Embed Size (px)
Citation preview

Volume 33, Issue 7 Summer 2015 SjogrensSyndromeFoundation @MoistureSeekers
In This Issue 5 Sjögren’s & Dry Eye 9 Dry Eye Glossary 12 In Memory & Honor 14 You Stood Up
continued page 2 t
continued page 8 t
As part of the Sjögren’s Syndrome Foundation’s (SSF) ongoing initiative to develop the first-ever U.S. Clinical Practice Guidelines (CPG) for Sjögren’s– we are proud to an-nounce that our Ocular Guidelines have been finalized and published. These guide-
lines, the “Ocular Management in Sjögren’s” will help to ensure the quality and consistency of care for the assessment and management of Sjögren’s patients who suffer from dry eye.
In 2010, the SSF initiated the development of clinical guideline recommendations for medical practitioners in three categories: rheumatology, oral medicine/dentistry and eye care providers. These guidelines are being developed by various committees of healthcare profes-sionals who each have taken on a different aspect of Sjögren’s – including systemic, ocular and oral manifestations.
Sjögren’s Syndrome Foundation Releases Clinical Practice
Guidelines for Ocular Management in Sjögren’s Patients
SSF Leaders Presented SSF’s Clinical Practice Guidelines during International Symposium
13thINTERNATIONALSYMPOSIUM ONSJÖGREN’SSYNDROME
Taking place every two years, the International Sympo-sium on Sjögren’s Syndrome (ISSS) brings together researchers and clinicians from around the world. This
symposium is the only scientific meeting that brings together a collaboration of rheumatologists, eye care providers, den-tists and researchers to present the latest scientific research and discuss clinical findings for Sjögren’s.
This four day conference, chaired by Roland Jonsson DMD, PhD, in Bergen, Norway began on May 19th and fea-tured numerous presentations on the various manifestations of Sjögren’s. This year, the Sjögren’s Syndrome Foundation (SSF) was honored to be invited to present the SSF’s work on developing the first-ever Clinical Practice Guidelines (CPG) for Sjögren’s. The presentation was given by four esteemed SSF volunteer medical leaders – Dr. Fred Vivino, Dr. Steven Carsons, Dr. Stephen Pflugfelder and Dr. Michael Brennan. These guidelines will help standardize patient care in the

The Moisture Seekers® Newsletter is published by the Sjögren’s Syndrome Foundation Inc., 6707 Democracy Blvd., Ste 325; Bethesda, MD 20817.
Copyright ©2015 Sjögren’s Syndrome Foundation Inc. ISSN 0899-637.
DISCLAIMER: The Sjögren’s Syndrome Foundation Inc. in no way endorses any of the medications, treat-ments, or products mentioned in advertisements or articles. This newsletter is for informational purposes only. Readers are advised to discuss any research news, drugs, treatments or products mentioned herein with their health care providers.
Board of DirectorsChairman of the Board
Ken Economou
Chairman-ElectStephen Cohen, OD
TreasurerVidya Sankar, DMD, MHS
SecretaryJanet E. Church
Immediate Past ChairmanS. Lance Forstot, MD
Esen K. Akpek, MDHerbert Baraf, MD, FACP, MACR
Pamela S. BrownNancy L. Carteron, MD, FACR
Jack Faricelli Denise Faustman, MD, PhD
Tricia GoodingCathy Ingels
Theresa Lawrence Ford, MDCynthia Lopynski
Mary McNeilKathy L. Sivils, PhD
Medical & Scientific Advisory Board
ChairmanDenise Faustman, MD, PhD
Esen Akpek, MDRichard Brasington, MD, FACRMichael Brennan, DDS, MHS
Steven E. Carsons, MD*Nancy L. Carteron, MD, FACR
Troy Daniels, DDS, MS*H. Kenneth Fisher, MD, FACP, FCCP
Gary Foulks, MD, FACSTheresa Lawrence Ford, MD
S. Lance Forstot, MDPhilip C. Fox, DDS*
Robert I. Fox, MD, PhD, FACP*Tara Mardigan, MS, MPH, RD
Austin Mircheff, PhDJohn Daniel Nelson, MD, FACS
Kelly Nichols, ODAthena Papas, DMD, PhD
Ann Parke, MDAndres Pinto, DMD
Nelson Rhodus, DMD, MPHVidya Sankar, DMD, MHSDaniel Small, MD, FACP
Neil Stahl, MDFrederick B. Vivino, MD, FACR
Jeffrey Wilson, MD, FACR
Chief Executive OfficerSteven Taylor
Director of Marketing/EditorElizabeth Trocchio
e-mail: [email protected] www.sjogrens.org
Founded by Elaine K. Harris in 1983
The work continues on 16 systemic manifestation guidelines and oral guidelines will each be published as they are finished and peer reviewed over the next year and coming years. The first set to be completed and peer reviewed is our ocular guidelines and we know you join with us in celebrat-ing this momentous milestone for the Foundation but most importantly for Sjögren’s patients!
SSF Ocular Guidelines Process:In creating the ocular guidelines, the 2007 report of the International
Workshop on Dry Eye (DEWS) was used as a starting point for panels of eye care providers and consultants to evaluate peer-reviewed publications and develop recommendations for the evaluation and management of dry eye disease associated with Sjögren’s. The publications were graded accord-ing to the American Academy of Ophthalmology Preferred Practice Pattern guidelines for level of evidence and the strength of recommendation was according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) guidelines. Final recommendations were then de-veloped using a Delphi process, which relies on a panel of experts answering questionnaires in two or more rounds.
The process of developing these guidelines was extremely rigorous and time consuming for the SSF and all the physicians who donated their time.
SSF Ocular Guidelines Symptom Evaluation Findings:The ocular CPG established that in a given patient, the clinician must
first determine whether the dry eye is due to inadequate production of tears (aqueous-deficient dry eye), excess evaporation, or a combination of both. The success of a treatment option depends upon this proper recognition and approach to therapy. Evaluation of a patient’s symptoms should be determined through a number of questionnaires that grade severity of symptoms. Practical considerations recommend the use of three specific questions (Table 1).
“Guidelines for Ocular Management” continued from page 1 t
continued page 6 t
Table 1
Key screening questions for dry eye disease. A patient reporting ‘Yes’ to any of the following warrants a full ocular examination
l How often do your eyes feel dryness, discomfort, or irritation? Would you say it is often or constantly? (Y/N)
l When you have eye dryness, discomfort, or irritation, does this impact your activities (e.g. do you stop or reduce your time doing them)? (Y/N)
l Do you think you have dry eye? (Y/N)
2 Summer 2015 / The Moisture Seekers

Available by prescription only.
Make your eyes your priority—call your optometrist or ophthalmologist, ask to get screened, and see if RESTASIS® is right for you.
Call your eye doctor and ask to get screened for Chronic Dry Eye disease caused by reduced tear production due to infl ammation.
Ask about RESTASIS® (Cyclosporine Ophthalmic Emulsion) 0.05%.
BE YOUR OWN ADVOCATE
® marks owned by Allergan, Inc. © 2015 Allergan, Inc., Irvine, CA 92612, U.S.A. APC66DP15
RESTASIS® is the only prescription treatment for this type of Chronic Dry Eye disease. You can use artifi cial tears for temporary relief, but they cannot help you make more of your own tears. Only continued use of RESTASIS® twice a day, every day, can help you make more tears. Individual results may vary.
Approved UseRESTASIS® Ophthalmic Emulsion helps increase your eyes’ natural ability to produce tears, which may be reduced by infl ammation due to Chronic Dry Eye. RESTASIS® did not increase tear production in patients using anti-infl ammatory eye drops or tear duct plugs.
Important Safety InformationDo not use RESTASIS® Ophthalmic Emulsion if you are allergic to any of the ingredients. To help avoid eye injury and contamination, do not touch the vial tip to your eye or other surfaces. RESTASIS® should not be used while wearing contact lenses. If contact lenses are worn, they should be removed prior to use of RESTASIS® and may be reinserted after 15 minutes. The most common side effect is a temporary burning sensation. Other side effects include eye redness, discharge, watery eyes, eye pain, foreign body sensation, itching, stinging, and blurred vision.You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.fda.gov/medwatch, or call 1-800-FDA-1088.Please see next page for the Brief Summary of the full Product Information.Call 1-866-271-6242 for more information.
Make more of your own tears.
TO GET DRY EYE ANSWERS,
Are you using arti� cial tears often?
Could you have a disease called Chronic Dry Eye, caused by reduced tear production due to in� ammation?
Have you called your optometrist or ophthalmologist, asked to get screened, and seen if RESTASIS® is right for you?
Go to restasis.com.Take the Dry Eye Quiz and show the results to your eye doctor.
BE YOUR OWN ADVOCATE
TO GET DRY EYE ANSWERS,TO GET DRY EYE ANSWERS,
Are you using arti� cial tears often?
Could you have a disease called Chronic Dry Eye, caused by reduced
Have you called your optometrist or ophthalmologist, asked to
APC66DP15_RSTSAd_Advocate_MoistreSeekrs.indd 1 5/14/15 12:40 PM

RESTASIS® (Cyclosporine Ophthalmic Emulsion) 0.05%BRIEF SUMMARY—PLEASE SEE THE RESTASIS® PACKAGE INSERT FOR FULL PRESCRIBING INFORMATION.INDICATION AND USAGERESTASIS® ophthalmic emulsion is indicated to increase tear production in patients whose tear production is presumed to be suppressed due to ocular inflammation associated with keratoconjunctivitis sicca. Increased tear production was not seen in patients currently taking topical anti-inflammatory drugs or using punctal plugs.CONTRAINDICATIONSRESTASIS® is contraindicated in patients with known or suspected hypersensitivity to any of the ingredients in the formulation.WARNINGS AND PRECAUTIONSPotential for Eye Injury and ContaminationTo avoid the potential for eye injury and contamination, be careful not to touch the vial tip to your eye or other surfaces.Use with Contact LensesRESTASIS® should not be administered while wearing contact lenses. Patients with decreased tear production typically should not wear contact lenses. If contact lenses are worn, they should be removed prior to the administration of the emulsion. Lenses may be reinserted 15 minutes following administration of RESTASIS® ophthalmic emulsion.ADVERSE REACTIONSClinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.In clinical trials, the most common adverse reaction following the use of RESTASIS® was ocular burning (17%).Other reactions reported in 1% to 5% of patients included conjunctival hyperemia, discharge, epiphora, eye pain, foreign body sensation, pruritus, stinging, and visual disturbance (most often blurring).Post-marketing ExperienceThe following adverse reactions have been identified during post approval use of RESTASIS®. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.Reported reactions have included: hypersensitivity (including eye swelling, urticaria, rare cases of severe angioedema, face swelling, tongue swelling, pharyngeal edema, and dyspnea); and superficial injury of the eye (from the vial tip touching the eye during administration).USE IN SPECIFIC POPULATIONSPregnancyTeratogenic Effects: Pregnancy Category CAdverse effects were seen in reproduction studies in rats and rabbits only at dose levels toxic to dams. At toxic doses (rats at 30 mg/kg/day and rabbits at 100 mg/kg/day), cyclosporine oral solution, USP, was embryo- and fetotoxic as indicated by increased pre- and postnatal mortality and reduced fetal weight together with related skeletal retardations. These doses are 5,000 and 32,000 times greater (normalized to body surface area), respectively, than the daily human dose of one drop (approximately 28 mcL) of 0.05% RESTASIS® twice daily into each eye of a 60 kg person (0.001 mg/kg/day), assuming that the entire dose is absorbed. No evidence of embryofetal toxicity was observed in rats or rabbits receiving cyclosporine at oral doses up to 17 mg/kg/day or 30 mg/kg/day, respectively, during organogenesis. These doses in rats and rabbits are approximately 3,000 and 10,000 times greater (normalized to body surface area), respectively, than the daily human dose.Offspring of rats receiving a 45 mg/kg/day oral dose of cyclosporine from Day 15 of pregnancy until Day 21 postpartum, a maternally toxic level, exhibited an increase in postnatal mortality; this dose is 7,000 times greater than the daily human topical dose (0.001 mg/kg/day) normalized to body surface area assuming that the entire dose is absorbed. No adverse events were observed at oral doses up to 15 mg/kg/day (2,000 times greater than the daily human dose).There are no adequate and well-controlled studies of RESTASIS® in pregnant women. RESTASIS® should be administered to a pregnant woman only if clearly needed.
Nursing MothersCyclosporine is known to be excreted in human milk following systemic administration, but excretion in human milk after topical treatment has not been investigated. Although blood concentrations are undetectable after topical administration of RESTASIS® ophthalmic emulsion, caution should be exercised when RESTASIS® is administered to a nursing woman.Pediatric UseThe safety and efficacy of RESTASIS® ophthalmic emulsion have not been established in pediatric patients below the age of 16.Geriatric UseNo overall difference in safety or effectiveness has been observed between elderly and younger patients.NONCLINICAL TOXICOLOGYCarcinogenesis, Mutagenesis, Impairment of FertilityCarcinogenesis: Systemic carcinogenicity studies were carried out in male and female mice and rats. In the 78-week oral (diet) mouse study, at doses of 1, 4, and 16 mg/kg/day, evidence of a statistically significant trend was found for lymphocytic lymphomas in females, and the incidence of hepatocellular carcinomas in mid-dose males significantly exceeded the control value.In the 24-month oral (diet) rat study, conducted at 0.5, 2, and 8 mg/kg/day, pancreatic islet cell adenomas significantly exceeded the control rate in the low-dose level. The hepatocellular carcinomas and pancreatic islet cell adenomas were not dose related. The low doses in mice and rats are approximately 80 times greater (normalized to body surface area) than the daily human dose of one drop (approximately 28 mcL) of 0.05% RESTASIS® twice daily into each eye of a 60 kg person (0.001 mg/kg/day), assuming that the entire dose is absorbed.Mutagenesis: Cyclosporine has not been found to be mutagenic/genotoxic in the Ames Test, the V79-HGPRT Test, the micronucleus test in mice and Chinese hamsters, the chromosome-aberration tests in Chinese hamster bone-marrow, the mouse dominant lethal assay, and the DNA-repair test in sperm from treated mice. A study analyzing sister chromatid exchange (SCE) induction by cyclosporine using human lymphocytes in vitro gave indication of a positive effect (i.e., induction of SCE).Impairment of Fertility: No impairment in fertility was demonstrated in studies in male and female rats receiving oral doses of cyclosporine up to 15 mg/kg/day (approximately 2,000 times the human daily dose of 0.001 mg/kg/day normalized to body surface area) for 9 weeks (male) and 2 weeks (female) prior to mating.PATIENT COUNSELING INFORMATIONHandling the ContainerAdvise patients to not allow the tip of the vial to touch the eye or any surface, as this may contaminate the emulsion. To avoid the potential for injury to the eye, advise patients to not touch the vial tip to their eye.Use with Contact LensesRESTASIS® should not be administered while wearing contact lenses. Patients with decreased tear production typically should not wear contact lenses. Advise patients that if contact lenses are worn, they should be removed prior to the administration of the emulsion. Lenses may be reinserted 15 minutes following administration of RESTASIS® ophthalmic emulsion.AdministrationAdvise patients that the emulsion from one individual single-use vial is to be used immediately after opening for administration to one or both eyes, and the remaining contents should be discarded immediately after administration.Rx Only
Based on package insert 71876US18 © 2015 Allergan, Inc. Irvine, CA 92612, U.S.A. ® marks owned by Allergan, Inc. APC60WT15 Patented. See www.allergan.com/products/patent_notices Made in the U.S.A.
FILL A RESTASIS® (CYCLOSPORINE OPHTHALMIC EMULSION) 0.05% PRESCRIPTION AND WE’LL SEND YOU A REBATE CHECK FOR $20!* IT’S EASY TO GET YOUR REBATE. JUST FILL OUT THIS INFORMATION AND MAIL.
Follow these 3 steps:1. Have your prescription for RESTASIS® filled at your pharmacy.2. Circle your out-of-pocket purchase price on the receipt.3. Mail this certificate, along with your original pharmacy receipt
(proof of purchase), to Allergan RESTASIS® Ophthalmic Emulsion $20 Rebate Program, P.O. Box 6513, West Caldwell, NJ 07007.
© 2014 Allergan, Inc., Irvine, CA 92612, U.S.A. ® marks owned by Allergan, Inc. Please allow 8 weeks for delivery of your rebate check. APC84HR14 Certificate expires 12/31/2015
Last Name First MI
Street Address
City State ZIP
* RESTASIS® Rebate Terms and Conditions: To receive a rebate for the amount of your prescription co-pay (up to $20), enclose this certificate and the ORIGINAL pharmacy receipt in an envelope and mail to Allergan RESTASIS® Ophthalmic Emulsion $20 Rebate Program, P.O. Box 6513, West Caldwell, NJ 07007. Please allow 8 weeks for receipt of rebate check. Prescriptions dated more than 60 days prior to the postmark date of your submission will not be accepted. One rebate per consumer. Duplicates will not be accepted. See rebate certificate for expiration date. Eligibility: Offer not valid for prescriptions reimbursed or paid under Medicare, Medicaid, or any similar federal or state healthcare program including any state medical or pharmaceutical assistance programs. Offer void where prohibited by law, taxed, or restricted. Amount of rebate not to exceed $20 or co-pay, whichever is less. This certificate may not be reproduced and must accompany your request for a rebate. Offer good only for one prescription of RESTASIS® Ophthalmic Emulsion and only in the USA and Puerto Rico. Allergan, Inc. reserves the right to rescind, revoke, and amend this offer without notice. You are responsible for reporting receipt of a rebate to any private insurer that pays for, or reimburses you for, any part of the prescription filled, using this certificate.
❑ Enroll me in the My Tears, My Rewards ® Program to save more!❑ I am not a patient enrolled in Medicare, Medicaid, or any similar
federal or state healthcare program.For more information, please visit our website, www.restasis.com.
APC66DP15_RSTSAd_Advocate_MoistreSeekrs.indd 2 5/14/15 12:40 PM

RENEW &
ENHANCE.
An Inside Look at Sjögren’s & Dry Eye
Congress officially declared July “Dry Eye Aware-ness Month” in 2005 to help educate the public about chronic dry eye symptoms and treatment
options. During the month of July, the SSF partners with other organizations to help educate ocular professionals about the importance of properly treating patients with dry eyes and the possibility of an underlying medical condition like Sjögren’s.
Chronic dry eye affects millions of Americans and has two main causes: decreased secretion of tears by the lacri-mal glands and loss of tears due to excess evaporation. Both can lead to ocular surface discomfort, often described as feeling of dryness, burning, a sandy/gritting sensation, itchi-ness, visual fatigue, sensitivity to light and blurred vision.
In Sjögren’s, a person’s white blood cells mistakenly invade moisture-producing glands, including the lacrimal glands, causing inflammation and reducing secretion, which causes dry eye to be one primary symptoms of the disease. The challenge is that normal healthy tears contain a complex mixture of proteins and other com-ponents that are essential for ocular health and comfort (see Figures 1&2 below) and this complex mixture is compromised with Sjögren’s.
Figure 1: Normal healthy tears.
Figure 2: Tears of chronic dry eye.
continued page 11 t
As the SSF Ocular Clinical Practice Guidelines (CPG) outline, treatment options for dry eye depends on the cause and severity in each individual patient, and it is important to be examined by an eye care professional who is trained to diagnose and treat ocular diseases – the SSF has also developed a few simple solutions for coping with chronic dry eye.
SSF Dry Eye Survival Tipsl Carry a wet washcloth in a zip-top bag to place on
your dry eyes when traveling.
Summer 2015 / The Moisture Seekers 5

NATURAL SOOTHING SOLUTIONS FOR IMMEDIATE AND LONG-TERM DRY EYE RELIEF.
• Soothing Moist-Heat Therapies for Any Budget
• Hydrating Nighttime and Daytime Shelter
• Moisturizing Skin Therapies Designed for Sensitive Dry Skin
• Doctor Recommended • New Products and Colors
“DEDICATED TO SEEING RELIEF”
www.eyeeco.com888.730.7999
15% Member Discount Online use promo code SSF or call toll-free 888.730.7999
EyeEco_Moisture Ad_05152015.indd 1 5/15/15 1:14 PM
While currently there is no single test to diagnose Sjögren’s, which is one of the reasons that the SSF research program focuses on Novel Diagnostics projects, there are a number of clinical tear function tests that can be performed in an office setting to evaluate dry eye patients and determine the volume and stability of tear function. This includes tear meniscus height and rapid tear film breakup time (TFBUT) and the Schirmer test to find the tear secretion rate that helps differentiate evap-orative dry eye from aqueous-deficient dry eye. A more advanced diagnosis of dry eye can be done by measuring tear film osmolarity. This test may also be used to moni-tor a therapy’s response.
Additional tests include evaluation of the lid blink function and health of the eyelid margin (particularly the meibomian glands) to quantify evaporative dry eye and the application of topical dyes, including fluorescein, rose bengal, and lissamine green, can be used to discover damage to the ocular surface.
SSF Ocular Guidelines Recommendations & Summary:
The algorithm presented in Figure 1 details the options available based upon both a patient’s severity
“Guidelines for Ocular Management” continued from page 2 t level and response to previous therapies. Recommenda-tions show how management of dry eye depends upon the nature of the dry eye and the severity of symptoms, further highlighting why an early Sjögren’s diagnosis and proper treatment is needed to help prevent the disease’s serious complications and improve a patient’s quality of life. As the disease’s severity increases, so does the type of treatment options that should be considered.
In early disease, tear replacement with topically applied artificial tear or lubricant solutions may be sufficient, but progressive or more severe inflammation of the lacrimal gland and ocular surface occur both as an inciting event in many cases and as a secondary effect as the dry eye disease worsens, called keratoconjunctivitis sicca (KCS), which can require the use of dietary supplements (omega 3 essen-tial fatty acids), anti-inflammatory measures (e.g., topical corticosteroids or cyclosporine), or oral secretagogues.
Eye care providers need to be aware that the presence of dry eye may signal the process of Sjögren’s, particular-ly when it is associated with inflammation, difficulty in management, or the presence of dry mouth, fatigue and joint pain. If Sjögren’s is suspected, a physician should re-fer the patient to a rheumatologist for systemic treatment and may refer the patient to other specialties as needed.
continued page 8 t
6 Summer 2015 / The Moisture Seekers

SSF
Clin
ical
Pra
ctic
e G
uide
lines
for
O
cula
r M
anag
emen
t in
Sjö
gren
’sG.
N. F
oulk
s, S.
L. F
orst
ot, P
.C. D
onsh
ik, J
.Z. F
orst
ot, M
.H. G
olds
tein
, M.A
. Lem
p, J.
D. N
elso
n, K
.K. N
ichol
s, S.
C. P
flugf
elde
r, J.M
. Tan
zer,
P. As
bell,
K.
Ham
mitt
, D.S
. Jac
obs,
F. Vi
vino
. For
the
Sjög
ren’
s Sy
ndro
me
Foun
datio
n Cl
inica
l Pra
ctice
Gui
delin
es C
omm
ittee
(CPG
C), B
ethe
sda,
MD,
USA
.
Ab
stra
ctP
urp
ose:
To p
rovi
de a
con
sens
us c
linica
l gui
delin
e fo
r man
agem
ent o
f dry
eye
dise
ase
asso
ciate
d w
ith S
jögr
en d
iseas
e (S
D) b
y ev
alua
ting
publ
ished
trea
tmen
ts a
nd re
com
men
ding
man
agem
ent o
ptio
ns.
Des
ign:
Cons
ensu
s pa
nel e
valu
atio
n of
repo
rted
treat
men
ts fo
r dry
eye
dise
ase.
Met
hod
s:Us
ing
the
2007
Rep
ort o
f the
Inte
rnat
iona
l Wor
ksho
p on
Dry
Eye
(DEW
S) a
s a
star
ting
poin
t, a
pane
l of e
ye c
are
prov
ider
s an
d co
n-su
ltant
s ev
alua
ted
peer
-revi
ewed
pub
licat
ions
and
dev
elop
ed re
com
men
datio
ns fo
r eva
luat
ion
and
man
agem
ent o
f dry
eye
dise
ase
asso
ciate
d w
ith S
jögr
en d
iseas
e. P
ublic
atio
ns w
ere
grad
ed a
ccor
ding
to th
e Am
erica
n Ac
adem
y of
Oph
thal
mol
ogy
Pref
erre
d Pr
actic
e Pa
ttern
gui
delin
es fo
r lev
el o
f evi
denc
e. S
treng
th o
f rec
omm
enda
tion
was
acc
ordi
ng to
the
Gra
ding
of R
ecom
men
datio
ns A
sses
s-m
ent,
Deve
lopm
ent a
nd E
valu
atio
n (G
RADE
) gui
delin
es a
nd re
com
men
datio
ns d
evel
oped
usin
g a
Delp
hi p
roce
ss.
Res
ults
:Ev
alua
tion
shou
ld in
clude
sym
ptom
s of
bot
h di
scom
fort
and
visu
al d
istur
banc
e as
wel
l as
dete
rmin
atio
n of
the
rela
tive
cont
ribut
ion
of a
queo
us p
rodu
ctio
n de
ficie
ncy
and
evap
orat
ive
loss
of t
ear v
olum
e. O
bjec
tive
para
met
ers
of te
ar fi
lm s
tabi
lity,
tear
osm
olar
ity,
degr
ee o
f lid
mar
gin
dise
ase,
and
ocu
lar s
urfa
ce d
amag
e sh
ould
be
used
to s
tage
sev
erity
of d
ry e
ye d
iseas
e to
ass
ist in
sel
ectin
g ap
prop
riate
trea
tmen
t opt
ions
. Pat
ient
edu
catio
n as
to th
e na
ture
of t
he p
robl
em, a
ggra
vatin
g fa
ctor
s, an
d go
als
of tr
eatm
ent a
re
criti
cal t
o su
cces
sful
man
agem
ent.
Tear
sup
plem
enta
tion
and
stab
iliza
tion,
con
trol o
f infl
amm
atio
n of
the
lacr
imal
gla
nds
and
ocul
ar
surfa
ce, a
nd p
ossib
le s
timul
atio
n of
tear
pro
duct
ion
are
treat
men
t opt
ions
that
are
use
d ac
cord
ing
to th
e ch
arac
ter a
nd s
ever
ity o
f dr
y ey
e di
seas
e.
Sum
mar
y:M
anag
emen
t gui
delin
es fo
r dry
eye
ass
ocia
ted
with
Sjö
gren
dise
ase
are
pres
ente
d.
Eva
luat
ion
of D
ry E
ye D
isea
sel
Sym
ptom
s
lSi
gns –
Tear
func
tion
(tear
sta
bilit
y an
d pr
oduc
tion,
tear
com
posit
ion,
osm
olar
ity, i
nflam
mat
ion)
–O
cula
r sur
face
dise
ase
(dye
sta
inin
g)–
Mei
bom
ian
glan
d ev
alua
tion
Man
agem
ent
of D
ry E
yeTr
eatm
ent
algo
rithm
bas
ed u
pon
sev
erity
leve
l and
res
pon
se t
o th
erap
y
Intr
oduc
tion
lTh
e Sj
ögre
n’s
Synd
rom
e Fo
unda
tion
(SSF
) set
abo
ut th
e es
tabl
ishm
ent o
f the
firs
t-eve
r U.S
. Clin
ical P
ract
ice G
uide
lines
inSj
ögre
n’s
to e
nsur
e qu
ality
and
con
siste
ncy
of c
are
for t
he a
sses
smen
t and
man
agem
ent o
f pat
ient
s.
lA
rece
nt s
urve
y of
SSF
mem
bers
reve
aled
that
the
sym
ptom
s of
dry
eye
wer
e th
e m
ost b
othe
rsom
e an
d ac
tivity
-lim
iting
asp
ect
of S
jögr
en’s
dise
ase.
lTh
e de
finiti
on o
f dry
eye
pro
vided
by
the
2007
Inte
rnat
iona
l Dry
Eye
Wor
ksho
p (D
EWS)
repo
rt is:
“Dr
y ey
e is
a m
ultif
acto
rial d
iseas
eof
the
tear
s and
ocu
lar s
urfa
ce th
at re
sults
in sy
mpt
oms o
f disc
omfo
rt, v
isual
dist
urba
nce,
and
tear
film
inst
abili
ty w
ith p
oten
tial
dam
age
to th
e oc
ular
surfa
ce. I
t is a
ccom
pani
ed b
y in
crea
sed
osm
olar
ity o
f the
tear
film
and
infla
mm
atio
n of
the
ocul
ar su
rface
.”
lDr
y ey
e is
usua
lly c
lass
ified
into
two
maj
or c
ateg
orie
s: aq
ueou
s-de
ficie
nt d
ry e
ye, i
n w
hich
tear
pro
duct
ion
is re
duce
d, a
nd e
vap-
orat
ive
dry
eye,
in w
hich
the
evap
orat
ion
of th
e te
ar fi
lm is
abn
orm
ally
high
. Bot
h ar
e as
socia
ted
with
Sjö
gren
dise
ase.
lIn
flam
mat
ion
of th
e la
crim
al g
land
and
ocu
lar s
urfa
ce o
ccur
bot
h as
an
incit
ing
even
t in
man
y ca
ses
and
as a
sec
onda
ry e
ffect
as th
e dr
y ey
e di
seas
e w
orse
ns, p
rom
ptin
g th
e na
me
as k
erat
ocon
junc
tiviti
s sic
ca (K
CS).
Dry
eye
asso
ciate
d w
ith S
jögr
en d
iseas
ein
volv
es g
reat
er s
ever
ity o
f aqu
eous
-defi
cient
dry
eye
as
wel
l as
grea
ter i
nflam
mat
ion.
lM
anag
emen
t stra
tegy
invo
lves
the
grad
atio
n of
sev
erity
of t
he d
ry e
ye b
ased
upo
n le
vel o
f disc
omfo
rt, in
terfe
renc
e w
ith a
ctiv
i-tie
s of
dai
ly liv
ing,
deg
ree
of c
linica
lly o
bser
vabl
e in
flam
mat
ion,
and
resp
onse
to p
revi
ous
ther
apy.
lAn
est
imat
ed 2
0 m
illio
n Am
erica
ns h
ave
dry
eye,
so
eye
care
pra
ctiti
oner
s w
ill fr
eque
ntly
enco
unte
r pat
ient
s w
ith d
ry e
ye s
ymp-
tom
s. It
is cr
itica
l to
cons
ider
Sjö
gren
dise
ase
in o
ne’s
dry
eye
patie
nts
and
refe
r the
m to
a rh
eum
atol
ogist
for d
iagn
osis
and
man
agem
ent.
Met
hod
sl
Ove
rarc
hing
met
hodo
logi
cal p
rincip
les
wer
e tra
nspa
renc
y, in
volv
emen
t of k
ey s
take
hold
ers,
and
cons
isten
cy.
lAm
erica
n Co
llege
of R
heum
atol
ogy
(ACR
) Con
flict
of I
nter
est F
orm
s as
wel
l as
ICM
JE-A
JO F
orm
s w
ere
com
plet
ed b
y al
l par
ticip
ants
.
lBi
as w
as re
duce
d as
muc
h as
pos
sible
by
pre-
defin
ing
para
met
ers
for
liter
atur
e se
arch
es a
nd d
ata
extra
ctio
n fo
r all
sele
cted
arti
cles.
lTo
p ex
perts
in th
eir r
espe
ctiv
e fie
lds
wer
e as
ked
to p
artic
ipat
e by
the
SSF
and
appo
inte
d ch
airs
.
lLi
tera
ture
eva
luat
ing
the
man
agem
ent o
f dry
eye
is li
mite
d an
d es
pecia
lly s
o in
Sjö
gren
dise
ase.
Stu
dies
on
Sjög
ren
dise
ase
patie
nts
are
iden
tified
. Stu
dies
on
non-
Sjö
gren
dise
ase
patie
nts
guid
ed m
anag
emen
tgu
idel
ines
whe
n co
nsid
ered
ess
entia
l or h
elpf
ul.
lPu
blica
tions
wer
e gr
aded
acc
ordi
ng to
the
Amer
ican
Acad
emy
of O
phth
alm
olog
yPr
efer
red
Prac
tice
Patte
rn g
uide
lines
for l
evel
of e
vide
nce.
Con
clus
ion
lTh
e O
cula
r Wor
king
Gro
up re
view
ed th
e ut
ility
of t
ests
use
d fo
r dia
gnos
is an
d di
seas
e se
verit
yan
d re
com
men
ded
guid
elin
es fo
r tre
atm
ent b
ased
on
grad
e of
sev
erity
.
lG
reat
er th
erap
eutic
opt
ions
and
bet
ter u
nder
stan
ding
of t
he c
linica
l cha
ract
erics
that
pred
ict re
spon
se to
thes
e th
erap
ies
now
are
ava
ilabl
e.
lTh
ese
findi
ngs
poin
t to
the
impo
rtanc
e of
con
duct
ing
wel
l-des
igne
d cli
nica
l tria
lsto
pro
vide
gui
danc
e fo
r the
pre
vent
ion
of d
enta
l car
ies.
Dry
eye
dise
ase
–
Aque
ous
defic
ienc
y w
itho
ut m
eibo
mia
n gl
and
dise
ase
Dry
Eye
Dise
ase
–
Aque
ous
defic
ienc
y w
ith
mei
bom
ian
glan
d di
seas
e
Dia
gnos
is
Trea
tmen
t | S
ever
ity L
evel
11
Sev
erity
Lev
el 2
S
ever
ity L
evel
3
Sev
erity
Lev
el 4
E
vid
ence
2 R
ecom
men
dat
ion
3
lEd
ucat
ion
and
envi
ronm
ent/d
iet m
odifi
catio
ngo
od
ST
RO
NG
l
Elim
inat
ion
of o
ffend
ing
syst
emic
med
icatio
ngo
od
ST
RO
NG
l
Artifi
cial t
ears
, gel
s, oi
ntm
ents
good
ST
RO
NG
lO
meg
a 3
esse
ntia
l fat
ty a
cid s
uppl
emen
tm
oder
ate
MO
DER
AT
E S
TR
ON
G
lAn
ti-in
flam
mat
ory
ther
apy:
cyclo
spor
ine
good
M
OD
ER
AT
E S
TR
ON
G
lAn
ti-in
flam
mat
ory
ther
apy:
pulse
ste
roid
sgo
od
MO
DER
AT
E S
TR
ON
G
lPu
ncta
l plu
gsgo
od
MO
DER
AT
E S
TR
ON
G
lSe
cret
agog
ues
good
M
OD
ER
AT
E S
TR
ON
G
lM
oist
ure
cham
ber s
pect
acle
sgo
od
MO
DER
AT
E S
TR
ON
G
lTo
pica
l aut
olog
ous
seru
mgo
od
MO
DER
AT
E S
TR
ON
G
lCo
ntac
t len
ses
good
M
OD
ER
AT
E S
TR
ON
G
lPe
rman
ent p
unct
al o
cclu
sion
good
M
OD
ER
AT
E S
TR
ON
G
lSy
stem
ic an
ti-in
flam
mat
ory
med
icatio
nm
oder
ate
DIS
CR
ET
ION
AR
Y
lEy
elid
sur
gery
good
M
OD
ER
AT
E S
TR
ON
G
lEd
ucat
ion
and
envi
ronm
ent/d
iet m
odifi
catio
ngo
od
ST
RO
NG
l
Elim
inat
ion
of o
ffend
ing
syst
emic
med
icatio
ngo
od
ST
RO
NG
l
Artifi
cial t
ears
with
lipi
d co
mpo
nent
good
ST
RO
NG
l
Eyel
id th
erap
y: w
arm
com
pres
s, m
assa
gego
od
ST
RO
NG
lO
meg
a 3
esse
ntia
l fat
ty a
cid s
uppl
emen
tm
oder
ate
MO
DER
AT
E S
TR
ON
G
lAn
ti-in
flam
mat
ory
ther
apy:
cyclo
spor
ine
good
M
OD
ER
AT
E S
TR
ON
G
lAn
ti-in
flam
mat
ory
ther
apy:
pulse
ste
roid
sgo
od
MO
DER
AT
E S
TR
ON
G
lTo
pica
l azit
hrom
ycin
good
M
OD
ER
AT
E S
TR
ON
G
lLi
poso
mal
spr
aygo
od
MO
DER
AT
E S
TR
ON
G
lPo
ssib
le o
ral d
oxyc
yclin
ego
od
MO
DER
AT
E S
TR
ON
G
lEx
pres
sion
of m
eibo
mia
n gl
ands
good
M
OD
ER
AT
E S
TR
ON
G
lPu
ncta
l plu
gsgo
od
MO
DER
AT
E S
TR
ON
G
lSe
cret
agog
ues
good
M
OD
ER
AT
E S
TR
ON
G
lM
oist
ure
cham
ber s
pect
acle
sgo
od
MO
DER
AT
E S
TR
ON
G
lTo
pica
l aut
olog
ous
seru
mgo
od
MO
DER
AT
E S
TR
ON
G
lCo
ntac
t len
ses
good
M
OD
ER
AT
E S
TR
ON
G
lPe
rman
ent p
unct
al o
cclu
sion
good
M
OD
ER
AT
E S
TR
ON
G
l(L
ipifl
ow p
ulse
d th
erm
al c
ompr
essio
n)in
suffi
cient
D
ISCR
ET
ION
AR
Y
l(P
robi
ng o
f mei
bom
ian
glan
d)in
suffi
cient
D
ISCR
ET
ION
AR
Y
lSy
stem
ic an
ti-in
flam
mat
ory
med
icatio
nm
oder
ate
DIS
CR
ET
ION
AR
Y
lEy
elid
sur
gery
good
M
OD
ER
AT
E S
TR
ON
G
1 As
sum
es u
se o
f the
Inte
rnat
iona
l Dry
Eye
Wor
ksho
p se
verit
y sc
ale
2
Evid
ence
is g
rade
d as
goo
d, m
oder
ate
and
insu
fficie
nt
3 R
ecom
men
datio
ns ra
nge
from
stro
ng, m
oder
ate
stro
ng a
nd d
iscre
tiona
ry
Dis
clos
ures
The
SSF
Clin
ical P
ract
ice G
uide
lines
initi
ativ
e is
fully
fund
ed b
y th
e Sj
ögre
n’s
Synd
rom
e Fo
unda
tion
with
no
corp
orat
e or
pha
rmac
eu-
tical
sup
port.
All
parti
cipan
ts fu
lly v
olun
teer
ed th
eir t
ime
and
com
plet
ed C
onfli
ct o
f Int
eres
t for
ms.
Ack
now
led
gem
ents
Th
e Sj
ögre
n’s
Synd
rom
e Fo
unda
tion
(SSF
) wish
es to
than
k th
e m
embe
rs o
f the
Ocu
lar W
orki
ng G
roup
for v
olun
teer
ing
thei
r tim
e an
d ex
perti
se to
dev
elop
ing
the
SSF
Clin
ical P
ract
ice G
uide
lines
for O
cula
r Man
agem
ent o
f Sjö
gren
’s an
d th
e SS
F Bo
ard
of D
irect
ors
whi
ch s
uppo
rted
this
initi
ativ
e.
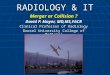
Fig
ure
1Tr
ea
tme
nt a
lgo
rithm
ba
sed
up
on
seve
rity
leve
l and
resp
ons
e to
the
rap
y
Ma
na
ge
me
nt
alg
orit
hm
ba
sed
up
on
de
term
ine
d le
vel o
f se
verit
y o
f d
ry e
ye d
isea
se u
sing
th
e In
tern
atio
na
l Dry
Eye
Wo
rksh
op
se
verit
y sc
ale
. Pro
gre
ssio
n o
f th
era
py
is d
ete
rmin
ed
by
resp
on
se t
o p
rior t
rea
tme
nt
op
tion
. Evi
de
nc
e a
nd
str
en
gth
of
rec
om
me
nd
atio
n a
re
ac
co
rdin
g t
o G
RA
DE
syst
em
.
Summer 2015 / The Moisture Seekers 7

We encourage all patients to share these new guide-lines with their eye care providers and talk to them about the recommended therapies published in these Ocular Clinical Practice Guidelines. Please also encourage them to sign up to receive the SSF’s Sjögren’s Quarterly, our complimentary scientific and medical journal written for healthcare providers. They can sign up by visiting our website at www.sjogrens.org or by calling the SSF office at (301)530-4420. Also, we encourage you to visit www.sjogrens.org to find the most updated information about upcoming SSF Clinical Practice Guidelines and
“Guidelines for Ocular Management” continued from page 6 t
United States by giving rheumatologists, eye care provid-ers, and dentists a road map of how to treat, monitor and manage their Sjögren’s patients. The SSF’s CPGs were displayed as abstract posters during the Symposium.
In addition to be given the opportunity to present our CPGs at the symposium, the SSF’s CEO Steven Taylor and VP of Medical & Scientific Affairs Kathy Hammitt, were invited to take part in a patient panel to highlight the collaboration of 18 international patient groups who are
Dr. Frederick Vivino, SSF Clinical Practice Guide-lines (CPG) Chair, displaying the SSF’s CPG abstract at the 13th International Symposium on Sjögren’s Syndrome (ISSS).
The ISSS luncheon meeting of the International Sjögren’s Network (ISN).
Steven Taylor, SSF CEO, presenting on the International Sjögren’s Network of Patient Groups.
“ISSS” continued from page 1 t
watch future issues of The Moisture Seekers for additional guidelines as they are published.
The Sjögren’s Syndrome Foundation Clinical Practice Guidelines Committee (CPGC): Gary N. Foulks, MD, FACS, S. Lance Forstot, MD, FACS, Peter C. Donshik, MD, Joseph Z. Forstot, MD, FACP, FACR, Michael H. Goldstein, MD, MM, Michael A. Lemp, MD, J. Daniel Nelson, MD, FACS, Kelly K. Nichols, OD, MPH, PhD, Stephen C. Pflugfelder, MD, Jason M. Tan-zer, Dmd, PhD, Penny Asbell, MD, MBA, FACS, Kather-ine Hammitt, MA, and Deborah S. Jacobs, MD. n
working together to increase awareness and research for Sjögren’s. Steven Taylor moderated this panel with Kathy Hammitt representing patients from the United States, Maggy Pincemin representing France and Anne Britt representing Norway. This lively panel was the first time that patients were invited to present at the International Symposium and the SSF was proud to lead this panel.
The SSF was also impressed by the representation by U.S. researchers and clinicians who presented throughout the conference. We would like to thank all of our members and supporters who make it possible for the Foundation to attend and present at key conferences, like the ISSS, so that we can continue to be the leading advocate for those who suffer from Sjögren’s! n
8 Summer 2015 / The Moisture Seekers

Dry Eye GlossaryAqueous-deficient Dry Eye: Disruption of the tear film
because of inadequate secretion of tears or because arter-ies become swollen and damaged.
Autologous Serum (Serum Tears): Autologous describes the fact that it is taken from the patient themselves; serum describes the component of the blood that is used to prepare the drop.
Blepharitis: Inflammation of the eyelids, often decreasing secretions from meibomian glands. Excess evaporation of tears can result, leading to dry eye.
Cornea: The clear dome on the front of the eye that covers the pupil and iris. Clear vision depends on a healthy, undamaged cornea.
Evaporative Dry Eye: Abnormally high evaporation of the tear film.
Lacrimal Glands: Glands that secrete water and most of the important proteins in tears.
Lateral Canthus: Corner of the eye situated laterally or away from the center of the face.
Meibomian Glands: Fat-producing glands in the eyelids that produce and secrete oils, an essential component of tears. These oils form a thin layer on top of the tear film, retarding evaporation.
Meibomian Gland Disease: The major cause of evaporative dry eye. One sign of meibomian gland disease is the pres-ence of foamy debris, particularly at the lateral canthus.
Puncta: Small holes in the eyelids that normally drain tears. Punctal closure allows maximum tear preservation in patients with severe dry eye.
Punctal Plugs: Inserted in the puncta to increase the vol-ume of tears retained on the surface of the eye.
Rose Bengal & Lissamine Green Test: Eyedrops con-taining dyes that an eye care specialist uses to examine the surface of the eye for dry spots.
Secretagogue: A substance/medication that can stimulate another substance (tears & saliva) to be secreted.
Schirmer Test: Measures tear production.
Tear Breakup Test: Measurement of tear breakup time is a standard part of the evaluation of dry eye since instability of the tear film is a characteristic of both queous-deficient and evaporative dry eye.
Tear Film: Protects and lubricates the cornea and the rest of the ocular surface. Natural tears are mostly water contain-ing a complex mixture of proteins and other components.
Tear Osmolarity Test: Measures the concentration of the tear film, which can be elevated in either queous-deficient or evaporative dry eye. n
Summer 2015 / The Moisture Seekers 9

©20
15 O
rtek
The
rape
utic
s, In
c. B
asic
Bite
s is
a re
gist
ered
trad
emar
k of
Ort
ek T
hera
peut
ics,
Inc.
Therapeutics, Inc.
Support your enamel health withBasicBites®... every day
sugar free soft chewsessential for individualswith dry mouth
®
BasicBites® are essential for
individuals with dry mouth.
These delicious soft chews contain a unique, patented blend of vital nutrients that naturally help support enamel health... just like saliva.
The revolutionary technology in
BasicBites Soft Chews was developed
at Stony Brook University School of
Dental Medicine.
•� Landmark� research� identified� beneficial� bacteria� on tooth surfaces. • These helpful bacteria naturally convert a nutrient discovered in saliva (and contained in BasicBItes) � into� tooth� protective� buffers� which� help keep teeth in their existing and healthy pH (acid/base) balance.
• Like healthy saliva, BasicBites also contain calcium to coat and support healthy enamel.
Two delicious BasicBites, every day, work behind the scenes to help maintain enamel health.
Leading dental professionals are recommending BasicBites. See why at www.basicbites.com/testimonials
120� ct-� 2� month� supply� carton,� chocolate-flavored
Only$39.95 2 month supply
Order Today with Free Shipping at basicbites.comor call800 - 863 - 9943
The Seriously Delicious Oral Care Breakthrough* Also an excellent source of calcium.
PRODUCTS 2014
C
M
Y
CM
MY
CY
CMY
K
SjogrensMoistureSeekersFullpgMECHRevised.pdf 6/22/15 1:27:43 PM

™ ® © 2014 MedActive Oral Pharmaceuticals, LLC.
For a list of pharmacies near you,
visit www.medactive.com or call 1-866-887-4867
NEW
• Immediate relief of oral discomfort
• Long-lasting, soft tissue conditioning
• As-needed saliva enhancement
• Supports a balanced flora
• Helps protect tooth enamel
Proudly Made in the U.S.A
Continuum™
A Comprehensive Oral Relief Protocol
Available Exclusively at your Local Independent Community Pharmacy
.
“Sjögren’s & Dry Eye” continued from page 5 t
l Avoid applying anything to the eyelids that can irritate your dry eye; products placed on the eyelid will get into the tear film.
l Sjögren’s patients with dry eye should carefully clean their eyelids with warm water or one of the commer-cially available eyelid cleansers.
l Try sterile eyelid cleansers or baby shampoo on a warm washcloth to help with blepharitis, a common condition in Sjögren’s that can cause chronic inflam-mation of the eyelids and eyelid margins.
l The mainstay of treatment for blepharitis, a chronic condition that accompanies dry eye and Sjögren’s, is warm compresses, lid massage and lid hygiene. If the blepharitis is acute, you might need a prescription antibiotic ointment.
l If your eyes are bothered by light, wear sunglasses or try lenses with a FL-41 filter.
l Use non-preserved artificial tears frequently and regularly, even when your eyes feel good. The goal is to keep your eyes comfortable, not to wait until they are uncomfortable.
l Keep the upper and lower eyelids free of facial creams at bedtime; they can enter the eye and cause irritation.
l Dry eye patients often develop or aggravate their envi-ronmental allergies. An over-the-counter allergy drop (even if preserved) used twice daily may help.
l Try ointments or gels at bedtime by first applying them only to the eyelids and lashes. If that is not helpful, place ~1/4 inch of ointment between the lower lid and eyeball.
l Eye ointments and gels can blur your vision and are usually reserved for overnight use.
l For dry eye, apply a warm, wet compress to the closed eyes using a washcloth. Apply at bedtime and upon awakening for 5 minutes, or more often if helpful.
l If your vision is blurred with artificial tear use, try a less thick (viscous) drop or ointment.
l Try moisture chamber glasses, wrap-around sunglass-es, or other glasses, goggles or shields to prevent mois-ture evaporation and offer protection from air currents that irritate your dry eye. n
Summer 2015 / The Moisture Seekers 11

Each fall your local United Way, Combined Federal Campaign, state
employee, and private employer payroll deduction campaigns begin.
We hope you will remember the Sjögren’s Syndrome Foundation when
choosing where to allocate your donation. (CFC #10603)
If we are not listed on the contribution form, you usually may write in
the Sjögren’s Syndrome Foundation.
Tell your co-workers, friends, and family members how important it
is to choose and write in the Sjögren’s Syndrome Foundation on their
campaign form, too.
If your employers will not allow you to write in the Sjögren’s
Syndrome Foundation, remind them that we are a national non-profit
501(C3) organization and qualify for most payroll deduction campaigns.
If they need more information, please contact the Foundation at
800-475-6473.
Just think – every dollar counts.
Last year alone – thanks to those who chose to give through their
employer’s payroll campaign – the Sjögren’s Syndrome Foundation was
able to increase its Research and Awareness commitments.
Remember, the Foundation has received the:
IT’S TIMEUnited Way • Combined Federal Campaign • State Payroll Deduction
In Memory of Barbara BirminghamMr. and Mrs. Romeo BunagMr. and Mrs. Teddy Puchala
Richard and Pat ZdanClaudia and Rich Kerbel
In Memory of Bonnie LittonKathy Hammitt
In Memory of Carol BogolMary Ellen Mitch
In Memory of Dennis Brintle Reid and Debbie Link
In Memory of Dolores B Ayotte Cecile Charpentier
Clayton AyotteJeremi Kahmke and Client Services Team
In Memory of Donald L GebhardtJohn and Luella Lokemoen
Mr. and Mrs. UlibarriWillis and Sherie Kelly
In Memory of Doris Zemaitis BauerW. J. Bauer
In Memory of Dr. Edmund C. BurkeDavid and Priscilla Sohn
In Memory of Edna Lee ParsonsBetty BurkemperDarlene March
Judy GrannemannLeona and Robert Forbeck
Page and Tina WagnerRay and Sherry Diederich
Suzanne SimkoIn Memory of Faye Eddins
Holy Cross Board of Directors Terri and Carol
In Memory of Gail HenleyJohn and Marie Benjamin
McDonald FamilyMr. and Mrs. James Oslin
Richard and Marjorie FisherIn Memory of George Jacobs
Barbara LevinJoan Goldberg
Scott and Debbie RudinIn Memory of Henrietta Hughes
Barbara and John DayEdward and Margaret DemeterLinda Coladonato and Joe Erb
Marie and Roger KingIn Memory of Margaret Spencer
Dane and Sharon AdamsDorothy BollingerLarry Wilson BRAS
Martin and Susan AckermannWilliam and Kathleen Reed
In Memory of Mary Ann Kern DickBobette Morgan
In Memory of Norm Talal, MD, PhD Kathy Hammitt
In Memory of Penny Hammond WolkSherree Meyers
In Memory of Sally ThorntonKathy Hammitt
Sjogren’s Syndrome Foundation San Diego – Imperial Chapter
In Memory of Selena JohnDave and Mary Lou
Gene and Sylvia GourleyIn Memory of Virginia G. Bullard
Dan KumarichGlenn and Dawn Confer
In Honor of Celine KirtsEileen and CJ
In Honor of Lizz ColavitaMoms Club of Abington Township
In Honor of Lydia Spiegelman and Beth DilkSue Laslo
In Honor of Marie KirekerMarilyn Yager
In Honor of Mary McNeilPaula and Ian Mercer
In Honor of Penny and Joe O’NeillPat and Ed MeyertholenIn Honor of Sara Camuti
Felicia and Dominick SansottaMarty and Phyllis Ryan
In Honor of Suzanne and Ray Paulson Stephen Cohen, ODIn Honor of Tim Lis
Heather Lis
Rememberyour loved ones and
special occasions with a donation to
the SSF in their name.
12 Summer 2015 / The Moisture Seekers

FInal Page 1Sjögren’s Syndrome FoundationNPC Audio CD Order Form: 8.5” x 11” – full bleed C M Y K
v 9 4 1 . 4 7 9 . 4 3 4 9
e p r o d u c t i o n @ r e d g r a s s - s t u d i o s . c o m SSF_15138.03
Non- Member Member Qty. Total
Special Panel Discussion & Overview: Systemic, Ocular and Oral Manifestations of Sjogren’s (2 hour CD) by Frederick Vivino, MD, MS, Stephen Cohen, OD, and Vidya Sankar, DMD, MHS. $40 $25
Neurological Complications and Sjogren’s by Julius Birnbaum, MD, MHS $30 $18
Treatment of Major Organ System Involvement in Sjogren’s by Daniel Small, MD $30 $18
Understanding the Otolaryngologic Manifestations of Sjogren’s by Myron B. Jones, MD $30 $18
Vaginal Issues and Sjogren’s by Colin MacNeill, MD $30 $18Maryland Residents add 6% sales tax
Shipping and Handling:U.S. Mail: $5 for first item + $1 for each additional itemCanada: $14 for first item + $1 for each additional itemOverseas: $22 for first item + $1 for each additional item
Total Amount Due
o Enclosed is a check or money order (in U.S. funds only, drawn on a U.S. bank, net of all bank charges) payable to SSF.
o MasterCard o VISA o Discover o AmEx Card Number __________________________________________________________________________________________________
Exp. Date ____________________ Security Code _________________ Signature ___________________________________________________________________________________________
Mail to SSF: BB&T Bank • PO Box 890612 • Charlotte, NC 28289-0612 or Fax to: 301-530-4415
Name ________________________________________________________________________________________________________
Address ______________________________________________________________________________________________________
City ________________________________________________________ State ___________ Zip ______________________
Telephone ______________________________ E-Mail _________________________________________________________
Missed the 2015 Conference?Get all the vital information you need on audio CD!
Four of our most popular talks from the 2015 National Patient Conference held in Tampa, Florida, are available for purchase as audio CDs. Each talk is 30-40 minutes long and comes with the handouts used by the presenter.
In addition to the individual talks, you can purchase the conference kick-off session, a two-hour overview of Sjögren’s, its manifestations and treatment options.
Buy just the talks you want to hear or purchase the whole set!
Learning to Thrive with Sjögren’s
Learning to Thrive with Sjögren’s
2015 National Patient Conference

The Sjögren’s Syndrome Foundation’s fiscal year end-ed on June 30th, and because of you standing up to Sjögren’s, we had an incredibly successful year.
It’s your help that allows the Foundation to continue to grow year after year! The SSF 2015-2016 National Event calendar will be released shortly, but you can view the first few events on the back of this issue.
The Foundation wants to thank everyone who stepped up by attending, volunteering or donating to one of our events over this past year! By working together with the many volunteers and participants in each community, our events alone raised over $500,000 to support the SSF’s scientific initiatives, research & patient programs. These SSF National Events included: l Union Brewhouse Golf Tournament – September 8, 2014l Brendanwood Financial Golf Tournament – September 12, 2014 l Cycle for Sjögren’s – September 13, 2014l Vermont Rockin’ Trail Run &Walk – October 4, 2014l Harrisburg Walkabout – October 18, 2014l Mysterious Comedy Night – November 1, 2014l Nashville Area Walkabout – November 8, 2014l Capital Region Walkabout – November 15, 2014l Chicago Area Streams in Desert Trivia – November 15, 2014l Boston Sip for Sjögren’s – November 16, 2014l Disneyworld Marathon & 10K – January 9-11, 2015 l Phoenix Walkabout & Health Fair – February 21, 2015l New York City Sip for Sjögren’s – March 16, 2015l National Patient Conference (NPC) – April 17-18, 2015 l Tampa Walkabout – April 18, 2015 l Philadelphia Walkabout & Health Fair – May 2, 2015l Dallas Walkabout & Health Fair – May 16, 2015l Northeast Ohio Walkabout – May 30, 2015l Atlanta Sip for Sjögren’s – May 31, 2015l Denver Walkabout – June 6, 2015l Greater Washington Region Walkabout & Health Fair –
June 13, 2015
You Stood Up!SSF Members Stand Up Around the Country
Thank you to our National Sponsor

And a special thank you to everyone who achieved our “Sjögren’s Star Status” by raising over $1,000 for an SSF Walkabout! View our Sjögren’s Stars on www.sjogrens.org.

The Moisture SeekersSjögren’s Syndrome Foundation Inc.6707 Democracy Blvd., Ste 325Bethesda, MD 20817
Phone: 800-475-6473 Fax: 301-530-4415
If you would like to receive this newsletter but are not currently an SSF Member, please contact us! 800-475-6473
Join in the fun! 2015 SSF Fall Event Calendar
sip for
a fine water tasting event
September 5-6 Team Sjögren’s
Disneyland Half-Marathon or 10K Anaheim, California
13 Cycle for Sjögren’s Marsh Jr. High School Chico, California
October 3 Nashville Area Walkabout
More information will be posted on the SSF website 10 Rockin’ Trail Run 10K or 5K
Niquette Bay State Park, Vermont 17 Harrisburg Walkabout
Harrisburg Mall Harrisburg, Pennsylvania
18 Northern Virginia Sip for Sjögren’s Frying Pan Farm Park Auditorium Herndon, Virginia
The SSF is very excited for all of our events coming this Fall. Look at our special event calendar below to see if there is an event coming to your area.
For us to grow and continue to fight for patients, we need volunteers to help us organize SSF events. If you are interested in getting involved, please contact Ben Basloe at (301) 530-4420 x207 or [email protected].