i fraskontext gjordes ej för någon av deltagarna. Dock noterades att flera av kontrollorden förekom ua i spontantalet hos M, medan så inte var fallet för T.
Eftersom M redan var inne i en positiv utvecklingsperiod fanns ett stort intresse och lust att arbeta med hans tal hos hans närmaste familj och varje besök på logopedmottagningen följdes upp med fortsatt stimulans i hemmet. T visade större motstånd mot att arbeta med sitt tal hemma, och samma fokus på talträningen fanns inte i hemmet under behandlingsperioden. Detta kan förstås också ha påverkat utvecklingen under behandlingen.
Slutsatser Båda barnen i studien har gjort tydliga framsteg under den korta men intensiva behandlingsperioden framför allt när det gäller hela ord, vilket talar för att DTTC är en effektiv behandlingsmetod vid verbal dyspraxi. Trots den korta behandlingsperioden uppvisade framför allt en av deltagarna terapitrötthet och det var svårt att hitta belöningar som var motiverande nog. För ännu bättre resultat bör man nog därför vänta in högre inre motivation och därmed kunna korta ned behandlingstiden betydligt och få en effektivare behandling. Sammanfattningsvis för båda deltagarna bedöms dock själva behandlingsperioden för kort för att kunna dra några riktigt tydliga slutsatser.

109
Referenser American Sppech‐Language‐Hearing Association (2007). Childhood Apraxia of Speech [Position
Statement] Tillgänglig på http://www.asha.org/policy.
Aziz, A. A., Shohdi, S., Osman, D. M., & Habib, E. I. (2010). Childhood apraxia of speech and multiple phonological disorders in cairo‐egyptian arabic speaking children: Language, speech, and oro‐motor differences. International Journal of Pediatric Otorhinolaryngology, 74(6), 578–585. doi: 10.1016/j.ijporl.2010.02.003
Björelius Hort, H. (2009). Are Oral and Verbal Motor Functions Related to Manual and Overall Motor Performance in Children with Developmental Apraxia of Speech? Examensarbete i logopedi, Karolinska Institutet, Institutionen för klinisk vetenskap, intervention och teknik.
Caruso, A. J., & Strand, E. A. (1999). Clinical management of motor speech disorders in children. New York: Thieme.
Davis, B. L., Jacks, A., & Marquardt, T. P. (2005). Vowel patterns in developmental apraxia of speech: Three longitudinal case studies. Clinical Linguistics & Phonetics, 19(4), 249–274. doi: 10.1080/02699200410001695367.
Forrest, K. (2003). Diagnostic criteria of developmental apraxia of speech used by clinical speech‐language pathologists. American Journal of Speech‐Language Pathology / American Speech‐Language‐Hearing Association, 12(3), 376–380. doi: 10.1044/1058‐0360(2003/083)
Giuffrida, C. G., Shea, J. B., & Fairbrother, J. T. (2002). Differential transfer benefits of increased practice for constant, blocked, and serial practice schedules. Journal of Motor Behavior, 34(4), 353–365.
Hall, K. G., & Magill, R. A. (1995). Variability of practice and contextual interference in motor skill learning. Journal of Motor Behavior, 27(4), 299–309.
Hellqvist, B. (2004) Fonemtestet, stora versionen. Skivarp: Pedagogisk design
Jacks, A., Marquardt, T. P., & Davis, B. L. (2006). Consonant and syllable structure patterns in childhood apraxia of speech: Developmental change in three children. Journal of Communication Disorders, 39(6), 424–441. doi: 10.1016/j.jcomdis.2005.12.005.
Lewis, B. A., Freebairn, L. A., Hansen, A. J., Iyengar, S. K., & Taylor, H. G. (2004). School‐age follow‐up of children with childhood apraxia of speech. Language, Speech, and Hearing Services in Schools, 35(2), 122–140.
Lundeborg, I. & McAllister, A. (2007). Treatment with a combination of intra‐oral sensory stimulation and electropalatography in child with severe developmental dyspraxia. Logopedics Phoniatrics Vocology, 32(2), 71–79
Morgan, A. T., & Vogel, A. P. (2009). A cochrane review of treatment for childhood apraxia of speech. European Journal of Physical and Rehabilitation Medicine, 45(1), 103–110.
Peter, B., & Stoel‐Gammon, C. (2008). Central timing deficits in subtypes of primary speech disorders. Clinical Linguistics & Phonetics, 22(3), 171‐198.
doi: 10.1080/02699200701799825
Shriberg, L. D., Aram, D. M., & Kwiatkowski, J. (1997). Developmental apraxia of speech: II. toward a diagnostic marker. Journal of Speech, Language, and Hearing Research : JSLHR, 40(2), 286–312.

110
Shriberg, L. D., & Kwiatkowski, J. (1982). Phonological disorders III: A procedure for assessing severity of involvement. The Journal of Speech and Hearing Disorders, 47(3), 256–270.
Strand EA, Stoeckel R, & Baas B. (2006). Treatment of severe childhood apraxia of speech: A treatment efficacy study. Journal of Medical Speech Language Pathology, 14(4), 297–307.
Strand, E., & Debertine, P. (2000). The efficacy of integral stimulation intervention with developmental apraxia of speech. Journal of Medical Speech Languange Pathology, 8(4), 295–300.
Terband, H., Maassen, B., Guenther, F. H., & Brumberg, J. (2009). Computational neural modeling of speech motor control in childhood apraxia of speech (CAS). Journal of Speech, Language, and Hearing Research : JSLHR, 52(6), 1595‐1609. doi:10.1044/1092‐4388(2009/07‐0283)

111
10. Sensorisk stimulans med eldtandborste och DTTC. En kombinerad behandling i två steg tillämpat på en 3‐årig flicka med förmodad verbal dyspraxi
Vanessa Westerlind, Röstkonsulten AB, Sverige
Sammanfattning En flicka på 3:3 år med fonologiska svårigheter och förmodad dyspraxi genomgick en kombinerad behandling i två steg. Första delen av behandlingen innehöll sensorisk stimulans med eltandborste och den andra delen av behandling genomfördes med DTTC – Dynamic Temporal and Tactic Cueing. Resultatet av behandlingen visade på att kombinationen av terapiformerna gav goda resultat. Efter den kombinerade behandlingen sågs en utveckling av deltagarens antal korrekt uttalade ord samt korrekt producerade konsonanter och vokaler, en utveckling som höll samma linje som procent poäng vid probe‐testning. En tydlig stegvis förbättring sågs under behandlingssteg 2 med DTTC vilket antydde att deltagaren var mottaglig för den integrerande behandlingen. Det går inte att avgöra om samma utveckling skett om behandlingen inte kombinerats med sensorisk stimulans med eltandborste men det kan dock konstateras att behandlingen med eltandborste på egen hand inte hade samma stora effekt på deltagarens talproduktion som den kombinerade behandlingen. Faktorerna motivation, fokuserad uppmärksamhet och typen av feedback var även viktiga i framgången till resultaten.
Bakgrund
Språkljudssvårigheter och verbal dyspraxi
Barn med språkljudssvårigheter är en mycket heterogen grupp där utmaningen kan vara att skilja mellan fonologiska och motoriska svårigheter, och där även vissa fall kan innehålla drag från båda håll (Kent, 2000). En försenad tal‐och språkutveckling kan bero på en samtidig förekomst av fonologiska och motoriska svårigheter, och motoriska svårigheter kan i sig påverka utvecklingen av fonologi och andra språkliga processer, vilket kan ses hos barn med motoriska planerings‐och programmeringssvårigheter (Caruso & Strand, 1999). Det finns även

112
de barn som har en försenad oralmotorisk utveckling. Barn som huvudsakligen följer den normala utvecklingen men är något omogna och klumpiga i sin artikulation och i enkla oralmotoriska uppgifter (McAllister, 2008).
Verbal dyspraxi beskrivs enligt ett flertal definitioner som avvikande sensomotorisk planering och programmering vilket ger sig i uttryck som oförmågan eller svårighet att producera viljemässiga talrörelser, vid frånvaro av pares eller svaghet i de muskler som svarar för talrörelserna (Caruso & Strand, 1999). American Speech Language Hearing Association (ASHA) (2007) benämner tillståndet verbal dyspraxi hos barn som Childhood Apraxia of Speech (CAS) och har enats i konsensus kring tre segmentella och supersegmentella särdrag vilka ses som karakteristiska vid verbal dyspraxi. Den första gäller inkonsekventa fel av upprepad produktion av konsonanter och vokaler i stavelser och ord, den andra gäller förekomsten av förlängd och förvrängd koartikulatorisk övergång mellan fonem och stavelser, och den tredje gäller förekomsten av en avvikande prosodi speciellt gällande ord‐och satsintonation hos dessa barn. Dessa drag ska dock inte ses som den enda och nödvändiga vid indikation om verbal dyspraxi (ASHA, 2007). Andra grundläggande symtom som kan förekomma vid verbal dyspraxi är svårigheter att utföra artikulatoriska uppgifter på uppmaning, trevande osäkra talrörelser, svag distinktion mellan tonande ‐tonlös, nasal‐ickenasal, aspirerad –oaspirerad samt specifika frikativor. Vanligen blir svårigheterna mer framträdande i och med ökat antal stavelser. Öppna stavelser, som /ka/ och /ga/ och onomatopoetiska ord kan länge dominerar talet hos barn med verbal dyspraxi (McAllister, 2008).
Behandling
Målsättningen med behandlingen vid verbal dyspraxi är en förbättrad kontroll av artikulatorerna och en ökad automatisering av talrörelser. Att inleda behandlingen med en kombination av enklare imitation och sensorisk taktil stimulans är vanligt (McAllister, 2008). Flera undersökningar har visat att sensorisk stimulans kan förändra retningen av motorneuron och förbättra motorkontroll och orofacial funktion (Andreatta & Barlow, 2003; Hejdedal & Westerlind, 2010; Hägg & Larsson 2004). Sensoriken är en viktig del av talet, där taktil och proprioceptiv feedback har stor betydelse för inställning och positionering av artikulationerna (Grossman, 1967). Interaktion mellan sinnesintryck och motorik gör att vi kan uppleva perception av vår egen kropp, planera och koordinera vår motorik, automatisera rörelser och rätta till rörelser i riktning och hastighet (Edebol Eeg‐Olofsson, 2001).
Behandling med eltandborste kan användas som verktyg för att ge vibrationer vid oralsensorisk stimulering. I en studie av Lundeborg och McAllister (2007) utvärderades en kombinerad behandling av oralsensorisk stimulans med eltandborste och elektropalatografi (EPG)‐terapi hos en flicka med grav verbal dyspraxi. De fann att kombinationen av terapiformerna gav goda resultat. Det framkom att flickans tal var förbättrat efter behandling med eltandborste i behandlingens första del, och att ytterligare förbättringar i artikulation och i talförståelighet kunde ses efter andra delen med EPG. Intraoral stimulans kan uppmärksamma och guida barnet i upptäckandet av tungans och läpparnas funktion. En förbättring av viljestyrd kontroll kräver dock aktiv och upprepad daglig träning (Autti‐Rämö, 2001). Viss kritik finns dock mot användningen av oralmotoriska övningar i behandling av talmotoriska svårigheter som inte innefattar diagnosen dysartri, exempelvis verbal dyspraxi. Det är dock viktigt att mot denna kritik sätta innehållet av behandling. I vilken kontext övningar används, för vilka barn samt för till hur stor del och under vilken tidpunkt i behandlingen (McCauley & Strand, 2008). Störst oro menar författarna McCauley och Strand, är när

113
oralmotoriska övningar används utan analys, isolerat eller som främsta behandlingsmetod för barn med verbal dyspraxi utan samtidig förekomst av dysartri.
En integrerad modell är troligtvis den vanligaste vid behandling av barn med verbal dyspraxi och innebär behandling där barnet härmar yttrande utifrån modell från logopeden. Fokus ligger både på auditiv och visuell information (Strand & Skinder, 1999). Övning efter modell fungerar vanligen bättre för barn med talmotoriska svårigheter då komplicerade och långa verbala instruktioner kan hämma förmågan att förstå och följa med i uppgifter (Caruso & Strand, 1999). Dynamic Temporal and Tactile Cueing (DTTC) är en integrerad behandlingsmetod som innefattar direkt imitation och instruktioner som ”lyssna på mig, titta på mig” där fokus ligger på rörelsemönstret för hela målorden och inte på de enskilda ljudsekvenserna. Taktila och gestikulerande ledtrådar används ofta för att underlätta inlärningen. DTTC håller sig till principer för motorinlärning i upplägget av behandling, så som i valet av storleken på stimuli‐materialet, antalet repetitioner och användning av underlättande tekniker som tar liten tid och håller barnets fokus till logopedens ansikte. De visuella, auditiva och taktila ledtrådarna suddas successivt ut i syfte att låta barnet utveckla en mer självständig skicklighet och förhoppningsvis med tiden till en mer automatiserad produktion (McCauley & Strand, 2008).
Principer för motorisk inlärning
I utformandet av behandling för barn med verbal dyspraxi är det viktigt att känna till och ta hänsyn till grundprinciperna för motorisk inlärning. Motorisk inlärning etableras genom erfarenheter som vi får utifrån praktiserande. Det finns tre grundläggande faktorer för motorinlärning; trygghet, motivation och fokuserad uppmärksamhet. Alla tre faktorer påverkas av det stimuli som används i behandlingen, dvs. vilka ord eller uttryck som används samt antalet och hur dessa presenteras och bearbetas. Valet bör anpassas så att tillräckligt med fokus finns för utförandet av den motoriska färdigheten som man vill träna (Caruso & Strand, 1999).
Två återkommande och särskiljande begrepp inom motorisk inlärning är samlad och spridd variation av övning och kan ses på utifrån innehåll, framförande och utförande av övning. Samlad övning kan vara exempel på när en rörelse eller ett set av rörelsemönster som i en stavelse övas upprepade gånger, medan spridd övning består av varierande rörelse som övas i olika kontexter och former som prosodi och volym. Samlad övning tenderar att ge snabba resultat av den specifika rörelse som tränas men med en begränsad användning i andra kontexter. Den spridda formen är långsammare i inlärning men åstadkommer användning i andra kontexter. Inlärningen har då inte fokus på en specifik motoriskförmåga utan på motorinlärning (Caruso & Strand, 1999). Användningen av de olika formerna är beroende av vilken motoriskförmåga som tränas (McCauley & Strand, 2008).
Behandlingsupplägg utifrån principerna för motorisk inlärning
Träningens intensitet varierar beroende på grad av svårighet och kan skilja sig mellan färre längre sessioner och kortare sessioner utspridda över fler tillfällen. För barn med utmärkande svårigheter förespråkas träning i kortare stunder vid fler tillfällen. Ett upplägg med färre men längre sessioner innehåller vanligen ett litet mindre antal stimuli, ett ord eller en fras för att barnet snabbt ska kunna ta till sig den motoriska förmågan. För kunna etablera motorinlärning och generalisera rörelsen till andra uttalanden behövs dock mer fördelade, korta sessioner.

114
Utvecklingen går inte lika fort men träningen ger mer överförbarhet till situationer utanför träningssituationen (Strand & Skinder, 1999).
Val av stimuli utgår ifrån stavelse struktur och innehåll av målljud, dvs. längd och fonetisk kontext. Stavelsestrukturen kan variera från CV‐ eller VC‐stavelser till CVC‐ till CCVC‐strukturer och vidare till längre ord, fraser och meningar. För barn som bara har vokaler i sitt tal börjar man vanligen med CV‐ och VC‐strukturer. I behandlingen ligger inte alltid fokus på måljuden utan innehållet av rätt antal stavelser, målljuden kan rättas till därefter. Det är viktigare att får barnet att utveckla längre stavelser än att ljuden ska vara rätt producerade. I val av målljud utgår man ifrån fonem som står barnet nära i utvecklingen. De fonem som utvecklas tidigast är vanligen mer synliga och har maximal auditiv och artikulatorisk kontrast. För att öva på kontrast och flexibilitet kan målorden till en början vara nonsensord för övning att växla mellan vokal och konsonant ex. bababa. Vidare byts den ena vokalen (baby) eller konsonanten (bada) ut. Vidare övning innehåller övning för flexibilitet från främre till bakre artikulationsställe, ex. katt, tack. För motivationen kan det vara bra att välja målord som är användbara och funktionella för barnet utanför träningssituationen. Det kan ge positiv upplevelse av att använda talet och ger barnet verktyg att uttrycka sig bättre i situationer med tidigare misslyckanden (Strand & Skinder, 1999).
Storleken, antalet stimuli variera också i och med svårighetsgrad hos barnet. För de barn som har grava svårigheter, få till inga förståeliga yttranden, inleds behandlingen med ett litet set innehållande 5‐6 stimuli/ord. Fler ord läggs sedan till och storleken blir större i och med att de motoriska processerna blir lättare. För barn med måttliga svårigheter är 8‐10 ord att föredra. För barn där de fonologiska svårigheterna bedöms vara det primära men där motoriska svårigheter även finns, kan antalet vara större men mer hänsyn bör tas till andra principer av motorinlärning som frekvensen av antalet repetitioner av rörelsemönstret. Valet av antalet repetitioner kan även ses utifrån motorinlärningsprinciperna mängd och spridd träningsform. Antalet repetitioner varierar från 10‐20 gånger och är beroende av antalet målord och om målorden presenteras i block eller randomiserat. I grunden beror antalet repetitioner på hur rätt, med vilken ansträngning, hastighet och prosodi barnet producerar orden. Tiden mellan modell och barnets yttranden blir även successivt mindre och mer randomiserat, vilket ger mer utrymme för användning av det motoriska minnet i planering av målordens rörelsemönster. (Strand & Skinder, 1999)
I behandlingsutförandet är det även viktigt att ta hänsyn till användningen av feedback och rörelsernas hastighet. Feedback kan ges för att skapa en medvetenhet om resultat och utförande. Det är viktigt att undvika fördröjning mellan utförandet och feedback. Det är inte heller effektivt att ge feedback vid varje utförande utan med större fördel efter några övningar. För mycket information kan missgynna istället för att stärka, speciellt för barn. Hastigheten i talrörelsen som utövas bör vara förminskad i början och gradvis öka till naturlig hastighet och prosodi. Vid minskad hastighet är det lättare att fokusera. Mer uppmärksamhet läggs på rörelserna och mer proprioceptiv feedback uppstår. Vid en långsammare hastighet ökar också rörelseomfånget. Ett för sakta tempo kan dock fördärva rörelsen och tajmingen, det är därför viktigt som kliniker att testa olika hastigheter i behandlingssituationen (Caruso & Strand, 1999).

115
Syfte och frågeställning Syftet med följande studie var att undersöka om en kombinerad behandling i två steg, del 1 med sensorisk stimulans med eltandborste och del 2 med behandling enligt DTTC, kunde utveckla talproduktionen hos en 3‐årig flicka med fonologiska svårigheter och förmodad verbal dyspraxi.
Metod
Deltagare
En flicka på 3:3 år som gick i behandling för sina fonologiska svårigheter tillfrågades genom målsmans godkännande att delta i studien. Flickans språkförståelse var god men hennes tal, som bestod av meningar, hade stora variationer innehållande rena och mycket svårförståeliga ord och frågetecken om eventuella inslag av verbal dyspraxi fanns. Hennes yttranden innehöll varierande vokalanvändning, förenkling av stavelsestruktur samt svårigheter med växling av konsonant och förekomst av h‐sering. Hon var svårförståelig hemma så som för andra utomstående och kunde bli ledsen, arg och förtvivlad när hon inte blev förstådd. Hörseln var undersökt och utan anmärkning. Information om behandlingsstudiens upplägg, inkluderande vikten av daglig träning hemma, gavs till flickans mor innan studien startades.
Utformning
Den kombinerade behandlingen bestod av två steg, där steg 1 innehöll sensorisk behandling med eltandborste i fem veckor och steg 2 innehöll behandling enligt DTTC i tre veckor. Mellan dessa två steg förekom ett uppehåll på sju veckor då ingen form av behandling genomfördes.
En multiple baseline‐mätning av deltagaren utfördes innan start av behandlingen, en gång i veckan i tre veckor. Mätningen innehöll test med NOT‐S (Bakke, Bergendal, McAllister, Sjögren & Åsten, 2007), test av tvåpunktsdiskriminering på läppar och tungspets samt oral stereognostisk förmåga ur STORM (Henningson, McAllister & Harstein, 2007) samt status av konsonant‐, vokal‐och ordproduktion med Fonemtest Kortversion (Hellqvist, 1984). Det sista tillfället för multiple baseline‐mätningen följdes av start av behandlingssteg 1 under samma besök. Samma mätinstrument som vid baseline‐mätningarna användes sedan för att utvärdera behandling; i slutet av sista behandlingstillfället för steg 1, efter uppehållet innan start av behandling steg 2 efter sista behandlingstillfället steg 2. Mätningarna i samband med behandlingsstegen benämns som mätning 1, 2 eller 3 efter den ordning de utfördes. Alla ovanstående mätningar videofilmades och analyserades i efterhand i slumpmässig ordning. Vid baseline‐mätningens första tillfälle samt vid sista mätningen efter steg 2 intervjuades deltagarens moder med frågorna från NOT‐S intervjudel.
En vecka efter start av behandlingssteg 1 start inkluderades ”probe‐test” (Strand & Skinder, 1999) i studien, vilka utfördes av författande logoped under resterande behandlingsbesök för båda stegen vilka till antalet blev sju tillfällen. Probe‐testningen innehöll 10 målord med initial bilabial med CVC‐och CVCV‐struktur; bok, boll, mugg, mun, pall, paj, pöl, bada, bulle, måla. Dessa ord valdes ut för att matcha strukturen av aktuellt behandlingsinnehåll. Orden valdes även ut efter Praxismaterialets bilder och med tanke på att de skulle vara användbara i deltagarens vardag. Varje ord presenterades fem gånger med en bild i en slumpmässig ordning i olika lek‐ och spelövningar.

116
I tabell 1 nedan finns en översikt över studiens utformning. Under behandlingens steg 1 träffade deltagaren författande logoped vid 5 tillfällen inkluderande mätning 1. Under behandlingens steg 2 var besöken tre till antalet inkluderande mätning 2 och 3. Under de veckor då inga besök förekom under behandlingsstegen utfördes behandlingen fortsatt dagligen hemma.
Tabell 1. En översikt över studiens upplägg samt bedömningarna i samband med baseline och de olika behandlingsstegen. F. K = Fonemtest Kortversion, NOT‐S U = NOT‐S undersökningsdel, STORM= Stockholms Oralmotoriska bedömningsprotokoll.
Baseline
mätning
Behandling
steg 1
Mätning 1 UPPEHÅLL 7 v.
Mätning 2 Behandling
steg 2
Mätning 3
NOT‐ S
STORM
F.K
5 veckor
Sensorisk
stimulans
med
eltandborste
4 probe‐test
NOT‐ S
STORM
F.K
NOT‐ S
STORM
F.K
3 veckor
DTTC
3 probe‐test
NOT‐ S
STORM
F.K
Behandlingens innehåll
Behandlingens steg 1 innehöll ett träningsprogram med eltandborste utformat efter modell från Oralmotorikteamet, Universitetssjukhuset Linköping och bestod av sju övningar (se bilaga). Varje övning utfördes fem gånger med korta, snabba stimuleringar i form av ”duttar”. Övningarna utfördes hemma dagligen medförälder och hos författande logoped en gång i veckan innan probe‐testningen.
Behandlingens steg 2 innehöll ett DTTC‐inspirerande tillvägagångssätt där deltagaren tränade på produktionen av åtta återkommande målord; båt, bil, mus, mätt, pil, baka, matta, mygga. Dessa ord valdes ut efter tidigare innehåll i deltagarens behandling som bestod av övningar för träning av bilabial i initial position i CVC‐ och CVCV‐struktur. Även dessa ord var tagna från Praxismaterialets bilder, utvalda efter möjlig användning i vardagen för deltagaren. Deltagaren fick under dessa övningar taktil, visuell och auditiv guidning och stimuli bearbetades i enlighet med DTTC från stöd till mer och mer självständig produktion om så var möjligt. Deltagaren presenterades för varje målordet i form av en bild som hon uppmanades benämna. Först testades ett visuellt stöd där författande logoped sökte deltagarens fokus till logopedens mun och de tillsammans producerade målordet. Om deltagaren behövde mer stöd användes taktil guidning genom att känna av och stanna länge i de olika positionerna för ljudproduktionen. Deltagaren fick även beskrivning och liknelser av hur artikulatorerna skulle röra sig och rörelsen för målordet vävdes samman utan ljud, tillsammans och sakta från mer till mindre stöd. Därefter lades ljudproduktion till rörelsemönstret och även här från mer till mindre stöd där deltagaren i slutet uppmanades repetera målordet på egen hand. Repetitionerna av varje målord utfördes cirka 20 gånger om inte målordet var uppnått, om så var fallet uppmanades deltagaren att repetera korrekt producerat målord fem gånger innan övergång till nästa målord. Behandlingen hemma utfördes en gång om dagen av förälder efter

117
instruktion i slutet av varje behandlingstillfälle, ibland var föräldern med i rummet under hela behandlingstillfället. För att skapa motivation och ge direkt feedback utövades stimuli i olika aktiviteter som spel eller målning, där deltagaren exempelvis kunde få stämpla en figur eller rita en del av en teckning efter utfört målord.
Vid första behandlingstillfället uppmärksammades att deltagaren hade mycket svårt att hitta produktionen av /t/ och /d/ som istället velariserades. Korrekt produktion av de utvalda orden var därav svår att uppnå och under första veckan på behandlingssteg 2 koncentrerades träningen till initial /t/ i enkel CV‐struktur. Resterande veckor fortsatte träningen med de från början utvalda orden trots svårigheter för deltagaren att producera dental klusil. Träning under detta behandlingssteg utfördes i likhet med steg 1 hemma dagligen tillsammans med modern i några minuter och en gång i veckan tillsamman med författande logoped i samband med probe‐testningen.
Analysmetoder
Ett medelvärde med standardavvikelse för bedömningstillfällenas resultat under multiplebaseline‐mätningen jämfördes med resultaten på mätning 1‐3. För NOT‐S intervjudel samt undersökningsdel beräknades råpoäng, från 0 till max 16 poäng per del, istället för materialets ursprungliga beräkning med en totalpoäng på 6 poäng, där 1 poäng ges peranmärkning per domän. Råpoängen ger en mer differentierad bild av individuell funktion eller dysfunktion. 1 poäng gavs vid ej korrekt utförd uppgift eller om deltagaren inte visade på något försök till utförande. Uppgiften pa‐ta‐kabedömdes inte enligt instruktioner för testet på barn under fem år. Enligt svenska normering av Gustavsson, Skoglund & Thelin (2007) kan barn med en typisk utveckling i åldergruppen 3:0–3:11 förväntas få en totalpoäng på 1,41 ± 0,96 för hela testet. Vilket kan tolkas som att anmärkning inom mer än tvådomäner bedöms som avvikande.
Bedömning av tvåpunktsdiskrimination och stereognostisk förmåga beräknades i enlighet med STORM:s manual. Tvåpunktsdiskriminationen kunde godkännas på 3, 5 eller 10 mm avstånd och vid test av stereognostisk förmåga beräknades antal felsvar med ett max på 8 poäng. Normering av tvåpunktsdiskrimination och intraoral stereognostisk förmåga av Andersson & Buhr (2009) fastställde ett medelvärde av antalet felsvar för tvåpunktsdiskrimination på 0,5 ± 1,1 och för stereognostisk förmåga på 3,1±2,2 för pojkar och flickor i åldern 5:6–5:11 år.
Resultatet på Fonemtest kortversion transkriberades och analyserade genom beräkning av PCC –Percentage of Consonants Correct efter modell av Shriberg & Kwiatkowski (1982) och med tillägg av PVC – Percentage of Vowels Correct och PWC – Percentage of Words Correct. Alla värden i resultatet avrundades till tal med en decimal.
Utöver resultaten ovan jämfördes probe‐testningarnas resultat från de sju tillfällena. Varje ord poängsattes vid probe‐testnigen med 0, 1 eller 2 poäng efter liknande modell av Yoder, Camarata och Gardner (2005) vid bedömning av förståelighet av tal hos barn med tal‐ och språksvårigheter. 0 sattes för icke korrekt produktion, 1 poäng om yttrandet innehöll korrekt initial konsonant samt efterföljande rätt vokal eller om yttrandet innehöll rätt antal fonem i stavelsestrukturen samt rätt artikulationsställe för den initiala konsonanten, och 2 poäng sattes för yttrande som var korrekt producerade. Poängen räknades sedan samman för alla målord som presenterats fem gånger och procent av antal poäng beräknades i jämförelse med högsta möjliga poäng för varje tillfälle, vilket var 200.

118
Resultat
NOT‐S
Poängen för NOT‐S undersökningsdel var bestående 1 poäng, för taluppgiften vid alla tillfällen. Vid NOT‐S intervjudel fick deltagaren 3 poäng fördelat på två områden (sensorik och vanor) innan den kombinerade behandlingen och 1 poäng efter inom området vanor. Innan behandlingen framkom enligt modern beteenden om att deltagaren stoppade så mycket mat i munnen så att det ibland blev svårt att tugga och hon spottade ut maten. Hon bet på naglarna samt sög och bet lite på läppen. Efter den kombinerade behandlingen bet deltagaren fortfarande på naglarna varje dag men de andra beteendena uppgavs inte längre. Totalt sett visar deltagaren avvikelser inom 3 domäner innan behandlingen och inom 2 efter behandlingen, vilket ger 3 respektive 2 poäng enligt NOT‐S ursprungliga beräkning och kan jämföras med medel för hennes åldergrupp (3:0–3:11) på 1,41 ± 0,96 poäng.
Tvåpunktsdiskrimination och intraoral stereognostisk förmåga
Vid test av tvåpunktsdiskrimination på läppar och tunga klarade deltagaren av att diskriminera på 3 mm avstånd för nästan alla delar vid alla tillfällen, med undantag för 5 mm för höger underläpp vid den första baseline‐mätningen och 5 mm för vänster överläpp vid baseline‐mätning 2. Under de resterande mätningarna var resultatet alltid 3 mm för var del. I Figur 1 nedan redovisas resultaten vid test av intraoral stereognosi med en standardavvikelse (SD) på 0,6 för baseline‐mätningen.
Figur 1. Deltagarens antal felsvar vid test av oral stereognosi.
Antalet felsvar är inom gränsvärdet för åldersgruppen 5:6–5:11 år (Andersson & Buhr, 2009) vid alla mättillfällen. Antalet felsvar minskar efter behandlingens steg 1 och är det samma efter uppehållet, men ökar med en poäng efter behandlingens steg 2 och ligger i nivå med resultat vid baseline‐mätningen.
Konsonant‐, vokal‐och ordproduktion
I Figurerna 2‐4 nedan redovisas procent korrekt producerade konsonanter (PCC), vokaler (PVC) och ord (PWC) utifrån Hellquist fonemtest kortversion. Bredden av deltagarens förenklade fonologi samt variationen mellan konsonant och vokal syns. Konsonant‐ och
Baseline Mätning 1 Mätning 2 Mätning 3
0
1
2
3
4
5
An
tal f
elsv
arl

119
vokalproduktionen tycks dock ha en gemensam utveckling, från en mindre procentandel korrekt producerade efter behandlingssteg 1 och till en stegvis ökad andel efter uppehållet och start av behandlingssteg 2. Andelen korrekt producerade ord är störst efter behandlingssteg 2.
Vid baseline‐mätningarna förekom endast apa korrekt producerat vid första mätningen efter behandlingssteg 1 och efter uppehållet producerade deltagaren napp korrekt men förenklade apa. Vid sista mätningen efter behandlingssteg 2 producerade deltagaren fyra ord korrekt; apa, napp, bok och nalle.
Probe‐testning
I Figur 5 nedan redovisas probe‐testernas resultat och utveckling under hela behandlingsperioden. Under behandlingssteg 1 ses en något svag förbättring, men som sedan sjunker till en procentandel under baseline vid mättillfälle 4, i slutet av sista
Baseline Mätning 1 Mätning 2 Mätning 3
0
10
20
30
40
50
60
70
80
90
100
Pro
cent
Baseline Mätning 1 Mätning 2 Mätning 3
0
10
20
30
40
50
60
70
80
90
100
Pro
cent
Baseline Mätning 1 Mätning 2 Mätning 3
0
10
20
30
40
50
60
70
80
90
100
Pro
cent
Figur 2. Antal korrekt producerade konsonanter i procent (PCC), SD 2,31 vid baseline
Figur 3. Antal korrekt producerade vokaler i procent (PVC), SD 0 vid baseline.
Figur 4. Antalet korrekt producerade ord i procent (PWC), SD 0,81 vid baseline.

120
behandlingstillfället för steg 1. Efter uppehållet och start av behandling steg 2 har procent andelen poäng ökat och fortsätter att stiga.
Figur 5. Procent rätt vid probe‐test av 10 ord. Tillfälle 1‐4 är utförda under behandlingssteg 1, tillfälle 5 vid start av behandlingssteg 2 och tillfälle 6 och 7 under samt vid avslut av behandlingssteg 2.
Diskussion och konklusion Resultaten vid NOT‐S undersökningsdel var bestående för deltagaren och uteslöt förekomst av oralmotoriska svårigheter utan verbalt inslag, då poäng endast gavs vid test av talproduktion. Viss förändring av deltagrens beteende framkom dock vid NOT‐S intervjudel. Efter behandlingen noterade modern ingen avvikelse inom domänen sensorik. Vad förändringen kan beror på kan diskuteras kring ålderns eventuella påverkan på utveckling av beteende men även sättas samma med ett mer stabilt resultat vid tvåpunktsdiskrimination och oral stereognosi efter behandlingens steg 1.
Totalt sett fick deltagaren 3 poäng vid NOT‐S (undersökningsdel och intervjudel) innan behandlingen vilket är något över testnormen och 2 poäng efter behandlingen vilket är inom testnormen.
Resultaten för tvåpunktsdiskrimination och oral stereognosi var inom normen redan vid baseline‐mätningen men deltagaren fick ett något bättre resultat efter behandlingsens steg 1, vilket nämnts ovan. Poängsättningen för oral stereognosi ökade dock vid sista mättillfället efter behandlingssteg 2 till samma värde som vid baseline. Skillnad är dock inte stor, inom normalvariationen och tycks inte alls påverka utvecklingen av deltagarens talproduktion. Vid sista mätningen efter behandlingssteg 2 producerade deltagaren fyra ord korrekt; apa, napp, bok och nalle, vilket är en ökning i jämförelse med de tidigare mättillfällena då deltagaren producerad ett korrekt målord. I stort ökade även deltagarens korrekt producerade konsonanter och vokaler med en u‐formad ökning, vilket även poängen vid probe‐testningen gjorde. Vid mättillfälle 1 av korrekt producerade konsonanter och vokaler och probe‐test tillfälle 4, efter behandlingens steg1, fick deltagaren ett lägre resultat än vid baseline. Resultatet kan ha påverkats av deltagarens dagsform, men även vara ett resultat i linje med
1315
16
10
20
31
41
1 2 3 4 5 6 7
0
10
20
30
40
50
60
70
80
90
100
Probe‐test tillfälle
Procent

121
en u‐formad utveckling, där deltagaren lär sig hantera de olika språkljuden och dess rörelsemönster. Trots dippen i mätresultaten och ett uppehåll på sju veckor med ingen förekomst av annan stimulans sågs en förbättring av antalet korrekt producerade konsonanter och vokaler samt en ökad procent poäng vid probe‐testningen vid mättillfälle 2 och prob‐test tillfälle 5. Därefter sågs en stegvis förbättring under behandlingssteg 2 med DTTC vilket tyder på att deltagaren var mottaglig för den integrerande behandlingen och utvecklades motoriskt då probe‐orden som inte tillämpades i behandlingen följde samma utveckling. Ett samband ses även mellan probe‐test orden och orden i fonemstatuset. Alla ord förutom nalle innehåller bilabialer, vilket behandlingens innehåll syftade tillträning av.
Resultatet av behandlingen visar att kombinationen av terapiformerna gav goda resultat för deltagaren som utvecklade sin talproduktion. Om utvecklingen varit den samma om behandlingen inte kombinerats med sensorisk stimulans med eltandborste är dock svårt att avgöra i denna studie. Det kan dock konstateras att behandlingen med eltandborste på egen hand inte hade samma stora effekt på deltagarens talproduktion som den kombinerade behandlingen. Viss påverkan med tillämpning av sensorisk stimulans syns dock i likhet med Lundeborg och McAllister (2007). Faktorerna motivation, fokuserad uppmärksamhet och typen av feedback var även viktiga i framgången till resultaten. Efter behandlingen kunde deltagarens uppmärksamhet lätt ledas till behandlarens mun och deltagaren tog snabbt efter modell. Resultaten visar att en kombinerad behandlingsmetod som innehåller sensorisk stimulans och som även följer principerna för motorisk inlärning kan vara lämplig för mindre barn som har fonologiska svårigheter som varken har det typiska utvecklingsmönstret eller diagnosen verbal dyspraxi, men förmodade planerings‐ och programmeringssvårigheter.
Av tidsmässiga skäl kunde inte en långvarig effekt av den kombinerade behandlingen undersökas. Inte heller kunde fler behandlingstillfällen genomföras under behandlingsperioden. Det skulle varit intressant att se om utveckling varit större om kontakten med logoped varit större och om utvecklingen skulle fortsätta i samma linje vid fortsatt användning av den integrerande behandlingen.

122
Referenser Andersson, M. & Buhr, U. (2009). Normering av test av intraoral stereognosi och
tvåpunktsdiskrimination hos barn i åldrarna 5;6‐7;0 år. Examensarbete i logopedi. Linköping: Institutionen för klinisk och experimentell medicin.
Andreatta, D.R. & Barlow, M.S. (2003).Movement‐related modulation of vibrotactil detection thresholds in the human orofacial system. Experimental Brain Research, 149, 75–82.
American Speech Language and Hearing Association (2007). Childhood Apraxia of Speech[Position Statement]
Autti‐Rämö, I. (2001). Pediatric neurological aspects on oral motor activity. In: Sillanpää, M. (ed.):Practices in Orofacial Therapy. Turku:Painosalma, s.7‐10.
Bakke, M., Bergendal, B., McAllister, A., Sjögren, L. & Åsten, P. (2007). Development and evaluation of comprehensive screening for orofacial dysfunction.Swedish Dental Journal, 31(2), 75–84.
Caruso, J.A. & Strand, A. E. (1999). Motor Speech Disorders in Children: Definitions, Background, and a Theoretical Framework. In: Caruso, J.A. & Strand, A.E. (Eds). Clinical Management of Motor Speech Disorders in Children. New York: Thieme, s.1–28.
Edebol Eeg‐Olofsson, K. (2001).Neurophysiological aspects on oral motor activity. In: Sillanpää, M. (ed.): Practices inOrofacial Therapy. Turku: Painosalma, s.1‐5.
Grossman, R. C. (1967). Methods of determing oral tactile experience.In: Bosma, J. F. (ed.). Symposium on oral sensation and perception,Springfield: Charles C. Thomas. s. 161–181.
Gustavsson, C., Skoglund, C. & Thelin, H. (2007). Normering av Orofacialt Test – Screening (NOT‐S) för barn i åldrarna 3 till 6 år. Examensarbete i logopedi. Linköping: Institutionen för klinisk och experimentell medicin.
Hejdedal, M. & Westerlind, V. (2010). Effekten av intra‐ och extraoralsensorisk intensivbehandling med eltandborste ‐ hos nio barn med Down Syndrom. Examensarbete i logopedi. Linköping: Institutionen för klinisk och experimentell medicin.
Hellqvist, B. (1999). Praxis. Pedagogisk Design, Malmö
Hellqvist, B (2004). Fonemtest Kortversion. Skivarp: Pedagogisk Design, 4 uppl.
Henningson, G., McAllister, A. & Harstein, M, (2007). STockholms ORalMotoriska bedömingsprotokoll.Stockholm: Danderyds sjukhus & Karolinska Institutet.
Hägg, M. & Larsson, B. (2004). Effects of Motor ans Sensory Stimulation in Stroke Patients with Long‐Lasting Dysphagia. Dysphagia. 19, 219–230.
Kent, R.D.(2000). Research on speech motor control and its disorders: a review and prospective.Journal of CommunicationsDisorders. 33(5), 391–428.
Lundeborg, I. & McAllister, A. (2007). Treatment with a combination of intra‐oral sensory stimulation and electropalatography in child with severe developmental dyspraxia. Logopedics Phoniatrics Vocology, 32(2), 71–79.
McAllister, A. (2008). Oralmotoriska störningar hos barn och ungdomar. I: Hartelius, L.,
Nettelbladt, U. & Hammarberg, B. (red.). Logopedi. Lund: Studentlitteratur, s. 377–386.
McCauley, J. R & Strand, A, E (2008). Treatment of Childhood Apraxia of Speech: Clinical Decision Making in the Use of Nonspeech Oral Motor Exercises. Semin Speech Lang, 29, 284–293.

123
McCauley, J. R & Strand, A, E (1999). Treatment of Children Exhibiting Phonological
Disorder with Motor Speech Involvement. I: Caruso, J.A. & Strand, A.E. (Eds). Clinical Management of Motor Speech Disorders in Children. New York: Thieme, s. 187–208.
Shriberg, L.D., & Kwiatkowski, J. (1982). Phonological Disorders III: a Procedure for Assessing Severity of Involvement. Journal of Speech and Hearing Disorders, 47, 256–270.
Strand, A.E & Skinder, A. (1999). Treatment of Developmental Apraxia of Speech: Integral
Stimulation Methods. I: Caruso, J.A. & Strand, A.E. (eds.). Clinical Management of Motor Speech Disorders in Children. New York: Thieme, s. 109–148.
Yoder, P., Camarata, S. & Gardner, E. (2005). Treatment Effects on Speech Intelligibility and Length of Utterance in Children with Specific Language and Intelligibillity Impairments. Journal of Early Intervention, 28, 34–49.