Embed Size (px)
Citation preview
SKELETAL SYSTEM
Science OlympidaAnatomy and Physiology
2009-2010Kathy Tripepi-Bova MSN, RN, CCNS, CCRN
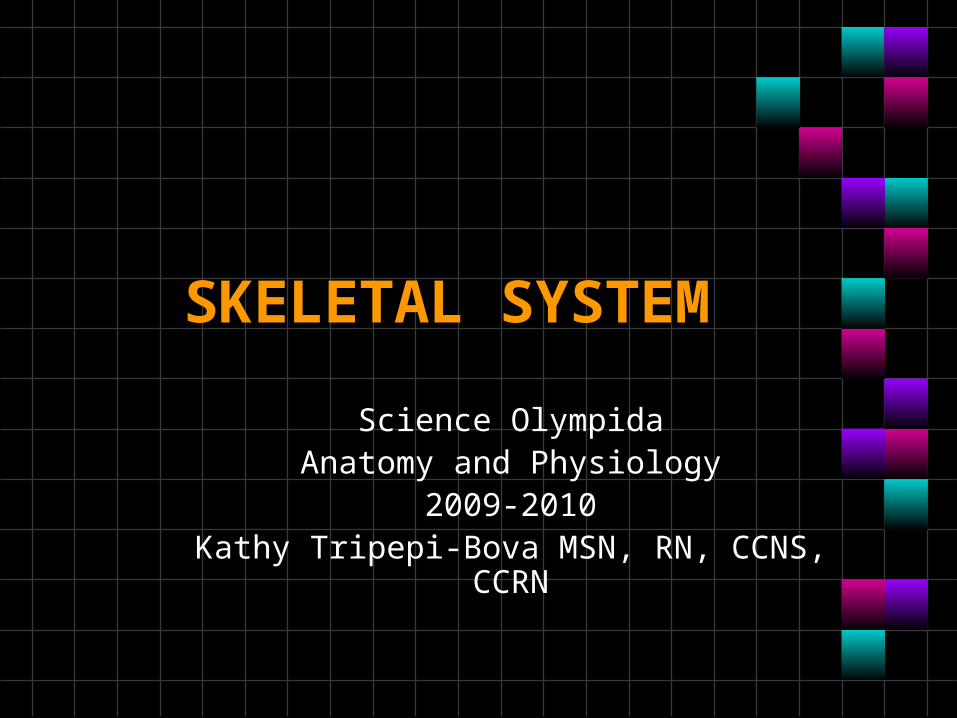
http://www.personal.psu.edu/faculty/j/a/jas43/skel/skeletal.htm
Functions
• Support & shape to body• Protect internal organs• Allow for movement in union with muscles• Storage of minerals (calcium,
phosphorus) & lipids• Blood cell production
Skeletal sections
• • 206 Bones• Axial skeleton: (80 bones) in
skull, vertebrae, ribs, sternum,hyoid bone
• Appendicular Skeleton: (126bones)- upper & lower extremitiesplus two girdles
• Half of bones in hands & feet

Radiography
X-ray of arm
CT
MRI
Types of Bones: Classification by shape
• Sesamoid bones: short bones within tendons (e.g.: patella)
• Flat bones: thin, flat & often curved (e.g.: sternum, scapulae, ribs & most skull bones)
• Irregular bones: odd shapes; don't fit into other classes (e.g.: hip bones & vertebrae
• Long bones – longer than they are wide (e.g., humerus)
• Short bones- cube shaped bones of the wrist and ankle
• Wormian bones: tiny bones in between major skull bones
Vertebrae (33)• Cervical (7)- transverse foramina, bifid
spinous processes, vertebral prominens• Atlas- 1st; supports head• Axis- 2nd; pivots to turn head
• Thoracic (12)- long spinous processes, rib facets
• Lumbar (5)- large bodies thick, short spinous processes
• Sacrum (5 fused)-five vertebrae fused at faint grooves called transverse lines
• Coccyx (4 fused)-”tail bone”
Articulating joint
• Articular capsule: a fibrous sac at a synovial joint that contains synovial fluid
• Articular capsule• External layer is a tough fibrous capsule that is
an extension of the periosea of the articulating bones
• The inner layer is the synovial membrane• Covers all internal joint surface s that are not
hyaline cartilage
• Synovial fluid• Synovial fluid is a thick, stringy fluid found
in the cavities of synovial joints.• synovial fluid reduces friction between the
and other tissues in joints to lubricate and cushion them during movement.
• Found within the articular cartilage
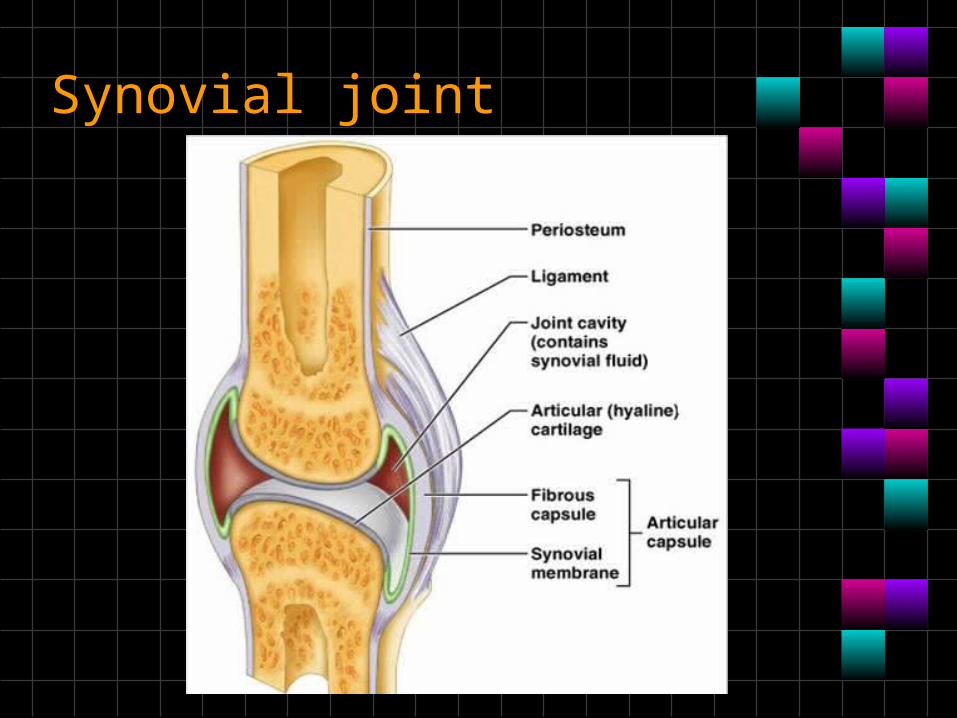
Synovial joint
Types of Synovial Joints (synovial fluid)*guy
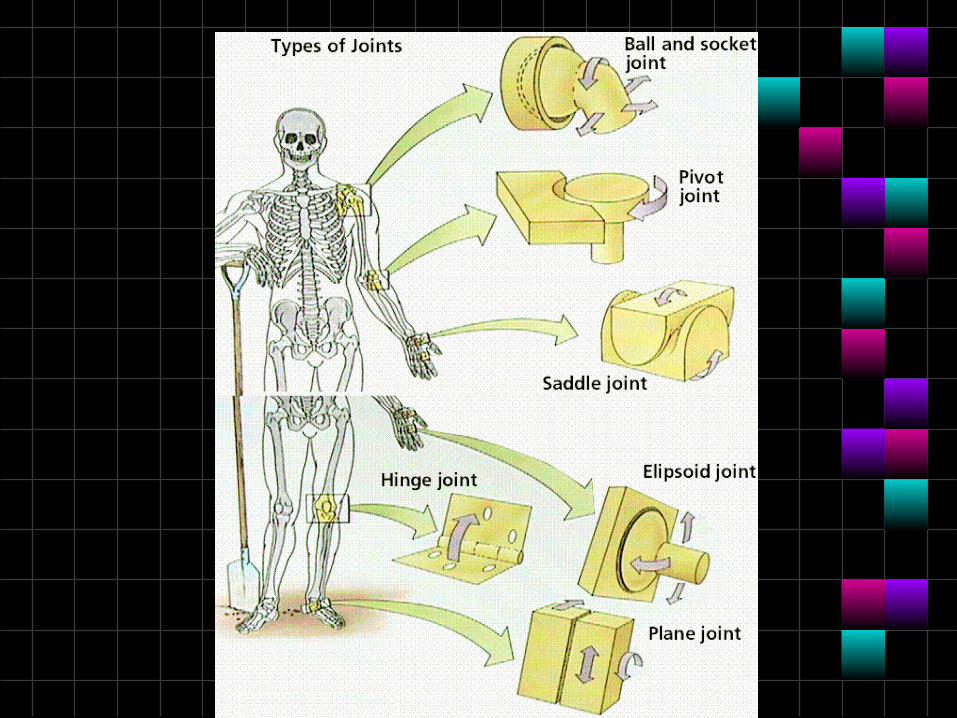
• Ball & Socket - allows for complete range of motion Example: shoulder, hip
• Pivot – one bone pivots in the arch of another Example: Axis/Atlas, and proximal radioulnar joint
• Saddle – two directional movement between thumb and trapezium carpel
Types of Synovial Joints
• Hinge – like door hinge – bending & extending Example: elbow, knee, finger joints
• Ellipsoid (Condyloid) – side to side and back & forth. Example – radius end into carpal bones
• Plane or Gliding – least moveable – side to side only Examples: intercarpal & intertarsal joints; between vertebrae
Types of cells constituting the bone
• Osteoblasts • bone forming cells synthesize and secrete
unmineralized ground substance and are found in areas of high metabolism within the bone
• do not have the ability to divide by mitosis • Osteocytes
• mature bone cells made from osteoblasts that have made bone tissue around themselves.
• maintain healthy bone tissue by secreting enzymes and controlling the bone mineral content;
• they also control the calcium release from the bone tissue to the blood.
• do not undergo mitosis
Types of cells constituting the bone• Osteoclasts –
• bone absorbing cell – • large cells that break down bone tissue• important to growth, healing, remodeling
• Bone lining cells • essentially inactive osteoblasts• Bone-lining cells- thought to regulate the
movement of calcium and phosphate into and out of the bone
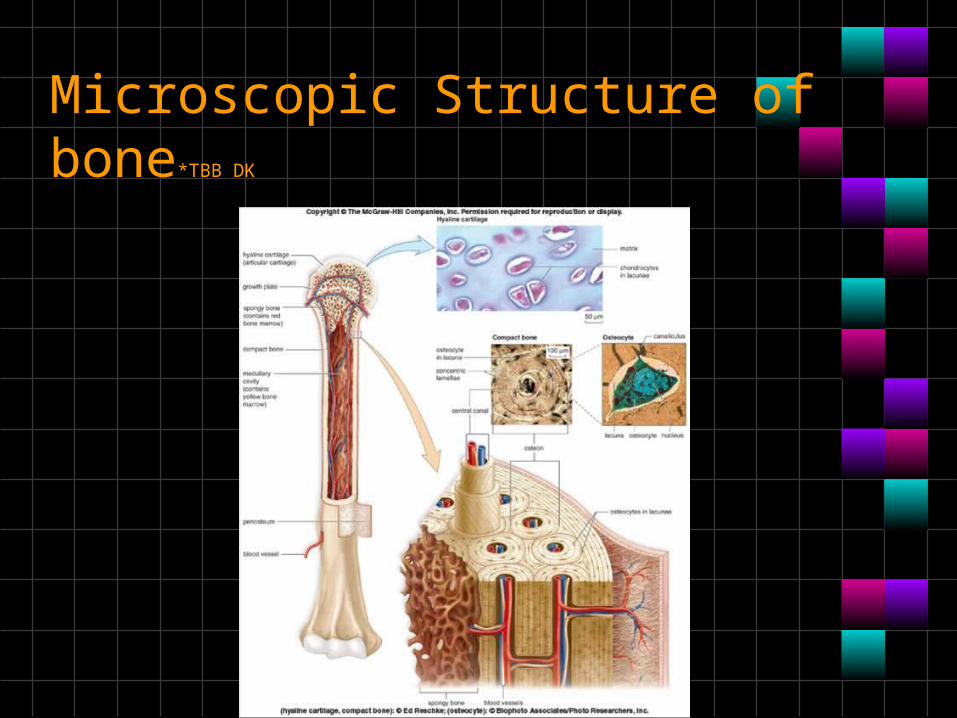
Microscopic Structure of bone*TBB DK
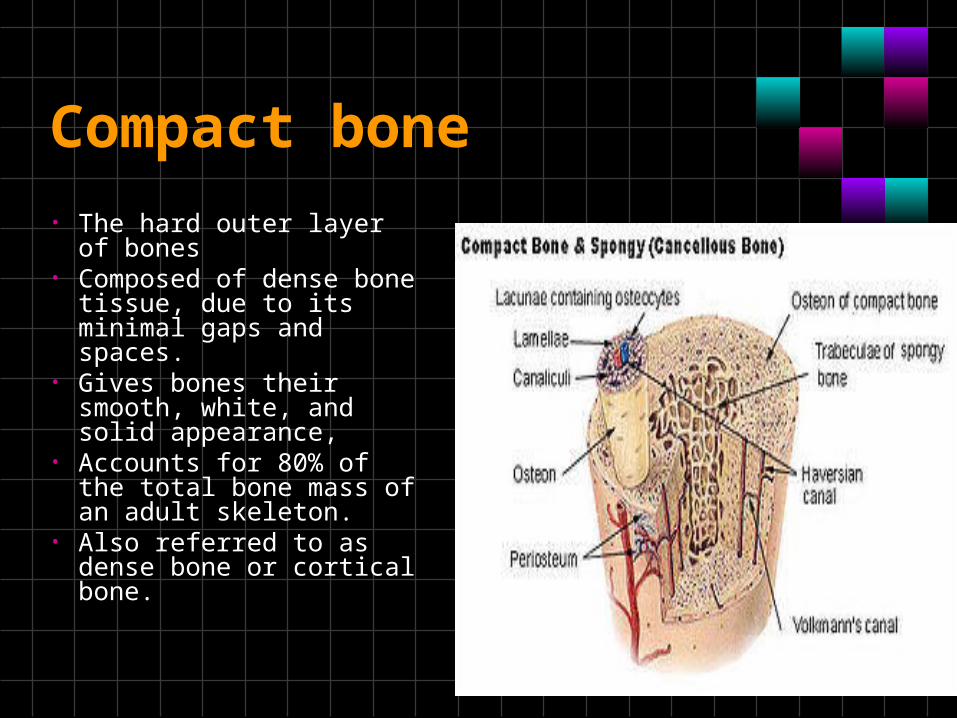
Compact bone
• The hard outer layer of bones
• Composed of dense bone tissue, due to itsminimal gaps and spaces.
• Gives bones their smooth, white, and solid appearance,
• Accounts for 80% of the total bone mass ofan adult skeleton.
• Also referred to as dense bone or cortical bone.
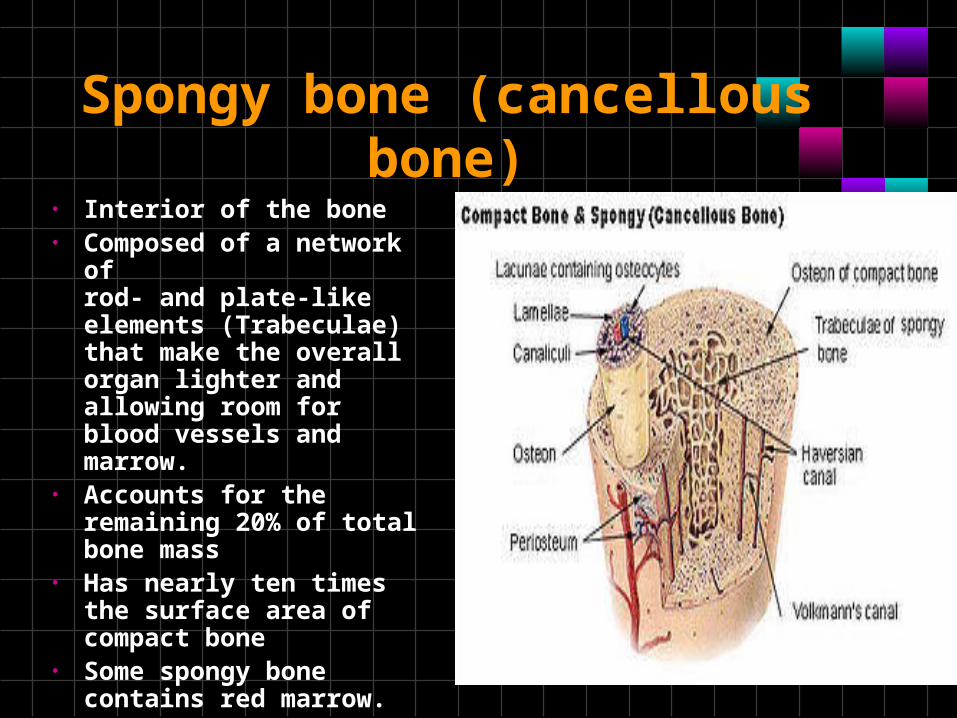
Spongy bone (cancellous bone)
• Interior of the bone• Composed of a network of
rod- and plate-like elements (Trabeculae) that make the overall organ lighter and allowing room for blood vessels and marrow.
• Accounts for the remaining 20% of total bone mass
• Has nearly ten times the surface area of compact bone
• Some spongy bone contains red marrow.
Red and Yellow Bone Marrow• The formation of blood cells, hematopoiesis,
takes place mainly in the red marrow of the bones.
• In infants, red marrow is found in the bone cavities. With age, it is largely replaced by yellow marrow for fat storage.
• In adults, red marrow is limited to the spongy bone in the skull, ribs, sternum, clavicles, vertebrae and pelvis
• Red marrow functions in the formation of red blood cells, white blood cells and blood platelets.
Cellular Structure of compact bone
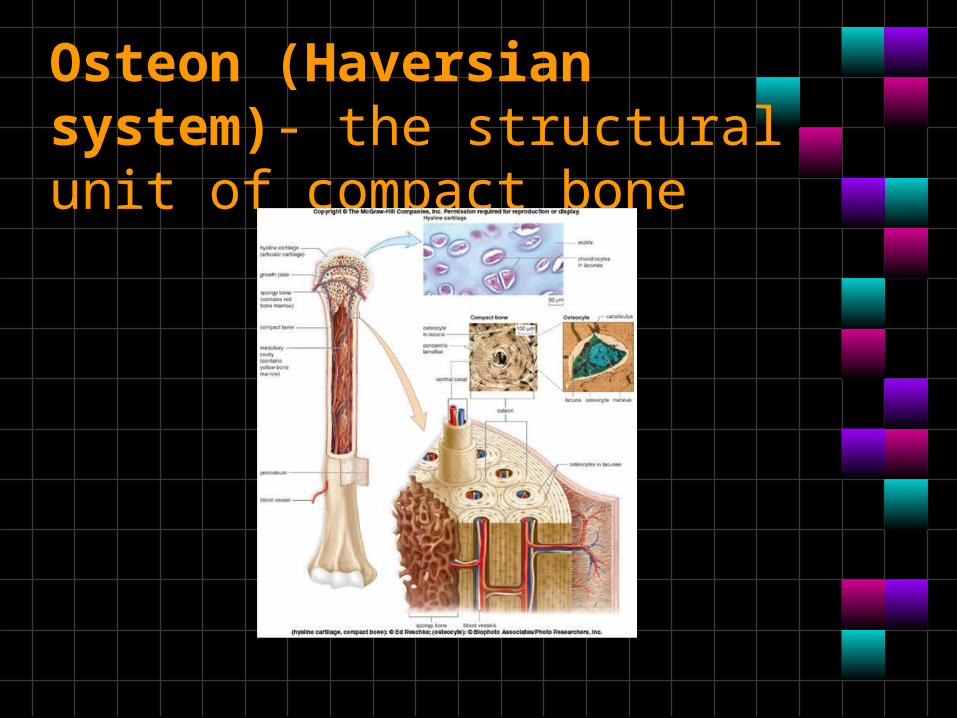
Osteon (Haversian system)- the structural unit of compact bone
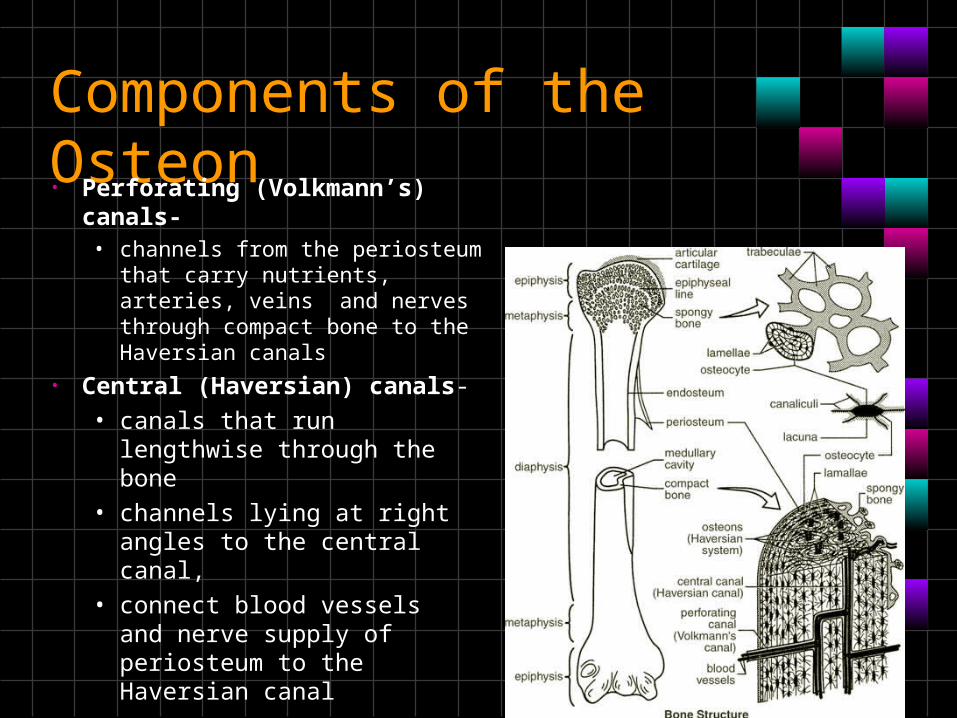
Components of the Osteon• Perforating (Volkmann’s)
canals- • channels from the periosteum
that carry nutrients, arteries, veins and nerves through compact bone to the Haversian canals
• Central (Haversian) canals-• canals that run lengthwise
through the bone• channels lying at right angles
to the central canal,• connect blood vessels and
nerve supply of periosteum to the Haversian canal
Components of the osteon
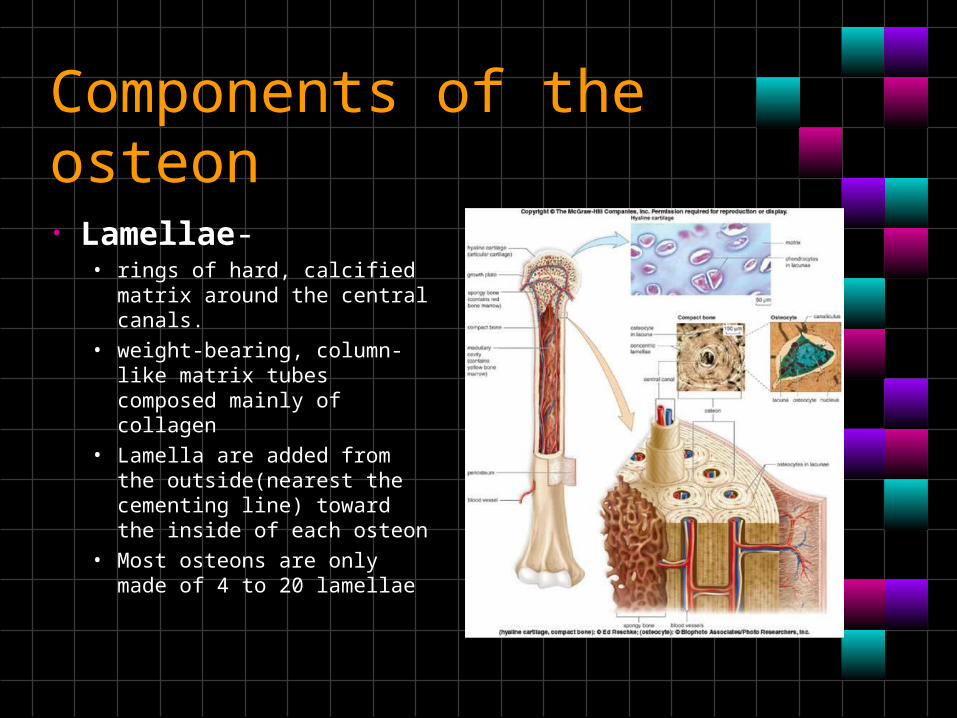
• Lamellae- • rings of hard, calcified
matrix around the central canals.
• weight-bearing, column-like matrix tubes composed mainly of collagen
• Lamella are added from the outside(nearest the cementing line) toward the inside of each osteon
• Most osteons are only made of 4 to 20 lamellae
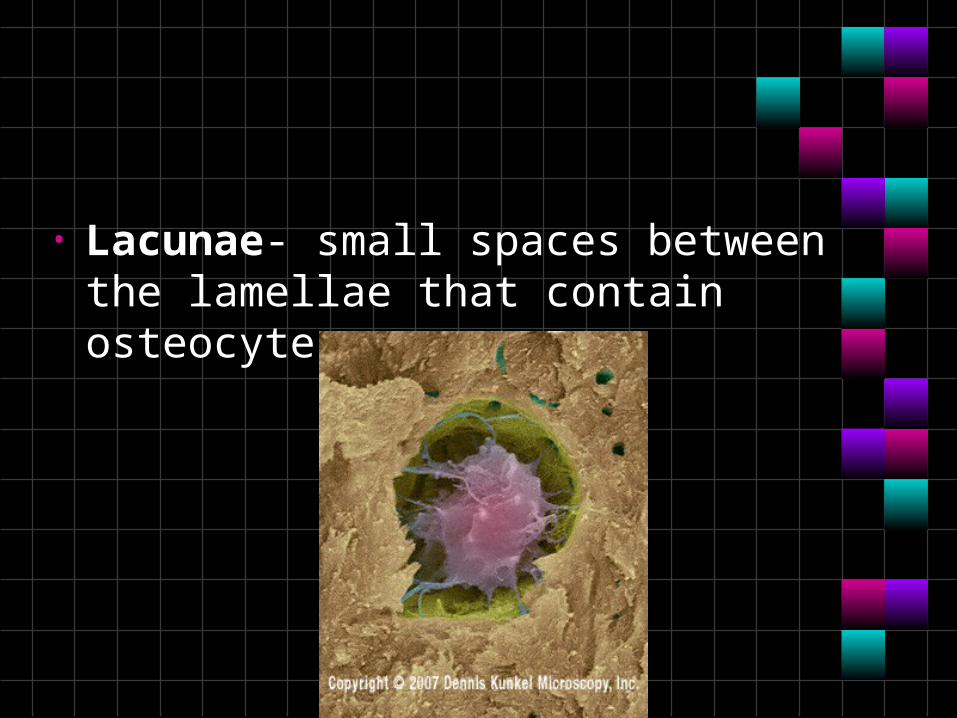
• Lacunae- small spaces between the lamellae that contain osteocytes
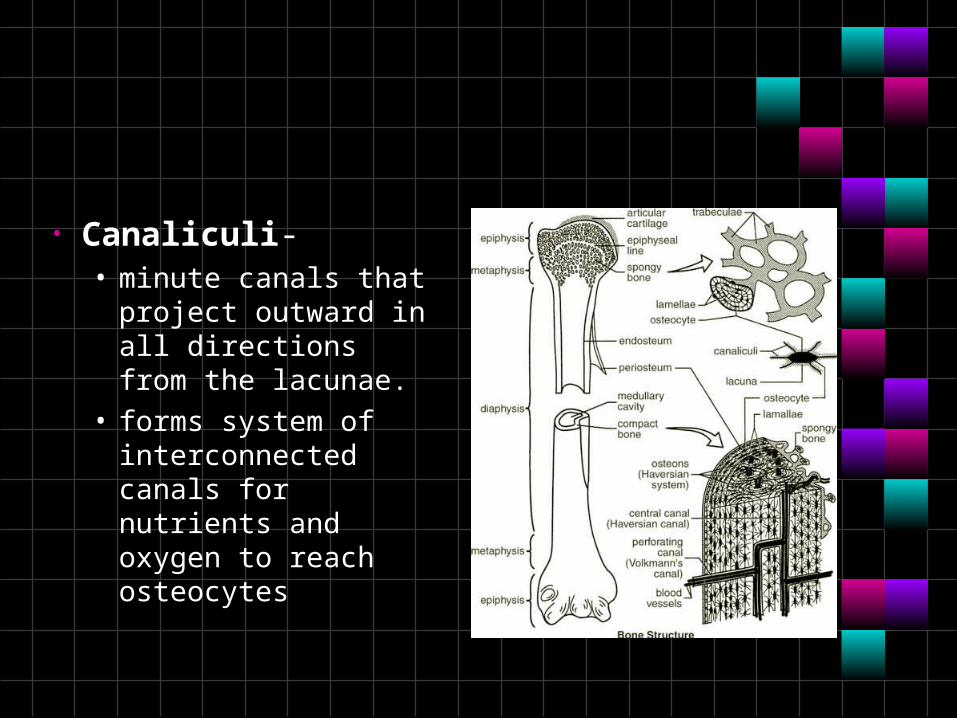
• Canaliculi- • minute canals that
project outward in all directions from the lacunae.
• forms system of interconnected canals for nutrients and oxygen to reach osteocytes
Bone lining
• Periosteum is a membrane that lines the outer surface of all bones except at the joints of long bones
• Endosteum is a thin layer of connective tissue which lines the surface of the bony tissue that forms the medullary cavity of long bones
Osteogenesis and ossification
• The process of bone tissue formation which leads to:• The formation of the bony skeleton
in embryos• Bone growth until early adulthood• Bone thickness, remodeling, and
repair
Formation of the Bony Skeleton
• The formation of bone during the fetal stage of development occurs by two processes: intramembranous ossification and endochondral ossification
• Begins at week 8 of embryo development
Intramembranous Ossification-initiation of bone development
• Fibrous connective tissue membranes are formed by mesenchymal cells • An ossification center appears in fibrous
connective tissue membrane • Bone matrix is secreted within the fibrous
membrane • Woven bone and periosteum form • Bone collar of compact bone forms, and red
marrow appears
Endochondral Ossification
• Begins in the second month of development
• occurs in long bones, such as limbs; • Uses hyaline cartilage "bones" as
models for bone construction• Requires breakdown of hyaline
cartilage prior to ossification
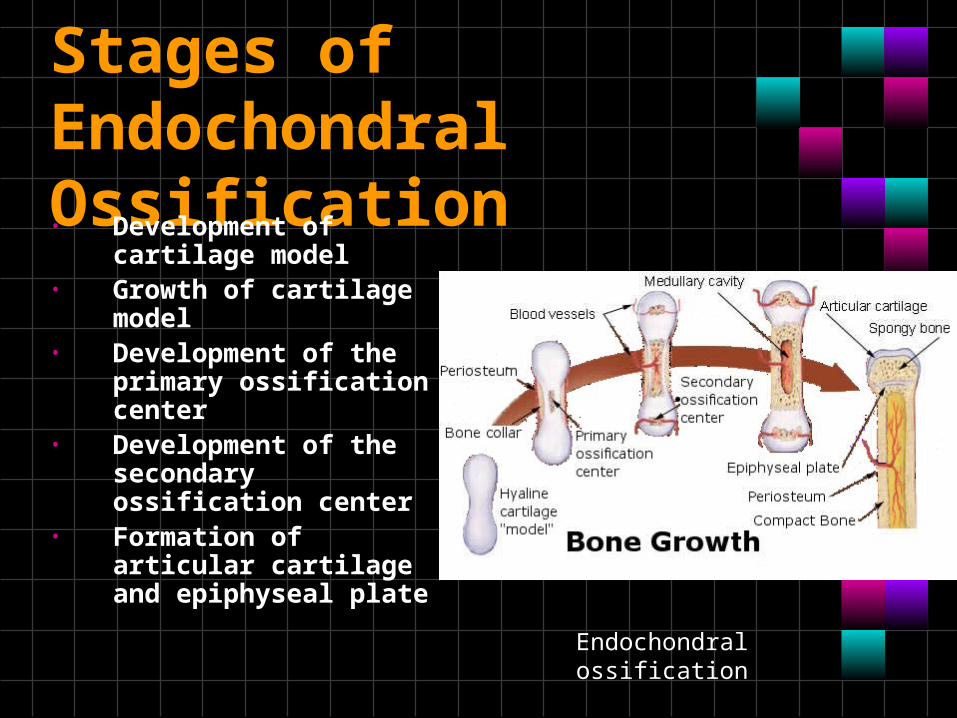
Stages of Endochondral Ossification• Development of
cartilage model • Growth of cartilage
model • Development of the
primary ossification center
• Development of the secondary ossification center
• Formation of articular cartilage and epiphyseal plate
Endochondral ossification
Postnatal Bone Growth
• Bone Growth in length*TBB DK
• Epiphyseal plate or cartilage growth plate• cartilage cells are produced by
mitosis on epiphyseal side of plate • cartilage cells are destroyed and
replaced by bone on diaphyseal side of plate
• Between ages 18 to 25, epiphyseal plates close.
• cartilage cells stop dividing and bone replaces the cartilage (epiphyseal line)
• Growth in length stops at age 25
Four zones of growth in epiphyseal plate *TBB DK
• Zone of resting cartilage• anchors growth plate to bone
• Zone of proliferating cartilage• rapid cell division (stacked coins)
• Zone of hypertrophic cartilage• cells enlarged & remain in columns
• Zone of calcified cartilage: • thin zone, • cells mostly dead since matrix calcified• osteoclasts removing matrix;• osteoblasts & capillaries move in to create
bone over calcified cartilage
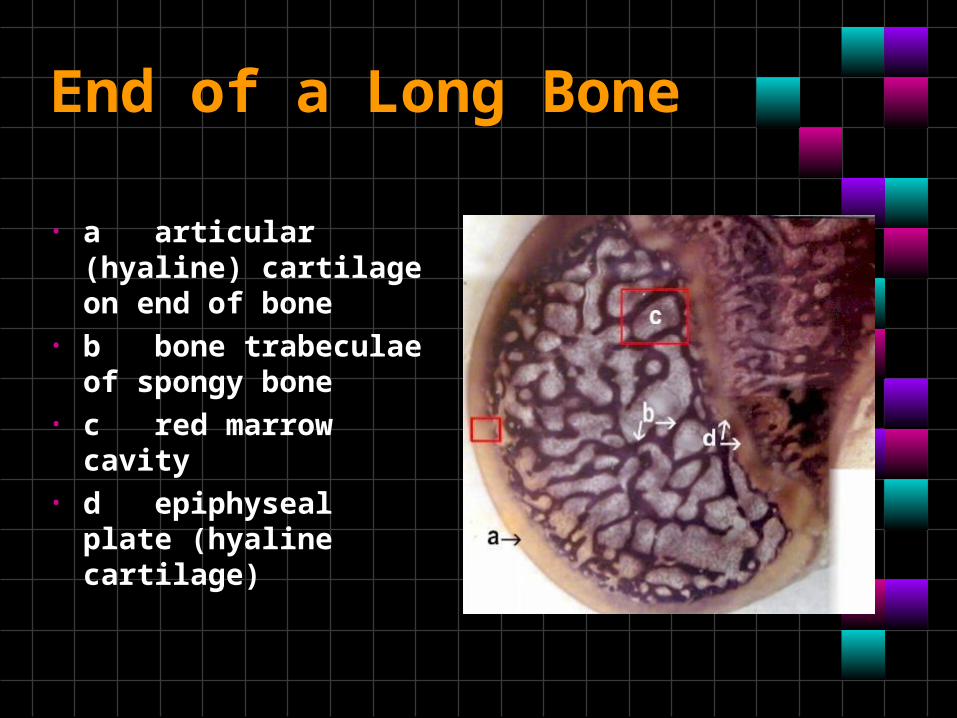
End of a Long Bone
• a articular (hyaline) cartilage on end of bone
• b bone trabeculae of spongy bone
• c red marrow cavity • d epiphyseal plate
(hyaline cartilage)
Long Bone Growth*TBB DK
• Interstitial growth is growth in the length of bone
• Appositional growth: increase in bone width
• Remodeling - bone is reabsorbed and added
Hormonal Regulation of Bone Growth During Youth
• During infancy and childhood, epiphyseal plate activity is stimulated by growth hormone
• During puberty, testosterone and estrogens:• Initially promote adolescent growth spurts• Causes masculinization and feminization of specific
parts of the skeleton • Later induce epiphyseal plate closure, ending
longitudinal bone growth
Hormonal Control of Remodeling
• Activity of parathyroid hormone and calcitonin is the mechanism to maintain blood calcium homeostasis, and balances
Bone Fractures
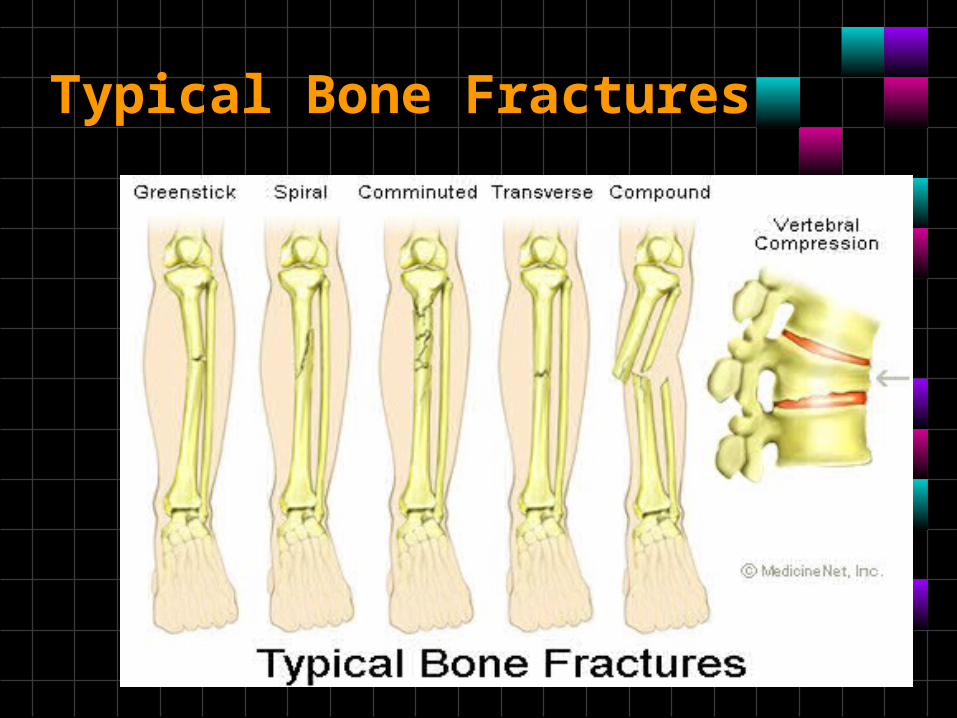
Typical Bone Fractures
• Pain when fractures occur, the pain is carried to the brain by nerves running through the periosteum
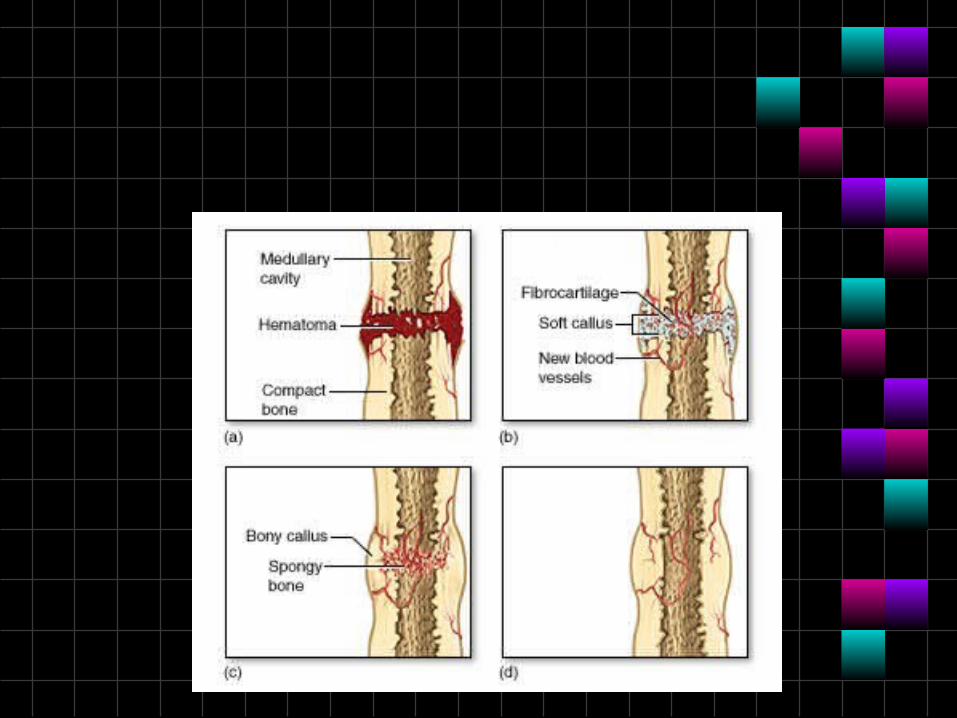
Fracture repair
1. Hematoma formation• Torn blood vessels hemorrhage• A mass of clotted blood
(hematoma) forms at the fracture site
• Site becomes swollen, painful, and inflamed
2. Fibrocartilaginous callus
• soft callus forms • Capillaries grow into the tissue and phagocytic
cells begin cleaning debris • Osteoblasts & fibroblasts migrate to fracture &
begin reconstructing bone • Fibroblasts secrete collagen fibers that
connect broken bone ends • Osteoblasts begin forming spongy bone • Osteoblasts furthest from capillaries secrete a
matrix externally bulging cartilaginous matrix that later calcifies
3. Bony callus formation
• New bone trabeculae appear in the fibrocartilaginous callus
• Fibrocartilaginous callus converts into a bony (hard) callus
• Bone callus begins 3-4 weeks after injury, and continues until firm union is formed 2-3 months later
• Bone remodeling • Excess material on the bone shaft
exterior and in the medullary canal is removed
• Compact bone is laid down to reconstruct shaft walls
• May take several months
Salter-Harris fracture classification system
• Fractures through a growth plate• Unique to pediatric patients
Type I
• A type 1 fracture is a transverse fracture through the hypertrophic zone of the physis. In this injury, the width of the physis is increased. The growing zone of the physis usually is not injured, and growth disturbance is uncommon.
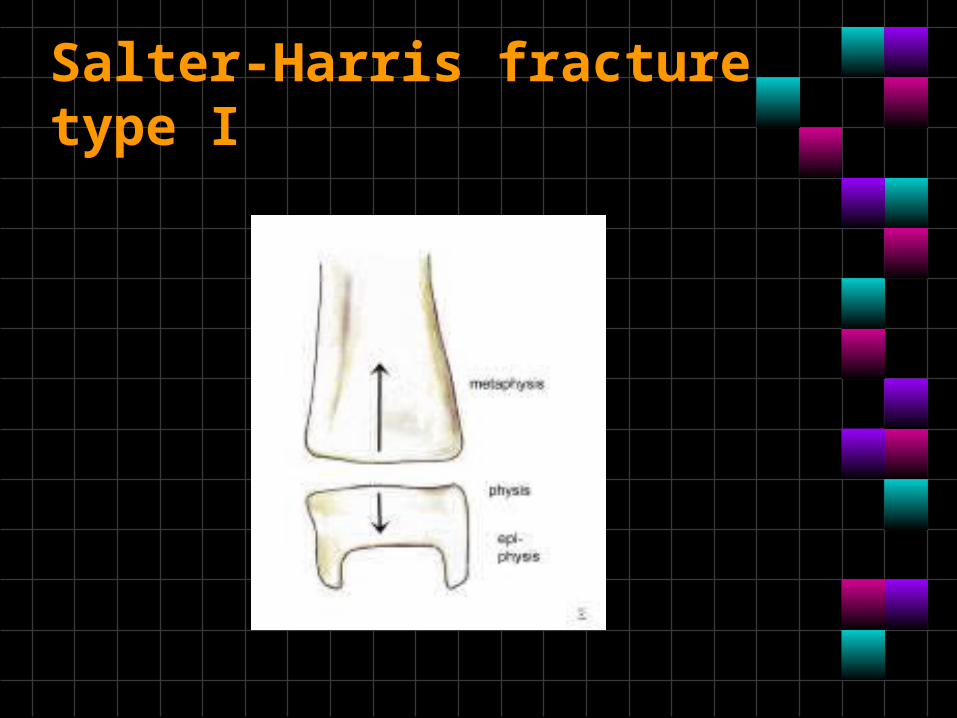
Salter-Harris fracture type I
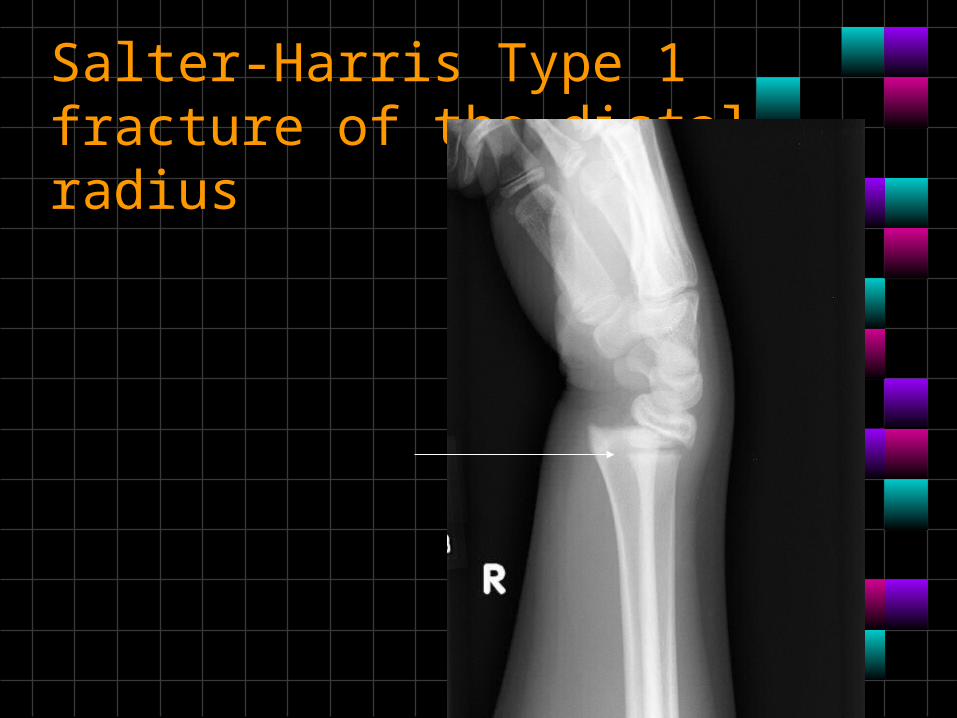
Salter-Harris Type 1 fracture of the distal radius
Type II
• A type II fracture is a fracture through the physis and the metaphysis, but the epiphysis is not involved in the injury.
• These fractures may cause minimal shortening; however, the injuries rarely result in functional limitations.
• Type II is the most common type of Salter-Harris fracture.
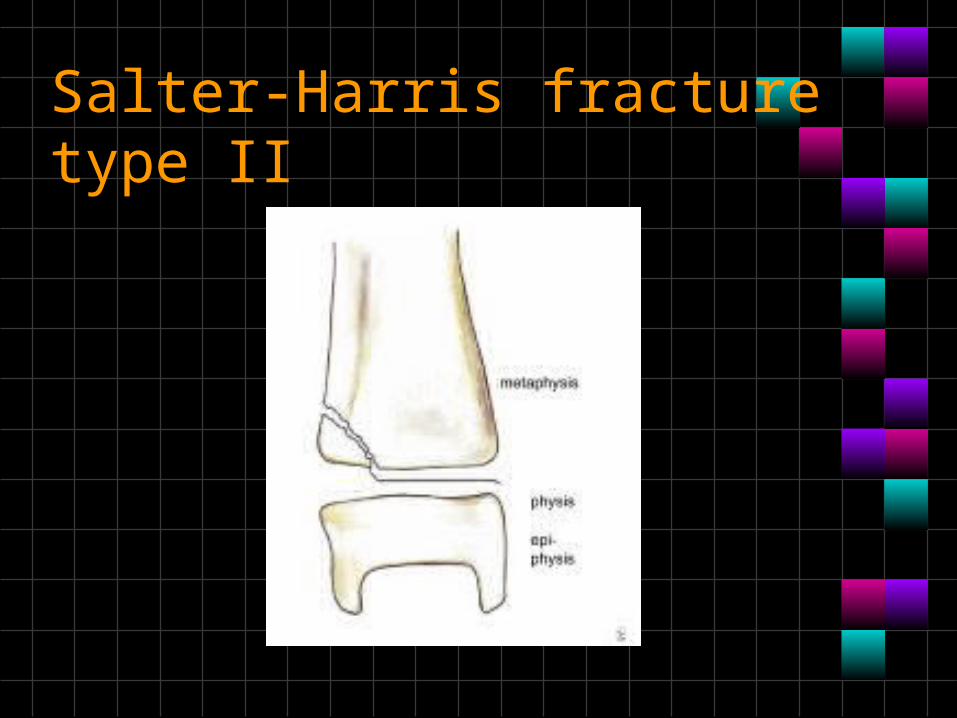
Salter-Harris fracture type II
Type III
• A type III fracture is a fracture through the physis and the epiphysis. This fracture passes through the hypertrophic layer of the physis and extends to split the epiphysis, inevitably damaging the reproductive layer of the physis.
• This type of fracture is prone to chronic disability because by crossing the physis, the fracture extends into the articular surface of the bone.
• The treatment for this fracture is often surgical
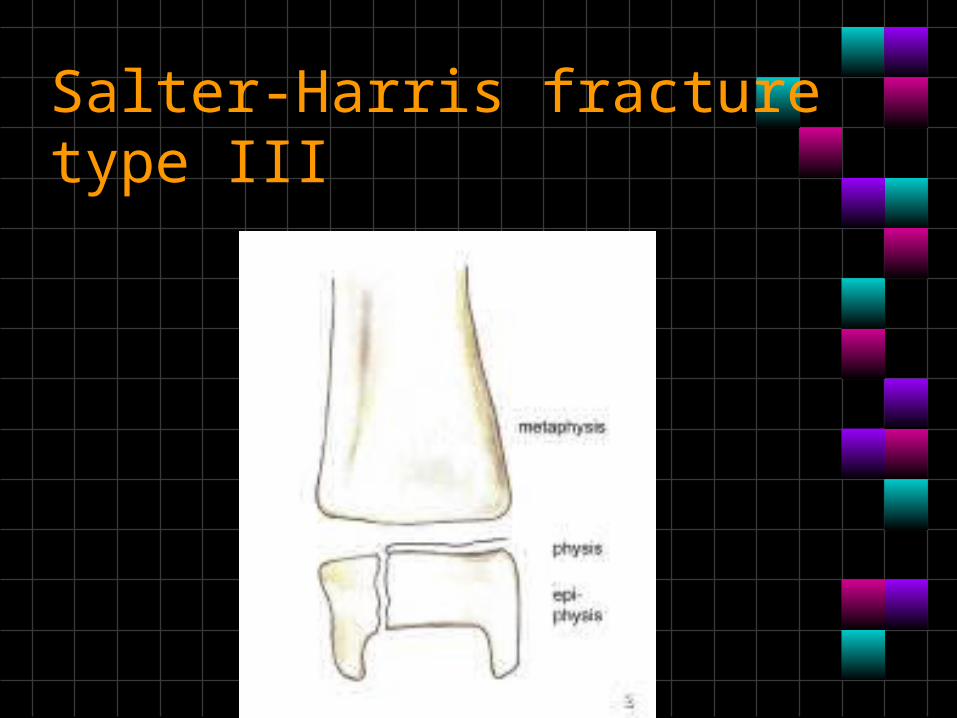
Salter-Harris fracture type III
Type IV
• A Type IV fracture involves all 3 elements of the bone: The fracture passes through the epiphysis, physis, and metaphysis.
• Similar to a type III fracture, a type IV fracture is an intra-articular fracture; thus, it can result in chronic disability.
• By interfering with the growing layer of cartilage cells, these fractures can cause premature focal fusion of the involved bone.
• These injuries can cause deformity of the joint.

Salter-Harris fracture type IV
Type V
• A type V injury is a compression or crush injury of the epiphyseal plate with no associated epiphyseal or metaphyseal fracture.
• This fracture is associated with growth disturbances at the physis. These injuries have a poor functional prognosis.
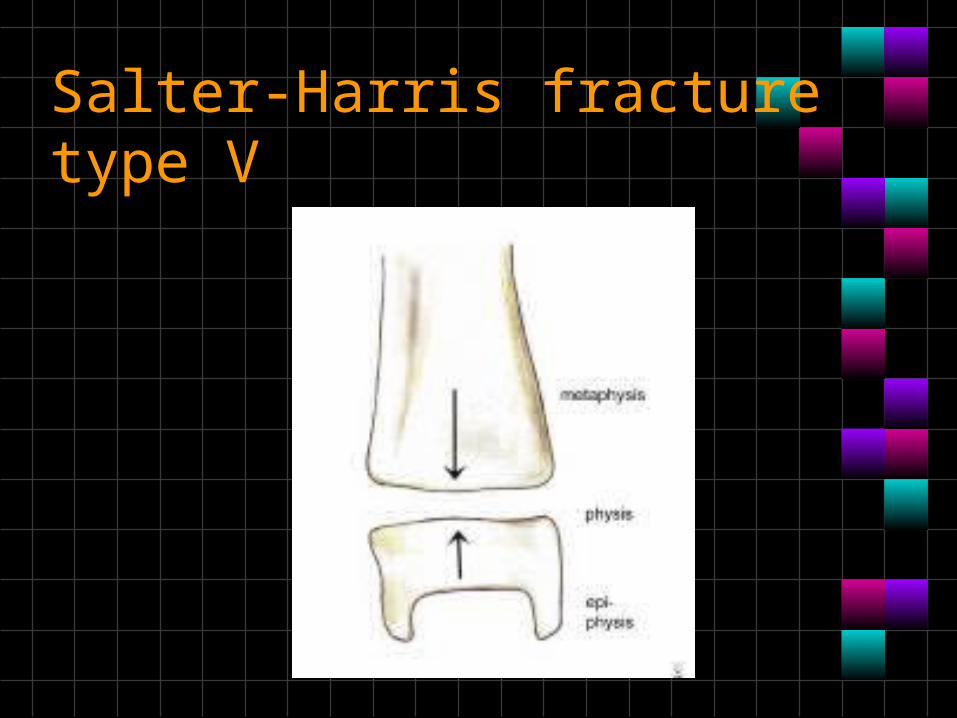
Salter-Harris fracture type V
• The classification can be remembered by a modified spelling of the word 'Salter' as follows:
• S = I = Separation • A = II = Above • L = III = Lower • T = IV = Through • R = V = Reduction
Cartilage – Characteristics and Types
• Mostly water; no blood vessels or nerve
• Tough, resilient• New cartilage forms from chondroblasts• Heals poorly
Hyaline Cartilages:
• fine collagen fiber matrix- most abundant type- found in articular (movable joint)cartilages, costal cartilages (connect ribs tosternum), respiratory cartilages (in larynx & upper respiratorypassageways) & nasal cartilages
• Elastic Cartilages:
• similar to hyaline cartilage, more elastic fibers (very flexible) – found in external ear& epiglottis (larynx covering
Fibrocartilage:
• rows of chondrocytes with thick collagen fibers; highly compressible with great tensile strength
• found in meniscus of the knee, intervertebral discs & pubic symphysis
Bone Markings are bulges, depressions, and holes
that serve as:
• Joint surfaces • Fossa - shallow, basinlike depression • condyle- rounded articular projection • Epicondyle - raised area above a condyle • Head -bony expansion on a narrow neck
Bone Markings are bulges, depressions, and holes that serve as:• Muscle & ligament attachment
• Trochanter- large, blunt, irregular surface • Tuberodsity- rounded projection • Process- any bony prominence • Crest- narrow, prominent ridge of bone • Line - narrow ridge of bone • Fovea - small pit like indent • Tubercle - small rounded projection • Ramus - armlike bar of bone • Spine - sharp, slender projection
Bone Markings are bulges, depressions, and holes that serve as:• Passageways for vessels, etc.
• Foreamen- round or oval opening through a bone
• Fissure - narrow, slit like opening • Meatus - canal-like passageway
• Space within a bone -sinus
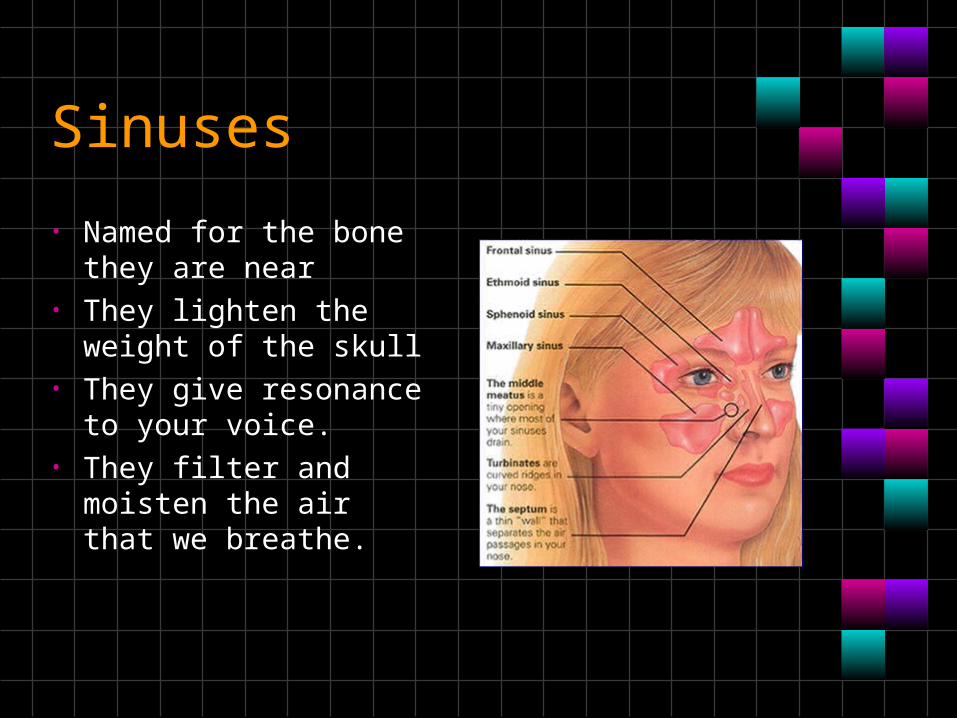
Sinuses
• Named for the bone they are near
• They lighten the weight of the skull
• They give resonance to your voice.
• They filter and moisten the air that we breathe.
Skull
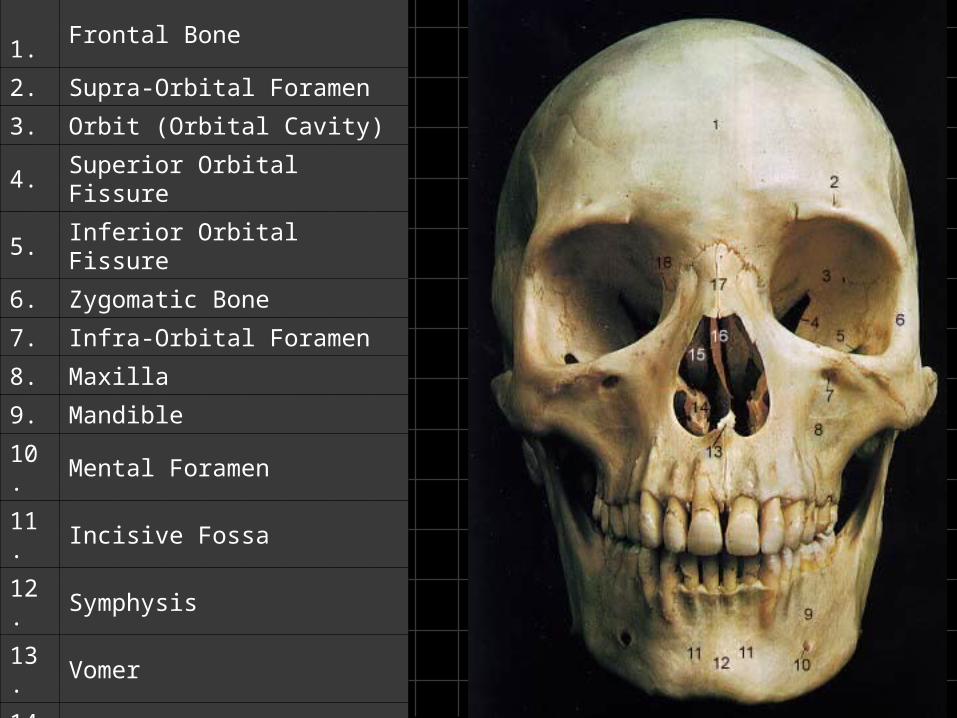
Anterior View
1.Frontal Bone
2. Supra-Orbital Foramen
3. Orbit (Orbital Cavity)
4. Superior Orbital Fissure
5. Inferior Orbital Fissure
6. Zygomatic Bone
7. Infra-Orbital Foramen
8. Maxilla
9. Mandible
10. Mental Foramen
11. Incisive Fossa
12. Symphysis
13. Vomer
14. Inferior Nasal Concha
15. Middle Nasal Concha
16. Perpendicular Plate of Ethmoid
17. Nasal Bone
18. Lacrimal
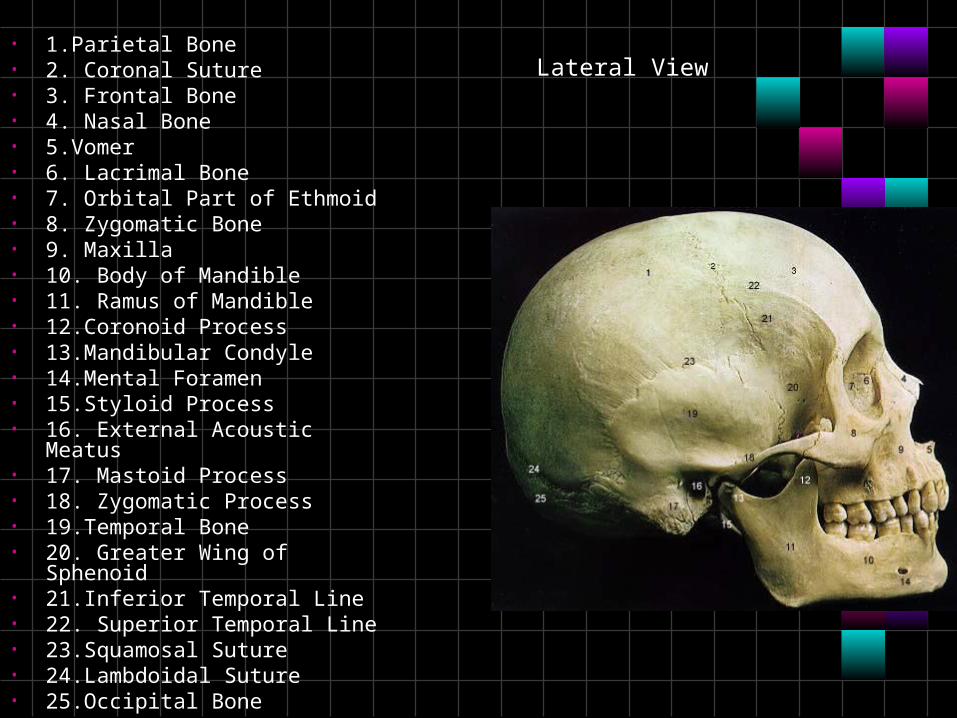
• 1.Parietal Bone• 2. Coronal Suture• 3. Frontal Bone• 4. Nasal Bone• 5.Vomer• 6. Lacrimal Bone• 7. Orbital Part of Ethmoid• 8. Zygomatic Bone• 9. Maxilla• 10. Body of Mandible• 11. Ramus of Mandible• 12.Coronoid Process• 13.Mandibular Condyle• 14.Mental Foramen• 15.Styloid Process• 16. External Acoustic Meatus• 17. Mastoid Process• 18. Zygomatic Process• 19.Temporal Bone• 20. Greater Wing of Sphenoid• 21.Inferior Temporal Line• 22. Superior Temporal Line• 23.Squamosal Suture• 24.Lambdoidal Suture• 25.Occipital Bone
Lateral View
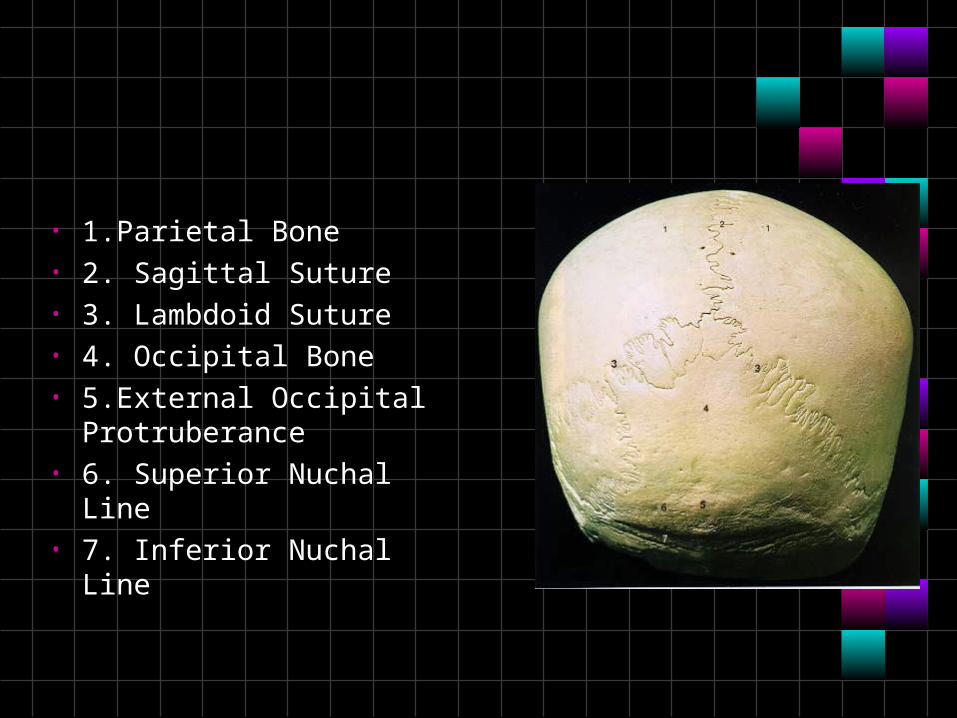
• 1.Parietal Bone• 2. Sagittal Suture• 3. Lambdoid Suture• 4. Occipital Bone• 5.External Occipital
Protruberance• 6. Superior Nuchal Line• 7. Inferior Nuchal Line
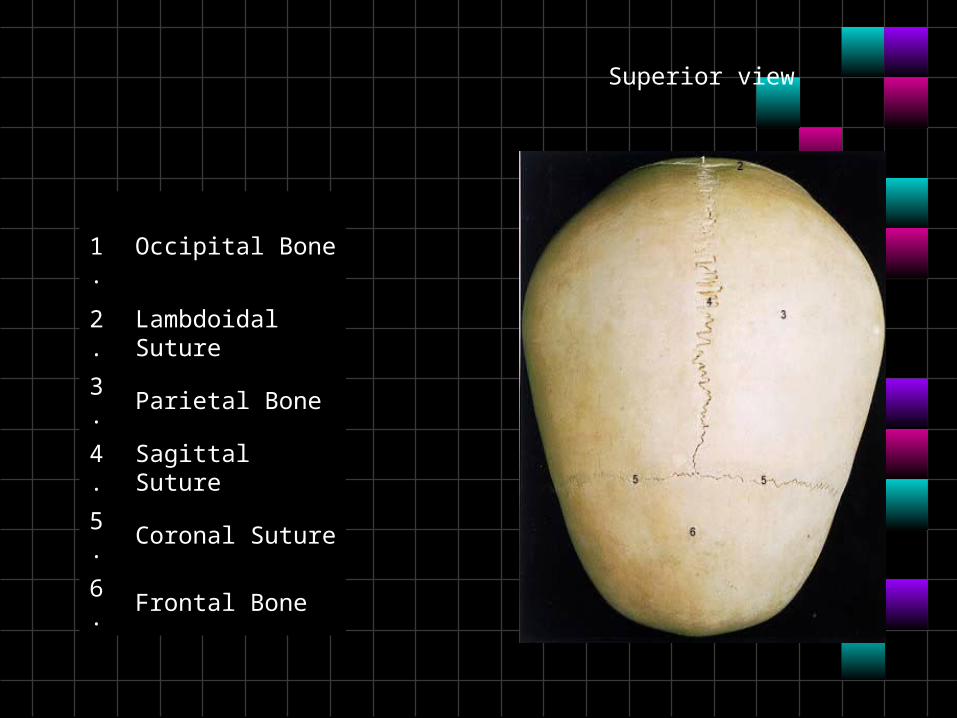
1.Occipital Bone
2. Lambdoidal Suture
3. Parietal Bone
4. Sagittal Suture
5. Coronal Suture
6. Frontal Bone
Superior view
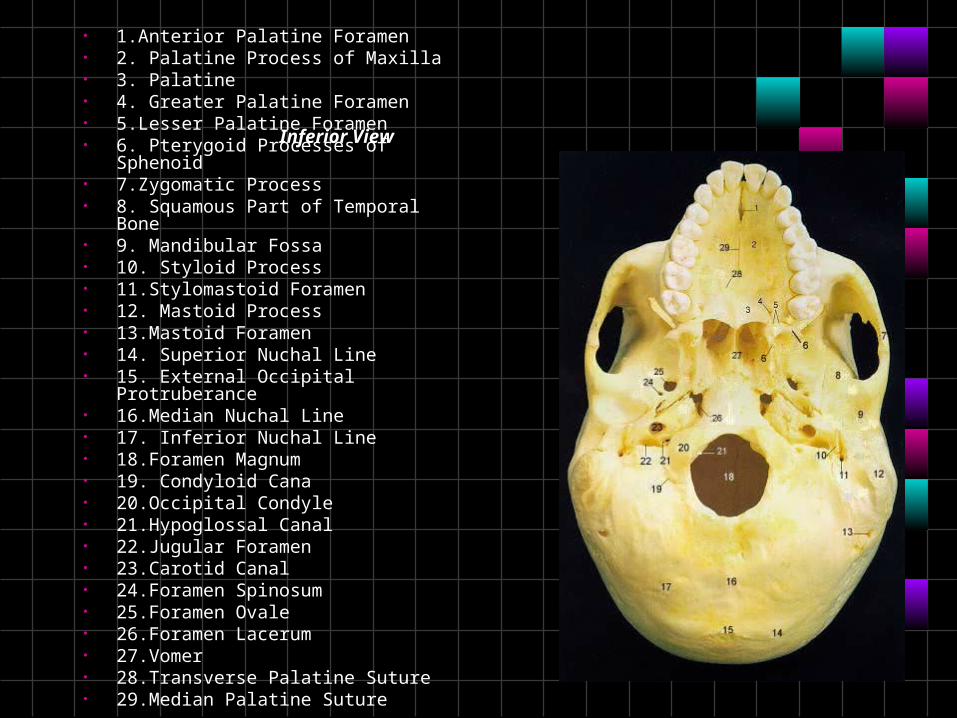
Inferior View
• 1.Anterior Palatine Foramen• 2. Palatine Process of Maxilla• 3. Palatine• 4. Greater Palatine Foramen• 5.Lesser Palatine Foramen• 6. Pterygoid Processes of Sphenoid• 7.Zygomatic Process• 8. Squamous Part of Temporal Bone• 9. Mandibular Fossa• 10. Styloid Process• 11.Stylomastoid Foramen• 12. Mastoid Process• 13.Mastoid Foramen• 14. Superior Nuchal Line• 15. External Occipital Protruberance• 16.Median Nuchal Line• 17. Inferior Nuchal Line• 18.Foramen Magnum• 19. Condyloid Cana• 20.Occipital Condyle• 21.Hypoglossal Canal• 22.Jugular Foramen• 23.Carotid Canal• 24.Foramen Spinosum• 25.Foramen Ovale• 26.Foramen Lacerum• 27.Vomer• 28.Transverse Palatine Suture• 29.Median Palatine Suture
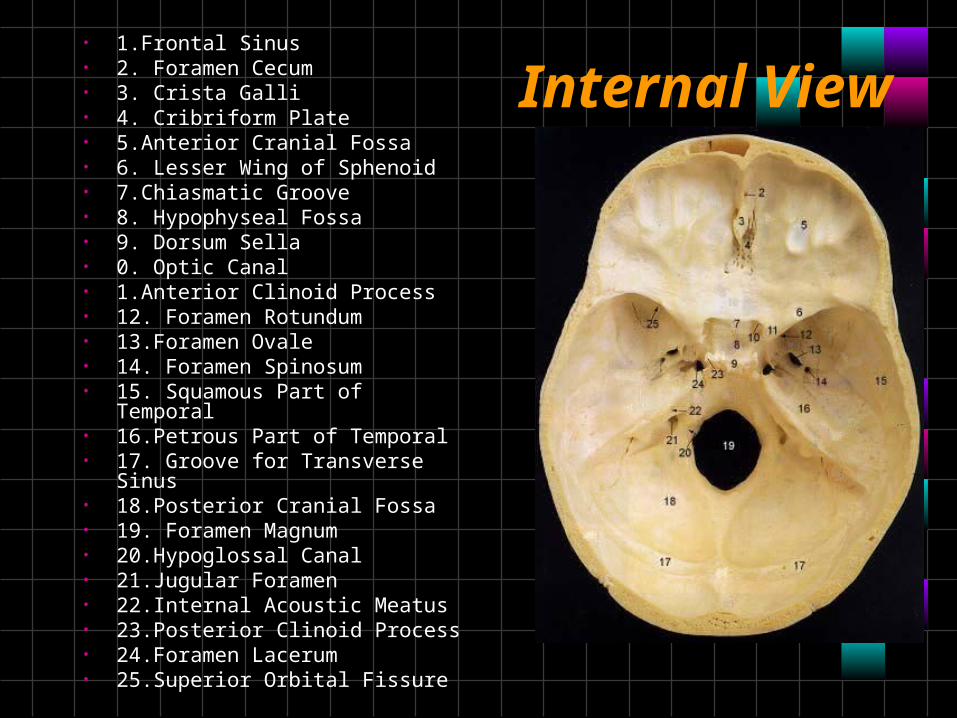
Internal View• 1.Frontal Sinus• 2. Foramen Cecum• 3. Crista Galli• 4. Cribriform Plate• 5.Anterior Cranial Fossa• 6. Lesser Wing of Sphenoid• 7.Chiasmatic Groove• 8. Hypophyseal Fossa• 9. Dorsum Sella• 0. Optic Canal• 1.Anterior Clinoid Process• 12. Foramen Rotundum• 13.Foramen Ovale• 14. Foramen Spinosum• 15. Squamous Part of Temporal• 16.Petrous Part of Temporal• 17. Groove for Transverse Sinus• 18.Posterior Cranial Fossa• 19. Foramen Magnum• 20.Hypoglossal Canal• 21.Jugular Foramen• 22.Internal Acoustic Meatus• 23.Posterior Clinoid Process• 24.Foramen Lacerum• 25.Superior Orbital Fissure
Nationals-foramina of the skull
• Table
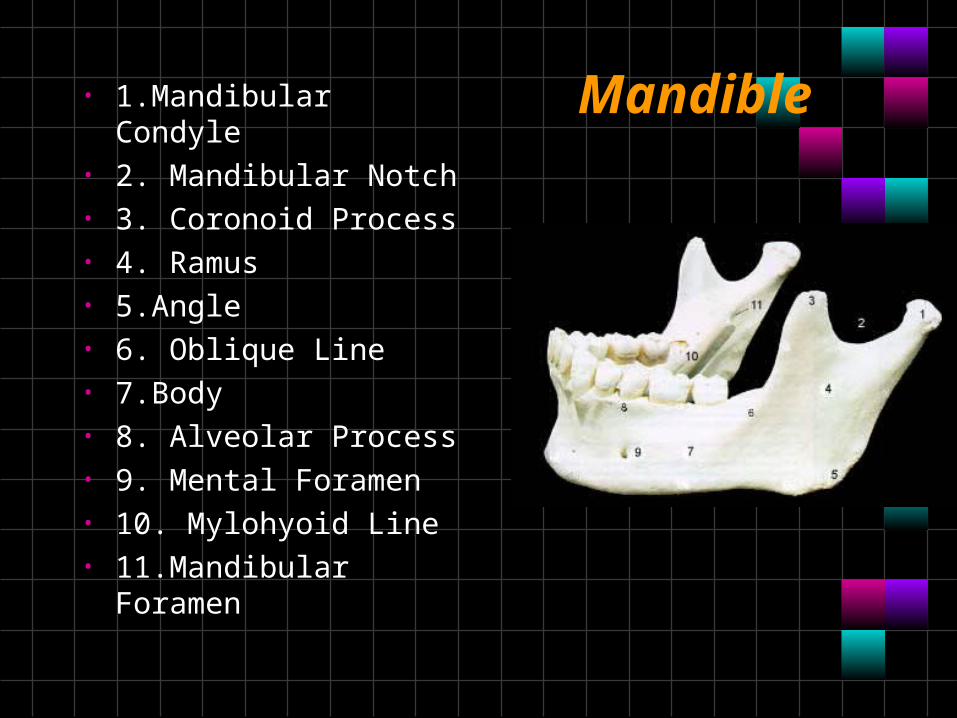
Mandible • 1.Mandibular Condyle• 2. Mandibular Notch• 3. Coronoid Process• 4. Ramus• 5.Angle• 6. Oblique Line• 7.Body• 8. Alveolar Process• 9. Mental Foramen• 10. Mylohyoid Line• 11.Mandibular Foramen
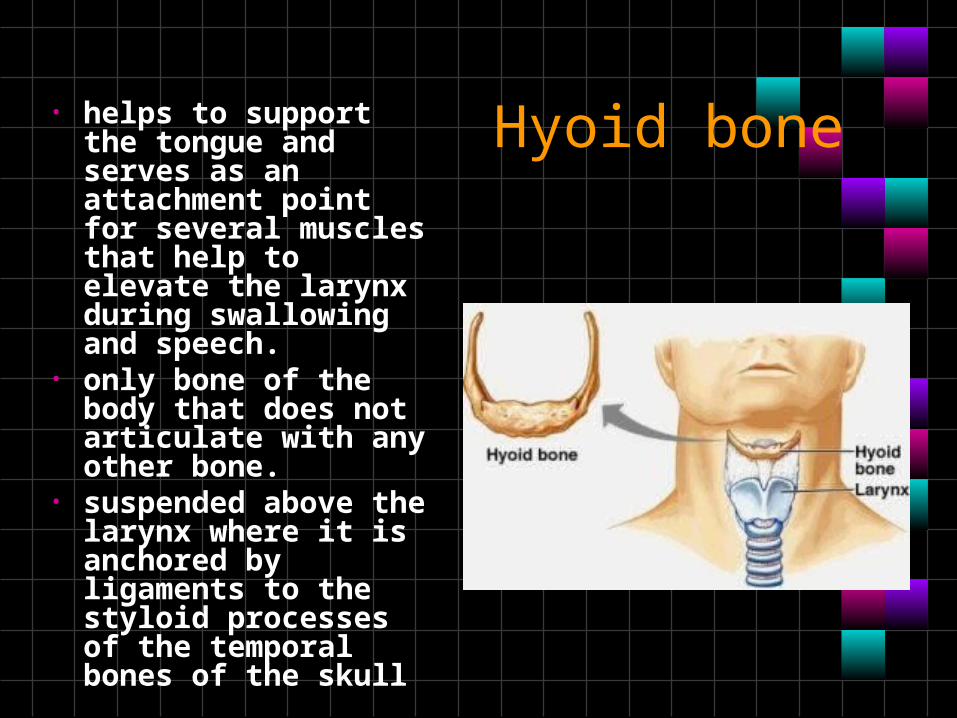
Hyoid bone• helps to support the tongue and serves as an attachment point for several muscles that help to elevate the larynx during swallowing and speech.
• only bone of the body that does not articulate with any other bone.
• suspended above the larynx where it is anchored by ligaments to the styloid processes of the temporal bones of the skull
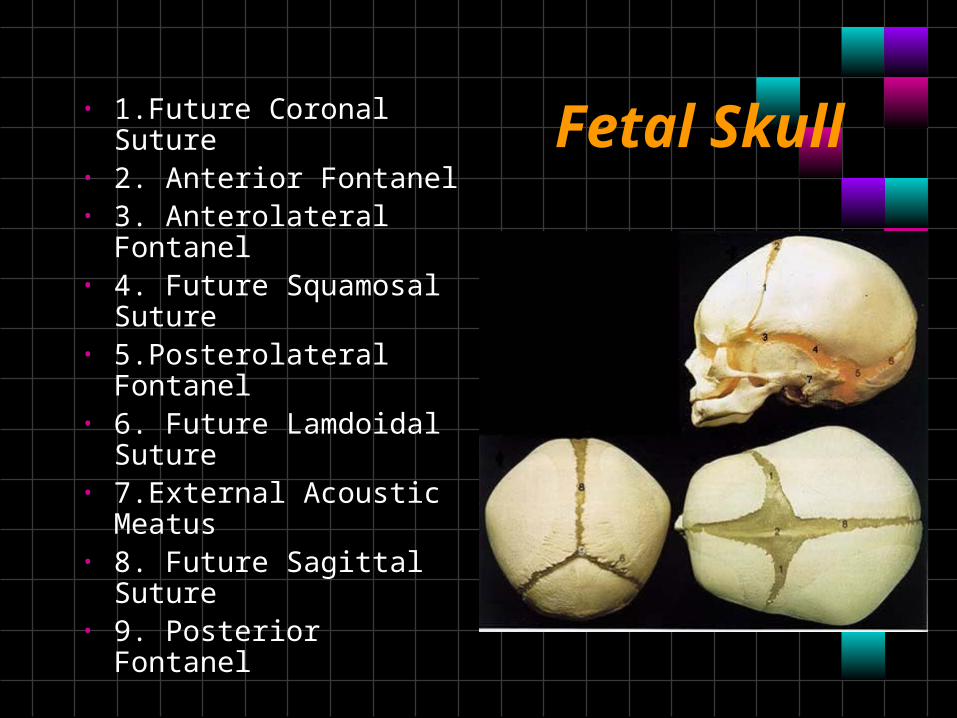
Fetal Skull• 1.Future Coronal Suture• 2. Anterior Fontanel• 3. Anterolateral
Fontanel• 4. Future Squamosal
Suture• 5.Posterolateral
Fontanel• 6. Future Lamdoidal
Suture• 7.External Acoustic
Meatus• 8. Future Sagittal
Suture• 9. Posterior Fontanel
Vertebral column
Atlas (C1)
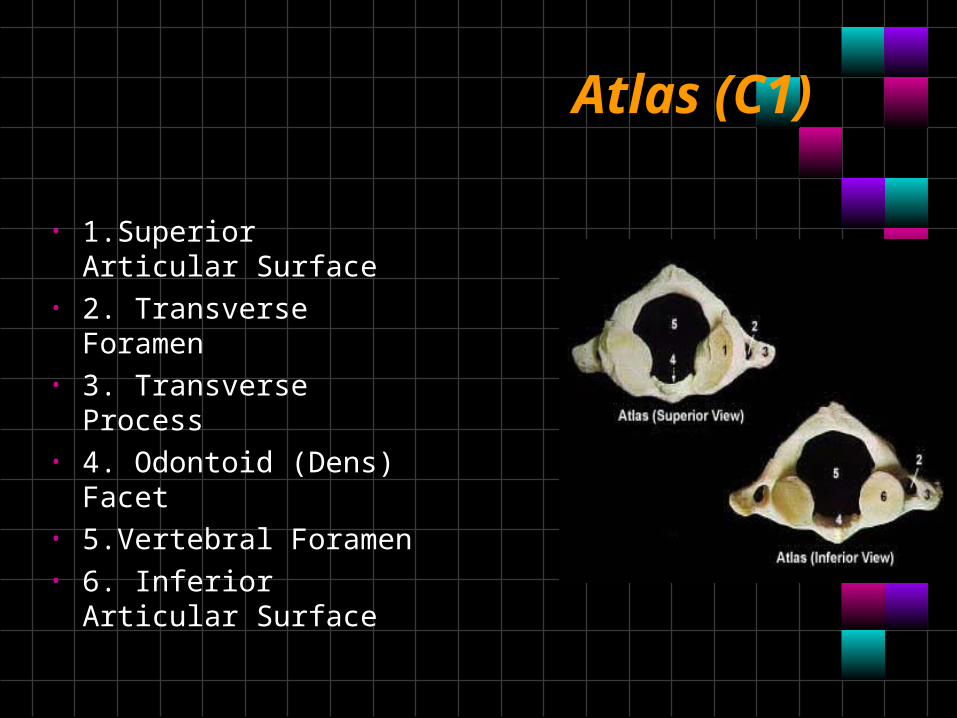
• 1.Superior Articular Surface
• 2. Transverse Foramen• 3. Transverse Process• 4. Odontoid (Dens)
Facet• 5.Vertebral Foramen• 6. Inferior Articular
Surface
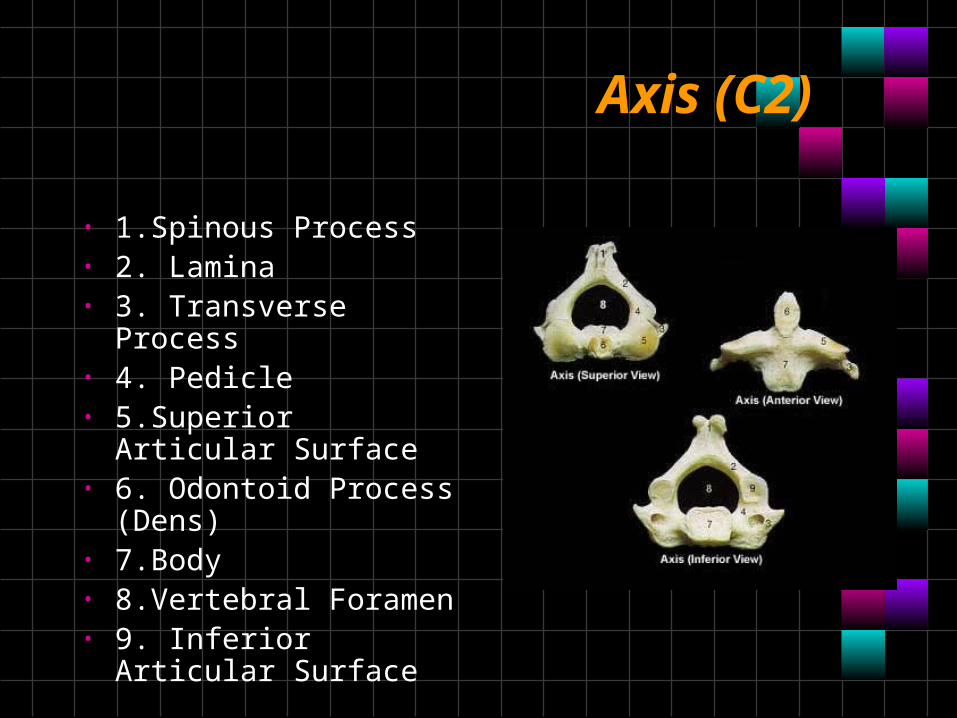
Axis (C2)
• 1.Spinous Process• 2. Lamina• 3. Transverse Process• 4. Pedicle• 5.Superior Articular
Surface• 6. Odontoid Process
(Dens)• 7.Body• 8.Vertebral Foramen• 9. Inferior Articular
Surface
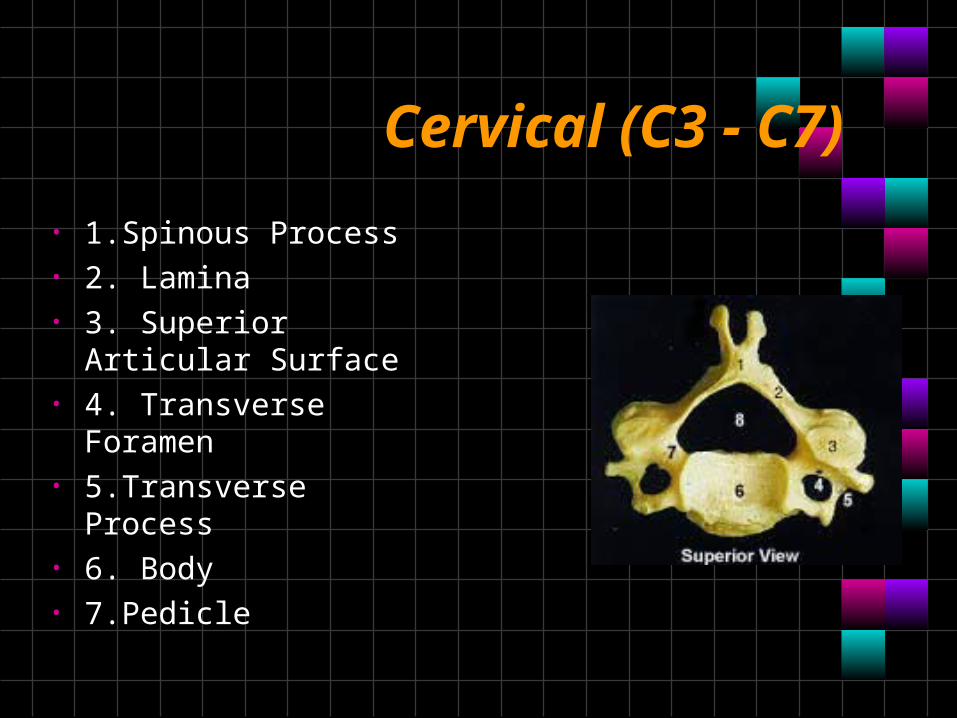
Cervical (C3 - C7)
• 1.Spinous Process• 2. Lamina• 3. Superior Articular
Surface• 4. Transverse Foramen• 5.Transverse Process• 6. Body• 7.Pedicle
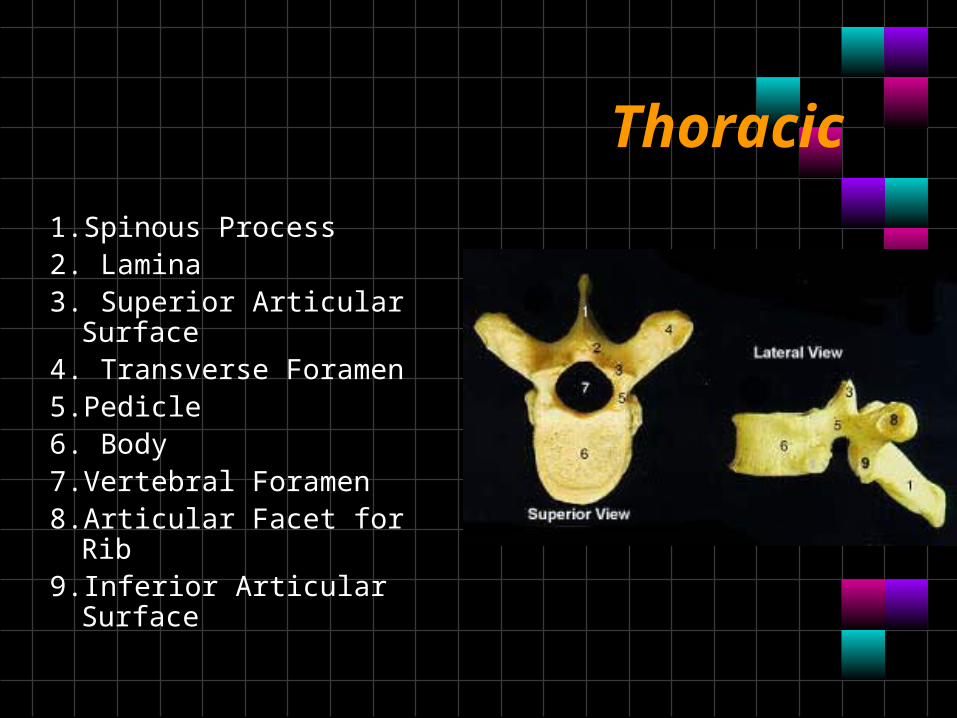
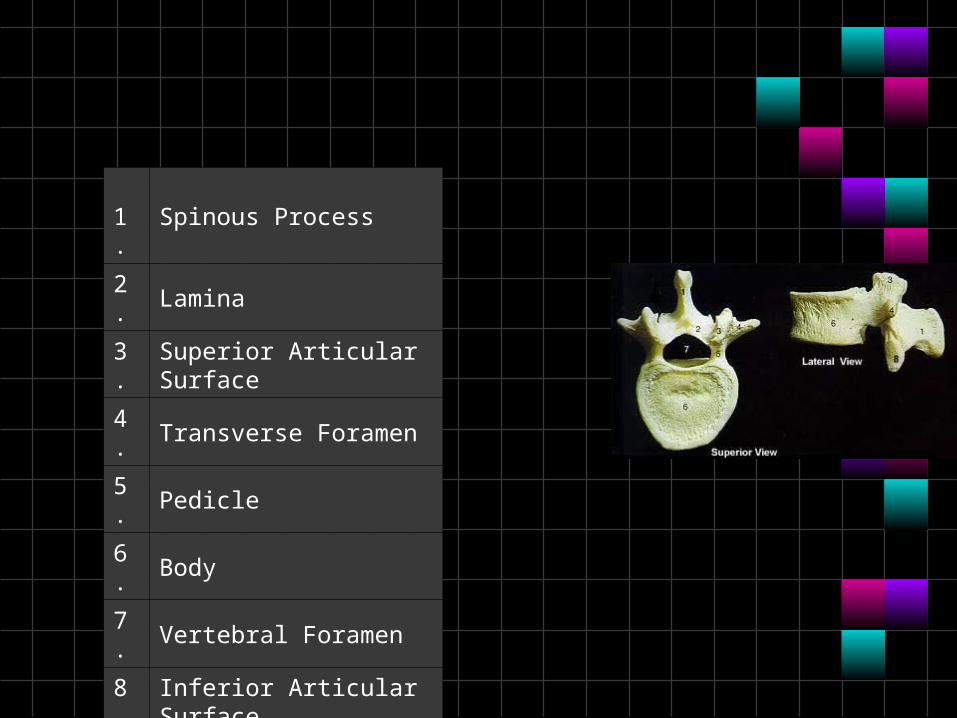
Thoracic
1.Spinous Process2. Lamina3. Superior Articular
Surface4. Transverse Foramen5.Pedicle6. Body7.Vertebral Foramen8.Articular Facet for Rib9.Inferior Articular Surface
Lumbar
1.Spinous Process
2. Lamina
3. Superior Articular Surface
4. Transverse Foramen
5. Pedicle
6. Body
7. Vertebral Foramen
8. Inferior Articular Surface
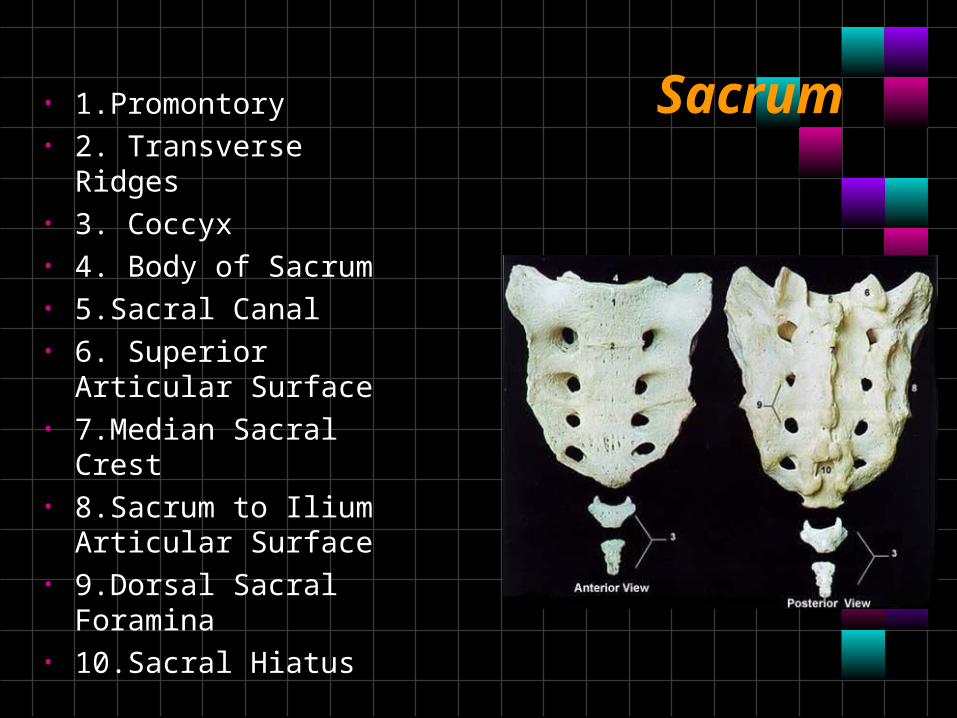
Sacrum• 1.Promontory• 2. Transverse Ridges• 3. Coccyx• 4. Body of Sacrum• 5.Sacral Canal• 6. Superior Articular
Surface• 7.Median Sacral Crest• 8.Sacrum to Ilium
Articular Surface• 9.Dorsal Sacral
Foramina• 10.Sacral Hiatus
Thoracic Bones
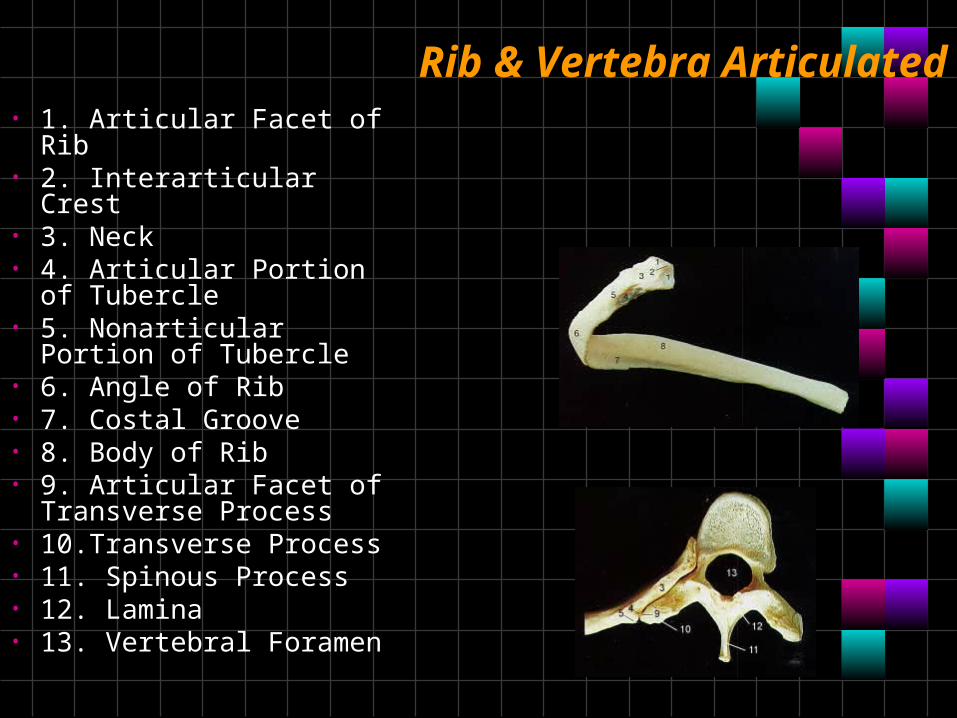
Rib & Vertebra Articulated• 1. Articular Facet of Rib• 2. Interarticular Crest• 3. Neck• 4. Articular Portion of
Tubercle• 5. Nonarticular Portion
of Tubercle• 6. Angle of Rib• 7. Costal Groove• 8. Body of Rib• 9. Articular Facet of
Transverse Process• 10.Transverse Process• 11. Spinous Process• 12. Lamina• 13. Vertebral Foramen
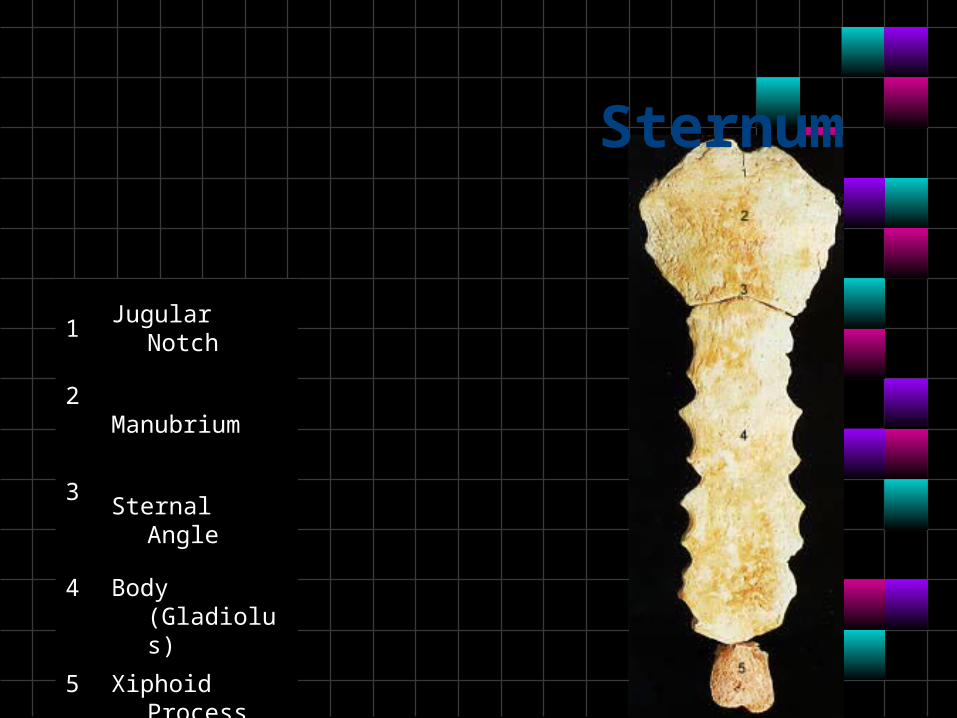
1.Jugular Notch
2. Manubrium
3. Sternal Angle
4. Body (Gladiolus)
5. Xiphoid Process
Sternum
Upper Limb Bones
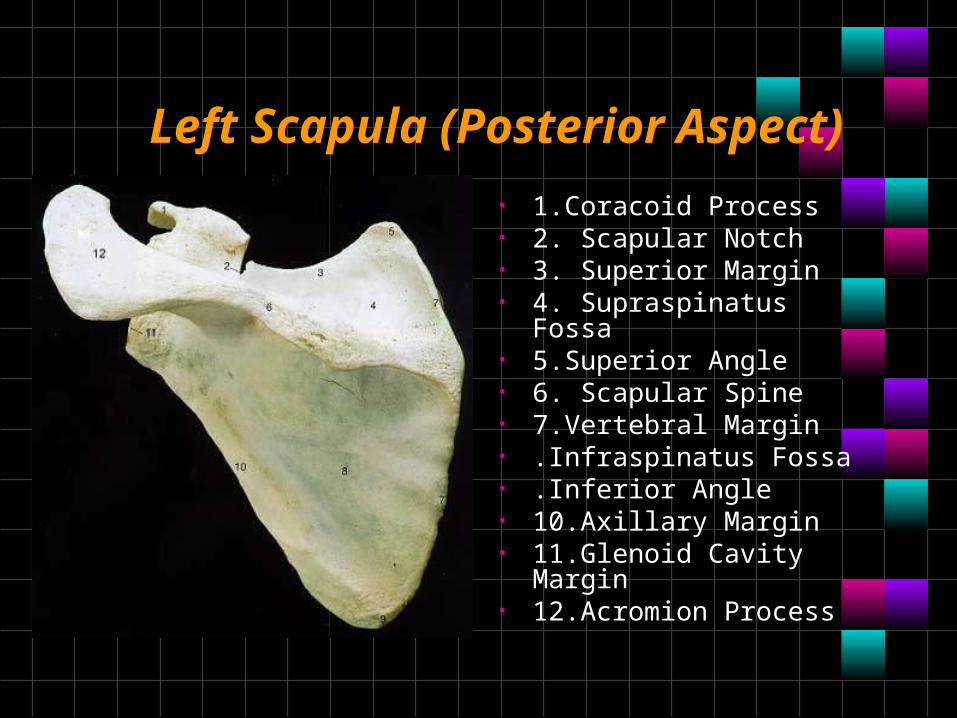
Left Scapula (Posterior Aspect)
• 1.Coracoid Process• 2. Scapular Notch• 3. Superior Margin• 4. Supraspinatus Fossa• 5.Superior Angle• 6. Scapular Spine• 7.Vertebral Margin• .Infraspinatus Fossa• .Inferior Angle• 10.Axillary Margin• 11.Glenoid Cavity Margin• 12.Acromion Process
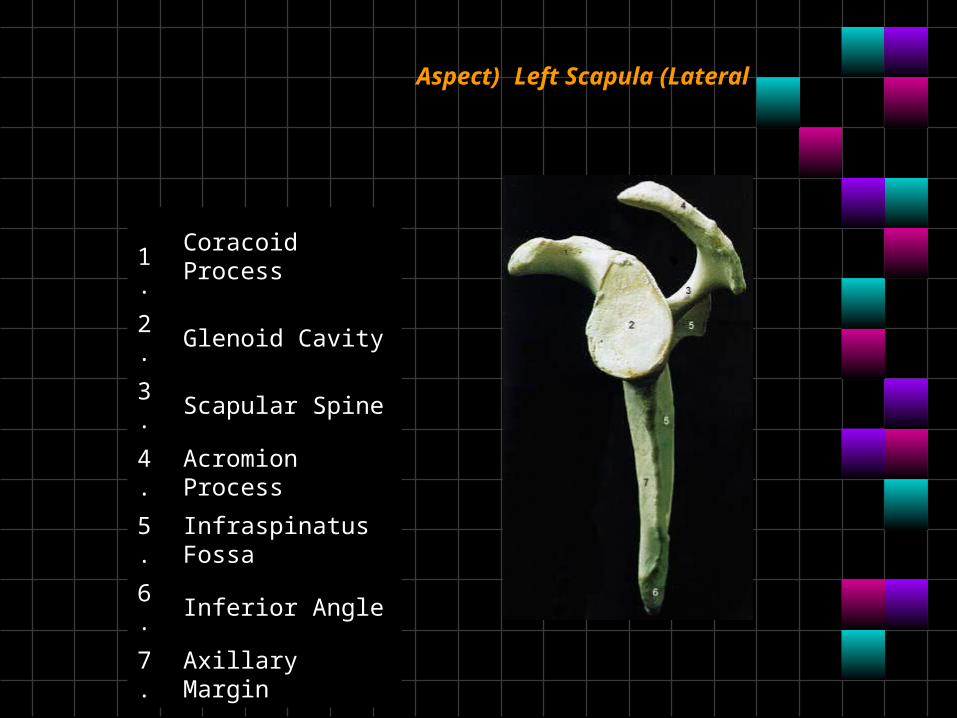
1.Coracoid Process
2. Glenoid Cavity
3. Scapular Spine
4. Acromion Process
5. Infraspinatus Fossa
6. Inferior Angle
7. Axillary Margin
Aspect) Left Scapula (Lateral
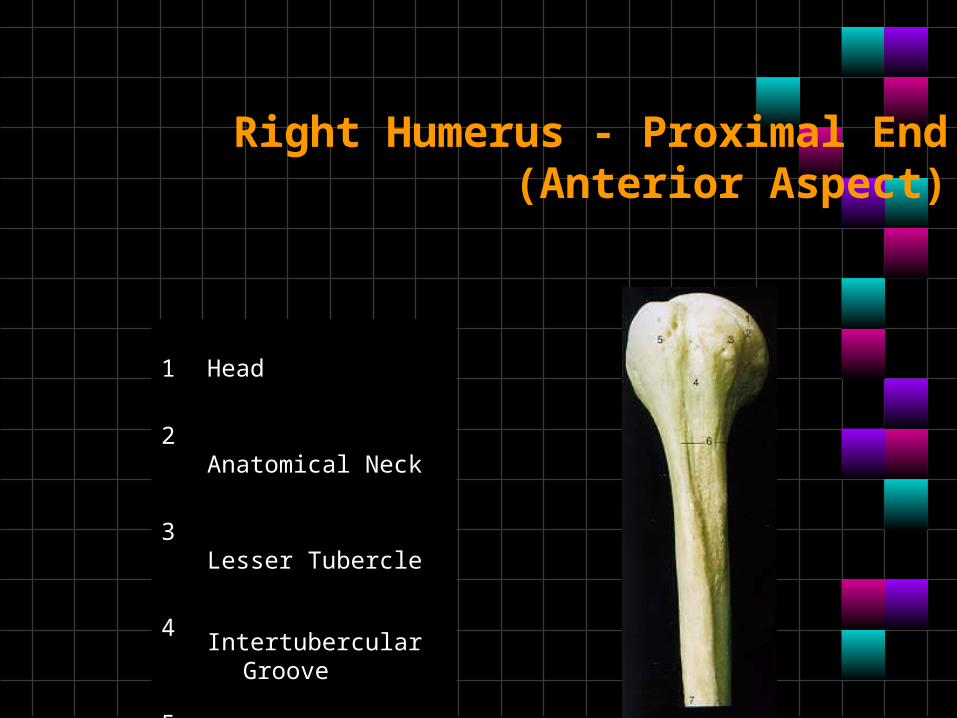
1.Head
2. Anatomical Neck
3. Lesser Tubercle
4. Intertubercular Groove
5. Greater Tubercle
6. Surgical Neck
7. Deltoid Tuberosity
Right Humerus - Proximal End (Anterior Aspect)
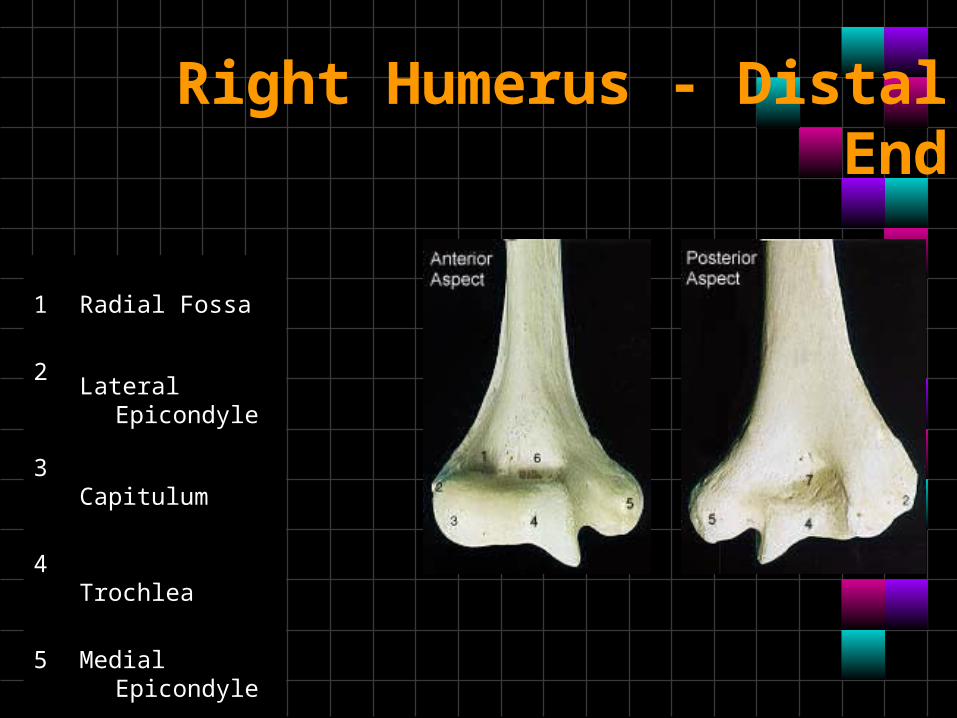
1.Radial Fossa
2. Lateral Epicondyle
3. Capitulum
4. Trochlea
5. Medial Epicondyle
6. Coronoid Fossa
7. Olecranon Fossa
Right Humerus - Distal End
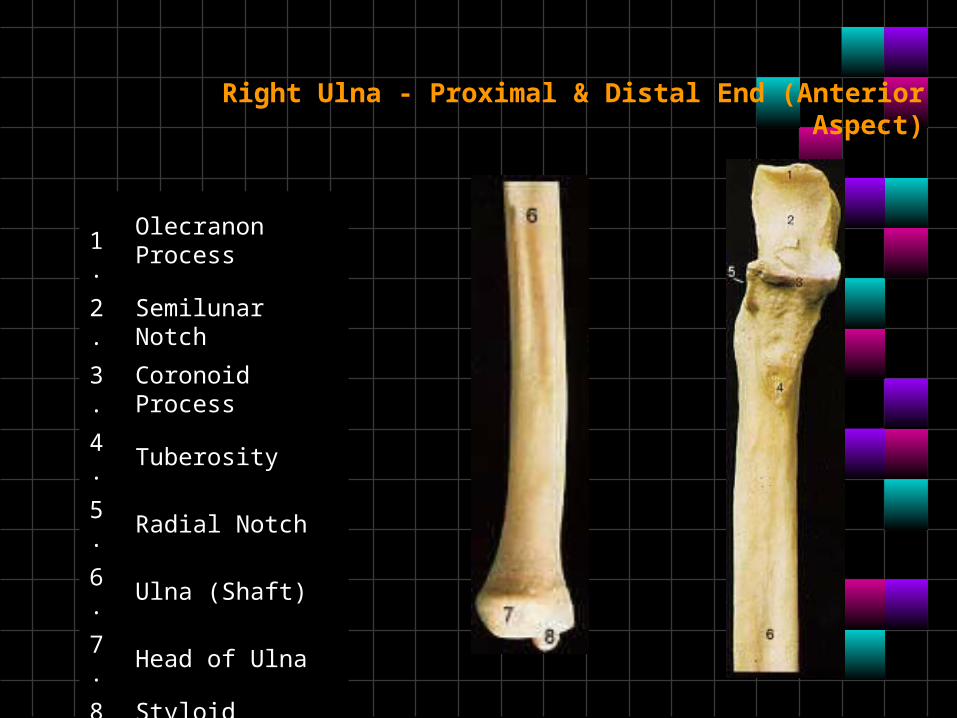
Right Ulna - Proximal & Distal End (Anterior Aspect)
1.Olecranon Process
2. Semilunar Notch
3. Coronoid Process
4. Tuberosity
5. Radial Notch
6. Ulna (Shaft)
7. Head of Ulna
8. Styloid Process
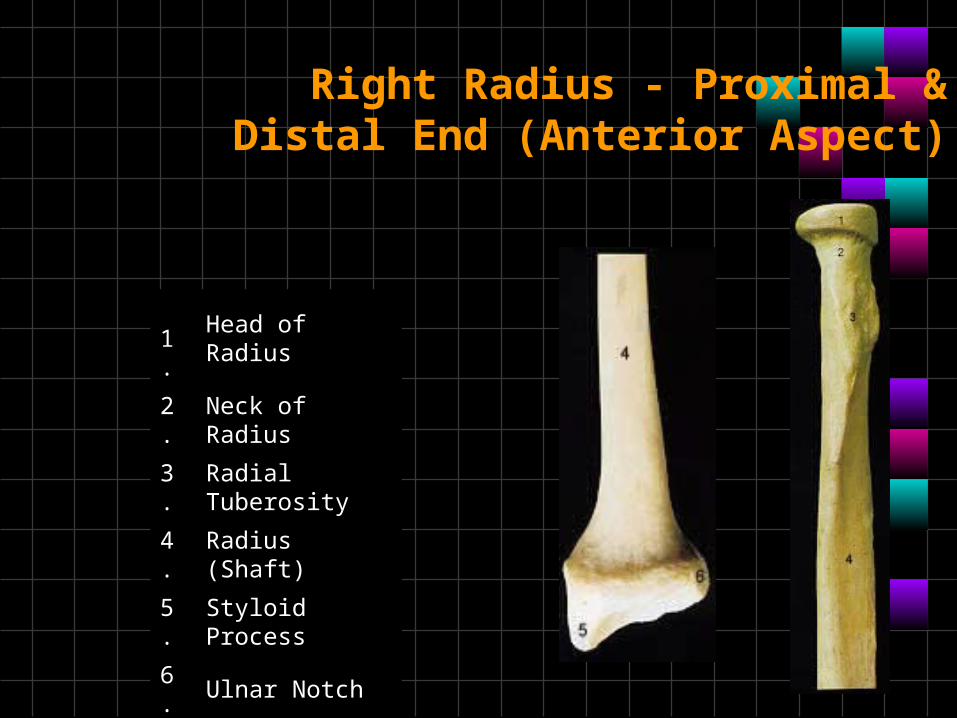
Right Radius - Proximal & Distal End (Anterior Aspect)
1.Head of Radius
2. Neck of Radius
3. Radial Tuberosity
4. Radius (Shaft)
5. Styloid Process
6. Ulnar Notch
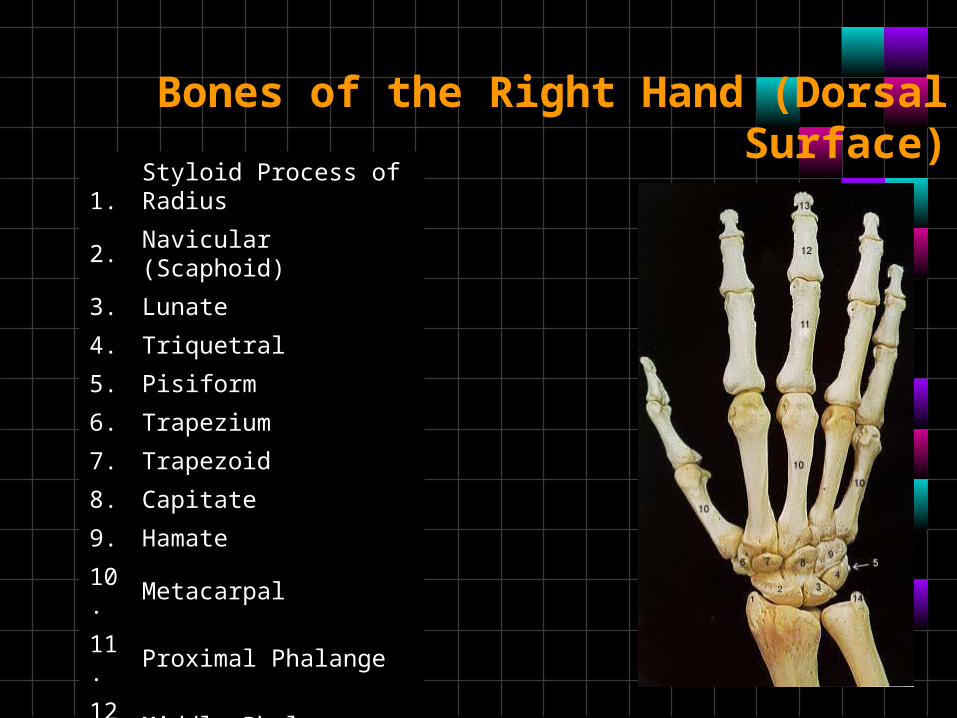
Bones of the Right Hand (Dorsal Surface)
1.Styloid Process of Radius
2. Navicular (Scaphoid)
3. Lunate
4. Triquetral
5. Pisiform
6. Trapezium
7. Trapezoid
8. Capitate
9. Hamate
10. Metacarpal
11. Proximal Phalange
12. Middle Phalange
13. Distal Phalange
14. Styloid Process of Ulna
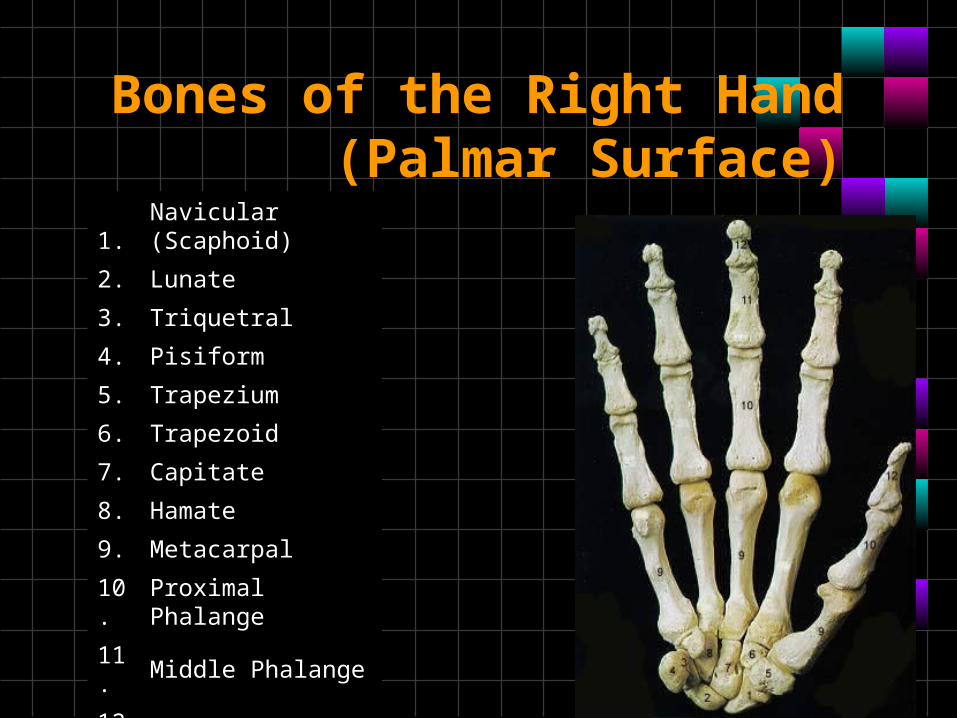
Bones of the Right Hand (Palmar Surface)
1.Navicular (Scaphoid)
2. Lunate
3. Triquetral
4. Pisiform
5. Trapezium
6. Trapezoid
7. Capitate
8. Hamate
9. Metacarpal
10. Proximal Phalange
11. Middle Phalange
12. Distal Phalange
Lower Limb Bones
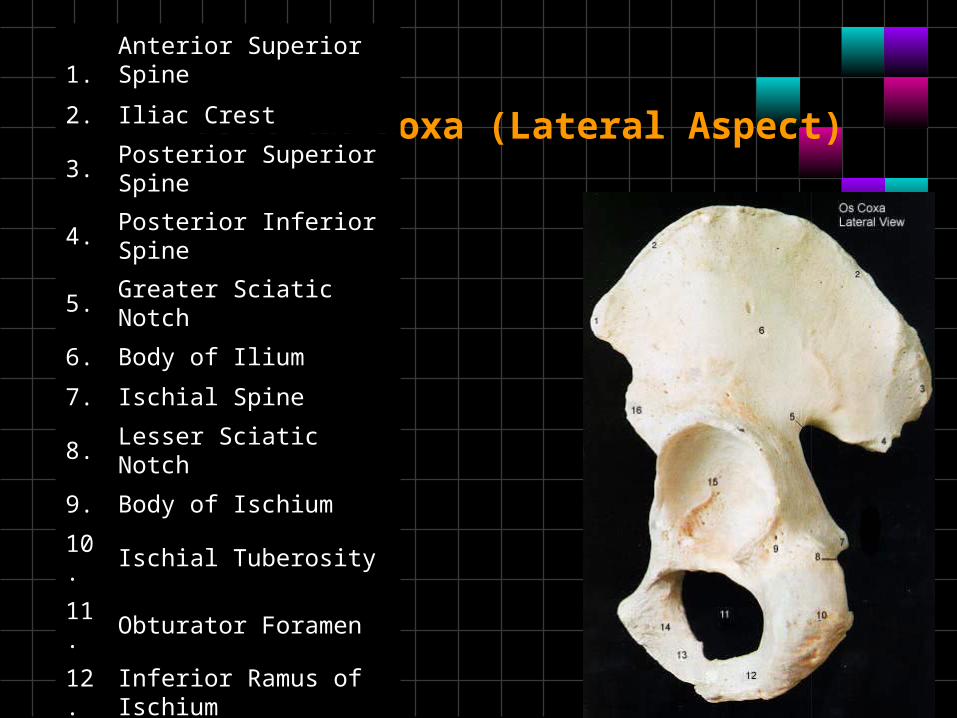
Left Os Coxa (Lateral Aspect)
1.Anterior Superior Spine
2. Iliac Crest
3. Posterior Superior Spine
4. Posterior Inferior Spine
5. Greater Sciatic Notch
6. Body of Ilium
7. Ischial Spine
8. Lesser Sciatic Notch
9. Body of Ischium
10. Ischial Tuberosity
11. Obturator Foramen
12. Inferior Ramus of Ischium
13. Inferior Ramus of Pubis
14. Body of Pubis
15. Acetabulum
16. Anterior Inferior Spine
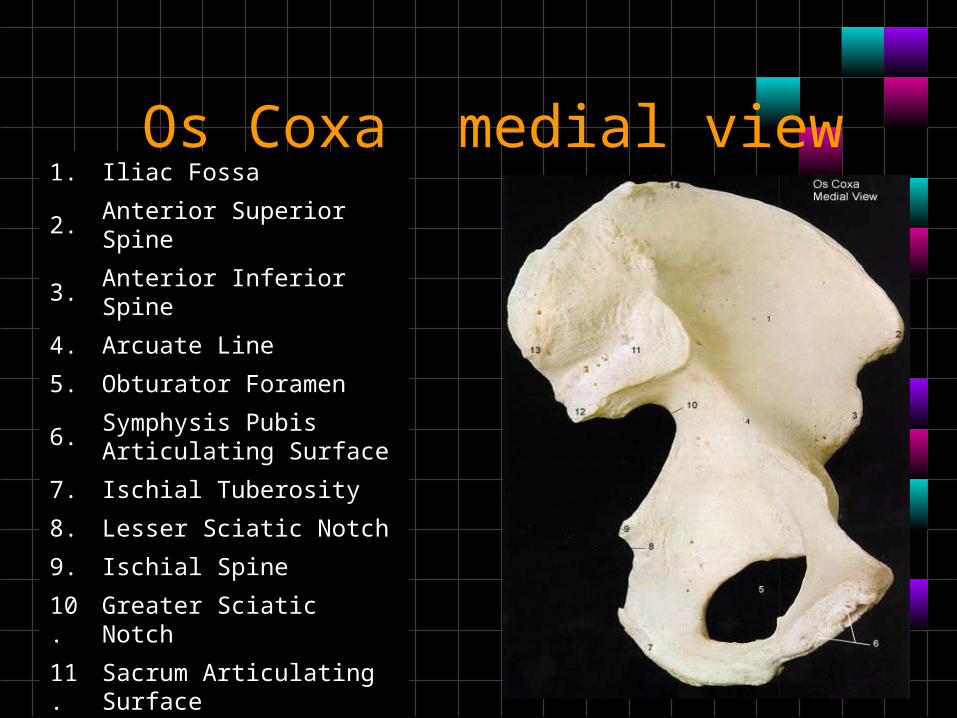
Os Coxa medial view1. Iliac Fossa
2. Anterior Superior Spine
3. Anterior Inferior Spine
4. Arcuate Line
5. Obturator Foramen
6. Symphysis Pubis Articulating Surface
7. Ischial Tuberosity
8. Lesser Sciatic Notch
9. Ischial Spine
10. Greater Sciatic Notch
11. Sacrum Articulating Surface
12. Posterior Inferior Spine
13. Posterior Superior Spine
14. Iliac Crest
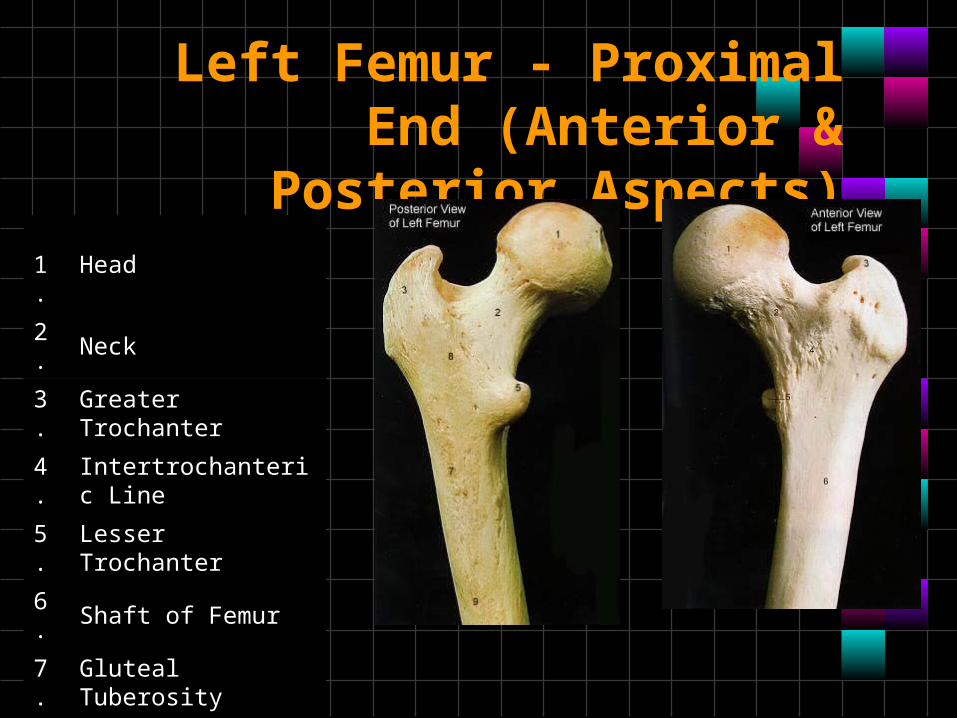
Left Femur - Proximal End (Anterior & Posterior Aspects)
1.Head
2. Neck
3. Greater Trochanter
4. Intertrochanteric Line
5. Lesser Trochanter
6. Shaft of Femur
7. Gluteal Tuberosity
8. Intertrochanteric Crest
9. Linea Aspera
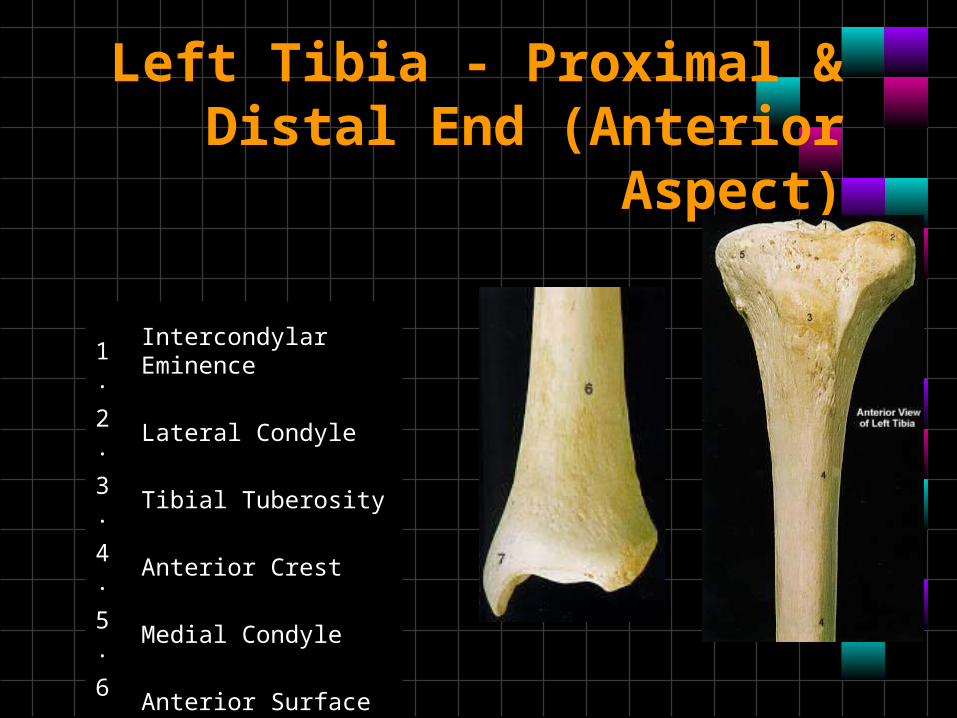
Left Tibia - Proximal & Distal End (Anterior Aspect)
1.Intercondylar Eminence
2. Lateral Condyle
3. Tibial Tuberosity
4. Anterior Crest
5. Medial Condyle
6. Anterior Surface
7. Medial Malleolus
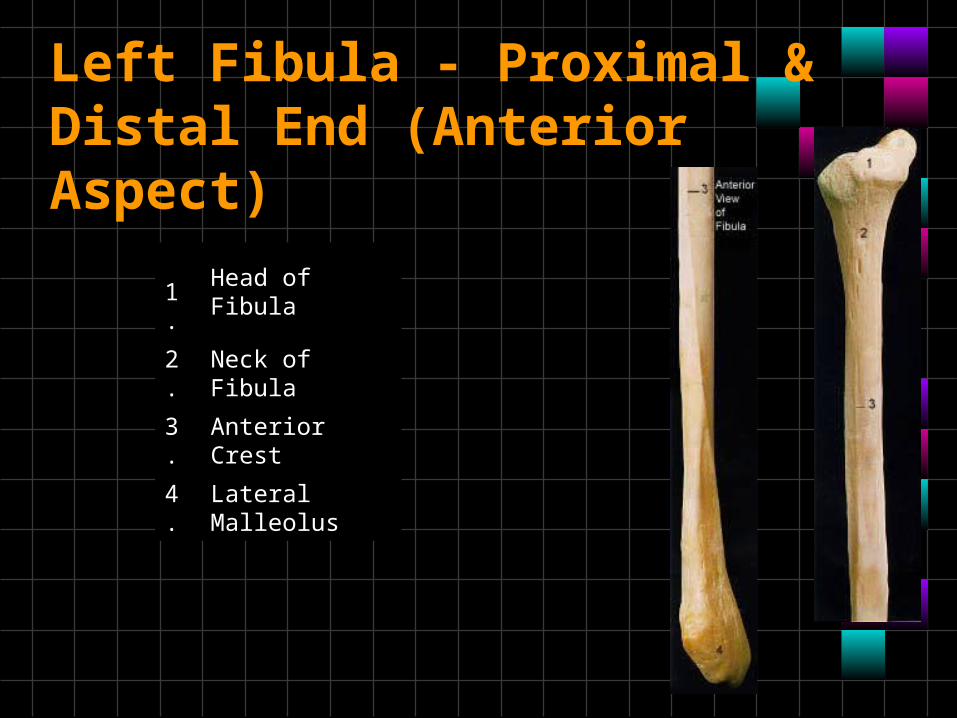
Left Fibula - Proximal & Distal End (Anterior Aspect)
1.Head of Fibula
2. Neck of Fibula
3. Anterior Crest
4. Lateral Malleolus
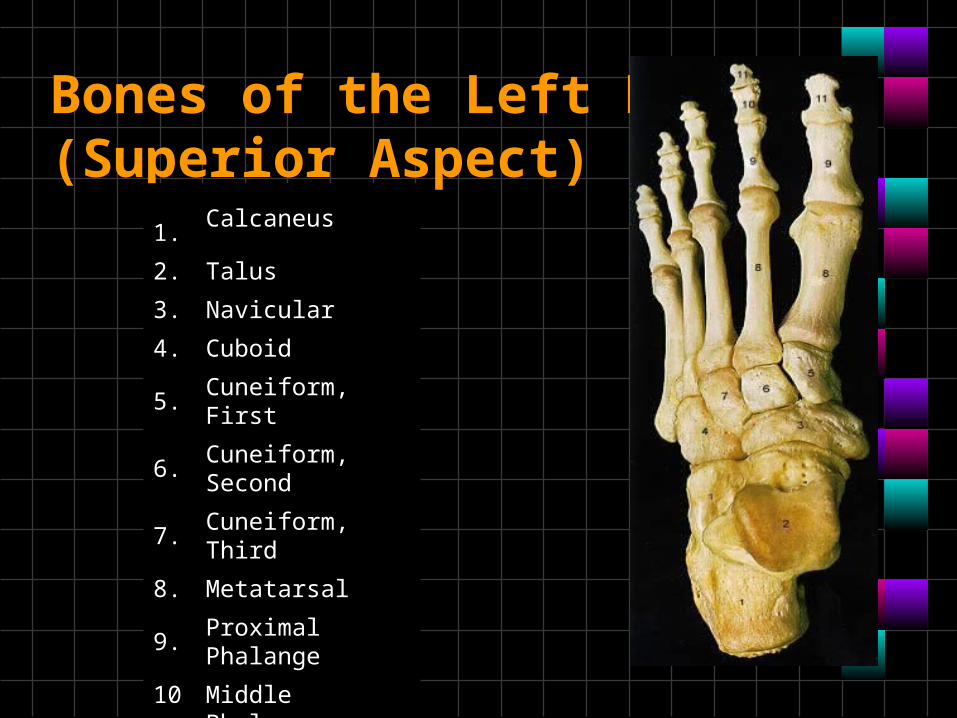
Bones of the Left Foot (Superior Aspect)
1.Calcaneus
2. Talus
3. Navicular
4. Cuboid
5. Cuneiform, First
6. Cuneiform, Second
7. Cuneiform, Third
8. Metatarsal
9. Proximal Phalange
10. Middle Phalange
11. Distal Phalange

Bones of the Left Foot (Lateral Aspect)
1.Calcaneus
2. Talus
3. Navicular
4. Cuboid
5. Cuneiform, First
6. Cuneiform, Second
7. Cuneiform, Third
8. Metatarsal
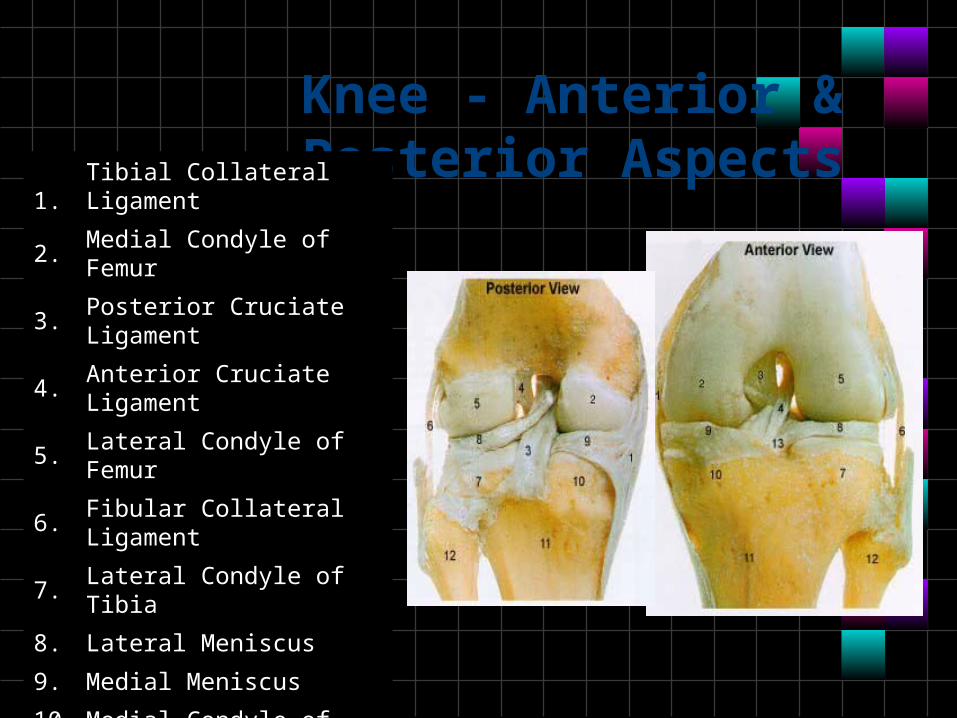
Knee - Anterior & Posterior Aspects
1.Tibial Collateral Ligament
2. Medial Condyle of Femur
3. Posterior Cruciate Ligament
4. Anterior Cruciate Ligament
5. Lateral Condyle of Femur
6. Fibular Collateral Ligament
7. Lateral Condyle of Tibia
8. Lateral Meniscus
9. Medial Meniscus
10. Medial Condyle of Tibia
11. Tibia
12. Fibula
13. Transverse Ligament

Skeletal Disorders
• Osteoarthritis• A type of arthritis marked by progressive
cartilage deterioration in synovial joints and vertebrae
The symptoms of osteoarthritis include:
• Deep aching joint pain that gets worse after exercise, or putting weight on it, and is relieved by rest
• Grating of the joint with motion • Joint pain in rainy weather • Joint swelling • Limited movement • Morning stiffness• No symptoms
• Medications• Nonsteroidals• Cox 2 inhibitors• Antiinflammatories
• Lifestyle change’• Applying heat and cold • Eating a healthy balanced diet • Getting rest • Losing weight if you are overweight • Protecting the joints
Osteoarthritis-treatment
• Physical therapy• Braces• Surgery
• Arthroscopy• Joint replacement

Arthritic joint x-ray
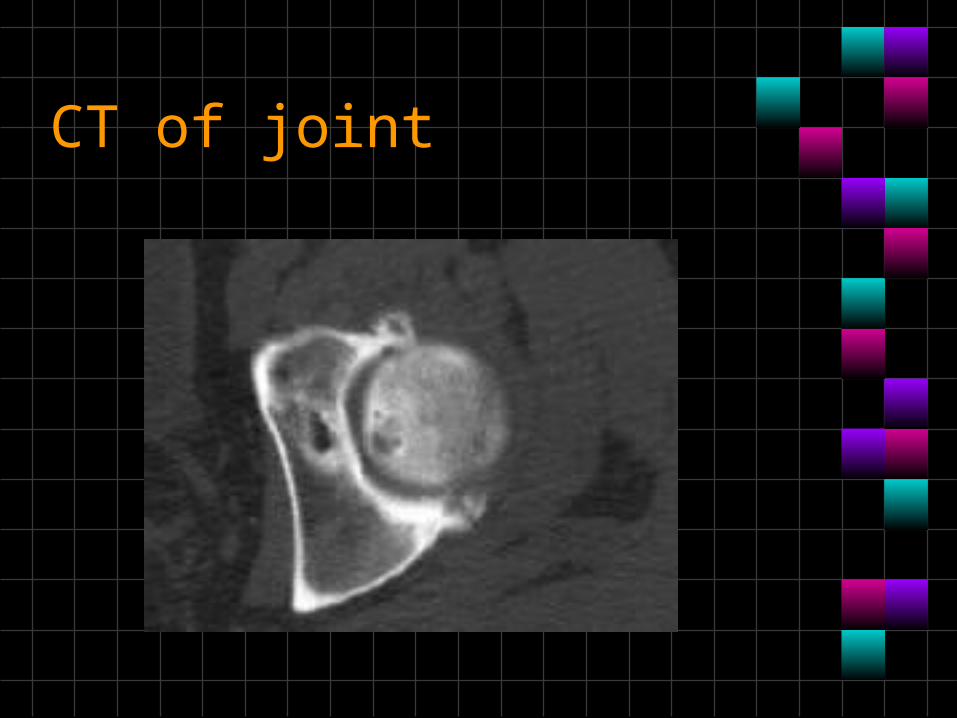
CT of joint
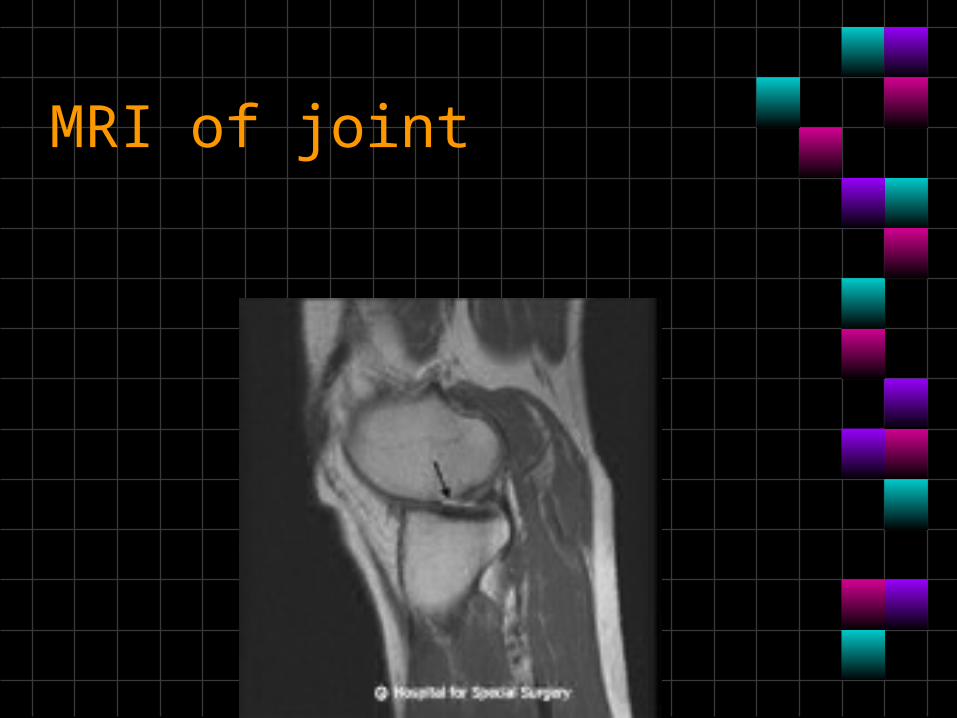
MRI of joint
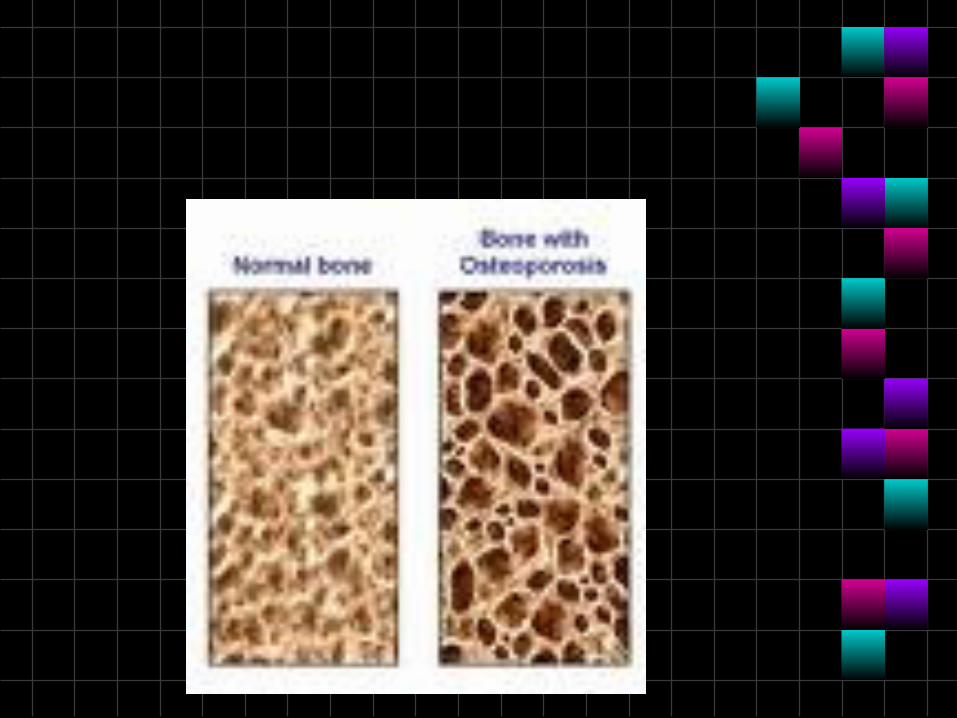
• Osteoporosis-• Loss of bone mass that occurs throughout
the skeleton.• Bones become very fragile
Causes of osteoporosis
• Female gender postmenopausal• Caucasian or Asian race;• Thin and small body frames;• Family history of osteoporosis (for example, having a
mother with an osteoporotic hip fracture doubles your risk of hip fracture);
• Personal history of fracture as an adult;• Cigarette smokingExcessive alcohol consumption;• Lack ofexercise;• Diet low in calcium;• Poor nutrition and poor general health;
Treatment for osteoporsis
• Bisphosphonates are — by far — the most common medications prescribed for osteoporosis treatment. These include:
• Alendronate (Fosamax) • Risedronate (Actonel) • Ibandronate (Boniva) • Zoledronic acid (Reclast)
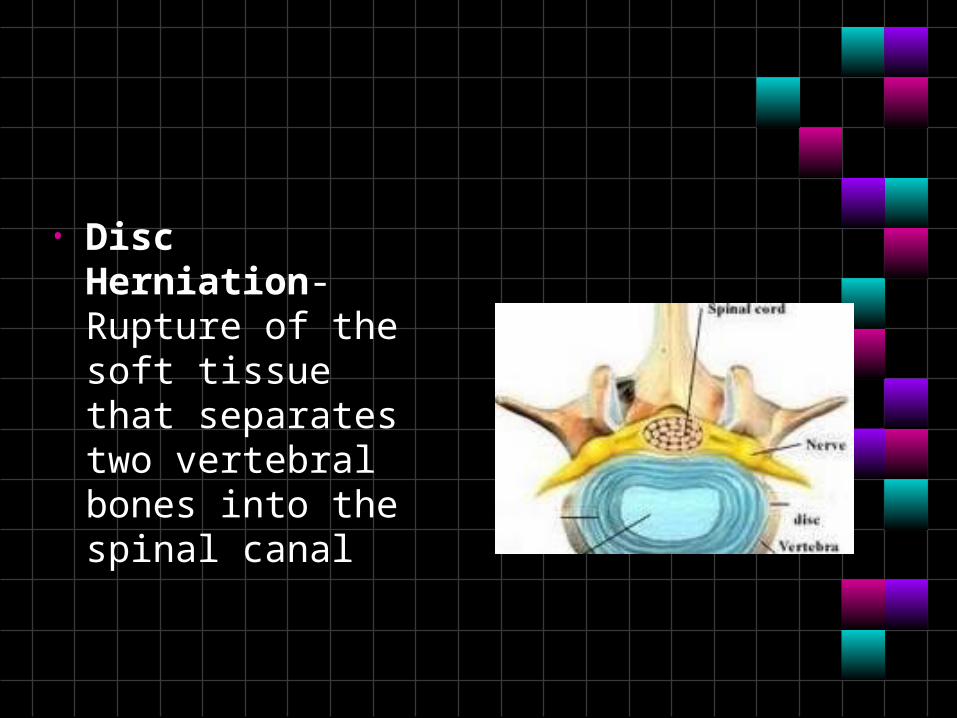
• Disc Herniation-Rupture of the soft tissue that separates two vertebral bones into the spinal canal
Sign and symptom
• Electric shock pain• Tingling and numbness• Muscle weakness• Loss of bladder control
Treatment
• Exercise• Medication-NSAIDs• Steroid injection in joint• surgery
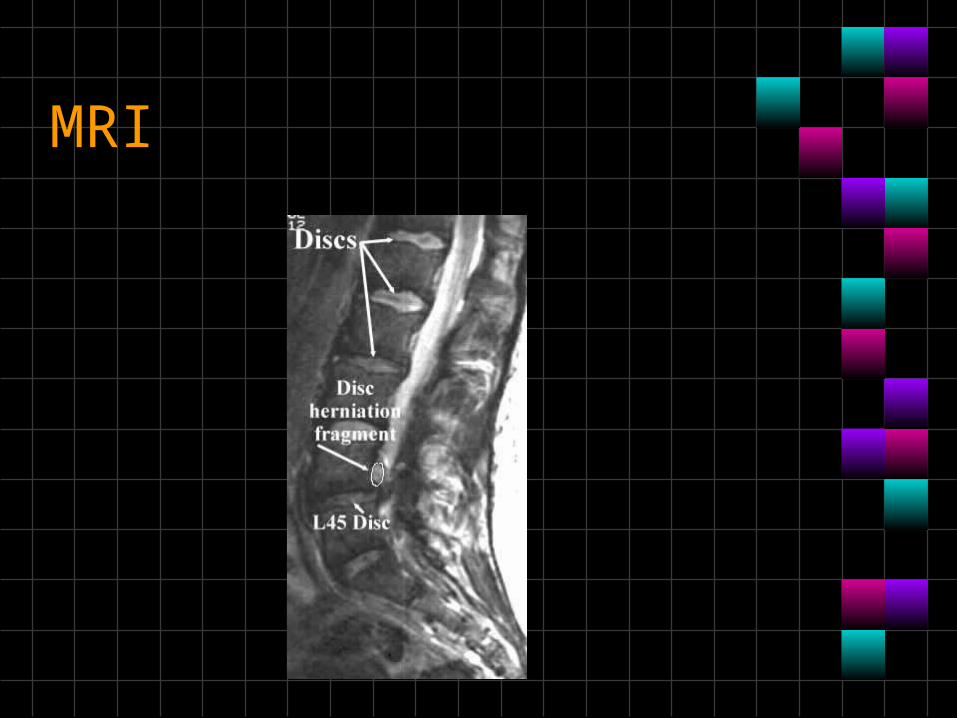
MRI
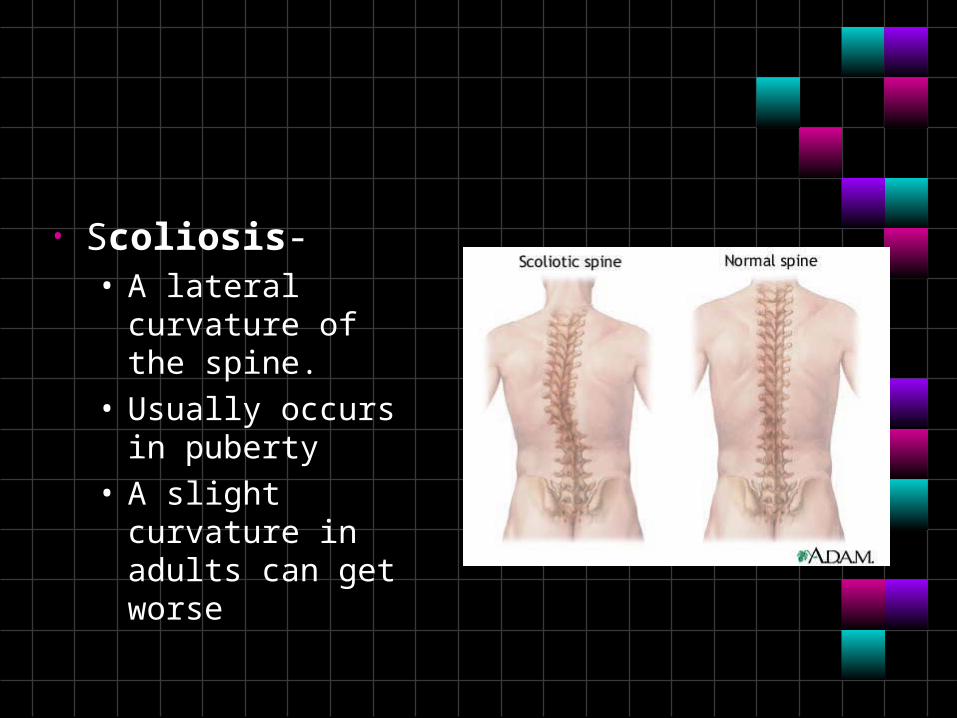
• Scoliosis-• A lateral curvature of
the spine.• Usually occurs in
puberty• A slight curvature in
adults can get worse
Treatment
• If the curve is less than 25°, no treatment is required, and the child can be reexamined every four to six months.
• If the curve is more then 25° but less than 30°, a back brace may be used for treatment.
• Curves more than 45° will need to be evaluated for the possibility of surgical correction. Surgical correction involves fusing vertebrae together to correct the curvature and may require inserting rods next to the spine to reinforce the surgery
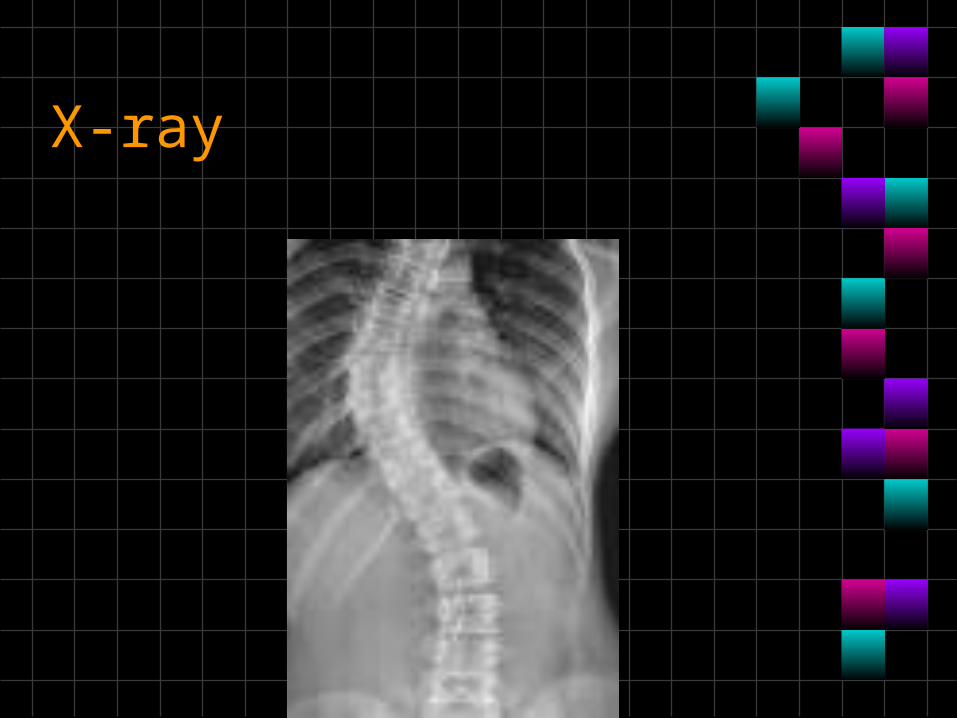
X-ray
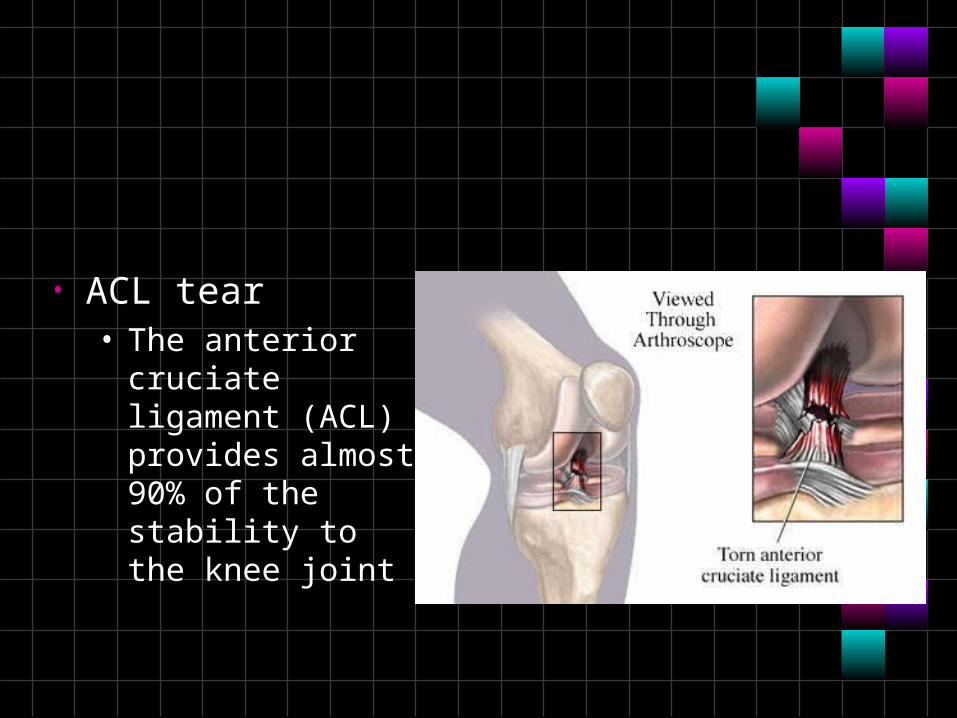
• ACL tear• The anterior cruciate
ligament (ACL) provides almost 90% of the stability to the knee joint

Immediate treatment
• R.I.C.E. stands for: • Rest - The individual is advised to rest the knee from
weight-bearing activities allowing the swelling to settle.
• Ice - Placing a cold compress or ice pack on the knee is helpful in controlling inflammation as well as helping to reduce pain.
• Compression - Utilizing an ace wrap for compression around the knee is beneficial to control the swelling.
• Elevation - Lying down with the leg elevated higher than the level of the chest is helpful in controlling and reducing swelling.
• ACL reconstruction is a highly successful operation. With good rehabilitation, 90% to 95% of individuals who undergo this surgery can expect to return to full sports participation within six months.
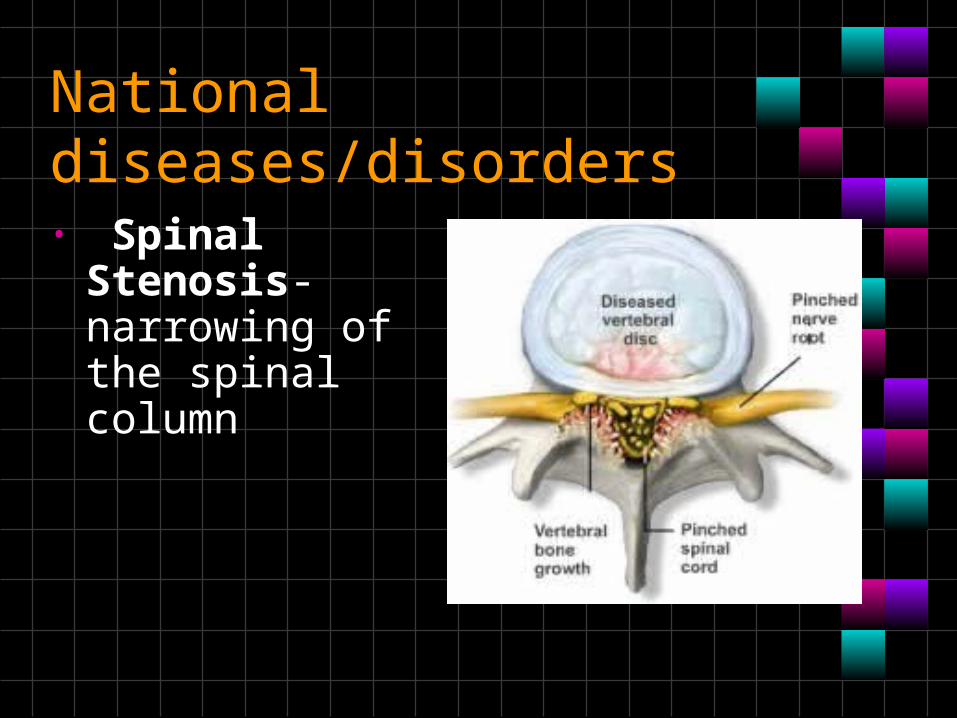
National diseases/disorders
• Spinal Stenosis-narrowing of the spinal column
Signs and symptoms
• Low back pain • Leg numbness and tingling • Limitations in walking
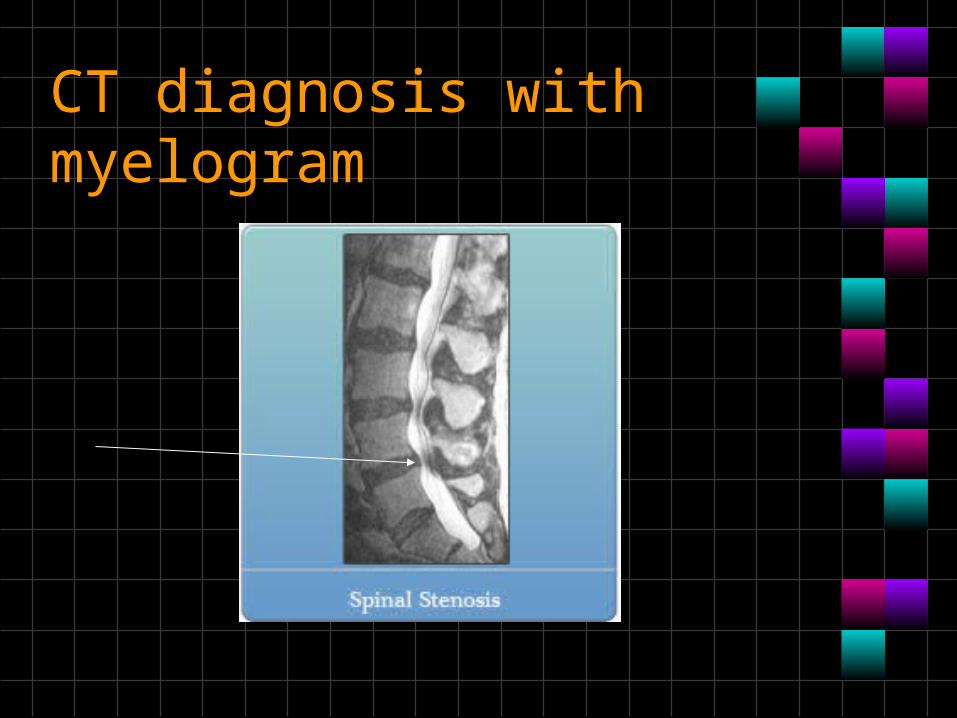
CT diagnosis with myelogram
• Exercise • Activity modification • Physical therapy• Epidural injections• Surgery
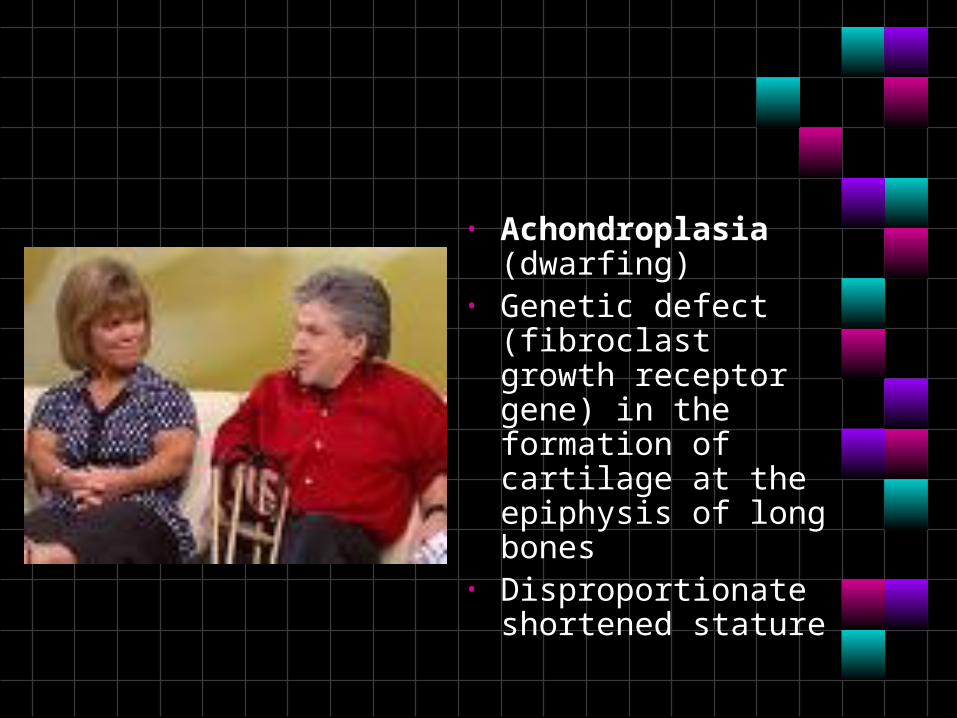
• Achondroplasia (dwarfing)
• Genetic defect (fibroclast growth receptor gene) in the formation of cartilage at the epiphysis of long bones
• Disproportionate shortened stature
• An average-size trunk • Short arms and legs, with particularly short upper
arms and upper legs • Short fingers, often with a wide separation
between the middle and ring fingers • Limited mobility at the elbows • A disproportionately large head, with a prominent
forehead and flattened bridge of the nose • Progressive development of bowed legs (genu
varum) • Progressive development of swayed lower back
(lordosis) • An adult height around 4 feet — about 122
centimeters (cm) • Treatments for most dwarfism-related conditions
don't increase stature but may lessen complications
• Juvenile Rheumatoid Arthritis-chronic inflammatory diseases involving the joints or other organs in children under 16
• Juvenile arthritis is different from adult arthritis in two ways: • children with arthritis sometimes outgrow the
illness, • tends to be difficult to diagnose because the
regular tests for arthritis are unreliable for children.• Systemic onset type begins with very high
fevers, frequently as a skin rash and shows evidence of inflammation in many internal organ systems as well as the joints
Symptoms:• Arthritis symptoms:
• Joint stiffness on arising in the morning • `Limited range of motion • Slow rate of growth or uneven arm or leg growth • Hot, swollen, painful joints • A child may stop using an affected limb • Back pain
• Systemic JRA symptoms:• Fever, usually high fevers every day • Rash that comes and goes with the fever • Swollen lymph nodes (glands)
• JRA can also cause eye inflammation. These symptoms include:• Red eyes • Eye pain • Photophobia (increased pain when looking at a light) • Visual changes
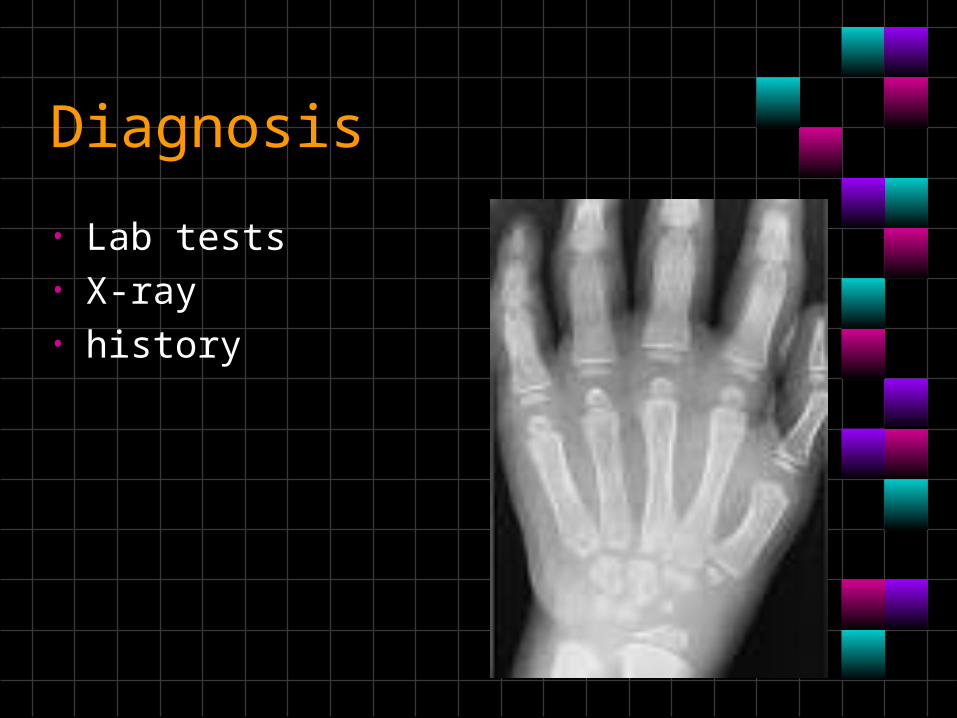
Diagnosis
• Lab tests• X-ray• history
Treatment
• Medicines used to treat this condition may include:• Nonsteroidal anti-inflammatory drugs (NSAIDs) • Corticosteroids • An antimalaria medicine called hydroxychloroquine, which helps
reduce inflammation related to JRA • Disease-modifying anti-rheumatic drugs (DMARDs), including
methotrexate • Biologic drugs, such as such as etanercept and infliximab,
which block high levels of inflammatory proteins• Note: Talk to your health care provider before giving aspirin or
NSAIDs to children.• Physical therapy and exercise programs may be recommended.
Surgery may be needed in some cases, including joint replacement
• Ankylosing spondylitis-• inflammation and
immobility of a joints in the spine
• A form of arthritis• Genetics plays a role
in the disease, but the cause of AS is still unknown
• Eventually, the whole back may become curved and inflexible if the bones fuse (this is known as "bamboo spine"). AS is a systemic disorder that may involve multiple organs, such as the:• eye (causing an inflammation of the iris, or iritis) • heart (causing aortic valve disease) • Lungs • skin (causing a scaly skin condition, or psoriasis) • gastrointestinal tract (causing inflammation within
the small intestine, called ileitis, or inflammation of the large intestine, called colitis)
Diagnosis
• Diagnosis is by signs and symptoms
Treatment
• Physical therapy• NSAIDS and antiinflammatory therapy• Bracing
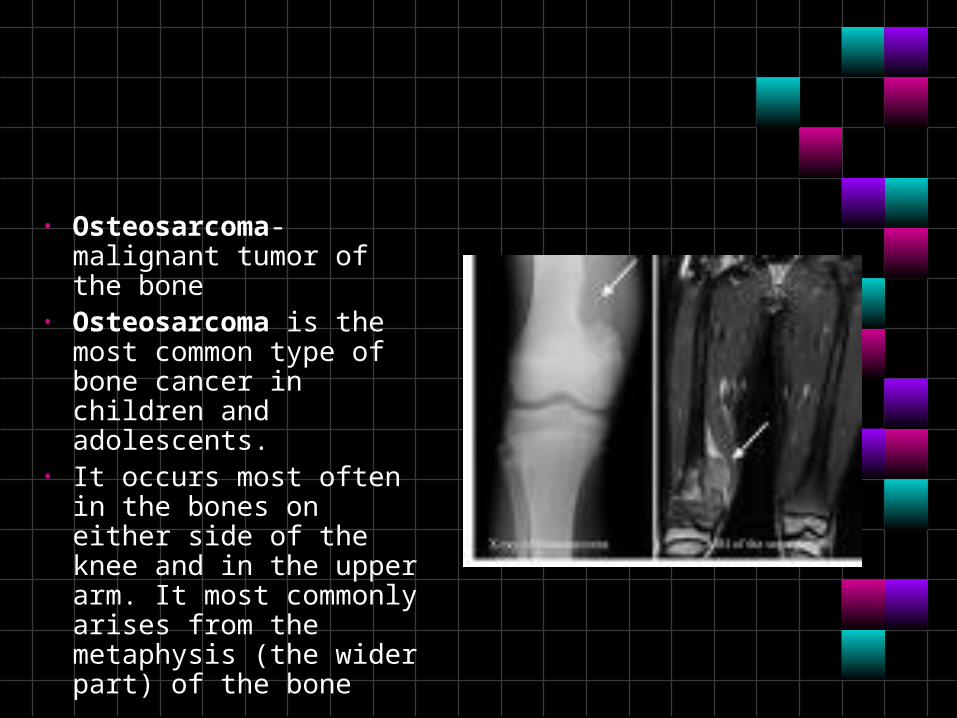
• Osteosarcoma-malignant tumor of the bone
• Osteosarcoma is the most common type of bone cancer in children and adolescents.
• It occurs most often in the bones on either side of the knee and in the upper arm. It most commonly arises from the metaphysis (the wider part) of the bone
Incidence• Each year in the United States,
osteosarcoma is diagnosed in approximately 400 children and adolescents younger than 20 years.
• The peak incidence of osteosarcoma is in the second decade of life, during the adolescent growth spurt. It is extremely rare in children before the age of 5 years.
• Osteosarcoma is somewhat more likely to affect males than females.
• The incidence in black children is higher than that in whites.
•
• The cause of osteosarcoma is unknown; however, irradiation and genetic influences have been implicated in its development
• Patients usually present with pain, swelling, and sometimes decreased joint motion.
• Occasionally, a patient may present with a fracture at the tumor site
• The work up of a patient with suspected osteosarcoma typically includes blood tests, plain x-rays and magnetic resonance imaging (MRI) of the affected bone, computerized tomography (CT) scan of the chest and a radionuclide bone scan.
• A biopsy is always required to make the diagnosis. It is preferable to have the biopsy done by the surgeon who will ultimately perform the definitive surgical treatment.
• Treatment of osteosarcoma includes surgery and chemotherapy.
• Surgical removal of all gross and microscopic tumor is required to prevent local tumor recurrence. Before the 1970s, amputation was the only surgical approach. Currently, 95 percent of patients with localized osteosarcoma of the extremity can be considered for limb-salvage surgery.
Survival Rates
• Currently, the estimated 5-year survival for patients with osteosarcoma is 65 percent compared with 15 percent in the early 1960s.
• The presence of metastasis at diagnosis has a major impact on patient survival. The estimated survival rate for patients with localized osteosarcoma is about 75 percent compared to 30 percent for patients with metastatic disease