Embed Size (px)
Citation preview

Systems Analysis of Errors
Debora Simmons, PhD, RN, CCNS

What is a Systems Approach?
Humans are fallible and errors are to be expected, even in the best organizations. Errors are seen as consequences rather than causes, having their origins not so much in the perversity of human nature as in "upstream" systemic factors.
Reason, 2000

What is a System?
A set or group of interacting, interrelated or interdependent elements or parts that are organized and integrated to form a collective unity or a unified whole to achieve a common objective
Reason,1990

Systems of the body
Interdependent – lung-heart- kidney Interactive –vascular-heart-kidney
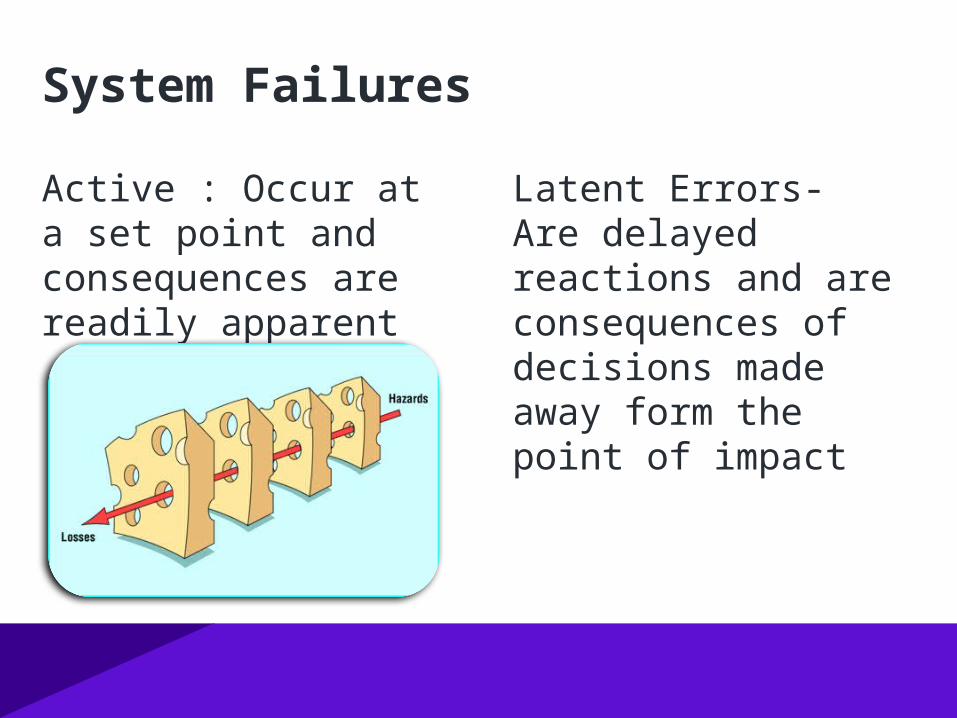
Active : Occur at a set point and consequences are readily apparent
Latent Errors- Are delayed reactions and are consequences of decisions made away form the point of impact
System Failures
James Reason

B James

A Path to Failure
Latent Current Active
Failures Conditions Failures DefensesACCIDENT
Cognitive Failures (Memory Lapses)
Slips
Mistakes
Workload
Equipment
Knowledge
Ability
Environment
Manufacture Design
Management Decisions
Policy

van der Schaff- modified for healthcare
Technical
Organizational
Human Factors
Adequate defenses
Return to Normal
Developing Errors
Near Miss
Dangerous Situation
Dangerous Situation
ERROR(Inadequate
Defenses)
ERROR(Inadequate
Defenses)

The Cause and Effect Principle

#1 Cause and Effect
Cause and effect are the same thingDiffer by how we perceive them in time
Effects Causes
Injury Caused By Fall
Fall Caused By Wet Surface
Wet Surface Caused By Leaky Valve
Leaky Valve Caused By Seal Failure
Seal Failure Caused By Not Maintained

#2 Cause and Effect
Cause and Effect are part of a continuum of causes A Primary Effect is the effect of a consequence that we want to prevent from occurring
CBCBCBCBCBInjury Fall
Wet Surface
Leaky Valve
Seal Failure
Not Main-tained

Cause and Effect # 3
Each effect has at least two causes in the form of actions and conditions Actions are momentary causes that bring conditions together to cause an effect
Conditions are causes that exist over time prior to an action
Primary Effect
Action
Condition
By

Cause and Effect Principle #4
An effect exists only if its causes exist at the same point in time and space
You have to have: the action and the conditions

Cause and Effect Principle # 5
There is never one cause

Problem Solving Using C/E
Identify causal relationships and control one or more of the causes to affect the problem in a way that meets the objectives
Understand the problem Use an effective tool set

Classic
If people are more
careful,
pay attention,
are more detailed
there will be a
decrease in errors
(My Mother)

New
It is the design of
objects,
activities,
procedures
patterns of behavior
that result in error
Norman and Reason

Human Factors Analysis
Properties of Memory
Decision Making
Information
Environment
Physical

Error is Inevitable Because of Human Limitations
Limited memory capacity Limited mental processing capacity Negative effects of stress - Tunnel vision Negative influence of fatigue and other
physiological factors Limited ability to multitask Flawed teamwork

Systems of Care
> 80 % medical error is system derived 95 % of mistakes are made by the good guys like
you and me Finding the “Bad Apples” and fixing them doesn’t
work – there aren’t enough The system solution – make it hard to do the
wrong thing

Nurse inadvertently connected a feeding of expressed breast milk to an intravenous line
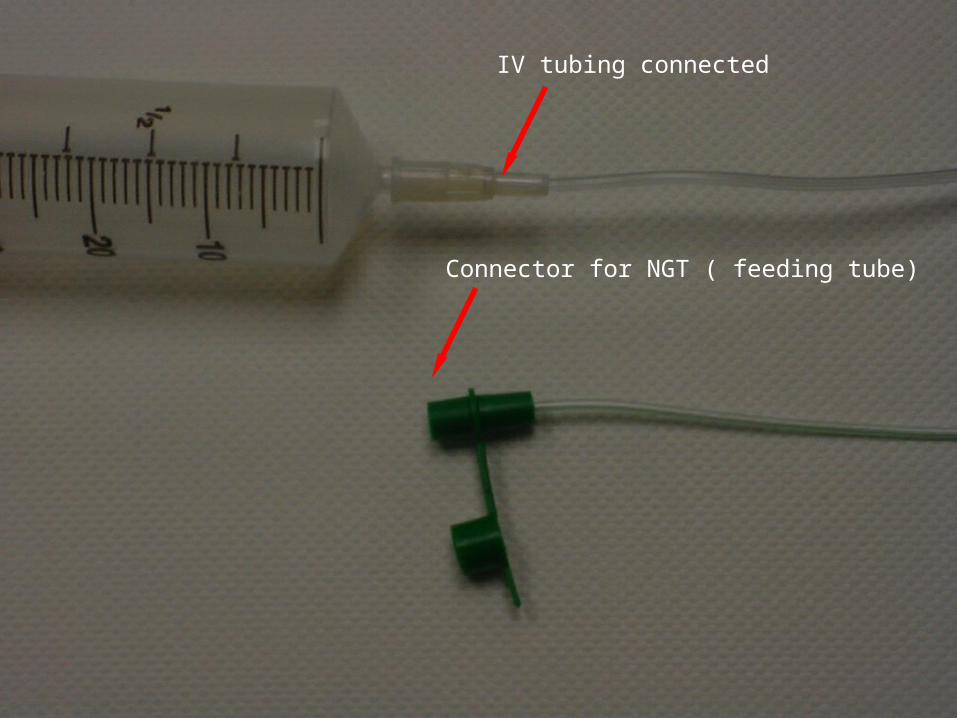
IV tubing connected
Connector for NGT ( feeding tube)

Connector for NGT (feeding tube) connected
IV tubing

IV tubing connected
Connector for NGT (feeding tube)

Syringe used for feeding

Syringe Pump used for IV infusions and Feeding through NGT

27


29
Central Venous Catheter
Gastrostomy TubeArterial Catheter
Epidural Catheter
2/7/00

Literature Search
First documented misconnection – 1972 (Wallace)
© 2006 Simmons & Graves

Joint Commission Institute for Safe
Medication Practices Food and Drug
Administration American Nurses
Association
American Association Medical Instrumentation
- 1996 and 2005
International Standards Organization
World Health Organization
California Bill 2013 deadaline
ADvaMED
Tubing misconnections

A review by USP of more than 1200 cases: Intravenous infusions connected to epidural lines, and epidural solutions (intended for
epidural administration) connected to peripheral or central IV catheters.
Bladder irrigation solutions using primary intravenous tubing connected as secondary
infusions to peripheral or central IV catheters.
Infusions intended for IV administration connected to an indwelling bladder (foley)
catheter.
Infusions intended for IV administration connected to nasogastric (NG) tubes.
Intravenous solutions administered with blood administration sets, and blood products
transfused with primary intravenous tubing.
Primary intravenous solutions administered through various other functionally dissimilar
catheters, such as external dialysis catheters, a ventriculostomy drain, an amnio-infusion
catheter, and the distal port of a pulmonary artery catheter.

Tubing Misconnections: Normalization of Deviance
Debora Simmons, Lene Symes, Peggi Guenter, and Krisanne Graves(Nutr Clin Pract. 2011;26:286-293)
Case reportsN =116 Adult (N=60)Child/infant (N=30)Not Specified (NS) (N=26)
Patient Outcome from 116 casesDeath (N=21) Survival:
Hypersensitivity and Hypercoagulopathy reaction (N=1)Septicemia/sepsis (N=16):
2 with neurologic damage2 with respiratory arrest33 with hypoxia1 with seizure & hypoglycemia5 with intracranial hemorrhage
Renal impairment (N=8)Respiratory arrest/distress (not listed above) (N=2)Neurologic damage (not listed above) (N=2), 1 with blindness & deafness
No harm, or outcome not given (N=12)

Enteral to Respiratory or Respiratory to Enteral

Majority = Blood pressure monitors to Intravenous lines
Gas to Intravenous line

Infusion and monitoring systems in healthcare are physiologically not compatible – many cause death if accidently connected to another
Infusion systems rely upon a single, universal connector- the luer tip/small bore connector
Routine tasks such as connecting tubing are at risk for “automatic mode errors”
Connecting Tubing - a high risk activity

Nurses’ Understanding of Tubing Misconnections between Enteral and Intravenous Systems: a
multiple case, explanatory, grounded theory study
July 6, 2011

What do nurses understand about tubing misconnections between enteral
and intravenous systems?

NURSES UNDERSTANDING OF TUBING MISCONNECTIONS BETWEEN ENTERAL AND INTRAVENOUS SYSTEMS
COGNITIVE CONSTRUCTS HUMAN ABILITY
KNOWLEDGE AND EXPERIENCE
ATTENTION CONTROL
EMOTIVE AND PHYSICAL
FACTORS OUT OF CONTROL OF THE NURSE IMPROBABILITY OR PROBABILITY
FATE
CHARACTERISTICS OF THE NURSE PATIENT or FAMILY
TECHNICAL PROPERTIES LABELS
LOCATION OF TUBE
PHYSICAL ATTRIBUTES PUMP, CONNECTOR AND SYRINGE
COLOR AND CONSISTENCY OF FLUID
WORK ENVIRONMENT LIGHTING
CHAOS
SHIFT CHANGE
POLICIES, SUPPLIES AND COST

Findings Cognitive Constructs Nurses have a wide variation in their knowledge
regarding the occurrence of tubing misconnections.
Limits on human ability, factors that nurses cannot control, and characteristics of the nurse, patient, and family may contribute to tubing misconnections.

Findings
Work Environment Multiple organizational practices do not support the
mental work of nurses. Healthcare has not applied common safety concepts to
the work environment.
Technical Properties Some nurses rely on physical attributes of attributes of
devices to cue them to make tubing connections. Others report that relying on such cues may lead to misconnections.

Future Research Cognitive Constructs Nursing education research : How do you imbed generic safety
knowledge within the nursing workforce? How can we improve human (nursing) ability to provide safe and
effective patient care in the face of complexity in healthcare?
Work Environment How can the work environment and organizational practices be
modified to support the work of nurses?
Technical Properties How do nurses’ attach meaning to common medical devices and
tasks? What design features of healthcare devices support nurses’ cognitive
work?

“This label has a good purpose.”
“This label is stupid.”
Variation in Understanding safety
Overarching Conclusions Nurses do not conceptualize making a tubing
connection as a linear process. Nursing has not assimilated basic safety principles
into practice. Factors related to the cognitive constructs of
nurses, the work environment, and technology properties are pervasive and create an environment that may be deadly for patients.

Human Factors the study of interrelationships between humans, the tools they use, and the environment in which they live and work
Used to design safer and more effective systems Commonly used in industry
(aviation,nuclear,chemical,production) Used in critical incident analysis
- 9/11, Chernobyl, Challenger, Three Mile Island

Human Factors
Cognitive Behavioral Individual Industrial Organizational Cultural
How do we make healthcare
errors?

Cognitive Psychology :The way we think and problem solve 1) Planning - gather information2) Storage – process information 3) Execution – make a decision

Memory Ability to store, retain, and subsequently
recall information Three main stages in the formation and
retrieval of memory:– Encoding (processing and combining of received information)
– Storage (creation of a permanent record of the encoded information)
– Retrieval/Recall (calling back the stored information in response to some cue for use in some process or activity)

Sensory Associations to Memory
Tying ribbon or string around a finger is the iconic mnemonic device for remembering a particular thought, which one consciously trains oneself to associate with the string.

Error Modes
Automatic ModeSlips Lapses
Non Automatic ModeMistakes

Automatic Mode –the state of mind where familiar actions take place effortlessly
Unconscious actions Are frequent in common familiar tasks Can not be escaped

Automatic Mode:
Slips- errors that occur during familiar actions and are governed by familiar impulses incorrect execution of a planned action occur when you automatically do something that you didn't mean to do
(Locking the keys in the car)

Habit Interruptions Hurry Fatigue
Anger Anxiety Boredom Fear
Causes of Slips and Lapses


Please comment
FDA Issues Feeding Tube Misconnection Guidance Document
To help combat the deadly problem of tubing misconnections, the U.S. Food ... manufacturers weigh the risk of small-bore connectors for enteral feeding tubes.
www.aami.org/news/2012/073012_connector.html

Van Der Shaf- modified for healthcare
Technical
Organizational
Human Factors
Adequate defenses
Return to Normal
Developing Errors
Near Miss
Dangerous Situation
Dangerous Situation
ERROR(Inadequate Defenses)
ERROR(Inadequate Defenses)

Managing Risk – The Three BehaviorsDavid Marx
Reckless Behavior
Intentional Risk-Taking
Manage through:
Disciplinary action
At-Risk Behavior
Unintentional Risk-Taking
Manage through:
Understanding our at-risk behaviors
Removing incentives for at-risk behaviors
Creating incentives for healthy behavior
Increasing situational awareness
Normal Error
Product of our current system design
Manage through changes in:
Processes
Procedures
Training
Design
Environment

Ooppps!!!!!!